Pre-operative categorization (triaging) of emergency surgical cases. A tool for improving patient care and emergency operating room efficiency
|
|
|
- Thomasina Burke
- 6 years ago
- Views:
Transcription
 of emergency surgical")

1 Pre-operative categorization (triaging) of emergency surgical cases A tool for improving patient care and emergency operating room efficiency
2 Introduction No national or provincial guidelines exist for the categorization or triaging of emergency surgical cases. In the current climate of shrinking elective operating time and increasing surgical waiting times, the present focus of health planners is to decrease elective waiting times by establishing initiatives aimed at improving overall theatre efficiency. Emergency surgical case loads form a significant and increasing percentage (average 5-7% annually) of all patients utilizing theatre facilities.
3 Why is elective surgery different from emergency surgery? Planned (patient, hospital, surgical/anaesthetic team). Length of surgery, hospital stay and morbidity and mortality can be predicted or inferred One surgical team has exclusive access to a predetermined number of operating hours Occurs during in hours when infrastructural support is at maximum Inefficiencies on any one slate are relatively static and thus (potentially) easily addressed

4 Definition of an emergency surgical case Unplanned and unscheduled manner. Acute surgical conditions Prompt and focused Minimize morbidity and mortality
 loading emergency lists with many non-urgent (but not purely elective)")
5 A bit of history Prior to 1992 only after hours emergency theatre Emergency cases crashed elective lists After 1992: With increasing burden of emergency cases,each surgical discipline gives up session to man 24 hour emergency theatre Increasing attrition of elective lists (66% decrease in elective slates since 1992) loading emergency lists with many non-urgent (but not purely elective) cases

6 Something has to give..

7 Do something!!!
8 Emergency Theatre Utilization Audit Carried out over 91 days from the second week of May 2006 Only cases booked on the emergency board audited 915 cases booked on emergency board during audit period 57 cases removed from the board and not re-booked A total of 858 cases booked on the emergency list were done during the audit period, but only 657 questionnaires were filled in giving a return rate of 77%
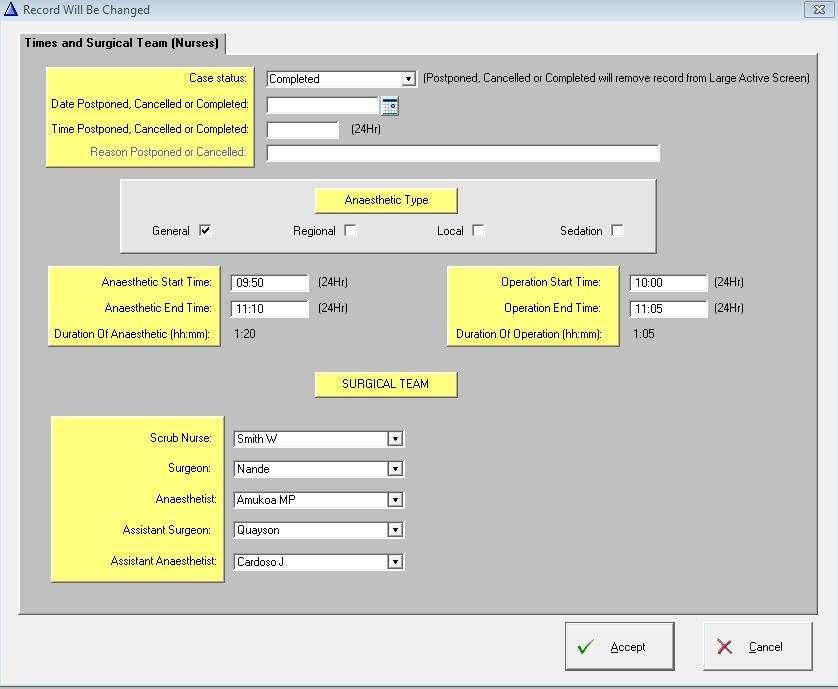
9 Emergency Theatre Case Audit Form Patient Sticker 1. Procedure booked: 2. Date and time case booked: 3. Patient evaluation by anaesthetist: on arrival in theatre in ward 4. Was patient ready for theatre when evaluated? YES NO 5. If not, state why: 6. Patient s ASA grade: I II III IV V 7. Date and time Patient sent for: 8. Time patient arrived in induction room: 9. Was surgeon available when required: YES NO 10. If not, state why: 11. Anaesthesia time: From: To: ; GA regional both 12. Surgical time: From: To: 13. Grade of surgeon performing operation: registrar consultant 14. Grade of anaesthetist responsible: jun. reg. sen. reg. consult. 15. Procedure: performed postponed cancelled abandoned 16. If case not performed state reason/s: Theatre: D:
10 Specialty Case Mix General/ICU Orthopaedics Vascular Not classified Neuro Obs/Gynae Ophthal MaxFax/ENT Trauma Uro/Renal Plastics Thoracics Emergency theatre audit 2006
11 600 87% Point of Evaluation by Anaesthesia 500 No. of Cases % 2.3% 0.7% 0 Theater Ward ICU Other
12 Grade of Anaesthesia Staff 52% No. of Cases % 21% Consultant Snr. Reg. Jnr.Reg/MO No Data 1%
13 Grade of Surgical Staff Operating 86% No. of Cases % 2% 0 Consultant Registrar No Data
14 Audit recommendations Dedicated, protected nursing team for emergency theatre Establishment of urgent theatre to deal with increasing number of less urgent cases Establishment of a Post Anaesthesia High Care Unit More active participation of on call team in the pre-operative assessment of cases booked on the emergency slate

15 Who will be responsible for assessment?

16 Triage registrar Senior registrar in cardiac rotation Evaluates ALL cases booked on the emergency board and consults with surgical team regarding optimisation strategy, if required. Link between emergency anaesthetic team and surgical team Dedicated to triage only, Monday to Friday
17 Surgical procedure: Emergency Case Evaluation Form Patient sticker Admission date: Time: Ward: Surgical specialty/firm: Date and time of booking: Initial categorization: R O Y G B (circle one) Date and time of surgery: Carbonated pad Hard copy remains in patient s folder Medical/surgical history: Risk assessment: ASA: NYHA: METS: Previous anaesthetic complications: Drug therapy: Drug allergy: General examination: Wt: BMI: Cardiovascular: Pulses: BP: JVP: H S: Murmurs: Respiratory/airway: Mallampati: AO-ROM: good restricted ThMD: adequate inadequate Other systems: Investigations Hb : Na+: ph: Plts : K+: pco₂: INR: Urea: po₂: Glucose: Creat: HCO₃: Albumin: GFR: BE: Other: CXR ECG Recommendations: Additional investigations: Group &Screen: X-match: Units Please refer patient to for consultation prior to planned procedure. Evaluated by: Time: Date: Speed dial: Bleep:

18 What about the surgeons?

19 Why triage emergency surgical cases? Decreases waiting times for sickest patients Improves management of clinical risk Decreases morbidity and mortality Promotes appropriate use of scarce resources Audit

20 Which triage tool.?
21 Principles are to identify The walking wounded Patients that need immediate help/evacuation and have good chance of survival/recovery Patients that are likely to die despite treatment The dead by using scoring systems based on physical/physiological parameters, and prioritise actions and resources towards those most likely to benefit.
22
23 The Cape Triaging Score (CTS) was developed by the Cape Triage Group¹ Introduced for use in emergency units throughout the country as well as in the pre-hospital setting. Has three versions: Adult, children, infant Uses a physiologically based scoring system (Triage Early Warning Score- TEWS) and certain discriminators (mechanism of injury, presentation, pain and discretion of senior health care professional responsible) that categorizes patients into one of five priority groups for medical attention.
24 Colour Status Red Immediate priority (resuscitation cases) Orange Very urgent priority- potentially life/limb threatening pathology Yellow Urgent priority- significant pathology Green Delayed priority minor injury/illness Blue Dead

25 Why not extend categorization beyond the ER?
26 Emergency case categorization chart The emergency surgical case categorization chart (ESCCC) is based on similar principles to the CTS. It has identical colour coded categories which define different levels of surgical acuity and gravity and suggests timing and urgency for operative intervention.
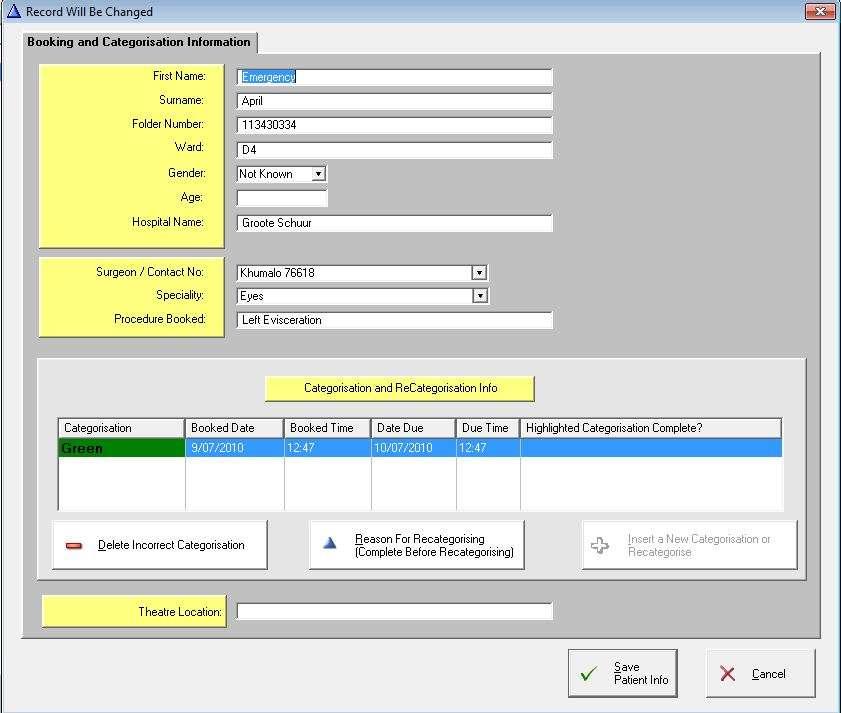
27 Icon Case Category Parameters Red Orange Yellow Green Blue Immediate Hot emergency Cold emergency Urgent Scheduled Immediate life saving operation, resuscitation simultaneous with surgical treatment e.g. resuscitative laparotomy, ruptured aortic aneurysm, threatened airway, cord prolapse, foetal bradycardia Operation as soon as possible after resuscitation (within 1 to2 hours) - e.g. ruptured ectopic pregnancy, leaking aortic aneurysm, cranial decompression, positive DPL in multiple trauma, threatened limb Operation within 6 hours of booking e.g. compound fractures, appendicitis, incarcerated hernia/intestinal obstruction, EUA for non-accidental injuries Operation not immediately life or limb saving but to be done within 24 hours of booking e.g. ORIF of simple fractures, bleeding haemorrhoids, I&D abscess Semi-urgent cases, to be done within 72 hours. Operation during in-hours on next available slate if possible
28 Management of system Blue cases become Green after 72 hours Green cases become yellow after 24 hours Yellow cases become orange after 6 hours Orange cases become red after 2 hours Booked cases must be assessed on an ongoing basis and recategorized as required The surgical team admitting a patient is responsible for the initial categorization of the case The anaesthetic team should be intimately involved in the triaging/categorization of cases with their surgical colleagues Arbitration between surgeons with similarly categorized patients regarding priority on emergency list to be decided by institution
29 What are the expected outcomes? Better communication and cohesion between emergency team Improved patient care (lower morbidiy and mortality) Better use of scarce emergency theatre time Appropriate use of resources Patient satisfaction
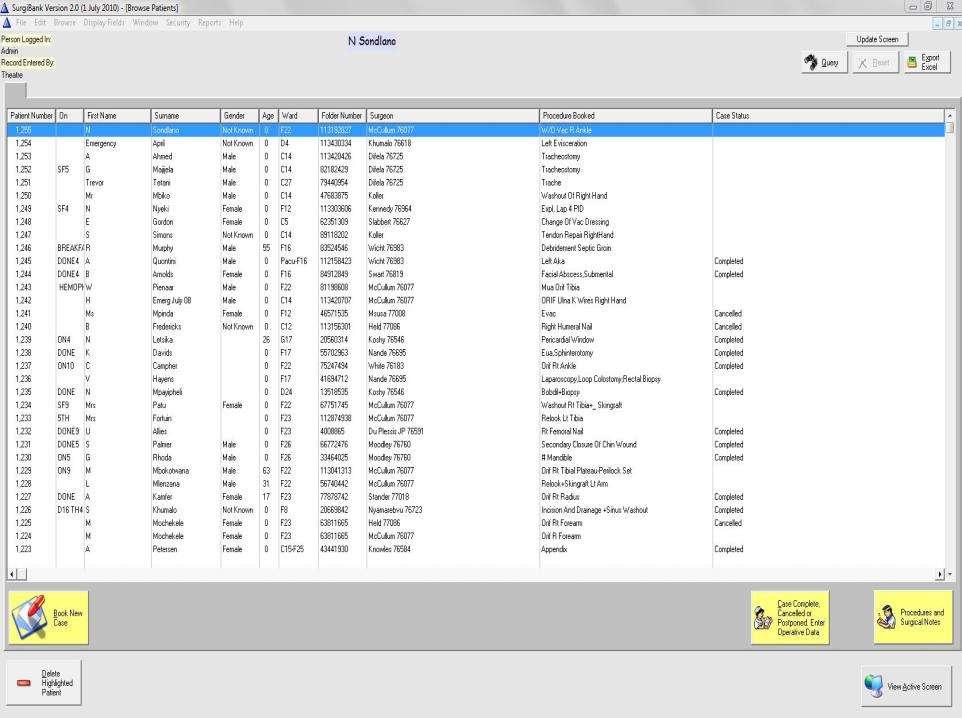
30 Status 2009 Urgent theatre one day per week (October 2008) Introduction of triage anaesthetic registrar (June 2009) Obligatory categorization of emergency cases by surgeon utilizing emergency case categorization chart (July 2009)
31 Triage registrar a great success Categorization by surgeons patchy Manual color coding by theatre staff inconsistent
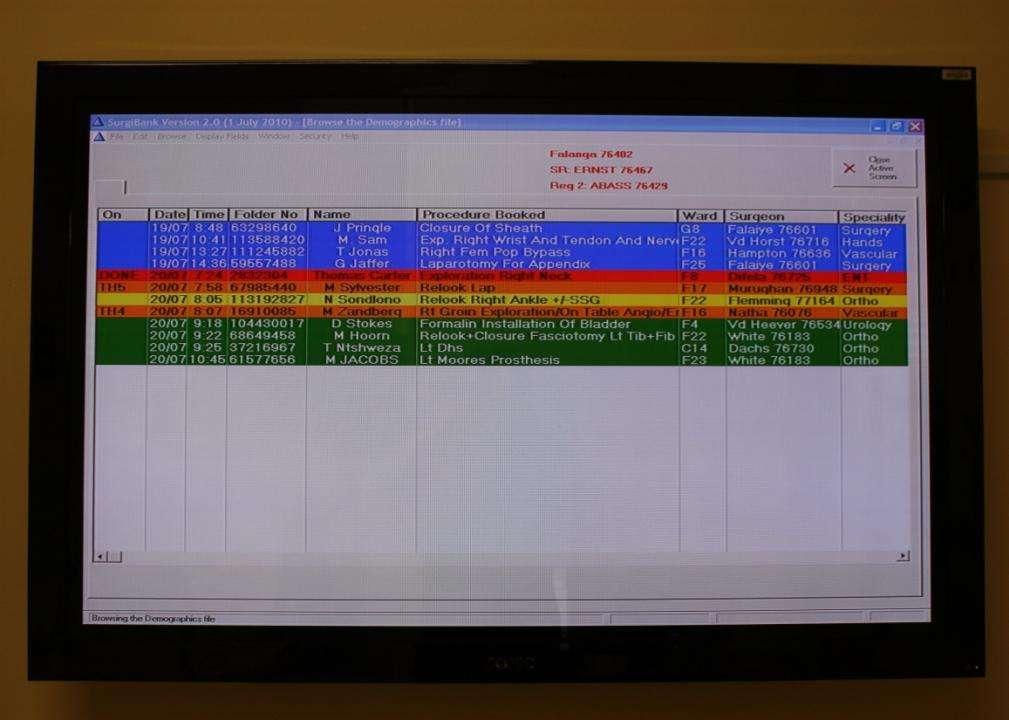
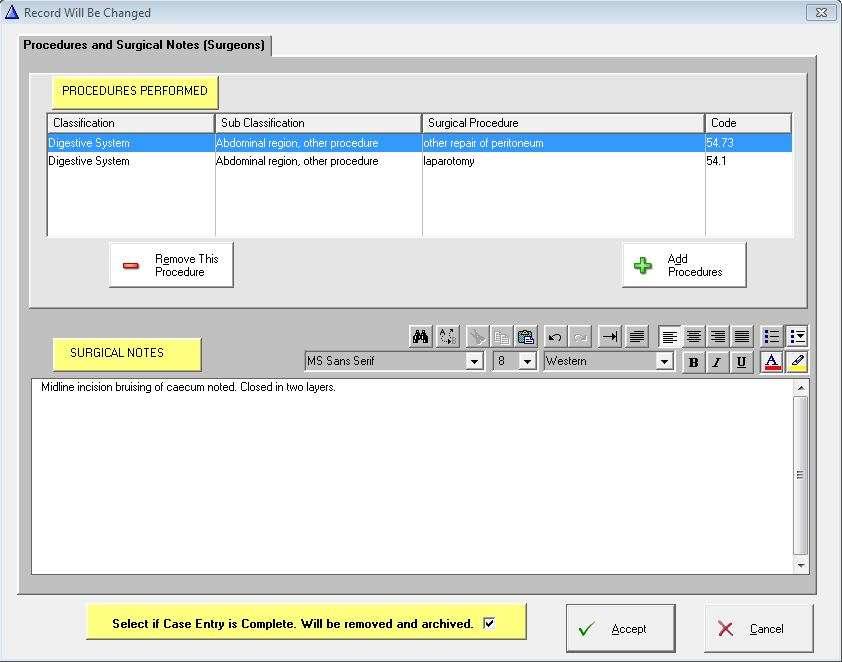
32 Where to from here? Computerize display of booking board to include automatic color coding of patients Computerize all input of data from emergency theatre currently entered in theatre registers etc

33
34
35
36
37
38
39
40
41 The electronic triage system (SurgiBank) has been enthusiastically embraced by nursing staff and anaesthetists despite early problems with program gremlins.

42 So far our surgical colleagues.
43 .. have generally been very positive, but there remain issues with compliance, particularly as regards the appropriate colour coding of patients and the entering of surgery specific data.
44 And now for some data..

45

46 Cases by Specialty Booked Completed Canc/post 0
47 Specialty Case Mix General/ICU Orthopaedics Vascular Not classified Neuro Obs/Gynae Ophthal MaxFax/ENT Trauma Uro/Renal Plastics Thoracics Emergency theatre audit 2006

48 26 Percentage of total: By specialty
49 Booked Completed Cancelled/Post Totals

50 52 Times cases done: :00-17:00 17:01-24:00 After Midnight No Data

51 63% Times cases done: % 15% 07:01-19:00 19:01-24:00 00:01-06:59
")

52 No. Cases (2524) Cancelled 14% Postponed 4% Completed 82%
53 No. of Cases Completed Cancelled Postponed % Recategorized % on time 232 (9%) 370 (15%) 856 (34%) 918 (36%) 166 (6%) 216 (93%) 341 (92%) 735 (86%) 692 (75%) 103 (62%) 16 (7%) (7%) 5 (1%) (11%) 31 (3%) (19%) 56 (6%) (31%) 11 (7%) 13 87
54

55
DRAFT POLICY GUIDELINES FOR THE BOOKING OF SURGICAL CASES ON THE EMERGENCY SLATE
 INTRODUCTION DRAFT POLICY GUIDELINES FOR THE BOOKING OF SURGICAL CASES ON THE EMERGENCY SLATE With the aim of improving emergency surgical case access to emergency theatre services the following areas
INTRODUCTION DRAFT POLICY GUIDELINES FOR THE BOOKING OF SURGICAL CASES ON THE EMERGENCY SLATE With the aim of improving emergency surgical case access to emergency theatre services the following areas
PRACTICE GUIDELINE EM014 IMPLEMENTATION OF THE SOUTH AFRICAN TRIAGE SCALE
 PRACTICE GUIDELINE EM014 IMPLEMENTATION OF THE SOUTH AFRICAN TRIAGE SCALE This Practice Guideline sets out a method for implementing triage in the Emergency Centre. Excluding the cover page, this Practice
PRACTICE GUIDELINE EM014 IMPLEMENTATION OF THE SOUTH AFRICAN TRIAGE SCALE This Practice Guideline sets out a method for implementing triage in the Emergency Centre. Excluding the cover page, this Practice
@ncepod #tracheostomy
 @ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
@ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
7 NON-ELECTIVE SURGERY IN THE NHS
 Recommendations Debate whether, in the light of changes to the pattern of junior doctors working, non-essential surgery can take place during extended hours. 7 NON-ELECTIVE SURGERY IN THE NHS Ensure that
Recommendations Debate whether, in the light of changes to the pattern of junior doctors working, non-essential surgery can take place during extended hours. 7 NON-ELECTIVE SURGERY IN THE NHS Ensure that
St. James s Hospital, Dublin.
 Position Senior House Officer in Anaesthesia Organisational Area Department of Anaesthesia, St. James s Hospital. Closing Date Sunday the 9 th July 2018 SACC Directorate. The Surgery, Anaesthesia and Critical
Position Senior House Officer in Anaesthesia Organisational Area Department of Anaesthesia, St. James s Hospital. Closing Date Sunday the 9 th July 2018 SACC Directorate. The Surgery, Anaesthesia and Critical
STAG TRAUMA. Quality Indicators
 STAG TRAUMA Quality Indicators Document Control Document Control Version Quality Indicators V3.3.doc Date Issued 03-09-2013 Author(s) Kirsty Ward Other Related Documents Comments to Angela Khan Document
STAG TRAUMA Quality Indicators Document Control Document Control Version Quality Indicators V3.3.doc Date Issued 03-09-2013 Author(s) Kirsty Ward Other Related Documents Comments to Angela Khan Document
St. James s Hospital, Dublin.
 Position Fellowship in Anaesthesia for Advanced Airway Management Assignment Department of Anaesthesia, St. James s Hospital. Commencement Date Monday, 09 th July, 2018. Purpose of the Post The St. James
Position Fellowship in Anaesthesia for Advanced Airway Management Assignment Department of Anaesthesia, St. James s Hospital. Commencement Date Monday, 09 th July, 2018. Purpose of the Post The St. James
Example Care Pathways
 Example Care Pathways Introduction The following care pathways have been adapted from those developed to sustain provision of general surgery for children in Scotland. We have tried to avoid being too
Example Care Pathways Introduction The following care pathways have been adapted from those developed to sustain provision of general surgery for children in Scotland. We have tried to avoid being too
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to use, share, and adapt it.
 Author(s): Antoinette A. Bradshaw, PhD, MS, BSN, RN, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author(s): Antoinette A. Bradshaw, PhD, MS, BSN, RN, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Patient information. Patients needing Orthopaedic Surgery due to Trauma Trauma and Orthopaedic Directorate PIF 555/V5
 Patient information Patients needing Orthopaedic Surgery due to Trauma Trauma and Orthopaedic Directorate PIF 555/V5 The following information is a general guide to the way the Orthopaedic Emergency Operating
Patient information Patients needing Orthopaedic Surgery due to Trauma Trauma and Orthopaedic Directorate PIF 555/V5 The following information is a general guide to the way the Orthopaedic Emergency Operating
Auckland District Health Board Summary 1 July 2011 to 30 June 2012 Serious and Sentinel Events
 DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
SOP no: A/003. To be revised in Date: February 2009
 PGWC Standard Operating Procedure Category: Operating theatre activity data Recording and reporting of cancellation of elective theatre operations and/or procedures Compiled by: Theatre Efficiencies Task
PGWC Standard Operating Procedure Category: Operating theatre activity data Recording and reporting of cancellation of elective theatre operations and/or procedures Compiled by: Theatre Efficiencies Task
Irish Children s Triage System (ICTS) Project
 Project") Irish Children s Triage System (ICTS) Project Presented by Ruth Devers CNM3 Children's University Hospital Temple St Mary Tumelty CNM3 National Children's Hospital, Tallaght Bridget Conway CNM3 Our Lady's
Irish Children s Triage System (ICTS) Project Presented by Ruth Devers CNM3 Children's University Hospital Temple St Mary Tumelty CNM3 National Children's Hospital, Tallaght Bridget Conway CNM3 Our Lady's
To teach residents the fundamentals of patient triage and prioritization of medical care.
 EMERGENCY MEDICINE Overview Most of the Emergency Medicine Experience occurs predominantly during PGY-1 or PGY-2 Emergency Blocks. In addition, all inpatient rotations provide residents varying degrees
EMERGENCY MEDICINE Overview Most of the Emergency Medicine Experience occurs predominantly during PGY-1 or PGY-2 Emergency Blocks. In addition, all inpatient rotations provide residents varying degrees
Course: Acute Trauma Care Course Number SUR 1905 (1615)
") Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD
 UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD Date of meeting: 25 July 2012 Title / Subject: Vascular Services at UHMBFT; the Impact of Centralising Inpatient and Emergency Vascular
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD Date of meeting: 25 July 2012 Title / Subject: Vascular Services at UHMBFT; the Impact of Centralising Inpatient and Emergency Vascular
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
West Middlesex Junior Doctors Handbook in Colorectal Surgery
 West Middlesex Junior Doctors Handbook in Colorectal Surgery Page 1 of 10 INTRODUCTION Welcome to surgery and to the colorectal team! This guide is meant to be just that, a guide and has been principally
West Middlesex Junior Doctors Handbook in Colorectal Surgery Page 1 of 10 INTRODUCTION Welcome to surgery and to the colorectal team! This guide is meant to be just that, a guide and has been principally
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England HS Foundation Trust Appendix 2 Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy
Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England HS Foundation Trust Appendix 2 Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy
Operating Theatres Data Standards - Phase 1
 For reference only Do Not Use For more information contact: cdsis@nhs.net Operating Theatres Data Standards - Phase 1 November 2006 National Clinical Dataset Development Programme (NCDDP) Support Team
For reference only Do Not Use For more information contact: cdsis@nhs.net Operating Theatres Data Standards - Phase 1 November 2006 National Clinical Dataset Development Programme (NCDDP) Support Team
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
anaesthetic services Chapter 15 Services for neuroanaesthesia and neurocritical care 2014 GUIDELINES FOR THE PROVISION OF ACSA REFERENCES
 Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
Chan Man Yi, NC (Neonatal Care) Dept. of Paed. & A.M., PMH 16 May 2017
 Dept. of Paed. & A.M., PMH 16 May 2017") The implementation of an integrated observation chart with Newborn Early Warning Signs (NEWS) to facilitate observation of infants at risk of clinical deterioration Chan Man Yi, NC (Neonatal Care) Dept.
The implementation of an integrated observation chart with Newborn Early Warning Signs (NEWS) to facilitate observation of infants at risk of clinical deterioration Chan Man Yi, NC (Neonatal Care) Dept.
WELCOME TO THE PEDIATRIC SURGERY SERVICE
 We re happy to welcome you to the Pediatric Surgery team. If you haven t done much pediatrics, sick children can be a bit intimidating but you will quickly discover a few things: it s easy to recognize
We re happy to welcome you to the Pediatric Surgery team. If you haven t done much pediatrics, sick children can be a bit intimidating but you will quickly discover a few things: it s easy to recognize
Alabama Trauma Center Designation Criteria
 2 Alabama Trauma Center Designation Criteria Office of Emergency Medical Services Master Checklist Alabama Trauma Center Designation Trauma Center Criteria: APPENDIX A Trauma Rules The following table
2 Alabama Trauma Center Designation Criteria Office of Emergency Medical Services Master Checklist Alabama Trauma Center Designation Trauma Center Criteria: APPENDIX A Trauma Rules The following table
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
Anaesthesia Fellow. Position Description. Department : Department of Anaesthesia & Perioperative Medicine
 Job Title : Anaesthesia Fellow Department : Department of Anaesthesia & Perioperative Medicine Location : Waitemata District Health Board Reporting To : Clinical Director Anaesthesia Direct Reports : Anaesthesia
Job Title : Anaesthesia Fellow Department : Department of Anaesthesia & Perioperative Medicine Location : Waitemata District Health Board Reporting To : Clinical Director Anaesthesia Direct Reports : Anaesthesia
It s not just Obs and Swabs!
 It s not just Obs and Swabs! Developing a pre-operative assessment service in a complex tertiary referral centre a multidisciplinary approach Emma McCone- Lead Pre op Sister Healthcare at its very best
It s not just Obs and Swabs! Developing a pre-operative assessment service in a complex tertiary referral centre a multidisciplinary approach Emma McCone- Lead Pre op Sister Healthcare at its very best
Lessons learned from VASM cases. Barry Beiles Clinical Director VASM
 Lessons learned from VASM cases Barry Beiles Clinical Director VASM Operative Mortality by specialty (n=5,184) Specialty Frequency (%) General surgery 2,073 (40.0%) Orthopaedic surgery 1,044 (20.1%) Neurosurgery
Lessons learned from VASM cases Barry Beiles Clinical Director VASM Operative Mortality by specialty (n=5,184) Specialty Frequency (%) General surgery 2,073 (40.0%) Orthopaedic surgery 1,044 (20.1%) Neurosurgery
HANDBOOK REGISTRARS, RESIDENTS INTERNS
 BOX HILL HOSPITAL DEPARTMENT OF ANAESTHESIA AND PERIOPERATIVE MEDICINE HANDBOOK FOR REGISTRARS, RESIDENTS AND INTERNS T A B L E O F C O N T E N T S 1. THE DEPARTMENT 2. WHO`S WHO 3. THEATRE SET UP 4. HOURS
BOX HILL HOSPITAL DEPARTMENT OF ANAESTHESIA AND PERIOPERATIVE MEDICINE HANDBOOK FOR REGISTRARS, RESIDENTS AND INTERNS T A B L E O F C O N T E N T S 1. THE DEPARTMENT 2. WHO`S WHO 3. THEATRE SET UP 4. HOURS
1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure
 ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
Peri-operative Pain Management - a multi-disciplinary team-based approach
 Peri-operative Pain Management - a multi-disciplinary team-based approach Dr Steven Wong Chief of Service Department of Anaesthesiology & OT Services Queen Elizabeth Hospital Outline Development of postoperative
Peri-operative Pain Management - a multi-disciplinary team-based approach Dr Steven Wong Chief of Service Department of Anaesthesiology & OT Services Queen Elizabeth Hospital Outline Development of postoperative
Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster.
 Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster. Working document The Critical Care Contingency Plan in the event of an emergency
Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster. Working document The Critical Care Contingency Plan in the event of an emergency
Delivering surgical services: options for maximising resources
 Delivering surgical services: options for maximising resources THE ROYAL COLLEGE OF SURGEONS OF ENGLAND March 2007 2 OPTIONS FOR MAXIMISING RESOURCES The Royal College of Surgeons of England Introduction
Delivering surgical services: options for maximising resources THE ROYAL COLLEGE OF SURGEONS OF ENGLAND March 2007 2 OPTIONS FOR MAXIMISING RESOURCES The Royal College of Surgeons of England Introduction
DMAT Intermediate Triage Lecture Notes Keith Conover, M.D., FACEP 1.0 7/11/14 Objectives: Describe the differences between START triage and ESI
 DMAT Intermediate Triage Lecture Notes Keith Conover, M.D., FACEP 1.0 7/11/14 Objectives: Describe the differences between START triage and ESI triage, both in terms of levels and context in which they
DMAT Intermediate Triage Lecture Notes Keith Conover, M.D., FACEP 1.0 7/11/14 Objectives: Describe the differences between START triage and ESI triage, both in terms of levels and context in which they
Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey
 Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey We want you to nominate the most important topics for future research in anaesthesia and perioperative care. We are therefore asking
Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey We want you to nominate the most important topics for future research in anaesthesia and perioperative care. We are therefore asking
The deteriorating patient recognition and management Dave Story
 The deteriorating patient recognition and management Dave Story MBBS, MD, BMedSci, FANZCA Professor and Foundation Chair of Anaesthesia Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU)
The deteriorating patient recognition and management Dave Story MBBS, MD, BMedSci, FANZCA Professor and Foundation Chair of Anaesthesia Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU)
Pre operative assessment
 Pre operative assessment Dr Anna Lipp Consultant Anaesthetist, Clinical lead day surgery and pre-op assessment Norfolk and Norwich University Hospital President-elect BADS Overview Organisational issues
Pre operative assessment Dr Anna Lipp Consultant Anaesthetist, Clinical lead day surgery and pre-op assessment Norfolk and Norwich University Hospital President-elect BADS Overview Organisational issues
Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition
 Nursing Competency Workbook 6th Edition") Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition The Royal Children's Hospital (RCH) Nursing Competency Workbook is a dynamic document that will
Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition The Royal Children's Hospital (RCH) Nursing Competency Workbook is a dynamic document that will
POLICY TITLE HIGHER LEVEL OF CARE (HLC) AND/OR LIFE, LIMB AND THREATENED ORGAN (LLTO)
 AND/OR LIFE, LIMB AND THREATENED ORGAN (LLTO)") Page 1 of 10 POLICY TITLE 1.0 PURPOSE Patients requiring higher level of care and/or life, limb and threatened organ care will be guaranteed access without exception to an acute care facility that has
Page 1 of 10 POLICY TITLE 1.0 PURPOSE Patients requiring higher level of care and/or life, limb and threatened organ care will be guaranteed access without exception to an acute care facility that has
CCT in Anaesthetics Assessment Guidance 2017
 CCT in Anaesthetics Assessment Guidance 2017 Royal College of Anaesthetists Introduction This document describes the various assessment methods used in the anaesthetic training programme. Trainees are
CCT in Anaesthetics Assessment Guidance 2017 Royal College of Anaesthetists Introduction This document describes the various assessment methods used in the anaesthetic training programme. Trainees are
Inpatient Rehabilitation Program Information
 Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann-Greater Heights has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann-Greater Heights has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
Inpatient Rehabilitation Program Information
 Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann The Woodlands has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
Inpatient Rehabilitation Program Information The Inpatient Rehabilitation Program at TIRR Memorial Hermann The Woodlands has a team of physicians, therapists, nurses, a case manager, neuropsychologist,
Title: ED Management of Trauma Patient Protocol
 Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Trauma Care Network News. West Midlands Major Trauma Clinical Lead appointed. Inside Issue 3. Issue 3
 Trauma Care Network News Issue 3 Inside Issue 3 Implementation of trauma care system Monitoring patient outcomes International Trauma Care Conference 23rd - 26th April West Midlands Major Trauma Clinical
Trauma Care Network News Issue 3 Inside Issue 3 Implementation of trauma care system Monitoring patient outcomes International Trauma Care Conference 23rd - 26th April West Midlands Major Trauma Clinical
Z: Perioperative Nursing Specialty
 Z: Perioperative Nursing Specialty Alberta Licensed Practical Nurses Competency Profile 263 Major Competency Area: Z Perioperative Nursing Specialty Priority: One Competency: Z-1 HPA Authorizations and
Z: Perioperative Nursing Specialty Alberta Licensed Practical Nurses Competency Profile 263 Major Competency Area: Z Perioperative Nursing Specialty Priority: One Competency: Z-1 HPA Authorizations and
Standard Operating Procedure Hospital Pre-alert & Patient Handover
 Standard Operating Procedure Hospital Pre-alert & Patient Handover No of Pages: 6 Unique reference No: Implementation date: 17 th May 2010 Version: Final Version 2.0 Next review date: May 2013 Title of
Standard Operating Procedure Hospital Pre-alert & Patient Handover No of Pages: 6 Unique reference No: Implementation date: 17 th May 2010 Version: Final Version 2.0 Next review date: May 2013 Title of
The Children s Hospital, Oxford. Tonsil Surgery (Tonsillectomy) Information for parents and carers
 Information for parents and carers") The Children s Hospital, Oxford Tonsil Surgery (Tonsillectomy) Information for parents and carers page 2 What is a tonsillectomy? A tonsillectomy is the surgical procedure to remove the tonsils. The tonsils
The Children s Hospital, Oxford Tonsil Surgery (Tonsillectomy) Information for parents and carers page 2 What is a tonsillectomy? A tonsillectomy is the surgical procedure to remove the tonsils. The tonsils
Investigation Outline for a Reportable Incident Non-Hospital Surgical Facility
 Investigation Outline for a Reportable Incident Non-Hospital Surgical Facility MANDATORY NOTIFICATION The Medical Director shall notify the College of Physicians & Surgeons of Alberta (Accreditation Department)
Investigation Outline for a Reportable Incident Non-Hospital Surgical Facility MANDATORY NOTIFICATION The Medical Director shall notify the College of Physicians & Surgeons of Alberta (Accreditation Department)
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Appendix 1 - Licensing and Audit Requirements for Emergency Department Services
 Appendix 1 - Licensing and Audit Requirements for Emergency Department Services Number Urgent Care Centres Emergency Department Emergency Department with Major Trauma Centre 1. Access 24/7 (This requirement
Appendix 1 - Licensing and Audit Requirements for Emergency Department Services Number Urgent Care Centres Emergency Department Emergency Department with Major Trauma Centre 1. Access 24/7 (This requirement
MODULE 4 Obstetric Anaesthesia and Analgesia
 MODULE 4 Obstetric Anaesthesia and Analgesia Duration required: A minimum 50 sessions (½ days) of clinical experience is required TE10 (2003) Recommendations for Vocational Training Programs Trainee s
MODULE 4 Obstetric Anaesthesia and Analgesia Duration required: A minimum 50 sessions (½ days) of clinical experience is required TE10 (2003) Recommendations for Vocational Training Programs Trainee s
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
For Large Groups Health Benefit Single Plan (HSA-Compatible)
") Financial Features (DED 1 ) (PBP 2 ) (DED is the amount the member is responsible for before Florida Blue pays) Out-of-Network Inpatient Hospital Facility Services Per Admission (PAD) Coinsurance (Coinsurance
Financial Features (DED 1 ) (PBP 2 ) (DED is the amount the member is responsible for before Florida Blue pays) Out-of-Network Inpatient Hospital Facility Services Per Admission (PAD) Coinsurance (Coinsurance
Critical Care Curriculum for Two-Month Rotation as Part of an Anesthesiology Residency
 DEPARTMENT OF ANESTHESIA Critical Care Curriculum for Two-Month Rotation as Part of an Anesthesiology Residency 1. An anesthesiology resident, during a two month rotation should gain exposure to the scope
DEPARTMENT OF ANESTHESIA Critical Care Curriculum for Two-Month Rotation as Part of an Anesthesiology Residency 1. An anesthesiology resident, during a two month rotation should gain exposure to the scope
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service SVTN North Bristol NHS Trust North Bristol NHS Trust Reception and Resuscitation Measures (T14-2B-1)
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service SVTN North Bristol NHS Trust North Bristol NHS Trust Reception and Resuscitation Measures (T14-2B-1)
Sample. A guide to development of a hospital blood transfusion Policy at the hospital level. Effective from April Hospital Transfusion Committee
 Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Standard of Care for MTC inpatients
 Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Organisational Audit Questions - Links to recommendations, standards and evidence
 Question Quoted recommendation/ standard / evidence Source Notes Section 1 - Hospital characteristics 1. a) How many adult in-patient or overnight beds (including 23- hours stay) are currently available
Question Quoted recommendation/ standard / evidence Source Notes Section 1 - Hospital characteristics 1. a) How many adult in-patient or overnight beds (including 23- hours stay) are currently available
Does a dedicated orthopaedic day surgery list improve delivery of trauma services?
 KEYWORDS Day surgery / Trauma / Finance / Orthopaedics / Fracture Provenance and Peer review: Unsolicited contribution; Peer reviewed; Accepted for publication January 2017. Does a dedicated orthopaedic
KEYWORDS Day surgery / Trauma / Finance / Orthopaedics / Fracture Provenance and Peer review: Unsolicited contribution; Peer reviewed; Accepted for publication January 2017. Does a dedicated orthopaedic
Admission Record IVF/Gynae
 Admission Record IVF/Gynae Surgeon: Operation : of Admission: Please state your full name and date of birth - correct Nurse Checklist Yes No Please tell me your full address - correct Consent form signed,
Admission Record IVF/Gynae Surgeon: Operation : of Admission: Please state your full name and date of birth - correct Nurse Checklist Yes No Please tell me your full address - correct Consent form signed,
Effective Date: 7/2004
 MEDICAL STAFF POLICY & PROCEDURE Page 1 of 6 Effective Date: 7/2004 Review/Revised: 9/1/2011 Policy No. MSP 003 Purpose: To assure that physicians at all levels are familiar with their roles during the
MEDICAL STAFF POLICY & PROCEDURE Page 1 of 6 Effective Date: 7/2004 Review/Revised: 9/1/2011 Policy No. MSP 003 Purpose: To assure that physicians at all levels are familiar with their roles during the
PLASTIC AND HAND SURGERY CORE OBJECTIVES
 PLASTIC AND HAND SURGERY CORE OBJECTIVES Through rotation on the plastic and hand surgery service, residents shall attain the following goals: I. Patient Care A. Preoperative Care: Residents will evaluate
PLASTIC AND HAND SURGERY CORE OBJECTIVES Through rotation on the plastic and hand surgery service, residents shall attain the following goals: I. Patient Care A. Preoperative Care: Residents will evaluate
TRAUMA AND EMERGENCY SURGERY CORE OBJECTIVES: PGY 4
 TRAUMA AND EMERGENCY SURGERY CORE OBJECTIVES: PGY 4 GOALS Through rotation on the trauma and emergency surgery service, residents shall attain the following goals: I. Patient Care A. Trauma Resuscitations
TRAUMA AND EMERGENCY SURGERY CORE OBJECTIVES: PGY 4 GOALS Through rotation on the trauma and emergency surgery service, residents shall attain the following goals: I. Patient Care A. Trauma Resuscitations
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
Jersey General Hospital, States of Jersey Individual Placement (Job) Descriptions for Foundation Year 2
 Descriptions for Foundation Year 2") Wessex Deanery Jersey General Hospital, States of Jersey Individual Placement (Job) Descriptions for Foundation Year 2 Placement The department The type of work to expect and learning opportunities Where
Wessex Deanery Jersey General Hospital, States of Jersey Individual Placement (Job) Descriptions for Foundation Year 2 Placement The department The type of work to expect and learning opportunities Where
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Implementation of the 10 minute meeting: a user s guide
 Implementation of the 10 minute meeting: a user s guide How a short daily meeting can save lives by helping emergency teams work together more effectively. What s the issue? A critical care outreach team
Implementation of the 10 minute meeting: a user s guide How a short daily meeting can save lives by helping emergency teams work together more effectively. What s the issue? A critical care outreach team
Having a staging laparoscopy
 Information for patients Having a staging laparoscopy Turnberg Building Upper GI General Surgery 0161 206 5062 Page 1 of 5 This booklet has four aims: l To help you and your family become better informed
Information for patients Having a staging laparoscopy Turnberg Building Upper GI General Surgery 0161 206 5062 Page 1 of 5 This booklet has four aims: l To help you and your family become better informed
Sentinel node biopsy. Patient Information to be retained by patient
 PLEASE PRINT WHOLE FORM DOUBLE SIDED ON YELLOW PAPER Patient Information to be retained by patient affix patient label Sentinel Node Biopsy What is a sentinel node biopsy? The lymphatic drainage from your
PLEASE PRINT WHOLE FORM DOUBLE SIDED ON YELLOW PAPER Patient Information to be retained by patient affix patient label Sentinel Node Biopsy What is a sentinel node biopsy? The lymphatic drainage from your
NCEPOD Recommendations that remain current
 NCEPOD Recommendations that remain current All recommendations from subsequent NCEPOD reports are considered current (Last updated 2014) 1989 The information systems, particularly clinical information
NCEPOD Recommendations that remain current All recommendations from subsequent NCEPOD reports are considered current (Last updated 2014) 1989 The information systems, particularly clinical information
GENERAL PRACTICE RESIDENCY TRAINING PROGRAM IN DENTISTRY
 GENERAL PRACTICE RESIDENCY TRAINING PROGRAM IN DENTISTRY The University of British Columbia, in conjunction with Vancouver General Hospital (VGH), a tertiary care facility and trauma center, offers positions
GENERAL PRACTICE RESIDENCY TRAINING PROGRAM IN DENTISTRY The University of British Columbia, in conjunction with Vancouver General Hospital (VGH), a tertiary care facility and trauma center, offers positions
APPENDIX I QUESTIONNAIRE FOR INTERVIEWING THE ANAESTHESIA PROVIDER
 APPENDIX I QUESTIONNAIRE FOR INTERVIEWING THE ANAESTHESIA PROVIDER We are carrying out a survey to establish the quality of anaesthesia care provided to Obstetric patients in East Africa. We therefore
APPENDIX I QUESTIONNAIRE FOR INTERVIEWING THE ANAESTHESIA PROVIDER We are carrying out a survey to establish the quality of anaesthesia care provided to Obstetric patients in East Africa. We therefore
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart
 Observation Chart") CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
Separating emergency and elective surgical care: Recommendations for practice
 Separating emergency and elective surgical care: Recommendations for practice THE ROYAL COLLEGE OF SURGEONS OF ENGLAND September 2007 2 SEPARATING EMERGENCY AND ELECTIVE SURGICAL CARE The Royal College
Separating emergency and elective surgical care: Recommendations for practice THE ROYAL COLLEGE OF SURGEONS OF ENGLAND September 2007 2 SEPARATING EMERGENCY AND ELECTIVE SURGICAL CARE The Royal College
Central Adelaide Local Health Network Clinical Directorate Structures
 Central Adelaide Local Health Network Clinical Directorate Structures Consultation Paper February 2014 Version 2 Document Information and Revision History 1. Version 2. Date 3. Comment 1.0 12 February
Central Adelaide Local Health Network Clinical Directorate Structures Consultation Paper February 2014 Version 2 Document Information and Revision History 1. Version 2. Date 3. Comment 1.0 12 February
Anaesthesia Fellow. Position Description CONTENTS OF DOCUMENT
 CONTENTS OF DOCUMENT INTRODUCTION & SUMMARY 2 KEY TASKS & EXPECTED OUTCOMES 3 BEHAVIOURAL COMPETENCIES 6 PERSON SPECIFICATION 7 DETAILED WORK PLAN 8 SPECIFIC FELLOWSHIPS Medical Education in Anaesthesia
CONTENTS OF DOCUMENT INTRODUCTION & SUMMARY 2 KEY TASKS & EXPECTED OUTCOMES 3 BEHAVIOURAL COMPETENCIES 6 PERSON SPECIFICATION 7 DETAILED WORK PLAN 8 SPECIFIC FELLOWSHIPS Medical Education in Anaesthesia
Insertion of a ventriculo-peritoneal or ventriculo-atrial shunt
 Department of Neurosurgery Insertion of a ventriculo-peritoneal or ventriculo-atrial shunt Information for patients Shunt surgery This leaflet explains what to expect when you are in hospital and during
Department of Neurosurgery Insertion of a ventriculo-peritoneal or ventriculo-atrial shunt Information for patients Shunt surgery This leaflet explains what to expect when you are in hospital and during
Acutely ill patients in hospital
 Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital Developed by the Centre for Clinical Practice at NICE Contents Key priorities for
Issue date: July 2007 Acutely ill patients in hospital Recognition of and response to acute illness in adults in hospital Developed by the Centre for Clinical Practice at NICE Contents Key priorities for
A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs.
 6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
Introduction to the Family Medicine-Emergency Medicine Rotation at the Hand & Upper Limb Centre. St Joseph s Health Centre London, Ontario
 Introduction to the Family Medicine-Emergency Medicine Rotation at the Hand & Upper Limb Centre St Joseph s Health Centre London, Ontario 2 Background: Residents who are enrolled in the Family Medicine
Introduction to the Family Medicine-Emergency Medicine Rotation at the Hand & Upper Limb Centre St Joseph s Health Centre London, Ontario 2 Background: Residents who are enrolled in the Family Medicine
Operating Theatre Performance (Scheduled Sessions) Policy
 Policy") Policy No: OP38 Version: 4.0 Name of Policy: Operating Theatre Performance (Scheduled Sessions) Policy Effective From: 24/08/2015 Date Ratified 22/07/2015 Ratified Theatre User Group Review Date 01/07/2017
Policy No: OP38 Version: 4.0 Name of Policy: Operating Theatre Performance (Scheduled Sessions) Policy Effective From: 24/08/2015 Date Ratified 22/07/2015 Ratified Theatre User Group Review Date 01/07/2017
STATEMENT OF PURPOSE: Emergency Department staff care for observation patients in two main settings: the ED observation unit (EDOU) and ED tower obser
 and ED tower obser") DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
4/10/2013. Learning Objective. Quality-Based Payment Models
 Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
Guidelines on Postanaesthetic Recovery Care
 Page 1 of 10 Guidelines on Postanaesthetic Recovery Care Version Effective Date 1 OCT 1992 2 FEB 2002 3 APR 2012 4 JUN 2017 Document No. HKCA P3 v4 Prepared by College Guidelines Committee Endorsed by
Page 1 of 10 Guidelines on Postanaesthetic Recovery Care Version Effective Date 1 OCT 1992 2 FEB 2002 3 APR 2012 4 JUN 2017 Document No. HKCA P3 v4 Prepared by College Guidelines Committee Endorsed by
The Higher Risk General Surgical Patient
 The Higher Risk General Surgical Patient Towards Improved Care for a Forgotten Group The Royal College of Surgeons of England and Department of Health Report on the Peri-operative Care of the Higher Risk
The Higher Risk General Surgical Patient Towards Improved Care for a Forgotten Group The Royal College of Surgeons of England and Department of Health Report on the Peri-operative Care of the Higher Risk
HENDRICKS REGIONAL HEALTH EMERGENCY MEDICINE RULES AND REGULATIONS
 I. Scope of Service HENDRICKS REGIONAL HEALTH EMERGENCY MEDICINE RULES AND REGULATIONS The Emergency Department offers emergency care twenty-four hours a day with at least one physician experienced in
I. Scope of Service HENDRICKS REGIONAL HEALTH EMERGENCY MEDICINE RULES AND REGULATIONS The Emergency Department offers emergency care twenty-four hours a day with at least one physician experienced in
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
National Early Warning Score (ViEWS) System. Recommendations for Audit. February 2012
 System. Recommendations for Audit. February 2012") National Early Warning Score (ViEWS) System Recommendations for Audit February 2012 Version 3 Acknowledgement: The National Early Warning Score and associated Education Programme Audit and Evaluation sub-group
National Early Warning Score (ViEWS) System Recommendations for Audit February 2012 Version 3 Acknowledgement: The National Early Warning Score and associated Education Programme Audit and Evaluation sub-group
HOW TO DO POST-HOC RESPONSE REVIEWS
 HOW TO DO POST-HOC RESPONSE REVIEWS Ken Hillman 6 th International Symposium on Rapid Response Systems and Medical Emergency Teams Pittsburgh, USA, 11 th -12 th May 2010 ACUTE HOSPITAL SYSTEM AUDIT OF
HOW TO DO POST-HOC RESPONSE REVIEWS Ken Hillman 6 th International Symposium on Rapid Response Systems and Medical Emergency Teams Pittsburgh, USA, 11 th -12 th May 2010 ACUTE HOSPITAL SYSTEM AUDIT OF
Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty
 Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty R. Michael Meneghini MD Associate Professor of Orthopaedic Surgery Indiana University School of Medicine Indianapolis,
Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty R. Michael Meneghini MD Associate Professor of Orthopaedic Surgery Indiana University School of Medicine Indianapolis,
How do we know the surgical checklist is making a meaningful. impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010
 How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
National Theatres Project Report
 National Theatres Project Report November 2006 Technical Appendix National Theatres Project Report November 2006 Technical Appendix Scottish Executive, Edinburgh 2007 ii National Theatres Project Crown
National Theatres Project Report November 2006 Technical Appendix National Theatres Project Report November 2006 Technical Appendix Scottish Executive, Edinburgh 2007 ii National Theatres Project Crown
UNIVERSITY OF NORTH DAKOTA COLLEGE OF NURSING AND PROFESSIONAL DISCIPLINES
 UNIVERSITYOFNORTHDAKOTA COLLEGEOFNURSINGANDPROFESSIONAL DISCIPLINES MASTEROFSCIENCE IN NURSEANESTHESIA CLINICALPRECEPTORHANDBOOK 2013 2014 Version 1.4 8/20/2013 Version 1.4 8/20/2013 PAGEINTENTIONALLYLEFTBLANK
UNIVERSITYOFNORTHDAKOTA COLLEGEOFNURSINGANDPROFESSIONAL DISCIPLINES MASTEROFSCIENCE IN NURSEANESTHESIA CLINICALPRECEPTORHANDBOOK 2013 2014 Version 1.4 8/20/2013 Version 1.4 8/20/2013 PAGEINTENTIONALLYLEFTBLANK
NORTHERN BEACHES INTENSIVE CARE SERVICE Mona Vale Campus Updated January 2009
 NORTHERN BEACHES INTENSIVE CARE SERVICE Mona Vale Campus Updated January 2009 Welcome to Intensive Care at Mona Vale Hospital. Please read the accompanying orientation document prepared for Medical Students
NORTHERN BEACHES INTENSIVE CARE SERVICE Mona Vale Campus Updated January 2009 Welcome to Intensive Care at Mona Vale Hospital. Please read the accompanying orientation document prepared for Medical Students
REPORT 1 PLANNED CARE
 REPORT 1 PLANNED CARE Contents Planned care vision c-3 Definition - Planned Care c-3 Current planned care services c-4 What patients say about current planned care services c-7 Vision c-8 Principles c-9
REPORT 1 PLANNED CARE Contents Planned care vision c-3 Definition - Planned Care c-3 Current planned care services c-4 What patients say about current planned care services c-7 Vision c-8 Principles c-9
Emergency Surgery. Standards for unscheduled surgical care. Guidance for providers, commissioners and service planners
 Emergency Surgery Standards for unscheduled surgical care Guidance for providers, commissioners and service planners February 2011 Produced by the Publications Department, The Royal College of Surgeons
Emergency Surgery Standards for unscheduled surgical care Guidance for providers, commissioners and service planners February 2011 Produced by the Publications Department, The Royal College of Surgeons
Please find below our questionnaire completed with the information we hold.
 September 2011 Please find attached a FOI request requesting information on the Trust s compliance of VTE prevention policies with national VTE best practice and policy. I would be grateful if the most
September 2011 Please find attached a FOI request requesting information on the Trust s compliance of VTE prevention policies with national VTE best practice and policy. I would be grateful if the most
Equivalence Guidance for GMP Domain 1
 Equivalence Guidance for GMP Domain 1 From 1 st August 2011 the new GMC approved curriculum in Intensive Care Medicine (ICM) came into effect. As a result of this new curriculum, all equivalence applications
Equivalence Guidance for GMP Domain 1 From 1 st August 2011 the new GMC approved curriculum in Intensive Care Medicine (ICM) came into effect. As a result of this new curriculum, all equivalence applications