Transition hôpital-domicile: Risques et opportunités! Pr Martine LOUIS SIMONET Formation Continue Médecins de Famille Genève 14 avril 2016
|
|
|
- Melissa Walters
- 6 years ago
- Views:
Transcription



1 Transition hôpital-domicile: Risques et opportunités! Pr Martine LOUIS SIMONET Formation Continue Médecins de Famille Genève 14 avril 2016
2 Transitional care is defined as a set of actions designed to ensure the coordination and continuity of health care as patients transfer between different locations or different levels of care within the same location. Les soins de transition sont définis comme un ensemble d actions visant à assurer la coordination et continuité des soins lorsqu un patient est transféré entre différents lieux ou différents niveaux de soins dans le même lieu. Coleman, J Am Geriatr Soc, 2003 Position Statement of the American Geriatrics Society Health Care Systems Committee
3 Health professionals Physicians Hospital-based Primary care Specialists Communication Collaboration Hospital care Emergency Acute care Rehabilitation Setting Nurses Nurse s aides Patient Home care Community care Other Physiotherapists Occupational therapists Nursing homes
4 Health professionals Physicians Hospital-based Primary care Specialists Communication Collaboration Hospital care Emergency Acute care Rehabilitation Setting Nurses Nurse s aides Patient Home care Community care Other Physiotherapists Occupational therapists Nursing homes
5 Transition from hospital to home IT MATTERS Increasingly recognized as a time of heightened vulnerability in safety and quality of patient care It is a process and not a unique procedure with increasingly recognized lapses in the key stages of the discharge process Improvements are definitely needed and feasible It is a real challenge for acute care services AND IT IS EXCITING!!!
6 Transition from hospital to home Forster et al. Ann Intern Med 2003; CMAJ 2004; J Gen Intern Med 2005 Adverse events in the 5 weeks following hospital discharge 1 patient out 5 (20%) 70% are due to medication Higher risk if: Treatment changes in the hospital High number of medications No knowledge of side effects High-risk class: antibiotics, cardiovascular, anticoagulants, corticosteroids, analgesics 62% preventable or ameliorable.
7 Transition from hospital to home Forster et al. Ann Intern Med 2003; CMAJ 2004; J Gen Intern Med 2005; Jenks et al.n Engl J Med 2009 Consequences on both health and costs Additional medical consultation 21% Emergency consultation 12% Readmission (30 days; 90 days) 20%; 30% $12 billion!!! Patients/caregiver satisfaction
8 Transition from hospital to home Forster et al. Ann Intern Med 2003; CMAJ 2004; J Gen Intern Med 2005; Jenks et al.n Engl J Med 2009 Ineffective communication/information transfer of critical elements of the care plan Patient-caregivers/practitioner/home health services Ineffective anticipation, planification, preparation Health professionals and coordination of the care plan Communication Physicians Primary care Specialists Collaboration Hospital care Emergency Acute care Rehabilitation Setting Nurses Nurse s aides Patient Home care Community care Other Physiotherapists Occupational therapists Nursing homes
9 Transition from hospital to home Forster et al. Ann Intern Med 2003; CMAJ 2004; J Gen Intern Med 2005; Jenks et al.n Engl J Med 2009 Ineffective communication/information transfer of critical elements of the care plan Ineffective anticipation, planification and coordination of the care plan Health professionals Communication Setting Nurses Nurse s aides Physicians Primary care Specialists Collaboration Patient Hospital care Emergency Acute care Rehabilitation Home care Community care Other Physiotherapists Occupational therapists Nursing homes
10 Deficits in communication between hospital-based and primary care physicians JAMA. 2007;297: Item Direct communication between hospital and primary care physicians Availability of a discharge summary at the first postdischarge visit at 4 weeks Discharge summary quality, lack of: diagnostic test results treatment or hospital course discharge medications Test results pending at discharge patient or family counseling follow-up plans Proportion 3%-20% 12%-34% 51%-77% 33%-63% 7%-22% 2%-40% 65% 90%-92% 2%-43%

11 Deficits in communication between hospital-based physicians and patients HUG-patient satisfaction questionnaire 2014 Information/explanation No/few At discharge Reason of medications 18% Adverse/side effects 32% Precautions/alerts to be aware of 44% When to resume normal activity 43% Well organized discharge 29%
12 Deficits in communication between hospital-based physicians and patients Forster et al. Ann Intern Med 2003; CMAJ 2004; J Gen Intern Med 2005; Jenks et al.n Engl J Med 2009 Low adherence to treatment: Errors in dosage, quantity, time.. Unintentional or intentional discharge medication discontinuation Spontaneous introduction of new medication Resuming previous treatment Duplication of medications Risk Low health literacy, cognitive deficits, self-efficacy Coleman; Arch Intern Med 2005;Am J Med Qual 2013
13 Causes: Transition from hospital to home Forster et al. Ann Intern Med 2003; CMAJ 2004; J Gen Intern Med 2005; Jenks et al.n Engl J Med 2009 Ineffective communication/information of critical elements of the care plan Ineffective anticipation, planification and Health professionals coordination of the care plan Physicians Primary care Specialists Communication Collaboration Hospital care Emergency Acute care Rehabilitation Setting Nurses Nurse s aides Patient Home care Community care Other Physiotherapists Occupational therapists Nursing homes
14 Ineffective anticipation and planification Chopard et al, Int J Epidemiol Inappropriate hospital days (AEP protocol) 35% of hospital days of which 50% related to the discharge process Awaiting for post-acute care facilities (50%) Medical indecision; Absence of the care plan; Patient and caregiver poorly informed; Awaiting for discharge organisation Risk if: Inappropriate admission > 80 years; comorbidities++
15 Transition from hospital to home How to improve? Health professionals Communication Setting Nurses Nurse s aides Physicians Primary care Specialists Collaboration Patient Hospital care Emergency Acute care Rehabilitation Home care Community care Other Physiotherapists Occupational therapists Nursing homes

16 Recommendations for improving care transitions at hospital discharge J Hosp Med 2007;2:
17 How to improve? J Hosp Med 2007;2: Ineffective communication/information transfer Educate and train students and physicians for effective communication Educate and inform patients and caregivers Inpatient-outpatient physician continuity Medication reconciliation Ineffective anticipation, planification and coordination Early identification of high risks patients Standardize the process and content of transitional care Involve all partners Improve instruments
18 How do we improve? Ineffective communication/information transfer Educate and train students and physicians for effective communication Educate and inform patients and caregivers Inpatient-outpatient physician continuity Medication reconciliation Ineffective anticipation, planification and coordination Early identification of high risks patients Standardize the process and content of transitional care Involve all partners Improve instruments
 Cinical")


19 Educate physicians and students Communication skills-based curriculum for effective communication Teaching Undergraduate Preclinical years (bachelor) Cinical compentencies 2 nd - 3 rde year Clinical years (master): 4 th 6 th year Issues Medical consultation Comprehensive repertoire of basic communication skills Patient-centered approach Postgraduate Residents SMIG Residents SMPR Complex settings Discharge interview Difficult physician-patient relationship Breaking bad news Conducting interview with families.


20 Educate the patient Precisions and precautions Reason for medication Side effects
 Results")

 Increased patient satisfaction (card very useful, 90%; used every day,")
21 Educate the patient Am J Med 2004;117:563-8 Intervention Structured patient-centered discharge interview (done by 73% of the residents) Results Increased Patient knowledge on: Reason for each medication Precautions to be observed Potential side effects Likelihood of the patient receiving information OR: 3.6 (95% IC: 1.5 à 4.4) Increased patient satisfaction (card very useful, 90%; used every day, 50%) Decreased Likelihood of patients interrupting their medication
22 How to improve? J Hosp Med 2007;2: Ineffective communication/information transfer Educate and train students and physicians for effective communication Educate and inform patients and caregivers Inpatient-outpatient physician continuity Medication reconciliation Ineffective anticipation, planification and coordination Early identification of high risks patients Standardize the process and content of transitional care Involve all partners Improve instruments
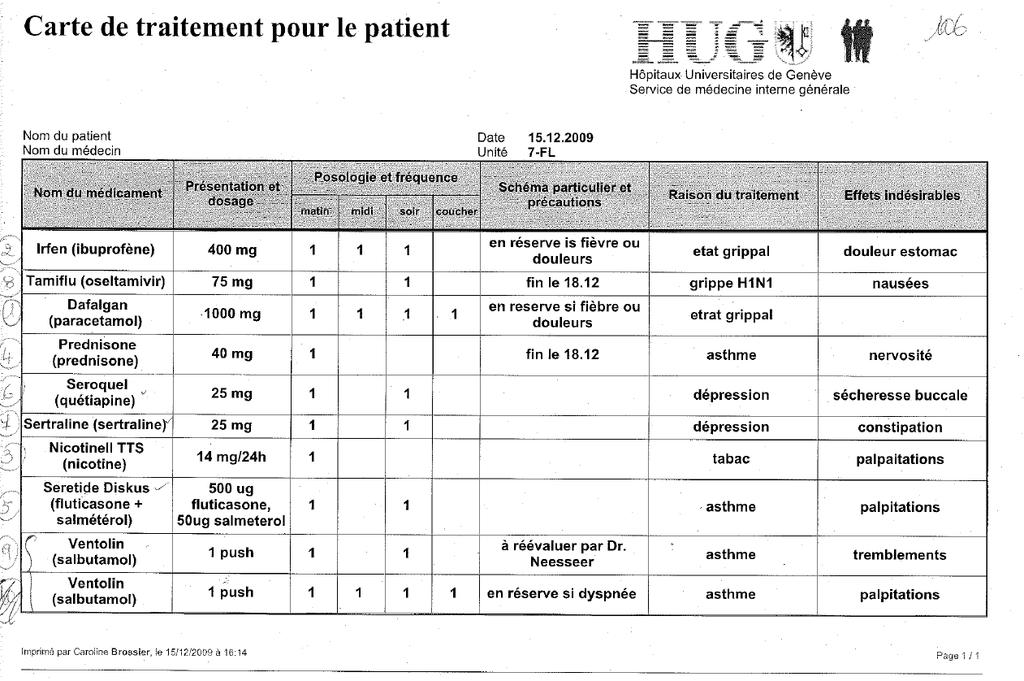
23 Medication reconciliation
 Deuxième clé nécessaire pour le prestataire de soins Données décentralisées Plan de traitement")
24 Dossier informatisé accessible Accès à tous les documents relevant pour la santé du patient Accès réglé par le patient (carte clé) Deuxième clé nécessaire pour le prestataire de soins Données décentralisées Plan de traitement partagé
25 Transition from hospital to home Forster et al. Ann Intern Med 2003; CMAJ 2004; J Gen Intern Med 2005; Jenks et al.n Engl J Med 2009 Ineffective communication/information of critical elements of the care plan Ineffective anticipation, planification and coordination of the care plan Health professionals Communication Setting How do we improve? Nurses Nurse s aides Physicians Primary care Specialists Collaboration Patient Hospital care Emergency Acute care Rehabilitation Home care Community care Other Physiotherapists Occupational therapists Nursing homes
26 Ineffective anticipation, planification and coordination of the care plan Early identification of high risk patients Predictive score Standardize the process and content of transitional care (involving all partners and improving instruments) Institutional quality improvement project («P9»..!) Health professionals Communication Setting Nurses Nurse s aides Physicians Primary care Specialists Collaboration Patient Hospital care Emergency Acute care Rehabilitation Home care Community care Other Physiotherapists Occupational therapists Nursing homes
 Nohelp provided by spouse/partner +4 Inability in medication self management +4 before")

27 BMC Health Services Research 2008, 8:154 > 8 points Sensibility 87% Specificity 63% Variable Point score Active medical problems +1 (per additional problem) Nohelp provided by spouse/partner +4 Inability in medication self management +4 before admission Dependent for transfers bed/chair on Day 3 +4 Dependent for bath / shower on Day 3 +4 Sensitivity points 1point 16 points Specificity Derivation cohort ROC area: 0.82 Validation cohort ROC area: 0.77
28 Validation of the Day 3-score in an other cohort Tertiary swiss hospital (Aarau) A Conca, A Gabele, Philipp Schuetz, M.Louis Simonet et al, 2015 submitted 1432 medical patients Day 3-Score Sensitivity Specificity AUC 0.82 Area under ROC curve = Cut-off > 8pts Sensitivity 84% Specificity 70%


29 Early identification of high risk patients M.Louis Simonet et al, BMC Health Services Research 2008 Intervention J3- Score SCORE Points Evaluation Number of active medical problems on admission No help provided by spouse +4 Inability in medication self management before admission +4 Dependency in bathing/shower on Day 3 +4 Dependency in transfers (bed/chair) on Day 3 +4 Day3 : Contact social worker Contact Date :. If any dependency, initiate mobilization physical therapy Request date Reminder Score 8 points This document must be kept in patient's chart 1pt/problem Total Consider home return? Score 8-15 points : (60% probability of home return) Early implementation of measures likely to reinforce the success of home return Score 16 points : (20% probability of home return) Early transfer planning to a post-acute care facility Yes No Patient's Identity Planned discharge date :.. Implemented measures :... Early transfer planning to a post-acute care facility PACF (name) :... Date of earliest possible transfer Application form completed on date :.. D5/D7/D9 : Planning reassessment : Date/Decisions : Results Decreased (patients score >8 pts) Length of stay (3.2) Inappropriate days (1.57) Inapropriate day due to discharge delays (1) Not increased Patients tranfer to a post-acute care facilities
30 Ineffective anticipation, planification and coordination of the care plan Early identification of high risk patients Predictive score Standardize the process and content of transitional care (involving all partners and improving instruments) Institutional quality improvement project (P9) Health professionals Communication Setting Nurses Nurse s aides Physicians Primary care Specialists Collaboration Patient Hospital care Emergency Acute care Rehabilitation Home care Community care Other Physiotherapists Occupational therapists Nursing homes
 and key informations necessary for the good progress Roles and responsibilities of each of the actors at every stage of the process Discharge essential")
31 Standardize content and process HUG- Institutional Project: Improvement of discharge preparation and anticipation Identification, definition and structuration of the process Key phases (admission, during hospitalisation, before/at discharge) and key informations necessary for the good progress Roles and responsibilities of each of the actors at every stage of the process Discharge essential communicating documents necessary for transitional care; their contents; when and to whom Development Standardized protocol allowing to start early the process (alerts), to follow it and to document it by all the involved actors Protocol integrated in the informatised medical record


32 Discharge planning protocol-admission Groupe P9 : Amélioration et anticipation de la sortie

33 Discharge planning protocol Discharge check list
34 34
35 Summary Transition from hospital to home (and vice-versa ) is a delicate and particularly vulnerable period, especially for elderly patients and/or with many comorbidities
36 Summary To improve Continuity and Coordination of care Hospitals must implement standardized discharge procedures to ensure Patients effective information and education at discharge (verbal, written) Patient s discharge at an appropriate time, with adequates notices; care needs met and organised Accurate, relevant and timely delivery of discharge informations to community care provider Medication reconciliation
37 To change the culture Summary Discharge planning and procedures should be integrated in the daily hospital care and start on admission Hospitals and Faculty must design and implement curricula for physicians and students to develop essential skills in transition care Effective communication Effective handovers Strong political, institutional and faculty will is now necessary to make it a definite priority objective
38 Summary Low level of evidence of effectiveness in improving patient outcomes Evaluation direly needed!!

39
40 Backup
41 Transition from hospital to home Evaluation Interventions Information/Communication Coordination Heterogeneity Multicomponents Non standardized Issues System-based outcomes Hospital use Readmission, LOS,.. Continuity of care Medication reconciliation Time discharge summary Primary care use Patient-centered outcomes Mortality Functional status Quality of life Satisfaction Caregiver burden

42 Changing the culture


43 Discharge planning protocol-admission Groupe P9 : Amélioration et anticipation de la sortie -

44
45 Réconciliation médicamenteuse Rôle des pharmaciens Outils informatiques
46 Dossier informatisé accessible Accès à tous les documents relevant pour la santé du patient Accès réglé par le patient (carte clé) Deuxième clé nécessaire pour le prestataire de soins Données décentralisées Connexion hautement sécurisée
Medication Reconciliation (MedRec)
") Session 6 Medication Reconciliation (MedRec) Rachel Pham, Hôpital Molière-Longchamps (HIS) Stephane Steurbaut, UZ Brussel 1. OBJECTIVES 2. «MEDREC» DEFINITION 3. HOW TO START A PROJECT? Session Plan 4.
Session 6 Medication Reconciliation (MedRec) Rachel Pham, Hôpital Molière-Longchamps (HIS) Stephane Steurbaut, UZ Brussel 1. OBJECTIVES 2. «MEDREC» DEFINITION 3. HOW TO START A PROJECT? Session Plan 4.
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: An opportunity to improve care, experience and reduce waste
 Transitions of Care: An opportunity to improve care, experience and reduce waste Dr. Paresh Dawda, Visiting Fellow, Australian Primary Health Care Research Institute, ANU Adjunct Associate Professor, University
Transitions of Care: An opportunity to improve care, experience and reduce waste Dr. Paresh Dawda, Visiting Fellow, Australian Primary Health Care Research Institute, ANU Adjunct Associate Professor, University
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE. By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012
 PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012 2 INTRODUCTION Who am I? Physician Assistant student Towson/CCBC
PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012 2 INTRODUCTION Who am I? Physician Assistant student Towson/CCBC
Improving Sign-Outs in Hospital Medicine
 Improving Sign-Outs in Hospital Medicine Arpana R. Vidyarthi, MD Assistant Professor of Medicine Division of Hospital Medicine Director of Quality, Division of Hospital Medicine Director, Patient Safety
Improving Sign-Outs in Hospital Medicine Arpana R. Vidyarthi, MD Assistant Professor of Medicine Division of Hospital Medicine Director of Quality, Division of Hospital Medicine Director, Patient Safety
Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Medication Reconciliation for Older Adults Transitioning from. Long-Term Care to Home. Allison (Leverett) Kackman
 Kackman") Medication Reconciliation for Older Adults Transitioning from Long-Term Care to Home By Allison (Leverett) Kackman Washington State University Spokane. Riverpoint campus Ubrary P.O. Box 1495 Spokane, WA
Medication Reconciliation for Older Adults Transitioning from Long-Term Care to Home By Allison (Leverett) Kackman Washington State University Spokane. Riverpoint campus Ubrary P.O. Box 1495 Spokane, WA
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
Adverse Drug Events and Readmissions: The Global Picture
 Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
The Heart of Care Redesign; Care Protocols. Paul N. Casale, MD, FACC Chief, Division of Cardiology Lancaster General Health
 The Heart of Care Redesign; Care Protocols Paul N. Casale, MD, FACC Chief, Division of Cardiology Lancaster General Health Lancaster General Health By the Numbers (Fiscal Year 2012) Beds: 631 in service
The Heart of Care Redesign; Care Protocols Paul N. Casale, MD, FACC Chief, Division of Cardiology Lancaster General Health Lancaster General Health By the Numbers (Fiscal Year 2012) Beds: 631 in service
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
Medication Management: Therapy Scope Versus Comfort Level
 Medication Management: Therapy Scope Versus Comfort Level Presented By: Cindy Krafft MS PT President Home Health Section APTA Director of Rehabilitation Consulting Services August 17, 2011 243 King Street,
Medication Management: Therapy Scope Versus Comfort Level Presented By: Cindy Krafft MS PT President Home Health Section APTA Director of Rehabilitation Consulting Services August 17, 2011 243 King Street,
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Objectives. Prevalence of Non-Adherence. Medications and Care Transitions. The Cost of Readmissions. The Pharmacist s Role in Improving Care 4/22/2015
 MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Direction du médicament. Sylvie Bouchard Director
 Direction du médicament Sylvie Bouchard Director South America mission 28 November 2016 Aim of the presentation To present INESSS s mandates with regard to medication To explain the Régime d assurance
Direction du médicament Sylvie Bouchard Director South America mission 28 November 2016 Aim of the presentation To present INESSS s mandates with regard to medication To explain the Régime d assurance
Rapid Recovery Therapy Program. GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen
 Rapid Recovery Therapy Program GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen $1 Million Photo credit: Physi-med.org Agenda About the Program Description of the Rapid Recovery Therapy
Rapid Recovery Therapy Program GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen $1 Million Photo credit: Physi-med.org Agenda About the Program Description of the Rapid Recovery Therapy
Karen Stasium, BS, MPT, COS C, HCS D
 Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Processing Enrolment/Consent Forms Reference Manual. For Primary Care Groups
 Processing Enrolment/Consent Forms Reference Manual For Primary Care Groups Ministry of Health and Long-Term Care Registration and Claims Branch April 2011 Version 1.4 Table of Contents Introduction...Intro-1
Processing Enrolment/Consent Forms Reference Manual For Primary Care Groups Ministry of Health and Long-Term Care Registration and Claims Branch April 2011 Version 1.4 Table of Contents Introduction...Intro-1
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
The impact of nighttime intensivists on medical intensive care unit infection-related indicators
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 The impact of nighttime intensivists on medical intensive care unit infection-related indicators Abhaya Trivedi
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 The impact of nighttime intensivists on medical intensive care unit infection-related indicators Abhaya Trivedi
Poor admission medication reconciliation can follow
 Importance of Medication Reconciliation in the Continuum of Care Cynthia R. Hennen, BS, RPh; and James A. Jorgenson, RPh, MS, FASHP Specialty Healthcare Benefits Council Poor admission medication reconciliation
Importance of Medication Reconciliation in the Continuum of Care Cynthia R. Hennen, BS, RPh; and James A. Jorgenson, RPh, MS, FASHP Specialty Healthcare Benefits Council Poor admission medication reconciliation
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
IMPROVING INPATIENT TO OUTPATIENT TRANSITION FOR GENERAL MEDICINE CLINIC PATIENTS
 IMPROVING INPATIENT TO OUTPATIENT TRANSITION FOR GENERAL MEDICINE CLINIC PATIENTS JULIE GILBREATH, MD, FACP; RAMON GALLEGOS, RN; PATRICIA REYES 8/2016-1/2017 1 THE TEAM CSE Participants: Julie Gilbreath,
IMPROVING INPATIENT TO OUTPATIENT TRANSITION FOR GENERAL MEDICINE CLINIC PATIENTS JULIE GILBREATH, MD, FACP; RAMON GALLEGOS, RN; PATRICIA REYES 8/2016-1/2017 1 THE TEAM CSE Participants: Julie Gilbreath,
Mary Stilphen, PT, DPT
 Mary Stilphen, PT, DPT Mary Stilphen PT, DPT is the Senior Director of Cleveland Clinic s Rehabilitation and Sports Therapy department in Cleveland, Ohio. Over the past 4 years, she led the integration
Mary Stilphen, PT, DPT Mary Stilphen PT, DPT is the Senior Director of Cleveland Clinic s Rehabilitation and Sports Therapy department in Cleveland, Ohio. Over the past 4 years, she led the integration
Home Assessments Resulting in a Positive Effect on Outcome Score Cards
 Home Assessments Resulting in a Positive Effect on Outcome Score Cards Presented by: Angela Benson, OTR/L, Clinical Specialist *graduated from Mount Aloysius College, Cresson, PA *9 years of experience
Home Assessments Resulting in a Positive Effect on Outcome Score Cards Presented by: Angela Benson, OTR/L, Clinical Specialist *graduated from Mount Aloysius College, Cresson, PA *9 years of experience
Novel combined patient instruction and discharge summary tool improves timeliness of documentation and outpatient provider satisfaction
 701053SMO0010.1177/2050312117701053SAGE Open MedicineGilliam et al. research-article2017 Original Article SAGE Open Medicine Novel combined patient instruction and discharge summary tool improves timeliness
701053SMO0010.1177/2050312117701053SAGE Open MedicineGilliam et al. research-article2017 Original Article SAGE Open Medicine Novel combined patient instruction and discharge summary tool improves timeliness
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility
 Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility Cynthia Williams, B.S.Pharm, FASHP Vice President/Chief Pharmacy Officer Riverside Health System, Newport
Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility Cynthia Williams, B.S.Pharm, FASHP Vice President/Chief Pharmacy Officer Riverside Health System, Newport
What are the potential ethical issues to be considered for the research participants and
 What are the potential ethical issues to be considered for the research participants and researchers in the following types of studies? 1. Postal questionnaires 2. Focus groups 3. One to one qualitative
What are the potential ethical issues to be considered for the research participants and researchers in the following types of studies? 1. Postal questionnaires 2. Focus groups 3. One to one qualitative
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
How to Improve the Discharge Process. Michelle Mourad, MD Ryan Greysen, MD
 How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
Communication in Healthcare: For Better Healing. Dr. Alexander Thomas President Consortium of Accredited Healthcare Organisations (CAHO)
") 1 Communication in Healthcare: For Better Healing Dr. Alexander Thomas President Consortium of Accredited Healthcare Organisations (CAHO) Executive Director, Association of Healthcare Providers, India
1 Communication in Healthcare: For Better Healing Dr. Alexander Thomas President Consortium of Accredited Healthcare Organisations (CAHO) Executive Director, Association of Healthcare Providers, India
Dimissione e periodo vulnerabile: come evitare le reospedalizzazioni precoci.
 Scompenso Cardiaco Acuto Convention Centri Scompenso Dimissione e periodo vulnerabile: come evitare le reospedalizzazioni precoci. G. Di Tano Cardiologia, Cremona Early Re-hospitalizations 30 days OHF
Scompenso Cardiaco Acuto Convention Centri Scompenso Dimissione e periodo vulnerabile: come evitare le reospedalizzazioni precoci. G. Di Tano Cardiologia, Cremona Early Re-hospitalizations 30 days OHF
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE)
") COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
Marshall Digital Scholar. Marshall University. Brittany Snodgrass. Charles K. Babcock Marshall University,
 Marshall University Marshall Digital Scholar Pharmacy Practice & Administration Faculty Research 2013 The impact of a community pharmacist conducted comprehensive medication review (CMR) on 30-day re-admission
Marshall University Marshall Digital Scholar Pharmacy Practice & Administration Faculty Research 2013 The impact of a community pharmacist conducted comprehensive medication review (CMR) on 30-day re-admission
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
Avoiding Errors During Transitions of Care: Medication Reconciliation
 in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT
 1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
The Glasgow Admission Prediction Score. Allan Cameron Consultant Physician, Glasgow Royal Infirmary
 The Glasgow Admission Prediction Score Allan Cameron Consultant Physician, Glasgow Royal Infirmary Outline The need for an admission prediction score What is GAPS? GAPS versus human judgment and Amb Score
The Glasgow Admission Prediction Score Allan Cameron Consultant Physician, Glasgow Royal Infirmary Outline The need for an admission prediction score What is GAPS? GAPS versus human judgment and Amb Score
REPORT OF THE COUNCIL ON MEDICAL SERVICE
 REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Hospital Discharge Communications Peter S. Lund, MD, Chair Reference Committee J (Candace E. Keller, MD, Chair)
REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Hospital Discharge Communications Peter S. Lund, MD, Chair Reference Committee J (Candace E. Keller, MD, Chair)
Since 1979 a variety of medical classification standards have been used to collect
 Medical classification systems in Canada: moving toward the year 2000 André N. Lalonde, MHA; Elizabeth Taylor Abstract THE USE OF DIFFERENT STANDARDS FOR CODING DIAGNOSES and procedures has been identified
Medical classification systems in Canada: moving toward the year 2000 André N. Lalonde, MHA; Elizabeth Taylor Abstract THE USE OF DIFFERENT STANDARDS FOR CODING DIAGNOSES and procedures has been identified
BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS
 BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS Senior s Month Education 2013 Sponsored by Regional Geriatric Program central (RGPc) Committee for the Enhancement of Elder
BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS Senior s Month Education 2013 Sponsored by Regional Geriatric Program central (RGPc) Committee for the Enhancement of Elder
RUNNING HEAD: HANDOVER 1
 RUNNING HEAD: HANDOVER 1 Evidence-Based Practice Project: Implementing Bedside Nursing Handover Jane Jones, BSN RN Austin State Univeristy August 18, 2017 RUNNING HEAD: HANDOVER 2 I. Introduction The purpose
RUNNING HEAD: HANDOVER 1 Evidence-Based Practice Project: Implementing Bedside Nursing Handover Jane Jones, BSN RN Austin State Univeristy August 18, 2017 RUNNING HEAD: HANDOVER 2 I. Introduction The purpose
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Electronic Health Records for research and Hospital management. The "Assistance Publique - Hôpitaux de Paris" initiative
 Electronic Health Records for research and Hospital management The "Assistance Publique - Hôpitaux de Paris" initiative Pr Philippe Lechat Clinical Research Department, St Louis Hospital, AP-HP, Paris
Electronic Health Records for research and Hospital management The "Assistance Publique - Hôpitaux de Paris" initiative Pr Philippe Lechat Clinical Research Department, St Louis Hospital, AP-HP, Paris
Using Data to Inform Quality Improvement
 20 15 10 5 0 Using Data to Inform Quality Improvement Ethan Kuperman, MD FHM Aparna Kamath, MD MS Justin Glasgow, MD PhD Disclosures None of the presenters today have relevant personal or financial conflicts
20 15 10 5 0 Using Data to Inform Quality Improvement Ethan Kuperman, MD FHM Aparna Kamath, MD MS Justin Glasgow, MD PhD Disclosures None of the presenters today have relevant personal or financial conflicts
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy
 Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Introduction. Fields marked with * are mandatory.
 Questionnaires on introducing the European Professional Ca doctors, pharmacists, physiotherapists, engineers, mountain agents(to competent authorities and other interested public a Fields marked with *
Questionnaires on introducing the European Professional Ca doctors, pharmacists, physiotherapists, engineers, mountain agents(to competent authorities and other interested public a Fields marked with *
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Preventing Avoidable Readmissions Together: Improving Discharge Summaries. R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC
 Preventing Avoidable Readmissions Together: Improving Discharge Summaries R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC Today s Objectives Identify elements of a complete discharge summary
Preventing Avoidable Readmissions Together: Improving Discharge Summaries R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC Today s Objectives Identify elements of a complete discharge summary
Model of Care Scoring Guidelines CY October 8, 2015
 Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Key Words: Transitions of care, care coordination, medication management, drug therapy problem
 Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015)
") 7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
Shaping Perceptions of Biopsychosocial Dementia Care with Interprofessional Collaboration DRS. BENJAMIN A. BENSADON & MARÍA ORDÓÑEZ
 Shaping Perceptions of Biopsychosocial Dementia Care with Interprofessional Collaboration DRS. BENJAMIN A. BENSADON & MARÍA ORDÓÑEZ FAU College of Medicine Small cohorts ( 64 students each) Longitudinal
Shaping Perceptions of Biopsychosocial Dementia Care with Interprofessional Collaboration DRS. BENJAMIN A. BENSADON & MARÍA ORDÓÑEZ FAU College of Medicine Small cohorts ( 64 students each) Longitudinal
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Question Patient #1 Patient #2 Patient #3 Patient #4 Patient #5 Number of days between the last discharge and this readmission date?
 Worksheet A: Chart Reviews of Patients Who Were Readmitted Conduct chart reviews of the last five readmitted patients. Reviewers should be physicians or nurses from the hospital and community settings.
Worksheet A: Chart Reviews of Patients Who Were Readmitted Conduct chart reviews of the last five readmitted patients. Reviewers should be physicians or nurses from the hospital and community settings.
Discharge to Assess Standards for Greater Manchester
 Discharge to Assess Standards for Greater Manchester 1 Contents 1. Introduction... 3 2. Definition of Discharge to Assess... 3 3. Discharge to Assess Pathways... 4 4. Greater Manchester Standards for Discharge
Discharge to Assess Standards for Greater Manchester 1 Contents 1. Introduction... 3 2. Definition of Discharge to Assess... 3 3. Discharge to Assess Pathways... 4 4. Greater Manchester Standards for Discharge
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
The importance of implementation science to help enhance quality improvement activities
 The importance of implementation science to help enhance quality improvement activities Jeremy Grimshaw Senior Scientist, Ottawa Hospital Research Institute Professor, Department of Medicine, University
The importance of implementation science to help enhance quality improvement activities Jeremy Grimshaw Senior Scientist, Ottawa Hospital Research Institute Professor, Department of Medicine, University
National Priorities for Improvement:
 National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
Outpatient management of community acquired pneumonia
 Outpatient management of community acquired pneumonia Wei Shen Lim Consultant Respiratory Physician Honorary Professor of Medicine (University of Nottingham) Nottingham University Hospitals NHS Trust What
Outpatient management of community acquired pneumonia Wei Shen Lim Consultant Respiratory Physician Honorary Professor of Medicine (University of Nottingham) Nottingham University Hospitals NHS Trust What
STROKE REHAB PROGRAM
 STROKE REHAB PROGRAM Allied Rehab Hospital is part of Allied Services Integrated Health System, the premier post-acute health-care system in Northeast Pennsylvania, and is the region s leading provider
STROKE REHAB PROGRAM Allied Rehab Hospital is part of Allied Services Integrated Health System, the premier post-acute health-care system in Northeast Pennsylvania, and is the region s leading provider
LTC Discharge and Transfer Requirements. Revised October 24, 2017
 LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
INTRODUCTION Reduce falls Improve patient outcomes Establish a baseline of falls in home care
 INTRODUCTION The Missouri Alliance for Home Care (MAHC) has developed a set of standardized tools for reporting and monitoring falls in patients under the care of home health. The program which began as
INTRODUCTION The Missouri Alliance for Home Care (MAHC) has developed a set of standardized tools for reporting and monitoring falls in patients under the care of home health. The program which began as
Partnering with Patients to Drive Safety and Quality
 Partnering with Patients to Drive Safety and Quality CLINICAL EXCELLENCE COMMISSION Virginia Armour Program Manager, Patient Based Care 2 November 2015 AHHA Patient engagement and the patient experience
Partnering with Patients to Drive Safety and Quality CLINICAL EXCELLENCE COMMISSION Virginia Armour Program Manager, Patient Based Care 2 November 2015 AHHA Patient engagement and the patient experience
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016
 UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
Hospital at home or acute hospital care: a cost minimisation analysis Coast J, Richards S H, Peters T J, Gunnell D J, Darlow M, Pounsford J
 Hospital at home or acute hospital care: a cost minimisation analysis Coast J, Richards S H, Peters T J, Gunnell D J, Darlow M, Pounsford J Record Status This is a critical abstract of an economic evaluation
Hospital at home or acute hospital care: a cost minimisation analysis Coast J, Richards S H, Peters T J, Gunnell D J, Darlow M, Pounsford J Record Status This is a critical abstract of an economic evaluation
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT
 CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
CMS OASIS Q&As: CATEGORY 2 - COMPREHENSIVE ASSESSMENT Q1. When are we required to collect OASIS? [Q&A EDITED 06/14] A1. The Condition of Participation (CoP) published in January 1999 requires a comprehensive
Targeting Readmissions:
 Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Medication Reconciliation Bundle of Care. Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013
 Medication Reconciliation Bundle of Care Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013 Overview Problem of medication errors at transitions of care Who is at risk Recognition as a patient
Medication Reconciliation Bundle of Care Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013 Overview Problem of medication errors at transitions of care Who is at risk Recognition as a patient
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division
 Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division SUICIDE RISK ASSESSMENT IN THE EMERGENCY DEPARTMENT May, 2014 Background The Quality and Patient Safety
Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division SUICIDE RISK ASSESSMENT IN THE EMERGENCY DEPARTMENT May, 2014 Background The Quality and Patient Safety
Value model in the new healthcare paradigm: Producing value at a single specialty center.
 Value model in the new healthcare paradigm: Producing value at a single specialty center. State of Spine Surgery Think Tank June 17, 2017 Catherine MacLean, MD, PhD Chief Value Medical Officer Center for
Value model in the new healthcare paradigm: Producing value at a single specialty center. State of Spine Surgery Think Tank June 17, 2017 Catherine MacLean, MD, PhD Chief Value Medical Officer Center for
Chapter 14 Regina Qu Appelle Regional Health Authority Safe and Timely Discharge of Hospital Patients 1.0 MAIN POINTS
 Chapter 14 Regina Qu Appelle Regional Health Authority Safe and Timely Discharge of Hospital Patients 1.0 MAIN POINTS Safe and timely discharge of patients from hospitals helps ensure patients well-being
Chapter 14 Regina Qu Appelle Regional Health Authority Safe and Timely Discharge of Hospital Patients 1.0 MAIN POINTS Safe and timely discharge of patients from hospitals helps ensure patients well-being
Medication Management: Is It in Your Toolbox?
 Medication Management: Is It in Your Toolbox? Brian K. Esterly, MBA, SVP, Corporate Development, excellerx, Inc. O: 215.282.1676, besterly@excellerx.com What has been your Medication Management experience?
Medication Management: Is It in Your Toolbox? Brian K. Esterly, MBA, SVP, Corporate Development, excellerx, Inc. O: 215.282.1676, besterly@excellerx.com What has been your Medication Management experience?
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
Optimizing pharmaceutical care via Health Information Technology:
 Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests