Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time
|
|
|
- Shawn Summers
- 5 years ago
- Views:
Transcription
1 This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Pat Rutherford Hospital Flow Professional Development Program April 4, 2016 Cambridge, MA
2 Session Objectives After this session, participants will be able to: Understand the conceptual framework for system optimization to ensure patient access and flow in acute care hospitals Utilize an approach for sense-making regarding various strategies for managing hospital operations and improving patient flow throughout the hospital Identify high leverage interventions for creating a sustainable system for hospital flow, so that patients receive the right care, in the right place, at the right time
3 Don Berwick s Reflections on Patient Flow 3 Not long after safety leapt to the top, I became aware of a second sleeping giant of a problem in care flow.tom Nolan (API, IHI) asserted that flow through the system was an issue in some ways every bit as crucial and challenging as safety, and that, like safety, the issue of flow had somehow become cut off in healthcare from the fundamental sciences that, correctly employed, could help break healthcare free of some costly fetters. The problem of flow in healthcare may not have the charisma of safety, but it has everything else: it is big (indeed gigantic!), pervasive, interesting, and highly remediable. pp. x, xi -- Donald M. Berwick, MD, MPP, FRCP, President Emeritus and Senior Fellow, Institute for Healthcare Improvement Kirk Jensen, Thom A. Mayer, Shari J. Welch, Carol Haraden, Leadership for Smooth Patient Flow, ACHE Management Series, Health Administration Press, 2007
4 Don Berwick s Reflections on Patient Flow 4 As in the world of patient safety, the intellectual challenges in the sciences of flow proved to be of two major types to master the complex theories and approaches that had matured in other industries and academic disciplines far from healthcare, and, at the same time, to adapt and invent new theories helpful in special contexts of healthcare systems. p.xi Will flow ever acquire the patina of charisma that fuels today s work on patient safety? I doubt it.but whether so honored or not, the problem of flow is every bit as consequential for the health of our systems and the well-being of our patients. p.xii -- Donald M. Berwick, MD, MPP, FRCP, President Emeritus and Senior Fellow, Institute for Healthcare Improvement Kirk Jensen, Thom A. Mayer, Shari J. Welch, Carol Haraden, Leadership for Smooth Patient Flow, ACHE Management Series, Health Administration Press, 2007
5 Hospital Flow: Impact on Patient Safety 5 Patient Story Last March, I went to the ED at a nearby hospital because I was experiencing severe head pain, extreme vertigo, some numbness on my left side, and was rather confused. I got there around 7PM, and I was seen for in an exam room the first time around midnight. Since I suffer from migraines, they assumed that s what was going on (regardless of me telling them that it was very different than my usual episodes). I was sitting there for so long because the place was filled with people and there were only 2 nurses in the ED. It was close to 4:30AM when I finally saw a physician, who said there s really not much they can do for me. He said it would be best to go home and rest in my own bed, since the hospital was way too crowded for me to stay. So I went home. I woke up around 9AM and felt like things were getting worse. I spoke to my friend who is a PA at another ED in Boston, and she told me to go back immediately and request imaging. I did. However, it was a fight to get neurological tests done. Pushing and pushing they finally agreed. I had suffered a vertebral artery dissection and a massive blood clot had formed near the tear. From that, I experienced a Transient Ischemic Attack that could have been a stroke. When they saw that, they apologized for sending me home because of the back up the night earlier. I wound up in the Neuro Unit for more than a week, and it took over six months to recover.

6 Hospital Flow: Impact on Patient Experience 6

7 Hospital Flow: Impact on Healthcare Costs 7 Boston Globe article (March 2016)


8 Hospital Flow: Impact on Healthcare Costs 8
9 Problem Statement for Hospital Flow Addressing vexing issues of timely access and patient flow throughout the hospital is essential to ensure safe, high quality, patient-centered care. Delays in treatment and failure to provide the right care, in the right place, at the right time, puts patients at risk for potential harm and sub-optimal care. Poorly managed patient flow in hospital settings also adds to the already taxing burden on clinicians and accelerates burnout. Improved timely access to appropriate care and hospital flow are critical levers to increase value, for patients, clinicians and health care systems.
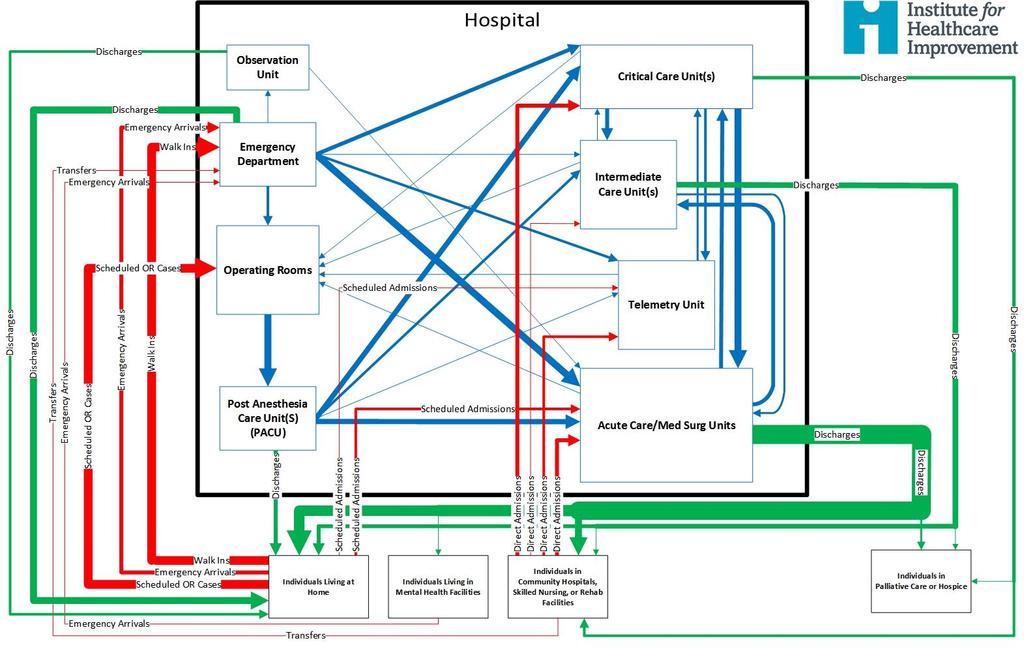
10 Problem Statement for Hospital Flow (2) Many health care professionals today realize that diversions and long waits and delays in the emergency department (ED) are a hospital-wide issue, not just an emergency department issue. The waits are often the result of emergency department beds being occupied by patients waiting for admission to the hospital. Lack of inpatient capacity also results in patients being boarded in the post-anesthesia care unit (PACU) and often managed on off service units. Unfortunately, understanding the problem is one thing, but actually improving hospital-wide patient flow is another.
11 Effects of High Utilization and Variability in Demand When the Emergency Department is overcrowded Patients may be diverted to other hospitals (external diversion) Patients leave without being seen Patients with acute illnesses experience delays in treatment Physicians, nurses and staff are overloaded (which often leads to medical errors and burnout of clinicians and staff) Throughput is decreased

12 Adoption of Effective Interventions 12 Leah S. Honigman Warner, Jesse M. Pines, Jennifer Gibson Chambers and Jeremiah D. Schuur, The Most Crowded US Hospital Emergency Departments Did Not Adopt Effective Interventions To Improve Flow, , Health Affairs, 34, no.12 (2015):
13 Effects of High Utilization and Variability in Demand (2) When hospital census is high Patients are boarded in the ED, waiting to be admitted to a hospital bed Patients have overnight stays in the Post-op Recovery Rooms Patients are admitted to alternative units or ICUs (internal diversions or off-service patients ) Patients may experience delays in treatment or delays or cancelations of surgery Physicians, nurses and staff are overloaded (which often leads to medical errors and burnout of clinicians and staff) Throughput is decreased (there are delays in transferring patients to appropriate units based on their clinical conditions and in discharging patients)
14 Hospital Flow: Key Learning To-Date Most hospitals are engaged in individual projects throughout the hospital to improve efficiencies and flow, but few have hospital-wide oversight systems to manage overall operations and patient flow throughout the hospital; there is a need for system-wide metrics to assess and manage patient flow at the macro whole-system level and in microsystems (OR, ED, ICUs, Med/Surg Units) Most hospitals are engaged in multiple efforts to improve flow, but few have shown quantitative results; need to develop performance targets to dramatically improve hospital operations and flow Few hospitals seem to be linking the shaping demand concept of decreasing overutilization of hospital services as a concurrent strategy to improve patient flow through the hospital [decreasing readmissions; proactive palliative care; reducing admissions for patient with complex needs; reducing low acuity ED visits; managing artificial variability in surgical scheduling]
15 Hospital Flow: Key Learning To-Date (2) There is a definitive need to simplify, standardize and sequence various matching capacity and demand strategies (variability management and daily real-time capacity and demand strategies) Current problems of patient flow in hospitals cannot be solved solely by efforts within the walls of the hospital (need partnerships with primary care, urgent care centers, specialty practices, mental health services, community-based care services, SNFs and nursing homes); Demonstrating a ROI for the systems moving to value-based payment models (or ACOs) should help to build will for improvement; avoiding capital expenditures is another incentive
16 Creating Value for Patients 16 Value should always be defined around the customer, and in a well-functioning health care system, the creation of value for patients should determine the rewards for all other actors in the system. Since value depends on results, not inputs, value in health care is measured by the outcomes achieved, not the volume of services delivered, and shifting focus from volume to value is a central challenge. Nor is value measured by the process of care used; process measurement and improvement are important tactics but are no substitutes for measuring outcomes and costs. Since value is defined as out. What Is Value in Health Care? Michael E. Porter, Ph.D. N Engl J Med 2010; 363: December 23, 2010
17 What are your performance goals? Decrease overutilization of hospital services? Relocate care to more appropriate care settings Reducing delays in treatment, surgery, transfers, discharge, etc.? Decreasing related medical errors and harm to patients? Manage LOS outliers? Optimize patient placement to insure the right care, in the right place, at the right time? Decrease external diversions? Decrease internal diversions ( off-service patients)? Maintain adequate staffing levels to maintain quality and safety? Increase clinician and staff satisfaction with hospital operations? Demonstrate a ROI for the hospital or the health system? Is your goal to have a high utilization of your hospital resources (procedures, beds and staff)? What is the right goal? What are the quality and safety balancing measures? When do you consider adding more bed capacity?

18 Hospital Occupancy Rates in MA (2012) 18 A national average occupancy of 78% applies to hospitals with 1,000 beds in the USA
19 Average Occupancy Rates (at hospital or unit levels) and the Day-to-Day Realities of Managing Patient Flow 19 # of Patients Time
20 Queuing Theory Systems serving unscheduled (uncontrolled) arrivals behave in a characteristic fashion. When (patient) inflow and service times are random, their response to increasing utilization is non-linear. As utilization rises above 80-85%, waits and rejections increase exponentially. At high levels of utilization small changes can lead to big improvements
21 Lessons from Queuing Theory 50% 45% 40% 35% Rejection rate 30% 25% 20% 15% 10% y = e x 5% R 2 = % 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% MICU utilization

22 Smaller hospitals and units have to run at lower average occupancy. This explains the observed higher nursing cost per bed day in smaller wards and the lower average occupancy observed to be associated with the smaller specialty bed pools. The figure of 3% turn-away was considered to be a pragmatic compromise between operational efficiency and the capital cost issues applicable to the UK but comes at the cost of not being able to guarantee waiting time targets. turn-away - a measure of the chaos, difficulty and effort implied in running the hospital, i.e. ambulances diverted elsewhere, patients held on trolleys in the emergency department, medical patients in surgical beds, cancelled operations, managers and clinicians hastily re-arranging schedules, bed management meetings and general operational complexity. Jones R (2011) Hospital bed occupancy demystified. British Journal of Healthcare Management 17(6):
23 Hospital Occupancy Rates Based on AHA data, overall nationwide hospital inpatient occupancy was 67.8% (AHA ); range was from 33.6% to 74%) Once managed efficiently, US hospitals, on average, could achieve an percent bed occupancy rate without adding beds at capital costs of approximately $1 million per bed. As a result of smoothing the scheduling of elective surgeries, improving discharge efficiencies and other interventions to improve flow at CCHMC, the hospital s quality of care improved even as the occupancy rate grew from 76 percent to 91 percent. Hospital officials also report improved overall safety for patients and reduction in stress on the doctors and nurses who treat them. Li E., Bisognano M. More Patients, Less Payment: Increasing Hospital Efficiency In The Aftermath Of Health Reform. Health Affairs, 2011, vol. 30, No. 1, pp
24 Complexity and Simplicity For the simplicity that lies this side of complexity, I would not give a fig, but for the simplicity that lies on the other side of complexity, I would give my life. (Oliver Wendell Holmes) Simplicity often lies on the other side of complexity, so for any problem, the more you can zoom out and embrace complexity, the better chance you have of zooming in on the simple details that matter most. (Eric Berlow)

25 Complexity and Simplicity
26
27 Hospital Flow: Strategies for System Optimization Demand System Strategies 1. Shape the Demand (reduce bed days; reduce ED visits; smooth elective surgeries and downstream bed utilization) 2. Match Capacity to Demand (reduce delays in moving patients to appropriate units throughout hospital; ensure patients are admitted to the appropriate unit) 3. Redesign the System (increase throughput; reduce bed days, manage LOS outliers, and reduce delays and waiting times)

28 Provost, L., and Bennett, B. (2015). What's your theory? Driver diagram serves as tool for building and testing theories for improvement. Quality Progress,
29 Strategies to Achieve System-Wide Hospital Flow Outcomes Strategies Primary Drivers Strategic Priority and Aligned Incentives Decrease overutilization of hospital services Optimize patient placement to insure the right care, in the right place, at the right time Increase clinician and staff satisfaction Demonstrate a ROI for the systems moving to bundled payment arrangements Will Ideas Execution Mutuality between Physicians and Hospital Executives Integrated Health Care Systems and/or ACOs Avoidance of Capital Expenditures Positive ROI and Financial Viability Shape the Demand Match Capacity and Demand Redesign the System Utilization of Hospital-wide Metrics to Guide Learning Within and Across Projects for Achieving Results Accountable Executive Leadership Providing Oversight of System-Level Performance Data Analytics to Provide Real-time Capacity and Demand Management and Forecasting Micro-system Quality Improvement Capability and Empowerment
30
31 Decrease overutilization of hospital services Optimize patient placement to insure the right care, in the right place, at the right time Increase clinician and staff satisfaction Demonstrate a ROI for the systems moving to bundled payment arrangements Driver Diagram: Ideas to Improve Hospital Flow Outcomes Primary Drivers Secondary Drivers Shape or Reduce Demand Match Capacity and Demand Redesign the System S1 Relocate care in ICUs in accordance with patients EOL wishes S2 Decrease demand for Med/Surg beds by preventing avoidable readmissions S3 Relocate low-acuity care in EDs to community-based care settings S4 Decrease artificial variation in surgical scheduling S5 Decrease demand for hospital beds by reducing hospital acquired conditions S6 Reduce ED visits & hospital admissions through delivering appropriate care S7 Oversight system for hospital-wide operations to optimize patient flow S8 Real-time demand and capacity management processes S9 Flex capacity to meet hourly, daily and seasonal variations in demand S10 Early recognition for high census and surge planning S11 Improve efficiencies and throughput in the OR, ED, ICUs and Med/Surg Units S12 Improve efficiencies & coordination of discharge processes S13 Service Line Optimization (frail elders, SNF residents, stroke patients, etc.) S14 Reducing unnecessary variations in care and managing LOS outliers Specific Change Ideas C1 Reliably identify EOL wishes and proactively create and execute advanced illness plans C1 Development of palliative care programs (hospital-based and communitybased) C2 Reduce readmissions for high risk populations C3 Extended hours in primary care practices C3 Develop partnerships with Urgent Care and Retail Clinics C3 Enroll patients in community-based mental health services C3 Paramedics & EMTs triaging & treating patients at home C4 Separate scheduled and unscheduled flows in the OR C4 Redesign surgical schedules to create an predictable flow of patients to downstream ICUs and inpatient units C5 Decrease complications/harm (HAPU, CAUTI, SSI, falls with harm) and subsequent LOS C6 Reliably use of clinical pathways and evidence-based medicine C7 Assess seasonal variations and changes in demand patterns and proactively plan for variations C8 Daily flow planning huddles (improve predictions to synchronize admissions, discharges and discharges) C8 Real-time demand and capacity problem-solving (managing constraints and bottlenecks) C9 Planning capacity to meet predicted demand patterns C10 High census protocols to expedite admissions from the ED and manage surgical schedules. C11 Increase OR throughput through efficiency changes C11 ED efficiency changes to decrease LOS C11 Decrease LOS in ICUs (timely consults, tests and procedures) C11 Decrease LOS on Med/Surg Units (case management for patients with complex medical and social needs) C12 Initiate final discharge preparations when the patient is clinically ready for discharge C13 Care management for vulnerable/high risk patient populations C14 Advance planning for transfers to community-based care settings C14 Cooperative agreements with rehab facilities, SNFs and nursing homes
32 Draft Hospital Flow Metrics Emergency Department Hospital Macro Average Occupancy Rate Readmissions within 1 week of discharge Readmissions within 30 days after discharge Patient experience (HCAHPS measures related to waits & delays) Clinician and staff satisfaction related to workload (ex. NDNQI) Number of off-service patients Number of HACs (ex. falls with injury, VAPs, etc.) ED diversions o # of diversions o hours per month Patients who left without being seen Visits per day Average length of stay o for patients who are discharged o for patients who are admitted Door to provider time Time from decision to admit to transfer to inpatient unit Number of ED boarders waiting to be admitted to a hospital bed Time from decision to have emergency surgery to OR Percentage of ESI level 4 & 5 patients (low acuity) Percentage of patients who were admitted
33 Draft Hospital Flow Metrics Med/Surg Units Critical Care Units Average Census Average Length of Stay Number of LOS outliers per month Number of decedents spending 7 or more days in the ICU in the last 6 months of life Number of ICU diversions due to lack of capacity (# of off-service patients ) Nursing Overtime Number of HACs Delays in Transferring Patients to Med/Surg Units Average Census Average Length of Stay Number of LOS outliers per month Nursing Overtime Number of HACs Median discharge time (or discharge profile) Operating Rooms Number of emergency cases by day Number of scheduled cases by day Percentage of OR utilization Number of changes from schedule for Elective Surgical Cases Actual and Scheduled Start Times for Elective Surgical Cases Nursing Overtime o OR o PACU Number of overnight PACU patients
34 Shape or Reduce Demand Shape or Reduce Demand S1 Relocate care in ICUs and Medical and Surgical Units in accordance with patients EOL wishes S2 Decrease demand for Med/Surg beds by preventing avoidable readmissions S3 Relocate low-acuity care in EDs to community-based care settings S4 Decrease artificial variation in surgical scheduling S5 Decrease demand for hospital beds by reducing harm and hospital acquired conditions S6 Reduce demand for ED visits and hospital admissions through delivering appropriate care

35 The Conversation Continuum
36 Strategies to Reduce Readmissions Rehospitalizations are frequent, costly, and actionable for improvement Focus on addressing the medical and social needs patients and family caregivers, not penalties. The IHI approach acts on multiple levels engaging hospitals and community providers, communities, and state leaders in pursuit of a common aim to reduce avoidable rehospitalizations Working to reduce rehospitalizations focuses on improved communication and coordination over time and across settings With patients and family caregivers; Between clinical providers; Between the medical and social services (e.g. aging services, etc.) Working to reduce rehospitalizations is one part of a comprehensive strategy to promote patient-centered care and appropriate utilization of health care resources
37 Emergency Severity Index (ESI) and Patient Acuity Degree of Acuity Level of Acuity Patient Condition/Description High LEVEL 1 EMERGENT LEVEL 2 URGENT Medium LEVEL 3 ACUTE Low LEVEL 4 ROUTINE LEVEL 5 ROUTINE Patients in this category require immediate attention with maximal utilization of resources to prevent loss of life, limb, or eyesight. Patients in this category should be seen by a physician because of high risk for rapid deterioration, loss of life, limb, or eyesight if treatment or interventions are delayed. Patients who develop a sudden illness or injury within hours. Symptoms and risk factors for serious disease do not indicate a likelihood of rapid deterioration in the near future. Patients with chronic complaints, medical maintenance, or medical conditions posing no threat to loss of life, limb, or eyesight. Patients in this category are currently stable and require no resources such as labs or x-ray.
38 Managing and Reducing Variability in Surgical Scheduling Natural Variability (Clinical Variability, Flow Variability, Professional Variability) Random Can not be eliminated (or even reduced) Must be optimally managed Artificial Variability Non-random Non-predictable (driven by unknown individual priorities) Should not be managed, must be identified and eliminated Eugene Litvak, PhD Institute for Healthcare Optimization
39 Separate Flows for Elective and Non-Elective Surgical Cases Mayo Clinic Florida Surgical volume and surgical minutes increased by 4% and 5%, respectively; Prime time use increased by 5%; Overtime staffing decreased by 27%; Day-to-day variability decreased by 20%; The number of elective schedule same day changes decreased by 70%; Staff turnover rate decreased by 41%. Net operating income and margin improved by 38% and 28%, respectively C. Daniel Smith, et al. Re-Engineering the Operating Room Using Variability Management to Improve Healthcare Value. Journal of the American College of Surgeons, Volume 216, Issue 4, Pages , April 2013
40 Smooth the Flow of Electively Scheduled Surgical Cases By applying variability methodology, queuing theory and the I/T/O model, hospitals can identify and eliminate many of the patient flow impediments caused by operational inefficiencies By smoothing the inherent peaks-and valleys of patient flow, and eliminating the artificial variability, that unnecessarily impair patient flow, hospitals can improve patient safety and quality while simultaneously reducing hospital waste and cost IOM Report :The Future of Emergency Care in the U.S. Health System (Hospital-Based Emergency Care: At the Breaking Point)
41 Match Capacity Demand S7 Oversight system for hospital-wide operations to optimize patient flow Match Capacity and Demand S8 Flex capacity to meet hourly, daily and seasonal variations in demand S9 Real-time demand and capacity management processes S10 Early recognition for high census and surge planning
42 Flex Capacity to Meet Seasonal, Day of the Week and Hourly Variations in Demand Can you predict a surge in admissions for patients with medical conditions in the winter months? Use seasonal flex units to manage increases in medical patients during the winter months Can you anticipate which units need more bed capacity? (which services consistently have a large number of off-service patients) Use data analytics to quantify needs of each service Do you have a regular surge of activity mid-week with the hospital census regularly reaching >95% occupancy? Smooth elective surgical schedules (particularly for patients who will require ICU care post-op)
43 Classic ED Patient Demand Patterns Emergency Department Admission Times : 1 Hour Increments Number Of Pts :00 1:00 2:00 3:00 4:00 5:00 6:00 7:00 8:00 9:00 10:00 11:00 12:00 13:00 14:00 15:00 16:00 17:00 18:00 19:00 20:00 21:00 22:00 23:00 FY2004 Q FY2005 Q [Trend-Star Data : Q-1 FY04 & 05
44 RN Capacity for Predicted ED Demand Aggregate Demand/RN Capacity Projected Total RN Demand Total RN Staffing
45 Admissions and Discharges Hospital Flow: Day of week, Hour of day, Emergency admissions, All admissions, Discharges
46 Redesign the System S11 Improve efficiencies and throughput in the OR, ED, ICUs and Med/Surg Units Redesign the System S12 Improve efficiencies & coordination of discharge processes S13 Service Line Optimization (frail elders, SNF residents, stroke patients, etc.) S14 Reducing unnecessary variations in care and managing LOS outliers
47 Moderate Urgent Care Home Supertrack/ Fast Track Urgent Care Supertrack/ Fast Track Home Urgent Care Moderate Moderate ED Moderate Urgent Care Home Critical Care Streams Home 2011, Jody Crane, MD, MBA, Charles E. Noon, Ph.D. Observation Pathways Algorithmic Dx and Tx Dx Limits Throughput Chest Pain CHF Asthma/COPD Gastro TIA Syncope Critical Care Pathways Algorithmic Dx/Tx Time Sensitive/ICU Code STEMI Code Sepsis Code Neuro Trauma Diagnostic Dilema Unclear Dx, Workup, and Tx Or Tx Duration/Outcome that is highly variable Variable, Staff/Patient Dependent Throughput
48 16-Bed MICU We need more beds! Emergency Center Reduced EC ICU admit time Sepsis Manage ment Bela Patel, MD and Khalid Almoosa, MD Reliable weaning protocol ICU VAP, CR-BSI bundles Standardize family meetings Reduce admission delays Stabilization Weaning Complications End-of- Life Ward Home Other facility Wards RRT team Sepsis protocol Weaning protocol VAP & BSI prevention Family meetings RRT to reduce floor codes
49 Sheffield Teaching Hospitals NHS Trust Focused on Geriatric Medicine Service: 33% of medicine patients over 75 with and increasing number over 90 years old; 50% were receiving specialized care/therapy; 50% awaiting discharge coordination Analysis of outlier hospital stays revealed multiple points when patients could have been discharged; 66% of frail elders arrived after 6PM and were not seen by geriatrician until the next morning (20% of patients had the diagnosis changed after being seen by the geriatrician) Changes: Matched specialist capacity to patient demand Developed a Frailty Unit with specialized focus and teams Sped up discharge process and patients discharged when medically ready; home assessment for safety and support (saved up to two weeks); Continuous improvement teams continuously looking for additional ways to shorten hospital stays Improving the flow of older people. Sheffield Teaching Hospital NHS Trust s experience of the Flow Cost Quality improvement programme April 2013 The Health Foundation
50 Sheffield Teaching Hospitals NHS Trust Improving the flow of older people. Sheffield Teaching Hospital NHS Trust s experience of the Flow Cost Quality improvement programme April 2013 The Health Foundation
51 Decrease overutilization of hospital services Optimize patient placement to insure the right care, in the right place, at the right time Increase clinician and staff satisfaction Demonstrate a ROI for the systems moving to bundled payment arrangements Driver Diagram: Ideas to Improve Hospital Flow Outcomes Primary Drivers Secondary Drivers Shape or Reduce Demand Match Capacity and Demand Redesign the System S1 Relocate care in ICUs in accordance with patients EOL wishes S2 Decrease demand for Med/Surg beds by preventing avoidable readmissions S3 Relocate low-acuity care in EDs to community-based care settings S4 Decrease artificial variation in surgical scheduling S5 Decrease demand for hospital beds by reducing hospital acquired conditions S6 Reduce ED visits & hospital admissions through delivering appropriate care S7 Oversight system for hospital-wide operations to optimize patient flow S8 Real-time demand and capacity management processes S9 Flex capacity to meet hourly, daily and seasonal variations in demand S10 Early recognition for high census and surge planning S11 Improve efficiencies and throughput in the OR, ED, ICUs and Med/Surg Units S12 Improve efficiencies & coordination of discharge processes S13 Service Line Optimization (frail elders, SNF residents, stroke patients, etc.) S14 Reducing unnecessary variations in care and managing LOS outliers Specific Change Ideas C1 Reliably identify EOL wishes and proactively create and execute advanced illness plans C1 Development of palliative care programs (hospital-based and communitybased) C2 Reduce readmissions for high risk populations C3 Extended hours in primary care practices C3 Develop partnerships with Urgent Care and Retail Clinics C3 Enroll patients in community-based mental health services C3 Paramedics & EMTs triaging & treating patients at home C4 Separate scheduled and unscheduled flows in the OR C4 Redesign surgical schedules to create an predictable flow of patients to downstream ICUs and inpatient units C5 Decrease complications/harm (HAPU, CAUTI, SSI, falls with harm) and subsequent LOS C6 Reliably use of clinical pathways and evidence-based medicine C7 Assess seasonal variations and changes in demand patterns and proactively plan for variations C8 Daily flow planning huddles (improve predictions to synchronize admissions, discharges and discharges) C8 Real-time demand and capacity problem-solving (managing constraints and bottlenecks) C9 Planning capacity to meet predicted demand patterns C10 High census protocols to expedite admissions from the ED and manage surgical schedules. C11 Increase OR throughput through efficiency changes C11 ED efficiency changes to decrease LOS C11 Decrease LOS in ICUs (timely consults, tests and procedures) C11 Decrease LOS on Med/Surg Units (case management for patients with complex medical and social needs) C12 Initiate final discharge preparations when the patient is clinically ready for discharge C13 Care management for vulnerable/high risk patient populations C14 Advance planning for transfers to community-based care settings C14 Cooperative agreements with rehab facilities, SNFs and nursing homes
52 Strategies to Achieve System-Wide Hospital Flow Outcomes Strategies Primary Drivers Strategic Priority and Aligned Incentives Decrease overutilization of hospital services Optimize patient placement to insure the right care, in the right place, at the right time Increase clinician and staff satisfaction Demonstrate a ROI for the systems moving to bundled payment arrangements Will Ideas Execution Mutuality between Physicians and Hospital Executives Integrated Health Care Systems and/or ACOs Avoidance of Capital Expenditures Positive ROI and Financial Viability Shape the Demand Match Capacity and Demand Redesign the System Utilization of Hospital-wide Metrics to Guide Learning Within and Across Projects for Achieving Results Accountable Executive Leadership Providing Oversight of System-Level Performance Data Analytics to Provide Real-time Capacity and Demand Management and Forecasting Micro-system Quality Improvement Capability and Empowerment
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time
 This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Hospital Flow Professional Development Program
This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Hospital Flow Professional Development Program
Hospital Flow: Right Care, in the Right Place, at the Right Time. Pat Rutherford, RN, MS Vice President, Institute for Healthcare Improvement
 Q11 This presenter has nothing to disclose Hospital Flow: Right Care, in the Right Place, at the Right Time Pat Rutherford, RN, MS Vice President, Institute for Healthcare Improvement IHI s National Forum
Q11 This presenter has nothing to disclose Hospital Flow: Right Care, in the Right Place, at the Right Time Pat Rutherford, RN, MS Vice President, Institute for Healthcare Improvement IHI s National Forum
Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand
 This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov. 2016 Frederick C. Ryckman, MD Professor of Surgery / Transplantation
This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov. 2016 Frederick C. Ryckman, MD Professor of Surgery / Transplantation
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Hospital Flow Case Study: Cincinnati Children s Hospital
 Hospital Flow Case Study: Cincinnati Children s Hospital Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati,
Hospital Flow Case Study: Cincinnati Children s Hospital Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati,
Achieving Hospital-wide Patient Flow
 WHITE PAPER Achieving Hospital-wide Patient Flow The Right Care, in the Right Place, at the Right Time AN IHI RESOURCE 20 University Road, Cambridge, MA 02138 ihi.org How to Cite This Paper: Rutherford
WHITE PAPER Achieving Hospital-wide Patient Flow The Right Care, in the Right Place, at the Right Time AN IHI RESOURCE 20 University Road, Cambridge, MA 02138 ihi.org How to Cite This Paper: Rutherford
Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA
 These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
Assessing and Optimizing Operations and Patient Flow in VHA Facilities
 Assessing and Optimizing Operations and Patient Flow in VHA Facilities A six-month professional development program for VHA leaders and staff PROFESSIONAL DEVELOPMENT PROGRAM Assessing and Optimizing Operations
Assessing and Optimizing Operations and Patient Flow in VHA Facilities A six-month professional development program for VHA leaders and staff PROFESSIONAL DEVELOPMENT PROGRAM Assessing and Optimizing Operations
Inpatient Flow Real Time Demand Capacity: Building the System
 Inpatient Flow Real Time Demand Capacity: Building the System Roger Resar, MD, Kevin Nolan, and Deb Kaczynski We would like to acknowledge the conceptual contributions of Diane Jacobsen, Marilyn Rudolph,
Inpatient Flow Real Time Demand Capacity: Building the System Roger Resar, MD, Kevin Nolan, and Deb Kaczynski We would like to acknowledge the conceptual contributions of Diane Jacobsen, Marilyn Rudolph,
Decreasing Environmental Services Response Times
 Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL
 Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
THE NEW IMPERATIVE: WHY HEALTHCARE ORGANIZATIONS ARE SEEKING TRANSFORMATIONAL CHANGE AND HOW THEY CAN ACHIEVE IT
 Today s challenges are not incremental, but transformational; across the country, many CEOs and executives in healthcare see the need not merely to improve traditional ways of doing business, but to map
Today s challenges are not incremental, but transformational; across the country, many CEOs and executives in healthcare see the need not merely to improve traditional ways of doing business, but to map
Online library of Quality, Service Improvement and Redesign tools. Discharge planning. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Hospital Patient Flow Capacity Planning Simulation Model at Vancouver Coastal Health
 Hospital Patient Flow Capacity Planning Simulation Model at Vancouver Coastal Health Amanda Yuen, Hongtu Ernest Wu Decision Support, Vancouver Coastal Health Vancouver, BC, Canada Abstract In order to
Hospital Patient Flow Capacity Planning Simulation Model at Vancouver Coastal Health Amanda Yuen, Hongtu Ernest Wu Decision Support, Vancouver Coastal Health Vancouver, BC, Canada Abstract In order to
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation
 Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Part 4. Change Concepts for Improving Adult Cardiac Surgery. In this section, you will learn a group. of change concepts that can be applied in
 Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Matching Capacity and Demand:
 We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
AirStrip ONE Cardiology
 AirStrip ONE Cardiology A Synchronized View of the Vital Patient Data Needed to Improve Care Heart disease is the leading cause of death in the U.S. The associated costs exceed $100 billion annually. AirStrip
AirStrip ONE Cardiology A Synchronized View of the Vital Patient Data Needed to Improve Care Heart disease is the leading cause of death in the U.S. The associated costs exceed $100 billion annually. AirStrip
Strategies to Achieve System- Wide Hospital Flow
 This presenter has nothing to disclose trategies to Achieve ystem- Wide Hospital Flow Pat Rutherford, Vice President, IHI IHI s ational Forum December 5, 2016 Orlando, Florida Hospital Flow: Impact on
This presenter has nothing to disclose trategies to Achieve ystem- Wide Hospital Flow Pat Rutherford, Vice President, IHI IHI s ational Forum December 5, 2016 Orlando, Florida Hospital Flow: Impact on
Boarding Impact on patients, hospitals and healthcare systems
 Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Perfecting Emergency Department Operations
 These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Publication Year: 2013
 THE INITIAL ASSESSMENT PROCESS ST. JOSEPH'S HEALTHCARE HAMILTON Publication Year: 2013 Summary: The Initial Assessment Process (IAP) was developed collaboratively by the emergency physicians, nursing,
THE INITIAL ASSESSMENT PROCESS ST. JOSEPH'S HEALTHCARE HAMILTON Publication Year: 2013 Summary: The Initial Assessment Process (IAP) was developed collaboratively by the emergency physicians, nursing,
The Nature of Emergency Medicine
 Chapter 1 The Nature of Emergency Medicine In This Chapter The ED Laboratory The Patient The Illness The Unique Clinical Work Sense Making Versus Diagnosing The ED Environment The Role of Executive Leadership
Chapter 1 The Nature of Emergency Medicine In This Chapter The ED Laboratory The Patient The Illness The Unique Clinical Work Sense Making Versus Diagnosing The ED Environment The Role of Executive Leadership
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Creating a Data-Driven Culture to Right-Size Capacity and Enhance Quality and Safety
 Creating a Data-Driven Culture to Right-Size Capacity and Enhance Quality and Safety MaryPat Sullivan, CNO and Chief Experience Officer, Overlook Medical Center, Atlantic Health System, Summit, NJ Jacalyn
Creating a Data-Driven Culture to Right-Size Capacity and Enhance Quality and Safety MaryPat Sullivan, CNO and Chief Experience Officer, Overlook Medical Center, Atlantic Health System, Summit, NJ Jacalyn
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
South Warwickshire s Whole System Approach Transforms Emergency Care. South Warwickshire NHS Foundation Trust
 South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
Emergency Department Patient Flow Strategies. University of Maryland Medical Center
 Emergency Department Patient Flow Strategies University of Maryland Medical Center Medical Admitting Officer Attending Hospitalist Hours: 9a 11p Mon Friday Goal to partner with ED team and provide oversight
Emergency Department Patient Flow Strategies University of Maryland Medical Center Medical Admitting Officer Attending Hospitalist Hours: 9a 11p Mon Friday Goal to partner with ED team and provide oversight
How Allina Saved $13 Million By Optimizing Length of Stay
 Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Kingston Hospital NHS Foundation Trust Length of stay case study. October 2014
 Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
Real Time Demand Capacity Surge Planning
 This presenter has nothing to disclose. Real Time Demand Capacity Surge Planning Katharine Luther, RN, MPM April 6, 2016 Theoretical Frameworks P2 Queuing Theory Compression wave Framework P3 Resar,, Roger
This presenter has nothing to disclose. Real Time Demand Capacity Surge Planning Katharine Luther, RN, MPM April 6, 2016 Theoretical Frameworks P2 Queuing Theory Compression wave Framework P3 Resar,, Roger
WHITE PAPER. Key Strategies for Improving Hospital Flow. Content
 WHITE PAPER Key Strategies for Improving Hospital Flow BY: Kirk B. Jensen, MD, MBA, FACEP Content The ED is a part of a hospital-wide system of patient flow Every system produces the results it is designed
WHITE PAPER Key Strategies for Improving Hospital Flow BY: Kirk B. Jensen, MD, MBA, FACEP Content The ED is a part of a hospital-wide system of patient flow Every system produces the results it is designed
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
The Impact of Emergency Department Use on the Health Care System in Maryland. Deborah E. Trautman, PhD, RN
 The Impact of Emergency Department Use on the Health Care System in Maryland Deborah E. Trautman, PhD, RN The Future of Emergency Care in the United States Health System Institute of Medicine June 2006
The Impact of Emergency Department Use on the Health Care System in Maryland Deborah E. Trautman, PhD, RN The Future of Emergency Care in the United States Health System Institute of Medicine June 2006
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Building Systems and Leadership for Transformation
 Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Emergency Medicine Programme
 Emergency Medicine Programme Implementation Guide 8: Matching Demand and Capacity in the ED January 2013 Introduction This is a guide for Emergency Department (ED) and hospital operational management teams
Emergency Medicine Programme Implementation Guide 8: Matching Demand and Capacity in the ED January 2013 Introduction This is a guide for Emergency Department (ED) and hospital operational management teams
Neurosurgery. Themes. Referral
 06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
Get A Seat at the Table
 Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance
 Directorate for Health Workforce and Performance") Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Managing Healthcare Payment Opportunity Fundamentals CENTER FOR INDUSTRY TRANSFORMATION
 Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement
 to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement") Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
Value model in the new healthcare paradigm: Producing value at a single specialty center.
 Value model in the new healthcare paradigm: Producing value at a single specialty center. State of Spine Surgery Think Tank June 17, 2017 Catherine MacLean, MD, PhD Chief Value Medical Officer Center for
Value model in the new healthcare paradigm: Producing value at a single specialty center. State of Spine Surgery Think Tank June 17, 2017 Catherine MacLean, MD, PhD Chief Value Medical Officer Center for
Clinical Program Cost Leadership Improvement
 Clinical Program Cost Leadership Improvement December 2017 Presbyterian recently developed a rapid-cycle process for integrating sustainable cost and quality improvements within clinical programs. Population
Clinical Program Cost Leadership Improvement December 2017 Presbyterian recently developed a rapid-cycle process for integrating sustainable cost and quality improvements within clinical programs. Population
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES
 EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Addressing ambulance handover delays: actions for local accident and emergency delivery boards
 Addressing ambulance handover delays: actions for local accident and emergency delivery boards Published by NHS England and NHS Improvement November 2017 Contents Foreword... 2 Actions to be taken now,
Addressing ambulance handover delays: actions for local accident and emergency delivery boards Published by NHS England and NHS Improvement November 2017 Contents Foreword... 2 Actions to be taken now,
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
The Case for Home Care Medicine: Access, Quality, Cost
 The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
How to Win Under Bundled Payments
 How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE
 EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
Prepared for Becker s ASC + Spine Conference. Transforming Spine Service Line Performance. Powered by Collaboration and Analytics
 June 11-13 2015 Prepared for Becker s ASC + Spine Conference Transforming Spine Service Line Performance Powered by Collaboration and Analytics Brain & Spine service line optimization case study Situation
June 11-13 2015 Prepared for Becker s ASC + Spine Conference Transforming Spine Service Line Performance Powered by Collaboration and Analytics Brain & Spine service line optimization case study Situation
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations
 ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
Final Version Simple Guide to the Care Act and Delayed Transfers of Care (DTOC) SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC)
 SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC)") SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC) 1. UNDERPINNING PRINCIPLES Across the whole system, our common aims are to: Improve services for patients by avoiding situations where,
SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC) 1. UNDERPINNING PRINCIPLES Across the whole system, our common aims are to: Improve services for patients by avoiding situations where,
Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty
 Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Examining a range of
Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Examining a range of
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
BIG ISSUES IN THE NEXT TEN YEARS OF IMPROVEMENT
 BIG ISSUES IN THE NEXT TEN YEARS OF IMPROVEMENT Academy for Health Services Research and Health Policy Annual Meeting Washington, DC: June 24, 2002 Donald M. Berwick, MD, MPP Patient and Community The
BIG ISSUES IN THE NEXT TEN YEARS OF IMPROVEMENT Academy for Health Services Research and Health Policy Annual Meeting Washington, DC: June 24, 2002 Donald M. Berwick, MD, MPP Patient and Community The
Value, Suffering, and 10 Things I Didn t Know Before My New Job
 Value, Suffering, and 10 Things I Didn t Know Before My New Job Thomas H. Lee, MD October 28, 2013 2 1 Why We Are Stuck 3 Getting Unstuck 2 Step One: Clarifying the Overarching Goal In the absence of an
Value, Suffering, and 10 Things I Didn t Know Before My New Job Thomas H. Lee, MD October 28, 2013 2 1 Why We Are Stuck 3 Getting Unstuck 2 Step One: Clarifying the Overarching Goal In the absence of an
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department
 Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Improving Patient Flow & Reducing Emergency Department (ED) Crowding
 Crowding") February 2010 URGENT MATTERS LEARNING NETWORK II ISSUE BRIEF 1 Improving Patient Flow & Reducing Emergency Department (ED) Crowding Robert Wood Johnson Foundation-Supported Learning Network of Hospitals
February 2010 URGENT MATTERS LEARNING NETWORK II ISSUE BRIEF 1 Improving Patient Flow & Reducing Emergency Department (ED) Crowding Robert Wood Johnson Foundation-Supported Learning Network of Hospitals
Pushing Case Management into the Future: Six Requirements to Drive Clinical and Financial Returns
 Pushing Case Management into the Future: Six Requirements to Drive Clinical and Financial Returns Authors: Loren Mann, Mark Werner, MD and Cynthia Bailey Hospital-based case management (CM) should be a
Pushing Case Management into the Future: Six Requirements to Drive Clinical and Financial Returns Authors: Loren Mann, Mark Werner, MD and Cynthia Bailey Hospital-based case management (CM) should be a
Can physicians do as well as orthopaedic surgeons: letting go of the discharge decision.
 Can physicians do as well as orthopaedic surgeons: letting go of the discharge decision. Dr. Simon Watkin Consultant physician NHS Borders Simon.watkin@borders.scot.nhs.uk What does it mean The establishment
Can physicians do as well as orthopaedic surgeons: letting go of the discharge decision. Dr. Simon Watkin Consultant physician NHS Borders Simon.watkin@borders.scot.nhs.uk What does it mean The establishment
Creating a No Wait ED
 This presenter has nothing to disclose Creating a No Wait ED Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Process Improvement
This presenter has nothing to disclose Creating a No Wait ED Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Process Improvement
Bundled Payments. AMGA September 25, 2013 AGENDA. Who Are We. Our Business Challenge. Episode Process. Experience
 Bundled Payments AMGA September 25, 2013 Who Are We AGENDA Our Business Challenge Episode Process Experience 1 Cleveland Clinic is transforming Fee for service Fee for value 3 Fast Facts 41,200 employees
Bundled Payments AMGA September 25, 2013 Who Are We AGENDA Our Business Challenge Episode Process Experience 1 Cleveland Clinic is transforming Fee for service Fee for value 3 Fast Facts 41,200 employees
THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT
 April 13, 2018 The Misadventures of the Recently-Discharged Older Adult THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT Robert E. Burke MD, MS April 13, 2018 I have no conflicts of interest to
April 13, 2018 The Misadventures of the Recently-Discharged Older Adult THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT Robert E. Burke MD, MS April 13, 2018 I have no conflicts of interest to
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
CAMDEN CLARK MEDICAL CENTER:
 INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
How Integrated Clinical Services and Technologies are Making Healthcare Work Better. Local Practice Divisional Support National Resources
 How Integrated Clinical Services and Technologies are Making Healthcare Work Better Local Practice Divisional Support National Resources YOUR PRESENTERS Kirk Jensen, MD, MBA, FACEP Chief Medical Officer,
How Integrated Clinical Services and Technologies are Making Healthcare Work Better Local Practice Divisional Support National Resources YOUR PRESENTERS Kirk Jensen, MD, MBA, FACEP Chief Medical Officer,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement?
 Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Expedition: Improving Safety and Reliability for Surgical Procedures
 These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
Getting the right case in the right room at the right time is the goal for every
 OR throughput Are your operating rooms efficient? Getting the right case in the right room at the right time is the goal for every OR director. Often, though, defining how well the OR suite runs depends
OR throughput Are your operating rooms efficient? Getting the right case in the right room at the right time is the goal for every OR director. Often, though, defining how well the OR suite runs depends
LWOT Reduction Plan Success Story: Advocate Trinity Hospital
 LWOT Reduction Plan Success Story: Advocate Trinity Hospital Draft Submitted Jan. 6, 2011 Jacquelyn Whitten, DNP, RN Kimberly McIntyre, EdD(c), MSN, RN Julian M. Magdaleno, MS February 19, 2012 The Leaving
LWOT Reduction Plan Success Story: Advocate Trinity Hospital Draft Submitted Jan. 6, 2011 Jacquelyn Whitten, DNP, RN Kimberly McIntyre, EdD(c), MSN, RN Julian M. Magdaleno, MS February 19, 2012 The Leaving
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Healthcare Reform Hospital Perspective
 Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
Select Medical TRANSITIONS OF CARE & CARE COORDINATION
 Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
Why Focus on Perioperative Services?
 1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through Telemedicine
 PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
Predictive Analytics and the Impact on Nursing Care Delivery
 Predictive Analytics and the Impact on Nursing Care Delivery Session 2, March 5, 2018 Whende M. Carroll, MSN, RN-BC - Director of Nursing Informatics, KenSci, Inc. Nancee Hofmeister, MSN, RN, NE-BC Senior
Predictive Analytics and the Impact on Nursing Care Delivery Session 2, March 5, 2018 Whende M. Carroll, MSN, RN-BC - Director of Nursing Informatics, KenSci, Inc. Nancee Hofmeister, MSN, RN, NE-BC Senior
HOW BPCI EPISODE PRECEDENCE AFFECTS HEALTH SYSTEM STRATEGY WHY THIS ISSUE MATTERS
 HOW BPCI EPISODE PRECEDENCE AFFECTS HEALTH SYSTEM STRATEGY Jonathan Pearce, CPA, FHFMA and Coleen Kivlahan, MD, MSPH Many participants in Phase I of the Medicare Bundled Payment for Care Improvement (BPCI)
HOW BPCI EPISODE PRECEDENCE AFFECTS HEALTH SYSTEM STRATEGY Jonathan Pearce, CPA, FHFMA and Coleen Kivlahan, MD, MSPH Many participants in Phase I of the Medicare Bundled Payment for Care Improvement (BPCI)
BUILDING THE PATIENT-CENTERED HOSPITAL HOME
 WHITE PAPER BUILDING THE PATIENT-CENTERED HOSPITAL HOME A New Model for Improving Hospital Care Authors Sonya Pease, MD Chief Medical Officer TeamHealth Anesthesia Kurt Ehlert, MD National Director, Orthopaedics
WHITE PAPER BUILDING THE PATIENT-CENTERED HOSPITAL HOME A New Model for Improving Hospital Care Authors Sonya Pease, MD Chief Medical Officer TeamHealth Anesthesia Kurt Ehlert, MD National Director, Orthopaedics
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus