Chronic Care Taking Disease Management Beyond Hospital Walls
|
|
|
- Philip Simon
- 5 years ago
- Views:
Transcription



1 Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical Solutions

2 2
3 3 The Chester County Hospital Founded in 1892 Independent, not-for-profit Licensed beds 221 Number of employees 1700 Emergency department visits 41,244 Cancer Center affiliated with HUP Pediatric and Level III NICU affiliated with CHOP Interventional Cardiology & Electrophysiology CV Surgery affiliated with The Cleveland Clinic
4 4 Disease Management A systematic population based approach to identify patients at risk Utilizes evidence based guidelines to prevent exacerbations and complications of chronic disease Supports the practitioner/patient relationship and plan of care Measures clinical and other outcomes to improve quality of care
5 5 Disease Management Support We do not take over management of patients from the PCP we support the medical plan of care Collaboration with outpatient managers of care to promote consistency in treatment, educational and intervention strategies Act as a resource for staff and patients
6 6 Why Heart Failure DM? Nationally Leading cause of hospitalization in persons over age 65 Costs $25.8 billion annually ALOS 6.2 days 20% - 50% readmission rate within 6 months 20% readmission patient failure to seek medical attention for worsening symptoms Our Experience 127 our highest volume DRG 2005 costs - $4,607, reim. - $4,252,997 ($354,926) ALOS 6.4 days Comparable Comparable

7 7 Heart Failure at CCH 467 discharges last year with a primary diagnosis of HF 75% of our HF patients group to DRG 127 DRG with greatest number of excess days Through-put issues/bed availability Core measure compliance
8 8 Our Starting Points Order sets Choose and check progress notes Discharge forms Discharge reminders Patient education material Medical and nursing staff education

9 Getting Started Physician Buy-In 9

10 10 Physician Concerns Patients will be confused Patients will stop coming for office visits Patients might be told something I don t want them to know Conflicting literature about the efficacy of DM programs

11 11 Success with Physician Buy-In Physician champion(s) Demonstration Progress reports Section meetings CME conferences Quality Council Newsletters 1:1 hallway conferences Luncheon meetings with PCPs Bi-weekly HF Taskforce Meetings
12 12 Skepticism to Collaboration Linking with a Cardiology Practice Increase patient satisfaction? Improve/enhance communications between inpatient and outpatient environments? Promote core measure documentation compliance? Reduce LOS when patient is admitted? Reduce admissions, ED visits and unscheduled office visits? Increase patient accountability?
13 13 How We Make It Work Admission notification Patient education Assessment for enrollment in telephone monitoring Assessment for enrollment in research study Assess medical record for compliance with core measures Interdisciplinary collaboration
14 14 CCH Admission Notifications 1. Soarian Workflow Alert. A patient with a admission DX suggesting CHF has been admitted. Patient's Name: ******** has been admitted to floor TELE Bed: The patient's MRN is ******* and their PT ID is 10000*******. The admitting diagnosis is ACUTE DYSPNEA STABLE PNEUMOTHORAX, LEFT PLEURAL FUSION,S/P CORONARY ARTERY BYPASS GRAFT 2. Soarian Workflow Alert. A patient with a history of CHF has been admitted. Patient's Name: ******** has been admitted to floor ACC Bed: OACC21. The patient's MRN is ****** and their PT ID is 10000******. The admitting diagnosis is LEFT TOTAL KNEE ARTHROPLASTY. The last inpatient admission for this patient was on: Unknown
15 15 CCH Admission Notifications 3. Soarian Workflow Alert. A patient enrolled in the outpatient CHF program has been admitted. Patient's Name: ********** has been admitted to floor TELE Bed: The patient's MRN is ******* and their PT ID is 10000*******. The admitting diagnosis is Unknown 4. Soarian Workflow Alert. A patient has just had a new BNP above 150. Patient's Name: ************ is on floor WW2 Bed: The patient's MRN is ****** and their PT ID is 10000*******. The admitting diagnosis is GROSS HEMATURIA. The reported BNP level was: 416
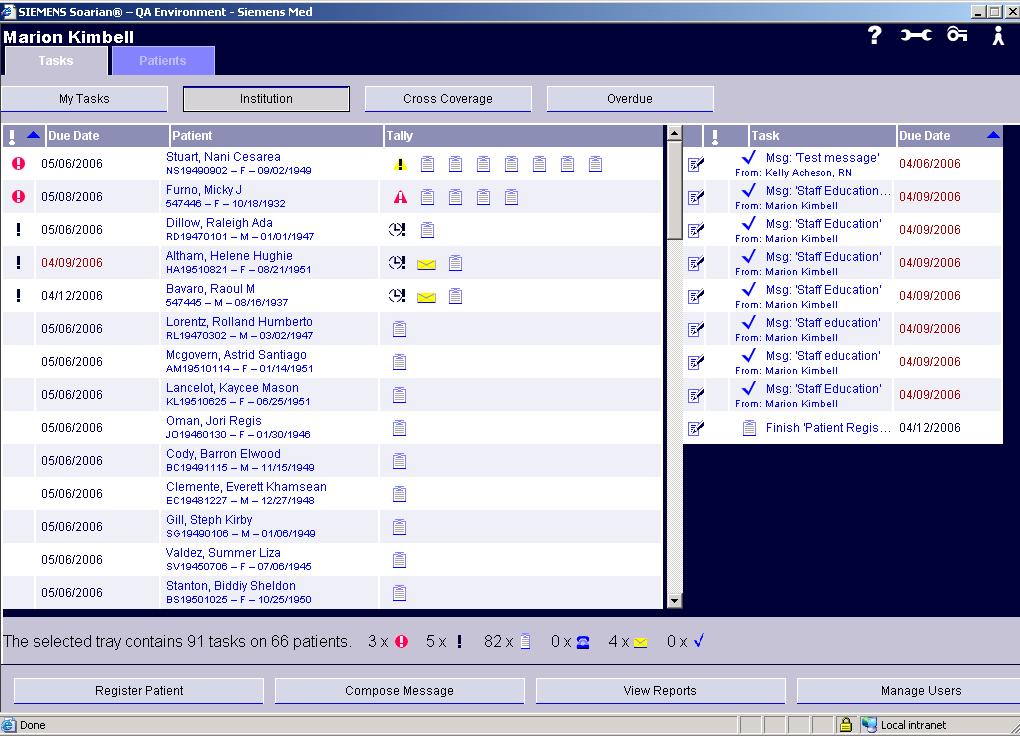
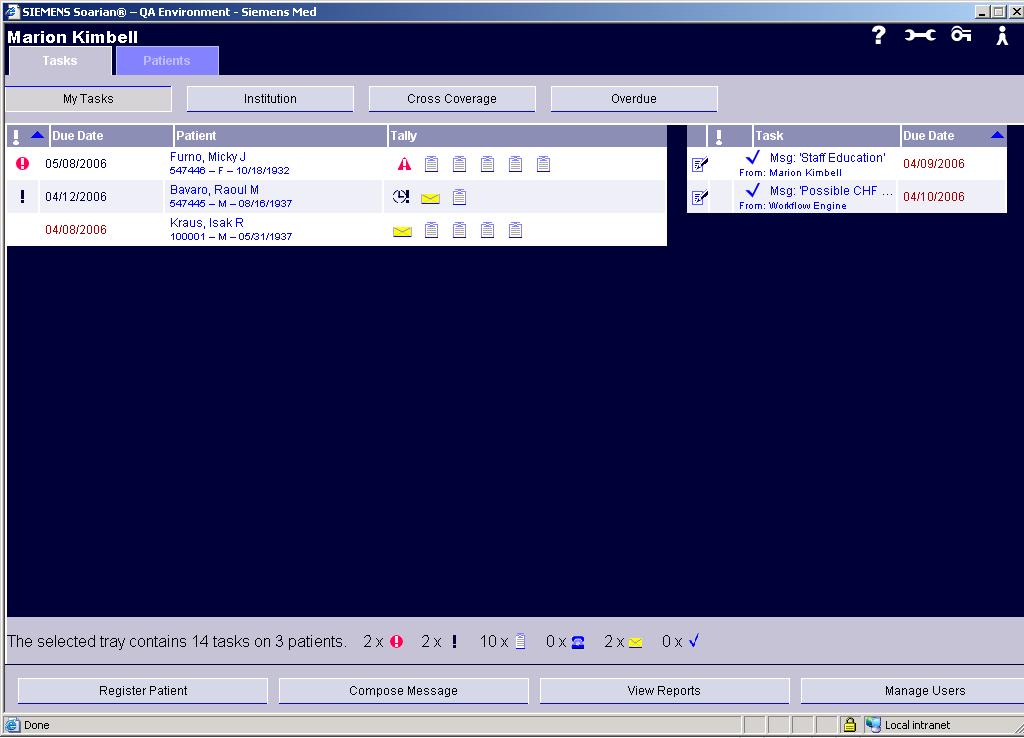
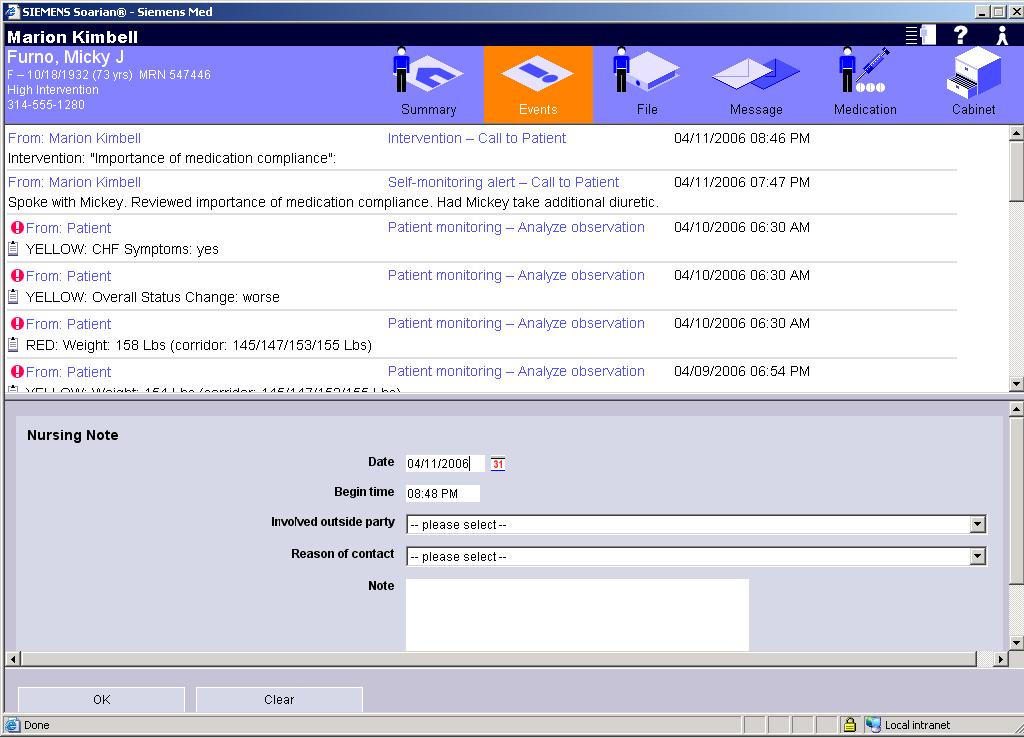
16 16 Soarian DM Computerized data base of HF patients enrolled in telephone monitoring Alerts trigger outbound calls Allows nurse to manage high number of patients and focus outbound calls Early intervention is facilitated Promotes continuum of care
17 17 Outcomes Recognition/acceptance within the organization as evidenced by medical and nursing requests for consults Community and regional recognition Increased collaboration/communication between inpatient and outpatient healthcare practitioners
18 18 Outcomes Reduced hospital visits Bed opportunity Increased awareness of physician practices d/t concurrent chart review Improved compliance with core measure documentation Positive patient feedback
19 19 Next Steps Hospital based HF Clinic Short stay inpatient unit Con-current coding Electronic notification based on EF Apply what we have learned to extend DM support to larger CV patient population Test Soarian DM 2.1




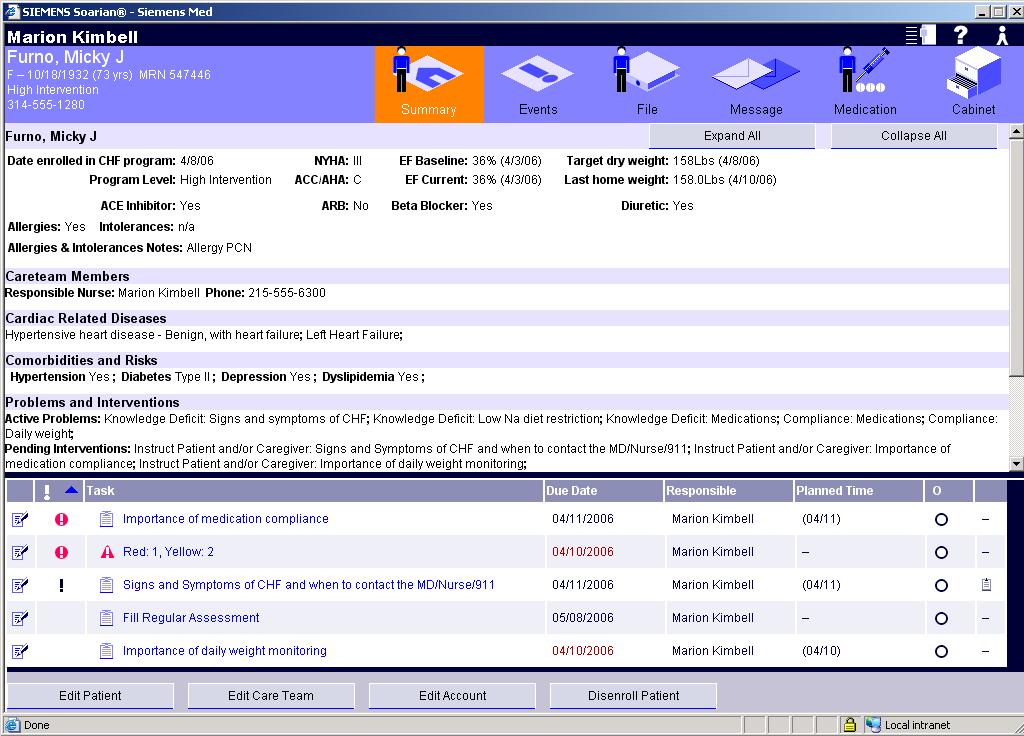
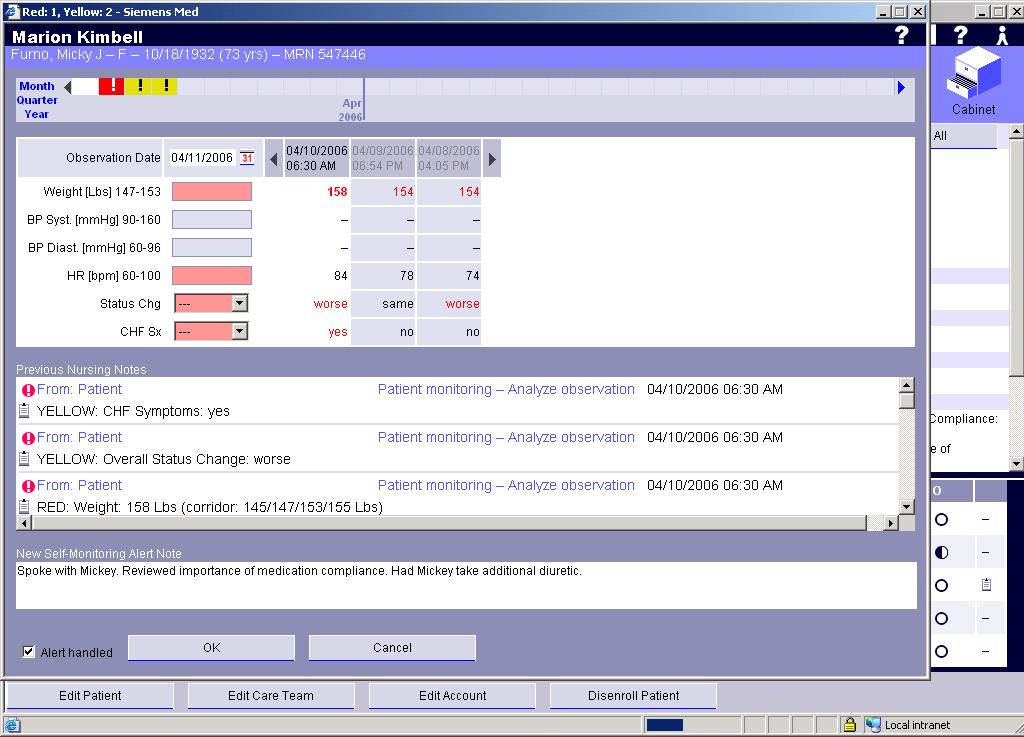
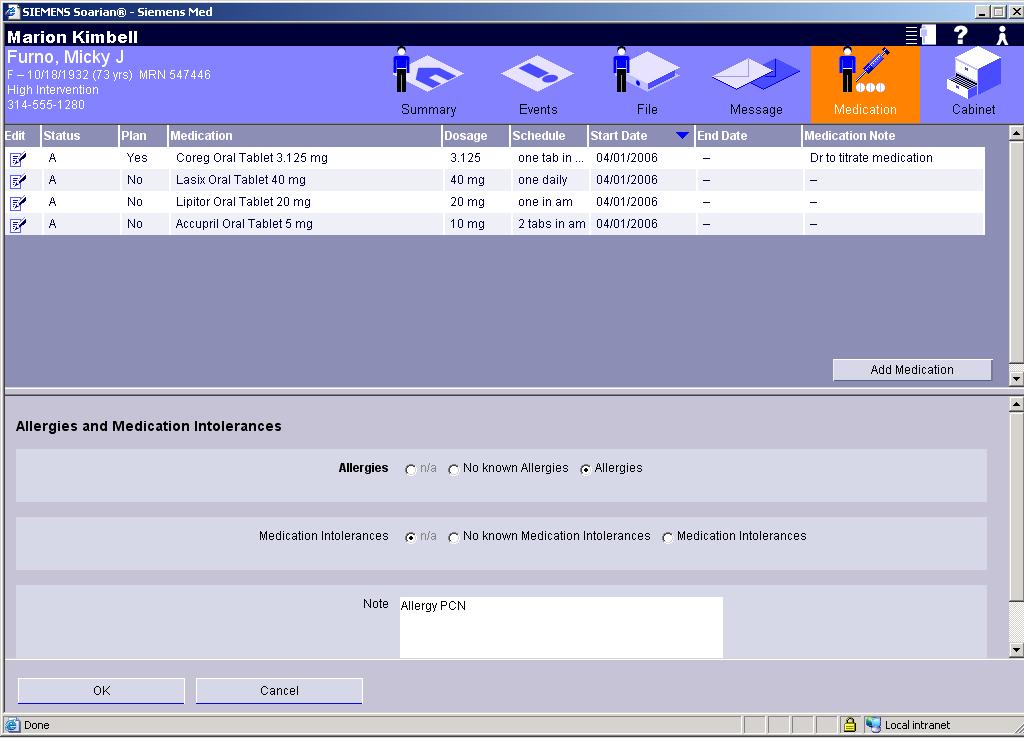
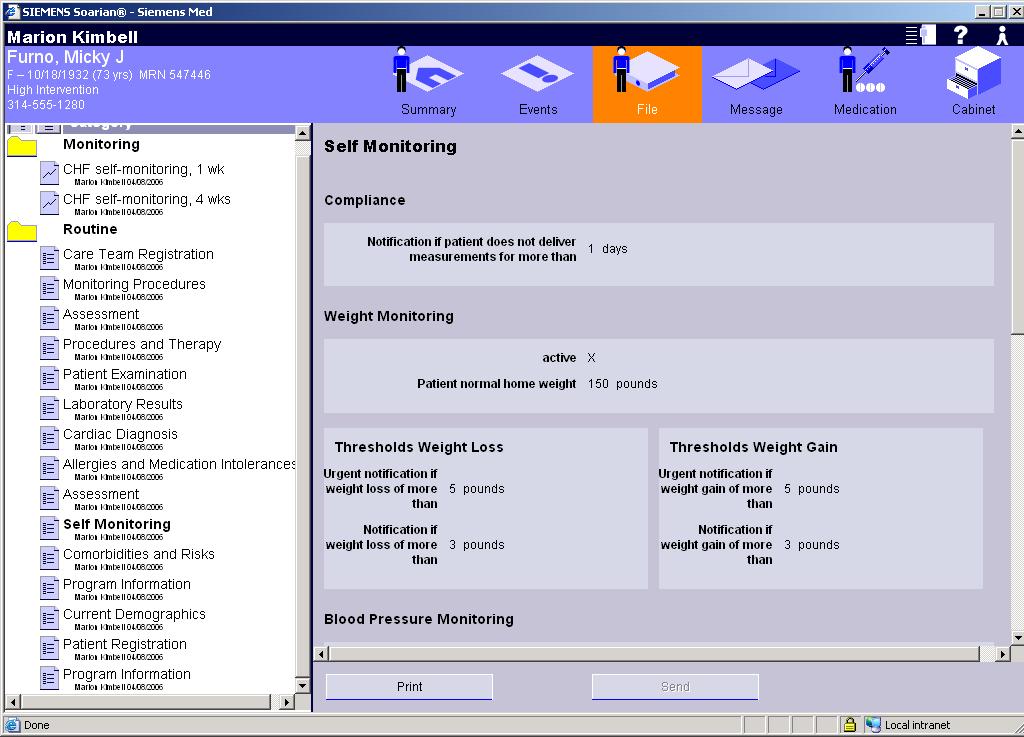
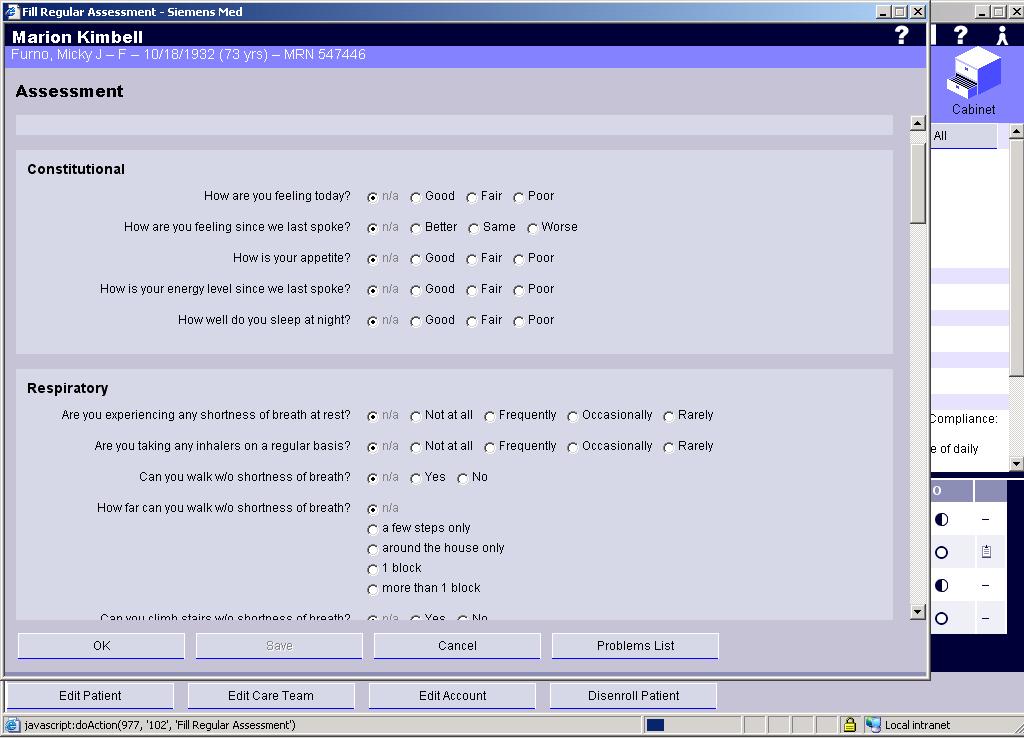
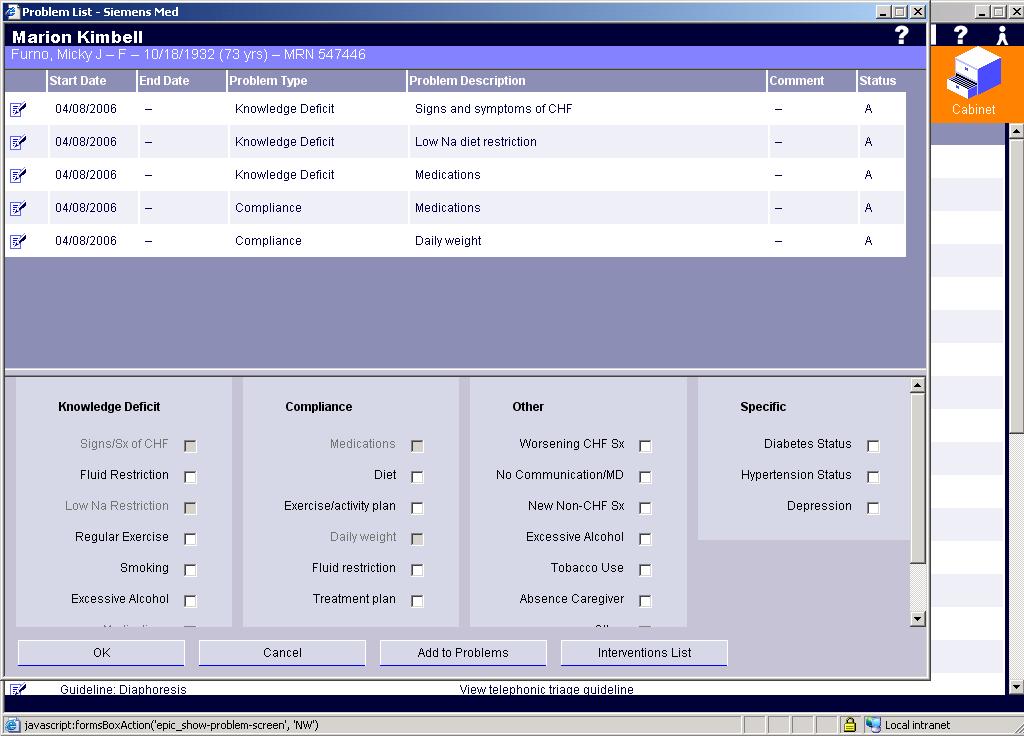
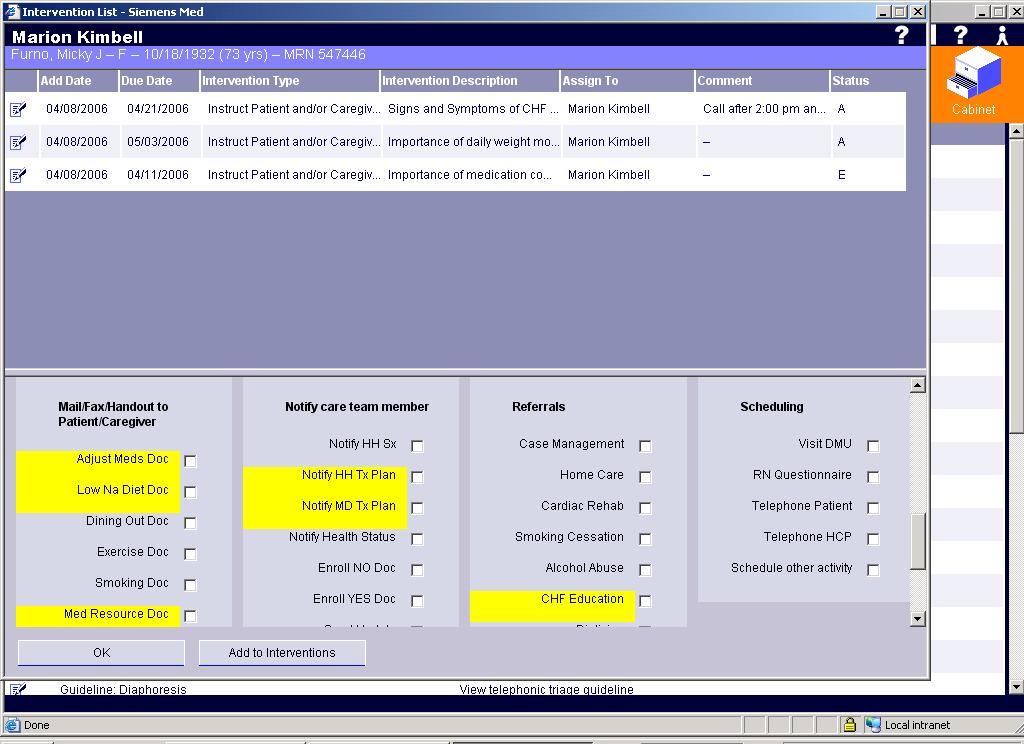
20 20 Soarian Disease Management Patient self monitoring via Interactive Voice Response Customizable notifications/reminders Patient compliance tracking Problems and interventions checklist Telephonic nursing assessments
21 21
22 22
23 23
24 24
25 25
26 26
27 27
28 28
29 29
30 30
31 31 Potential Impact of Disease Management Programs Reduce Negative Financial Impact of treating chronic ill patients by reducing Admission LOS and ER visits Optimize Resources by freeing up valuable resources for higher reimbursable procedures Improve Quality of Care by delivering better care to at risk patients Revenue Quality Efficiency Improve Patient Affinity by keeping valuable patients tied to your organization Prepare for Future Revenue anticipate reimbursement for disease management services (CMS)
32 Questions? 32
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Cutting Avoidable Readmissions Starts in the Emergency Department
 WHITE PAPER Cutting Avoidable Readmissions Starts in the Emergency Department SMARTER EMERGENCY CARE: EVERYWHERE, EVERY TIME. Our experience and innovative approach offers smarter solutions for emergency
WHITE PAPER Cutting Avoidable Readmissions Starts in the Emergency Department SMARTER EMERGENCY CARE: EVERYWHERE, EVERY TIME. Our experience and innovative approach offers smarter solutions for emergency
Consumer ehealth Affinity Group
 Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair
 William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair What are the revenue streams What are the expenses How does the hospital
William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair What are the revenue streams What are the expenses How does the hospital
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting
 Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of
 2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
Webinar. Reducing Readmissions with BI and Analytics. 23 March 2018 Copyright 2016 AAJ Technologies All rights reserved.
 Webinar Reducing Readmissions with BI and Analytics Copyright Reducing 2016 Readmissions AAJ Technologies with BI and All rights Analytics reserved. www.aajtech.com Hospital Readmissions Michele Russell,
Webinar Reducing Readmissions with BI and Analytics Copyright Reducing 2016 Readmissions AAJ Technologies with BI and All rights Analytics reserved. www.aajtech.com Hospital Readmissions Michele Russell,
Personalized Primary Care Annual Meeting. Care Management Catherine Hamilton, BSN, MS, MBA
 Personalized Primary Care Annual Meeting Care Management Catherine Hamilton, BSN, MS, MBA Care Manager Assessments 75% of care managers assessed Observed processes Evaluated against NCQA 2014 Medical Home
Personalized Primary Care Annual Meeting Care Management Catherine Hamilton, BSN, MS, MBA Care Manager Assessments 75% of care managers assessed Observed processes Evaluated against NCQA 2014 Medical Home
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Priceless Partners: Common Patients, Common Goals
 Priceless Partners: Common Patients, Common Goals Erin Hodson, RN, BSN, ACM Senior Director Case Management Inova Fairfax Hospital Pamela Andrews, RN, MSW, MBA, CCM, ACM Director Medical Management INTotal
Priceless Partners: Common Patients, Common Goals Erin Hodson, RN, BSN, ACM Senior Director Case Management Inova Fairfax Hospital Pamela Andrews, RN, MSW, MBA, CCM, ACM Director Medical Management INTotal
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study
 Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Programs and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance Program
 s and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance HealthPartners Disease and Case Management programs are targeted to those who have been identified with a
s and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance HealthPartners Disease and Case Management programs are targeted to those who have been identified with a
UTILIZATION MANAGEMENT AND CARE COORDINATION Section 8
 Overview The focus of WellCare s Utilization Management (UM) Program is to provide members access to quality care and to monitor the appropriate utilization of services. WellCare s UM Program has five
Overview The focus of WellCare s Utilization Management (UM) Program is to provide members access to quality care and to monitor the appropriate utilization of services. WellCare s UM Program has five
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Pay-for-Performance. GNYHA Engineering Quality Improvement
 Pay-for-Performance GNYHA Engineering Quality Improvement The Writing Is On The Wall IOM Report - Rewarding Provider Performance: Aligning Incentives In Medicare 9/21/06 Medicare P4P and quality improvement
Pay-for-Performance GNYHA Engineering Quality Improvement The Writing Is On The Wall IOM Report - Rewarding Provider Performance: Aligning Incentives In Medicare 9/21/06 Medicare P4P and quality improvement
Preventing Avoidable Readmissions Together: Improving Discharge Summaries. R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC
 Preventing Avoidable Readmissions Together: Improving Discharge Summaries R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC Today s Objectives Identify elements of a complete discharge summary
Preventing Avoidable Readmissions Together: Improving Discharge Summaries R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC Today s Objectives Identify elements of a complete discharge summary
An Integrated Approach to Heart Failure Care. Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN
 An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
The Chester County Hospital Staff Informatics Council Meeting Minutes
 Present: See Attendance Sheet Chair: Kathy Zopf-Herling, MSN, RN- BC and Lindsay Pritchett, BSN, RN, CMSRN Date: 09/17/2013 Time 7:00 AM to 11:00 AM Location: Building 606 Training Room A Absent: Recorder:
Present: See Attendance Sheet Chair: Kathy Zopf-Herling, MSN, RN- BC and Lindsay Pritchett, BSN, RN, CMSRN Date: 09/17/2013 Time 7:00 AM to 11:00 AM Location: Building 606 Training Room A Absent: Recorder:
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
The In and Out of the Medicare Two Midnight Rule. Disclaimer. Objectives 3/31/2014
 The In and Out of the Medicare Two Midnight Rule Brenda Keeling, RN, CPHQ, CCM Patient Response, Inc. 1 Disclaimer Information enclosed was current at the time it was presented. Medicare policy changes
The In and Out of the Medicare Two Midnight Rule Brenda Keeling, RN, CPHQ, CCM Patient Response, Inc. 1 Disclaimer Information enclosed was current at the time it was presented. Medicare policy changes
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012
 Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Illinois Department of Public Health Critical Access Hospital Program Certification Process Preparation
 Illinois Department of Public Health Critical Access Hospital Program Certification Process Preparation Overview of the process The Critical Access Hospital (CAH) program is an opportunity for rural hospitals
Illinois Department of Public Health Critical Access Hospital Program Certification Process Preparation Overview of the process The Critical Access Hospital (CAH) program is an opportunity for rural hospitals
Emerging Strategies for Improving Hospital Medicine
 Emerging Strategies for Improving Hospital Medicine Improving efficiency, patient safety, metrics and satisfaction Improving communication among the patient s community of caregivers Your Presenters Francisco
Emerging Strategies for Improving Hospital Medicine Improving efficiency, patient safety, metrics and satisfaction Improving communication among the patient s community of caregivers Your Presenters Francisco
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers
 Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Readmission Reduction and the ACO
 Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
Sandra Robinson, RN, MSN, ACM, CEN
 Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Retrospective Bundles
 Bundled Payment for Care Improvement (BPCI) Overview Shawn Matheson MBA, LNHA, FACHCA Market Manager Idaho Health Care Association Annual Convention Boise, ID July 13, 2017 Retrospective Bundles Surgeon
Bundled Payment for Care Improvement (BPCI) Overview Shawn Matheson MBA, LNHA, FACHCA Market Manager Idaho Health Care Association Annual Convention Boise, ID July 13, 2017 Retrospective Bundles Surgeon
Hot Spotter Report User Guide
 PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
Learning Objectives. CDI Counts: Metrics for the CDI Professional. At the completion of this educational activity, the learner will be able to:
 1 CDI Counts: Metrics for the CDI Professional Rani Stoddard, MBA, RN, RHIT, CPHQ, CPHQ, RHIT, CCDS, C CDI CDI Supervisor Henry Mayo Newhall Hospital Valencia, CA Learning Objectives At the completion
1 CDI Counts: Metrics for the CDI Professional Rani Stoddard, MBA, RN, RHIT, CPHQ, CPHQ, RHIT, CCDS, C CDI CDI Supervisor Henry Mayo Newhall Hospital Valencia, CA Learning Objectives At the completion
CMS Quality Program- Outcome Measures. Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018
 CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Caring for the Whole Patient Predictive Analytics Technology, Socio-demographic Insights, and Improved Patient Outcomes Randy K.
 WHITE PAPER Caring for the Whole Patient Randy K. Hawkins, MD Caring for the Whole Patient Socio-demographic data, not normally present in the electronic health record, and not routinely found in the hands
WHITE PAPER Caring for the Whole Patient Randy K. Hawkins, MD Caring for the Whole Patient Socio-demographic data, not normally present in the electronic health record, and not routinely found in the hands
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017
 Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
at OU Medicine Leadership Development Institute August 6, 2010
 Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Basic Utilization and Case Management
 & CHAPTER 7 Basic Utilization and Case Management I Bartlett CHAPTER Learning, STUDY LLC REVIEW 1. Goal of utilization management is to see that each member receives the appropriate level of care at an
& CHAPTER 7 Basic Utilization and Case Management I Bartlett CHAPTER Learning, STUDY LLC REVIEW 1. Goal of utilization management is to see that each member receives the appropriate level of care at an
6.6 million. 3,400+ physicians & scientists. Cleveland Clinic bundled payment program key learnings
 If you are considering implementing or expanding a bundled payment program, the Cleveland Clinic offers four key learnings. When Cleveland Clinic sought to develop a way to automate bundled payments around
If you are considering implementing or expanding a bundled payment program, the Cleveland Clinic offers four key learnings. When Cleveland Clinic sought to develop a way to automate bundled payments around
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Improving Heart Failure Outcomes through Interactive Patient Care: The Sentara Virginia Beach General Hospital Experience
 WHITE PAPER Improving Heart Failure Outcomes through Interactive Patient Care: The Sentara Virginia Beach General Hospital Experience 06.05.09 executive summary In the United States, Heart Failure has
WHITE PAPER Improving Heart Failure Outcomes through Interactive Patient Care: The Sentara Virginia Beach General Hospital Experience 06.05.09 executive summary In the United States, Heart Failure has
Referrals, Prior Authorizations, Medical Management, and Appeals
 Referrals, Prior Authorizations, Medical Management, and Appeals 1 An Independent Licensee of the Blue Cross Blue Shield Association 044506 (12-21-2017) 2017 Premera. Proprietary and Confidential. Referrals
Referrals, Prior Authorizations, Medical Management, and Appeals 1 An Independent Licensee of the Blue Cross Blue Shield Association 044506 (12-21-2017) 2017 Premera. Proprietary and Confidential. Referrals
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Case managers are consummate team players, working with. IssueBrief
 IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
The Nexus of Quality and Finance
 The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
8/31/2015. Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success. Vanderbilt University Medical Center
 Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
Health Reform and IRFs
 American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Disease Management at Anthem West Or: what have we learned in trying to design these programs?
 Disease Management at Anthem West Or: what have we learned in trying to design these programs? Lisa M. Latts, MD, MSPH Regional Medical Director May 12, 2003 Anthem Inc. Anthem Inc. Headquarters: Indianapolis
Disease Management at Anthem West Or: what have we learned in trying to design these programs? Lisa M. Latts, MD, MSPH Regional Medical Director May 12, 2003 Anthem Inc. Anthem Inc. Headquarters: Indianapolis
Quality, Cost and Business Intelligence in Healthcare
 Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING
 HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM
 THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
Mercy Virtual. Transforming Medicine and Value Through Virtual Care. Randall S Moore, MD, MBA. Orlando, FL. September, 2017
 Mercy Virtual Transforming Medicine and Value Through Virtual Care Randall S Moore, MD, MBA Orlando, FL September, 2017 The opinions expressed are those of the presenter and do not necessarily state or
Mercy Virtual Transforming Medicine and Value Through Virtual Care Randall S Moore, MD, MBA Orlando, FL September, 2017 The opinions expressed are those of the presenter and do not necessarily state or
Best Practices: Access Case Management
 Best Practices: Access Case Management Sarah M. Clark, RN-BC, BSN, MHA/INF, CCM Manager, Care Coordination Education Sentara Healthcare August 15, 2013 1 Objectives Identify key components of an effective
Best Practices: Access Case Management Sarah M. Clark, RN-BC, BSN, MHA/INF, CCM Manager, Care Coordination Education Sentara Healthcare August 15, 2013 1 Objectives Identify key components of an effective
2017 State of Consumer Telehealth: Insights from Hospital Executives
 2017 State of Consumer Telehealth: Insights from Hospital Executives #BeckersHR18 May 15, 2018 1 Presenter / Agenda 1 About Teladoc 2 Survey Overview 3 Key Findings 4 Success Factors Alan Roga, MD, FACEP
2017 State of Consumer Telehealth: Insights from Hospital Executives #BeckersHR18 May 15, 2018 1 Presenter / Agenda 1 About Teladoc 2 Survey Overview 3 Key Findings 4 Success Factors Alan Roga, MD, FACEP
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
Buchanan, 1996; Knaus, Felton, Burton, Fobes, & Davis 1997, J. of Nsg Administration
 Can Patients with Moderate to High Risk Acute Coronary Syndromes Be Cared For safely in a Cardiac Acute Care Unit (ACU) Introduction Several studies have evaluated the safety of managing g patient with
Can Patients with Moderate to High Risk Acute Coronary Syndromes Be Cared For safely in a Cardiac Acute Care Unit (ACU) Introduction Several studies have evaluated the safety of managing g patient with
Changing Paradigm of Cardiovascular Care- Service Line vs Departmental
 Changing Paradigm of Cardiovascular Care- Service Line vs Departmental Michael A. Acker, MD William Measey Professor of Surgery Chief of Cardiovascular Surgery Director of Penn Medicine Heart and Vascular
Changing Paradigm of Cardiovascular Care- Service Line vs Departmental Michael A. Acker, MD William Measey Professor of Surgery Chief of Cardiovascular Surgery Director of Penn Medicine Heart and Vascular
NOTE: New Hampshire rules, to
 NOTE: New Hampshire rules, 309.01 to 309.08 Email Request: Selected Items in Table of Contents: (8) Time Of Request: Sunday, August 07, 2011 18:11:07 EST Send To: MEGADEAL, ACADEMIC UNIVERSE UNIVERSITY
NOTE: New Hampshire rules, 309.01 to 309.08 Email Request: Selected Items in Table of Contents: (8) Time Of Request: Sunday, August 07, 2011 18:11:07 EST Send To: MEGADEAL, ACADEMIC UNIVERSE UNIVERSITY
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Improving Care Transitions
 Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Molina Healthcare Michigan Health Care Services Department Phone: (855) Fax: (800)
 Fax: (800)") Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Select Medical TRANSITIONS OF CARE & CARE COORDINATION
 Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
from 7 to 9 and Mira Room 9 to 11
 Minutes Purpose Attendees Meeting Time Meeting Location The Chester County Hospital Staff Informatics Council April 17, 2012 To discuss Informatics related issues: new functionality, revisions and patient
Minutes Purpose Attendees Meeting Time Meeting Location The Chester County Hospital Staff Informatics Council April 17, 2012 To discuss Informatics related issues: new functionality, revisions and patient
Minnesota Statewide Quality Reporting and Measurement System: APPENDICES TO MINNESOTA ADMINISTRATIVE RULES, CHAPTER 4654
 Minnesota Statewide Quality Reporting and Measurement System: APPENDICES TO MINNESOTA ADMINISTRATIVE RULES, CHAPTER 4654 DECEMBER 2017 APPENDICES TO MINNESOTA ADMINISTRATIVE RULES, CHAPTER 4654 Minnesota
Minnesota Statewide Quality Reporting and Measurement System: APPENDICES TO MINNESOTA ADMINISTRATIVE RULES, CHAPTER 4654 DECEMBER 2017 APPENDICES TO MINNESOTA ADMINISTRATIVE RULES, CHAPTER 4654 Minnesota
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Linking Supply Chain, Patient Safety and Clinical Outcomes
 Premier s Vision for High Performing Healthcare Organizations: Linking Supply Chain, Patient Safety and Clinical Outcomes Joe M. Pleasant Sr. VP and CIO Premier Inc. Global GS1 Conference Hong Kong October
Premier s Vision for High Performing Healthcare Organizations: Linking Supply Chain, Patient Safety and Clinical Outcomes Joe M. Pleasant Sr. VP and CIO Premier Inc. Global GS1 Conference Hong Kong October
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
Unifying Real-Time Mobile Rounds with Follow Up Care Calls to Improve Patient Experience and Outcomes
 Unifying Real-Time Mobile Rounds with Follow Up Care Calls to Improve Patient Experience and Outcomes Sue Murphy, RN BSN MS Chief Experience Officer Becker's 3rd Annual Health IT + Revenue Cycle 2017 1
Unifying Real-Time Mobile Rounds with Follow Up Care Calls to Improve Patient Experience and Outcomes Sue Murphy, RN BSN MS Chief Experience Officer Becker's 3rd Annual Health IT + Revenue Cycle 2017 1