Facing the Crisis of Adult Primary Care
|
|
|
- Audrey Stephens
- 5 years ago
- Views:
Transcription
1 Facing the Crisis of Adult Primary Care July 27, 2010 Thomas Bodenheimer MD Center for Excellence in Primary Care Department of Family and Community Medicine University of California, San Francisco
2 Agenda The adult primary care practitioner crisis Declining access to primary care Confronting the adult primary care crisis 2
3 The adult primary care crisis 1/3 of U.S. physicians practice primary care, compared with 50% in most developed nations 2007 survey of fourth-year students, 7% planned careers in adult primary care. Hauer et al, JAMA 2008;300:1154 Reasons for lack of interest in primary care careers: PCPs earn on average 54% of what specialists earn, and most medical students graduate with >$120,000 in debt The work life of the PCP is stressful Medical students experience dysfunctional primary care and the medical school culture is hostile to primary care 3
4 Family Medicine Residency Positions and Number Filled by U.S. Medical School Graduates Bodenheimer T. N Engl J Med 2006;355:

5 Proportions of Third-Year Internal Medical Residents Choosing Careers as Generalists, Subspecialists, and Hospitalists Bodenheimer, N Engl J Med 2006;355:
6 Primary Care Physicians to Population Ratio (Physicians per 100,000 persons) 6

7 Adult Care: Projected Generalist Supply vs. Population Growth + Aging Shortage 2025: 35-44,000 Demand: adult pop n growth/aging Supply, Family Med, General Internal Med Colwill et al., Health Affairs, 2008:w
8 NP/PAs to the rescue? NP graduates have fallen from 8,200 in 1998 to 5,900 in % of NPs go into primary care. PA graduate numbers stable at 4,200 for several years. 32% of PAs practice in primary care. About half of NP/PAs are in primary care: increasingly choosing specialist offices, EDs, inpatient settings. Even with NP/PAs entering primary care, the primary care practitioner to population ratio will fall by 9% from 2005 to Colwill et al, Health Affairs Web Exclusive, April 29, 2008; Bodenheimer et al, Health Affairs 2009;28:64. 8


9 Underrepresented Minorities* (URMs) as % of U.S. Population and Selected Health Professions Medical students from underrepresented minorities are much more likely to choose primary care *African-Americans, Latinos, American Indians 9
10 Access to adult primary care 2008: 28% of Medicare patients without PCP had difficulty finding new PCP 17% increase from 2006 Medicare patients having difficulty finding new specialist decreased from 18% in 2006 to 11% in MedPAC. Report to Congress, March
11 Access to adult primary care 22% of Medicare patients and 31% of patients with private insurance had unwanted delay obtaining appointment for routine care in MedPAC. Report to Congress, March % of adults with PCP had trouble contacting the physician by phone, obtaining care after hours, or experiencing timely office visits. Closing the Divide. Commonwealth Fund,
12 Geographic distribution Primary care physician:population ratio Urban: 100/100,000 population Rural: 46/100,000 population Rural areas 21% of the U.S. population 10% of physicians 65 million people live in primary care health profession shortage areas 12
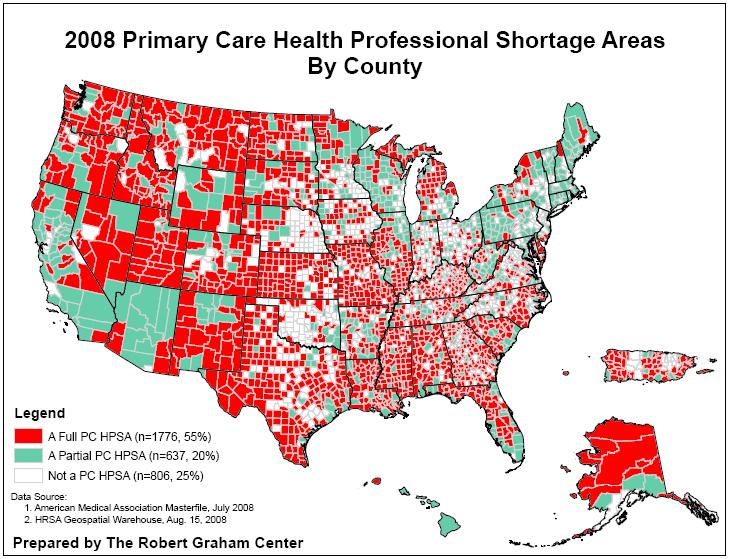
13 13
14 Access to adult primary care 46% of Californians going to ED said the problem could have been handled in primary care, but they were unable to access PCP. California HealthCare Foundation, Oct Medicaid patients of primary care practices with more than 12 evening hours per week utilized the ED 20% less than those cared for in practices with no evening hours. Lowe et al. Medical Care 2005;43:

15 70% of adult PCPs take no Medicaid patients or limit the number 15
16 Access to adult primary care Massachusetts after coverage expansion 2009 average wait time to see new PCP: 44 days (over 6 weeks), up from 33 days in survey: 52% of Massachusetts residents reported going to ED for themselves or their family in past year. Physician dissatisfaction: Family medicine: 45% General internal medicine: 55% Mass Medical Society Physician Workforce Study,
17 Workload of U.S. adult primary care A PCP with a panel of 2500 average patients will spend 7.4 hours per day doing recommended preventive care. Yarnall et al. Am J Public Health 2003;93:635 A PCP with a panel of 2500 average patients will spend 10.6 hours per day doing recommended chronic care Ostbye et al. Annals of Fam Med 2005;3:209 Average panel size in U.S.: 2300 Average panel size in Veterans Admin.: 1200 Average panel size in community clinics:
18 Workload of U.S. adult primary care Survey of 422 general internists and family physicians ( ): 48%: work pace is chaotic 78%: little control over the work 27%: definitely burning out 30%: likely to leave the practice within two years Linzer et al. Annals of Internal Medicine 2009;151:
19 Unsustainable work life: The 15-minute visit syndrome 50% of patients leave the PCP office visit without understanding what the physician said. Roter and Hall. Ann Rev Public Health 1989;10:163; Schillinger et al. Arch Intern Med 2003;163:83 Patients making an initial statement of their problem are interrupted by the PCP after an average of 23 seconds. Marvel et al. JAMA 1999;281:283 Patients do not participate in decisions 91% of the time in primary care. Braddock et al. JAMA 1999;282;
20 The dilemma Panel size too large for lone PCP to manage. We can t reduce panel size due to worsening shortage of PCPs. Shortage = larger panels, poorer access, more PCP burnout. 20
21 Solution: Health care reform and primary care Increased Title VII funding for primary care residencies Increased National Health Service Corps funding Primary care extension program: practice coaches to help primary care practices become PCMHs 10% increase in Medicare payments to primary care Medicaid to pay primary care same rates as Medicare Innovation center to stimulate PCMH pilots and payment reform for primary care 21
22 Solution: National policy options Money: drastic reduction in PCP-specialty income gap RBRVS reform SGR reform Payment reform Debt relief Practice transformation to reduce PCP stress Medical education reform Culture Curriculum Primary care experience Medicare GME reform Bodenheimer et al., A Lifeline for Primary Care, N Engl J Med 2009;360:
23 Solution: Practice of the future 8-10 PCP face-to-face visits per day. Reduces burnout. Serious investment in team-building. About 100 patients touched each day: , phone, outreach for chronic/ preventive care, group visits, visits with other team members. Minority of encounters physician face-to-face visits. Patients not requiring PCP expertise see other team members. RN care management for high-cost patients with complex health care needs. Margolius and Bodenheimer, Health Affairs, May 2010 Bodenheimer and Berry-Millett, Care Management of Patients with Complex Healthcare Needs, 2009, Robert Wood Johnson Foundation, 23
24 Solution: Payment reform Fee-for-service add-ons Additional payment for non-visit-based care coordination, pay for performance Fees for non-practitioner services (pay RNs, pharmacists, health coaches, panel managers) Get rid of fee-for-service Globally budget primary care practices via riskadjusted capitation Extra payments for preventive services, extended hours, high-quality and patient experience Reward primary care for reducing ED visits, hospitalizations, total health care costs 24
25 Will we succeed in reversing the adult primary care shortage? Not for a long time, if ever The only hope is for payers (Medicare, Medicaid, commercial) to partner with primary care practices to reform payment and transform the practices Pay RN care managers, pharmacists, health coaches, panel managers, and other nonpractitioner personnel for their work Pay for phone visits and e-visits needed to reduce demand for face-to-face visits 25


26 SoonerCare Health Management Program Mike Herndon, D.O. Medical Director, Health Care Management
27 SoonerCare Health Management Program Existing Health Management Program, mandated by OK legislature in 2006 Dual-Armed Approach Nurse Case Management Focuses on high-risk patients selfmanagement Practice Facilitation (PF) Focuses on practice improvement Reducing Disparities at the Practice Site (RDPS) developed through partnership with existing contractor, Iowa Foundation for Medical Care (IFMC) 8 PFs statewide No grant funds used to pay PF salaries. 60+% of grant funds go toward RDPS provider incentives 2
28 Goals of Practice Facilitation Redesign care delivery process for patients with chronic conditions by: Focusing on quality of care Focusing on office efficiency 3
29 Practice Selection for RDPS Predictive Modeling Software - MEDai Practice criteria for RDPS: 500 Medicaid members on panel 30 or > Diabetics 15 or > Minorities Not previously facilitated 4
30 How to get in the door? OHCA program coordinator calls to set up the pitch Face-to-face pitch is conducted with provider and clinic staff, OHCA program coordinator and IFMC PF manager Discuss goals of PF services, incentives, emphasize free service Acceptance select start date, do introduction with PF, get PF agreements signed 5
31 So what do PFs do? Team development Workflow redesign Involve all clinic staff, practicing at the top of their license (e.g., standing orders) Registry Deployment Establish use within office workflow Maintenance Develop resource library, educational materials PDSA cycles education, facilitation, self-assessment Stage One 5 to 6 weeks, full-time (4 days per week); weekly follow-up X 1 month, taper frequency to support sustainability Stage Two 2 to 3 weeks 6
32 Week 1 How exactly do they do it? Full assessment (self-assessment, process mapping, workflow, pain points) Identify prevalence of chronic disease and associated cost drivers (e.g., claims data, chart reviews, performance management system, and MEDai) Data findings presentation Week 2 Basic use of CareMeasures registry (or approved substitute), including data entry and Patient Care Summary (outstanding care opportunities) utilization: Processes for identifying patients, gaps and methods to close gaps Process for Patient Care Summary utilization, including who will print if practice plans to print/standing orders Additional functionalities Identify processes for data entry (data, demographics, clinical information, whose task will it be), Patient Care Summary printing and report follow up (PF will assist in initial data entry) 7
33 Week 3 How exactly do they do it? (continued) Focus on specific strategies to improve provider/patient interactions: Standing orders (discussion, policy creation, implementation) Further develop team roles Utilization of patient education resource library Schedule appropriate follow-up visit No show/no call reduction strategies Establish and begin distribution of written educational materials, including disease-specific materials Week 4 Begin assessment of care management processes (educational plan, self-management tools, community resources, tracking) and provide some introductory care management tools 8
34 How exactly do they do it? -continued- Weeks 1 through 4 Team development / job descriptions Policy and procedure development Staff education Disease-specific best practices Practice redesign principles (self-mapping, QA/QI principles, PDSA, performance monitoring) Maintain weekly one-to-one meetings with PCP including monitoring of: Satisfaction Support Provider input regarding PI processes 9
35 What are the successes? Engaged all 10 selected practices 50% of practices have embraced registry and actively utilize it High degree of receptivity and no negative feedback regarding PF Cost savings: HMP independent evaluation of 62 practices (2/1/08-6/30/09) $2.8 million aggregate savings when using Trend Line Method Improvement of 16.5% on disease management quality measures in all HMP-facilitated practices Positive, cooperative relationship with IFMC 10
36 What were Oklahoma s obstacles? Practice staff turnover Weakness of provider buy-in and leadership Registry data entry too timeconsuming Practice provider and staff capabilities education, computer literacy Unwillingness to change content not broke, why fix it? Competing initiatives REC, PCMH, PQRI, PRN, Medical Association Lack of contract flexibility to make modifications NCMs disconnected from providers/practice Program staff turnover 11
37 Lessons learned? Provider leadership and buy-in are critical Need for collaboration with other payors/initiatives No two practices are alike; there is no mold Practices with electronic medical records are more complex to facilitate Leave contract language broad allow for design flexibility Foster support within & from own agency; stay visible; PF services touch many other areas (PCMH, compliance audits, etc.) Practices are largely overwhelmed 12
38 If we had it to do all over again Develop and utilize practice application process for selection strategy Develop dual roles of a practice-level facilitator and a practice-level NCM Write contract to allow program modification for integration with other initiatives PCMH, REC, etc 13
39 Vermont Models for Improving Medicaid Primary Care Center for Health Care Strategies Webinar July 27, 2010 Susan Besio, Ph.D., Commissioner Department of Vermont Health Access (Medicaid) Vermont Health Care Reform

40 Vermont PCP Context Relatively good distribution of Primary Care Providers (PCPs) statewide 800 PCPs in 300 practices in 13 Hospital Service Areas 77% of practices have 1-5 PCPs 18% of practices have 6-10 PCPs 5% of practices have 11+ PCPs Three major health plan carriers + Medicaid + Medicare Most PCPs participate in all plans History of working together 2
41 Vermont Medicaid Strategies to Support Primary Care Medicaid Chronic Care Initiative Blueprint Integrated Medical Home Pilots Health IT Medicaid Rate Support 3
42 Medicaid Chronic Care Initiative Targeted at individuals with 1+ of 11 chronic conditions Referrals from PCPs, ERs, state human service departments, predictive modeling Individuals with high risk levels are prioritized Statewide Community-based teams of state employed RN s and Social Workers (1-5 staff in each of 8 regions; 18 total) Direct patient, primary care provider and ER contact Contract with APS Healthcare for those w/ less intense needs Telephonic Support Disease Management Coordinators: Data gathering and member education RN Health Coaches Social Worker RN Health Coaches in 2 regions 4
43 Medicaid Community Care Team Services: Develop relationships with emergency room staff Facilitate access to medical home Develop individualized holistic plans of care Optimize adherence rates to chronic disease treatment, health maintenance and screening Coordinate medical services, including behavioral health and substance abuse resources Arrange transportation to doctor s offices if necessary Attend doctor s office visits with patients as needed Provide health coaching and education Support and encouragement to make lifestyle changes Assistance with accessing community resources (housing, food and fuel assistance, etc ) 43 5
44 Medicaid CCI: Provider Benefits Supports the Providers Plan of Care for their patients Provides members with education and encouragement to self-manage their chronic conditions Reduces inappropriate use of the Emergency Room; reduces hospital admissions Gives PCP information on why patients use Emergency Room, prescription fills, etc. Provides members with support upon discharge from the hospital and link back to PCP Improves access to care by providing direct contact with RN Health Coaches and Care Coordinators Decreases no- show rates (due to higher patient engagement, transportation to appointments) 6
45 Blueprint Integrated Medical Home Pilots Multidisciplinary care support teams (CHT Teams) Local Support & population management Support general health maintenance of target population as well as care for chronic conditions Financial reform (incl. Medicaid & 3 major commercial insurers) Payment to practices based on NCQA PCMH score Conducted by UVM Shared costs for Community Health Teams State subsidizing Medicare portion Health Information Technology Web-based clinical tracking system (DocSite) Visit planners & population reports Electronic prescribing Updated EMRs to match program goals and clinical measures in DocSite Health information exchange network Community Activation & Prevention Prevention specialist as part of CHT Community profiles & risk assessments 7

 Team members move as individuals across")


46 Team supports active caseload of 5,000 patients and oversees a total of 20,000 target population Team composition varies by community (Formal Team) Team coordinates with already existing community resources (Functional Team) Team members move as individuals across practice sites Are linked via an health information infrastructure that includes EMRs, hospital data sources, a health information exchange network, and a centralized registry Designed to be flexible and scalable Costs: $350,000 per 5-FTE team (equal shares by 5 payers) 7/28/2010 8
47 Blueprint Expansion Act 128 of 2010 Moves the Blueprint to DVHA (Organizational Integration with Medicaid, Health Care Reform, HIT Responsibility) Expands the Blueprint for Health to at least two primary care practices in every hospital services area no later than July 1, 2011, and no later than October 1, 2013 to primary care practices statewide whose owners wish to participate No later than January 1, 2011, health insurers and hospitals will be required to participate in the Blueprint for Health as a condition of doing business in this state. Doctors and other health care professionals are encourages to participate 9
48 Blueprint: Provider Benefits All of the CCI Provider benefits on Slide 6, plus Provides patient registry tool for panel management of key clinical indicators Provides EHR-like clinical management tool if don t have EHR Provides support for clinical practice change (peer support, training, direct work with office staff) Provides direct access to Community Health Team and their specialists (e.g., nutrition, behavioral health) Brings Prevention Specialists into primary care setting 10
49 Vermont Medicaid PCP Payments Enhanced Payment ($150) for working with Medicaid Community Care Team Paid at Case Closure (met all goals, transferred to APS, lost, opted out) Have protected Evaluation and Management Codes at 100% of 2006 Medicare levels since of current Medicare rate Pay $5.00 pmpm to be PCP of record for a Medicaid enrollee ($5.3 million annually) Plus Blueprint Payments for NCQA Scores and support for Community Health Teams 11

50 HIT & HIE In 2005, VT authorized and funded a single statewide Regional Health Information Organization (RHIO): VITL (Vermont Information Technology Leaders), a public/private partnership, 501(c)3 Developed 1 st statewide HIE Plan, including standards based architecture for statewide HIE Medication History Pilot Project in Emergency Rooms 2007 HCR legislation: $1 m multi-payer investment in EHR adoption and deployment in small practice primary care 2008: Health IT Fund - 0.2% fee on paid medical claims for 7 years Electronic Health Records for primary care practices Development of State-wide Health Information Exchange Infrastructure 2009: Moved HIT responsibility to DVHA Division for Health Care Reform Integrates HIT and Medicaid 12


51 Blueprint Integrated Pilots Health Information Infrastructure 13
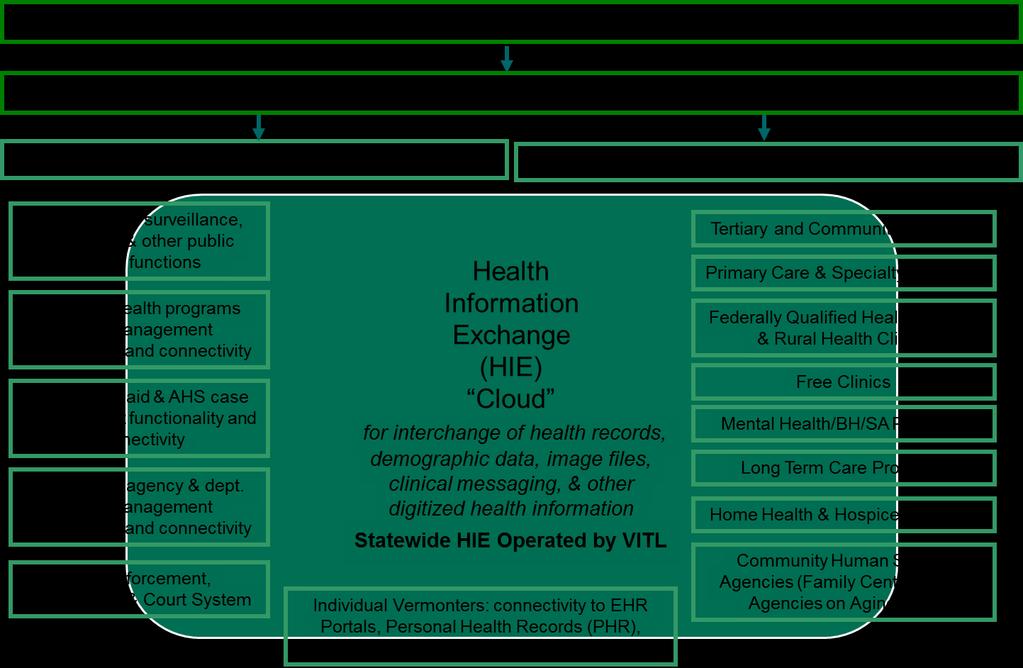
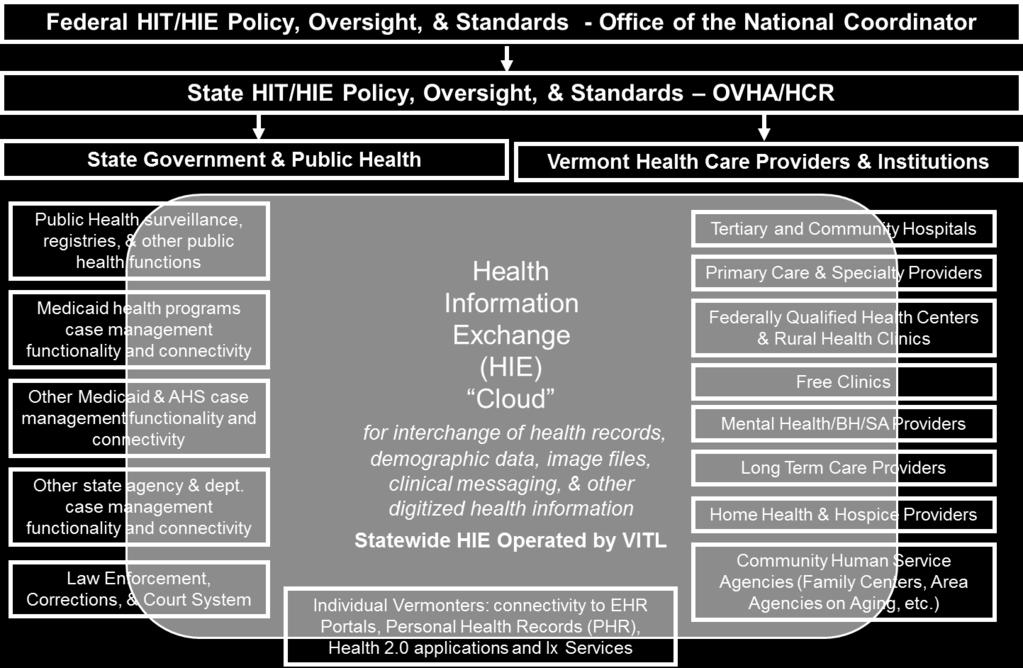
52 14
53 For More Information Medicaid Chronic Care Initiative dvha.vermont.gov/for-consumers/vermont-chroniccare-initiative-vcci Blueprint For Health healthvermont.gov/blueprint.aspx 15
Solving the adult primary care crisis: it s time to think differently
 Solving the adult primary care crisis: it s time to think differently Thomas Bodenheimer MD, MPH Center for Excellence in Primary Care (CEPC) UCSF Department of Family and Community Medicine Presenter
Solving the adult primary care crisis: it s time to think differently Thomas Bodenheimer MD, MPH Center for Excellence in Primary Care (CEPC) UCSF Department of Family and Community Medicine Presenter
The SoonerCare Health Management Program
 The SoonerCare Health Management Program National Medicaid Congress June 13, 2011 Washington, DC Dr. Michael Herndon Oklahoma Health Care Authority Mike Speight Iowa Foundation for Medical Care Why did
The SoonerCare Health Management Program National Medicaid Congress June 13, 2011 Washington, DC Dr. Michael Herndon Oklahoma Health Care Authority Mike Speight Iowa Foundation for Medical Care Why did
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Rethinking the model of primary care. Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine
 Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
Blueprint Integrated Pilot Programs
 Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Resilience Strategies for Team Care THOMAS BODENHEIMER MD, MPH CENTER FOR EXCELLENCE IN PRIMARY CARE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO
 Resilience Strategies for Team Care THOMAS BODENHEIMER MD, MPH CENTER FOR EXCELLENCE IN PRIMARY CARE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Upon completion of this educational activity, participants will
Resilience Strategies for Team Care THOMAS BODENHEIMER MD, MPH CENTER FOR EXCELLENCE IN PRIMARY CARE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Upon completion of this educational activity, participants will
Overview. Patient Centered Medical Home. Demonstrations and Pilots: Judith Steinberg, MD, MPH March 6, 2009
 Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model. The New Accountable Care Business Model
 Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
The Patient Centered Medical Home Will It Make A Difference?
 The Patient Centered Medical Home Will It Make A Difference? 2009 Population Health Colloquium Department of Health Policy Thomas Jefferson University March 2009 Michael S. Barr, MD, MBA, FACP Vice President,
The Patient Centered Medical Home Will It Make A Difference? 2009 Population Health Colloquium Department of Health Policy Thomas Jefferson University March 2009 Michael S. Barr, MD, MBA, FACP Vice President,
The Future of Delivery System Reform in Medi-Cal: Moving Medi-Cal Forward
 The Future of Delivery System Reform in Medi-Cal: Moving Medi-Cal Forward Cindy Mann Partner Manatt Health July 13, 2016 Agenda 2 Project Overview Medi-Cal Today Vision for the Future of Medi-Cal Near
The Future of Delivery System Reform in Medi-Cal: Moving Medi-Cal Forward Cindy Mann Partner Manatt Health July 13, 2016 Agenda 2 Project Overview Medi-Cal Today Vision for the Future of Medi-Cal Near
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
Medical Home Renovations: A Patient-centered Medical Home Case Study
 Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
A Journey PCMH & Practice Transformation PCMH 101. Kentucky Primary Care Association Lexington Kentucky June 11, 2014
 A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Multi-Payer Investments in Primary Care: Policy and Measurement Strategies
 Multi-Payer Investments in Primary Care: Policy and Measurement Strategies Prepared by: Center for Health Care Strategies & State Health Access Data Assistance Center July 2014 Table of Contents Introduction...
Multi-Payer Investments in Primary Care: Policy and Measurement Strategies Prepared by: Center for Health Care Strategies & State Health Access Data Assistance Center July 2014 Table of Contents Introduction...
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
SoonerCare Health Management Program 2 nd National Predictive Modeling Summit. Washington, DC.
 SoonerCare Health Management Program 2 nd National Predictive Modeling Summit. Washington, DC. Lynn Puckett Oklahoma Health Care Authority Karl Weimer MEDai, Inc., An Elsevier Company 08/28/2008 1 Agenda
SoonerCare Health Management Program 2 nd National Predictive Modeling Summit. Washington, DC. Lynn Puckett Oklahoma Health Care Authority Karl Weimer MEDai, Inc., An Elsevier Company 08/28/2008 1 Agenda
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
Healthcare Service Delivery and Purchasing Reform in Connecticut
 Healthcare Service Delivery and Purchasing Reform in Connecticut Presentation to National Association of Medicaid Directors November 9, 2011 Mark Schaefer Director, Medical Care Administration Health Purchasing
Healthcare Service Delivery and Purchasing Reform in Connecticut Presentation to National Association of Medicaid Directors November 9, 2011 Mark Schaefer Director, Medical Care Administration Health Purchasing
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
6/5/2013 7:22:00 AM Building Teams at the Associates in Internal Medicine: The Medical Huddle as a First Step
 6/5/2013 7:22:00 AM Building Teams at the Associates in Internal Medicine: The Medical Huddle as a First Step Abstract In the current model of health care delivery, the primary care physician works alone
6/5/2013 7:22:00 AM Building Teams at the Associates in Internal Medicine: The Medical Huddle as a First Step Abstract In the current model of health care delivery, the primary care physician works alone
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Health System Transformation and Modern Day Chronic Care NAMD, November Judy Mohr Peterson, Ph.D. Dir. of Medical Assistance Programs
 Health System Transformation and Modern Day Chronic Care NAMD, November 2013 Judy Mohr Peterson, Ph.D. Dir. of Medical Assistance Programs Modern Day Chronic Care: Holistic, Person- Centered, Team Based,
Health System Transformation and Modern Day Chronic Care NAMD, November 2013 Judy Mohr Peterson, Ph.D. Dir. of Medical Assistance Programs Modern Day Chronic Care: Holistic, Person- Centered, Team Based,
September, James Misak, M.D. Linda Stokes, MSPH The MetroHealth System
 Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships
 States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
A Pharmacist Network for Integrated Medication Management in the Medical Home
 A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
SNC BRIEF. Safety Net Clinics of Greater Kansas City EXECUTIVE SUMMARY CHALLENGES FACING SAFETY NET PROVIDERS TOP ISSUES:
 EXECUTIVE SUMMARY The Safety Net is a collection of health care providers and institutes that serve the uninsured and underinsured. Safety Net providers come in a variety of forms, including free health
EXECUTIVE SUMMARY The Safety Net is a collection of health care providers and institutes that serve the uninsured and underinsured. Safety Net providers come in a variety of forms, including free health
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Medical Home Summit September 20, 2011
 Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Meaningful Use of an EHR System
 Meaningful Use of an EHR System Slide content by: David Ford of CMA CalHIPSO Meaningful Use Consultant & Reena Samantaray Director of Outreach & Education, CalHIPSO July 2010 Presented by Dr. Sherellen
Meaningful Use of an EHR System Slide content by: David Ford of CMA CalHIPSO Meaningful Use Consultant & Reena Samantaray Director of Outreach & Education, CalHIPSO July 2010 Presented by Dr. Sherellen
University of California, Davis Family Practice Center: Update 2014
 University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Transformational Payment Reform: How will FQHC s survive?
 Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
State Leadership for Health Care Reform
 State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
AccessHealth Spartanburg
 TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Patient Centered Medical Home
 Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
NCQA s Patient-Centered Medical Home Recognition and Beyond. Tricia Marine Barrett, VP Product Development
 NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
PCMH and the Care of Complex High Cost Patients
 PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community. Stewards of Change June 11, 2013
 An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Patient-Centered Medical Home Best Practices: Case Study Examples
 Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Closing the Referral Loop Tool Kit: Improving Ambulatory Referral Management
 Closing the Referral Loop Tool Kit: Improving Ambulatory Referral Management A joint initiative of PCPI and The Wright Center for Graduate Medical Education July 25, 2017 Agenda Introductions Environment
Closing the Referral Loop Tool Kit: Improving Ambulatory Referral Management A joint initiative of PCPI and The Wright Center for Graduate Medical Education July 25, 2017 Agenda Introductions Environment
State Leaders: Setting the Pace Building a Transformed Health Care Workforce: Moving from Planning to Implementation
 State Leaders: Setting the Pace Building a Transformed Health Care Workforce: Moving from Planning to Implementation Daniel Derksen M.D. Director, Center for Rural Health Health Workforce Policy Academy
State Leaders: Setting the Pace Building a Transformed Health Care Workforce: Moving from Planning to Implementation Daniel Derksen M.D. Director, Center for Rural Health Health Workforce Policy Academy
MEDICAID MEDICAL HOMES PAYING ON A PER MEMBER, PER MONTH BASIS. By: Susan Price, Senior Attorney
 December 8, 2011 2011-R-0394 MEDICAID MEDICAL HOMES PAYING ON A PER MEMBER, PER MONTH BASIS By: Susan Price, Senior Attorney You asked how many state Medicaid programs using a patient-centered medical
December 8, 2011 2011-R-0394 MEDICAID MEDICAL HOMES PAYING ON A PER MEMBER, PER MONTH BASIS By: Susan Price, Senior Attorney You asked how many state Medicaid programs using a patient-centered medical
Safety Net Success: Evaluation of the Illinois Medicaid Medical Home Program. Fourth National Medical Home Summit, February 27 29, 2012
 Safety Net Success: Evaluation of the Illinois Medicaid Medical Home Program Fourth National Medical Home Summit, February 27 29, 2012 History of Illinois Health Connect Implemented in 2006; driven by
Safety Net Success: Evaluation of the Illinois Medicaid Medical Home Program Fourth National Medical Home Summit, February 27 29, 2012 History of Illinois Health Connect Implemented in 2006; driven by
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
A Care Coordination Model for Value-Based Performance Programs
 A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
Comparison of ACP Policy and IOM Report Graduate Medical Education That Meets the Nation's Health Needs
 IOM Recommendation Recommendation 1: Maintain Medicare graduate medical education (GME) support at the current aggregate amount (i.e., the total of indirect medical education and direct graduate medical
IOM Recommendation Recommendation 1: Maintain Medicare graduate medical education (GME) support at the current aggregate amount (i.e., the total of indirect medical education and direct graduate medical
Moving HIT and Meaningful Use
 Moving HIT and Meaningful Use Tim Gutshall, MD March 30, 2011 EHR Adoption in Iowa Less than 50 percent of Iowa physicians have adopted EHRs As late as 2009, 89 percent of Iowa s hospitals still used some
Moving HIT and Meaningful Use Tim Gutshall, MD March 30, 2011 EHR Adoption in Iowa Less than 50 percent of Iowa physicians have adopted EHRs As late as 2009, 89 percent of Iowa s hospitals still used some
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Brooke Salzman, MD Assistant Professor Department of Family and Community Medicine Division of Geriatric Medicine Thomas Jefferson University
 Brooke Salzman, MD Assistant Professor Department of Family and Community Medicine Division of Geriatric Medicine Thomas Jefferson University Tuesday, March 2 nd, 2010 Health Care Delivery Reform In its
Brooke Salzman, MD Assistant Professor Department of Family and Community Medicine Division of Geriatric Medicine Thomas Jefferson University Tuesday, March 2 nd, 2010 Health Care Delivery Reform In its
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Aligning Executive, Physician and Staff Compensation with Population Health Goals
 Aligning Executive, Physician and Staff Compensation with Population Health Goals WILLIAM F. JESSEE, MD, FACMPE Becker s Hospital Review 8th Annual Meeting Chicago, IL April 17, 2017 0 Welcome Today s
Aligning Executive, Physician and Staff Compensation with Population Health Goals WILLIAM F. JESSEE, MD, FACMPE Becker s Hospital Review 8th Annual Meeting Chicago, IL April 17, 2017 0 Welcome Today s
The Nursing Workforce: Challenges for Community Health Centers and the Nation s Well-being
 The Nursing Workforce: Challenges for Community Health Centers and the Nation s Well-being Jane K Kadohiro, DrPH, APRN, CDE University of Hawaii at Manoa Overview Today s nursing workforce Determinants
The Nursing Workforce: Challenges for Community Health Centers and the Nation s Well-being Jane K Kadohiro, DrPH, APRN, CDE University of Hawaii at Manoa Overview Today s nursing workforce Determinants
MAKING PROGRESS, SEEING RESULTS
 MAKING PROGRESS, SEEING RESULTS VALUE-BASED CARE REPORT HUMANA.COM/VALUEBASEDCARE Y0040_GCHK4DYEN 1117 Accepted 2 Americans are sick and getting sicker, with millions of us living with chronic conditions
MAKING PROGRESS, SEEING RESULTS VALUE-BASED CARE REPORT HUMANA.COM/VALUEBASEDCARE Y0040_GCHK4DYEN 1117 Accepted 2 Americans are sick and getting sicker, with millions of us living with chronic conditions
The Integration of Behavioral Health and Primary Care: A Leadership Perspective
 The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
HIT Innovations to Build an Empowering and Learning Culture March 2, 2016
 HIT Innovations to Build an Empowering and Learning Culture March 2, 2016 Jignesh Sheth, MD, Senior Vice President for Clinical Operations Courtney Dempsey, Clinical Innovation Specialist Conflict of Interest
HIT Innovations to Build an Empowering and Learning Culture March 2, 2016 Jignesh Sheth, MD, Senior Vice President for Clinical Operations Courtney Dempsey, Clinical Innovation Specialist Conflict of Interest
The American Recovery and Reinvestment Act: Incentivizing Investments in Healthcare
 The American Recovery and Reinvestment Act: Incentivizing Investments in Healthcare AT&T, Healthcare, and You Overview The American Recovery and Reinvestment Act of 2009 (ARRA) allocated more than $180
The American Recovery and Reinvestment Act: Incentivizing Investments in Healthcare AT&T, Healthcare, and You Overview The American Recovery and Reinvestment Act of 2009 (ARRA) allocated more than $180
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Payment and Delivery System Reform in Vermont: 2016 and Beyond
 Payment and Delivery System Reform in Vermont: 2016 and Beyond Richard Slusky, Director of Reform Green Mountain Care Board Presentation to GMCB August 13, 2015 Transition Year 2016 1. Medicare Waiver
Payment and Delivery System Reform in Vermont: 2016 and Beyond Richard Slusky, Director of Reform Green Mountain Care Board Presentation to GMCB August 13, 2015 Transition Year 2016 1. Medicare Waiver
Is your clinic upstream ready?
 Is your clinic upstream ready? Are you happy? Rishi Manchanda MD MPH @RishiManchanda Burned Out 37.5% 1 Patient Experience Hope Satisfaction Trust Outcomes Effective interventions Prevent illness Advance
Is your clinic upstream ready? Are you happy? Rishi Manchanda MD MPH @RishiManchanda Burned Out 37.5% 1 Patient Experience Hope Satisfaction Trust Outcomes Effective interventions Prevent illness Advance
Patient-Centered Primary Care
 Patient-Centered Primary Care Greg Moody, Director Office of Health Transformation July 30, 2014 www.healthtransformation.ohio.gov Agenda 1. Health System Challenges 2. Health System Trends in Primary
Patient-Centered Primary Care Greg Moody, Director Office of Health Transformation July 30, 2014 www.healthtransformation.ohio.gov Agenda 1. Health System Challenges 2. Health System Trends in Primary
Creating the Collaborative Care Team
 Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Risk Stratification for Population Health Management
 STEPS FOR SUCCESS IN Risk Stratification for Population Health Management EVERY DOCTOR HAS EXPERIENCED THE 80/20 RULE WHEN IT COMES TO TREATING THEIR SICKEST PATIENTS, says Leonard Fromer, MD, FAAFP, Executive
STEPS FOR SUCCESS IN Risk Stratification for Population Health Management EVERY DOCTOR HAS EXPERIENCED THE 80/20 RULE WHEN IT COMES TO TREATING THEIR SICKEST PATIENTS, says Leonard Fromer, MD, FAAFP, Executive
AmeriHealth Michigan Provider Overview. April, 2014
 AmeriHealth Michigan Provider Overview April, 2014 Who We Are Our Mission Dual Demonstration of Michigan AmeriHealth VIP Care Plus Agenda Our Record of Success Integrated Care Management Provider Partnerships
AmeriHealth Michigan Provider Overview April, 2014 Who We Are Our Mission Dual Demonstration of Michigan AmeriHealth VIP Care Plus Agenda Our Record of Success Integrated Care Management Provider Partnerships
Introducing AmeriHealth Caritas Iowa
 Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
All ACO materials are available at What are my network and plan design options?
 ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
The Physician s Perspective
 The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010
 The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010 This document is a summary of the key health information technology (IT) related provisions
The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010 This document is a summary of the key health information technology (IT) related provisions
Practice Facilitators - Catalyst for Medical Home Transformation
 March 27, 2012 Practice Facilitators - Catalyst for Medical Home Transformation Lyndee Knox, PhD, Vanessa Nguyen, MPH, & Diana Traje, MPH Who we are 2 LA Net a Primary Care Practice Based Research & Resource
March 27, 2012 Practice Facilitators - Catalyst for Medical Home Transformation Lyndee Knox, PhD, Vanessa Nguyen, MPH, & Diana Traje, MPH Who we are 2 LA Net a Primary Care Practice Based Research & Resource
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home
 Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
The influx of newly insured Californians through
 January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
A legacy of primary care support underscores Priority Health s leadership in accountable care
 Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
How Many Doctors, Nurses, and Other Health Professionals Do You Need?
 How Many Doctors, Nurses, and Other Health Professionals Do You Need? The Impact of New Delivery System Models on Your State s Workforce Needs? Barbara F. Brandt, PhD, Director Associate Vice President
How Many Doctors, Nurses, and Other Health Professionals Do You Need? The Impact of New Delivery System Models on Your State s Workforce Needs? Barbara F. Brandt, PhD, Director Associate Vice President
Doctor Shortage: CONDITION CRITICAL RESULTS OF HANYS 2012 PHYSICIAN ADVOCACY SURVEY
 Doctor Shortage: CONDITION CRITICAL RESULTS OF HANYS 2012 PHYSICIAN ADVOCACY SURVEY Primary care physicians are at the forefront of a physician shortage that continues to worsen in New York State, according
Doctor Shortage: CONDITION CRITICAL RESULTS OF HANYS 2012 PHYSICIAN ADVOCACY SURVEY Primary care physicians are at the forefront of a physician shortage that continues to worsen in New York State, according
Patient-Centered Medical Homes in Rural and Underserved Areas: A Webinar and Peer Discussion for Primary Care Offices
 Patient-Centered Medical Homes in Rural and Underserved Areas: A Webinar and Peer Discussion for Primary Care Offices Association of State and Territorial Health Officials (ASTHO) August 17, 2016 Dial-In
Patient-Centered Medical Homes in Rural and Underserved Areas: A Webinar and Peer Discussion for Primary Care Offices Association of State and Territorial Health Officials (ASTHO) August 17, 2016 Dial-In
Lessons Learned in Care Management. Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference
 Lessons Learned in Care Management Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference 1 Objectives: Rationale for team-based care model Lessons learned in implementing
Lessons Learned in Care Management Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference 1 Objectives: Rationale for team-based care model Lessons learned in implementing
Connecticut Department of Public Health and Community Pharmacists Medication Management Services
 Connecticut Department of Public Health and Community Pharmacists Medication Management Services MODERATOR: Marie Smith, PharmD Palmer Professor and Assistant Dean, Practice and Public Policy Partnerships,
Connecticut Department of Public Health and Community Pharmacists Medication Management Services MODERATOR: Marie Smith, PharmD Palmer Professor and Assistant Dean, Practice and Public Policy Partnerships,
Medication Management Services in Connecticut
 Medication Management Services in Connecticut Connecticut Department of Public Health, UConn School of Pharmacy and Community Pharmacies Mehul Dalal, MD, MSc, MHS - Chronic Disease Director, CT Department
Medication Management Services in Connecticut Connecticut Department of Public Health, UConn School of Pharmacy and Community Pharmacies Mehul Dalal, MD, MSc, MHS - Chronic Disease Director, CT Department
POPULATION HEALTH LEARNING NETWORK 1
 In partnership with the California Health Care Foundation (CHCF) and the Blue Shield of California Foundation (BSCF), the Center for Care Innovations (CCI) is launching a Population Heath Learning Network
In partnership with the California Health Care Foundation (CHCF) and the Blue Shield of California Foundation (BSCF), the Center for Care Innovations (CCI) is launching a Population Heath Learning Network
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS
 UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management