Completion Report. Project Number: Loan Number: 1538 March Bangladesh: Urban Primary Health Care Project
|
|
|
- Noreen Marshall
- 5 years ago
- Views:
Transcription

1 Completion Report Project Number: Number: 1538 March 2007 Bangladesh: Urban Primary Health Care Project
2
3 CURRENCY EQUIVALENTS Currency Unit taka (Tk) At Appraisal At Project Completion (15 July 1997 ) (31 January 2006) Tk1.00 = $ $ $1.00 = Tk43.65 Tk66.55 ABBREVIATIONS ADB Asian Development Bank ARI acute respiratory infection ASKS Annanya Samaj Kallyan Sangostha BAPSA Bangladesh Association for Prevention of Septic Abortion BCC behavioral change communication BWHC Bangladesh Women s Health Coalition BRM Bangladesh Resident Mission CCC Chittagong City Corporation CRHCC comprehensive reproductive health care center DCC Dhaka City Corporation EA executing agency HIV human immunodeficiency virus IA imprest account ISI integrated supervisory instrument KCC Khulna City Corporation LGD Local Government Division MSCS Marie Stopes Clinic Society NGO nongovernment organization PA partnership agreement PCC&MEC Population Crisis Control & Mass Education Committee PCR project completion report PHCC primary health care center PIO project implementation office PIU project implementation unit PSKP Progoti Samaj Kallyan Protisthan PSTC Population Services and Training Center RCC Rajshahi City Corporation TB tuberculosis bacillus UPHCP Urban Primary Health Care Project UTPS Unity Through Population Services NOTES (i) (ii) The fiscal year (FY) of the Government of Bangladesh ends on 30 June. FY before a calendar year denotes the year in which the fiscal year ends, e.g., FY2000 ends on 30 June In this report, "$" refers to US dollars.
4 CONTENTS Page BASIC DATA Map i v I. PROJECT DESCRIPTION 1 A. Introduction and Rationale 1 B. Components and Outputs 1 II. EVALUATION OF DESIGN AND IMPLEMENTATION 2 A. Relevance of Design and Formulation 2 B. Project Outputs 3 C. Project Costs 5 D. Disbursements 6 E. Project Schedule 6 F. Implementation Arrangements 6 G. Conditions and Covenants 7 H. Consultant Recruitment and Procurement 7 I. Performance of Consultants, Contractors, and Suppliers 7 J. Performance of the Borrower and the Executing Agency 7 K Performance of the Asian Development Bank 8 III. EVALUATION OF PERFORMANCE 8 A. Relevance 8 B. Effectiveness in Achieving Outcome 8 C. Efficiency in Achieving Outcome and Outputs 9 D. Preliminary Assessment of Sustainability 10 E. Impact 11 IV. OVERALL ASSESSMENT AND RECOMMENDATIONS 11 A. Overall Assessment 11 B. Lessons Learned 12 C. Recommendations 13 APPENDIXES 1. Partnership s and Overall Performance Patients Attended and Served by the Partner Agencies Service Charges and Cost Recovery Status of Establishment of Primary Health Care Infrastructure List of Training and Workshops Status of Project Support Staff, Consultant, and Logistics Disbursements of Proceeds Implementation Schedule Appraisal vs Actual Status of Compliance with Conditions and Covenants Project Benefits and Impact Updated Project Framework 48
5 Vice President Director General Country Director Team Leader Team Member L. Jin, Operations Group K. Senga, South Asia Department (SARD) Hua Du, Bangladesh Resident Mission (BRM) Jamal Mahmood, Head, Social Sector, BRM, SARD M.N. Alam, Assistant Project Analyst, BRM and, a staff consultant
6
7 BASIC DATA A. Identification 1. Country 2. Number 3. Project Title 4. Borrower 5. Executing Agency 6. Amount of 7. Project Completion Report Number B. Data 1. Appraisal Date Started Date Completed 2. Negotiations Date Started Date Completed 3. Date of Board Approval 4. Date of 5. Date of Effectiveness In Actual Number of Extensions 6. Closing Date In Actual Number of Extensions 7. Terms of Service Charges Maturity (number of years) Grace Period (number of years) Bangladesh 1538-BAN(SF) Urban Primary Health Care Project People s Republic of Bangladesh Local Government Division, Ministry of Local Government Rural Development & Cooperatives SDR29,487, May May August August September December March March June June % Disbursements a. Dates Initial Disbursement 23 June 1998 Effective Date 30 March 1998 Final Disbursement 30 January 2006 Original Closing Date 30 June 2003 Time Interval (months) 91.2 Time Interval 63.0
8 ii Category or Subloan b. Amount ($ 000) Original Allocation Last Revised Allocation Amount Added/ (Cancelled) Net Amount Available Amount Disbursed Undisbursed Balance 01 5,346 9,344 3,998 9,344 6,237 3, ,100 2,808 (6,292) 2,808 2, ,591 12,546 (3,045) 12,546 11,102 1, ,032 3, ,056 2, (93) ,965 0 (3,908) 0 0 Total 40,000 31,024 (8,919 1 ) 31,024 24,139 6, Local Costs (Financed) - Amount ($) 16,593,825 - Percent of Local Costs 66% - Percent of Total Cost 43% C. Project Data 1. Project Cost ($ 000) Cost Appraisal Estimate Actual Foreign Exchange Cost 16,980 13,421 Local Currency Cost 43,020 24,915 Total 60,000 38, Financing Plan ($ 000) Cost Appraisal Estimate Actual Implementation Costs Borrower Financed 15,520 8,323 ADB Financed 39,350 23,513 UNFPA Financed 1,020 4,238 NDF Financed 3,460 1,637 Total 59,350 37,711 IDC Costs Borrower Financed 0 ADB Financed Other External Financing 0 Total 60,000 38,336 ADB = Asian Development Bank, IDC = interest during construction, NDF = Nordic Development Fund, and UNFPA = United Nations Family Planning Assistance. 1 First partial cancellation of $6,923, on 19 February 2002, and second partial cancellation of $1,995, on 28 October Final cancellation of $6,884, during closing of account on 30 January 2006.
9 iii 3. Cost Breakdown by Project Component $ 000) Component Appraisal Estimate Actual A. Base Costs 1. Civil Works 8,100 9, Land Acquisition 4, Partnership s 15,591 11, Medical Equipment, Furniture and Vehicles 900 1, Office Equipment, Furniture and Vehicles Training and Development Consulting Services 1,080 1, Research and Benefit Monitoring and Evaluation 3,032 2, Health Education 1, Drugs, Vaccines, Contraceptive and Medical Supplies 11,700 3, Incremental Recurrent Costs 626 1,072 Subtotal (A) 48,042 33,310 B. Contingencies 1. Duty and Taxes 6,192 1, Manpower 2, Physical Contingencies 2, Price Contingencies 2,269 0 Subtotal (B) 11,308 4,401 Service Charges During Project Period Total 60,000 38, Project Schedule Item Appraisal Estimate a Actual a Selection of a survey firm August 1997 November 1998 Selection of international consultants August 1997 January 1999 Selection of engineering firm August 1997 October 1998 Demarcation of work area of partnership agreements January 1998 November 1998 Baseline survey May 1998 April 1999 Contracts for partnership agreements January 1999 July 2000 Site selection for the health care centers June 1997 January 1998 Land acquisition October 1997 January 1998 Civil works January 1998 December 1999 Management training for city corporations staff November 1998 April 2002 Financial management training April 1998 May 2002 PHC management training for partner agency staff February 1999 May 2002 Continuing training July 1999 October 2001 Recruitment of PIU staff (including consultants) November 1997 January 1998 Benefit monitoring and evaluation, and operations research October 1998 November 1998 a Denotes start date. PIU = project implementation unit; and PHC = primary health care
10 iv 5. Project Performance Report Ratings Implementation Period Development Objectives Ratings Implementation Progress From 16 September 1997 to 30 June 2005 S S S = satisfactory D. Data on Asian Development Bank Missions Name of Mission Date No. of Persons No. of Person- Days Specialization of Members a Appraisal 7 29 May d, e, f. g Inception Jun a, b Review 1 25 Sep 1 Oct a Review 2 26 Jan 1 Feb a Special Administration (SLA) May a Review Sep a SLA 2 29 Feb 1 Mar a Review Mar a Review Jun a SLA Nov a Review 6 23 Jan 2 Feb a Midterm Review May a, b Review Nov a, b Review Mar a, b Review Nov a, b Review 10 3 Apr 7 Jun a, b Review Oct a, b Review 12 1 Apr 5 May a, b Review Sep 12 Oct a, b Review Jun a, b Project Completion Review Sep a, b, c a Specializations of mission members are as follows: a - project specialist, b - project analyst, c - staff consultant, d- social sector specialist, e - economist, f - health specialist, and g - counsel.

11 v
12
13 A. Introduction and Rationale I. PROJECT DESCRIPTION 1. The health status of the urban poor in Bangladesh has worsened, due to severe poverty and lack of primary health care facilities and resources. The Government of Bangladesh, with assistance from the Asian Development Bank (ADB), prepared the Urban Primary Health Care Project 3 (the Project) in 1997 to sustainably improve the health of the urban poor, particularly poor women and children. The project design emphasized (i) delivery of primary health care services through public-private partnership; (ii) strengthening of urban primary health care infrastructure; and (iii) capacity building of the health departments of the major city corporations to plan, finance, budget, monitor and supervise primary health care service delivery. The Project covered the city corporations of Chittagong, Dhaka, Khulna, and Rajshahi, and particularly the slums located in populous areas inhabited by poorer city dwellers (see Project Map). The Project started in March 1998 on a pilot basis and completed on 30 June The Project was prepared following the recommendations of ADB s health and population sector assistance strategy, including area-specific interventions, long-term resource commitments, increased efficiency, complementarities among concerned aid donors, publicprivate partnership, and a concentration on high-risk groups such as the urban poor, and particularly women and children. The primary objective of the Project was to improve the health of the urban poor and reduce mortality and morbidity, especially among women and children, by increasing access to quality primary health care services. B. Components and Outputs 3. The Project comprised four components: (i) provision of primary health care through partnership agreements, (ii) strengthening the urban primary health care infrastructure, (iii) building capacity of city corporations and their partners, and (iv) support for project implementation and operationally relevant research. 1. Provision of Primary Health Care through Partnership s 4. This component included delivery of essential primary health care services through contracted nongovernmental organizations (NGOs) or private providers via competitive partnership agreements. The primary health care service packages were: (i) immunization; (ii) micronutrient support, particularly vitamin A; (iii) family planning; (iv) prenatal, obstetrical, and postpartum care; (v) systemic case management of pneumonia and diarrhea in children; (vi) case management of tuberculosis (TB) and reproductive tract infections in adults; (vii) health education on selected project-related topics; and (viii) support to victims of violence against women. The Project targeted delivery of primary health care services in the slums and densely populated areas of the four city corporations, divided into 16 partnership agreement areas, each covering an estimated 300, ,000 people. 2. Strengthening the Urban Primary Health Care Infrastructure 5. This component included provision for establishment of 183 new primary health care 3 ADB Report and Recommendation of the President to the Board of Directors on a Proposed to the People s Republic of Bangladesh for Urban Primary Health Care Project. Manila ( No.1538-BAN [SF] for $70.0 million, approved on 16 September 1997).
14 2 centers (PHCC) and 7 comprehensive reproductive health care centers (CRHCC) in newly constructed multi-story buildings and in rented buildings, with the necessary equipment and furniture. While the respective city corporations would retain ownership of the primary health care infrastructure, the facilities would be used by the contracted partner agencies and serve approximately 50,000 people per center. Clinics were to be established on the second floors, with the ground floors rented to earn income to support proper upkeep of each of the newly constructed centers. 3. Building the Capacity of the City Corporations and Partner Agencies 6. The Project provided several capacity-building measures to sustain improvements in primary health care by strengthening the capacity of the local government in general and reorganizing the health departments of the four city corporations in particular to plan, finance, budget, monitor and supervise urban primary health care services. The capacity-building measures included: (i) establishing dedicated units within each city corporation to handle these functions;(ii) training in specific urban primary health care topics; (iii) fellowships in primary health care management, health finance, and health management information systems; (iv) study tours; (v) systematic supervision using an integrated supervisory instrument (ISI); (vi) training of city corporation supervisors in the use of the ISI; and (vii) informational seminars and training for the partner agencies. 4. Support for Project Implementation and Operationally Relative Research 7. The Project also provided support for establishment and management of a project implementation unit (PIU) within the Dhaka City Corporation (DCC), headed by a project director, and project implementation offices (PIOs) in each of the Chittagong, Khulna, and Rajshahi city corporations. The Project also supported operationally relevant research to test new interventions that could be added to the primary health care service packages. II. EVALUATION OF DESIGN AND IMPLEMENTATION A. Relevance of Design and Formulation 8. The project design was relevant to ADB s operational strategy in Bangladesh, which addressed the overarching objective of poverty reduction through provision of social services, focusing on primary health care, family planning, and nutrition to improve health conditions. The project design was consistent with ADB s urban sector strategy, focusing on (i) restructuring institutional and fiscal relations between government and city corporations; (ii) improving management capability at city corporation level; (iii) poverty reduction-related investments; and (iv) increased investment in urban infrastructure facilities and services, with particular focus on the urban poor, slum dwellers, and the squatter population. 9. The project design was also relevant to the five principles of the ADB health and population sector strategy (1995) for Bangladesh, including: (i) improvement in the management of the health care system; (ii) greater involvement of the private sector, including the NGOs; (iii) increasing the resources devoted to recurrent costs; (iv) improving the skills of health workers; and (v) increasing the use of cost-recovery mechanisms. The ADB health and population sector strategy recommended: (i) having a clear thematic focus and concentrating on a specific area, rather than trying to do everything; (ii) making a long-term commitment of resources to the areas the government and ADB decide to invest in; (iii) encouraging innovation as a means to increase efficiency; (iv) complementing the work of other aid agencies; and (v) concentrating on
15 3 high-risk groups such as the urban poor, and particularly women and children. The health and population sector strategy recommended an investment in urban primary health care as an urgent priority. 10. The project design was also relevant to the government s major development priorities of reducing population growth and increasing the commitment to provide access to primary health care, family planning and safe delivery, and maternal and child care. The project design was relevant to the government s health and population sector strategy, which formed the basis of the national health policy, and which included: (i) an emphasis on client needs, especially those of women; (ii) increasing the quality, efficiency, and equity of services; (iii) an essential health service package, with emphasis on preventive interventions and activities related to maternal and child care; (iv) an increased role for the private sector, including the NGOs; (v) provision of one-stop service for health and population services; and (vi) increased attention to cost recovery and higher efficiency of resource utilization in the public sector. 11. The project design was sound and replicable; the relevance of the project design did not change between appraisal and completion, as indicated by the adoption of the same design by a subsequent similar project. The project was designed with extensive stakeholder participation and ownership. B. Project Outputs 1. Provision of Primary Health Care through Partnership s 12. Through a competitive bidding process the Project concluded 16 partnership agreements (10 in Dhaka, 3 in Chittagong, 2 in Khulna, and 1 in Rajshahi city corporations) with nine local NGOs and the Chittagong City Corporation for provision of primary health care services. The innovative partnership between the public and private sector in providing primary health care services proved satisfactory in reaching the poor particularly women and children with quality services. The project monitoring and evaluation system assessed the performance of the partner agencies using common health-related performance indicators, and was found to be satisfactory. The partnership agreements, area demarcations, and an assessment of their overall performance are in Appendix 1. The partner agencies provided million different services to 6.16 million patients, including attending 29,915 child deliveries (19,483 normal deliveries and 10,432 caesarian sections). In addition, million people were covered under the behavioral change communication (BCC) program by the partner agencies. Distressed women who were victims of violence received psychological, physical, and legal assistance from the centers. Details are in Appendix The partner agencies provided a range of primary health care services covering the following areas: (i) reproductive health care, safe motherhood, contraception and reproductive tract infections; (ii) maternal and child health care; (iii) vaccinations; (iv) management of common and minor diseases and injuries; (v) control of endemic diseases including tuberculosis, pneumonia, and diarrhea; (vi) nutrition-related services (e.g., counseling, growth monitoring, micronutrient supply); (vii) diagnostic services; (viii) management of emerging problems (such as dengue and AIDS 4 ); (ix) health education, behavioral change communication and adolescent health; (x) violence against women; and (xi) normal and caesarian section child deliveries. The services were provided at subsidized rates approved by the respective city 4 Acquired immunodeficiency syndrome
16 4 corporations. The service charges were nominal and much cheaper than prevailing market rates, so that the poor could avail the services. Details are in Appendix 3, Table A In addition to highly subsidized rates (paid by 51.0% of patients), 23.7% patients received services at no cost, and 25.3% at partial cost. Details are in Appendix 3, Table A Despite providing subsidized, no-cost and partial-cost services, the Project attempted to attain partial cost recovery. The level of cost recovery attained by different partner organizations varied, depending on the location, economic profiles of the patients, and volume and efficiency of operation of the individual partner agencies. The cost recovery varied from 3% to 31%. The cost per patient also varied for different partner agencies (from Tk76 to Tk212). Details are in Appendix 3, Table A Strengthening the Urban PHC Infrastructure 16. The Project established 180 health care centers (163 PHCCs and 17 CRHCCs), equal to 95% of the 190 centers (183 PHCCs and 7 CRHCCs) envisaged at appraisal. Considering the lack of land in suitable locations, particularly in the DCC area, the midterm review revised the original appraisal projection calling for establishment of 143 centers in constructed buildings and 47 centers in rented buildings. Details are in Appendix 4, Table A4.1 and Table A4.2. Ultimately, 125 centers (116 PHCCs and 9 CRHCCs) were established in constructed buildings and the remaining 55 centers (47 PHCCs and 8 CRHCCs) were established in suitable privately owned rented buildings. Details are in Appendix 4, Table A Initial plans called for the PHCCs and CRHCCs to be located in two-story buildings constructed with foundations suitable for four-story buildings, thus providing for possible vertical expansion. The plan provided for renting the ground floors to generate income for the centers, with the first floors used for health care and maternity services. Renting the ground floors proved unsuitable, and the space was instead used by the centers for service delivery. Each PHCC and CRHCC was provided with the necessary furniture and equipment. In addition, the partner agencies established 662 satellite clinics to extend services into the immediate neighborhoods of the people being served, especially slum dwellers. Furthermore, public toilets were constructed at 36 significant public places in the DCC to improve the fragile environmental sanitation facilities. Details are in Appendix 4, Table A In all, 125 primary health care centers were established on land owned by the respective city corporations, with no need for land acquisition, resettlement and payment of compensation. Although the respective city corporations own the infrastructure, the concerned partner agencies contracted the use of the centers, through partnership agreements, to serve the catchments population. An engineering consultant firm was engaged for design and construction supervision of the civil works. 3. Building the Capacity of the City Corporations and their Partners 19. Several capacity-building measures were undertaken for building the capacity of the four city corporations in general, and their health departments in particular, to plan, finance, budget, monitor and supervise primary health care services. The capacity-building measures included: (i) establishing dedicated units within each city corporation to handle these functions; (ii) training in specific topics in urban primary health care; (iii) fellowships in primary health care management, health finance, and health management information systems; (iv) study tours; (v) systematic supervision using an ISI; (vi) training of city corporation supervisors in the use of ISI;
17 5 and (vii) informational seminars and training for the partner agencies. Training and workshops conducted under the Project are listed in Appendix Major training activities included: (i) management training for all staff and financial management training for relevant staff of the health departments of the four city corporations, (ii) management training followed by refresher training for city corporation health department staff, and (iii) primary health care management training followed by refresher training for staff of the partner agencies. The management training for the health department staff of city corporations included: (i) general management of partnership agreements; (ii) strength, weakness, opportunity, and threat analysis; (iii) project planning cycles; (iv) project logical framework; and (v) ISIs. Financial management training was also arranged for the staff of the partner agencies. Training for partner agency staff on management of primary health care included (i) guidelines for service delivery; (ii) TB management for paramedics, laboratory technicians, counselors, and training of trainers; (iii) control of diarrheal disease; (iv) acute respiratory infection (ARI) management; (v) management of an expanded program of immunization (EPI); and (vi) training on breastfeeding and nutrition. The Project also provided refresher training, particularly with respect to management, monitoring and supervision, for the staff of city corporations and partner agencies. In addition, the Project provided study tours and fellowships. 4. Supports for Project Implementation and Operationally Relative Research 21. The Project provided implementation support for establishing a PIU in the DCC and PIOs in the Chittagong, Khulna, and Rajshahi city corporations. The implementation support included necessary incremental project staff, vehicles, office equipment, furniture, medical equipment and accessories and drugs, and selected program operating costs. Details are in Appendix The Project carried out six operationally relevant research projects through reputable research institutes and agencies, and tested new interventions to include in the primary health care service packages. The research topics were: (i) Improved Hygiene Education (conducted by the National Institute of Preventive and Social Medicine); (ii) Community Based Safe Motherhood and Improved Weaning Practices (conducted by the Institute of Child and Maternal Health); (iii) Violence Against Women, and Effectiveness of HIV Vaccine (conducted by the International Center for Diarrheal Disease Research, Bangladesh); and (iv) Algorithm for Sexually Transmitted Disease (STD)/Reproductive Tract Infection (RTI) (conducted by the Obstetrical and Gynecological Society of Bangladesh). The outcome of the six research projects provided valuable findings and recommendations that would be useful in future expansion of the scope of primary health care services, in formulating future primary health care policies and plans, and in planning similar programs. The recommendations were implementable and cost effective, and relevant to the critical needs of primary health care services. 23. The Project undertook an extensive program of health education and BCC and produced a variety of promotional materials, including stickers, posters, newsletters/bulletins, billboards, hoarding, bus panels, street dramas, folk songs, film-shows, TV spots, a service delivery guidebook, a health workers guidebook, an exhibition and workshop, and electronic and print media advertisements. C. Project Costs 24. The total project cost was estimated at $60.0 million equivalent, with $17.0 million (28.3%) in foreign currency and $43.0 million equivalent (71.7%) in local currency. The actual
18 6 cost at project completion was $38.3 million equivalent, including a foreign currency cost of $13.4 million (35%) and local currency cost of $24.9 million equivalent (65%). The actual expenditure for both foreign currency and local currency was reduced by 21% and 42% respectively. The ADB loan amount under the Project was $40.0 million, of which million (60%) was utilized, for a loan savings of $15.86 million. The loan savings were due to the low recruitment cost of local NGOs rather than international NGOs; saving from drugs, vaccines, contraceptives, and medicines (which were mostly included in the partner agency budgets); and appreciation 5 of the US dollar against the Bangladeshi taka. The unspent loan amount ($15.86 million) was cancelled. 6 D. Disbursements 25. Out of the total ADB loan of $40.0 million, $24.14 million equivalent was disbursed by loan closing. Of the total amount disbursed, $7.55 million was in foreign currency and the remaining $16.59 million equivalent in local currency. Analysis of the disbursement schedule shows that the disbursement schedule at appraisal was realistic, as it was very close to actual disbursements, indicating smooth fund flow for project implementation. An imprest account was established for the project loan funds and statement of expenditure procedures was followed. The imprest account and statement of expenditure procedures aided in smooth project implementation. The turnover of the imprest account was satisfactory, with a ratio of 2.6. Disbursements in both $ and SDR are in Appendix 7. E. Project Schedule 26. The loan agreement was signed on 23 December 1997 and became effective on 30 March There was an initial delay of about 18 months to start project implementation, because responsibility for primary health care services had not be assigned to the respective city corporations by the Ministry of Health and Family Welfare, a situation beyond the control of the executing agency (EA). Consequently, engagement of the partner agencies was delayed. However, the Project was extended for a total of 24 months and all targeted activities were satisfactorily completed. Details are in Appendix 8. F. Implementation Arrangements 27. The EA for the Project was the Local Government Division (LGD) of the Ministry of Local Government, Rural Development and Cooperatives. LGD executed the project implementation through the four city corporations and provided overall guidance and coordination. The DCC was the main implementing agency; the three other city corporations were associate implementing agencies. A PIU headed by a project director was established at Dhaka with 59 staff (Appendix 6, Table A6.1). Four deputy project directors (one from each of the four city corporations) assisted the project director from the PIOs of the respective city corporations. The PIU was responsible for implementing the activities of the Project. 28. A project steering committee was constituted with the LGD Secretary as chairperson, project director as member-secretary, and members from the Ministry of Health and Family Welfare, Economic Relations Division, Implementation Monitoring Evaluation Division, Planning 5 At appraisal $1=Tk43.65, while at completion (as of loan closing on 30 January 2006) $1=Tk 66.55, for an increase of 52%. 6 First cancellation of $6,923, on 19 February 2002, second cancellation of $1,995, on 28 October 2002, and final cancellation of $6,884, on 30 January 2006.
19 7 Commission, NGO affairs bureau, NGOs, Ministry of Women and Children Affairs, and representatives of the four city corporations. The steering committee met regularly as needed and provided necessary guidance and policy decisions to the Project. 29. In addition, a project implementation coordination committee was established headed by the chief health officer of the DCC. Other members of the coordination committee were the chief health officers of the other three city corporations, the directorate of heath services, the directorate of family welfare, and the local government division, with the project director serving as member secretary. The project coordination committee ensured necessary implementation coordination and oversaw the day-to-day activities of the Project. The PIU implemented the Project with assistance of the steering committee, coordination committee, concerned agencies, partner agencies, consultants, and research organizations. G. Conditions and Covenants 30. The conditions and covenants were generally complied with. The conditions and covenants were realistic and achievable, although there were delays in meeting a few conditions and covenants. Reorganization of the city corporation health departments could not be completed during the project period because the Ministry of Establishment and Ministry of Finance did not issue the necessary approvals; the reorganization plan is being pursued under the on-going second phase of the urban primary health care project (UPHCP). Details are in Appendix 9. H. Consultant Recruitment and Procurement 31. Goods and services were procured following ADB s Procurement Guidelines (April 2006, as amended from time to time) and the ADB Guidelines for Use of Consultants (April 2006, as amended from time to time). The Project did not experience any major problems or difficulties related to procurement. I. Performance of Consultants, Contractors, and Suppliers 32. There was no separate technical assistance for advisory consulting services under the Project. However, 79 person-months of international and 164 person-months of domestic consultant services were utilized under the loan. The performance of the consultants was generally satisfactory. The performance of the civil works contractors and the suppliers of furniture, office equipment, medical equipment, chemicals, and vehicles were also generally satisfactory. J. Performance of the Borrower and the Executing Agency 33. The performance of the Borrower was satisfactory. The Borrower made available necessary counterpart funds in time and responded quickly and positively to specific recommendations made by ADB for accelerating project implementation. 34. The performance of the EA, including the four city corporations, was also satisfactory, as they successfully implemented all project components. The EA implemented the Project with the necessary cooperation and assistance of the directorate general health services, directorate general family welfare, partner agencies, local leaders and elite, and participation of the beneficiaries. The EA responded quickly to ADB s requests and recommendations and assisted the review missions. The EA was responsive with respect to site selection, design and approval,
20 8 construction, benefit monitoring and evaluation, operation and maintenance of the primary health care centers and facilities through the partner agencies, and ensuring delivery of quality primary health care services to the poor urban population, especially women and children. K. Performance of the Asian Development Bank 35. ADB s performance was satisfactory. ADB fielded 19 missions, including 15 review missions on regular (as needed) intervals to closely review and assess progress; problems and constraints relating to implementation were identified through field visits and discussions with the Borrower, EA, consultants, and other stakeholders, including the beneficiaries. ADB s Bangladesh Resident Mission (BRM) closely monitored project implementation and promptly acted on requests for approval, disbursements, changes and modifications as needed from time to time. ADB closely followed up with the government on policy maters to comply with important loan covenants. The Borrower and the EA highly appreciated the support and assistance provided by ADB, and particularly the BRM. III. EVALUATION OF PERFORMANCE A. Relevance 36. The project design was highly relevant as it addressed the critical issue of primary health care for the urban population, comprising poor slum and squatter dwellers who lacked necessary health care services. The project interventions addressed fragile urban primary health care facilities, enhanced their outreach and servicing capability, and ensured wide coverage of the essential primary health care needed by poor women and children. The positive impact on and popularity of the Project among the poor urban population led to a request by the government for a second phase, following essentially the same design adopted in the Project; the second phase has been approved by ADB. 37. The project design remained relevant to ADB s country operational strategy addressing overarching poverty reduction through the delivery of social services such as primary basic health care, family planning, and nutrition, especially in the urban sector, where hundreds of thousands of poor women and children live in slums and squatter settlements with no health care facilities and services. The project design was also highly relevant to ADB s overall health sector strategy, which continued to emphasize the importance and cost effectiveness of investment in primary health care. The overall strategy also continued to be based on improvement of the management of health care systems and the skills of health workers, participation of the private sector, increased emphasis on recurrent costs, and increasing focus on cost-recovery. The project design was relevant to the government development and health sector strategy to expand access to primary health care, family planning and safe child delivery, and child and maternal care with emphasis on client needs, quality and efficiency of services, cost-recovery, and resource mobilization. B. Effectiveness in Achieving Outcome 38. The Project was effective in achieving its intended outcomes, which comprise: (i) effective public private partnership for delivery of primary health care in a sustainable and costeffective manner, (ii) expansion of access to quality urban primary health care services through strengthening of urban primary health infrastructure, (iii) building the capacity of the city corporations and partners, and (iv) providing implementation support and conducting operationally relevant research. The Project established effective partnerships between the city
21 9 corporations and partner agencies through partnership agreements and proved that delivery of quality primary health care services, particularly among poor urban women and children, is both feasible and cost-effective. The partner agencies have satisfactorily operated primary health care centers and served 6.16 million patients with million services. In addition, million people were covered by a BCC program. The Project s external monitoring evaluation found that the partner agencies performed satisfactorily. 39. The project implementation mechanism proved effective in achieving the outcome of expanding access to affordable quality primary health care services through establishment of 180 primary health care centers. Each center was equipped with necessary furniture, office equipment, medical equipment and accessories, chemicals, and drugs. Professionals and experienced health service providers run the centers under the management of the partner agencies. The expanded access has proven effective and beneficial, especially to poor urban women and children. In addition to providing primary health care services and drugs at subsidized rates, poor patients were served at no charge, or charged only a portion of the already subsidized rates; without these low-cost services, the poor might not have had access to any medical treatment. 40. Service delivery at the primary health care centers was effective, with the centers providing user-friendly services for almost all major primary health care services. The centers also established an effective referral system to appropriate hospitals and clinics. The project completion review mission met a number of patients during field visits and gathered that the patients have high confidence in the facilities and services of the primary health care centers in terms of health center management, patient management, affordable cost of services and drugs, cleanliness, and quality of services. 41. The project implementation was effective in terms of building the capacity of city corporations, and particularly their health departments. In addition to organizational restructuring and delineation of responsibilities between city corporations and the health services and family welfare directorates, the Project made significant institutional and management improvements, especially with respect to planning, finances, budgeting, monitoring, and collaboration with private health care service providers. A dedicated unit has been established under each city corporation that is capable of handling these functions effectively. Provisions for training, fellowships, study tours, etc. were effective in building the capacity of the city corporations to operate the primary health care centers and sustainably deliver services under the publicprivate partnership arrangements established under the Project. 42. Project implementation was effective in undertaking operationally relevant research. The Project contracted six relevant research projects to four reputable research institutions and agencies. The research outputs produced were of high quality, and added new interventions to the primary health care service packages, including: (i) introduction of new vaccines, (ii) means for improving personal hygiene, (iii) community-based safe motherhood services, (iv) means for improving weaning practices, and (v) means of preventing violence against women and reproductive tract infection. The research outputs may also serve as a basis for further research and innovation on primary health care services. C. Efficiency in Achieving Outcome and Outputs 43. Project implementation was efficient in achieving the intended outcome of providing cost-effective quality primary health care services to the urban population, especially poor and disadvantaged women and children, through public-private partnership. The Project succeeded
22 10 in expanding access to primary health care services by constructing and renting infrastructure and establishing capable and dedicated primary health care units in the city corporations. In addition, the Project strengthened the capacity and skills of the partner agencies to effectively and reliably offer affordable good quality primary health care services directly to the poor. 44. The primary health care infrastructure established under the Project will continue to serve the need of the poor and disadvantaged, especially the women and children. The Project served over 6.16 million people with million services, including 3.02 million poor and disadvantaged, and targeted million people through BCC. Each center served an average of 85,550 patients per year (171% more than the target of 50,000). The project completion review survey found that the beneficiary patients who had received services from the primary health care centers benefited from and were satisfied with the quality of services. The survey also found a reduction of morbidity and maternal and child mortality in the catchment areas. 45. The public-private partnership proved to be an effective and replicable mechanism for ensuring expanded access to quality primary health care to the urban population, particularly poor women and children. The approach is cost-effective for the government (costing less than general health services), partner agencies (with technical and financial support from government), and the urban population (who receive quality health care close to where they live, on an affordable, reduced- or no-cost basis). 46. During the Project, vitamin A supplementation among children aged 6 months to 6 years increased from 26.0% in 2001 to 92.0% in Visits by professional health workers to women who had become pregnant during the preceding 12 months increased from 18.0% in 2001 to 97.8% in Mothers of under-5 children who knew at least three signs and symptoms of acute respiratory infection requiring referral increased from 45.0% in 2001 to 55.9% in Mothers with under-5 children who knew how to correctly prepare oral rehydration solution increased from 65.0% in 2001 to 95.0% in The contraceptive prevalence rate among married women of reproductive age (15 49) increased from 38.0% in 2001 to 88.6% in 2006, while the number of married women who knew at least three modern contraceptive methods increased from 34.0% in 2001 to 84.0% in Women who had delivered children in the preceding 12 months and were attended by a trained health worker increased from 22.0% in 2001 to 97.8% in Distressed women who were the victims of violence received psychological, physical, and legal assistance from the partner agencies through the centers. Use of iodized salt by slum households increased from 44.0% in 2001 to 95.8% in Details are in Appendix 10. D. Preliminary Assessment of Sustainability 47. The Project is likely to be sustainable as demonstrated by the commitments made by the EA and partner agencies, the skills gained by their staff in the area of primary health care services, and patient satisfaction with and confidence in services. Sustainability is further ensured through (i) a supportive government policy for private sector involvement, through public-private partnership; (ii) the emphasis, in government policy, on primary health care for the urban population and increasing public investment; and (iii) increased budgetary allocations and donor support for urban primary health care. 48. The partner agencies have gained considerable management skills. Health workers have demonstrated their skills and capability by expanding outreach to almost double (171%) the number of patients targeted, thereby helping to ensure Project sustainability, which is highly dependant on the interest and commitment of the partner agencies. All the partner agencies
23 11 have demonstrated their continued interest, commitment, and involvement and have continued to successfully manage the primary health care centers and deliver quality primary health care services following Project completion on 30 June Sustainability has further enhanced due to the design and implementation of a follow-up project with participation of most of the existing partner agencies. E. Impact 49. The Project significantly impacted poverty by improving the health condition of the urban population, through a combination of awareness raising and quality primary health care services provided at affordable, reduced, or no cost; services included immunization, family planning, maternal and childcare, and general health and nutrition. The final project household survey indicated a reduction in maternal mortality from 2.6 in 2001 to 2.2 in 2006 (per 1,000 deliveries); under-5 child mortality also dropped during the project period, from 83.4 in 2001 to 74.3 in 2006 (per 1,000 live births). Infant mortality was reduced from 66.6 in 2001 to 62.0 in 2006 (per 1,000 live births). The incidence of several chronic diseases was also considerably reduced during the Project, as a result of preventive measures that resulted in reduced morbidity. Details are in Appendix The Project created employment for a large number of people particularly health workers, trained birth attendants and technicians employed with the PHCCs and CRHCCs. The income of patients increased indirectly, through longer work hours (due to reduced illness), better health conditions, and longer life. The patients also saved time and money by having access to quality health care services close to their homes. The beneficiary households also saved money through access to health care at below-market rates. 51. The Project s institutional impact included strengthening the health departments of the city corporations, in terms of (i) their capacity for planning, finance, auditing, and monitoring and evaluation; and (ii) their experience and skill in providing primary health services through publicprivate partnership with private service providers. 52. The Project supported the city corporations in eradicating filaria, malaria, dengue, and other mosquito-borne diseases. Improvements in the overall environmental (e.g. general cleanliness) of the urban areas, particularly the slums and squatter settlements, contributed to reduction of the incidence of several diseases. 53. The Project significantly impacted the primary health, family welfare, and nutrition of the urban population, and particularly women and children. The Project achieved improvements in a number of primary health care indicators. The mortality of under 5 children reduced from 83.4 in 2001 to 74.5 in 2006 (per 1,000 live births), and infant mortality dropped from 66.7 in 2001 to 62.4 in 2006 (per 1,000 live births). Immunization of children (aged months) increased from 53.0% in 2001 to 81.8% in The percentage of women who were pregnant in the preceding months and had received tetanus toxoid vaccine at least twice increased from 54.0% in 2001 to 90.6% in Details are in Appendix 10. IV. OVERALL ASSESSMENT AND RECOMMENDATIONS A. Overall Assessment 54. The Project was implemented as conceived at appraisal, without any major changes in the objectives, components, implementation procedures, and monitoring and evaluation system.
24 12 The difficulty in obtaining the necessary land for establishment of primary health care centers in new buildings caused the Project to also establish centers in privately-owned, rented buildings. The design for providing primary health care services among the urban population through public-private partnership proved satisfactory, and the follow-up project has adapted the same design and approach. 55. The Project closely monitored performance, including performance of the partner agencies, project outputs, outcomes, and impacts, through an external monitoring agency, following the ADB Handbook on Benefit Monitoring and Evaluation and using objectively verifiable indicators. The monitoring was carried out at various stages (at baseline survey, midterm, and the end of the Project). An updated project framework in Appendix 11 provides more detail. 56. The Project design was (i) highly relevant, effective and efficacious in achieving the outcomes; (ii) efficient in achieving outcome and outputs; and (iii) likely sustainable: it significantly impacted on poverty through improvement of the health condition, reduction of mortality and morbidity, and improvement of the nutrition status of the urban poor, and particularly women and children. The Project design and implementation were sound, replicable, and in high demand by the urban population, as demonstrated by the implementation of the ongoing follow-up project; most target outputs and outcomes have been met (see updated project framework in Appendix 11). The Project is therefore, rated as successful. B. Lessons Learned 57. Public-private partnerships for primary health care service delivery among the urban poor, and particularly women and children, proved to be a replicable, effective, and innovative approach. 58. Pro-poor targeting is difficult without necessary and adequate provisions and safeguards in the bidding process for selection of partner agencies. 59. Site selection is often constrained when striking a balance between the availability of land and the suitability of the site, in terms the ease of access by poor women and children, which varies with proximity to slums and squatter settlements and other health service facilities. The design of existing urban primary health care centers, particularly the CRHCCs, should be improved with respect to layout and internal arrangements, so as to make them more patient friendly. 60. There is a need for increased awareness among catchment area residents regarding the availability of primary health care facilities and services, so as to maximize utilization of infrastructure. 61. Efficient cash and fund flows are essential for smooth operation of the partner agencies. 62. Depreciation of local currency can generate huge funding surpluses. 63. Coordination among local government agencies, the Ministry of Health and Family Welfare, and other concerned stakeholders needs to be further improved.
25 13 C. Recommendations 1. Project-Related 64. Land is scarce within the major city corporation areas. When establishing health-related infrastructure in new buildings, greater emphasis should be placed on undertaking rigorous public consultations and surveys, considering among others factors (i) the economic profile of the majority of the population, (ii) the vicinity of slums and squatters, (iii) the distance from other health service facilities, and (iv) accessibility. 65. The existing design of the primary health care infrastructure, and particularly the internal arrangements, should be improved, so as to increase the utilization of space, improve convenience for both patients and staff, and provide suitable locations for an operating theatre and labor room, medicine stores, toilets, stairs, ramp, waiting room, etc. The existing maternity area should be placed on the ground instead of the second floor, to facilitate access to the critical patients admitting labor room and operation theatre, in the absence of elevators. Provision should be made for a ramp in addition to stairs on the landing from the ground floor, for use of wheel chairs and trolleys by the disabled. The health center design should provide a healthy environment, with adequate ventilation (using fresh air) and natural light. The design should maintain a provision for future vertical expansion, given the increasing demand for both indoor and outdoor services. 66. The partner agencies should be given a minimum target for reaching the poor (say 30% of target poor people of the catchments area), as contractual disincentives may otherwise be invoked under the partnership agreement. Monitoring and evaluation of inputs, outputs, outcomes, and impact should be disaggregated by economic status. 67. In the future, similar projects may include increased provisions for professional consultation, diagnosis (including common laboratory tests), and supplies of essential drugs. 68. The project performance evaluation report may be prepared in mid Approval and implementation of the reorganization of the city corporations health departments should be ensured through close monitoring under the ongoing second phase. 70. In the future, similar programs should include special activities for awareness raising about the availability of health care facilities. 71. In the future, similar programs should have flexible disbursement mechanism to ensure smooth flow of funds to the partner agencies. 72. Future project designs should include mechanisms to avoid start-up delays, and adopt flexible provision for utilization of surplus funds that accrue for various reasons (including in particular exchange fluctuations), to ensure full utilization of project funds and delivery of needed services to beneficiaries. 2. General 73. Providing urban primary health care services through partnership agreements proved to be a sound, feasible, innovative, and replicable approach, which should be continued as an alternative primary health care service delivery mechanism, and expanded in other urban areas.
26 14 Appendix 1 PARTNERSHIP AGREEMENTS AND OVERALL PERFORMANCE Table A1.1: Partnership s and Areas of Operation Partner Agency Partnership Catchments Areas A. Dhaka City Corporation (DCC) 1. Bangladesh Women s Health Coalition (BWHC) 2. Bangladesh Women s Health Coalition (BWHC) 3. Bangladesh Association for Prevention of Septic Abortion (BAPSA) 4. Population Services and Training Center (PSTC) DCC PA 01 DCC PA 02 DCC PA 03 Dhalpur, Golapbagh; West Dhulaipar, Jatrabari; Jele para, South Jatrabari; Muradpur; Gandaria, Natun Jorain; Sutrapur (Loharpole) Aga Sadek Road; Becharam Dhewri; Imamganj, Armanitola; Majed Sardar Road; Haji Mainuddin Road; Tantibazar, Nabab Bari, Islampur; Farashganj. Hazaribagh park; Hazaribagh near Bara Masjid; Azimpur; Nowabganj; Shahid nagar Community Center; Shahidnagar beside Beribandh; Bakshi Bazar; Islambagh; Sultanganj, Kamrangirchar. DCC PA 04-A Sheddeshwari Circular Road; Uttar Mugda, Jheelpar; Ahmadbagh; Dakkhin Kamalapur; Arambagh; AGB Colony, Motijheel; Uttar Shahjahanpur 5. Shimantik DCC PA 04-B Dakkhin Goran; Tilpapara, Khilgaon; Maradia Main Road; Gulbagh, Malibagh. 6. Nari-Maitre DCC PA 05 Bara Maghbazar; Madhubagh, West Dhanmondi; Elephant Road; Topkhana Road; 7. Marie Stopes Clinic Society (MSCS) 8. Unity Through Population Services (UTPS) 9. Progoti Samaj Kalyan Protisthan (PSKP) 10. Unity Through Population Services (UTPS) DCC PA 06 DCC PA 07 Lalmatia Housing Estate; Busbari, Mohammadpur; Humayun Road, Mohammadpur; Noorjahan Road, Mohammadpur; Salimullah Road, Mohammadpur; Sher-e-bangla Road, Royer Bazar; Sultanganj, Royer Bazar. Harirampur Road, Mirpur; Chaitali Sarak, Mirpur; Kallyanpur, Maiddha Paikpara, Mirpur; West Agargaon; Uttar Ibrahimpur; Uttar Kafrul. DCC PA 08 Pallabi, Mirpur; Arambagh Residential Area, Mirpur, Block F, Sector-2; Mirpur; Block F, Sector-1, Mirpur. DCC PA 09 B. Chittagong City Corporation (CCC) 11. Chittagong City Corporation (CCC) CCC PA 01 Road-11, Uttara; Road-34; Sector 7, Uttara Model Town, Sector- 4, Uttara Model Town; Faidabad, Uttara; Ashkona, Uttara; Amtali, Mohakhali; Maddhaya Badda. South Pahartali; Jalalabad; Chandgaon; Mohora; East Sholoshahar, West Sholoshahar; North Pahartali; West Bakalia; Jamalkhan; Rampur; North Halishahar; East Madarbari; Patharghata; Boxirhat; Goshaildanga; Middle Halishahar; South Middle Halishahar, North Patenga, South Patenga. 12. Mamata CCC PA 02 Panchlaish; Lalkhan Bazar; Enayet Bazar; Agrabad; West Madar Bari; Feringhee Bazar. 13. Chittagong City Corporation (CCC) CCC PA 03 South Kattali; Chawkbazar; East Bakalia; Anderkilla; Dewan Bazar.
27 Appendix 1 15 Partner Agency Partnership Catchments Areas C. Khulna City Corporation (KCC) 14. Progoti Samaj Kalyan Protisthan (PSKP) 15. Population Crisis Control & Mass Education Committee (PCC-MEC) KCC PA 01 KCC PA 02 Mujgunni Bastuhara Colony; Wondarland Shishu park; New Market Road; Rayer Mohal Main Road, Boyra; North Khalishpur; Khalishpur Charahat; Khalishpur Housing Colony. Azizmore, Boyra; Nurnagar, Boyra; Sanadanga, Dighirpar; Khalashi, Sanadanga; Golokmoni Shishupark; Siddika Mohalla; West Baniakhamar, Barabari. D. Rajshahi City Corporation (RCC) 16. Annanya Samaj Kallyan RCC PA 01 Protisthan (ASKS) Source: Executing Agency project completion report, Ward-1, Kashiadangarmore; Ward-2, Purbahargram; Ward-12, Fodkipara Padmarpar; Ward-13, Kadirganj; Ward-15, Sapura Gurasthan; Ward-18, Chotabanagram. Table A1.2: Overall Performance of the Partner Organizations Partnership Points Scored by Partner Agencies through Monitoring of Partner NGOs Midterm M&E Baseline- PIU Total Ranking Midterm 1. BWHC DCC PA st 2. MSCS DCC PA nd 3. Mamata CCC PA rd 4. PSKP DCC PA th 5. PSTC DCC PA-4a th 6. BAPSA DCC PA th 7. SHIMANTIC DCC PA-4b th 8. BWHC DCC PA th 9. PSKP KCC PA th 10. Nari Maitree DCC PA th 11. ASKS RCC PA th 12. UTPS DCC PA th 13. UTPS DCC PA th 14. CCC CCC PA th 15. PCC&MEC KCC PA th 16. CCC CCC PA th ASKS = Annanya Samaj Kallyan Sangostha; BAPSA = Bangladesh Association for Prevention of Septic Abortion; BWHC = Bangladesh Women s Health Coalition; CCC = Chittagong City Corporation; MSCS = Marie Stopes Clinic Society; PCC&MEC = Population Crisis Control & Mass Education Committee; PSKP = Progoti Samaj Kallyan Protisthan; PSTC = Population Services and Training Center; and UTPS = Unity Through Population Services. Ranking given by the external monitoring and evaluation consultants are: maximum increase between baseline and midterm is 50 score, midterm score is 100 and project monitoring score is 100, project monitoring score is 100, and PIU monitoring score is 210. Source: Executing agency project completion report 2006.
28 16 Appendix 2 Partner(s) PATIENTS ATTENDED AND SERVED BY THE PARTNER AGENCIES Partner Total Clients Normal Delivery Caesarian Delivery Total Delivery Total Total BCC Performance Services 1. BWHC PA-1 497,323 3,067 1,701 4,768 1,466,038 1,021, BWHC PA-2 312, ,975 3,091, BAPSA PA-3 418, ,095 1,078,835 1,440, PSTC DCC PA-4a 476,535 1, ,728 1,587,497 3,657, Shimantik DCC PA-4b 360, ,369 1,095,508 1,710, Nari-Maitre DCC PA-5 179, ,285 1,991, MSCS DCC PA-6 494,345 3,944 1,696 5,640 1,965,295 1,927, UTPS DCC PA-7 341, , , , PSKP DCC PA-8 455,228 1, ,568 1,107, , UTPS DCC PA-9 141, , ,286 2,195, CCC CCC PA-1 586, ,395,351 1,954, Mamata CCC PA-2 632,877 1,930 2,802 4, ,748 2,231, CCC CCC PA-3 129, , , PSKP KCC, PA-1 462, ,241,338 1,504, PCC & MEC KCC, PA-2 192, ,127 3,676, ASKS RCC, PA-1 479,550 1, ,032 1,180, ,910 Total 6,159,723 19,483 10,432 29,915 16,353,687 28,586,471 ASKS = Annanya Samaj Kallyan Sangostha; BAPSA = Bangladesh Association for Prevention of Septic Abortion; BCC = behavioral change communication; BWHC = Bangladesh Women s Health Coalition; CCC = Chittagong City Corporation; MSCS = Marie Stopes Clinic Society; PSTC = Population Services and Training Center; PSKP = Progoti Samaj Kallyan Protisthan; PCC-MEC = Population Crisis Control & Mass Education Committee; and UTPS = Unity Through Population Services. Source: Executing agency project completion report 2006.
29 Appendix 3 17 SERVICE CHARGES AND COST RECOVERY Table A3.1: Approved Subsidized Service Charges (in taka) Service(s) Charge(s) Service(s) Charge(s) Antenatal Care Registration Fee 5 Adolescent Health Care RT/ STI Asthma Nebulization 60 Sputum for AFB Free ASO Titre 150 Serum Billirubin 80 Blood Sugar Test 60 SGOT 100 Blood Grouping Test 30 SGPT 100 Blood Urea 100 Serum Creatine 100 Child Health Care Serum Cholesterol 100 Child Immunization & Hep-B Vaccination Free Serum Calcium 150 Counseling Free Serum Alkaline Phosphate 100 Caesarian Delivery 3,000 5,000 Stool R/M/E 30 D&C 1,000-2,000 TTC, DC, Hb%, ESR 70 Gynecological Problem TT Service (15-49) Women Free Family Planning Services Condom Free TPHA 100 HbsAg Test 100 Urine R/M/E 30 Limited Curative Care Ultra-sonogram Neonatal Care Urine Sugar Test 15 Normal Delivery Urine Albumin Test 15 M.R Service 350 VDRL 60 Obstetric Care Widal Test 100 Primary & Emergency Services (cut, burn, fracture, minor aliments etc.) RT/STI Post Natal Care Sputum for AFB Free Pregnancy Test D&C = dilution and cleaning, EPI = expanded program of immunization, RT = routine test, MR = menstruation regularization, NVD = normal vaginal delivery, and TB = tuberculosis basillus. Notes: Service Charges: Service charges (medical consultation fees) are substantially below local market rates. EPI services, including TT and family planning services (except condoms, which cost Tk0.10) are free. Tuberculosis diagnosis and treatment is free. Pathological Service: All pathological services are provided at 50% 60% below the local market price. Delivery Service: Normal vaginal delivery charge is only Tk300 Tk500, or 20% 25% of the local market rate. Caesarian Delivery: The caesarian section delivery charge is Tk3,000 Tk5,000, which is less than half the local market rate. Medicines: Medicines are distributed to patients at 75% of market prices. Ambulatory Services: Ambulatory service is provided free of charge, 24 hours per day. Free Service: The absolutely poor ( red cardholders ) can access all services at no cost. Patients who do not hold red cards but cannot pay fees also get services at no or reduced cost. Source: Executing agency project completion report 2006
30 18 Appendix 3 Partner NGOs Table A3.2: Patients Served Free, Partially Free, and Without any Subsidy Partner Free Patients Served Partial Payment Full Payment Total % Patients Served Full Partial Full Payment Payment 1. BWHC DCC PA01 92,193 21, , , BWHC DCC PA02 26,587 18, , , BAPSA DCC PA03 9, , , , PSTC DCC PA4a 133, , , , SHIMANTIK DCC PA4b 75, , , , NARI-MAITRE DCC PAO5 12,514 53, , , MSCS DCC PAO6 122,903 43, , , UTPS DCC PA07 44, , , , PSKP DCC PA08 16,225 89, , , UTPS DCC PA09 17,965 49,450 73, , CCC CCC PA-1 586, , MAMATA CCC PA02 125, , , , CCC CCC PA-3 129, , PSKP KCC PA01 32, , , , PCC&MEC KCC PA02 1,212 35, , , ASKS RCC PA01 32,749 79, , , Total 1,458,642 1,563,204 3,137,877 6,159, ASKS = Annanya Samaj Kallyan Sangostha; BAPSA = Bangladesh Association for Prevention of Septic Abortion; BWHC = Bangladesh Women s Health Coalition; CCC = Chittagong City Corporation; MSCS = Marie Stopes Clinic Society; PSTC = Population Services and Training Center; PSKP = Progoti Samaj Kallyan Protisthan; PCC & MEC = Population Crisis Control & Mass Education Committee; and UTPS = Unity through Population Services. Source: Executing agency project completion report 2006
31 Appendix 3 19 Partner NGOs Table A3.3: Cost-Recovery Achieved by the Partner Organizations Partner s Total Patients Money from UPHCP Income from Fees Total Income (Taka) Cost Recovery (%) a Cost per Patient (Taka) b 1. BWHC DCC PA01 497,323 53,501,923 13,053,501 66,585, BWHC DCC PA02 312,466 32,991,414 6,189,084 37,337, BAPSA DCC PA03 418,517 31,386,008 9,408,318 42,025, PSTC DCC PA4a 476,535 50,415,302 5,718,402 55,232, Shimantik DCC PA4b 360,793 27,990,739 5,744,916 33,735, Nari-Maitre DCC PAO5 179,040 33,195,576 4,885,163 37,915, MSCS DCC PAO6 494,345 52,333,879 22,853,676 73,229, UTPS DCC PA07 341,625 30,753,270 5,073,525 35,765, PSKP DCC PA08 455,228 27,169,534 6,526,025 34,397, UTPS DCC PA09 141,142 31,866,451 5,434,805 37,334, CCC CCC PA-1 586,520 78,830,264 4,770,180 78,116, Mamata CCC PA02 632,877 42,753,957 12,558,688 49,076, CCC PA-3 CCC PA-3 129,032 16,427, ,206 16,691, PSKP KCC PA01 462,675 38,412,419 5,942,740 44,654, PCC & MEC KCC PA02 192,055 34,633,757 3,557,628 38,154, ASKS RCC PA01 479,550 51,318,176 4,074,728 55,260, Total 6,159, ,980, ,357, ,513, ASKS = Annanya Samaj Kallyan Sangostha; BAPSA = Bangladesh Association for Prevention of Septic Abortion; BWHC = Bangladesh Women s Health Coalition; CCC = Chittagong City Corporation; MSCS = Marie Stopes Clinic Society; PSTC = Population Services and Training Center; PSKP = Progoti Samaj Kallyan Protisthan; PCC & MEC = Population Crisis Control & Mass Education Committee; and UTPS = Unity Through Population Services. a Cost Recovery (%) = Total income /Total expenditure x 100. b Cost per client = Total operational cost/ clients served (excluding BCC services). Source: Executing Agency project completion report 2006
32 20 Appendix 4 STATUS OF ESTABLISHMENT OF PRIMARY HEALTH CARE INFRASTRUCTURE Table A4.1: Primary Health Care Centers and Comprehensive Reproductive Health Care Centers Established City Corporation Centers Established in Constructed Infrastructure Centers Established in Rented Infrastructure Total Centers Established PHCCs CRHCCs Total PHCCs CRHCCs Total PHCCs CRHCCs Total 1. Dhaka City Corporation Chittagong City Corporation Khulna City Corporation Rajshahi City Corporation Total CRHCC = comprehensive reproductive health care center, and PHCC = primary health care center. Source: Executing Agency. City Corporation Table A4.2: Construction of Infrastructure for the Centers PHCCs CRHCCs Total Original Revised Actual Original Revised Actual Original Revised Actual 1 Dhaka City Corporation Chittagong City Corporation Khulna City Corporation Rajshahi City Corporation Total CRHCC = comprehensive reproductive health care center, and PHCC = primary health care center. Source: Executing Agency. Table A4.3: Status of the Utilization of the PHCCs and CRHCCs (June 2005) City Corporation PHCCs CRHCCs Total Used Yet to be Used Total Used Yet to be Used Total Used Yet to be Used Total 1 Dhaka City Corporation Chittagong City Corporation Khulna City Corporation Rajshahi City Corporation Total CRHCC = comprehensive reproductive health care center, and PHCC = primary health care center. Source: Executing Agency. Table A4.4: Establishment of Satellite Clinics and Public Toilets (June 2005) City Corporation Satellite Clinics Public Toilets 1. Dhaka City Corporation Chittagong City Corporation Khulna City Corporation Rajshahi City Corporation 36 0 Total Source: Executing Agency.
33 Appendix 5 21 LIST OF TRAINING AND WORKSHOPS 1. Training needs assessment workshop arranged by the project implementation unit (PIU) on 19 September 2001, attended by all partners, health departments and PIU staff. 2. Initial quality circle network workshop was held in Chittagong on 16 January 2002 with the objective of introducing an approach that could be used by partners and health departments to continuously improve quality in a participatory way that would meet their own needs. Administrators, doctors, and paramedics from Mamata clinic attended the workshop. 3. Initial quality circle network was held in Rajshahi on 7 February 2002, attended by about 45 participants including managers, doctors, paramedics, and nurses from the city corporation and partners. 4. Seminar was arranged with the objective of (i) sharing the preliminary findings of the study for domestic violence against women, (ii) sharing different dimensions of violence against women and relevant interventions among the service providers, and (iii) to formulate further activities to address violence against women under the Urban Primary Health Care Project (UPHCP). 5. The PIU and Mitra and Associates arranged a workshop on the Integrated Supervisory Instrument (ISI) on 11 March 2002, in two sessions lasting two days each. Participants included partner agency project managers and management information system (MIS) officers, and deputy project directors, MIS officers and relevant project implementation office (PIO) staff of the four city corporations health departments. 6. In order to initiate an urban tuberculosis (TB) control program in Dhaka city, different courses on TB were held at the TB Control and Training Institute during 9 25 March 2002, including a management course on TB control for medical doctors; a mid-level course on TB control for paramedics (50 participants in 2 batches); an orientation on TB control program for counselors (101 participants in four batches); and one training course for laboratory technicians. 7. A feasibility study regarding ultra sonograms was conducted for the Nordic Development Fund by 15 March A national workshop on health education message development was arranged by the Voluntary Health Service Society (VHSS) on 30 April Prior to that, initial workshops were arranged in Dhaka, Chittagong, Khulna and Rajshahi. The VHSS arranged the national workshop on Health Education Message Development on 30 April 2002 in Dhaka. A national workshop on Improvement of Service Delivery was held on 16 April in Khulna at Progoti Samaj Kalyan Protisthan, and on 17 April 2002 in Khulna, organized by the Population Crisis Control & Mass Education Committee. 9. The first general management training course was arranged by The Bangladesh Institute of Management (BIM) at their premises from 27 April to 2 May 2002; participants included project managers, financial managers, clinic managers, and health officers.
34 22 Appendix A workshop on the development of a communication strategy and message concepts for improved complementary feeding (weaning) practices in urban areas was arranged by the Institute of Child and Mother Health (ICHM) in April A Financial Management Course-1 for the UPHCP was held in Dhaka during May 2002; participants included project managers, and financial managers in charge of partners and PIOs. 12. With the help of the National Tuberculosis Program in Bangladesh, the UPHCP, through its partners, initiated an Urban TB Control Program in Dhaka from 20 April to 9 May with courses that included a management course on TB control for medical officers, a mid-level course on TB control for paramedics, an orientation on the TB control program for counselors, and a laboratory course TB control for laboratory technicians. A TB training for doctors was held in MSCS. 13. Management training with special attention to health care management was organized by the BIM in all cities (Dhaka, Chittagong, Khulna, and Rajshahi). 14. The International Center for Diarrheal Disease Research, Bangladesh and Naripokkho conducted a dissemination seminar of the study on women s health and domestic violence on 9 May 2002 at the Center on Integrated Rural Development for Asia and Pacific (CIRDAP) Auditorium. 15. Extended program of immunization (EPI) training was undertaken for partners and staff. 16. Management training with special attention to health care, third module, was held during 5 6 July 2002 for Dhaka Health Department and partner agencies. 17. Management training with special attention to health care, third module, was held during July 2002 for Chittagong Health Department and partner agencies. 18. A second general management training course was arranged by BIM at their premises during August 2002, with participants such as project managers, financial managers of outside Dhaka, clinic managers, and health officers. 19. Nagorik Uddyog organized training on women s human rights and violence against women for the staff of Bangladesh Association for Prevention of Septic Abortion, Progoti Samaj Kalyan Protisthan, and SHIMANTIK during August Management training with special attention to health care, third module, for Khulna Health Department and partner agencies, was held during 4 5 September Management training with special attention to health care, third module, for Rajshahi Health Department and partner agencies, was held during September Pathological training for five laboratory technicians in tuberculosis was arranged during 2 19 September 2002 by the TB control program in the Tuberculosis Control Campus at Mohakhali.
35 Appendix A financial management course-2 for UPHCP was held in Dhaka during September 2002 with participants that included project managers, financial managers in charge of Phase II partners, and PIOs. 24. Management training with special attention to health care management, in modules of 2 days per month, was held on a regular basis in each one of the four city corporation areas. 25. A service delivery guidebook was finalized through the VHSS in cooperation with partners and PIU. 26. To expand the urban TB control at the Dhaka City National Tuberculosis Control Program of the Directorate General of Health Services (DGHS), the Ministry of Health and Family Welfare (MOHFW) arranged training for five partners in second phase partnership areas. The training for the medical officers cum clinic managers was held during November 2002; training for the paramedics (a mid-level course on TB control) was held in December 2002 in several batches; training for the counselors (a field-level course on TB control) was held also in December 2002 in three batches. 27. The diarrheal diseases control program of the DGHS arranged training in diarrheal diseases for one paramedic from each partnership area in Dhaka Shishu Hospital during December Management training with special attention to health care management (fourth module) for respective health departments and partner agencies was held during 5 6 October 2002 for Dhaka; October 2002 for Chittagong; October 2002 for Khulna; and January 2003 for Rajshahi. 29. Management training with special attention to health care management (fifth module) for respective health departments and partner agencies was held during December 2002 for Chittagong; December 2002 for Khulna; December 2002 for Dhaka; and February 2003 for Rajshahi. 30. An overseas fellowship program was undertaken from 20 October to 30 December 2002; participants were Project deputy secretaries and deputy project directors. 31. Mitra and Associates held an ISI-revision workshop with all partners on 30 January A first annual strategic planning cycle training course for health care management was arranged by the BIM it its premises during February 2003 with participants such as project managers. 33. Management training with special attention to health care, sixth module, for the health department and partner agencies was held during March 2003, April 2003, May 2003, and 8 10 April 2003 respectively for the city corporations of Khulna, Chittagong, Rajshahi, and Dhaka. 34. The National Institute of Preventive and Social Medicine arranged a workshop on the dissemination of improved hygiene education on 19 March A central advocacy and planning meeting in order to enhance the eleventh National Immunization Day 2003 was organized on 24 February for project and partner staff.
36 24 Appendix World TB days were supported by all partners on 24 March 2003, 2004, and The DGHS national tuberculosis control program arranged training in TB control for the medical officers and laboratory technicians respectively during 5 7 April 2003 and 8 10 April The second training session for medical officers of the annual strategic planning cycle for health care management was arranged in Dhaka during May 2003 at the BIM. 39. An orientation session was held in 2 July 2003 at the auditorium of Nagar Bhaban, of the Dhaka City Corporation, which was attended by 10 medical officers from each partner agency. 40. A workshop on improved weaning practices in urban areas through behavioral change communication was conducted by the ICMH during September 2003 for five medical officers, and during September 2003 for six paramedics and three counselors from each partner agency. 41. Training on menstrual regulation was held from 1 to15 July 2003 with one medical officer from each partner agency. 42. A training of trainers course for management of TB was conducted by the National TB and Leprosy Control Office from 30 August to 4 September 2003; one medical officer from each partner agency attended. 43. Training on clinical management was conducted during 3 30 October 2003; and one paramedic from each partner agency participated. 44. Clinical counseling training was held at MFSTC, in which three counselors from each partner agency participated. The training took place in three sessions: during 1 5 November 2003, 8 12 November 2003, and November A basic course on clinic contraception and HIV/AIDS 7 and reproductive tract infection/sexually transmitted infections (RTI/STI) case management and male involvement was held during December 2003 at Marie Stopes Clinic Society attended by one medical officer from each partner agency. 46. Need-based advanced skill trainings in child development, childhood interventions and integrated case management were conducted during 2004 and 2005 in nine sessions. Eleven medical officers and six paramedics from each partner agencies participated in the training. 47. Training on project financial administration was conducted by the Population Services and Training Center (PSTC) during October 2004; project managers, and finance and administrative staff from each partner agency participated. 48. An orientation program on RTI was held on 21 October 2004 at Nagar Bhaban Conference room with project managers, clinic managers, and medical officers from the partner agencies. 7 Human immunodeficiency virus/acquired immunodeficiency syndrome.
37 Appendix Stakeholder workshop was held on 8 November 2004 at the auditorium of the Bangladesh Institute of Administration and Management (BIAM) with the project manager, quality assurance officer, MIS officer, paramedics and other clients. 50. The Bangladesh Institute of Management (BIM) conducted a training course in four batches on general management for five medical officers and one clinical manager from each partner agency during 2004 and The Bangladesh Institute of Management (BIM) conducted training of the trainers of urban primary health care project (UPHCP) during 15 January to 1 May 2005 and one medical officer from each partner agency attended. 52. Training on obstetrics-gynecology and anesthesia was held during 1 30 February 2005 with two medical officers from each partner agency (one for obstetrics-gynecology and one for anesthesia). 53. Training on computer applications using MS-Word, Excel, Access and the Internet was conducted by Bangladesh Institute of Management (BIM) from 8 January to 8 February The 48-hour course was held in three sessions; all UPHCP PIU staff participated in the training. 54. Training on the urban reproductive health MIS was conduced on 21 March All senior monitoring officers, one administrative officer, one counselor, and one accountant participated in the training. 55. Training on clinical contraception for one medical officer from each partner agency (one month held from 9 April to 9 May 2005) and one nurse from each partner agency (15 days held during 9 26 April 2005) was organized by the Project. 56. Training on TB management (modular course) for two medical officers from each partner agency was held on 28 April 2005 at the TB Leprosy Institute. 57. Training on Norplant was held at MFSTC from 29 May to 2 June 2005 for one medical officer and two paramedics from each partner agency. 58. Training on behavioral change communication (BCC) was conducted by National Institute of Population Research and Training, Dhaka. A total of 180 participants (counselors, community mobilizers, and BCC workers) from 16 partner agencies participated in 6 groups during A follow-up workshop on the research project phase III regarding the development of an urban TB control program was held on 23 September 2004 at PSTC; project managers from all project agencies attended. 60. A workshop on vitamin A capsules was held on 10 July 2004 at Nagar Bhaban; one medical officer from each partner agency participated. 61. A general management course with emphasis on problem solving and management style for middle level managers and clinic managers was conducted by BIM at the Chittagong campus from 29 January to 10 February 2005, attended by five medical officers, one councilor and one accountant from three partner agencies of Chittagong City Corporation.
38 26 Appendix A workshop on the Skilled Birth Attendants (SBA) Program in Bangladesh and its linkages was held on April 2005 with one medical officer from each partner agency. 63. Training on clinical contraception, HIV/AIDS and RTI/STI was conducted by MFSTC, Dhaka, attended by one medical officer (9 April to 9 May 2005) and one paramedic (11 April to 26 April 2005) from each partner agency. 64. An orientation workshop was held on TB control program on 8 June 2005 with one medical officer and project manger from each partner agency. 65. Refresher training on Norplant was held during 3 7 July 2005 for two medical officers and one paramedic from each partner agency. Source: Executing agency project completion report 2006
39 Appendix 6 27 STATUS OF PROJECT SUPPORT STAFF, CONSULTANTS, AND LOGISTICS A. Project Support Staff Table A6.1: Incremental Project Implementation Staff Provision per Actual Position Project Proforma Total PIU/DCC RCC CCC KCC 1. Project Director Deputy Project Director Senior Accounts Officer Executive Engineer Senior Monitoring and Evaluation Officer 6. Program Officer Research Officer Logistic and Store Management Officer 9. Accounts Officer Assistant Engineer Sub-Assistant Engineer Personal Assistant to the Project Director 13. Accountant Office Assistant Computer Operator Driver Messenger MLSS Total CCC = Chittagong City Corporation; DCC = Dhaka City Corporation; KCC = Khulna City Corporation; MLSS = Member of Lower Subordinate Service; PIU = project implementation unit; and RCC = Rajshahi City Corporation. Source: Executing agency project completion report B. Summary of Consulting Services Table A6.2: Consultant Inputs Position Consultant Input Person months Appraisal Actual A. International Consultant 1. Partnership Specialist Management Development and Training Specialist Total (A) B. Domestic Consultants 1. Project Implementation Specialist Health Finance Specialist Total (B) Source: Executing agency project completion report 2006.
40 28 Appendix 6 Table A6.3: Major Reports Produced and Activities Undertaken by the Consultants Report(s)/Activitie(s) Time 1. Household Survey Baseline household survey March 2000 Midterm household survey October 2003 Endline household survey December 2004 Final household survey June Health Facility Survey Baseline health facility survey (phase I) May 2002 Baseline health facility survey (phase II) September 2002 Midterm health facility survey November 2002 Final health facility survey August Integrated Supervisory Instrument Integrated Supervisory Instrument - First Round (phase I) February 2002 Integrated Supervisory Instrument - First Round (phase II) November 2002 Integrated Supervisory Instrument - Second Round (phase I) July 2002 Integrated Supervisory Instrument - Second Round (phase II) and Third August 2003 Round (phase I) Integrated Supervisory Instrument - Fourth Round (phase I) and Third Round October 2004 (phase II) Integrated Supervisory Instrument - Fifth Round (phase I) and Fourth Round June 2005 (phase II) 4. Participatory Rapid Appraisal July 2000 Source: Executing agency project completion report C. Logistics Support Item Table A6.4: Vehicles Allocation per Actual Project Proforma Total PMU DCC CCC RCC KCC 1. Jeep Sedan Microbus Motorcycle Pickup Van CCC = Chittagong City Corporation; DCC = Dhaka City Corporation; KCC = Khulna City Corporation; PP=project proforma; PMU = project management unit; and RCC = Rajshahi City Corporation. Source: Executing agency project completion report 2006.
41 Appendix 6 29 Table A6.5: Office Equipment Item Provision per Actual Project Proforma Total PMU DCC CCC RCC KCC PA 1. Multimedia projector Note book Document camera Flatbed scanner Projection screen Mobile phone with SIM Telephone set Photocopier Accounting software Desktop computers, Printers and UPS 7. Laptop computers Overhead projector Screen Slide projector Still camera Meeting Microphones Generator Air conditioner Audio visual Color TV TV trolley DVD player Refrigerator Volt stabilizer for refrigerator Volt stabilizer for TV Facsimile machines Furniture (sets) Carpet (square feet) 5,000 4,000 2, , PHC medical equipment 135 sets Maternity center equipment 16 sets CCC = Chittagong City Corporation; DCC = Dhaka City Corporation; KCC = Khulna City Corporation; PA = partner agency; PMU = project management unit; RCC = Rajshahi City Corporation; and UPS = uninterrupted power supply. Source: Executing agency project completion report 2006.
42 30 Appendix 6 Table A6.6: Furniture Item Allocation per Actual Project Proforma Total PMU DCC CCC RCC KCC 1. Tables 2. Chairs 3. Cabinets Full table Secretariat table Executive table Conference table Tea making table Table side rack Drawer unit Computer table Revolving foam arm Simple foam cushion arm Simple foam cushion armless Simple wooden armless Sofa Swivel chair File cabinet Book/file shelves Book/file shelves (glass door) Almirah Photocopier table Easel board White board Table top glass VIPP board Iron safe CCC = Chittagong City Corporation; DCC = Dhaka City Corporation; KCC = Khulna City Corporation; PMU = project management unit; and RCC = Rajshahi City Corporation. Source: Executing agency project completion report 2006.
43 Appendix 7 31 Category or Subloan(s) DISBURSEMENTS OF LOAN PROCEEDS Table A7.1: Allocation and Actual Disbursement of Proceeds ($'000) Original Allocation Last Amount Revised Added/ Allocation Cancelled Net Amount Amount Available Disbursed Undisbursed Balance Civil works $ 5,346 9,344 3,998 9,344 6,237 3,107 SDR 3,941 6,822 2,881 6,822 4,672 2,150 Drugs and medical supplies $ 9,100 2,808 (6,292) 2,808 2, SDR 6,708 2,032 (4,676) 2,032 1, Office equipment, furniture, $ and vehicle SDR Partnership agreement $ 15,591 12,546 (3,045) 12,546 11,102 1,444 SDR 11,493 8,981 (2,512) 8,981 8, Health education $ SDR Research and BME $ 3,032 3, ,056 2, SDR 2,235 2, ,249 1, Training and development $ SDR Consulting services $ (93) SDR (74) Administrative, operation & $ maintenance SDR Service charge $ SDR Unallocated $ 3,965 - (3,908) SDR 2,923 - (2,923) Total $ 40,000 31,024 (8,921) 31,024 24,139 6,885 SDR 29,487 22,429 (7,058) 22,429 17,697 4,732 BME = benefit monitoring evaluation; SDR = special drawing rights; and $ = United States dollars Source = Executing agency and Bangladesh Resident Mission.
44 32 Appendix 7 Table A7.2: Annual Actual Disbursement of Proceeds Year Annual Disbursement Cumulative Disbursement $ SDR $ SDR , , , , , , , , ,136, ,638, ,639, ,999, ,874, ,826, ,514, ,825, ,510, ,485, ,024, ,311, ,939, ,832, ,964, ,144, ,107, ,120, ,071, ,264, ,530, ,360, ,601, ,625, ,536, ,072, ,138, ,697, Total 24,138, ,697, SDR = special drawing rights; and $ = United States dollars. Source = Executing agency and Bangladesh Resident Mission. Figure A7.1: Annual Actual Disbursement of Proceeds 30,000, ,000, Disbursement 20,000, ,000, ,000, ,000, Year Annual Disbursement $ Cumulative Disbursement $

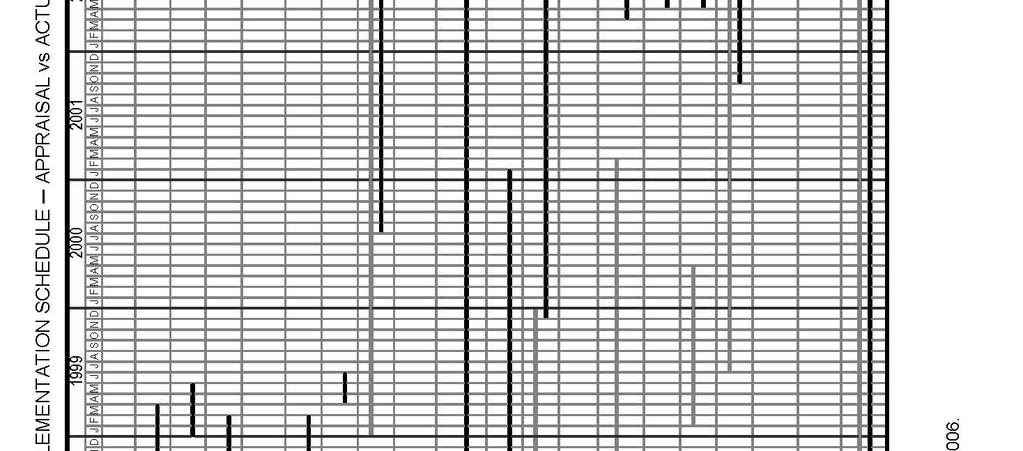
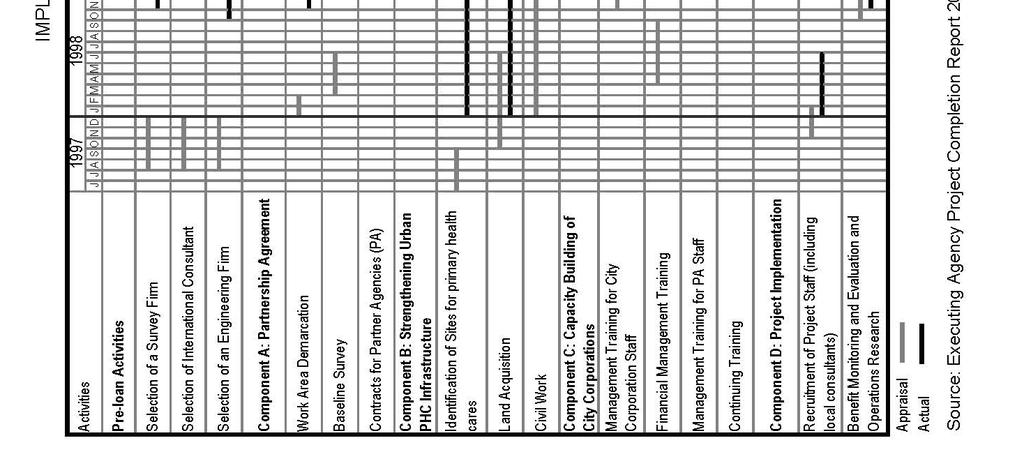
45 Appendix 8 33
Uzbekistan: Woman and Child Health Development Project
 Validation Report Reference Number: PVR-331 Project Number: 36509 Loan Number: 2090 September 2014 Uzbekistan: Woman and Child Health Development Project Independent Evaluation Department ABBREVIATIONS
Validation Report Reference Number: PVR-331 Project Number: 36509 Loan Number: 2090 September 2014 Uzbekistan: Woman and Child Health Development Project Independent Evaluation Department ABBREVIATIONS
FRAMEWORK FINANCING AGREEMENT. (National Highway Development Sector Investment Program Project 1) between ISLAMIC REPUBLIC OF PAKISTAN.
 between ISLAMIC REPUBLIC OF PAKISTAN.") FRAMEWORK FINANCING AGREEMENT (National Highway Development Sector Investment Program Project 1) between ISLAMIC REPUBLIC OF PAKISTAN and ASIAN DEVELOPMENT BANK DATED 29 October 2005 FRAMEWORK FINANCING
FRAMEWORK FINANCING AGREEMENT (National Highway Development Sector Investment Program Project 1) between ISLAMIC REPUBLIC OF PAKISTAN and ASIAN DEVELOPMENT BANK DATED 29 October 2005 FRAMEWORK FINANCING
Health and Nutrition Public Investment Programme
 Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
ASIAN DEVELOPMENT BANK PCR:BAN 18036
 ASIAN DEVELOPMENT BANK PCR:BAN 18036 PROJECT COMPLETION REPORT ON THE SECOND HEALTH AND FAMILY PLANNING SERVICES PROJECT (Loan No. 1074-BAN[SF]) IN BANGLADESH July 2001 CURRENCY EQUIVALENTS Currency Unit
ASIAN DEVELOPMENT BANK PCR:BAN 18036 PROJECT COMPLETION REPORT ON THE SECOND HEALTH AND FAMILY PLANNING SERVICES PROJECT (Loan No. 1074-BAN[SF]) IN BANGLADESH July 2001 CURRENCY EQUIVALENTS Currency Unit
Nepal: Small Towns Water Supply and Sanitation Sector Project
 Validation Report Reference Number: PVR 193 Project Number: 31402 Loan Number: 1755(SF) November 2012 Nepal: Small Towns Water Supply and Sanitation Sector Project Independent Evaluation Department ABBREVIATIONS
Validation Report Reference Number: PVR 193 Project Number: 31402 Loan Number: 1755(SF) November 2012 Nepal: Small Towns Water Supply and Sanitation Sector Project Independent Evaluation Department ABBREVIATIONS
Public Disclosure Copy. Implementation Status & Results Report Global Partnership for Education Grant for Basic Education Project (P117662)
") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized AFRICA Liberia Education Global Practice Recipient Executed Activities Specific Investment
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized AFRICA Liberia Education Global Practice Recipient Executed Activities Specific Investment
ASIAN DEVELOPMENT BANK
 ASIAN DEVELOPMENT BANK PPA: PAK 26373 PROJECT PERFORMANCE AUDIT REPORT ON THE POPULATION PROJECT (Loan 1277-PAK[SF]) IN PAKISTAN December 2003 CURRENCY EQUIVALENTS Currency Unit Pakistan rupee/s (PRe/PRs)
ASIAN DEVELOPMENT BANK PPA: PAK 26373 PROJECT PERFORMANCE AUDIT REPORT ON THE POPULATION PROJECT (Loan 1277-PAK[SF]) IN PAKISTAN December 2003 CURRENCY EQUIVALENTS Currency Unit Pakistan rupee/s (PRe/PRs)
Completion Report. Project Number: Loan Number: 2449-INO(SF) October Indonesia: Rural Infrastructure Support to the PNPM Mandiri Project
 October Indonesia: Rural Infrastructure Support to the PNPM Mandiri Project") Completion Report Project Number: 40247 Loan Number: 2449-INO(SF) October 2012 Indonesia: Rural Infrastructure Support to the PNPM Mandiri Project CURRENCY EQUIVALENTS Currency Unit rupiah (Rp) At Appraisal
Completion Report Project Number: 40247 Loan Number: 2449-INO(SF) October 2012 Indonesia: Rural Infrastructure Support to the PNPM Mandiri Project CURRENCY EQUIVALENTS Currency Unit rupiah (Rp) At Appraisal
TA: TRANSIT-ORIENTED DEVELOPMENT AND IMPROVED TRAFFIC MANAGEMENT IN GCC
 Greater Dhaka Sustainable Urban Transport Project (RRP BAN 42169) TA: TRANSIT-ORIENTED DEVELOPMENT AND IMPROVED TRAFFIC MANAGEMENT IN GCC A. TA Description 1. The Government of Bangladesh has requested
Greater Dhaka Sustainable Urban Transport Project (RRP BAN 42169) TA: TRANSIT-ORIENTED DEVELOPMENT AND IMPROVED TRAFFIC MANAGEMENT IN GCC A. TA Description 1. The Government of Bangladesh has requested
Papua New Guinea: Implementation of the Electricity Industry Policy
 Technical Assistance Report Project Number: 46012 December 2012 Papua New Guinea: Implementation of the Electricity Industry Policy The views expressed herein are those of the consultant and do not necessarily
Technical Assistance Report Project Number: 46012 December 2012 Papua New Guinea: Implementation of the Electricity Industry Policy The views expressed herein are those of the consultant and do not necessarily
Global Partnership on Output-based Aid Grant Agreement
 Public Disclosure Authorized GPOBA GRANT NUMBER TF010757 Public Disclosure Authorized Public Disclosure Authorized Global Partnership on Output-based Aid Grant Agreement (Philippines Public Health Project)
Public Disclosure Authorized GPOBA GRANT NUMBER TF010757 Public Disclosure Authorized Public Disclosure Authorized Global Partnership on Output-based Aid Grant Agreement (Philippines Public Health Project)
Completion Report. Project Number: Loan Number: 1762(SF) September Bhutan: Health Care Reform Program
 September Bhutan: Health Care Reform Program") Completion Report Project Number: 33071 Loan Number: 1762(SF) September 2006 Bhutan: Health Care Reform Program CURRENCY EQUIVALENTS Currency Unit Ngultrum (Nu) At Appraisal At Program Completion 25 May
Completion Report Project Number: 33071 Loan Number: 1762(SF) September 2006 Bhutan: Health Care Reform Program CURRENCY EQUIVALENTS Currency Unit Ngultrum (Nu) At Appraisal At Program Completion 25 May
NATIONAL COMMUNITY EMPOWERMENT PROGRAM IN URBAN AREAS FOR APPROVED ON NOVEMBER 20, 2012 REPUBLIC OF INDONESIA
 The World Bank DOCUMENT OF THE WORLD BANK REPORT NO.: RES25530 RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF NATIONAL COMMUNITY EMPOWERMENT PROGRAM IN URBAN AREAS FOR 2012-2015 APPROVED ON
The World Bank DOCUMENT OF THE WORLD BANK REPORT NO.: RES25530 RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF NATIONAL COMMUNITY EMPOWERMENT PROGRAM IN URBAN AREAS FOR 2012-2015 APPROVED ON
Completion Report. Pakistan: Balochistan Devolved Social Services Program
 Completion Report Project Number: 37218 Loan Numbers: 2202, 2203, and 2204 Grant Number: 0028 December 2011 Pakistan: Balochistan Devolved Social Services Program CURRENCY EQUIVALENTS Currency Unit Pakistan
Completion Report Project Number: 37218 Loan Numbers: 2202, 2203, and 2204 Grant Number: 0028 December 2011 Pakistan: Balochistan Devolved Social Services Program CURRENCY EQUIVALENTS Currency Unit Pakistan
PROJECT PREPARATORY TECHNICAL ASSISTANCE
 Appendix 3 11 A. Justification PROJECT PREPARATORY TECHNICAL ASSISTANCE 1. The government has identified the priority areas to be covered under the ensuing project. A PPTA is necessary to provide sound
Appendix 3 11 A. Justification PROJECT PREPARATORY TECHNICAL ASSISTANCE 1. The government has identified the priority areas to be covered under the ensuing project. A PPTA is necessary to provide sound
Completion Report. Project Number: Loan Number: 2230-PAK October Pakistan: Rural Enterprise Modernization Project
 Completion Report Project Number: 38447 Loan Number: 2230-PAK October 2010 Pakistan: Rural Enterprise Modernization Project CURRENCY EQUIVALENTS Currency Unit Pakistan rupee/s (PRe/PRs) At Appraisal At
Completion Report Project Number: 38447 Loan Number: 2230-PAK October 2010 Pakistan: Rural Enterprise Modernization Project CURRENCY EQUIVALENTS Currency Unit Pakistan rupee/s (PRe/PRs) At Appraisal At
TERMS OF REFERENCE: PRIMARY HEALTH CARE
 TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
GRANT AGREEMENT (ADB Strategic Climate Fund) (Greater Mekong Subregion Biodiversity Conservation Corridors Project Additional Financing)
 (Greater Mekong Subregion Biodiversity Conservation Corridors Project Additional Financing)") GRANT NUMBER 0426-CAM (SCF) GRANT AGREEMENT (ADB Strategic Climate Fund) (Greater Mekong Subregion Biodiversity Conservation Corridors Project Additional Financing) (Cambodia Component) between KINGDOM
GRANT NUMBER 0426-CAM (SCF) GRANT AGREEMENT (ADB Strategic Climate Fund) (Greater Mekong Subregion Biodiversity Conservation Corridors Project Additional Financing) (Cambodia Component) between KINGDOM
Public Disclosure Copy
 Public Disclosure Authorized AFRICA Burundi Health, Nutrition & Population Global Practice IBRD/IDA Investment Project Financing FY 2017 Seq No: 2 ARCHIVED on 20-Dec-2017 ISR29199 Implementing Agencies:
Public Disclosure Authorized AFRICA Burundi Health, Nutrition & Population Global Practice IBRD/IDA Investment Project Financing FY 2017 Seq No: 2 ARCHIVED on 20-Dec-2017 ISR29199 Implementing Agencies:
Technical Assistance to the Republic of Philippines for the Support for Health Sector Reform
 Technical Assistance TAR: PHI 39066 Technical Assistance to the Republic of Philippines for the Support for Health Sector Reform September 2005 CURRENCY EQUIVALENTS (as of 5 August 2005) Currency Unit
Technical Assistance TAR: PHI 39066 Technical Assistance to the Republic of Philippines for the Support for Health Sector Reform September 2005 CURRENCY EQUIVALENTS (as of 5 August 2005) Currency Unit
(Financed by the Japan Fund for Poverty Reduction)
") Technical Assistance Report Project Number: 49276-001 Capacity Development Technical Assistance (CDTA) December 2015 India: Supporting Rajasthan s Productive Clusters in the Delhi Mumbai Industrial Corridor
Technical Assistance Report Project Number: 49276-001 Capacity Development Technical Assistance (CDTA) December 2015 India: Supporting Rajasthan s Productive Clusters in the Delhi Mumbai Industrial Corridor
The World Bank Romania Secondary Education Project (P148585)
") Public Disclosure Authorized Public Disclosure Authorized The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF ROMANIA SECONDARY EDUCATION PROJECT APPROVED ON MARCH 16, 2015 TO ROMANIA
Public Disclosure Authorized Public Disclosure Authorized The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF ROMANIA SECONDARY EDUCATION PROJECT APPROVED ON MARCH 16, 2015 TO ROMANIA
UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION
 COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION") UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION UNICEF H&NH Outcome: UNICEF H&N OP #: 3 UNICEF Work Plan Activity: Objective:
UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION UNICEF H&NH Outcome: UNICEF H&N OP #: 3 UNICEF Work Plan Activity: Objective:
Acronyms and Abbreviations
 Redacted Acronyms and Abbreviations CES CIP FP ISDP MCHIP MOH NGO OFDA PHC PHCC PITC PPH USAID WES Central Equatoria State County Implementing Partner Family Planning Integrated Service Delivery Project
Redacted Acronyms and Abbreviations CES CIP FP ISDP MCHIP MOH NGO OFDA PHC PHCC PITC PPH USAID WES Central Equatoria State County Implementing Partner Family Planning Integrated Service Delivery Project
Implementation Status & Results Central African Republic Multisectoral HIV/AIDS Project (P073525)
") losure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results Central African Republic Multisectoral HIV/AIDS Project
losure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results Central African Republic Multisectoral HIV/AIDS Project
ARTICLE I. Grant Regulations; Definitions
 3 ARTICLE I Grant Regulations; Definitions Section 1.01. All provisions of the Special Operations Grant Regulations of ADB, dated 7 February 2005 (the Grant Regulations ), are hereby made applicable to
3 ARTICLE I Grant Regulations; Definitions Section 1.01. All provisions of the Special Operations Grant Regulations of ADB, dated 7 February 2005 (the Grant Regulations ), are hereby made applicable to
Local Government Unit Private Infrastructure Project Development Facility (Loan 1729-PHI) in the Philippines
 in the Philippines") Project Completion Report PCR: PHI 32485 Local Government Unit Private Infrastructure Project Development Facility (Loan 1729-PHI) in the Philippines June 2005 CURRENCY EQUIVALENTS Currency Unit peso/s
Project Completion Report PCR: PHI 32485 Local Government Unit Private Infrastructure Project Development Facility (Loan 1729-PHI) in the Philippines June 2005 CURRENCY EQUIVALENTS Currency Unit peso/s
UHC. Moving toward. Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES. Public Disclosure Authorized
 Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
Republic of Indonesia: Water Supply and Sanitation Sector Development Project
 Technical Assistance Report Project Number: 43304-022 Capacity Development Technical Assistance (CDTA) November 2011 Republic of Indonesia: Water Supply and Sanitation Sector Development Project (Financed
Technical Assistance Report Project Number: 43304-022 Capacity Development Technical Assistance (CDTA) November 2011 Republic of Indonesia: Water Supply and Sanitation Sector Development Project (Financed
Pacific Urban Development Investment Planning and Capacity Development Facility
 Technical Assistance Report Project Number: 51175-001 Transaction Technical Assistance Facility (F-TRTA) July 2017 Pacific Urban Development Investment Planning and Capacity Development Facility This document
Technical Assistance Report Project Number: 51175-001 Transaction Technical Assistance Facility (F-TRTA) July 2017 Pacific Urban Development Investment Planning and Capacity Development Facility This document
Mauritania Red Crescent Programme Support Plan
 Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
Regional: Supporting the Cities Development Initiative for Asia
 Technical Assistance Report Project Number: 47285 Regional Capacity Development Technical Assistance (R-CDTA) November 2013 Regional: Supporting the Cities Development Initiative for Asia (Cofinanced by
Technical Assistance Report Project Number: 47285 Regional Capacity Development Technical Assistance (R-CDTA) November 2013 Regional: Supporting the Cities Development Initiative for Asia (Cofinanced by
Fiduciary Arrangements for Grant Recipients
 Table of Contents 1. Introduction 2. Overview 3. Roles and Responsibilities 4. Selection of Principal Recipients and Minimum Requirements 5. Assessment of Principal Recipients 6. The Grant Agreement: Intended
Table of Contents 1. Introduction 2. Overview 3. Roles and Responsibilities 4. Selection of Principal Recipients and Minimum Requirements 5. Assessment of Principal Recipients 6. The Grant Agreement: Intended
United Nations Peace Building Fund Grant Agreement
 Public Disclosure Authorized OFFICIAL DOCUMENTS Public Disclosure Authorized GRANT NUMBER TF018255 United Nations Peace Building Fund Grant Agreement (Additional Financing for the Productive Social Safety
Public Disclosure Authorized OFFICIAL DOCUMENTS Public Disclosure Authorized GRANT NUMBER TF018255 United Nations Peace Building Fund Grant Agreement (Additional Financing for the Productive Social Safety
People s Republic of China: Strengthening the Role of E-Commerce in Poverty Reduction in Southwestern Mountainous Areas in Chongqing
 Technical Assistance Report Project Number: 51022-001 Knowledge and Support Technical Assistance (KSTA) December 2017 People s Republic of China: Strengthening the Role of E-Commerce in Poverty Reduction
Technical Assistance Report Project Number: 51022-001 Knowledge and Support Technical Assistance (KSTA) December 2017 People s Republic of China: Strengthening the Role of E-Commerce in Poverty Reduction
Contracting Out Health Service Delivery in Afghanistan
 Contracting Out Health Service Delivery in Afghanistan Dr M.Nazir Rasuli General director Care of Afghan Families,CAF. Kathmando Nepal 12 Jun,2012 Outline 1. Background 2. BPHS 3. Contracting with NGOs,
Contracting Out Health Service Delivery in Afghanistan Dr M.Nazir Rasuli General director Care of Afghan Families,CAF. Kathmando Nepal 12 Jun,2012 Outline 1. Background 2. BPHS 3. Contracting with NGOs,
SESSION #6: DESIGNING HEALTH MARKET INTERVENTIONS Part 1
 SESSION #6: DESIGNING HEALTH MARKET INTERVENTIONS Part 1 Stewardship vs. market forces in RMNCAH-N markets Markets organized along continuum of stewardship vs market forces LAPM: Long Acting Permanent
SESSION #6: DESIGNING HEALTH MARKET INTERVENTIONS Part 1 Stewardship vs. market forces in RMNCAH-N markets Markets organized along continuum of stewardship vs market forces LAPM: Long Acting Permanent
(Pyidaungsu Hluttaw Law (2015) No. ) 1376ME The Pyidaunsu Hluttaw (the Union Parliament) now therefore promulgates this law.
 No. ) 1376ME The Pyidaunsu Hluttaw (the Union Parliament) now therefore promulgates this law.") Population Control Healthcare Law (draft) (Pyidaungsu Hluttaw Law (2015) No. ) 1376ME 2015 The Pyidaunsu Hluttaw (the Union Parliament) now therefore promulgates this law. Chapter I Title and Definition
Population Control Healthcare Law (draft) (Pyidaungsu Hluttaw Law (2015) No. ) 1376ME 2015 The Pyidaunsu Hluttaw (the Union Parliament) now therefore promulgates this law. Chapter I Title and Definition
OFFICIAL DOCUMENTS.I
 Public Disclosure Authorized OFFICIAL DOCUMENTS.I Public Disclosure Authorized PPIN MULTI-DONOR TRUST FUND GRANT NUMBER TF018108 Pakistan Partnership for Improved Nutrition Multi-Donor Trust Fund Grant
Public Disclosure Authorized OFFICIAL DOCUMENTS.I Public Disclosure Authorized PPIN MULTI-DONOR TRUST FUND GRANT NUMBER TF018108 Pakistan Partnership for Improved Nutrition Multi-Donor Trust Fund Grant
Rajasthan Urban Sector Development Program
 India: Rajasthan Urban Sector Development Program Project Name Rajasthan Urban Sector Development Program Project Number 42267-026 Country Project Status Project Type / Modality of Assistance Source of
India: Rajasthan Urban Sector Development Program Project Name Rajasthan Urban Sector Development Program Project Number 42267-026 Country Project Status Project Type / Modality of Assistance Source of
Global Environment Facility Trust Fund Grant Agreement
 CONFORMED COPY GEF TRUST FUND GRANT NUMBER TF099857 Global Environment Facility Trust Fund Grant Agreement (Nyika Transfrontier Conservation Area Project) between REPUBLIC OF MALAWI and INTERNATIONAL BANK
CONFORMED COPY GEF TRUST FUND GRANT NUMBER TF099857 Global Environment Facility Trust Fund Grant Agreement (Nyika Transfrontier Conservation Area Project) between REPUBLIC OF MALAWI and INTERNATIONAL BANK
RBF in Zimbabwe Results & Lessons from Mid-term Review. Ronald Mutasa, Task Team Leader, World Bank May 7, 2013
 RBF in Zimbabwe Results & Lessons from Mid-term Review Ronald Mutasa, Task Team Leader, World Bank May 7, 2013 Outline Country Context Technical Design Implementation Timeline Midterm Review Results Evaluation
RBF in Zimbabwe Results & Lessons from Mid-term Review Ronald Mutasa, Task Team Leader, World Bank May 7, 2013 Outline Country Context Technical Design Implementation Timeline Midterm Review Results Evaluation
The World Bank Sustainable Rural Sanitation Services Program for Results (P154112)
") Public Disclosure Authorized MIDDLE EAST AND NORTH AFRICA Egypt, Arab Republic of Water Global Practice IBRD/IDA Program-for-Results FY 2016 Seq No: 1 ARCHIVED on 05-Nov-2015 ISR21200 Implementing Agencies:
Public Disclosure Authorized MIDDLE EAST AND NORTH AFRICA Egypt, Arab Republic of Water Global Practice IBRD/IDA Program-for-Results FY 2016 Seq No: 1 ARCHIVED on 05-Nov-2015 ISR21200 Implementing Agencies:
Selected Strategies to Improve Access to and Quality of Urban Primary Health Care. Abdullah Baqui, DrPH, MPH, MBBS Johns Hopkins University
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
PROJECT PREPARATORY TECHNICAL ASSISTANCE
 A. Justification PROJECT PREPARATORY TECHNICAL ASSISTANCE 1. A project preparatory technical assistance (PPTA) is required to support the Ministry of New and Renewable Energy (MNRE) and Solar Energy Corporation
A. Justification PROJECT PREPARATORY TECHNICAL ASSISTANCE 1. A project preparatory technical assistance (PPTA) is required to support the Ministry of New and Renewable Energy (MNRE) and Solar Energy Corporation
World Bank Iraq Trust Fund Grant Agreement
 Public Disclosure Authorized Conformed Copy GRANT NUMBER TF054052 Public Disclosure Authorized World Bank Iraq Trust Fund Grant Agreement Public Disclosure Authorized (Emergency Disabilities Project) between
Public Disclosure Authorized Conformed Copy GRANT NUMBER TF054052 Public Disclosure Authorized World Bank Iraq Trust Fund Grant Agreement Public Disclosure Authorized (Emergency Disabilities Project) between
CONSOLIDATED RESULTS REPORT. Country: ANGOLA Programme Cycle: 2009 to
 CONSOLIDATED RESULTS REPORT Country: ANGOLA Programme Cycle: 2009 to 2014 1 1. Key Results modified or added 2. Key Progress Indicators 3. Description of Results Achieved PCR 1: Accelerated Child Survival
CONSOLIDATED RESULTS REPORT Country: ANGOLA Programme Cycle: 2009 to 2014 1 1. Key Results modified or added 2. Key Progress Indicators 3. Description of Results Achieved PCR 1: Accelerated Child Survival
Global Partnership on Output-based Aid Grant Agreement
 Public Disclosure Authorized CONFORMED COPY GPOBA GRANT NUMBER TF096551-BD Public Disclosure Authorized Global Partnership on Output-based Aid Grant Agreement (Rural Electrification and Renewable Energy
Public Disclosure Authorized CONFORMED COPY GPOBA GRANT NUMBER TF096551-BD Public Disclosure Authorized Global Partnership on Output-based Aid Grant Agreement (Rural Electrification and Renewable Energy
OBA Urban Sanitation Facility for the Greater Accra Metropolitan Area (GAMA) (P145139)
 (P145139)") Public Disclosure Authorized AFRICA Ghana Water Global Practice Recipient Executed Activities Investment Project Financing FY 2014 Seq No: 3 ARCHIVED on 10-May-2017 ISR25522 Implementing Agencies: Public
Public Disclosure Authorized AFRICA Ghana Water Global Practice Recipient Executed Activities Investment Project Financing FY 2014 Seq No: 3 ARCHIVED on 10-May-2017 ISR25522 Implementing Agencies: Public
Project Administration Instructions
 Project Administration Instructions PAI 1.01 Page 1 of 5 INITIAL PROJECT ADMINISTRATION ACTIVITIES A. Introduction 1. The Project Administration Instructions (PAIs) outline ADB s policies and procedures
Project Administration Instructions PAI 1.01 Page 1 of 5 INITIAL PROJECT ADMINISTRATION ACTIVITIES A. Introduction 1. The Project Administration Instructions (PAIs) outline ADB s policies and procedures
COUNTRY PROFILE: LIBERIA LIBERIA COMMUNITY HEALTH PROGRAMS JANUARY 2014
 COUNTRY PROFILE: LIBERIA JANUARY 2014 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
COUNTRY PROFILE: LIBERIA JANUARY 2014 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
India: Agribusiness Infrastructure Development Investment Program (Tranche 2)
") Completion Report Project Number: 37091-033 Loan Number: 2837 August 2017 India: Agribusiness Infrastructure Development Investment Program (Tranche 2) This document is being disclosed to the public in
Completion Report Project Number: 37091-033 Loan Number: 2837 August 2017 India: Agribusiness Infrastructure Development Investment Program (Tranche 2) This document is being disclosed to the public in
Promoting Reproductive, Maternal, Neonatal, Child, and Adolescent Health in Mozambique
 Promoting Reproductive, Maternal, Neonatal, Child, and Adolescent Health in Mozambique An Investment Case for the Global Financing Facility POLICY Brief November 2017 Overview To accelerate progress on
Promoting Reproductive, Maternal, Neonatal, Child, and Adolescent Health in Mozambique An Investment Case for the Global Financing Facility POLICY Brief November 2017 Overview To accelerate progress on
Promoting South Asian Regional Economic Cooperation II
 Technical Assistance Report Project Number: 40371-01 Regional Capacity Development Technical Assistance (R-CDTA) December 2008 Promoting South Asian Regional Economic Cooperation II The views expressed
Technical Assistance Report Project Number: 40371-01 Regional Capacity Development Technical Assistance (R-CDTA) December 2008 Promoting South Asian Regional Economic Cooperation II The views expressed
TERMS OF REFERENCE FOR CONSULTANTS
 TERMS OF REFERENCE FOR CONSULTANTS A. Consulting Firm The Asian Development Bank (ADB) will engage a consulting firm in accordance with its Guidelines on the Use of Consultants (2013, as amended from time
TERMS OF REFERENCE FOR CONSULTANTS A. Consulting Firm The Asian Development Bank (ADB) will engage a consulting firm in accordance with its Guidelines on the Use of Consultants (2013, as amended from time
GRANT AGREEMENT (Special Operations) (Hairatan to Mazar-e-Sharif Railway Project) between ISLAMIC REPUBLIC OF AFGHANISTAN. and ASIAN DEVELOPMENT BANK
 (Hairatan to Mazar-e-Sharif Railway Project) between ISLAMIC REPUBLIC OF AFGHANISTAN. and ASIAN DEVELOPMENT BANK") GRANT NUMBER 0161-AFG(SF) GRANT AGREEMENT (Special Operations) (Hairatan to Mazar-e-Sharif Railway Project) between ISLAMIC REPUBLIC OF AFGHANISTAN and ASIAN DEVELOPMENT BANK DATED 30 SEPTEMBER 2009 GAS:
GRANT NUMBER 0161-AFG(SF) GRANT AGREEMENT (Special Operations) (Hairatan to Mazar-e-Sharif Railway Project) between ISLAMIC REPUBLIC OF AFGHANISTAN and ASIAN DEVELOPMENT BANK DATED 30 SEPTEMBER 2009 GAS:
Rural Community Finance Project. Negotiated financing agreement
 Document: EB 2015/LOT/P.37/Sup.1 Date: 17 December 2015 Distribution: Public Original: English E Republic of Liberia Rural Community Finance Project Negotiated financing agreement For: Information Negotiated
Document: EB 2015/LOT/P.37/Sup.1 Date: 17 December 2015 Distribution: Public Original: English E Republic of Liberia Rural Community Finance Project Negotiated financing agreement For: Information Negotiated
FOR OFFICIAL USE ONLY RESTRUCTURING PAPER ON A
 Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY Report No: RES22379 Public Disclosure Authorized Public Disclosure Authorized RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING
Public Disclosure Authorized Document of The World Bank FOR OFFICIAL USE ONLY Report No: RES22379 Public Disclosure Authorized Public Disclosure Authorized RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING
Sources for Sick Child Care in India
 Sources for Sick Child Care in India Jessica Scranton The private sector is the dominant source of care in India. Understanding if and where sick children are taken for care is critical to improve case
Sources for Sick Child Care in India Jessica Scranton The private sector is the dominant source of care in India. Understanding if and where sick children are taken for care is critical to improve case
Précis WORLD BANK OPERATIONS EVALUATION DEPARTMENT WINTER 1999 N U M B E R 1 7 6
 Précis WORLD BANK OPERATIONS EVALUATION DEPARTMENT WINTER 1999 N U M B E R 1 7 6 Meeting the Health Care Challenge in Zimbabwe HE WORLD BANK HAS USUALLY DONE THE RIGHT thing in the Zimbabwe health sector,
Précis WORLD BANK OPERATIONS EVALUATION DEPARTMENT WINTER 1999 N U M B E R 1 7 6 Meeting the Health Care Challenge in Zimbabwe HE WORLD BANK HAS USUALLY DONE THE RIGHT thing in the Zimbabwe health sector,
DOCUMENTS GPOBA GRANT NUMBER TF Global Partnership on Output-based Aid. Grant Agreement
 GPOBA GRANT NUMBER TF092629 DOCUMENTS Global Partnership on Output-based Aid Grant Agreement (Extending Telecommunications in Rural Indonesia Project) between REPUBLIC OF INDONESIA and INTERNATIONAL BANK
GPOBA GRANT NUMBER TF092629 DOCUMENTS Global Partnership on Output-based Aid Grant Agreement (Extending Telecommunications in Rural Indonesia Project) between REPUBLIC OF INDONESIA and INTERNATIONAL BANK
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r
 RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
In , WHO technical cooperation with the Government is expected to focus on the following WHO strategic objectives:
 VANUATU Vanuatu, a Melanesian archipelago of 83 islands and more than 100 languages, has a land mass of 12 189 square kilometres and a population of 234 023 in 2009 (National Census). Vanuatu has a young
VANUATU Vanuatu, a Melanesian archipelago of 83 islands and more than 100 languages, has a land mass of 12 189 square kilometres and a population of 234 023 in 2009 (National Census). Vanuatu has a young
ASIAN DEVELOPMENT BANK Operations Evaluation Department
 ASIAN DEVELOPMENT BANK Operations Evaluation Department PROJECT PERFORMANCE EVALUATION REPORT IN THE LAO PEOPLE S DEMOCRATIC REPUBLIC In this electronic file, the report is followed by Management s response.
ASIAN DEVELOPMENT BANK Operations Evaluation Department PROJECT PERFORMANCE EVALUATION REPORT IN THE LAO PEOPLE S DEMOCRATIC REPUBLIC In this electronic file, the report is followed by Management s response.
Trust Fund Grant Agreement
 Public Disclosure Authorized CONFORMED COPY GRANT NUMBER TF057872-GZ Public Disclosure Authorized Trust Fund Grant Agreement (Palestinian NGO-III Project) Public Disclosure Authorized between INTERNATIONAL
Public Disclosure Authorized CONFORMED COPY GRANT NUMBER TF057872-GZ Public Disclosure Authorized Trust Fund Grant Agreement (Palestinian NGO-III Project) Public Disclosure Authorized between INTERNATIONAL
AUDIT UNDP BOSNIA AND HERZEGOVINA GRANTS FROM THE GLOBAL FUND TO FIGHT AIDS, TUBERCULOSIS AND MALARIA. Report No Issue Date: 15 January 2014
 UNITED NATIONS DEVELOPMENT PROGRAMME AUDIT OF UNDP BOSNIA AND HERZEGOVINA GRANTS FROM THE GLOBAL FUND TO FIGHT AIDS, TUBERCULOSIS AND MALARIA Report No. 1130 Issue Date: 15 January 2014 Table of Contents
UNITED NATIONS DEVELOPMENT PROGRAMME AUDIT OF UNDP BOSNIA AND HERZEGOVINA GRANTS FROM THE GLOBAL FUND TO FIGHT AIDS, TUBERCULOSIS AND MALARIA Report No. 1130 Issue Date: 15 January 2014 Table of Contents
Indonesia Project for Strengthening District Health in Sulawesi
 Indonesia Project for Strengthening District Health in External Evaluator: Taro Tsubogo (KRI International Corp.) and Ministry of Health 1 1. Project Profile and Japan s ODA Loan Field Survey: October,
Indonesia Project for Strengthening District Health in External Evaluator: Taro Tsubogo (KRI International Corp.) and Ministry of Health 1 1. Project Profile and Japan s ODA Loan Field Survey: October,
HEALTH POLICY, LEGISLATION AND PLANS
 HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
Public Disclosure Copy. Implementation Status & Results Report Second Private Sector Competitiveness and Economic Diversification Prj (P144933)
") Public Disclosure Authorized AFRICA Lesotho Finance, Competitiveness and Innovation Global Practice IBRD/IDA Investment Project Financing FY 2014 Seq No: 10 ARCHIVED on 08-May-2018 ISR30476 Implementing
Public Disclosure Authorized AFRICA Lesotho Finance, Competitiveness and Innovation Global Practice IBRD/IDA Investment Project Financing FY 2014 Seq No: 10 ARCHIVED on 08-May-2018 ISR30476 Implementing
Report and Recommendation of the President to the Board of Directors
 Report and Recommendation of the President to the Board of Directors Project Number: 44304-01 October 2010 Proposed Loan and Administration of Grant Papua New Guinea: Microfinance Expansion Project CURRENCY
Report and Recommendation of the President to the Board of Directors Project Number: 44304-01 October 2010 Proposed Loan and Administration of Grant Papua New Guinea: Microfinance Expansion Project CURRENCY
India: Madhya Pradesh State Roads Sector Project II
 Completion Report Project Number: 37328-013 Loan Number: 2330 September 2015 India: Madhya Pradesh State Roads Sector Project II This document is being disclosed to the public in accordance with ADB s
Completion Report Project Number: 37328-013 Loan Number: 2330 September 2015 India: Madhya Pradesh State Roads Sector Project II This document is being disclosed to the public in accordance with ADB s
Implementation Status & Results Congo, Democratic Republic of Emergency Demobilization and Reintegration Project (P078658)
") Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results Congo, Democratic Republic of Emergency Demobilization and Reintegration Project (P078658) Operation
Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results Congo, Democratic Republic of Emergency Demobilization and Reintegration Project (P078658) Operation
IMCI at the Referral Level: Hospital IMCI
 Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI at the Referral Level: Hospital IMCI 6 IMCI at the Referral Level: Hospital IMCI Hospital referral care:
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI at the Referral Level: Hospital IMCI 6 IMCI at the Referral Level: Hospital IMCI Hospital referral care:
Report and Recommendation of the President to the Board of Directors
 Report and Recommendation of the President to the Board of Directors Project Number: 47354-003 April 2015 Proposed Results-Based Loan and Administration of Technical Assistance Grant India: Supporting
Report and Recommendation of the President to the Board of Directors Project Number: 47354-003 April 2015 Proposed Results-Based Loan and Administration of Technical Assistance Grant India: Supporting
Cambodia: Reproductive Health Care
 Cambodia: Reproductive Health Care Ex post evaluation report OECD sector BMZ project ID 2002 66 619 Project executing agency Consultant Year of ex-post evaluation report 13020/Reproductive health care
Cambodia: Reproductive Health Care Ex post evaluation report OECD sector BMZ project ID 2002 66 619 Project executing agency Consultant Year of ex-post evaluation report 13020/Reproductive health care
The World Bank Swaziland Health, HIV/AIDS and TB Project (P110156)
") Public Disclosure Authorized AFRICA Swaziland Health, Nutrition & Population Global Practice IBRD/IDA Specific Investment Loan FY 2011 Seq No: 12 ARCHIVED on 29-Jun-2017 ISR28124 Implementing Agencies:
Public Disclosure Authorized AFRICA Swaziland Health, Nutrition & Population Global Practice IBRD/IDA Specific Investment Loan FY 2011 Seq No: 12 ARCHIVED on 29-Jun-2017 ISR28124 Implementing Agencies:
The World Bank Vietnam Climate Innovation Center (VCIC) RETF (P155260)
 RETF (P155260)") Public Disclosure Authorized Public Disclosure Authorized The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF VIETNAM CLIMATE INNOVATION CENTER (VCIC) RETF APPROVED ON OCTOBER 30,
Public Disclosure Authorized Public Disclosure Authorized The World Bank RESTRUCTURING PAPER ON A PROPOSED PROJECT RESTRUCTURING OF VIETNAM CLIMATE INNOVATION CENTER (VCIC) RETF APPROVED ON OCTOBER 30,
National Programme for Family Planning and Primary Health Care
 Government of Pakistan Ministry of Health PHC Wing National Programme for Family Planning and Primary Health Care The Lady Health Workers Programme 2008 Background and Objectives The Lady Health Workers
Government of Pakistan Ministry of Health PHC Wing National Programme for Family Planning and Primary Health Care The Lady Health Workers Programme 2008 Background and Objectives The Lady Health Workers
This document is being disclosed to the public in accordance with ADB s Public Communications Policy 2011.
 Technical Assistance Report Project Number: 51336-001 Knowledge and Support Technical Assistance (KSTA) February 2018 Capacity Building Support for Asia-Pacific Economic Cooperation Financial Regulators
Technical Assistance Report Project Number: 51336-001 Knowledge and Support Technical Assistance (KSTA) February 2018 Capacity Building Support for Asia-Pacific Economic Cooperation Financial Regulators
Terms of Reference. Consultancy for Third Party Monitor for the Aga Khan Development Network Health Action Plan for Afghanistan (HAPA)
") Terms of Reference Consultancy for Third Party Monitor for the Aga Khan Development Network Health Action Plan for Afghanistan (HAPA) I. Purpose and Objectives of the Assignment Aga Khan Foundation Canada
Terms of Reference Consultancy for Third Party Monitor for the Aga Khan Development Network Health Action Plan for Afghanistan (HAPA) I. Purpose and Objectives of the Assignment Aga Khan Foundation Canada
National Health Strategy
 State of Palestine Ministry of Health General directorate of Health Policies and Planning National Health Strategy 2017-2022 DRAFT English Summary By Dr. Ola Aker October 2016 National policy agenda Policy
State of Palestine Ministry of Health General directorate of Health Policies and Planning National Health Strategy 2017-2022 DRAFT English Summary By Dr. Ola Aker October 2016 National policy agenda Policy
The World Bank Swaziland Health, HIV/AIDS and TB Project (P110156)
") Public Disclosure Authorized AFRICA Swaziland Health, Nutrition & Population Global Practice IBRD/IDA Specific Investment Loan FY 2011 Seq No: 10 ARCHIVED on 27-Jun-2016 ISR24063 Implementing Agencies:
Public Disclosure Authorized AFRICA Swaziland Health, Nutrition & Population Global Practice IBRD/IDA Specific Investment Loan FY 2011 Seq No: 10 ARCHIVED on 27-Jun-2016 ISR24063 Implementing Agencies:
Loan No INO: POOR FARMERS INCOME IMPROVEMENT THROUGH INNOVATION PROJECT. INCEPTION MISSION May 21 June 5, 2003 MEMORANDUM OF UNDERSTANDING
 Loan No. 1909-INO: POOR FARMERS INCOME IMPROVEMENT THROUGH INNOVATION PROJECT I. INTRODUCTION INCEPTION MISSION May 21 June 5, 2003 MEMORANDUM OF UNDERSTANDING 1. An ADB Inception Mission (the Mission)
Loan No. 1909-INO: POOR FARMERS INCOME IMPROVEMENT THROUGH INNOVATION PROJECT I. INTRODUCTION INCEPTION MISSION May 21 June 5, 2003 MEMORANDUM OF UNDERSTANDING 1. An ADB Inception Mission (the Mission)
El Salvador: Basic Health Programme in the Region Zona Oriente / Basic health infrastructure
 El Salvador: Basic Health Programme in the Region Zona Oriente Ex post evaluation OECD sector BMZ programme ID 1995 67 025 Programme-executing agency Consultant 1220 / Basic health infrastructure Ministry
El Salvador: Basic Health Programme in the Region Zona Oriente Ex post evaluation OECD sector BMZ programme ID 1995 67 025 Programme-executing agency Consultant 1220 / Basic health infrastructure Ministry
Period of June 2008 June 2011 Partner Country s Implementing Organization: Federal Cooperation
 Summary of Terminal Evaluation Results 1. Outline of the Project Country: Sudan Project title: Frontline Maternal and Child Health Empowerment Project (Mother Nile Project) Issue/Sector: Maternal and Child
Summary of Terminal Evaluation Results 1. Outline of the Project Country: Sudan Project title: Frontline Maternal and Child Health Empowerment Project (Mother Nile Project) Issue/Sector: Maternal and Child
Sudan High priority 2b - The principal purpose of the project is to advance gender equality Gemta Birhanu,
 Sudan 2017 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives WORLD RELIEF (WORLD RELIEF) Comprehensive Primary Health Care Services For Vulnerable Communities in West
Sudan 2017 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives WORLD RELIEF (WORLD RELIEF) Comprehensive Primary Health Care Services For Vulnerable Communities in West
PROJECT INFORMATION DOCUMENT (PID) APPRAISAL STAGE Report No.: PIDA2678. Project Name. Region. Country
 APPRAISAL STAGE Report No.: PIDA2678. Project Name. Region. Country") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized PROJECT INFORMATION DOCUMENT (PID) APPRAISAL STAGE Report No.: PIDA2678 Project Name
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized PROJECT INFORMATION DOCUMENT (PID) APPRAISAL STAGE Report No.: PIDA2678 Project Name
Biennial Collaborative Agreement
 Biennial Collaborative Agreement between the Ministry of Health of Kazakhstan and the Regional Office for Europe of the World Health Organization 2010/2011 Signed by: For the Ministry of Health Signature
Biennial Collaborative Agreement between the Ministry of Health of Kazakhstan and the Regional Office for Europe of the World Health Organization 2010/2011 Signed by: For the Ministry of Health Signature
Rural Enterprise Finance Project. Negotiated financing agreement
 Document: EB 2018/123/R.8/Sup.1 Agenda: 5(a)(i) Date: 6 April 2018 Distribution: Public Original: English E Republic of Mozambique Rural Enterprise Finance Project Negotiated financing agreement Executive
Document: EB 2018/123/R.8/Sup.1 Agenda: 5(a)(i) Date: 6 April 2018 Distribution: Public Original: English E Republic of Mozambique Rural Enterprise Finance Project Negotiated financing agreement Executive
Implementation Status & Results Swaziland Swaziland Health, HIV/AIDS and TB Project (P110156)
") Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results Swaziland Swaziland Health, HIV/AIDS and TB Project (P110156) Operation Name: Swaziland Health,
Public Disclosure Authorized Public Disclosure Authorized The World Bank Implementation Status & Results Swaziland Swaziland Health, HIV/AIDS and TB Project (P110156) Operation Name: Swaziland Health,
ASIAN DEVELOPMENT BANK
 ASIAN DEVELOPMENT BANK PROJECT ADMINISTRATION MEMORANDUM FOR THE JFPR GRANT ASSISTANCE TO THE LAO PEOPLE S DEMOCRATIC REPUBLIC FOR COMMUNITY ACTION FOR PREVENTING HIV/AIDS 1/ (JFPR: REG-9006) DRAFT 29
ASIAN DEVELOPMENT BANK PROJECT ADMINISTRATION MEMORANDUM FOR THE JFPR GRANT ASSISTANCE TO THE LAO PEOPLE S DEMOCRATIC REPUBLIC FOR COMMUNITY ACTION FOR PREVENTING HIV/AIDS 1/ (JFPR: REG-9006) DRAFT 29
HEALTH POLICY, LEGISLATION AND PLANS
 HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
HEALTH POLICY, LEGISLATION AND PLANS Health Policy Policy guidelines for health service provision and development have also been provided in the Constitutions of different administrative period. The following
THE GLOBAL FUND to Fight AIDS, Tuberculosis and Malaria
 THE GLOBAL FUND to Fight AIDS, Tuberculosis and Malaria Guidelines for Performance-Based Funding Table of Contents 1. Introduction 2. Overview 3. The Grant Agreement: Intended Program Results and Budget
THE GLOBAL FUND to Fight AIDS, Tuberculosis and Malaria Guidelines for Performance-Based Funding Table of Contents 1. Introduction 2. Overview 3. The Grant Agreement: Intended Program Results and Budget
Proposed Grant Assistance Kyrgyz Republic: Improving Livelihoods of Rural Women through Development of Handicrafts Industry
 Grant Assistance Report Project Number: 40539 November 2006 Proposed Grant Assistance Kyrgyz Republic: Improving Livelihoods of Rural Women through Development of Handicrafts Industry (Financed by the
Grant Assistance Report Project Number: 40539 November 2006 Proposed Grant Assistance Kyrgyz Republic: Improving Livelihoods of Rural Women through Development of Handicrafts Industry (Financed by the
Solomon Islands experience Final 5 June 2004
 Solomon Islands experience Final 5 June 2004 1. Background Information Solomon Islands is a Pacific island nation with a total population of 409,042, an annual growth rate of 2.8% and a life expectancy
Solomon Islands experience Final 5 June 2004 1. Background Information Solomon Islands is a Pacific island nation with a total population of 409,042, an annual growth rate of 2.8% and a life expectancy
Afghanistan Reconstruction Trust Fund Grant Agreement
 Public Disclosure Authorized OFFICIAL DOCUMENTS ARTF GRANT NUMBER TFOAO730 Public Disclosure Authorized Public Disclosure Authorized Afghanistan Reconstruction Trust Fund Grant Agreement (Higher Education
Public Disclosure Authorized OFFICIAL DOCUMENTS ARTF GRANT NUMBER TFOAO730 Public Disclosure Authorized Public Disclosure Authorized Afghanistan Reconstruction Trust Fund Grant Agreement (Higher Education
Mongolia: Managing Soil Pollution in Ger Areas through Improved On-site Sanitation Project
 Trust Fund Project Administration Manual Project Number: 49113 Grant Numbers: GXXXX October 2016 Mongolia: Managing Soil Pollution in Ger Areas through Improved On-site Sanitation Project (Financed by
Trust Fund Project Administration Manual Project Number: 49113 Grant Numbers: GXXXX October 2016 Mongolia: Managing Soil Pollution in Ger Areas through Improved On-site Sanitation Project (Financed by
CONCEPT NOTE Community Maternal and Child Health Project Relevance of the Action Final direct beneficiaries
 CONCEPT NOTE Project Title: Community Maternal and Child Health Project Location: Koh Kong, Kep and Kampot province, Cambodia Project Period: 24 months 1 Relevance of the Action 1.1 General analysis of
CONCEPT NOTE Project Title: Community Maternal and Child Health Project Location: Koh Kong, Kep and Kampot province, Cambodia Project Period: 24 months 1 Relevance of the Action 1.1 General analysis of
PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Report No.: AB5998 Project Name. Leveraging ICT for Governance, Growth and Employment Project Region
 CONCEPT STAGE Report No.: AB5998 Project Name. Leveraging ICT for Governance, Growth and Employment Project Region") Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Report No.: AB5998 Project Name Leveraging
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized PROJECT INFORMATION DOCUMENT (PID) CONCEPT STAGE Report No.: AB5998 Project Name Leveraging
Prof E Seekoe Head: School of Health Sciences & ASELPH Programme Manager
 Prof E Seekoe Head: School of Health Sciences & ASELPH Programme Manager Strengthening health system though quality improvement is the National Health Ministers response to the need for transforming policy
Prof E Seekoe Head: School of Health Sciences & ASELPH Programme Manager Strengthening health system though quality improvement is the National Health Ministers response to the need for transforming policy