Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR.
|
|
|
- Ashley Mills
- 5 years ago
- Views:
Transcription
1 Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR. TOM HOPKINS 1
2 Learning Objectives Describe the Duke University Health System Care Redesign performance improvement approach Describe the key interventions and outcomes from the Care Redesign work Describe the prioritization methodology to select focus areas 2
3 Agenda Background of Care Redesign work at Duke Program management: Improvement process Intervention examples Performance reporting Communication tools Prioritization methodology to select new projects Case study Future directions Q&A 3
4 BACKGROUND 4



5 Care Redesign Background - Beginning FY12: Oversight Committee formed to govern changes Aims: Improving outcomes and experience of care Improving the health of populations Reducing the cost of care Key Lessons Avoided days in the hospital Reduced unplanned returns Opportunity identification could be more systematic FY13: Convened 7 clinical teams Primarily Cardiac and Orthopedic (2 bundled payment pilots) FY14: Convened 9 additional teams Surgical, Medical, GYN, Peds Projects took months Partnership to analyze clinical cost data and track financial benefits could be expanded 5

6 Care Redesign Background Phase FY14-FY15: Transforming our Future Care Redesign Project Consultant engagement Projects identified based on largest variation in variable direct cost/case Guided teams through 16 Week Design process and 16 Week Implementation process FY16 to Current: Duke Care Redesign Program Team of industrial engineers, healthcare business professionals and quality improvement nurses hired and based in Performance Services Partnership with Epic (EHR), Patient education, Research Services, and Finance Developed annual assessment process to target projects based on health system priorities Project schedules based on scope and deliverables, using Six Sigma improvement methodology 6
7 Project Teams To Date Developed a redesign approach Then a program Now tackling even bigger areas July 2012 June 2014 Clinical Teams FY13: Prepare for Bundled Payments PCI CHF Total Hip Total Knee Hip Fracture CVA TIA FY14: Spread Outcomes/Waste Improvement Afib Ablation CABG Cardiac Valve Replacement Bariatric Surgery Total Laparoscopic Hysterectomy Cystectomy Colorectal Surgery Peds Asthma COPD Exacerbation Wave 1 January 2014 June 2017 Clinical Teams Hip and Knee: Next Wave of Improvements Septicemia - Adult Hematological Malignancies Spine Wave 2 Complex ICU Adult Complex ICU and Septicemia - Peds Neonatology Obstetric Deliveries Wave 3 Heart Transplant and VAD Kidney and Liver Transplant Pediatric Cardiac Surgery Wave 4 PCI + Diagnostic Cath: Next Wave of Improvements Cerebrovascular Disease: Next Wave of Improvements Renal Failure Wave 5 Colorectal Surgery: Next Wave of Improvements Lung Transplant Psychological and Behavioral Disorders Wave 6 Nephrectomy and Prostatectomy July Clinical Teams Spring FY17 Lower Extremity Wound and Amputation OR Utilization Improvement Infusion Denials Improvement Cardiac Bundled Payment Preparation (AMI and CABG) Fall FY18 Inpatient Imaging Appropriateness Avoiding Outliers in Length of Stay Delirium Management and Prevention Inpatient Mobility Improvement
8 IMPROVEMENT PROCESS 8
9 Care Redesign Summary Why? What do we do? How do we do it? What results have we achieved? To improve quality and experience outcomes for our patients To improve value for our patients To simplify and streamline processes Guide redesign efforts for identified patient populations across the health system Bring expertise related to project management, quality improvement, and change management Pair members of our team with clinical leaders and process experts of the identified populations to facilitate improvement work Complete data analysis, stakeholder interviews, and process maps Determine project goals, identify key drivers, brainstorm and select solutions Develop solutions Implement and monitor results Improvements for patients and care teams across 30+ teams Demonstrated LOS and cost savings Collaboration with electronic health record and Research Services to develop cutting edge solutions Developed an annual assessment process to select future projects 9


10 The How of Care Redesign The Magical Combination Clinicians Staff Care Redesign Project Manager Clinical Expertise + Process Expertise + Project Management, Quality Improvement, and Change Management Expertise = 10
11 Team Co-Leads and Project Managers are Assigned at Project Launch Care Redesign Team Co-Leads Physician and Nurse Serves as the clinical expert for the care redesign population Identifies multidisciplinary membership and key stakeholders Establishes professional, collaborative, inclusive atmosphere for the team Ensures that evidence and leading practice are incorporated throughout the design phase Serves as the bridge to build system-wide relationships and consensus among physicians and nurses in partnership with hospital-level physician and nurse leads Uses/supports data to focus initiatives and drive care redesign Supports the identification and prioritization of initiatives Presents team status to Oversight Committee Care Redesign Project Manager Manages project and guides team through improvement process: Schedules and facilitates meeting Communicates and follows up on action-items between meetings Analyzes data to identify key drivers Collaborates with Core Team and Sub-Team members to design and document future state Supports Care Redesign Team Co-Leads in identification of risks and barriers Develops performance reports and targets with team Manages implementation of care redesign elements Page 11
12 Program Leadership Partners Care Redesign Medical Director Acts as physician leader to break down organizational barriers, address issues raised by peer clinician leaders and shepherd project through appropriate clinical committees Mentors Clinical Team co-leads Works with co-leads to ensure clinical guidelines incorporate latest evidence Collaborates with Project Manager and Care Redesign Program Leads to refine project scope and to ensure interventions are likely to achieve targeted impacts Nursing Lead Mentors team co-leads and ensures nurse involvement across DUHS Communicates progress to DUHS nursing leadership and facilitates CPC approval process Facilitates collaboration with patient and staff education Coordinates with nursing informatics to ensure appropriate integration of Care Redesign workflows with Epic 12
13 Other Key Partners Involved with Projects Each team is partnered with a representative from: Epic provider builder Research services Clinical education and professional development Finance Multidisciplinary core team is assembled with members from Providers, Physicians, Ancillary Services (pharmacy, case management, PT, OT, pharmacy, respiratory therapy, etc), Patient Education, Patient Advisory Council member 13
14 Improvement Process Analyze current state process and data; Conduct staff and patient interviews; Gather best practice evidence; Identify key drivers; Launch Core Team Validate key drivers and establish subteams; Brainstorm improvement strategies with subteams; Create prioritized list of initiatives; Develop initiatives Complete initiative design; Develop key performance indicators; Finalize any pilot plans Develop implementation plan, that includes communication and staff education plan; Finalize SBARs and submit to Epic Implement; Monitor go-live with teams and adjust as needed; Review performance reports; Launch continuous improvement 14 Tollgate sessions setup with project manager and Care Redesign leadership team to assess project direction and discuss any support needed

15 Care Redesign Oversight Committee Responsibilities Membership Provide oversight for the Care Redesign program Review and approve Team Charters Review and approve design initiatives Hold teams accountable to achieve team milestones and performance targets Review progress to ensure redesign initiatives are on track Resolve issues and remove barriers to making progress Support prioritization and phasing of new projects Chief Medical Officer, DUHS (Chair) Executive Vice President, DUHS Chief Nursing Officer, DUHS Hospital Presidents Chief Health Information Officer, DUHS Associate Chief Financial Officer, DUHS Associate VP Performance Services, DUHS Clinical Department Chairs (Ad Hoc) 15

16 Examples of Improvement Tools Used 16
17 INTERVENTION EXAMPLES 17

18 Intervention Examples Patient Impact Theme Intervention Team Improvement of pain control Improvement of time to therapy Strategies to reduce complications Improvement of outpatient access Improvement of patient education and expectations Multimodal pain management Hip and Knee Replacement Development of pain regimes; pain education added to Lung Transplant pre-op class NEWS score and BPA alerting RN Sepsis Efficiency of induction process OB Transfer center workflow design Stroke Sedation protocol PICU, PCICU, Adult ICU Protocol for evaluation of GI hemorrhage Proactive identification of need for dialysis Infection prevention tactics Febrile neutropenia prophylaxis Shifting chemotherapy regimens to outpatient setting Expedited vascular access process Transitional medical home program Patient journey board Careplan in Epic and DUHS education materials Heart Transplant and VAD Renal Failure Adult ICU Hematologic Malignancies Hematologic Malignancies Renal Failure ICN Peds Cardiac Surgery Colorectal Surgery, Urology 18


19 Intervention Examples Care Team Impact Theme Intervention Team Increased data and information available to guide decision making Improvements in workflow and communication Epic clinical data summary view; patient risk assessment and mitigation process Epic clinical data summary view Daily rounding process standards; patient family communication bundle ICU and transplant joint rounds Kidney and Liver Transplant PICU, PCICU, Adult ICU Adult ICU Lung Transplant 19
20 PERFORMANCE REPORTING 20
21 Outcome Performance Reporting 21
22 Team Specific Key Process Metric Reporting Examples 22
23 COMMUNICATION TOOLS 23

24 Communication Tools Project and Program Project Biweekly project updates to coleads and key stakeholders Routine co-lead meetings to discuss project strategy Program Routine meetings with hospital CMOs/CNOs Quarterly updates at hospital leadership councils Monthly Care Redesign Oversight Committee meetings à team report-outs and program updates Featured teams and patient impact stories on Duke Intranet Sharepoint website (*next slide) 24

25 Care Redesign Sharepoint Site Share monthly project updates and key learnings List of all current projects Post implementation toolkits for new staff training Submit new project ideas List and pictures of Care Redesign project managers 25
26 PRIORITIZATION METHODOLOGY TO SELECT NEW PROJECTS 26
27 Annual Project Planning Timeline Winter Fall Fall projects launched Collect project ideas from stakeholders and DUHS leaders Complete variation and external benchmark analysis Spring Care Redesign Oversight Committee sets priorities for upcoming fiscal year Score top ~15 projects with prioritization matrix Spring projects launched Summer Care Redesign Oversight Committee selects projects using prioritization matrix 27
28 Fall Prioritization FY18 Project Matrix Prioritization Summer 2017 # Project Ideas Quality/ Safety Priority Primary Patient Experience Margin Improvement Secondary Ease of Implementation Total - Magnitude of Impact 1 Liver failure Low Low Medium Medium Inpatient imaging utilization Medium High Medium Not Complex Inpatient mobility improvement Medium High High Complex Endoscopy cancellation rate Low High Medium Medium Readmissions - Hospital care transitions model High Medium Medium Complex Rapid IP to OP transition for DPC patients Low Medium Medium Complex Peds Neurology and Neurosurgery LOS Low Medium Low Medium LOS Outlier management Medium Medium High Medium Sepsis High Medium Low Medium Sickle Cell readmissions Low Medium Medium Medium ICN LOS improvements Low Low High Complex Surgical patient flow Medium Medium Medium Complex Tracheostomy Low Medium High Complex Delirium management and prevention High Medium High Complex Avoidable ED Utilization Medium High Low Medium
29 CASE STUDY 29

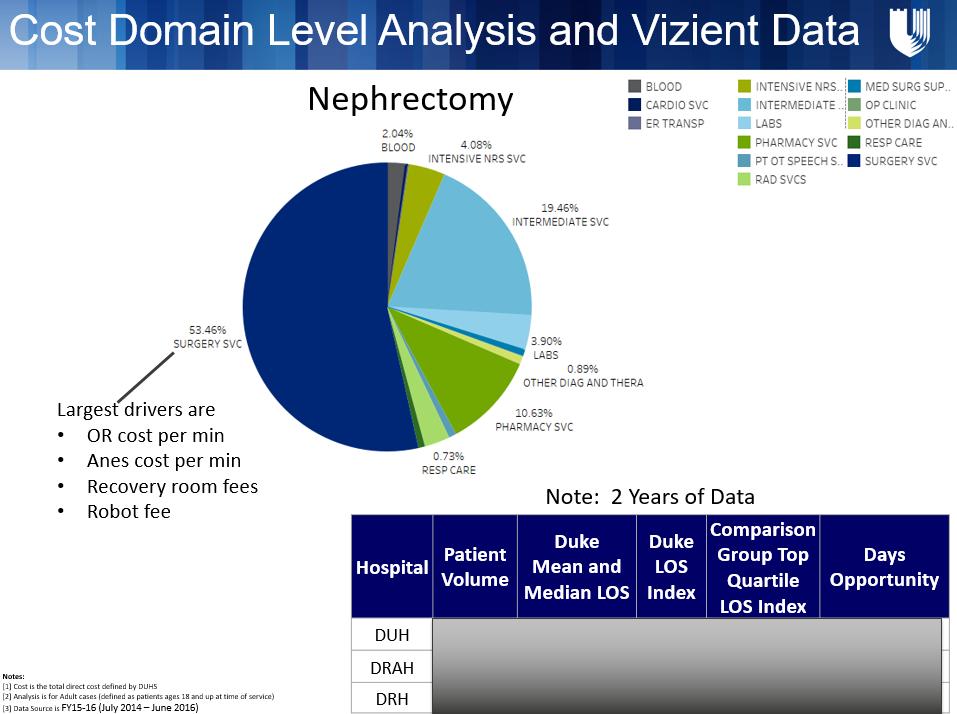
30 Nephrectomy and Prostatectomy Project selected in Fall 2016 Formal memo noting roles and responsibilities sent to physician and nurse co-lead Multidisciplinary core team kicked off in December
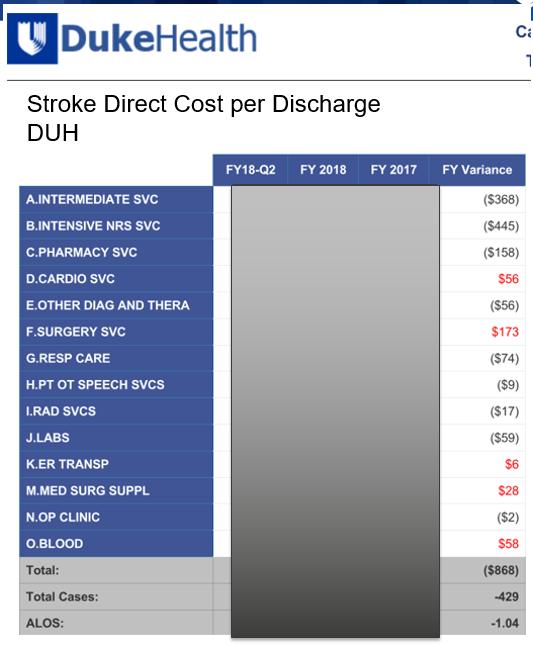
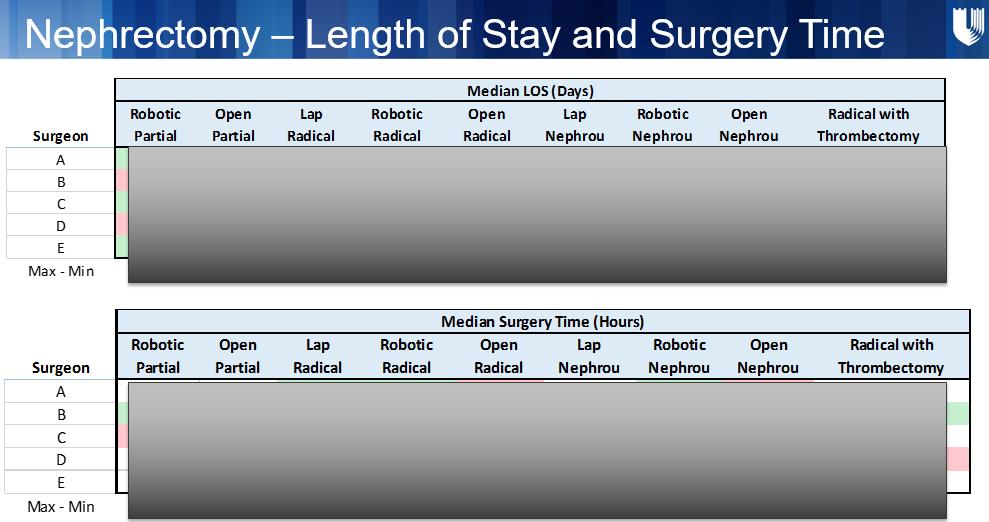
31 Define/Measure - Improvement Phase Project charter drafted Data analyzed: Vizient comparative data analyzing LOS, readmissions, and mortality Internal direct cost/case data analyzing variation by provider and service group HCAHPS patient experience Other process metric data analyzed as relevant (i.e. OR case times, infections, NSQIP, etc) Stakeholder interviews conducted and key themes summarized Best practice evidence analyzed by Research Services team 31

 [3] Data Source is FY15-16 (July 2014")
32 Cost Domain Level Analysis Nephrectomy Prostatectomy Kelli Notes: [1] Cost is the total direct cost defined by DUHS [2] Analysis is for Adult cases (defined as patients ages 18 and up at time of service) [3] Data Source is FY15-16 (July 2014 June 2016)
33
34 Analyze - Improvement Phase Quantitative and qualitative data summarized into key driver diagram Subteams formed to tackle key drivers Brainstorming sessions held to validate key drivers and brainstorm solutions 34


35 Subteam Structure Pre-op Periop Post-op Standardization of Surgeon Practice Patterns 35

36 Improve and Control Improvement Phase Subteams complete intervention design Develop key process metrics Finalize any pilot plans Develop implementation plan, including communication and staff education plan Finalize IT requests and submit to Epic Implement; monitor and adjust as needed Review performance reports and launch continuous improvement 36



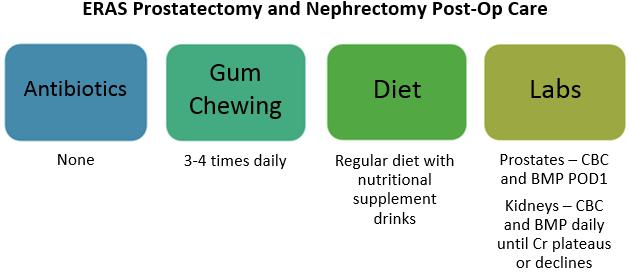
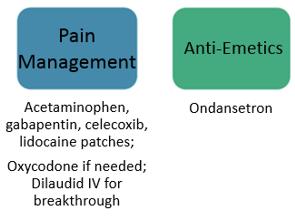
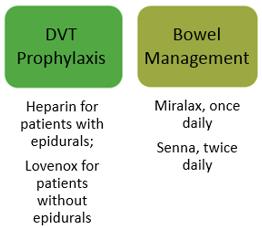
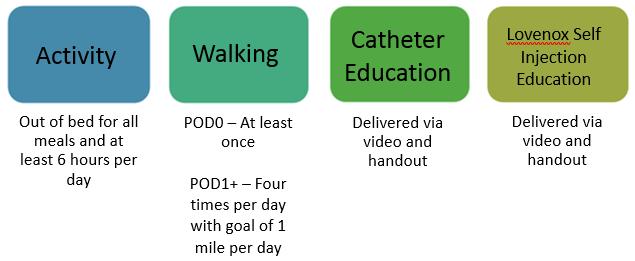
37 Standardized Practice Patterns ERAS Prostatectomy and Nephrectomy Pre-Op Care 37
38 Standardized Practice Patterns 38
39 Standardized Practice Patterns 39
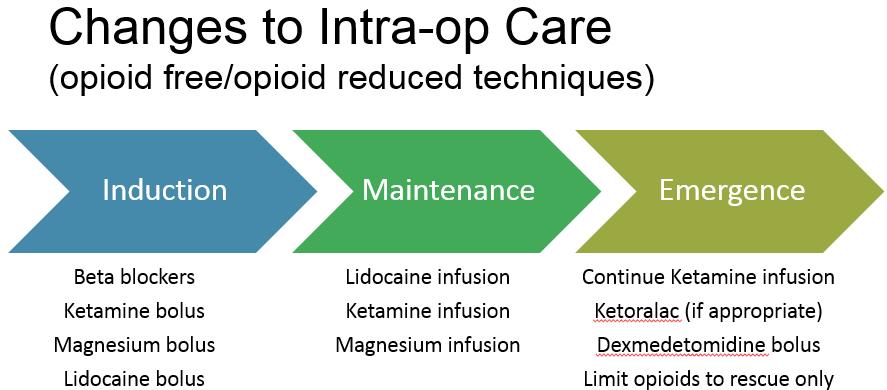
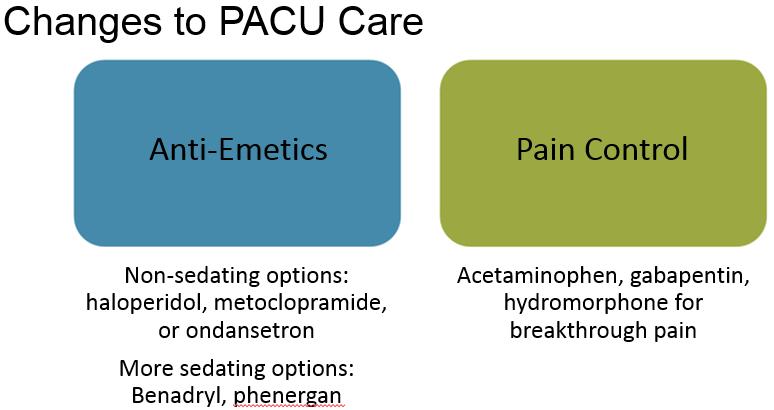
40 Implementation Slide Example - Implement Early Recovery After Surgery (ERAS) Principles Why Change? Each of the surgeons performing prostatectomies and nephrectomies has different pre-op and post-op practice patterns. There is no standardized anesthesia pathway for this patient population. Data for other patient populations shows that implementing ERAS principles reduces length of stay and reduces complications. What are the Changes? Standardize pre-op and post-op practice patterns and hardcode via pre-op and post-op order sets Create narcotic sparing anesthesia pathways for prostatectomies and nephrectomies Create pocket cards to remind providers of which text to use in the patients AVS and which drugs to prescribe at discharge What is the Plan for Changing? Orders sets will go live in Epic on 7/19/17 Physicians will be educated during Grand Rounds on 7/19/17; the Epic Concierge will set up favorites by 8/1/17 Nursing staff and anesthesia staff will be educated through July 2017 Go live will be on 8/1/17 Who Should I Contact with Questions about This Change? Urologist Project Co-lead ERAS Coordinator Clinical Leader on 6300 Project Co-Lead Anesthesiologist Urology APP 40


41 Enhanced Patient Education 41


42 Process Metric Examples 42
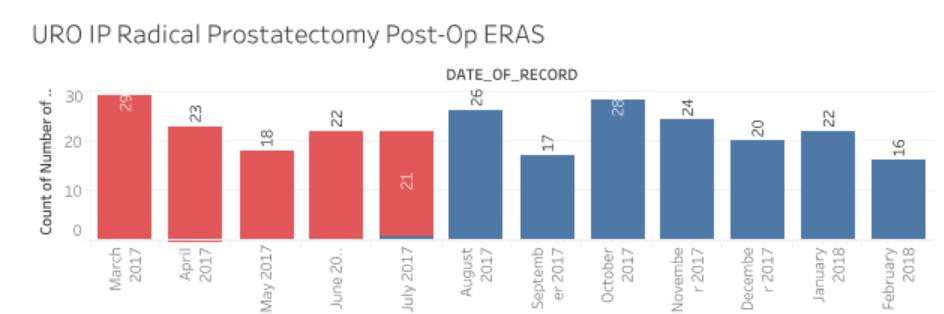
43 Initial Outcome Data Results % Improvement Metric (Pre to Post - 5 months) HCAHPS Pain Management 3% 30 Day Readmission Rate 23% ALOS 7% 43
44 Key Lessons Learned Importance of physician and nursing co-lead to drive change Good quantitative and qualitative data drive decision-making Project management resource can help move work forward faster Process metric and outcome data feedback is critical to teams Important collaborators include Epic, Finance, and Research Services Identify operational home for control and continuous improvement phase 44
45 FUTURE DIRECTIONS 45
46 Continue to evolve improvement approach Integrate approach with Lean quality management system Better engage frontline staff and connect key initiatives across projects Hardwire changes through standard work and new management tools Pilot clinical consensus group Develop approach and framework Leverage current infrastructure and identify key metrics of success Develop 3 year strategic goals Complete best-practice benchmarking sessions with other programs Outline key priorities with Oversight Committee Advance on Value Transition goals and gain more experience in population health projects 46
47 Q&A 47

48 Question and Answer What tactics to reduce clinical variation have worked at your organization? What have been the challenges? What sustainment tactics have you used? How does your organization prioritize areas to focus on? 48
49 Contact Information Caitlin Daley Dr. George Cheely Dr. Tom Hopkins 49

50 Performance Services Website: Duke Performance Services 50
Balancing State, Federal and Internal Bundle Payment Initiatives
 Balancing State, Federal and Internal Bundle Payment Initiatives Vanderbilt University Medical Center Brittany Cunningham, MSN, RN, CSSBB Director, Episodes of Care Key Take Aways What are the different
Balancing State, Federal and Internal Bundle Payment Initiatives Vanderbilt University Medical Center Brittany Cunningham, MSN, RN, CSSBB Director, Episodes of Care Key Take Aways What are the different
Clinical Program Cost Leadership Improvement
 Clinical Program Cost Leadership Improvement December 2017 Presbyterian recently developed a rapid-cycle process for integrating sustainable cost and quality improvements within clinical programs. Population
Clinical Program Cost Leadership Improvement December 2017 Presbyterian recently developed a rapid-cycle process for integrating sustainable cost and quality improvements within clinical programs. Population
9/29/2017. Enhanced Recovery After Surgery at the University of Virginia Medical Center. Disclosures. Objectives. None
 Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Why Focus on Perioperative Services?
 1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
SANTA ROSA MEMORIAL HOSPITAL AND AFFILIATED ENTITIES ONGOING PROFESSIONAL PRACTICE EVALUATION POLICY (OPPE)
") SANTA ROSA MEMORIAL HOSPITAL AND AFFILIATED ENTITIES ONGOING PROFESSIONAL PRACTICE EVALUATION POLICY (OPPE) Discussion Draft August 6, 2017 Horty, Springer & Mattern, P.C. 250979.8 ONGOING PROFESSIONAL
SANTA ROSA MEMORIAL HOSPITAL AND AFFILIATED ENTITIES ONGOING PROFESSIONAL PRACTICE EVALUATION POLICY (OPPE) Discussion Draft August 6, 2017 Horty, Springer & Mattern, P.C. 250979.8 ONGOING PROFESSIONAL
LVHN Sepsis Quality Improvement Project
 LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
Bethesda Hospital PGY1 Residency Program Learning Experiences
 Bethesda Hospital PGY1 Residency Program Learning Experiences Required rotations Orientation This rotation will orient the resident to hospital pharmacy and the responsibilities of a staff pharmacist.
Bethesda Hospital PGY1 Residency Program Learning Experiences Required rotations Orientation This rotation will orient the resident to hospital pharmacy and the responsibilities of a staff pharmacist.
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Perioperative Surgical Home
 None Disclosures Debnath Chatterjee, M.D. Associate Professor of Anesthesiology CRASH 2015 - Vail, Colorado 2 Learning Objectives What is the PSH model? Describe the concept of the Perioperative Surgical
None Disclosures Debnath Chatterjee, M.D. Associate Professor of Anesthesiology CRASH 2015 - Vail, Colorado 2 Learning Objectives What is the PSH model? Describe the concept of the Perioperative Surgical
NASHP s 30 th Annual State Health Policy Conference. Timeline of Tennessee Health Care Innovation Initiative
 STATE OF TENNESSEE NASHP s 30 th Annual State Health Policy Conference 10/25/2017 Timeline of Tennessee Health Care Innovation Initiative 2012 2013 2014 2015 2016 2017 1210 Stakeholder Meetings 16 Partnerships
STATE OF TENNESSEE NASHP s 30 th Annual State Health Policy Conference 10/25/2017 Timeline of Tennessee Health Care Innovation Initiative 2012 2013 2014 2015 2016 2017 1210 Stakeholder Meetings 16 Partnerships
4/10/2013. Learning Objective. Quality-Based Payment Models
 Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
AHRQ Safety Program for Improving Surgical Care and Recovery. ACS Quality and Safety Conference New York City July 21, 2017
 AHRQ Safety Program for Improving Surgical Care and Recovery ACS Quality and Safety Conference New York City July 21, 2017 1 Project goals To measurably improve patient outcomes in five surgical areas
AHRQ Safety Program for Improving Surgical Care and Recovery ACS Quality and Safety Conference New York City July 21, 2017 1 Project goals To measurably improve patient outcomes in five surgical areas
Enhanced Recovery After Surgery (ERAS) for Elective Colon Resection Surgery at Vancouver General Hospital. What is Possible?
 for Elective Colon Resection Surgery at Vancouver General Hospital. What is Possible?") Enhanced Recovery After Surgery (ERAS) for Elective Colon Resection Surgery at Vancouver General Hospital What is Possible? BC Provincial Collaborative November 25, 2014 Disclosure Statement I do not have
Enhanced Recovery After Surgery (ERAS) for Elective Colon Resection Surgery at Vancouver General Hospital What is Possible? BC Provincial Collaborative November 25, 2014 Disclosure Statement I do not have
Understanding the Implications of Total Cost of Care in the Maryland Market
 Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
ABOUT THE CONE HEALTH NETWORK OF SERVICES
 THE MOSES H. CONE MEMORIAL HOSPITAL (536 beds) Critical Care Services All system ICU patients are monitored with the help an electronic ICU monitoring system (VISICU ). Emergency Services Medical Intensive
THE MOSES H. CONE MEMORIAL HOSPITAL (536 beds) Critical Care Services All system ICU patients are monitored with the help an electronic ICU monitoring system (VISICU ). Emergency Services Medical Intensive
Care Redesign: Budgeted Episodes for Total Knee Replacement
 Care Redesign: Budgeted Episodes for Total Knee Replacement Wade Johannessen, PhD Director, Sg2 Allen Marsh Ortho/Neuro Service Line Director CaroMont Health October 13, 2011 Chicago London www.sg2.com
Care Redesign: Budgeted Episodes for Total Knee Replacement Wade Johannessen, PhD Director, Sg2 Allen Marsh Ortho/Neuro Service Line Director CaroMont Health October 13, 2011 Chicago London www.sg2.com
Physician Executive Council. Using the Perioperative Surgical Home to Improve Joint Replacement
 Physician Executive Council Using the Perioperative Surgical Home to Improve Joint Replacement 9 Today s Presenters Julie Riley Physician Executive Council Senior Consultant 202-266-5628 RileyJu@advisory.com
Physician Executive Council Using the Perioperative Surgical Home to Improve Joint Replacement 9 Today s Presenters Julie Riley Physician Executive Council Senior Consultant 202-266-5628 RileyJu@advisory.com
BUILDING THE PATIENT-CENTERED HOSPITAL HOME
 WHITE PAPER BUILDING THE PATIENT-CENTERED HOSPITAL HOME A New Model for Improving Hospital Care Authors Sonya Pease, MD Chief Medical Officer TeamHealth Anesthesia Kurt Ehlert, MD National Director, Orthopaedics
WHITE PAPER BUILDING THE PATIENT-CENTERED HOSPITAL HOME A New Model for Improving Hospital Care Authors Sonya Pease, MD Chief Medical Officer TeamHealth Anesthesia Kurt Ehlert, MD National Director, Orthopaedics
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES. James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Comprehensive Program and 5 Key Aspects James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Comprehensive Program and 5 Key Aspects James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
Emory Healthcare s Approach to Clinical Effectiveness. Gregory J. Esper, MD, MBA Director, New Care Models, Emory Healthcare
 Emory Healthcare s Approach to Clinical Effectiveness Gregory J. Esper, MD, MBA Director, New Care Models, Emory Healthcare Disclosures Consultant, NeuroOne, Inc. Board Member, Georgia Tech Masters of
Emory Healthcare s Approach to Clinical Effectiveness Gregory J. Esper, MD, MBA Director, New Care Models, Emory Healthcare Disclosures Consultant, NeuroOne, Inc. Board Member, Georgia Tech Masters of
Partnerships: Developing an Elective Joint Replacement Program
 Partnerships: Developing an Elective Joint Replacement Program Amy R. Ehrlich, MD Angela Schonberg, MPT Wojciech Rymarowicz, MPT Overview Session Overview: Montefiore network Program Development Data and
Partnerships: Developing an Elective Joint Replacement Program Amy R. Ehrlich, MD Angela Schonberg, MPT Wojciech Rymarowicz, MPT Overview Session Overview: Montefiore network Program Development Data and
Shared Governance and Analytics Framework Improves Quality
 Shared Governance and Analytics Framework Improves Quality Session 154, March 7, 2018 Kate Mundell, MBA, PMP MultiCare Connected Care Amber Theel, BSN, MBA, CPHQ, CPHRM MultiCare Health System 1 Conflict
Shared Governance and Analytics Framework Improves Quality Session 154, March 7, 2018 Kate Mundell, MBA, PMP MultiCare Connected Care Amber Theel, BSN, MBA, CPHQ, CPHRM MultiCare Health System 1 Conflict
Rural-Relevant Quality Measures for Critical Access Hospitals
 Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
Care Redesign: An Essential Feature of Bundled Payment
 Issue Brief No. 11 September 2013 Care Redesign: An Essential Feature of Bundled Payment Jett Stansbury Director, New Payment Strategies, Integrated Healthcare Association Gabrielle White, RN, CASC Executive
Issue Brief No. 11 September 2013 Care Redesign: An Essential Feature of Bundled Payment Jett Stansbury Director, New Payment Strategies, Integrated Healthcare Association Gabrielle White, RN, CASC Executive
Hip Today Home Tomorrow:
 Hip Today Home Tomorrow: A Collaborative Effort between an Orthopedic Practice and a Hospital to Create an Innovative Outpatient Total Hip Replacement Program Kimberley Murray RN MS CNS-CNOR Kelly Keenan
Hip Today Home Tomorrow: A Collaborative Effort between an Orthopedic Practice and a Hospital to Create an Innovative Outpatient Total Hip Replacement Program Kimberley Murray RN MS CNS-CNOR Kelly Keenan
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
TRANSFORMING CARE DELIVERY
 APRIL 2015 TRANSFORMING CARE DELIVERY THE POWER OF CLINICAL VARIATION MANAGEMENT About The Chartis Group The Chartis Group is a national advisory services firm that provides strategic planning, accountable
APRIL 2015 TRANSFORMING CARE DELIVERY THE POWER OF CLINICAL VARIATION MANAGEMENT About The Chartis Group The Chartis Group is a national advisory services firm that provides strategic planning, accountable
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Learning Experiences Descriptions
 Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Connecting the Revenue and Reimbursement Cycles
 Connecting the Revenue and Reimbursement Cycles Tuesday, August 19 th, 2014 Toni G. Cesta, Ph.D., RN, FAAN Consultant and Partner Case Management Concepts New York Office And Bev Cunningham, MS, RN Vice
Connecting the Revenue and Reimbursement Cycles Tuesday, August 19 th, 2014 Toni G. Cesta, Ph.D., RN, FAAN Consultant and Partner Case Management Concepts New York Office And Bev Cunningham, MS, RN Vice
Healthcare Reform Hospital Perspective
 Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
Report of the Incidence and Prevalence of Diseases and other Health Related Issues in Saudi Arabia
 Report of the Incidence and Prevalence of Diseases and other Health Related Issues in Saudi Arabia A study for the SMLE Blueprint Project Heba AlManea Assessment Executive Specialist, SCFHS Dr Abdulmohsen
Report of the Incidence and Prevalence of Diseases and other Health Related Issues in Saudi Arabia A study for the SMLE Blueprint Project Heba AlManea Assessment Executive Specialist, SCFHS Dr Abdulmohsen
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
Sepsis, An Interdisciplinary and Collaborative Approach. Bassett Medical Center October/November 2017
 Sepsis, An Interdisciplinary and Collaborative Approach Bassett Medical Center October/November 2017 Bassett Medical Center 180 bed acute care inpatient teaching facility in Cooperstown, New York is the
Sepsis, An Interdisciplinary and Collaborative Approach Bassett Medical Center October/November 2017 Bassett Medical Center 180 bed acute care inpatient teaching facility in Cooperstown, New York is the
HOW TO GET STARTED
 0.01 BUNDLING AND VALUE BASED CARE: Tony DiGioia, MD and Gigi Crowley HOW TO GET STARTED TONY@PFCUSA.ORG DEC 12 2017 40 Minutes 0.02 The existing deficiencies in health care cannot be corrected simply
0.01 BUNDLING AND VALUE BASED CARE: Tony DiGioia, MD and Gigi Crowley HOW TO GET STARTED TONY@PFCUSA.ORG DEC 12 2017 40 Minutes 0.02 The existing deficiencies in health care cannot be corrected simply
How to Win Under Bundled Payments
 How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
H-SAA AMENDING AGREEMENT
 H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: NORTH EAST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND (the Hospital ) WHEREAS
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: NORTH EAST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND (the Hospital ) WHEREAS
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
Bringin it to the Bedside: Staff-Driven Savings
 Bringin it to the Bedside: Staff-Driven Savings Jackie Noll, MSN, RN, CEN, Senior Director of Nursing, The Children s Hospital of Philadelphia (CHOP) Amy Gallagher, MS, PharmD, Senior Director of Home
Bringin it to the Bedside: Staff-Driven Savings Jackie Noll, MSN, RN, CEN, Senior Director of Nursing, The Children s Hospital of Philadelphia (CHOP) Amy Gallagher, MS, PharmD, Senior Director of Home
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Benchmarking and Key Metrics Utilized by HSCT Administrators. Clint Divine, MBA, MSM Administrative Director, BMT
 Benchmarking and Key Metrics Utilized by HSCT Administrators Clint Divine, MBA, MSM Administrative Director, BMT 1 When you ve seen one HSCT program, you ve seen one HSCT program Although, there are many
Benchmarking and Key Metrics Utilized by HSCT Administrators Clint Divine, MBA, MSM Administrative Director, BMT 1 When you ve seen one HSCT program, you ve seen one HSCT program Although, there are many
ACHIEVING PHYSICIAN INTEGRATION WITH THE CO-MANAGEMENT MODEL
 ACHIEVING PHYSICIAN INTEGRATION WITH THE CO-MANAGEMENT MODEL Presented by: Joseph F. Corfits, Jr. FHFMA, Chief Financial Officer Unity Point Health Des Moines Stephen G. Taylor, MD Des Moines Orthopaedic
ACHIEVING PHYSICIAN INTEGRATION WITH THE CO-MANAGEMENT MODEL Presented by: Joseph F. Corfits, Jr. FHFMA, Chief Financial Officer Unity Point Health Des Moines Stephen G. Taylor, MD Des Moines Orthopaedic
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING
 MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of October, 2016
 is made as of the 1 st day of October, 2016") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of October, 216 B E T W E E N: SOUTH WEST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND St. Joseph's Health
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of October, 216 B E T W E E N: SOUTH WEST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND St. Joseph's Health
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Hospital Perioperative Assessment Statement of Work. Prepared by Amblitel Date
 Hospital Perioperative Assessment Statement of Work Prepared by Amblitel Date 1 Table of Contents Background... 3 Objective... 3 Scope of Work... 3 Phase 1 - Establish Overall Project Structure and Process...
Hospital Perioperative Assessment Statement of Work Prepared by Amblitel Date 1 Table of Contents Background... 3 Objective... 3 Scope of Work... 3 Phase 1 - Establish Overall Project Structure and Process...
Clinical and Financial Benefits of IT Implementation
 Clinical and Financial Benefits of IT Implementation October 24, 2014 Replace text box with chapter logo (on all master slides) Who Is HIMSS Analytics? A subsidiary of HIMSS We collect data on what information
Clinical and Financial Benefits of IT Implementation October 24, 2014 Replace text box with chapter logo (on all master slides) Who Is HIMSS Analytics? A subsidiary of HIMSS We collect data on what information
H-SAA AMENDING AGREEMENT B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND
 AND") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND WOMEN'S COLLEGE
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND WOMEN'S COLLEGE
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment
 Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
Session 183, March 7, 2018 Sue Murphy, RN, BSN, MS, Chief Experience Officer, UChicago Medicine
 Chief Experience Officer: The New Leader Driving Innovation to Transform Healthcare for Patients, Families and Care Teams Session 183, March 7, 2018 Sue Murphy, RN, BSN, MS, Chief Experience Officer, UChicago
Chief Experience Officer: The New Leader Driving Innovation to Transform Healthcare for Patients, Families and Care Teams Session 183, March 7, 2018 Sue Murphy, RN, BSN, MS, Chief Experience Officer, UChicago
Surgeon Champion: Getting Started, What You Need to Know
 Surgeon Champion: Getting Started, What You Need to Know Ninh T. Nguyen, MD, FACS Professor of Surgery Surgeon Champion Vice-Chair, Dept Surgery University of California, Irvine, Medical Center, Orange,
Surgeon Champion: Getting Started, What You Need to Know Ninh T. Nguyen, MD, FACS Professor of Surgery Surgeon Champion Vice-Chair, Dept Surgery University of California, Irvine, Medical Center, Orange,
Presentation Outline
 Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Medical Intensive Care Unit Rotation EUHM
 PGY 2 Residency Training Program Medical Intensive Care Unit Rotation EUHM Preceptor: Derek M. Polly, PharmD Office: EUHM, 2 nd Floor, Room 2182 Hours: ~ 7:30 4:00 Desk: 404 686 5674 Pager: 404 686 5500
PGY 2 Residency Training Program Medical Intensive Care Unit Rotation EUHM Preceptor: Derek M. Polly, PharmD Office: EUHM, 2 nd Floor, Room 2182 Hours: ~ 7:30 4:00 Desk: 404 686 5674 Pager: 404 686 5500
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
Physician Performance Analytics: A Key to Cost Savings
 Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Driving Obstetrical Excellence Through a Council Structure
 Driving Obstetrical Excellence Through a Council Structure Elizabeth Deckers, MD Director of Labor and Delivery, Hartford Hospital Deborah Feldman, M.D. Division director, Maternal Fetal Medicine, Hartford
Driving Obstetrical Excellence Through a Council Structure Elizabeth Deckers, MD Director of Labor and Delivery, Hartford Hospital Deborah Feldman, M.D. Division director, Maternal Fetal Medicine, Hartford
Improving Care Transitions
 Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
F 5 STANDING COMMITTEES. Finance and Asset Management Committee. UW Medicine Clinical Transformation Project INFORMATION
 STANDING COMMITTEES F 5 Finance and Asset Management Committee UW Medicine Clinical Transformation Project INFORMATION This item is being presented for information only. Attachment Clinical Transformation
STANDING COMMITTEES F 5 Finance and Asset Management Committee UW Medicine Clinical Transformation Project INFORMATION This item is being presented for information only. Attachment Clinical Transformation
Ambulatory Care Model
 Ambulatory Care Model Hong Kong May 2013 Andrew Stripp Deputy Chief Executive & Chief Operating Officer Outline What is the Alfred Centre? How does it fit into Alfred Health service model Key aspects of
Ambulatory Care Model Hong Kong May 2013 Andrew Stripp Deputy Chief Executive & Chief Operating Officer Outline What is the Alfred Centre? How does it fit into Alfred Health service model Key aspects of
ASCO s Quality Training Program
 ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
OUTPATIENT TOTAL JOINT
 OUTPATIENT TOTAL JOINT REPLACEMENTS How to Prepare, Transition and Deliver High Quality of Care Becker s ASC 22 nd Annual Meeting October 22-24, 2015 Chicago, IL Marcia A. Friesen, RN, BS, FAIHQ, FACHE
OUTPATIENT TOTAL JOINT REPLACEMENTS How to Prepare, Transition and Deliver High Quality of Care Becker s ASC 22 nd Annual Meeting October 22-24, 2015 Chicago, IL Marcia A. Friesen, RN, BS, FAIHQ, FACHE
Service Lines and Activity Based Costing Improve Outcomes
 Service Lines and Activity Based Costing Improve Outcomes Session 230, February 23, 2017 Robert A. DeMichiei CPA, Executive Vice President and Chief Financial Officer, UPMC Robert Edwards MD, Professor
Service Lines and Activity Based Costing Improve Outcomes Session 230, February 23, 2017 Robert A. DeMichiei CPA, Executive Vice President and Chief Financial Officer, UPMC Robert Edwards MD, Professor
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems NPSS Asheville, NC
 Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Enhanced Recovery Implementing Meaningful Change
 Enhanced Recovery Implementing Meaningful Change Jeff Simmons MD Associate Professor UAB Department of Anesthesiology and Perioperative Medicine I have no relevant financial relationships to disclose.
Enhanced Recovery Implementing Meaningful Change Jeff Simmons MD Associate Professor UAB Department of Anesthesiology and Perioperative Medicine I have no relevant financial relationships to disclose.
The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Jefferson Health
 The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Jefferson Health 2. Title Of Initiative Implementation of a Patient Blood Management
The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Jefferson Health 2. Title Of Initiative Implementation of a Patient Blood Management
When you have to be right. Increase Competence. Improve Outcomes. Health. Lippincott Professional Development Collection. Lippincott Solutions
 When you have to be right Increase Competence. Improve Outcomes. Health Lippincott Professional Development Collection Lippincott Solutions Lippincott Professional Development Collection Lippincott Professional
When you have to be right Increase Competence. Improve Outcomes. Health Lippincott Professional Development Collection Lippincott Solutions Lippincott Professional Development Collection Lippincott Professional
Provider Profile GENERAL DETAILS STATE/ PROVINCE: OTHERS (PLEASE SPECIFY): CONTACT DETAILS DESIGNATION NAME PHONE MOBILE
: CONTACT DETAILS DESIGNATION NAME PHONE MOBILE") Provider Profile Dear Valued Provider, Kindly fill up this form with the information requested below. Availability of accurate and detailed information about your facility will definitely help QLM staff
Provider Profile Dear Valued Provider, Kindly fill up this form with the information requested below. Availability of accurate and detailed information about your facility will definitely help QLM staff
National Priorities for Improvement:
 National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
Bundled Payments. AMGA September 25, 2013 AGENDA. Who Are We. Our Business Challenge. Episode Process. Experience
 Bundled Payments AMGA September 25, 2013 Who Are We AGENDA Our Business Challenge Episode Process Experience 1 Cleveland Clinic is transforming Fee for service Fee for value 3 Fast Facts 41,200 employees
Bundled Payments AMGA September 25, 2013 Who Are We AGENDA Our Business Challenge Episode Process Experience 1 Cleveland Clinic is transforming Fee for service Fee for value 3 Fast Facts 41,200 employees
Session 92AB Improving Patient Experience and Outcomes Using Real-Time Care Rounding Technology
 Prepared for the Foundation of the American College of Healthcare Executives Session 92AB Improving Patient Experience and Outcomes Using Real-Time Care Rounding Technology Presented by: Sue Murphy Alison
Prepared for the Foundation of the American College of Healthcare Executives Session 92AB Improving Patient Experience and Outcomes Using Real-Time Care Rounding Technology Presented by: Sue Murphy Alison
ENHANCE HEALTHCARE CONSULTING E. COUNTRY CLUB DRIVE, SUITE 2810 AVENTURA, FL
 In today s healthcare environment, anesthesia groups have many issues to deal with, including ACO s, pressure on reimbursement, quality tracking, the surgical home, and pressure on hospital subsidies.
In today s healthcare environment, anesthesia groups have many issues to deal with, including ACO s, pressure on reimbursement, quality tracking, the surgical home, and pressure on hospital subsidies.
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Tools & Resources for QI Success
 Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
Overview of Alaska s Hospitals and Nursing Homes. House HSS Committee March 1, 2012
 Overview of Alaska s Hospitals and Nursing Homes House HSS Committee March 1, 2012 Alaska Hospital and Nursing Homes Testifying Today Fairbanks Memorial Hospital Mike Powers Central Peninsula Hospital
Overview of Alaska s Hospitals and Nursing Homes House HSS Committee March 1, 2012 Alaska Hospital and Nursing Homes Testifying Today Fairbanks Memorial Hospital Mike Powers Central Peninsula Hospital
Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand
 This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov. 2016 Frederick C. Ryckman, MD Professor of Surgery / Transplantation
This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov. 2016 Frederick C. Ryckman, MD Professor of Surgery / Transplantation
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
National Clinical Audit programme
 National Clinical Audit programme Danny Keenan Medical Director www.hqip.org.uk Who are HQIP? HQIP is a not-for profit, professional/patient partnership, aiming to change and improve health and social
National Clinical Audit programme Danny Keenan Medical Director www.hqip.org.uk Who are HQIP? HQIP is a not-for profit, professional/patient partnership, aiming to change and improve health and social
New Models in Payment: Joint Replacements. Sharon Eloranta, MD February 18, 2016
 New Models in Payment: Joint Replacements Sharon Eloranta, MD February 18, 2016 Qualis Health A leading national population health management organization The Medicare Quality Innovation Network - Quality
New Models in Payment: Joint Replacements Sharon Eloranta, MD February 18, 2016 Qualis Health A leading national population health management organization The Medicare Quality Innovation Network - Quality
Ohio SIM: Episode-based Payment Update. Webinar September 21, 2017
 Ohio SIM: Episode-based Payment Update Webinar September 21, 2017 www.healthtransformation.ohio.gov Ohio was awarded a federal grant to test multi-payer, value-based payment models HI WA OR NV CA ID AZ
Ohio SIM: Episode-based Payment Update Webinar September 21, 2017 www.healthtransformation.ohio.gov Ohio was awarded a federal grant to test multi-payer, value-based payment models HI WA OR NV CA ID AZ
IHI Expedition. Expedition: Preparing Care Teams for Bundled Payments Session 5: Care Team Redesign
 May 19, 2015 Begins at 1:00 PM IHI Expedition Expedition: Preparing Care Teams for Bundled Payments Session 5: Care Team Redesign Trisha Frick, MS, RN Nick Bassett, MBA Lucy Savitz, PhD, MBA Molly Bogan,
May 19, 2015 Begins at 1:00 PM IHI Expedition Expedition: Preparing Care Teams for Bundled Payments Session 5: Care Team Redesign Trisha Frick, MS, RN Nick Bassett, MBA Lucy Savitz, PhD, MBA Molly Bogan,
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Introduction. Staffing to demand increases bottom line revenue for the facility through increased volume and throughput and elimination of waste.
 Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
HRET HIIN Readmissions Virtual Event. Fishbowl Event #5: The Fish Finale September 14, 2017
 HRET HIIN Readmissions Virtual Event Fishbowl Event #5: The Fish Finale September 14, 2017 1 Shereen Shojaat, MS Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Poll 1: How did you get here? How did
HRET HIIN Readmissions Virtual Event Fishbowl Event #5: The Fish Finale September 14, 2017 1 Shereen Shojaat, MS Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Poll 1: How did you get here? How did
Avoidable Imaging Wave II. How MIPS, CPIA, CEDR metrics relate to E-QUAL Clinician Engagement in Avoidable Imaging Initiatives
 Avoidable Imaging Wave II How MIPS, CPIA, CEDR metrics relate to E-QUAL Clinician Engagement in Avoidable Imaging Initiatives Presenters Dr. Jay Schuur Dr. John Sverha Disclaimer The project described
Avoidable Imaging Wave II How MIPS, CPIA, CEDR metrics relate to E-QUAL Clinician Engagement in Avoidable Imaging Initiatives Presenters Dr. Jay Schuur Dr. John Sverha Disclaimer The project described
Nursing Unit Descriptions UCHealth Memorial Hospital Central
 Nursing Unit Descriptions UCHealth Memorial Hospital Central ACUTE CARE SERVICES Neuroscience 5C Neuroscience is a 24-bed unit with all private rooms for our patients. The department specializes in acute
Nursing Unit Descriptions UCHealth Memorial Hospital Central ACUTE CARE SERVICES Neuroscience 5C Neuroscience is a 24-bed unit with all private rooms for our patients. The department specializes in acute
Hospital Service Accountability Agreements
 2017-2018 Schedule A Funding Allocation 2017-2018 [1] Estimated Funding Allocation Section 1: FUNDING SUMMARY LHIN FUNDING LHIN Global Allocation (Includes Sec. 3) Health System Funding Reform: HBAM Funding
2017-2018 Schedule A Funding Allocation 2017-2018 [1] Estimated Funding Allocation Section 1: FUNDING SUMMARY LHIN FUNDING LHIN Global Allocation (Includes Sec. 3) Health System Funding Reform: HBAM Funding
Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty
 Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty R. Michael Meneghini MD Associate Professor of Orthopaedic Surgery Indiana University School of Medicine Indianapolis,
Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty R. Michael Meneghini MD Associate Professor of Orthopaedic Surgery Indiana University School of Medicine Indianapolis,
CENTERS OF EXCELLENCE/HOSPITAL VALUE TOOL 2011/2012 METHODOLOGY
 A CENTERS OF EXCELLENCE/HOSPITAL VALUE TOOL 2011/2012 METHODOLOGY Introduction... 2 Surgical Procedures/Medical Conditions... 2 Patient Outcomes... 2 Patient Outcomes Quality Indexes... 3 Patient Outcomes
A CENTERS OF EXCELLENCE/HOSPITAL VALUE TOOL 2011/2012 METHODOLOGY Introduction... 2 Surgical Procedures/Medical Conditions... 2 Patient Outcomes... 2 Patient Outcomes Quality Indexes... 3 Patient Outcomes
over Foremost A Story of Clinical Excellence Built on Strong Clinical Differentiators A Legacy of Excellence Million Clinicians Health Checks
 A Legacy of Excellence Foremost 6 14 42 121 12 Million Health Checks over 8000 Clinicians Apollo Hospitals Group https://www.apollohospitals.com Talk to Apollo Hospitals on Social Media A Story of Clinical
A Legacy of Excellence Foremost 6 14 42 121 12 Million Health Checks over 8000 Clinicians Apollo Hospitals Group https://www.apollohospitals.com Talk to Apollo Hospitals on Social Media A Story of Clinical