AN OVERVIEW of TARGET HF: QUALIFYING for the HONOR ROLL and a DETAILED FOCUS on MEDICATION COMPLIANCE (ACE/ARB, ADLOSTERONE ANTAGONIST, and EBBB)
|
|
|
- Lee Baldwin
- 5 years ago
- Views:
Transcription
1 AN OVERVIEW of TARGET HF: QUALIFYING for the HONOR ROLL and a DETAILED FOCUS on MEDICATION COMPLIANCE (ACE/ARB, ADLOSTERONE ANTAGONIST, and EBBB) HAZLETON GENERAL HOSPITAL HAZLETON, PENNSYLVANIA PRESENTERS: ANDREA ANDREWS, RN / CHCQM DIRECTOR QUALITY / CASE MANAGEMENT ANTHONY VALENTE, MD / FACP VICE PRESIDENT OF MEDICAL AFFAIRS 1
2 Our objectives for this teleconference will be to: (1) Discuss ways to improve quality, care transitions, and outcomes for patients with heart failure utilizing patient-centered domains, and (2) Discuss medication optimization in heart failure patients. 2 2
3 Target: Heart Failure is a national initiative of the American Heart Association that provides healthcare professionals with resources and materials designed to help advance heart failure awareness, prevention, and treatment. Hazleton General Hospital is committed to providing quality, evidencebased standard of care for our heart failure patient population. Heart failure is one of our top 5 DRG admissions and one of our top readmit DRG s. To help you better understand our care of the heart failure patient, let me provide you with a background of our journey. 3 3
4 We began our journey in the care of our heart failure patients in January, 2007, when we were invited to be a part of the Accelerating Best Care (ABC) in Pennsylvania Program funded by our state legislature. Representatives from The Baylor Health Care System, who developed the ABC at Baylor program, showed us the results of their quality improvement program. They explained the cultural changes needed to improve quality and the practical tools needed to accomplish their goals. The basis of the ABC Program is to break a problem down into small pieces, like a puzzle, quickly analyze the problem through data collection, implement interventions, and analyze results adding additional interventions if needed, all in a short period of time. 4 4
5 Prior to learning the methodology of the ABC Program, departments would identify problems and tackle the whole problem. Findings were: Team work with other affected departments was sometimes present, but not always; Months and months of data would be collected; Interventions were delayed; quality targets were not always met and Improvements were not noted in a timely fashion. A core group of 14 individuals, from different disciplines within our organization, began rigorous training on the ABC process in January, Training, conducted by coaches from Baylor and Thomas Jefferson, focused on the structure, process, and outcomes of improving quality using the ABC methodology and laid the groundwork for projects the core group were to complete. 5

6 Five quality initiatives were selected to go through the ABC methodology of quality improvement during the training period. One of these projects involved our HF core measures, first focusing on HF discharge instructions. WHY HEART FAILURE? Top Admission Diagnosis Most Common Reason for Readmission Core Measure Financial Impact Our HF Team was formed and the assessment of all patients on the telemetry unit was our focus. The baseline for our heart failure discharge instruction core measure compliance for January, 2007 was 79%. 6 6
7 Our team identified the need for standing order sets for CHF admissions. These were implemented and made mandatory for use by the Medical Staff, with support from the Medical Executive Committee leadership. To increase compliance with our core measures more importantly to provide quality care to each of our CHF patients every time all the time, we placed a yellow CHF form on the front of the charts for all CHF patients with the words STOP CHF on them. 7 A CHF discharge instruction form was developed and implemented to be utilized for all CHF discharges. This form addressed all the required elements by CMS which include the following: Diet Activity Medications Weight Symptoms Follow-up 7
8 After implementation of these interventions, our compliance for heart failure discharge instructions went to 100% in May, For a better understanding of where HGH began its journey with HF core measures, and where it journeyed to, please note the following: Evaluation Baseline Data in 2004 LVS Function 67% ACE or ARBfor LVSD 48% Adult Smoking Cessation 19% Discharge Instructions 14% 8 8
9 First Quarter 2012 Second Quarter 2012 Third Quarter 2012 Fourth Quarter 2012 LVS Function 100% 100% 100% 100% ACEor ARB for LVSD 100% 100% 100% 100% Discharge Instructions 98% 98% 100% 100% HF Patient Appropriateness of Care Compliance 99% 99% 100% 100% 9 9

10 To sustain our HF compliance, as evidenced by the previous slide, we have implemented the following through our ABC process: Placed a clinical quality data RN specialist on the clinical units monitoring the care our HF patients receive in real-time Have revised our HF discharge instructions to include a follow-up call to the patient within 72 hours of discharge Collaborated with our home health agency in utilizing home telehealth monitors for our HF patients who request our agency and who meet criteria for these monitors

 and identify any real or potential problems.")
11 These monitors assess weight, blood pressure, 02 saturations, and pulse, along with a set of questions individually selected for each patient regarding edema, shortness of breath, meds, etc. These monitors are set up to be checked daily and the information is then sent to a secure website, which our home health nurses check on a daily basis (Monday Friday) and identify any real or potential problems. If a problem is identified, the home health nurse calls the patient for more information and then either calls the physician or sends a nurse out to evaluate
12 ACCOMPLISMENTS AT HGH with OUR HF CORE MEASURE PROCESS Have submitted our CHF order sets and medication forms to the AHA, and were chosen to have our CHF tools posted in the GWTG Tool Library. Remain a HF mentor hospital for the IHI 5,000,000 Lives Campaign Had an article, showcasing our Heart Failure Tools, appear in the December, 2009 issue of Critical Pathways in Cardiology journal. Received our Target: HF first time Status/Recognition in Received the Gold Plus Heart Failure Award in 2011 (3 years in a row). (Will be submitting our application for 2012/2013 and for Target: HF in 2012/2013). Have received the five star rating for treatment of our HF patients from Healthgrades
13 When providing optimal HF care, we benefit in many ways: LOS is decreased Utilization of resources is decreased and most importantly, patient satisfaction is increased. Hazleton General Hospital continued its journey in caring for the heart failure patient by submitting an honor roll award application for Target: HF in We were one of two hospitals in the Nation that was recognized as a Target Heart Failure Honor Roll Hospital in The US New and World Report ad in August,
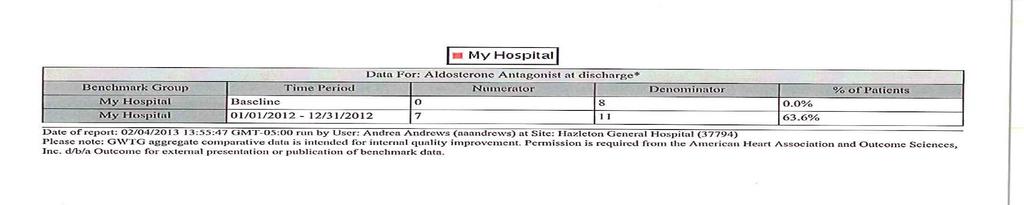
14 Our compliance to the required measures (where 50% compliance was needed) is as follows. (1) ACE/ARB at discharge 100% compliance (2) EBBB 75% compliance (3) Aldosterone Antagonist at Discharge 80% compliance (4) Follow-up visit within 7 days or less 87.5% compliance (5) Referred to HF disease management, 60 minutes patient education, or HF interactive workbook 100% compliance The Target: Heart Failure Mission involves 3 key patient-centered care domains that I will address at this time, as they pertain to Hazleton General Hospital and it s heart failure patients


15 15 15
16 16 16

17 17 17
18 18 18

19 19 19
20 20 20


21 21 21
22 1. Medication optimization regarding discharge use of ACE/ARB, EBBB, and Aldosterone antagonist in all eligible heart failure patients. (a) ACE/ARB at discharge for calendar year 2012 we are at 100% compliance. (b)ebbb for calendar year 2012, we are at 72% compliance. In order to address the EBBB and Aldosterone antagonist medication optimization, we have revised our HF order sets to include these meds. We have also heightened awareness with our medical staff, Pharmacy and nursing in regards to medication optimization of our heart failure patients through use of evidence-based standards of care and team collaboration
23 (c) Aldosterone antagonist at discharge for calendar year 2012, we are at 63.6% compliance. This measure addresses heart failure patients with LVSD with no contraindications or documented intolerance to this medication
24 24 24
25 25 25
26 26 26
27 27 27
28 2. Early follow-up and care coordination early post-discharge followup with visit or phone call scheduled to occur within 7 days of hospital discharge for calendar year 2012, we are at 90.3% compliance. Nursing is responsible for meeting this measure and we have a Clinical Quality Data RN Specialist who reviews this daily. We also try to place our heart failure patients on our telemetry unit. We also make the post-discharge appointment for heart failure patients, whom we have identified as our high-risk population for calendar year 2012, we are at 96.8% compliance
29 3. Enhanced patient education this involves referral to HF disease management, 60 minutes of patient education, or HF interactive workbook for calendar year 2012, we are at 98% compliance. We have revised our CHF Discharge Instructions to include the AHA s Information Prescription for Healthier Living with HF which we give to the patient
30 2/12/



31 31 31
32 We also begin HF education / teaching on admission, and reiterate again at discharge. We use the CHF teaching / discharge instruction form
33 33 33

34 We have an ABC team that remains in place working with nursing, the medical staff, home health and other involved ancillary departments in providing the best care to our HF patients every time, all the time utilizing evidence-based standards of care and team collaboration. We definitely have room for improvement with EBBB and Aldosterone antagonists ordered at discharge, and this is where our focus will be with our ABC team as we strive to improve the care of our heart failure patients and maintain Target: HF Status/Recognition
35 35 35
36 For more information contact: Andrea Andrews Director of Quality / Case Management Hazleton General Hospital aandrews@ggha.org Anthony Valente, M.D./FACP Vice President of Medical Affairs 36 36
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 2/27/2013 2010, American Heart Association 2 1
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 2/27/2013 2010, American Heart Association 2 1
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
University Cincinnati Medical Center
 University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients
 Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
Home Health Agencies & Reducing Readmissions. presented by Misty Kevech, RN, MS, COS C, CCP HHQI RN Project Coordinator WVMI & Quality Insights
 Home Health Agencies & Reducing Readmissions presented by Misty Kevech, RN, MS, COS C, CCP HHQI RN Project Coordinator WVMI & Quality Insights Objectives Describe the benefits of collaborating and utilizing
Home Health Agencies & Reducing Readmissions presented by Misty Kevech, RN, MS, COS C, CCP HHQI RN Project Coordinator WVMI & Quality Insights Objectives Describe the benefits of collaborating and utilizing
American College of Cardiology Patient Navigator Program Focus MI National PROGRAM REQUIREMENTS
 American College of Cardiology Patient Navigator Program Focus MI National 1. Participant Responsibilities PROGRAM REQUIREMENTS 1.1. Program Management 1.1.1. Upon opting-in to the Patient Navigator Program
American College of Cardiology Patient Navigator Program Focus MI National 1. Participant Responsibilities PROGRAM REQUIREMENTS 1.1. Program Management 1.1.1. Upon opting-in to the Patient Navigator Program
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Thinking Differently about Hospital Readmissions
 Thinking Differently about Hospital Readmissions LaNita Knoke RN, BS, CMCN Healthcare Strategist Senior Care Continuum Each Home Instead Senior Care franchise office is independently owned and operated.
Thinking Differently about Hospital Readmissions LaNita Knoke RN, BS, CMCN Healthcare Strategist Senior Care Continuum Each Home Instead Senior Care franchise office is independently owned and operated.
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
UPMC Health Plan. Value Based Insurance Design (VBID) Spark Your Health
 Spark Your Health") UPMC Health Plan Value Based Insurance Design (VBID) Spark Your Health Value Based Insurance Design (VBID) Spark Your Health Medicare Advantage Summit April 6, 2017 Helene Weinraub 1 The statements contained
UPMC Health Plan Value Based Insurance Design (VBID) Spark Your Health Value Based Insurance Design (VBID) Spark Your Health Medicare Advantage Summit April 6, 2017 Helene Weinraub 1 The statements contained
Hamilton Health Sciences STRATEGIC PLAN. Patients PLAN AT A GLANCE People. Sustainability. Research, Innovation & Learning
 Patients Hamilton Health Sciences STRATEGIC PLAN PLAN AT A GLANCE 2016-2017 Research, Innovation & Learning Hamilton Health Sciences STRATEGIC PLAN PLAN AT A GLANCE 2016-2017 Rob MacIsaac President and
Patients Hamilton Health Sciences STRATEGIC PLAN PLAN AT A GLANCE 2016-2017 Research, Innovation & Learning Hamilton Health Sciences STRATEGIC PLAN PLAN AT A GLANCE 2016-2017 Rob MacIsaac President and
Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments
 Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments Prepared by National Institute of Whole Health www.niwh.org Accredited by the Institute for Credentialing
Patient Health Education: What Physicians Need to Know to Thrive in Today s Healthcare Environments Prepared by National Institute of Whole Health www.niwh.org Accredited by the Institute for Credentialing
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Improving Heart Failure Outcomes through Interactive Patient Care: The Sentara Virginia Beach General Hospital Experience
 WHITE PAPER Improving Heart Failure Outcomes through Interactive Patient Care: The Sentara Virginia Beach General Hospital Experience 06.05.09 executive summary In the United States, Heart Failure has
WHITE PAPER Improving Heart Failure Outcomes through Interactive Patient Care: The Sentara Virginia Beach General Hospital Experience 06.05.09 executive summary In the United States, Heart Failure has
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Heart Failure Education Consider Health Literacy
 Heart Failure Education Consider Health Literacy Sandy Hall RN BSN Heart Failure Case Manager Mercy Medical Center Des Moines, IA August 2012 What does this mean to you? Cardiac diet 1 Is it this? Low
Heart Failure Education Consider Health Literacy Sandy Hall RN BSN Heart Failure Case Manager Mercy Medical Center Des Moines, IA August 2012 What does this mean to you? Cardiac diet 1 Is it this? Low
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Heart Failure Clinic a Multidisciplinary approach. Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM
 Heart Failure Clinic a Multidisciplinary approach Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
Heart Failure Clinic a Multidisciplinary approach Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
MAHP Annual Conference. October 18 th -19th
 MAHP Annual Conference October 18 th -19th Learning Objectives Highlight UMMC s National Business strategy Provide MAHP members a UMMC Center for Telehealth update Understand the need for Telehealth services
MAHP Annual Conference October 18 th -19th Learning Objectives Highlight UMMC s National Business strategy Provide MAHP members a UMMC Center for Telehealth update Understand the need for Telehealth services
PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER
 PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER PROJECT PURPOSE To reduce hospital readmissions for CHF, pneumonia patients To improve patient satisfaction with the discharge
PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER PROJECT PURPOSE To reduce hospital readmissions for CHF, pneumonia patients To improve patient satisfaction with the discharge
Stroke Coordinator Boot Camp
 Stroke Coordinator Boot Camp Gena Kreiner RN BSN FHS Stroke Coordinator Karen C. Kiesz MN RN CNRN SCRN MHS Stroke Program Manager Lisa Shumaker, BSN, RN, CMSRN (Moderator) PRMC- Everett Stroke Program
Stroke Coordinator Boot Camp Gena Kreiner RN BSN FHS Stroke Coordinator Karen C. Kiesz MN RN CNRN SCRN MHS Stroke Program Manager Lisa Shumaker, BSN, RN, CMSRN (Moderator) PRMC- Everett Stroke Program
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
An Integrated Approach to Heart Failure Care. Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN
 An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
The Patient Protection and Affordable Care Act of 2010
 INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
CKHA Quality Improvement Plan (QIP) Scorecard
 Scorecard") CKHA Quality Improvement Plan () Scorecard 217-18 Quality dimension Performance Indicator 217-18 Performance Goals results where available Current Value Page Safety Medication Reconciliation completed
CKHA Quality Improvement Plan () Scorecard 217-18 Quality dimension Performance Indicator 217-18 Performance Goals results where available Current Value Page Safety Medication Reconciliation completed
The Power of Clinical Callbacks: Preventing Early Readmissions with Clinical Callbacks. Cheryl Crumpton, BSN, RN, CEN
 The Power of Clinical Callbacks: Preventing Early Readmissions with Clinical Callbacks Cheryl Crumpton, BSN, RN, CEN Making the Patient Call Manager (PCM) Connection Quality Initiative Improve Clinical
The Power of Clinical Callbacks: Preventing Early Readmissions with Clinical Callbacks Cheryl Crumpton, BSN, RN, CEN Making the Patient Call Manager (PCM) Connection Quality Initiative Improve Clinical
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Patient and Family Caregiver Interview Tool
 Patient and Family Caregiver Interview Tool Instructions: We recommend you select at least 5-10 patients who have been readmitted to your organization within the past 30 days to include in the group of
Patient and Family Caregiver Interview Tool Instructions: We recommend you select at least 5-10 patients who have been readmitted to your organization within the past 30 days to include in the group of
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
United Medical ACO Participation Criteria
 United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
2015 Executive Overview
 An Independent Licensee of the Blue Cross and Blue Shield Association 2015 Executive Overview Criteria for the Blue Cross and Blue Shield of Alabama Hospital Tiered Network will be updated effective January
An Independent Licensee of the Blue Cross and Blue Shield Association 2015 Executive Overview Criteria for the Blue Cross and Blue Shield of Alabama Hospital Tiered Network will be updated effective January
The 5 W s of the CMS Core Quality Process and Outcome Measures
 The 5 W s of the CMS Core Quality Process and Outcome Measures Understanding the process and the expectations Developed by Kathy Wonderly RN,BSPA, CPHQ Performance Improvement Coordinator Developed : September
The 5 W s of the CMS Core Quality Process and Outcome Measures Understanding the process and the expectations Developed by Kathy Wonderly RN,BSPA, CPHQ Performance Improvement Coordinator Developed : September
TEES, ESK & WEAR VALLEYS NHS FOUNDATION TRUST: DEVELOPING A MODEL LINE FOR RECOVERY- FOCUSED CARE
 TEES, ESK & WEAR VALLEYS NHS FOUNDATION TRUST: DEVELOPING A MODEL LINE FOR RECOVERY- FOCUSED CARE Summary Tees, Esk and Wear Valleys NHS Foundation Trust (TEWV) adapted the model line concept from industry
TEES, ESK & WEAR VALLEYS NHS FOUNDATION TRUST: DEVELOPING A MODEL LINE FOR RECOVERY- FOCUSED CARE Summary Tees, Esk and Wear Valleys NHS Foundation Trust (TEWV) adapted the model line concept from industry
Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through Telemedicine
 PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
Medicare Beneficiary Quality Improvement Project. March 11, Chillicothe, Mo.
 Medicare Beneficiary Quality Improvement Project March 11, 2015 - Chillicothe, Mo. 1 Welcome and MBQIP Overview 2 Introductions Dana Downing, B.S., MBA, CPHQ Jim Mikes, ScD, MPH Melissa VanDyne, B.S. CAHs
Medicare Beneficiary Quality Improvement Project March 11, 2015 - Chillicothe, Mo. 1 Welcome and MBQIP Overview 2 Introductions Dana Downing, B.S., MBA, CPHQ Jim Mikes, ScD, MPH Melissa VanDyne, B.S. CAHs
The ABC s of Antibiotic Stewardship Georgia s Approach. Presentation to: 2018 Flex Program Reverse Site Visit Presented by: Lisa Carhuff MSN RN
 The ABC s of Antibiotic Stewardship Georgia s Approach Presentation to: 2018 Flex Program Reverse Site Visit Presented by: Lisa Carhuff MSN RN 0 Wednesday, July 18, 2018 Learning Objectives Describe the
The ABC s of Antibiotic Stewardship Georgia s Approach Presentation to: 2018 Flex Program Reverse Site Visit Presented by: Lisa Carhuff MSN RN 0 Wednesday, July 18, 2018 Learning Objectives Describe the
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
Foreign Service Benefit Plan
 Simple Steps to Living Well Together Foreign Service Benefit Plan 2018 Wellness Benefits and Incentive Rewards Health Plan Accredited by The FOREIGN SERVICE BENEFIT PLAN has Health Plan Accreditation from
Simple Steps to Living Well Together Foreign Service Benefit Plan 2018 Wellness Benefits and Incentive Rewards Health Plan Accredited by The FOREIGN SERVICE BENEFIT PLAN has Health Plan Accreditation from
Exacerbation of Condition. VNAA Best Practice for Home Health
 Exacerbation of Condition VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Discuss two reasons why it is important to help a patient identify changes in their condition
Exacerbation of Condition VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Discuss two reasons why it is important to help a patient identify changes in their condition
2017 Edition. MIPS Guide. The rule is in and Medicare physician payments are changing. What does that mean for you?
 2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
Evaluation of the Hywel Dda Community Pharmacist pilot optimising medicines treatment in heart failure.
 Evaluation of the Hywel Dda Community Pharmacist pilot optimising medicines treatment in heart failure. Authors: Gareth Holyfield (Principal Pharmacist, Public Health Wales) Don Wilkes (Community Pharmacist,
Evaluation of the Hywel Dda Community Pharmacist pilot optimising medicines treatment in heart failure. Authors: Gareth Holyfield (Principal Pharmacist, Public Health Wales) Don Wilkes (Community Pharmacist,
A Care Transitions Project
 Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
DELTA CARE CHANGING LIVES. A CARE TRANSITION PROGRAM of EPHRAIM MCDOWELL HEALTH DR. JOAN HALTOM, PHARM.D, FKSHP GAIL SHEARER, BSN, MBA,CCM
 DELTA CARE CHANGING LIVES A CARE TRANSITION PROGRAM of EPHRAIM MCDOWELL HEALTH DR. JOAN HALTOM, PHARM.D, FKSHP GAIL SHEARER, BSN, MBA,CCM DELTA CARE Delta Care is an Innovative approach to transitioning
DELTA CARE CHANGING LIVES A CARE TRANSITION PROGRAM of EPHRAIM MCDOWELL HEALTH DR. JOAN HALTOM, PHARM.D, FKSHP GAIL SHEARER, BSN, MBA,CCM DELTA CARE Delta Care is an Innovative approach to transitioning
Increasing Self Care Compliance with Follow-up Appointments
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-18-2015 Increasing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-18-2015 Increasing
UW HEALTH JOB DESCRIPTION
 Job Code: 801008 UW HEALTH JOB DESCRIPTION Outcomes Manager- Medicine FLSA Status: Exempt Mgt. Approval: Barbara Liegel Date: 9-16 HR Approval: R. Temple Date: 9-16 JOB SUMMARY The Outcomes Manager is
Job Code: 801008 UW HEALTH JOB DESCRIPTION Outcomes Manager- Medicine FLSA Status: Exempt Mgt. Approval: Barbara Liegel Date: 9-16 HR Approval: R. Temple Date: 9-16 JOB SUMMARY The Outcomes Manager is
Hospital Compare Quality Measures: 2008 National and Florida Results for Critical Access Hospitals
 Hospital Compare Quality Measures: National and Results for Critical Access Hospitals Michelle Casey, MS, Michele Burlew, MS, Ira Moscovice, PhD University of Minnesota Rural Health Research Center Introduction
Hospital Compare Quality Measures: National and Results for Critical Access Hospitals Michelle Casey, MS, Michele Burlew, MS, Ira Moscovice, PhD University of Minnesota Rural Health Research Center Introduction
Southeast Michigan See You in 7 Hospital Collaborative: Session 2 Webinar. Tuesday, June 19 at 8 am
 Southeast Michigan See You in 7 Hospital Collaborative: Session 2 Webinar Tuesday, June 19 at 8 am Agenda Administrative Buy-In & Getting Projects Off the Ground - Maureen Bowman, R.N., Vice President
Southeast Michigan See You in 7 Hospital Collaborative: Session 2 Webinar Tuesday, June 19 at 8 am Agenda Administrative Buy-In & Getting Projects Off the Ground - Maureen Bowman, R.N., Vice President
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Transitions of Care. Scott Clark, President Leading Edge Health Care
 Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Connect HF Solution. Case Study. Reducing 30-Day Heart Failure. How Process Optimization and Peer-to-Peer Connections Standardized HF Care
 Connect HF Solution Case Study Reducing 30-Day Heart Failure Readmissions How Process Optimization and Peer-to-Peer Connections Standardized HF Care C a s e Study Reducing 30-Day Heart Failure Readmissions
Connect HF Solution Case Study Reducing 30-Day Heart Failure Readmissions How Process Optimization and Peer-to-Peer Connections Standardized HF Care C a s e Study Reducing 30-Day Heart Failure Readmissions
Outline 11/17/2014. Overview of the Issue Program Overview Program Components Program Implementation
 Physical Health Integration in a Behavioral Health Setting Robin Reed, MD, MPH Rupal Yu, MD, MPH Acknowledgements The Duke Endowment Piedmont Health Services Carolina Advanced Health Community Care of
Physical Health Integration in a Behavioral Health Setting Robin Reed, MD, MPH Rupal Yu, MD, MPH Acknowledgements The Duke Endowment Piedmont Health Services Carolina Advanced Health Community Care of
Using A Data Warehouse and Analytics to Drive Population Health Management
 Success Story Using A Data Warehouse and Analytics to Drive Population Health Management HEALTHCARE ORGANIZATION Large Medical Center TOP RESULTS Enabled pay-for-performance (P4P) incentive payment reporting
Success Story Using A Data Warehouse and Analytics to Drive Population Health Management HEALTHCARE ORGANIZATION Large Medical Center TOP RESULTS Enabled pay-for-performance (P4P) incentive payment reporting
Chronic Care Taking Disease Management Beyond Hospital Walls
 Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
The TeleHealth Model THE TELEHEALTH SOLUTION
 The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure
 Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure November 16, 2016 Panelists Corinne Bott-Silverman, M.D., Cardiologist,
Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure November 16, 2016 Panelists Corinne Bott-Silverman, M.D., Cardiologist,
Healthcare Analytics & Managing Population Health
 Healthcare Analytics & Managing Population Health Victoria Tiase, MS, RN, Director Informatics Strategy, NewYork-Presbyterian Hospital Kathleen McGrow, MS, RN, PMP, Director Customer Marketing, Caradigm
Healthcare Analytics & Managing Population Health Victoria Tiase, MS, RN, Director Informatics Strategy, NewYork-Presbyterian Hospital Kathleen McGrow, MS, RN, PMP, Director Customer Marketing, Caradigm
A. Commissioning for Quality and Innovation (CQUIN)
") A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM
 ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM Objectives Understand the needs/goals that the Community Paramedic program was designed to address Understand how Abbeville County implemented
ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM Objectives Understand the needs/goals that the Community Paramedic program was designed to address Understand how Abbeville County implemented
The Nexus of Quality and Finance
 The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
SEE WHAT S NEW TO THE THIRD EDITION!
 Nursing Research: Reading, Using and Creating Evidence, Third Edition Janet Houser, PhD, RN ISBN-13: 978-1-2840-4329-7 Product With Access Code - 550 pages - 2015 Will Publish: 11/1/2013 SEE WHAT S NEW
Nursing Research: Reading, Using and Creating Evidence, Third Edition Janet Houser, PhD, RN ISBN-13: 978-1-2840-4329-7 Product With Access Code - 550 pages - 2015 Will Publish: 11/1/2013 SEE WHAT S NEW
QUEST: Collaboration for Performance
 QUEST: Collaboration for Performance The National Pay for Performance Summit San Francisco, CA March 8, 2010 Carolyn Scott, RN, M.Ed., MHA Vice President, Performance Improvement and Quality, Premier,
QUEST: Collaboration for Performance The National Pay for Performance Summit San Francisco, CA March 8, 2010 Carolyn Scott, RN, M.Ed., MHA Vice President, Performance Improvement and Quality, Premier,
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
2018 Practice Improvement Program (PIP) Orientation. January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP)
 Orientation. January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP)") 2018 Practice Improvement Program (PIP) Orientation January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP) Practice Improvement Program (PIP) Leadership Team James Glauber, Chief
2018 Practice Improvement Program (PIP) Orientation January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP) Practice Improvement Program (PIP) Leadership Team James Glauber, Chief
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Centralizing Multi-Hospital Mortality Reviews
 December 7, 2016 Session Codes: D4 (9:30am-10:45am) & E4 (11:15am - 12:30pm) Centralizing Multi-Hospital Mortality Reviews IHI 28 th National Forum Mark P Jarrett, MD, MBA, MS SVP, Chief Quality Officer,
December 7, 2016 Session Codes: D4 (9:30am-10:45am) & E4 (11:15am - 12:30pm) Centralizing Multi-Hospital Mortality Reviews IHI 28 th National Forum Mark P Jarrett, MD, MBA, MS SVP, Chief Quality Officer,
A20, B20. This presenter has nothing to disclose
 A20, B20 This presenter has nothing to disclose What Matters to You? Using Co-design to Revolutionize Patient Experience Christina Gunther-Murphy, MBA, The Institute for Healthcare Improvement Beth Hennessey,
A20, B20 This presenter has nothing to disclose What Matters to You? Using Co-design to Revolutionize Patient Experience Christina Gunther-Murphy, MBA, The Institute for Healthcare Improvement Beth Hennessey,
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
The STAAR Initiative
 The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE
 CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE Joy Goebel RN MN PhD Associate Professor of Nursing California State University Long Beach Objectives Discuss similarities
CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE Joy Goebel RN MN PhD Associate Professor of Nursing California State University Long Beach Objectives Discuss similarities
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
WEBINAR: Check. Change. Control. Cholesterol April 4, 2018
 WEBINAR: Check. Change. Control. Cholesterol April 4, 2018 Good afternoon, everyone. My name is Alberta I am from the New England QIN-QIO and I will be your moderator for today s webinar, Check. Change.
WEBINAR: Check. Change. Control. Cholesterol April 4, 2018 Good afternoon, everyone. My name is Alberta I am from the New England QIN-QIO and I will be your moderator for today s webinar, Check. Change.
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive