2016 Medical Home Summit. Reducing Hospital. Innovative Model of Care
|
|
|
- Barbra Cooper
- 5 years ago
- Views:
Transcription
1 2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD
2 Who We Are Since our inception in 1994, New West Physicians has grown to become the largest primary care group practice in Colorado Primary care, hospitalists, mid levels, and selected specialties 100+ providers 17 offices throughout the Denver Metro area Employees - $58M Revenue
3 Quality In 2011, the American Hospital Association commissioned a national study on Accountable Care and chose four delivery systems representing different models of care. New West Physicians was chosen as the primary care model for that study. In 2013, New West Physicians received the Colorado Best Practice of the Year Award by the Colorado Academy of Family Physicians Foundation. In 2015 the AMGA awarded NWP the Acclaim Award for the organization which most closely approaches the ideal health system as measured by the IOM Triple Aim
4 Critical Issue of Readmissions Medicare 30 day all cause readmission rate = 18% Yearly cost to CMS = $17 billion Large impact on MA risk pools CMS Star 3 point measure
5 NWP Readmission rate Medicare 6.6% Commercial 3.1%
6 Reasons for Readmission Medication reconciliation issues Inadequate transition of care planning Delayed follow-up with PCP Lack of follow-up on needed post discharge issues Communication breakdown with patient/family
7 PCP as Care Coordinator Supported by infrastructure Diabetes Center Behavioral Health Center SWAT Team Urgent Care Center Case management in the ER TOC Program
8 Top 10 Admission Diagnoses DESCRIPTION Count Claim Amount LOC OSTEOARTHROSIS-LOWER LEG 206 $1,133,342 UNSPECIFIED SEPTICEMIA 116 $724,834 LOC OSTEOARTHROSIS-PELVIC RGN&THIGH 78 $445,706 ACUT MI SUBNDOCRDL INFARCT INIT EOC 54 $345,539 PNEUMONIA, ORGANISM UNSPECIFIED 54 $192,950 UNSPECIFIED ACUTE RENAL FAILURE 48 $144,540 OBST CHRONIC BRONCHITIS W/EXACERBAT 46 $143,862 ATRIAL FIBRILLATION 46 $102,772 CLOS FX INTERTROCH SECTION FEM 40 $214,582 ACUTE RESPIRATORY FAILURE 40 $208,121
9 Hospital Program NWP Hospitalists at our 5 main hospitals NWP Case management daily at all facilities At every admission: Psychosocial evaluation Home safety evaluation Evaluation of any outpatient PCP deficiencies Advanced directives
10 Emergency Room Management Appropriate patients evaluated in ER Case management in ER with direct SNF transfer Hospitalist ER Programs Atrial fibrillation Syncope Chest pain
11 Patient Perception of Discharge From total care to zero care there is no button to push! Passive care to active care Bewildering circumstances Degree of disability underestimated
12 Transitions of Care Three areas of responsibility Inpatient case manager Hospitalist Transition of care mid level provider
13 Transitions of Care Case Manager Responsibilities Correct level of care chosen All ancillaries arranged Family expectations clarified Psychosocial issues addressed
14 Transitions of Care Hospitalist Responsibilities PCP Contacted on day of discharge TOC Midlevel contacted for complex cases Key issues, findings, and follow-up items tasked to the PCP at time of discharge SNF Transfers SNFist contacted and discharge summary completed at time of discharge
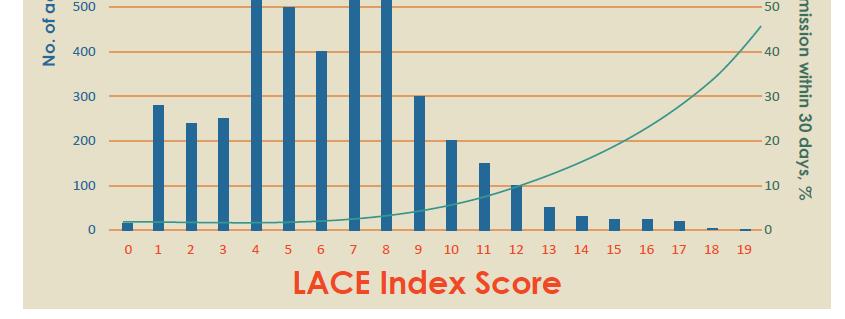
15 Transitions of Care TOC Midlevel Responsibilities Red/yellow/green designation LACE Model Telephonic contact with patient Med reconciliation PCP Follow-up scheduled Specialty and ancillary follow-up arranged
16 Lace Model Length of stay Acuity of the admission Co-morbidities Emergency room visits in the prior 6 months Lace scores range from 1-19 and predict the risk of death and readmission in the first 30 days post discharge
17 Charlson Co-Morbidity Score 1 each: Myocardial infarct, congestive heart failure, peripheral vascular disease, dementia, cerebrovascular disease, chronic lung disease, connective tissue disease, ulcer, chronic liver disease, diabetes. 2 each: Hemiplegia, moderate or severe kidney disease, diabetes with end organ damage, tumor, leukemia, lymphoma. 3 each: Moderate or severe liver disease. 6 each: Malignant tumor, metastasis, AIDS.
18
19
20 Use of Lace Tool 6-9 score Mid level judgment as to whether to refer to case management 10 or above all referred to case management Patients with very complex initial presentations are referred irrespective of Lace score
21 Transitions of Care TOC Midlevel/PCP Integration PCP tasked with all details of communication Medication list reconciled/rx s sent if needed Problem list updated including new RAF codes All hospital records forwarded Follow-up appointment scheduled
22 SNF Management Dedicated SNF Network Admissions 24/7 including ER High quality/efficiency facilities Single SNF practice covers citywide Hospitalists contacted prior to transfer Case managers on site for review and meetings twice weekly
23 Advanced Care Planning Transitional care program designed for intensive home based 3 month case management for advanced and/or complex illness Palliative care program mandatory for oncologists to introduce palliative care for all Stage III and IV cancers Hospice care program integrated with the above two programs
24 Optio Care Support Pilot of NWP and Denver Hospice Collaborative approach with Registered Nurse and Licensed Social Worker In home and telephonic Focus: Engagement with primary care physician Medication reconciliation and management Red Flag education Steps to recognize change in health and empower client to take appropriate action Address psychosocial needs that are inhibiting the client to manage health Successful hand-off at end of care cycle to case manager within PCP practice
25
26 Who Will Succeed? Shift from patient to population management Comprehensive care at all levels and locations Accurate, timely and actionable data Focused case management Aligned compensation model
27 Thank you and Opportunity for Questions Scott Clemens, MD 9950 W. 80 th Ave Ste23, Arvada, CO The mission of New West Physicians is "to enhance the physical, mental and spiritual health of communities we serve through an integrated, primary-care owned and patient centered healthcare delivery system."
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Saint Agnes Hospital. Pharmacist utilization of the LACE tool to prevent hospital readmissions. Program/Project Description, including Goals:
 Saint Agnes Hospital Pharmacist utilization of the LACE tool to prevent hospital readmissions Program/Project Description, including Goals: Safe transitions of care have always been a frontline patient
Saint Agnes Hospital Pharmacist utilization of the LACE tool to prevent hospital readmissions Program/Project Description, including Goals: Safe transitions of care have always been a frontline patient
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Improve Your Revenue for the Services Your Provide with Proper Coding and Documentation. by Christina Rock, BSN, RN Supervisor, Clinical Education
 Improve Your Revenue for the Services Your Provide with Proper Coding and Documentation by Christina Rock, BSN, RN Supervisor, Clinical Education Objectives Awareness of resources and reference materials
Improve Your Revenue for the Services Your Provide with Proper Coding and Documentation by Christina Rock, BSN, RN Supervisor, Clinical Education Objectives Awareness of resources and reference materials
Appendix: Assessments from Coping with Cancer
 Appendix: Assessments from Coping with Cancer Primary Independent Variable of Interest (assessed at baseline with medical chart review and confirmed with clinician) 1. What treatments is the patient currently
Appendix: Assessments from Coping with Cancer Primary Independent Variable of Interest (assessed at baseline with medical chart review and confirmed with clinician) 1. What treatments is the patient currently
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017
 Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
O U T C O M E. record-based. measures HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT
 HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT record-based O U Michael Goldacre, David Yeates, Susan Flynn and Alastair Mason National Centre for Health Outcomes Development
HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT record-based O U Michael Goldacre, David Yeates, Susan Flynn and Alastair Mason National Centre for Health Outcomes Development
Comparison of Care in Hospital Outpatient Departments and Physician Offices
 Comparison of Care in Hospital Outpatient Departments and Physician Offices Final Report Prepared for: American Hospital Association February 2015 Berna Demiralp, PhD Delia Belausteguigoitia Qian Zhang,
Comparison of Care in Hospital Outpatient Departments and Physician Offices Final Report Prepared for: American Hospital Association February 2015 Berna Demiralp, PhD Delia Belausteguigoitia Qian Zhang,
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
domains of disorders 1. Urgent/Emergent Care and challenge 2. HUMS hypothesis 3. High users, multiple systems, and multiple
 Maria X Martinez 1. Urgent/Emergent Care and challenge 2. HUMS hypothesis 3. High users, multiple systems, and multiple domains of disorders 4. Was FY 11-12 different? 5. IDS goals: 1. Targeted Street
Maria X Martinez 1. Urgent/Emergent Care and challenge 2. HUMS hypothesis 3. High users, multiple systems, and multiple domains of disorders 4. Was FY 11-12 different? 5. IDS goals: 1. Targeted Street
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
10/2/2017. Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative. Problem. Problem
 Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Referrals, Prior Authorizations, Medical Management, and Appeals
 Referrals, Prior Authorizations, Medical Management, and Appeals 1 An Independent Licensee of the Blue Cross Blue Shield Association 044506 (12-21-2017) 2017 Premera. Proprietary and Confidential. Referrals
Referrals, Prior Authorizations, Medical Management, and Appeals 1 An Independent Licensee of the Blue Cross Blue Shield Association 044506 (12-21-2017) 2017 Premera. Proprietary and Confidential. Referrals
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
Medicare Advantage in Practice: Enhanced Care Models for High Need Patients
 Medicare Advantage in Practice: Enhanced Care Models for High Need Patients Rebekah Dube, Pharm.D. VP, Health Plan Clinical Programs & Interim VP, Health Plan Products Who is Martin s Point Health Care?
Medicare Advantage in Practice: Enhanced Care Models for High Need Patients Rebekah Dube, Pharm.D. VP, Health Plan Clinical Programs & Interim VP, Health Plan Products Who is Martin s Point Health Care?
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Model of Care Training
 Medicare Advantage Special Needs Plan Chronic Care Program Model of Care Training 2012-2013 Course Overview This course will describe: PHP s Model of Care Chronic Care Program Health Homes Interdisciplinary
Medicare Advantage Special Needs Plan Chronic Care Program Model of Care Training 2012-2013 Course Overview This course will describe: PHP s Model of Care Chronic Care Program Health Homes Interdisciplinary
New pharmacy practice opportunity: Enhancement of the transitions of care process
 New pharmacy practice opportunity: Enhancement of the transitions of care process EMMA GORMAN, PHARMD CLINICAL ASSISTANT PROFESSOR DEPARTMENT OF PHARMACY PRACTICE D YOUVILLE SCHOOL OF PHARMACY BUFFALO,
New pharmacy practice opportunity: Enhancement of the transitions of care process EMMA GORMAN, PHARMD CLINICAL ASSISTANT PROFESSOR DEPARTMENT OF PHARMACY PRACTICE D YOUVILLE SCHOOL OF PHARMACY BUFFALO,
From Risk Scores to Impactability Scores:
 From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
BreakThrough Care Center: A New Care Model for High Risk Patients. Dr. Richard Krouse Dr. Paul Merrick
 BreakThrough Care Center: A New Care Model for High Risk Patients Dr. Richard Krouse Dr. Paul Merrick About DMG Why Population Health About BreakThrough Care Center Patient Stories Questions? About DuPage
BreakThrough Care Center: A New Care Model for High Risk Patients Dr. Richard Krouse Dr. Paul Merrick About DMG Why Population Health About BreakThrough Care Center Patient Stories Questions? About DuPage
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM
 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling
 Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
The Physician s Perspective
 The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Highline Health Connections: Care Navigation for Vulnerable Populations
 Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
Retrospective Bundles
 Bundled Payment for Care Improvement (BPCI) Overview Shawn Matheson MBA, LNHA, FACHCA Market Manager Idaho Health Care Association Annual Convention Boise, ID July 13, 2017 Retrospective Bundles Surgeon
Bundled Payment for Care Improvement (BPCI) Overview Shawn Matheson MBA, LNHA, FACHCA Market Manager Idaho Health Care Association Annual Convention Boise, ID July 13, 2017 Retrospective Bundles Surgeon
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound
 Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
New Options in Chronic Care Management
 New Options in Chronic Care Management Numbers reveal the need for CCM, as it eases the burden for patients and providers. 2015 Wellbox Inc. No portion of this white paper may be used or duplicated by
New Options in Chronic Care Management Numbers reveal the need for CCM, as it eases the burden for patients and providers. 2015 Wellbox Inc. No portion of this white paper may be used or duplicated by
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
The new role of hospitalists. Keeping patients out of the hospital. Cynthia Litt, MPH Eugene Kim, MD
 The new role of hospitalists. Keeping patients out of the hospital Cynthia Litt, MPH Eugene Kim, MD Cedars-Sinai Health System Cedars-Sinai Medical Center Medical Delivery Network Education and Research
The new role of hospitalists. Keeping patients out of the hospital Cynthia Litt, MPH Eugene Kim, MD Cedars-Sinai Health System Cedars-Sinai Medical Center Medical Delivery Network Education and Research
Central Ohio Primary Care (COPC) Spotlight on Innovation
 Spotlight on Innovation") Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Sandra Robinson, RN, MSN, ACM, CEN
 Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Integrated Care Management in the Age of Population Health: What does that mean?!?
 Integrated Care Management in the Age of Population Health: What does that mean?!? Integrated Care Management Conference September 21 and 22, 2016 Dot Verbrugge, MD Medical Director of Integrated Care
Integrated Care Management in the Age of Population Health: What does that mean?!? Integrated Care Management Conference September 21 and 22, 2016 Dot Verbrugge, MD Medical Director of Integrated Care
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
Special Needs Plan (SNP) Model of Care Training 2018
 Model of Care Training 2018") Special Needs Plan (SNP) Model of Care Training 2018 Table of Contents Training Overview Pg. 1 Denver Health Medical Plan s (HMO SNP) MOC Annual Training Pg. 2 Special Needs Plans (SNPs) Pg. 2 Special
Special Needs Plan (SNP) Model of Care Training 2018 Table of Contents Training Overview Pg. 1 Denver Health Medical Plan s (HMO SNP) MOC Annual Training Pg. 2 Special Needs Plans (SNPs) Pg. 2 Special
Intermediate Coronary Care Unit Rotation
 1 Intermediate Coronary Care Unit Rotation Section of Cardiology Dartmouth-Hitchcock Medical Center (2008-2009) I. Overview of Rotation The cardiology-specific critical care experience is in the Intermediate
1 Intermediate Coronary Care Unit Rotation Section of Cardiology Dartmouth-Hitchcock Medical Center (2008-2009) I. Overview of Rotation The cardiology-specific critical care experience is in the Intermediate
Partnering with Hospice: Reducing Skilled Nursing Facility to Hospital Readmissions
 Partnering with Hospice: Reducing Skilled Nursing Facility to Hospital Readmissions Scott Lavis, LICSW, CT Community Liaison Kline Galland Hospice Objectives for Today Quick review of regulations that
Partnering with Hospice: Reducing Skilled Nursing Facility to Hospital Readmissions Scott Lavis, LICSW, CT Community Liaison Kline Galland Hospice Objectives for Today Quick review of regulations that
Community Health Needs Assessment Three Year Summary
 Community Health Needs Assessment Three Year Summary 2013 2016 Community Health Needs Assessment Three Year Summary 2014 2016 Key needs were identified by community stakeholders which included the following:
Community Health Needs Assessment Three Year Summary 2013 2016 Community Health Needs Assessment Three Year Summary 2014 2016 Key needs were identified by community stakeholders which included the following:
Outcome Measures: Reform at the Core: Page 1. The Triple Aim Goals. Getting Down into the Weeds
 Outcome Measures: Getting Down into the Weeds LeadingAge Missouri Fall Conference 18 September 2013 Andy Edeburn, VP of Continuum Strategies 2 Reform at the Core: The Triple Aim Goals Better Care Improve/maintain
Outcome Measures: Getting Down into the Weeds LeadingAge Missouri Fall Conference 18 September 2013 Andy Edeburn, VP of Continuum Strategies 2 Reform at the Core: The Triple Aim Goals Better Care Improve/maintain
Monarch HealthCare, a Medical Group, Inc.
 Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
2015 National Training Program. History of Modern Hospice. Hospice Legislative History. Medicare s Coverage of Hospice Services
 2015 National Training Program Medicare s Coverage of Hospice Services For Those Who Counsel People With Medicare July 2015 History of Modern Hospice 1948 English physician Dame Cicely Saunders works with
2015 National Training Program Medicare s Coverage of Hospice Services For Those Who Counsel People With Medicare July 2015 History of Modern Hospice 1948 English physician Dame Cicely Saunders works with
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
2015 Quality Improvement Work Plan Summary
 2015 Quality Improvement Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how
2015 Quality Improvement Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how
Core Metrics for Better Care, Lower Costs, and Better Health
 Core Metrics for Better Care, Lower Costs, and Better Health IOM Roundtable on Value & Science-Driven Health Care September 27, 2012 Washington, D.C. Sam Nussbaum, M.D. Executive Vice President, Clinical
Core Metrics for Better Care, Lower Costs, and Better Health IOM Roundtable on Value & Science-Driven Health Care September 27, 2012 Washington, D.C. Sam Nussbaum, M.D. Executive Vice President, Clinical
2017 Catastrophic Care. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
Mental Health at Mercy Health: Treating the Whole Person. David E. Blair, MD Mercy Health Physician Partners President and CMO
 Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Mercy Virtual. Transforming Medicine and Value Through Virtual Care. Randall S Moore, MD, MBA. Orlando, FL. September, 2017
 Mercy Virtual Transforming Medicine and Value Through Virtual Care Randall S Moore, MD, MBA Orlando, FL September, 2017 The opinions expressed are those of the presenter and do not necessarily state or
Mercy Virtual Transforming Medicine and Value Through Virtual Care Randall S Moore, MD, MBA Orlando, FL September, 2017 The opinions expressed are those of the presenter and do not necessarily state or
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP)
 & Chronic Care Improvement Program (CCIP)") Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT
 1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
University Cincinnati Medical Center
 University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention
 Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Community Discharge and Rehospitalization Outcome Measures (Fiscal Year 2011)
") Andrew Kramer, MD Ron Fish, MBA Sung-joon Min, PhD Providigm, LLC Community Discharge and Rehospitalization Outcome Measures (Fiscal Year 2011) A report by staff from Providigm, LLC, for the Medicare Payment
Andrew Kramer, MD Ron Fish, MBA Sung-joon Min, PhD Providigm, LLC Community Discharge and Rehospitalization Outcome Measures (Fiscal Year 2011) A report by staff from Providigm, LLC, for the Medicare Payment
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Bundled Payment Primer
 Bundled Payment Primer CMS Opened Application February 14, 2014 Why this matters to you! Bundling is a New Business Model Bundling is a focused opportunity to manage risk and achieve gain Control of a
Bundled Payment Primer CMS Opened Application February 14, 2014 Why this matters to you! Bundling is a New Business Model Bundling is a focused opportunity to manage risk and achieve gain Control of a
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home. Your thoughts
 Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
ACO S SUCCESS AND IMPACTS ON FINANCE AND REVENUE CYCLE
 Ralph Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701.239.8594 ACO S SUCCESS AND IMPACTS ON FINANCE AND REVENUE CYCLE CONTEXT Increasing number of critical access hospitals and other rural providers
Ralph Llewellyn, CPA, CHFP Partner rllewellyn@eidebailly.com 701.239.8594 ACO S SUCCESS AND IMPACTS ON FINANCE AND REVENUE CYCLE CONTEXT Increasing number of critical access hospitals and other rural providers
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Turning Big Data Into Better Care
 Turning Big Data Into Better Care Dickson Advanced Analytics DA 2 Who is CHS and What is DA 2? 2 Who is CHS? Hospitals 42 Employees 62K Care Centers 900+ Physicians 3K Licensed Beds 7,800 Nurses 14K 3
Turning Big Data Into Better Care Dickson Advanced Analytics DA 2 Who is CHS and What is DA 2? 2 Who is CHS? Hospitals 42 Employees 62K Care Centers 900+ Physicians 3K Licensed Beds 7,800 Nurses 14K 3
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING
 HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
REDUCING READMISSIONS
 REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures. Learning Objectives
 Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Centralizing Multi-Hospital Mortality Reviews
 December 7, 2016 Session Codes: D4 (9:30am-10:45am) & E4 (11:15am - 12:30pm) Centralizing Multi-Hospital Mortality Reviews IHI 28 th National Forum Mark P Jarrett, MD, MBA, MS SVP, Chief Quality Officer,
December 7, 2016 Session Codes: D4 (9:30am-10:45am) & E4 (11:15am - 12:30pm) Centralizing Multi-Hospital Mortality Reviews IHI 28 th National Forum Mark P Jarrett, MD, MBA, MS SVP, Chief Quality Officer,
Emerging Issues in Post Acute Care Trends
 Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Down the Rabbit Hole C2C DATA & THE LA JEWISH HOME. Molly Forrest, CEO President LA Jewish Home April 4, 2017
 Down the Rabbit Hole C2C DATA & THE LA JEWISH HOME Molly Forrest, CEO President LA Jewish Home April 4, 2017 Medicare, Social Security & Medicaid Changes +65 Martin Short +75 Tina Turner Aging Today &
Down the Rabbit Hole C2C DATA & THE LA JEWISH HOME Molly Forrest, CEO President LA Jewish Home April 4, 2017 Medicare, Social Security & Medicaid Changes +65 Martin Short +75 Tina Turner Aging Today &
Community Health Excellence (CHE) Grant Program Application Guide
 Grant Program Application Guide") Community Health Excellence (CHE) Grant Program 2018 2019 Application Guide CHE Mission and Goals The PacificSource Community Health Excellence (CHE) initiative was created to align with and support the
Community Health Excellence (CHE) Grant Program 2018 2019 Application Guide CHE Mission and Goals The PacificSource Community Health Excellence (CHE) initiative was created to align with and support the
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?