Dimissione e periodo vulnerabile: come evitare le reospedalizzazioni precoci.
|
|
|
- Erin Paul
- 6 years ago
- Views:
Transcription



1 Scompenso Cardiaco Acuto Convention Centri Scompenso Dimissione e periodo vulnerabile: come evitare le reospedalizzazioni precoci. G. Di Tano Cardiologia, Cremona





2 Early Re-hospitalizations 30 days OHF - Chronic HF De novo HF Worsening HF ED Hospital Admission for AHF Early and Later Post-discharge period OHF - Chronic HF In-hospital Mortality Early Mortality The steps of Heart Failure patient s journey DT14



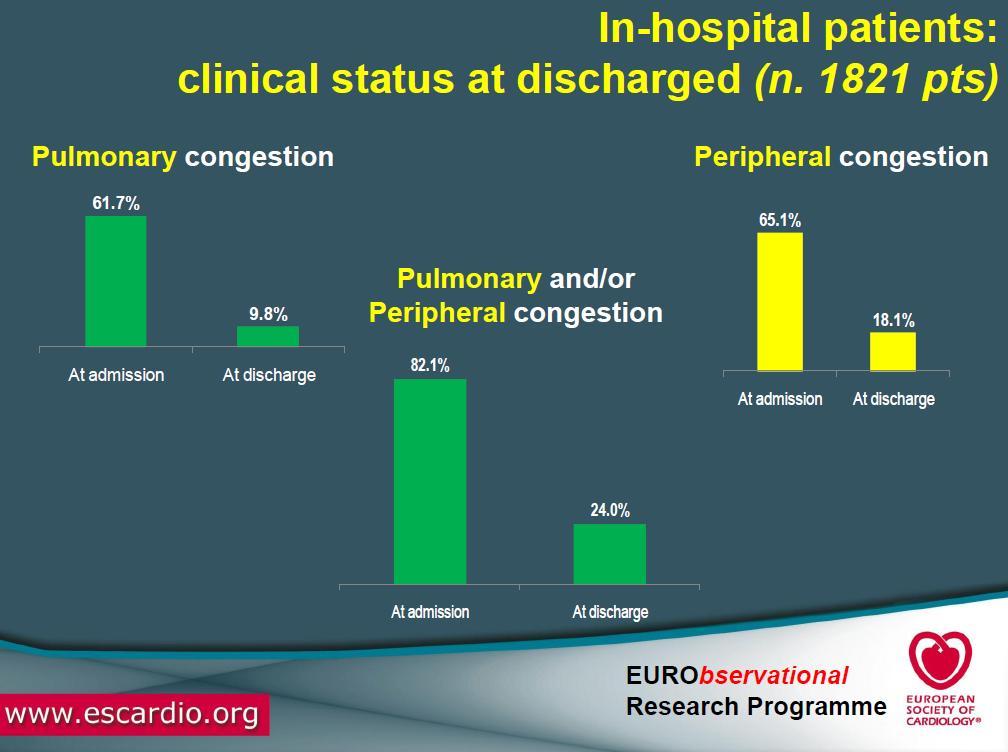
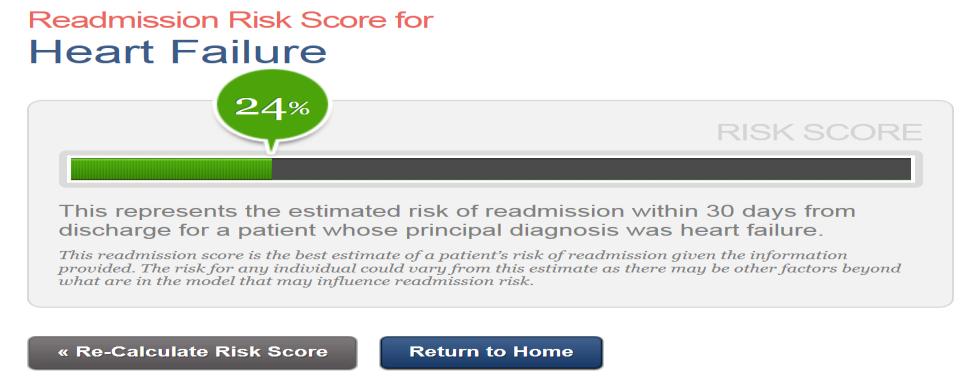
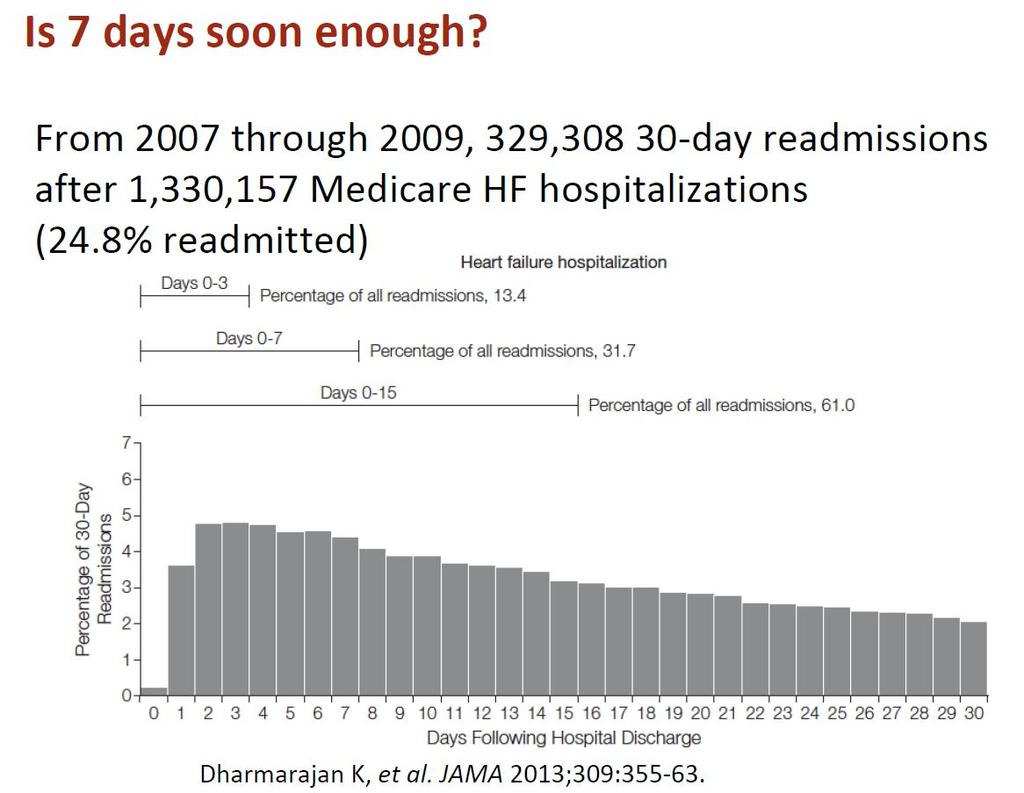
3 Rehospitalization is high in the early and later phase after hospitalization 30 days from discharge 1 patient out of 4 is readmitted
4 Progetto re-ospedalizzazioni precoci Area Scompenso The 30-day metric in Acute Heart Failure revisited. Data from IN-HF Outcome, an Italian Nationwide Cardiology Registry 1855 AHF enrolled 118 (6.4%) died in-hospital 159 transferred to other hospital 57 discharged to skilled nursing facilities 1 lost 1520 Discharged home 94 readmitted (6.1%) - 91% for CV causes - 42 dead (2.8%) 0 At 30 days from discharge 126 overall dead or readmitted (8.3%) At 30 days from 0 admission 7.6% dead G. Di Tano, R. De Maria et al. EJHF submitted




5 IN-HF 30 day outcome in 1520 discharged home 30-d read-free survivors 30-d readmitted or dead
6 Logistic regression independent predictors of death+ readmission or readmission at 30 days Combined death+read p 0R 95% Days Length of stay Worsening HF vs de novo Inotropes ACE/ARBs at discharge C statistic Days Length of stay Worsening HF vs de novo ACE/ARBs at discharge C statistic Il pz che muore/rericovera nelle Cardiologie a breve, ha SC cronico avanzato, disf renale, degenza lunga, con inotropi, meno RAS-inib.


7 Predictors of 30-Day Readmission in 412 Pts Hospitalized With Decompensated Heart Failure ( Hernadez MB et al, Clin. Cardiol )

8 TROPONIN, injury, cardiovascular events AST/ALT, organ damage


9 IN HOSPITAL Early HF readmission and 30-day mortality are associated with the process of inpatient care Meta-analysis of 13 studies: The risk of early readmission is increased by 55% when inpatient care is of relatively low quality... I was discharged early! They told me to just take these tablets!!! Ashton CM et al. Ann Intern Med. 2005;122:415. Ashton CM et al. Med Care. 2007;35:1044
10



11 Valle R et al
12 Discharge and Follow-up: The beginning of the journey of a vulnerable patient For many if not most patients, hospitalization is just one step in chronic Heart Failure Once acute decompensation is stabilized we move quikly to optimize chronic therapy IN HOSPITAL to prevent rehospitalization. PRE-DISCHARGE therapy determines early outcome

13 2001
14

15
16 Hospital Discharge Recommendation or Indication COR LOE Performance improvement systems in the hospital and early postdischarge outpatient setting to identify HF for GDMT I B Before hospital discharge, at the first postdischarge visit, and in subsequent follow-up visits, the following should be addressed: a) initiation of GDMT if not done or contraindicated; b) causes of HF, barriers to care, and limitations in support; c) assessment of volume status and blood pressure with adjustment of HF therapy; d) optimization of chronic oral HF therapy; e) renal function and electrolytes; f) management of comorbid conditions; g) HF education, self-care, emergency plans, and adherence; and h) palliative or hospice care. I B Multidisciplinary HF disease-management programs for patients at high risk for hospital readmission are recommended A follow-up visit within 7 to 14 days and/or a telephone follow-up within 3 days of hospital discharge is reasonable Use of clinical risk-prediction tools and/or biomarkers to identify higher-risk patients is reasonable I IIa IIa B B B
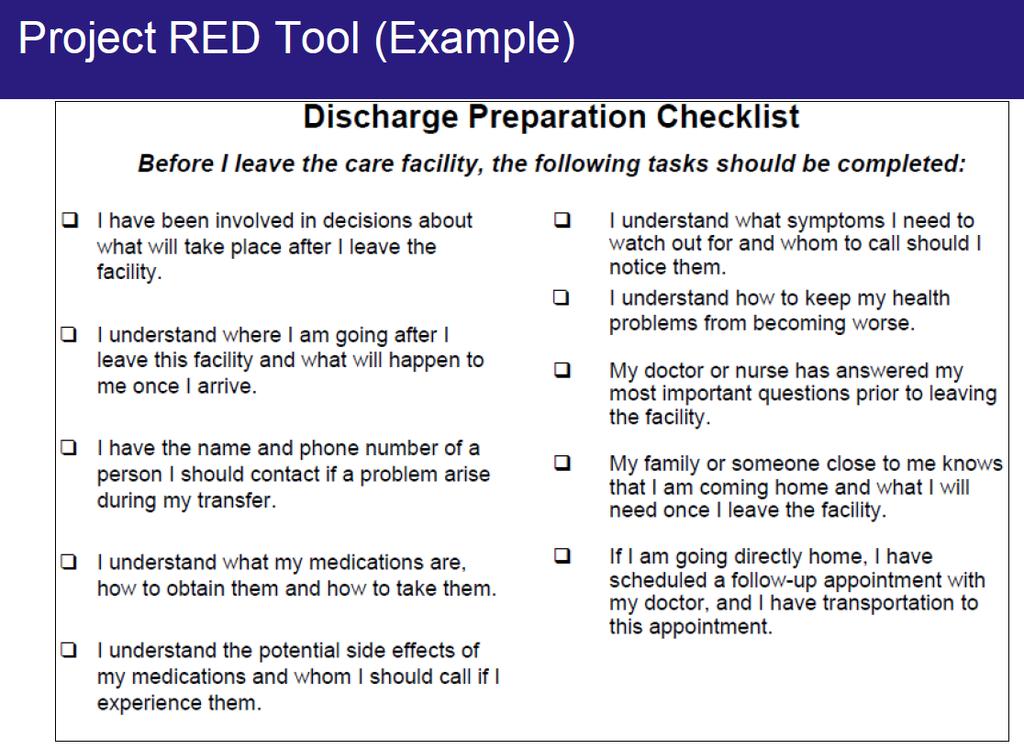
 Information about disease or condition When to call physician or seek emergency care Form for writing down questions Map for locating appointments (optional) Other information about your center")
17 Patient Care Plan Date of discharge Name and contact information for physician and DA Medications Pending tests and results Follow-up appointments Calendar Other orders (diet, activity, etc.) Information about disease or condition When to call physician or seek emergency care Form for writing down questions Map for locating appointments (optional) Other information about your center (optional)
18
19 (52% of HF patients are not seen in the first 30 days after a hospitalization... Jencks et al. N Engl J Med 2009 )

20 First post-discharge assessment When?
21
22 For a patient hospitalized due to AHF, pre-discharge phase is crucial for the optimal preparation to the vulnerable period of transition from in-patient to out-patient care. During this phase the following aspects should be addressed: Disease-modifying therapies should be initiated before discharge and carefully optimized during early post-discharge period. Comorbid conditions detected and managed. Patients at the highest risk identified and carefully followed. Potential precipitant causes of recurrent HF characterised. Patients enrolled in the multi-faced disease management projects.

23
24
25
26
27
 1) Partnering with local hospitals to reduce readmissions (0.34 percentage point; P=0.020) 2) Having nurses responsible for medication reconciliation (0.18 percentage point; P=0.")
28 Circ Cardiovasc Qual Outcomes ) Partnering with community physicians or physician groups to reduce readmission (0.33 percentage point lower RSRRs; P=0.017) 1) Partnering with local hospitals to reduce readmissions (0.34 percentage point; P=0.020) 2) Having nurses responsible for medication reconciliation (0.18 percentage point; P=0.002) 3) Arranging a follow-up appointment before discharge (0.19 percentage point; P=0.037) 4) Having a process in place to send all discharge paper or electronic summaries directly to the patient s primary physician (0.21 percentage point; P=0.004), 5) Assigning staff to follow up on test results that return after the patient is discharged (0.26 percentage point; P=0.049)

29 Un MINIMAL DATA SET alla dimissione per il Medico di Famiglia

")
30 FOLLOW-UP DOPO LA DIMISSIONE OSPEDALIERA PZ A BASSO PROFILO DI RISCHIO Follow-up di 1-(3)-6 mesi presso l ambulatorio Scompenso Cardiaco per up-tritation della terapia, FU strumentale, valutazione devices, PZ AD ALTO PROFILO DI RISCHIO Decorso osp. BNP no - Re-ammissione - compliance Disf. Renale Comorbidità +++ Score +++ Visita precoce (< 7 gg) presso l Ambulatorio Scompenso Cardiaco Protocolli Terapeutici ambulatoriali Pz stabile Pz instabile Stretto monitoraggio telefonico domiciliare Reinvio e coinvolgimento del MMG - Follow-up telefonico Prosecuzione del Follow-up (tempi succ visita variabili ) ambulatoriale e telefonico


31 N Engl J Med 370;8, 2014
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions
 1 The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions Julia N. Clarkson, Susan D. Schaffer, Joshua J. Clarkson Heart failure (HF) is a pressing concern to public
1 The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions Julia N. Clarkson, Susan D. Schaffer, Joshua J. Clarkson Heart failure (HF) is a pressing concern to public
Challenging The 2015 PH Guidelines - comments from the Nurses. Wendy Gin-Sing RN MSc Pulmonary Hypertension CNS Imperial College Healthcare NHS Trust
 Challenging The 2015 PH Guidelines - comments from the Nurses Wendy Gin-Sing RN MSc Pulmonary Hypertension CNS Imperial College Healthcare NHS Trust Recommendations for pulmonary hypertension expert referral
Challenging The 2015 PH Guidelines - comments from the Nurses Wendy Gin-Sing RN MSc Pulmonary Hypertension CNS Imperial College Healthcare NHS Trust Recommendations for pulmonary hypertension expert referral
University Cincinnati Medical Center
 University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
From Risk Scores to Impactability Scores:
 From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Brittany Turner, 2015 PharmD Candidate 1 Justin Campbell, PharmD 2 Katie McKinney, PharmD, MS, BCPS 2
 Discharge Medication Concierge Program: A pilot project in heart failure to reduce readmission rates, improve patient satisfaction, and increase pharmacy business metrics Brittany Turner, 2015 PharmD Candidate
Discharge Medication Concierge Program: A pilot project in heart failure to reduce readmission rates, improve patient satisfaction, and increase pharmacy business metrics Brittany Turner, 2015 PharmD Candidate
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
New pharmacy practice opportunity: Enhancement of the transitions of care process
 New pharmacy practice opportunity: Enhancement of the transitions of care process EMMA GORMAN, PHARMD CLINICAL ASSISTANT PROFESSOR DEPARTMENT OF PHARMACY PRACTICE D YOUVILLE SCHOOL OF PHARMACY BUFFALO,
New pharmacy practice opportunity: Enhancement of the transitions of care process EMMA GORMAN, PHARMD CLINICAL ASSISTANT PROFESSOR DEPARTMENT OF PHARMACY PRACTICE D YOUVILLE SCHOOL OF PHARMACY BUFFALO,
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT)
") Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Chronic Care Taking Disease Management Beyond Hospital Walls
 Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Heart Failure Nurse Practitioner Role Development and Proposal. Anita M. Wilson, BSN, RN. ACNP, DNP Student Creighton University
 1 Heart Failure Nurse Practitioner Role Development and Proposal Anita M. Wilson, BSN, RN ACNP, DNP Student Creighton University PO Box 21 Kingsley, IA 51028 abwilson@frontiernet.net 712-490-8347 Mary
1 Heart Failure Nurse Practitioner Role Development and Proposal Anita M. Wilson, BSN, RN ACNP, DNP Student Creighton University PO Box 21 Kingsley, IA 51028 abwilson@frontiernet.net 712-490-8347 Mary
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons
 Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
2) The percentage of discharges for which the patient received follow-up within 7 days after
 The percentage of discharges for which the patient received follow-up within 7 days after") Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Objectives. Prevalence of Non-Adherence. Medications and Care Transitions. The Cost of Readmissions. The Pharmacist s Role in Improving Care 4/22/2015
 MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT
 1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Models of community heart failure care pathways. Dr Jim Moore GP & GPSI Cardiology Cheltenham,GLOS
 Models of community heart failure care pathways Dr Jim Moore GP & GPSI Cardiology Cheltenham,GLOS Declaration of Conflict of Interests Dr Jim Moore GP and GPwSI in Cardiology, Cheltenham NICE Guideline
Models of community heart failure care pathways Dr Jim Moore GP & GPSI Cardiology Cheltenham,GLOS Declaration of Conflict of Interests Dr Jim Moore GP and GPwSI in Cardiology, Cheltenham NICE Guideline
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
INTERMACS has a Key Role in Reporting on Quality Metrics
 INTERMACS has a Key Role in Reporting on Quality Metrics Robert L Kormos MD FACS, FAHA FRCS(C) Director Artificial Heart Program University of Pittsburgh Medical Center The Patient Protection and Affordable
INTERMACS has a Key Role in Reporting on Quality Metrics Robert L Kormos MD FACS, FAHA FRCS(C) Director Artificial Heart Program University of Pittsburgh Medical Center The Patient Protection and Affordable
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Improving Care Transitions
 Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Home Assessments Resulting in a Positive Effect on Outcome Score Cards
 Home Assessments Resulting in a Positive Effect on Outcome Score Cards Presented by: Angela Benson, OTR/L, Clinical Specialist *graduated from Mount Aloysius College, Cresson, PA *9 years of experience
Home Assessments Resulting in a Positive Effect on Outcome Score Cards Presented by: Angela Benson, OTR/L, Clinical Specialist *graduated from Mount Aloysius College, Cresson, PA *9 years of experience
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Chronic Disease Management Resources & Services
 Chronic Disease Management Resources & Services Michelle Nelson, RN, BSN Director of Ambulatory Services & Chronic Disease Management Gidgett Bates, RN, BSN Manager of Palliative Care, Diabetes Education,
Chronic Disease Management Resources & Services Michelle Nelson, RN, BSN Director of Ambulatory Services & Chronic Disease Management Gidgett Bates, RN, BSN Manager of Palliative Care, Diabetes Education,
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
MediServe. More than 25 Years Serving the Rehab and Respiratory Communities
 MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
Causes and Consequences of Regional Variations in Health Care Resources in Ontario
 Causes and Consequences of Regional Variations in Health Care Resources in Thérèse A. Stukel, Ph.D. DA Alter, R Saskin, DM Rothwell Institute for Clinical Evaluative Sciences, Health Services Restructuring
Causes and Consequences of Regional Variations in Health Care Resources in Thérèse A. Stukel, Ph.D. DA Alter, R Saskin, DM Rothwell Institute for Clinical Evaluative Sciences, Health Services Restructuring
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Baystate Medical Center
 Baystate Medical Center STAAR Collaborative February 2 & 3 2011 680 bed tertiary care referral center ( ~1M) Flagship of Baystate Health 42 k admissions/year Annual surgical volume: 29,043 Western Campus
Baystate Medical Center STAAR Collaborative February 2 & 3 2011 680 bed tertiary care referral center ( ~1M) Flagship of Baystate Health 42 k admissions/year Annual surgical volume: 29,043 Western Campus
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations. Aetna s Compassionate Care SM Program
 Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE. Measure Information Form
 Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE Measure Set: CMS Readmission Measures Set Measure ID #: READM-30-HWR Measure Information Form Performance Measure Name:
Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE Measure Set: CMS Readmission Measures Set Measure ID #: READM-30-HWR Measure Information Form Performance Measure Name:
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy
 Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
CV SURGERY 30 DAY RE-ADMISSION. CMS IS WATCHING YOU, AND YOU, AND ME TOO.
 CV SURGERY 30 DAY RE-ADMISSION. CMS IS WATCHING YOU, AND YOU, AND ME TOO. THE TEAM UTAH VALLEY HOSPITAL John Mitchell, MD January 16, 2016 Centers for Medicare and Medicaid Services Federally funded inpatient
CV SURGERY 30 DAY RE-ADMISSION. CMS IS WATCHING YOU, AND YOU, AND ME TOO. THE TEAM UTAH VALLEY HOSPITAL John Mitchell, MD January 16, 2016 Centers for Medicare and Medicaid Services Federally funded inpatient
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals
 Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transition hôpital-domicile: Risques et opportunités! Pr Martine LOUIS SIMONET Formation Continue Médecins de Famille Genève 14 avril 2016
 Transition hôpital-domicile: Risques et opportunités! Pr Martine LOUIS SIMONET Formation Continue Médecins de Famille Genève 14 avril 2016 Transitional care is defined as a set of actions designed to ensure
Transition hôpital-domicile: Risques et opportunités! Pr Martine LOUIS SIMONET Formation Continue Médecins de Famille Genève 14 avril 2016 Transitional care is defined as a set of actions designed to ensure
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know
 New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know Presented by: Kathy Pellatt, Senior Quality Improvement Analyst LeadingAge New York
New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know Presented by: Kathy Pellatt, Senior Quality Improvement Analyst LeadingAge New York
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Objectives 9/18/2018. Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018
 Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018") Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018 Mission: The trusted voice for aging. Objectives List the five(5) case mix components
Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018 Mission: The trusted voice for aging. Objectives List the five(5) case mix components
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Continuing Education Disclosures
 Supporting CHF Patients in the Home Setting through a Comprehensive Community Approach Diane Schuh, RN, BSN Aurora Sheboygan Memorial Medical Center September 26, 2017 Continuing Education Disclosures
Supporting CHF Patients in the Home Setting through a Comprehensive Community Approach Diane Schuh, RN, BSN Aurora Sheboygan Memorial Medical Center September 26, 2017 Continuing Education Disclosures
January 4, Via Electronic Mail to file code CMS-3317-P
 701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
An Integrated Approach to Heart Failure Care. Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN
 An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
Leveraging Your Facility s 5 Star Analysis to Improve Quality
 Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Heart Failure Clinic a Multidisciplinary approach. Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM
 Heart Failure Clinic a Multidisciplinary approach Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
Heart Failure Clinic a Multidisciplinary approach Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
AN OVERVIEW of TARGET HF: QUALIFYING for the HONOR ROLL and a DETAILED FOCUS on MEDICATION COMPLIANCE (ACE/ARB, ADLOSTERONE ANTAGONIST, and EBBB)
") AN OVERVIEW of TARGET HF: QUALIFYING for the HONOR ROLL and a DETAILED FOCUS on MEDICATION COMPLIANCE (ACE/ARB, ADLOSTERONE ANTAGONIST, and EBBB) HAZLETON GENERAL HOSPITAL HAZLETON, PENNSYLVANIA PRESENTERS:
AN OVERVIEW of TARGET HF: QUALIFYING for the HONOR ROLL and a DETAILED FOCUS on MEDICATION COMPLIANCE (ACE/ARB, ADLOSTERONE ANTAGONIST, and EBBB) HAZLETON GENERAL HOSPITAL HAZLETON, PENNSYLVANIA PRESENTERS:
Connect HF Solution. Case Study. Reducing 30-Day Heart Failure. How Process Optimization and Peer-to-Peer Connections Standardized HF Care
 Connect HF Solution Case Study Reducing 30-Day Heart Failure Readmissions How Process Optimization and Peer-to-Peer Connections Standardized HF Care C a s e Study Reducing 30-Day Heart Failure Readmissions
Connect HF Solution Case Study Reducing 30-Day Heart Failure Readmissions How Process Optimization and Peer-to-Peer Connections Standardized HF Care C a s e Study Reducing 30-Day Heart Failure Readmissions
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL MEASURES REGISTRY ONLY
 Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
Hamilton Health Sciences STRATEGIC PLAN. Patients PLAN AT A GLANCE People. Sustainability. Research, Innovation & Learning
 Patients Hamilton Health Sciences STRATEGIC PLAN PLAN AT A GLANCE 2016-2017 Research, Innovation & Learning Hamilton Health Sciences STRATEGIC PLAN PLAN AT A GLANCE 2016-2017 Rob MacIsaac President and
Patients Hamilton Health Sciences STRATEGIC PLAN PLAN AT A GLANCE 2016-2017 Research, Innovation & Learning Hamilton Health Sciences STRATEGIC PLAN PLAN AT A GLANCE 2016-2017 Rob MacIsaac President and
Karen Stasium, BS, MPT, COS C, HCS D
 Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
CPT only copyright 2014 American Medical Association. All rights reserved. 12/23/2014 Page 537 of 593
 Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2015 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL
Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2015 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 2. Expedition Coordinator
 Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 2/27/2013 2010, American Heart Association 2 1
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 2/27/2013 2010, American Heart Association 2 1
Objectives. Integrating Palliative Care Principles into Critical Care Nursing
 1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Use of Health Information Technology to Reduce Health Risk
 Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure
 Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure November 16, 2016 Panelists Corinne Bott-Silverman, M.D., Cardiologist,
Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure November 16, 2016 Panelists Corinne Bott-Silverman, M.D., Cardiologist,
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
Kentucky Stroke Transitions Assistance Resource
 Kentucky Stroke Transitions Assistance Resource Patrick Kitzman, Ph.D., MSPT, Division of Physical Therapy, University of Kentucky Violet Sylvia, Ph.D., Director ARH System of Rehabilitation Services Kentucky
Kentucky Stroke Transitions Assistance Resource Patrick Kitzman, Ph.D., MSPT, Division of Physical Therapy, University of Kentucky Violet Sylvia, Ph.D., Director ARH System of Rehabilitation Services Kentucky
MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care 8/12/2015.
 Preparing for Risk-Based Outcomes of Bundled Care 8/12/2015.") MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care August 13, 2015 Eric M. Rogers MEd RT(R) Managing Consultant erogers@bkd.com Jeff Bond President
MEDICARE COMPREHENSIVE CARE FOR JOINT REPLACEMENT MODEL (CCJR) Preparing for Risk-Based Outcomes of Bundled Care August 13, 2015 Eric M. Rogers MEd RT(R) Managing Consultant erogers@bkd.com Jeff Bond President
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart