Context Matters: Neighborhood Socioeconomic Disadvantage and Health in Transitions
|
|
|
- Allyson Dennis
- 6 years ago
- Views:
Transcription
1 Context Matters: Neighborhood Socioeconomic Disadvantage and Health in Transitions Amy JH Kind, MD, PhD Associate Director-Clinical Madison VA Geriatrics Research Education and Clinical Center (GRECC) & Associate Professor, Division of Geriatrics University of Wisconsin School of Medicine and Public Health Financial Disclosures Amy JH Kind, MD, PhD: Funding: NIH/National Institutes on Aging NIH/National Institutes on Minority Health and Health Disparities US Department of Veterans Affairs US Centers for Medicare and Medicaid Services Multiple non-profit foundations Consultant, State of Maryland 1
2 Case: One of Many 78yo hospitalized with pneumonia Mild dementia, not recognized Discharged on oral antibiotic x 7 days Discharge teaching performed once (intensively) on the day of discharge. Caregiver not notified. (Daughter working 2 jobs to make ends meet.) Home health won t visit due to neighborhood safety concerns. Rehospitalized 3 days later; recurrent pneumonia Antibiotic prescription found in patient s pocket. He forgot to fill the medication. Overview The influence of socioeconomic contextual disadvantage on health outcomes and rehospitalization Tools for improving care transitions in vulnerable populations Harnessing protocolized adaptation to achieve local program sustainability, especially in lowresource settings 2

3 Overview The influence of socioeconomic contextual disadvantage on health outcomes and rehospitalization Tools for improving care transitions in vulnerable populations Harnessing protocolized adaptation to achieve local program sustainability, especially in lowresource settings Socioeconomic Disadvantage The state of being challenged by low income, limited education, and substandard living conditions for both the person and his or her social network* *Shavers, J Natl Med Assoc, 2007; Cederberg et al, EPASI, 2009 ( 3

4 Neighborhood Socioeconomic Disadvantage Impacts Health Associated with behaviors*, access to food**, safety Linked to outcomes like mortality, development of diabetes***, birth weight Health indicators improve with moving persons to areas of less concentrated poverty *Lantz et al, JAMA, 1998; **Franco et al, Am J Prev Med, 2008; Hsieh and Pugh, Criminal Justice Review, 1993; ***Christine et al, JAMA Int Med, 2015; Joynt and Jha, JAMA, 2013; Blumenshine, et al, Am J Prev Med, 2010; Ludwig et al, NEJM, 2011; Milbank Q, 1990; Krumholz, NEJM,
 neighborhood (N=4,604 families) Five cities: Baltimore, Boston, Chicago, Los Angeles, New York Data collected for 10-15 years post-randomization * Ludwig et al,")
5 Moving to Opportunity Study Sponsored by the US Dept of Housing and Urban Development (HUD) Random lottery ( ) offered some public housing families, but not others, the chance to move into a less distressed (lower-poverty) neighborhood (N=4,604 families) Five cities: Baltimore, Boston, Chicago, Los Angeles, New York Data collected for years post-randomization * Ludwig et al, Science, 2012 Included measures on racial segregation of neighborhoods Results Moving from a high-poverty to lower-poverty neighborhood leads to long-term improvements in adult physical and mental health and subjective wellbeing, despite not affecting economic self-sufficiency. * Ludwig et al, Science,
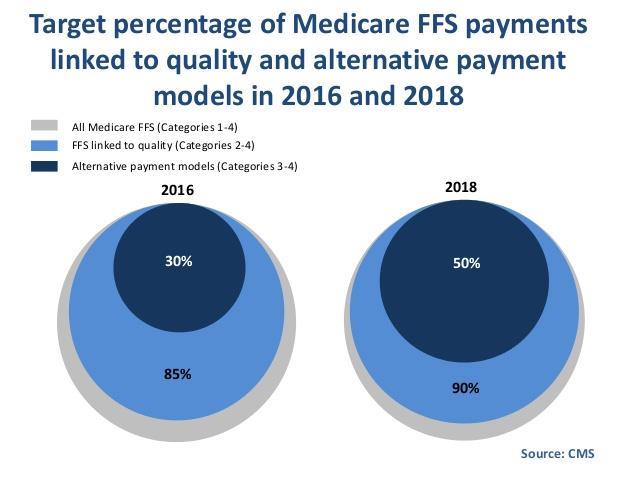
6 Case: One of Many Does Context Impact 78yo hospitalized with pneumonia Mild dementia, not recognized Discharged on oral antibiotic x 7 days Discharge teaching performed once (intensively) on the day of discharge. Caregiver not notified. (Daughter working 2 jobs to make ends meet.) Home health won t Rehospitalization visit due to neighborhood safety concerns. Risk? Rehospitalized 3 days later; recurrent pneumonia Antibiotic prescription found in patient s pocket. He forgot to fill the medication. 30-Day Rehospitalizations Affect 1 in 5 hospitalized Medicare patients* Cost more than $30 billion annually Target of hospital-based Medicare payment penalties Rehospitalization measures to which these penalties are linked adjust for patient comorbidities, but do not account for socioeconomic factors *Patient Protection and Affordable Care Act, Pub. L. No Stat 119 (2010) 6


7 Rehospitalization Penalties Disproportionately Impact Hospitals Serving the Disadvantaged Safety-net hospitals have borne a disproportionate share of rehospitalization penalties since their initiation in 2012 >2 times the risk of being penalized *Joynt and Jha, JAMA, Jan 2013 Context (Credit: AP/Robert F. Bukaty) 7



8 Context cnbc.com 8
9 US Senate Finding bipartisan approaches to improve the US health care system has been a challenge, but considering socioeconomic status in readmission rates is one area of remarkable consensus. (JAMA, July 2015) Andrew Boozary, MD, MPP, Harvard Joseph Manchin III, US Senate, D-West Virginia Roger Wicker, JD, US Senate, R-Mississippi Harnessing the Area Deprivation Index (ADI) A validated census-based measure Factor-based index, 17 US Census-based indicators Correlated with multiple county-level health outcomes Cardiovascular mortality Cancer mortality Cervical cancer prevalence Re-constructed and validated at the Census block-group (i.e., neighborhood ) level *Singh, Am J Public Health, 2003; Singh and Siahpush, Int J Epidemiol, 2006; Kind et al, Annals of Internal Medicine,

10 ADI Components Education Income Poverty Housing Cost Housing Quality Employment Single-parent Households *Singh, Am J Public Health, 2003; Singh and Siahpush, Int J Epidemiol, 2006; Kind Neighborhood Socioeconomic Disadvantage Increases Rehospitalization Risk *Kind et al, Annals of Internal Medicine, Dec

11 Risk for Rehospitalization *Kind et al, Annals, Dec 2014 Powerful Predictor Living in a severely disadvantaged neighborhood predicts rehospitalization as powerfully as the presence of illnesses, such as chronic pulmonary disease Stronger predictor than diabetes or Medicaid Association remains regardless of hospital *Kind et al, Annals, Dec

12 Locations of the 15% Most Disadvantaged US Neighborhoods Based on 2000 ADI *Kind et al, Annals, Dec 2014 Free On-Line 2000 ADI Look-up tool: Data set: 12

13 Brisk Use of On-Line Tool Individual look-up tool accessed >3000 times since publication in December 2014 Full dataset downloaded >400 times by state/federal agencies, several notable health systems and universities State Departments of Health Massachusetts General Hospital, Brigham and Women s, Johns Hopkins and others Blue Shield of California R01 NIH - National Institute on Minority Health and Health Disparities* Update the ADI, and assess geographic stability and association consistency Investigate hospital versus neighborhood effects Identify and study resiliency at the hospital level *1R01MD (PI: Kind) 13

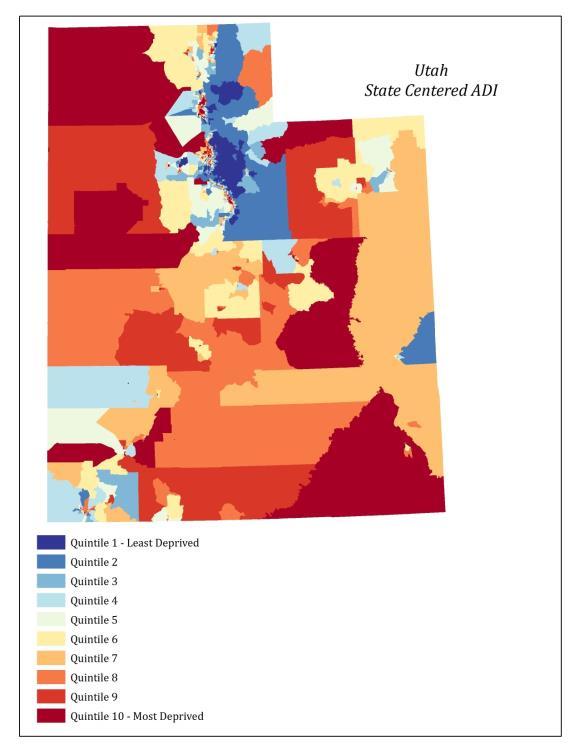
14 2013 ADI 14
15 2013 Colorado Next Steps Socioeconomic contextual disadvantage and Program targeting Policy Research to clarify health impact 15

16 Overview The influence of socioeconomic contextual disadvantage on health outcomes and rehospitalization Tools for improving care transitions in vulnerable populations Harnessing protocolized adaptation to achieve local program sustainability, especially in lowresource settings Case: One of Many 78yo hospitalized with pneumonia Mild How dementia, not recognized Can Discharged on oral antibiotic x 7 days Discharge teaching performed once (intensively) on the day of discharge. Caregiver not notified. (Daughter working We 2 jobs to make Help? ends meet.) Home health won t visit due to neighborhood safety concerns. Rehospitalized 3 days later; recurrent pneumonia Antibiotic prescription found in patient s pocket. He forgot to fill the medication. 16

17 US Health System: 50 Years Ago Hospital Primary Care US Health System: Today Hospital Primary Care Assisted Living Facilities Nursing Home Long- Term Hospitals Inpatient Rehabilitation 17

18 Post-Hospital Transitions are Difficult for Patients Patients are often not prepared for next setting Little patient empowerment in hospital Lack of reinforced patient education * Coleman. JAGS. 2003;51: Transitional Care Broadly, a set of actions designed to ensure the coordination and continuity of health care as patients transfer between different locations or different levels of care in the same location* * Coleman. JAGS
19 Common Misperceptions Discharge practice = transitional care Discharge is only one piece of a high-quality transition Any post-discharge phone call or contact = transitional care Not all phone calls/contacts are created equal Transitional care is not necessary if I use teach back Many patients will not fully understand their care plan without reinforced messaging over time Components of Effective Transitional Care Multi-component, multi-disciplinary, team-based care Clear integration with both inpatient and outpatient sites of care Reinforced messages over time Patient-centered Post-hospital support needs vary; transitional care must be tailored to these needs 19
20 Concept for Comprehensive Post-Hospital Transitional Care Hospitalized Population Home- Visit Based Transitional Care Program Coordinated- Transitional Care Program (C-TraC) Hospital-Based C-TraC Nurses Outpatient Integration Highest-Risk Veterans *Veteran must be geographically close & agreeable to a home-visit *Could be identified by C-TraC nurses in addition to pre-defined patient characteristics All Higher-Risk Veterans *Examples: cognitively impaired or lives-alone or prior hospitalization or medically complex *Could be identified via existing C-TraC protocols in addition to referrals from veteran s care team Strong Discharge Practices Medication Reconciliation Discharge Teaching/Materials Medical Follow-Up Plans Quality Discharge Documentation All Hospitalized Patients * Programs are additive. They are not mutually-exclusive. Unpublished figure, Amy JH Kind, MD, PhD Concept for Comprehensive Post-Hospital Transitional Care Hospitalized Population Home- Visit Based Transitional Care Program Coordinated- Transitional Care Program (C-TraC) Hospital-Based C-TraC Nurses Outpatient Integration Highest-Risk Patients *Patient must be geographically close & agreeable to a home-visit *Could be identified by C-TraC nurses in addition to pre-defined patient characteristics All Higher-Risk Veterans *Examples: cognitively impaired or lives-alone or prior hospitalization or medically complex *Could be identified via existing C-TraC protocols in addition to referrals from veteran s care team Strong Discharge Practices Medication Reconciliation Discharge Teaching/Materials Medical Follow-Up Plans Quality Discharge Documentation All Hospitalized Patients * Programs are additive. They are not mutually-exclusive. Unpublished figure, Amy JH Kind, MD, PhD 20

21 Concept for Comprehensive Post-Hospital Transitional Care Hospitalized Population Home- Visit Based Transitional Care Program Coordinated- Transitional Care Program (C-TraC) Hospital-Based C-TraC Nurses Outpatient Integration Highest-Risk Patients *Patient must be geographically close & agreeable to a home-visit *Could be identified by C-TraC nurses in addition to pre-defined patient characteristics All Higher-Risk Veterans *Examples: cognitively impaired or lives-alone or prior hospitalization or medically complex *Could be identified via existing C-TraC protocols in addition to referrals from veteran s care team Strong Discharge Practices Medication Reconciliation Discharge Teaching/Materials Medical Follow-Up Plans Quality Discharge Documentation All Hospitalized Patients * Programs are additive. They are not mutually-exclusive. Unpublished figure, Amy JH Kind, MD, PhD 21
22 Unmet Need Many of the patients who need transitional care cannot access such services Socioeconomically disadvantaged populations Areas with poor health care access Need transitional care programs that adapt, succeed and sustain in underserved and disadvantaged areas Concept for Comprehensive Post-Hospital Transitional Care Hospitalized Population Home- Visit Based Transitional Care Program Coordinated- Transitional Care Program (C-TraC) Hospital-Based C-TraC Nurses Outpatient Integration Highest-Risk Patients *Patient must be geographically close & agreeable to a home-visit *Could be identified by C-TraC nurses in addition to pre-defined patient characteristics All Higher-Risk Patients *Examples: cognitively impaired or lives-alone or prior hospitalization or medically complex Strong Discharge Practices Medication Reconciliation Discharge Teaching/Materials Medical Follow-Up Plans Quality Discharge Documentation All Hospitalized Patients * Programs are additive. They are not mutually-exclusive. Unpublished figure, Amy JH Kind, MD, PhD 22
23 VA Coordinated-Transitional Care Program (C-TraC) Phone-based program Specially-trained RN nurse case manager Protocolized encounters Teachings based on theory of Spaced Retrieval* Method of learning information by practicing recalling that information over increasingly longer periods of time Applicable in early stages of dementia Caregivers involved, activated at each step * Bourgeois, et al, J Comm Disord, 2003; Camp et al, Appl Cog Psych, C-TraC Goals 1. Educate and empower the patient/caregiver in medication management 2. Ensure the patient/caregiver has medical follow-up 3. Educate the patient/caregiver regarding red flags 4. Ensure the patient/caregiver knows whom to contact if questions arise * Kind, Health Affairs,

24 Eligibility Hospitalized on non-psychiatric acute-care ward Discharged to community AND one or more of the following: 1. Have documentation of dementia, delirium or cognitive impairment years or older AND lives alone OR had a previous hospitalization in past 12 months * Kind, Health Affairs, Coordinated-Transitional Care (C-TraC) Program * Kind at al, JAGS,


25 C-TraC: In-Hospital Visit C-TraC: Telephone Follow-up Initial call is hours after discharge with caregiver/veteran to reinforce Medication management Medical follow-up 3 Red flags C-TraC Nurse case manager contact information Average 36 min per call Patient led medication reconciliation 1 in 3 have medication discrepancies Active coordination with outpatient providers 25
 0.")
26 C-TraC Cut Rehospitalizations 30-day rehospitalizations cut by 1/3 when compared to baseline group C-TraC Group (N = 500) Establishment period (Months 1-6), n = 103 Intervention period (Months 7-18), n= Day Rehospitalization Adjusted** 95% CI P-Value Odds Ratio 1.00 Ref 0.56 (0.33, 0.94) **Multivariate logistic regression model adjusted for veteran age, gender, race, Medicaid status, education level, VA service connected status; w hether veteran lives alone; presence of dementia/other cognitive impairment/delirium; charlson comorbidity score; needing more help w ith bathing, dressing, transferring and toileting in 2 w eeks prior to hospitalization; decline in ability to stand or w alk in 2 w eeks prior to hospitalization; and w hether veteran manages ow n medications * Kind, Health Affairs, The Coordinated-Transitional Care (C-TraC) Program Net cost avoidance of over $1,200 per Veteran served Veterans and caregivers reported high satisfaction with intervention, decreased caregiver stress; Providers loved the program C-TraC successfully sustained (and expanded) at multiple VA and non-va launch sites 26
 and grassroots program growth www.hipxchange.")
27 C-TraC Continues to Disseminate Mentored C-TraC launches at a range of VA and private hospitals throughout US Boston VA Hospital newest C-TraC site Mentored implementations, free on-line toolkit (>500 downloads) and grassroots program growth 5-year NIH-funded RCT to evaluate C-TraC s impact in a non-va dementia-specific population (results in 2020) Initial Dissemination Results * Kind et al, JAGS,
28 Overview The influence of socioeconomic contextual disadvantage on health outcomes and rehospitalization Tools for improving care transitions in vulnerable populations Harnessing protocolized adaptation to achieve local program sustainability, especially in lowresource settings Goal: Engineer Sustainable Programs for the Most Socioeconomically Disadvantaged Areas *Kind et al, Annals, Dec

29 Specific Steps Medicare-funded 2-year C-TraC Pilot Dissemination to Rural Colorado Implementation science to engineer a platform for sustainment at the microsystem level Replicate, adapt, succeed & sustain Protocolized adaptation in dissemination Completion: 2017 * Kind et al, JAGS 2016 Implementation Mentoring* for C-TraC months for full process Pre-Conditions Identification of need Review existing interventions Pre- Implementation Core elements Customize delivery Logistics/training Implementation Process evaluation Feedback/protocol refinement Maintenance and Evolution Sustain Disseminate 1. Document existing local discharge processes 2. Provide a comprehensive overview of C-TraC 1. Convene local multidisciplinary keystakeholder group 2. Coach local keystakeholders to define local high-impact outcomes, goals 3. Detailed discussion of core C-TraC elements, processes 4. Formally adapt C-TraC operations to accommodate local VA system 5. Ensure integration with (not duplication of) existing processes 6. Train newly hired C-TraC local staff in clinical program delivery, and provide on-going coaching of program leadership in program assessment, reporting and administrative barrier reduction 1. Coach local C-TraC staff to ensure they achieve widespread local stakeholder engagement prior to launch 2. Coach local C TraC leadership through iterative phased protocol refinement post-launch 3. Mentor local teams to perform continuous process monitoring, documentation 4. Mentor local C-TraC teams to perform key outcome monitoring and reporting to ensure strongest chances of post-grant sustainability 1. Mentor local C-TraC teams in final results feedback to health system leadership and stakeholders 2. Achieve local C-TraC program sustainment * Adapted from CDC s Replicating Effective Programs Implementation Theory Model * Kind et al, JAGS,

30 2013 Colorado Conclusions Context matters: It impacts patient health as well as care delivery Context must be carefully considered in the engineering of solutions to eliminate health disparities New tools and approaches are available More work in this area is needed 30
31 Acknowledgements Dissemination Team/Collaborators Alan Bridges Becky Kordahl Sanjay Asthana Laury Jensen Ken Shay Karen Massey VISN 12 Leadership Madison VA Hospital Leadership VACO Leadership UWHC Leadership Beth Houlahan Maria Brenny-Fitzpatrick UWHC C-TraC Team Madison VA C-TraC Team Andrea Gilmore-Bykovskyi Korey Kennelty Jane Brock Steve Jencks Funding NIA 2P50AG (Asthana PI; Kind Project 3 PI) NIMHD R01MD (Kind PI) NIA Beeson Career Development Award (1K23AG034551) Madison VA GRECC VA T-21 GEC: Innovative Patient Centered Alternatives to Institutional Care VA Office of Rural Health Wisconsin Partnership Program New Investigator Award Centers for Medicare and Medicaid Services Thank you! C-TraC patients and families 31
The Coordinated-Transitional Care (C-TraC) Program
 Program") The Coordinated-Transitional Care (C-TraC) Program Amy JH Kind, MD, PhD Associate Director-Clinical Madison VA Geriatrics Research Education and Clinical Center (GRECC) & Associate Professor, Division
The Coordinated-Transitional Care (C-TraC) Program Amy JH Kind, MD, PhD Associate Director-Clinical Madison VA Geriatrics Research Education and Clinical Center (GRECC) & Associate Professor, Division
Neighborhoods, resources and capacity to improve
 Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Care Coordination What Matters
 Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
FUNCTIONAL DISABILITY AND INFORMAL CARE FOR OLDER ADULTS IN MEXICO
 FUNCTIONAL DISABILITY AND INFORMAL CARE FOR OLDER ADULTS IN MEXICO Mariana López-Ortega National Institute of Geriatrics, Mexico Flavia C. D. Andrade Dept. of Kinesiology and Community Health, University
FUNCTIONAL DISABILITY AND INFORMAL CARE FOR OLDER ADULTS IN MEXICO Mariana López-Ortega National Institute of Geriatrics, Mexico Flavia C. D. Andrade Dept. of Kinesiology and Community Health, University
EFFECTIVE CARE FOR HIGH-NEED PATIENTS
 1 EFFECTIVE CARE FOR HIGH-NEED PATIENTS Opportunities for Improving Outcomes, Value, and Health Danielle Whicher PhD, MHS National Academy of Medicine November 11, 2017 2 Formerly the Institute of Medicine,
1 EFFECTIVE CARE FOR HIGH-NEED PATIENTS Opportunities for Improving Outcomes, Value, and Health Danielle Whicher PhD, MHS National Academy of Medicine November 11, 2017 2 Formerly the Institute of Medicine,
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Caregiving: Health Effects, Treatments, and Future Directions
 Caregiving: Health Effects, Treatments, and Future Directions Richard Schulz, PhD Distinguished Service Professor of Psychiatry and Director, University Center for Social and Urban Research University
Caregiving: Health Effects, Treatments, and Future Directions Richard Schulz, PhD Distinguished Service Professor of Psychiatry and Director, University Center for Social and Urban Research University
Reducing healthcare disparities in materially deprived patients
 Reducing healthcare disparities in materially deprived patients Integrated Care Management Conference September 21-22, 2016 Presenter: Andrew J Knighton PhD CPA Intermountain Institute for Healthcare Delivery
Reducing healthcare disparities in materially deprived patients Integrated Care Management Conference September 21-22, 2016 Presenter: Andrew J Knighton PhD CPA Intermountain Institute for Healthcare Delivery
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Understanding Readmissions after Cancer Surgery in Vulnerable Hospitals
 Understanding Readmissions after Cancer Surgery in Vulnerable Hospitals Waddah B. Al-Refaie, MD, FACS John S. Dillon and Chief of Surgical Oncology MedStar Georgetown University Hospital Lombardi Comprehensive
Understanding Readmissions after Cancer Surgery in Vulnerable Hospitals Waddah B. Al-Refaie, MD, FACS John S. Dillon and Chief of Surgical Oncology MedStar Georgetown University Hospital Lombardi Comprehensive
Aging in Place: Do Older Americans Act Title III Services Reach Those Most Likely to Enter Nursing Homes? Nursing Home Predictors
 T I M E L Y I N F O R M A T I O N F R O M M A T H E M A T I C A Improving public well-being by conducting high quality, objective research and surveys JULY 2010 Number 1 Helping Vulnerable Seniors Thrive
T I M E L Y I N F O R M A T I O N F R O M M A T H E M A T I C A Improving public well-being by conducting high quality, objective research and surveys JULY 2010 Number 1 Helping Vulnerable Seniors Thrive
By Julie Berez Mentor: Matthew McHugh PhD JD, MPH, RN, CRNP
 Can Nurse Staffing Levels Improve Hospital Readmissions Performance? By Julie Berez Mentor: Matthew McHugh PhD JD, MPH, RN, CRNP Presentation Outline Overview of Readmissions Reduction Program Study Significance
Can Nurse Staffing Levels Improve Hospital Readmissions Performance? By Julie Berez Mentor: Matthew McHugh PhD JD, MPH, RN, CRNP Presentation Outline Overview of Readmissions Reduction Program Study Significance
Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes. James X. Zhang, PhD, MS The University of Chicago
 Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes James X. Zhang, PhD, MS The University of Chicago April 23, 2013 Outline Background Medicare Dual eligibles Diabetes mellitus Quality
Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes James X. Zhang, PhD, MS The University of Chicago April 23, 2013 Outline Background Medicare Dual eligibles Diabetes mellitus Quality
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
VJ Periyakoil Productions presents
 VJ Periyakoil Productions presents Oscar thecare Cat: Advance Lessons Learned Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil,
VJ Periyakoil Productions presents Oscar thecare Cat: Advance Lessons Learned Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil,
Version 1.0 (posted Aug ) Aaron L. Leppin. Background. Introduction
 Aaron L. Leppin. Background. Introduction") Describing the usefulness and efficacy of discharge interventions: predicting 30 day readmissions through application of the cumulative complexity model (protocol). Version 1.0 (posted Aug 22 2013) Aaron
Describing the usefulness and efficacy of discharge interventions: predicting 30 day readmissions through application of the cumulative complexity model (protocol). Version 1.0 (posted Aug 22 2013) Aaron
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
The Medical Home Model: What Is It And How Do Social Workers Fit In?
 I S S U E 10 A P R I L 2 0 1 1 PracticePerspectives The National Association of Social Workers 750 First Street NE Suite 700 Stacy Collins, MSW Senior Practice Associate scollins@naswdc.org Washington,
I S S U E 10 A P R I L 2 0 1 1 PracticePerspectives The National Association of Social Workers 750 First Street NE Suite 700 Stacy Collins, MSW Senior Practice Associate scollins@naswdc.org Washington,
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
HOW WILL MINORITY-SERVING HOSPITALS FARE UNDER THE ACA?
 HOW WILL MINORITY-SERVING HOSPITALS FARE UNDER THE ACA? Ashish K. Jha, MD, MPH Boston Medical Center, March 2012 Agenda for today s talk Why focus on providers that care for minorities and other underserved
HOW WILL MINORITY-SERVING HOSPITALS FARE UNDER THE ACA? Ashish K. Jha, MD, MPH Boston Medical Center, March 2012 Agenda for today s talk Why focus on providers that care for minorities and other underserved
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate
 TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
National Council for Behavioral Health. Trauma-informed Primary Care: Fostering Resilience and Recovery Learning Community
 National Council for Behavioral Health Trauma-informed Primary Care: Fostering Resilience and Recovery Learning Community Request for Applications INTRODUCTION The National Council for Behavioral Health
National Council for Behavioral Health Trauma-informed Primary Care: Fostering Resilience and Recovery Learning Community Request for Applications INTRODUCTION The National Council for Behavioral Health
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers
 Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Evidence Summary for the Care Transitions Program
 Social Programs That Work Review Evidence Summary for the Care Transitions Program HIGHLIGHTS: PROGRAM: The Care Transitions Program is a low-cost hospital discharge planning and home follow-up program
Social Programs That Work Review Evidence Summary for the Care Transitions Program HIGHLIGHTS: PROGRAM: The Care Transitions Program is a low-cost hospital discharge planning and home follow-up program
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Supplementary Online Content
 Supplementary Online Content Buurman BM, Parlevliet JL, Allore HG, et al. Comprehensive geriatric assessment and transitional care in acutely hospitalized patients: the Transitional Care Bridge Randomized
Supplementary Online Content Buurman BM, Parlevliet JL, Allore HG, et al. Comprehensive geriatric assessment and transitional care in acutely hospitalized patients: the Transitional Care Bridge Randomized
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Improving Care Transitions: Creating Your Evidence-Based Approach
 Improving Care Transitions: Creating Your Evidence-Based Approach Jack Chase, MD Director of Operations, UCSF Family Medicine Inpatient Service San Francisco General Hospital Assistant Clinical Professor
Improving Care Transitions: Creating Your Evidence-Based Approach Jack Chase, MD Director of Operations, UCSF Family Medicine Inpatient Service San Francisco General Hospital Assistant Clinical Professor
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures. Learning Objectives
 Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Community Development and Health: Alignment Opportunities for CDFIs and Hospitals
 Community Development and Health: Alignment Opportunities for CDFIs and Hospitals Summary of Chicago Convening: October 21 22, 2015 Overview Expansion in coverage and a shift in payment models from volume
Community Development and Health: Alignment Opportunities for CDFIs and Hospitals Summary of Chicago Convening: October 21 22, 2015 Overview Expansion in coverage and a shift in payment models from volume
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Bridges UW Health Transitions of Care
 Bridges UW Health Transitions of Care Spring 2016 Volume 6 Inside this issue: Community Partner Corner 2 Finding TC Notes in Health Link 2 Surgical Transitions Program Kudos from Our Patients 3 3 Need
Bridges UW Health Transitions of Care Spring 2016 Volume 6 Inside this issue: Community Partner Corner 2 Finding TC Notes in Health Link 2 Surgical Transitions Program Kudos from Our Patients 3 3 Need
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Health and Long-Term Care Use Patterns for Ohio s Dual Eligible Population Experiencing Chronic Disability
 Health and Long-Term Care Use Patterns for Ohio s Dual Eligible Population Experiencing Chronic Disability Shahla A. Mehdizadeh, Ph.D. 1 Robert A. Applebaum, Ph.D. 2 Gregg Warshaw, M.D. 3 Jane K. Straker,
Health and Long-Term Care Use Patterns for Ohio s Dual Eligible Population Experiencing Chronic Disability Shahla A. Mehdizadeh, Ph.D. 1 Robert A. Applebaum, Ph.D. 2 Gregg Warshaw, M.D. 3 Jane K. Straker,
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
2018 DOM HealthCare Quality Symposium Poster Session
 Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
2012 Community Health Needs Assessment
 2012 Community Health Needs Assessment University Hospitals (UH) long-standing commitment to the community spans more than 145 years. This commitment has grown and evolved through significant thought and
2012 Community Health Needs Assessment University Hospitals (UH) long-standing commitment to the community spans more than 145 years. This commitment has grown and evolved through significant thought and
EuroHOPE: Hospital performance
 EuroHOPE: Hospital performance Unto Häkkinen, Research Professor Centre for Health and Social Economics, CHESS National Institute for Health and Welfare, THL What and how EuroHOPE does? Applies both the
EuroHOPE: Hospital performance Unto Häkkinen, Research Professor Centre for Health and Social Economics, CHESS National Institute for Health and Welfare, THL What and how EuroHOPE does? Applies both the
Long-Stay Alternate Level of Care in Ontario Mental Health Beds
 Health System Reconfiguration Long-Stay Alternate Level of Care in Ontario Mental Health Beds PREPARED BY: Jerrica Little, BA John P. Hirdes, PhD FCAHS School of Public Health and Health Systems University
Health System Reconfiguration Long-Stay Alternate Level of Care in Ontario Mental Health Beds PREPARED BY: Jerrica Little, BA John P. Hirdes, PhD FCAHS School of Public Health and Health Systems University
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals
 Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Medical Care Meets Long-Term Services and Supports (LTSS)
") Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
ACCESS TO MENTAL HEALTH CARE IN RURAL AMERICA: A CRISIS IN THE MAKING FOR SENIORS AND PEOPLE WITH DISABILITIES
 ACCESS TO MENTAL HEALTH CARE IN RURAL AMERICA: A CRISIS IN THE MAKING FOR SENIORS AND PEOPLE WITH DISABILITIES A Capitol Hill Briefing Sponsored by the: AMERICAN MENTAL HEALTH COUNSELORS ASSOCIATION (AMHCA)
ACCESS TO MENTAL HEALTH CARE IN RURAL AMERICA: A CRISIS IN THE MAKING FOR SENIORS AND PEOPLE WITH DISABILITIES A Capitol Hill Briefing Sponsored by the: AMERICAN MENTAL HEALTH COUNSELORS ASSOCIATION (AMHCA)
Community Health Needs Assessment July 2015
 Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Predicting Transitions in the Nursing Workforce: Professional Transitions from LPN to RN
 Predicting Transitions in the Nursing Workforce: Professional Transitions from LPN to RN Cheryl B. Jones, PhD, RN, FAAN; Mark Toles, PhD, RN; George J. Knafl, PhD; Anna S. Beeber, PhD, RN Research Brief,
Predicting Transitions in the Nursing Workforce: Professional Transitions from LPN to RN Cheryl B. Jones, PhD, RN, FAAN; Mark Toles, PhD, RN; George J. Knafl, PhD; Anna S. Beeber, PhD, RN Research Brief,
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Predicting use of Nurse Care Coordination by Patients in a Health Care Home
 Predicting use of Nurse Care Coordination by Patients in a Health Care Home Catherine E. Vanderboom PhD, RN Clinical Nurse Researcher Mayo Clinic Rochester, MN USA 3 rd Annual ICHNO Conference Chicago,
Predicting use of Nurse Care Coordination by Patients in a Health Care Home Catherine E. Vanderboom PhD, RN Clinical Nurse Researcher Mayo Clinic Rochester, MN USA 3 rd Annual ICHNO Conference Chicago,
Community Mental Health and Care integration. Zandrea Ware and Ricardo Fraga
 Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
Evaluation of a High Risk Case Management Pilot Program for Medicare Beneficiaries with Medigap Coverage
 Evaluation of a High Risk Case Management Pilot Program for Medicare Beneficiaries with Medigap Coverage American Public Health Association Monday, October 29, 2012: 10:30 AM-12:00 PM Kevin Hawkins, PhD
Evaluation of a High Risk Case Management Pilot Program for Medicare Beneficiaries with Medigap Coverage American Public Health Association Monday, October 29, 2012: 10:30 AM-12:00 PM Kevin Hawkins, PhD
Team Building Storyboard Template
 Team Building Storyboard Template Storyboard purpose: To assist teams in telling their team members and organization s story. Behavioral Health Discharge Management Team Motto: We provide quality patient
Team Building Storyboard Template Storyboard purpose: To assist teams in telling their team members and organization s story. Behavioral Health Discharge Management Team Motto: We provide quality patient
January 4, Via Electronic Mail to file code CMS-3317-P
 701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
Abstract Session G3: Hospital-Based Medicine
 Abstract Session G3: Hospital-Based Medicine Emergency Department Utilization by Primary Care Patients at an Urban Safety-Net Hospital Karen Lasser 1 ; Jeffrey Samet 1 ; Howard Cabral 2 ; Andrea Kronman
Abstract Session G3: Hospital-Based Medicine Emergency Department Utilization by Primary Care Patients at an Urban Safety-Net Hospital Karen Lasser 1 ; Jeffrey Samet 1 ; Howard Cabral 2 ; Andrea Kronman
Special Needs Program Training. Quality Management Department
 10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
Click to edit Master title style
 Preventing, Detecting and Managing Chronic Disease for Medicare Kenneth E. Thorpe, Ph.D. Robert W. Woodruff Professor and Chair of the Department of Health Policy & Management, Rollins School of Public
Preventing, Detecting and Managing Chronic Disease for Medicare Kenneth E. Thorpe, Ph.D. Robert W. Woodruff Professor and Chair of the Department of Health Policy & Management, Rollins School of Public
CALIFORNIA HEALTHCARE FOUNDATION. Medi-Cal Versus Employer- Based Coverage: Comparing Access to Care JULY 2015 (REVISED JANUARY 2016)
") CALIFORNIA HEALTHCARE FOUNDATION Medi-Cal Versus Employer- Based Coverage: Comparing Access to Care JULY 2015 (REVISED JANUARY 2016) Contents About the Authors Tara Becker, PhD, is a statistician at the
CALIFORNIA HEALTHCARE FOUNDATION Medi-Cal Versus Employer- Based Coverage: Comparing Access to Care JULY 2015 (REVISED JANUARY 2016) Contents About the Authors Tara Becker, PhD, is a statistician at the
Issue Brief. Maine s Health Care Workforce. January Maine s Unique Challenge. Current State of Maine s Health Care Workforce
 January 2009 Issue Brief Maine s Health Care Workforce Affordable, quality health care is critical to Maine s continued economic development and quality of life. Yet substantial shortages exist at almost
January 2009 Issue Brief Maine s Health Care Workforce Affordable, quality health care is critical to Maine s continued economic development and quality of life. Yet substantial shortages exist at almost
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network. Monday, September 12, 2011
 Care Coordination and the Role of the Aging Network. Monday, September 12, 2011") National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
Test bank PowerPoint slides for each chapter Instructor guides for each chapter (with answers for discussion questions and case studies)
") This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
CAREGIVING COSTS. Declining Health in the Alzheimer s Caregiver as Dementia Increases in the Care Recipient
 CAREGIVING COSTS Declining Health in the Alzheimer s Caregiver as Dementia Increases in the Care Recipient National Alliance for Caregiving and Richard Schulz, Ph.D. and Thomas Cook, Ph.D., M.P.H. University
CAREGIVING COSTS Declining Health in the Alzheimer s Caregiver as Dementia Increases in the Care Recipient National Alliance for Caregiving and Richard Schulz, Ph.D. and Thomas Cook, Ph.D., M.P.H. University
Kalispell Regional Healthcare Kalispell, Montana Managing the Needs of Medically and Socially Complex Patients or Superutilizers
 Kalispell Regional Healthcare Kalispell, Montana Managing the Needs of Medically and Socially Complex Patients or Superutilizers A small number of individuals drive much of the cost in the American health
Kalispell Regional Healthcare Kalispell, Montana Managing the Needs of Medically and Socially Complex Patients or Superutilizers A small number of individuals drive much of the cost in the American health
Long Term Care. Lecture for HS200 Nov 14, 2006
 Long Term Care Lecture for HS200 Nov 14, 2006 Steven P. Wallace, Ph.D. Professor, Dept. Community Health Sciences, SPH and Associate Director, UCLA Center for Health Policy Research What is long-term care
Long Term Care Lecture for HS200 Nov 14, 2006 Steven P. Wallace, Ph.D. Professor, Dept. Community Health Sciences, SPH and Associate Director, UCLA Center for Health Policy Research What is long-term care
From Risk Scores to Impactability Scores:
 From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
CLOSING THE DIVIDE: HOW MEDICAL HOMES PROMOTE EQUITY IN HEALTH CARE
 CLOSING DIVIDE: HOW MEDICAL HOMES PROMOTE EQUITY IN HEALTH CARE RESULTS FROM 26 HEALTH CARE QUALITY SURVEY Anne C. Beal, Michelle M. Doty, Susan E. Hernandez, Katherine K. Shea, and Karen Davis June 27
CLOSING DIVIDE: HOW MEDICAL HOMES PROMOTE EQUITY IN HEALTH CARE RESULTS FROM 26 HEALTH CARE QUALITY SURVEY Anne C. Beal, Michelle M. Doty, Susan E. Hernandez, Katherine K. Shea, and Karen Davis June 27
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
A23/B23: Patient Harm in US Hospitals: How Much? Objectives
 A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Reducing Hospital Readmissions for Vulnerable Patient Populations: Policy Concerns and Interventions
 Reducing Hospital Readmissions for Vulnerable Patient Populations: Policy Concerns and Interventions Jacob Roberts Washington and Lee University 17 Poverty and Human Capability: A Research Seminar Winter
Reducing Hospital Readmissions for Vulnerable Patient Populations: Policy Concerns and Interventions Jacob Roberts Washington and Lee University 17 Poverty and Human Capability: A Research Seminar Winter
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
The Number of People With Chronic Conditions Is Rapidly Increasing
 Section 1 Demographics and Prevalence The Number of People With Chronic Conditions Is Rapidly Increasing In 2000, 125 million Americans had one or more chronic conditions. Number of People With Chronic
Section 1 Demographics and Prevalence The Number of People With Chronic Conditions Is Rapidly Increasing In 2000, 125 million Americans had one or more chronic conditions. Number of People With Chronic
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON
 THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations
THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations
NGA Paper. Using Data to Better Serve the Most Complex Patients: Highlights from NGA s Intensive Work with Seven States
 NGA Paper Using Data to Better Serve the Most Complex Patients: Highlights from NGA s Intensive Work with Seven States Executive Summary Across the country, health care systems continue to grapple with
NGA Paper Using Data to Better Serve the Most Complex Patients: Highlights from NGA s Intensive Work with Seven States Executive Summary Across the country, health care systems continue to grapple with
Community Health Improvement Plan
 Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Minority Serving Hospitals and Cancer Surgery Readmissions: A Reason for Concern
 Minority Serving Hospitals and Cancer Surgery : A Reason for Concern Young Hong, Chaoyi Zheng, Russell C. Langan, Elizabeth Hechenbleikner, Erin C. Hall, Nawar M. Shara, Lynt B. Johnson, Waddah B. Al-Refaie
Minority Serving Hospitals and Cancer Surgery : A Reason for Concern Young Hong, Chaoyi Zheng, Russell C. Langan, Elizabeth Hechenbleikner, Erin C. Hall, Nawar M. Shara, Lynt B. Johnson, Waddah B. Al-Refaie
Opportunities and Issues Related to BH Services in Primary Care
 Opportunities and Issues Related to BH Services in Primary Care Roger Kathol, MD, CPE President, Cartesian Solutions, Inc. Adjunct Professor, Internal Medicine & Psychiatry, University of Minnesota Clinical
Opportunities and Issues Related to BH Services in Primary Care Roger Kathol, MD, CPE President, Cartesian Solutions, Inc. Adjunct Professor, Internal Medicine & Psychiatry, University of Minnesota Clinical
Comparison of Care in Hospital Outpatient Departments and Physician Offices
 Comparison of Care in Hospital Outpatient Departments and Physician Offices Final Report Prepared for: American Hospital Association February 2015 Berna Demiralp, PhD Delia Belausteguigoitia Qian Zhang,
Comparison of Care in Hospital Outpatient Departments and Physician Offices Final Report Prepared for: American Hospital Association February 2015 Berna Demiralp, PhD Delia Belausteguigoitia Qian Zhang,
January 04, Submitted Electronically
 January 04, 2016 Submitted Electronically Mr. Andy Slavitt Acting Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
January 04, 2016 Submitted Electronically Mr. Andy Slavitt Acting Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
FirstHealth Moore Regional Hospital. Implementation Plan
 FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
Access to Mental Health Services Among Patients at Health Centers and Factors Associated with Unmet Needs
 Access to Mental Health Services Among Patients at Health Centers and Factors Associated with Unmet Needs Emily Jones, Lydie A. Lebrun-Harris, Alek Sripipatana, Quyen Ngo-Metzger Journal of Health Care
Access to Mental Health Services Among Patients at Health Centers and Factors Associated with Unmet Needs Emily Jones, Lydie A. Lebrun-Harris, Alek Sripipatana, Quyen Ngo-Metzger Journal of Health Care
Course Module Objectives
 Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of