Readmission Partnership Between Acute Care and Post-Acute Care
|
|
|
- Garey James
- 5 years ago
- Views:
Transcription
 Amanda Melvin, MSW Referral Development Coordinator Radford Health & Rehab Center The Woodlands Health & Rehab")
1 Readmission Partnership Between Acute Care and Post-Acute Care Melissa Suzuki, MSW Regional UR Case Manager Specialist Commonwealth Care of Roanoke (CCR) Amanda Melvin, MSW Referral Development Coordinator Radford Health & Rehab Center The Woodlands Health & Rehab Center

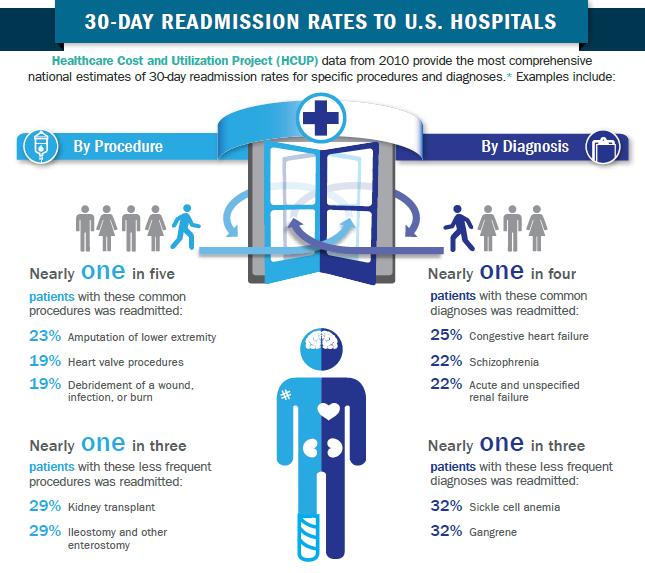
2 Acute Care Readmission Statistics Retrieved from:

3 Acute Care Readmission Statistics by Payer Retrieved from:
4 Readmissions Reduction Program Established in the 2010 Affordable Care Act, allows the CMS to withhold inpatient prospective payments to shortterm acute hospitals with excessive readmissions for certain conditions. Study published in the Annals of Internal Medicine, concluded that hospital readmissions across the U.S. indeed declined starting with the ACA, and that moreover, hospitals with the highest readmission rates before 2010 improved the most in the years following.
5 Carilion Roanoke Memorial Readmissions The Centers for Medicare & Medicaid Services will withhold $2.6 million of Roanoke Memorial s payment for fiscal year 2017 Roanoke Memorial receives about $303 million a year in revenue from Medicare and $96 million from Medicaid. The penalty is about $1.2 million less than this year, reflecting improvements that began a couple of years ago. Roanoke Memorial is among 19 out of Virginia s 79 hospitals that were penalized. Source:
6 Decreasing readmissions Roanoke Memorial began to show improvements in its readmission rate in 2015 Greater improvement came by having social workers begin to work with at-risk patients from the time they enter the emergency department to make sure they have support once they leave.
7 Programs in place at Carilion Roanoke Memorial Hospital to prevent readmissions. Care Management Department made up of : -Social Workers (MSW) -Case Managers (RN) -Utilization Management -Central Resource Center -CARES Department.
8 LACE Score used within Care Management Lace Score: = Low Risk for Readmission = Moderate Risk for Readmission = High Risk for Readmission
9 Preventing Readmissions in Acute Care Daily Rounding with Interdisciplinary Team Based Approach Biopsychosocial Assessments on all Patients Daily charting requirements in Epic Discharge instructions discussed with patient/nurse
10 Evolent Health Partners with Carilion Clinic Evolent Health partners with leading health systems to drive valuebased care transformation. Providing clinical, analytical and financial capabilities, Evolent helps physicians and health systems achieve superior quality and cost results. Evolent's approach breaks down barriers, aligns incentives and powers a new model of care delivery resulting in meaningful alignment between providers, payers, physicians and patients SOURCE: Evolent Health
 will be wearing this bracelet.")

11 CRMH HEART SURGERY PATIENT Beginning Summer 2017, all recent cardiac surgery patients discharged from Carilion Roanoke Memorial Hospital (CRMH) will be wearing this bracelet. The bracelet will remind patients or caregivers to call the Cardiothoracic Surgery Service ANYTIME they have a question OR an urgent need that takes them to an Emergency Department, Urgent Care Center, or Doctor s Office.

12 Quarterly Skilled Facility Meeting Skilled Nursing Facility Representatives/Administrators meet to discuss readmission trends and collaborate on identifying additional ways to prevent readmissions
13 Impact of Readmissions Multiple readmissions have been associated with: Increase cost of healthcare dollars (estimated $17.4 billion annually) Deterioration in overall health status Increased risk for medical errors Increased risk of duplication of services, testing, etc.. Research has shown that majority of readmissions are preventable These are associated with indicators of substandard care during the initial admission such as; poor resolutions of the main problem, unstable therapy at discharge, and inadequate post discharge care Additional research has shown that some readmissions can be prevented by implementing effective patient education, predischarge assessments, and appropriate aftercare services
14 Safe Transitions: A method to help reduce readmissions Brief History and Key Factors Definition and Purpose Prior to Admission Day of Admission During Skilled Stay Week of Discharge Day of Discharge Post Discharge
15 Brief history and Key Factors Large majority of serious medical errors involve miscommunication during the hand-off between medical providers Improving transitions between care venues has been identified as an important strategy in helping to decrease readmission rates, improve patient health, enhance patient care quality and safety, reduce inefficiencies, and lower costs Unsatisfactory care transitions increase the probability of a decline in health status, thus increasing likelihood of a readmission Key factors or root causes behind failed care transitions: Lack of provider coordination and information sharing Lack of follow up from physicians and other caregivers Lack of patient/caregiver knowledge and empowerment Accountability breakdowns
16 Definition and Purpose Safe Transitions: to provide a seamless handoff or discharge from subacute back to home or lower level of care in the community. Purpose: improve post discharge patient outcomes reduce hospital readmission rates reduce possible adverse reactions improve health maintain patient in community longer improve quality of life for patient and families
17 More Definitions and Purpose 7 Key components for a Safe Transition to occur: Leadership Support Interdisciplinary Collaboration Early Identification of Patients at Risk Transitional Planning from Day 1 Medication Management Patient and Family Engagement Transfer of Information
18 Prior to Admission Meet with patient and family at hospital Gather relevant information from Case Manager Discussions w/patient and family Set the expectations (short stay v. LTC) Determine safe transition goal Identify any potential barriers and address (i.e. copay concerns, lack of support, etc..) Schedule TBAA Complete Admission packet if able Collect any POA/Advance Directive paperwork Introduce Safe Transitions booklet
19 Initial Admission to Center Orient patient/family to center, provide Welcome Packet, escort them to their room, ensure they get settled in Admission assessments should be completed within first hours Nursing Admission Assessments and Skilled Care notes Therapy evaluations Social Work Admission assessment Activities assessment Dietary assessment and preferences TBAA held within first 72 hours Interdisciplinary attendance and engagement is critical Reiterate expectations of stay Develop plan of care with input from patient/caregiver Review goals of patient Identify barriers to obtaining goals and how they will be addressed
20 During Skilled Stay Weekly UR meeting PPS/Clinical Reimbursement management daily Critical to providing the right level of care throughout the stay Continue to analyze discharge plan and identify barriers and record these along the way Utilize Safe Transition form if patient has appointments Daily clinical meeting Analyze patient progress, changes in condition, etc.
21 Week of Safe Transition Finalize Discharge Plan Review medications with patient/family Schedule follow up appointments with PCP and specialists as indicated Ensure patient/caregiver education has been completed and utilize Teach Back method to gauge level of understanding Arrange follow up services HHC DME Community resources
22 Day of Safe Transition Provide patient/family with completed Discharge folder Contact info for HHC company Contact info for social worker or center Educational material about diagnosis Med list Discharge instruction form Review med list with patient/family again. Give them the opportunity to ask questions. Inform patient/family that they may be able to return within 30 days if they decline or don t manage well once home, instead of going to hospital
23 Post Safe Transition Social Service staff completes follow up call within initial hours after patient has left facility Big topics to focus on: Ensure patient was able to obtain meds Home Health services started Verify/confirm any scheduled follow up appointments Discuss any concerns patient/family has experienced since leaving the center Reiterate option to readmit back to center within 30 days if they experience a decline or are not able to manage at home Reiterate if they have any questions to feel free to reach back out to the center Additional follow up calls performed as needed, best practice after the initial call is to complete additional calls around 7days, 14days, and 30days. Coordinate information sharing and additional calls with downstream providers like HH if possible
24 Questions?
25 Resources Healthcare Cost and Prevention and Utilization Project HCUP Statistical Briefs #153 and #154: SOURCE Evolent Health Suzanne DelBoccio, MS, RN, CENP, FACHE; Debra F Smith, MSW, LCSW, CCM; Melissa Hicks MSN, RN-BC; Pamela Voight Lowe, MSN, RN, CPHQ, NE-BC; Joy E Graves-Rust; Jennifer Volland, DHA, RN, MBB, CPHQ, NEA- BC, FACHE; Sarah Fryda, BA, MS. Successes and Challenges in Patient Care Transition Programming. Online J Issues Nurs. 2015; 20(3). 4/26/2016 Improving Care Transitions: A Strategy for Reducing Readmissions. The Center for Improving Value in Health Care, 2012 Transitions of Care: The need for a more effective approach to continuing patient care. The Joint Commission Center for Transforming Healthcare, 2012
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Priceless Partners: Common Patients, Common Goals
 Priceless Partners: Common Patients, Common Goals Erin Hodson, RN, BSN, ACM Senior Director Case Management Inova Fairfax Hospital Pamela Andrews, RN, MSW, MBA, CCM, ACM Director Medical Management INTotal
Priceless Partners: Common Patients, Common Goals Erin Hodson, RN, BSN, ACM Senior Director Case Management Inova Fairfax Hospital Pamela Andrews, RN, MSW, MBA, CCM, ACM Director Medical Management INTotal
Mission Health Care Network. April 2017
 Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Healthcare Reimbursement Change VBP -The Future is Now
 Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
The Patient Protection and Affordable Care Act of 2010
 INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Stroke Patients: Transition From Hospital to Home
 Stroke Patients: Transition From Hospital to Home Lauren Pond RN CCM Administrative Director, Case Management Jennifer Thiesen RNP CCRN Director, Care Transitions Presenter Disclosure Information Lauren
Stroke Patients: Transition From Hospital to Home Lauren Pond RN CCM Administrative Director, Case Management Jennifer Thiesen RNP CCRN Director, Care Transitions Presenter Disclosure Information Lauren
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
snapshot Improving Experience of Care Scores Alone is NOT the Answer: Hospitals Need a Patient-Centric Foundation
 SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
The Park at Allens Creek Suite Allens Creek Road Rochester, NY 14618
 The Park at Allens Creek Suite 100 132 Allens Creek Road Rochester, NY 14618 Phone: (585) 473-7573 Fax: (585) 473-7641 www.mcms.org mcms@mcms.org Monroe County Medical Society Quality Collaborative Community
The Park at Allens Creek Suite 100 132 Allens Creek Road Rochester, NY 14618 Phone: (585) 473-7573 Fax: (585) 473-7641 www.mcms.org mcms@mcms.org Monroe County Medical Society Quality Collaborative Community
The Impact of Health Care Reform on Long- Term Care
 The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
Iowa Medicaid: Innovations & Initiatives
 Iowa Medicaid: Innovations & Initiatives ICD-10 ACA Expansion Presumptive Eligibility Health Information Technology PERM DHS Initiatives Adult Quality Measures SIM CDAC Topics 2 ICD-10 3 1 ICD-10 Background
Iowa Medicaid: Innovations & Initiatives ICD-10 ACA Expansion Presumptive Eligibility Health Information Technology PERM DHS Initiatives Adult Quality Measures SIM CDAC Topics 2 ICD-10 3 1 ICD-10 Background
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of
 2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
 Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
2 nd Annual PPS Quality and Patient Safety Conference
 2 nd Annual PPS Quality and Patient Safety Conference Jointly Sponsored by MHA and Stratis Health Welcome and Introduction Jennifer Lundblad, PhD, MBA, President & CEO, Stratis Health Healthcare-Centric
2 nd Annual PPS Quality and Patient Safety Conference Jointly Sponsored by MHA and Stratis Health Welcome and Introduction Jennifer Lundblad, PhD, MBA, President & CEO, Stratis Health Healthcare-Centric
Reducing Hospital Readmissions and The Critical Role of Physician Leadership
 Reducing Hospital Readmissions and The Critical Role of Physician Leadership The Process of Designing our Readmission Reduction Plan, the Final Plan and the Critical Role of Physician Leadership Jeffrey
Reducing Hospital Readmissions and The Critical Role of Physician Leadership The Process of Designing our Readmission Reduction Plan, the Final Plan and the Critical Role of Physician Leadership Jeffrey
Physician Compensation in an Era of New Reimbursement Models
 2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
COPD & Pneumonia Readmission Reduction Program. October 25, 2017
 COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
Case managers are consummate team players, working with. IssueBrief
 IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
Accountable Care and Governance Challenges Under the Affordable Care Act
 Accountable Care and Governance Challenges Under the Affordable Care Act The First National Congress on Healthcare Clinical Innovations, Quality Improvement and Cost Containment October 26, 2011 Doug Hastings
Accountable Care and Governance Challenges Under the Affordable Care Act The First National Congress on Healthcare Clinical Innovations, Quality Improvement and Cost Containment October 26, 2011 Doug Hastings
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Community Paramedicine Seminar July, 20th 2015
 Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT
 Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
CMS Hospital Discharge Planning Standards 101. Friday, March 21st, 2014
 CMS Hospital Discharge Planning Standards 101 Friday, March 21st, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education Consulting Board Member
CMS Hospital Discharge Planning Standards 101 Friday, March 21st, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education Consulting Board Member
ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods
 A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Health Management Policy
 Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
SIM PCMH/MiPCT Partnership Initiative Application Period - Submission Deadline September 30
 Michigan Primary Care Transformation www. mipct.org Volume 5 Issue 9 September 26, 2016 SIM PCMH/MiPCT Partnership Initiative Application Period - Submission Deadline September 30 Important Dates: MiPCT
Michigan Primary Care Transformation www. mipct.org Volume 5 Issue 9 September 26, 2016 SIM PCMH/MiPCT Partnership Initiative Application Period - Submission Deadline September 30 Important Dates: MiPCT
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Emerging Issues in Post Acute Care Trends
 Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
Central Ohio Primary Care (COPC) Spotlight on Innovation
 Spotlight on Innovation") Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Measuring Value and Outcomes for Continuous Quality Improvement. Noelle Flaherty MS, MBA, RN, CCM, CPHQ 1. Jodi Cichetti, MS, RN, BS, CCM, CPHQ
 Noelle Flaherty MS, MBA, RN, CCM, CPHQ 1 Jodi Cichetti, MS, RN, BS, CCM, CPHQ Leslie Beck, MS 1 Amanda Abraham MS 1 Maria Uriyo, PhD, MHSA, PMP 1 1. Johns Hopkins Healthcare LLC, Baltimore Maryland Corresponding
Noelle Flaherty MS, MBA, RN, CCM, CPHQ 1 Jodi Cichetti, MS, RN, BS, CCM, CPHQ Leslie Beck, MS 1 Amanda Abraham MS 1 Maria Uriyo, PhD, MHSA, PMP 1 1. Johns Hopkins Healthcare LLC, Baltimore Maryland Corresponding
ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists
 DECLINE Facility Assessment Checklists") ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to activities of daily living
ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to activities of daily living
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Post Hospital outreach Coordination of care Member education Provider collaboration
 Program Description and Summary The Care Coordination Program conducts identification and outreach to members in the home setting who may benefit from care and disease management services. The Care Coordination
Program Description and Summary The Care Coordination Program conducts identification and outreach to members in the home setting who may benefit from care and disease management services. The Care Coordination
Accountable Care in Infusion Nursing. Hudson Health Plan. Mission Statement. for all people. INS National Academy of Infusion Therapy
 Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
QUALITY AND COMPLIANCE
 2015 HCCA SOUTHEAST CONFERENCE JANUARY 23, 2015 QUALITY AND COMPLIANCE Katie Fink Donna Lewis Susan Walberg Presenters Katie Fink Senior Counsel Office of Counsel to the Inspector General U.S. Department
2015 HCCA SOUTHEAST CONFERENCE JANUARY 23, 2015 QUALITY AND COMPLIANCE Katie Fink Donna Lewis Susan Walberg Presenters Katie Fink Senior Counsel Office of Counsel to the Inspector General U.S. Department
Engaging Providers in Integrated Care Programs
 Engaging Providers in Integrated Care Programs November 6, 2014 4:00 PM Eastern The Integrated Care Resource Center, an initiative of the Centers for Medicare & Medicaid Services Medicare-Medicaid Coordination
Engaging Providers in Integrated Care Programs November 6, 2014 4:00 PM Eastern The Integrated Care Resource Center, an initiative of the Centers for Medicare & Medicaid Services Medicare-Medicaid Coordination
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS. Amy Hancock, CEO Presented to: CPERI April 16, 2018
 DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015
 Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
Community Paramedicine Seminar Milbank Memorial Fund, Nov
 Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Advocate Physician Partners approach to Population Health
 Advocate Physician Partners approach to Population Health Don Calcagno President, Advocate Physician Partners March 9, 2016 Who are Advocate Health Care and Advocate Physician Partners? 1 Advocate Health
Advocate Physician Partners approach to Population Health Don Calcagno President, Advocate Physician Partners March 9, 2016 Who are Advocate Health Care and Advocate Physician Partners? 1 Advocate Health
Institutional Handbook of Operating Procedures Policy
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Unifying Real-Time Mobile Rounds with Follow Up Care Calls to Improve Patient Experience and Outcomes
 Unifying Real-Time Mobile Rounds with Follow Up Care Calls to Improve Patient Experience and Outcomes Sue Murphy, RN BSN MS Chief Experience Officer Becker's 3rd Annual Health IT + Revenue Cycle 2017 1
Unifying Real-Time Mobile Rounds with Follow Up Care Calls to Improve Patient Experience and Outcomes Sue Murphy, RN BSN MS Chief Experience Officer Becker's 3rd Annual Health IT + Revenue Cycle 2017 1
Innovations in Community- Based Advanced Illness Care: A Population Health Approach
 Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
The Role & Challenges of Hospital Care Coordination in a POP HEALTH WORLD
 The Role & Challenges of Hospital Care Coordination in a POP HEALTH WORLD Presented by: Mary Jane Fellers, RN, BSN, MBA Senior Director, UM & Care Coordination OhioHealth Columbus, Ohio Replace text box
The Role & Challenges of Hospital Care Coordination in a POP HEALTH WORLD Presented by: Mary Jane Fellers, RN, BSN, MBA Senior Director, UM & Care Coordination OhioHealth Columbus, Ohio Replace text box
Improving Discharge Instructions with Technology
 Improving Discharge Instructions with Technology Sandra Thompson, CHPQ, CPHRM, CHEP, HACP, CSHA Administrator Quality/Risk/Compliance Laurens County Health Care System Laurens County Health Care System
Improving Discharge Instructions with Technology Sandra Thompson, CHPQ, CPHRM, CHEP, HACP, CSHA Administrator Quality/Risk/Compliance Laurens County Health Care System Laurens County Health Care System
04/08/2015. Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists. Pharmacist Objectives. Technician Objectives
 1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
5/26/2015. January 26, 2015 INCENTIVES AND PENALTIES. Medicare Readmission Penalties. CMS Bundled Payment Providers & ACOs in NE
 Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Avoiding Errors During Transitions of Care: Medication Reconciliation
 in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
Preventing Avoidable Readmissions Together: Improving Discharge Summaries. R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC
 Preventing Avoidable Readmissions Together: Improving Discharge Summaries R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC Today s Objectives Identify elements of a complete discharge summary
Preventing Avoidable Readmissions Together: Improving Discharge Summaries R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC Today s Objectives Identify elements of a complete discharge summary
Hospice Policies & Procedures PATIENT CARE
 Hospice Policies & Procedures PATIENT CARE Copyright 2017 by Weatherbee Resources, Inc. All rights reserved. Purchasers of Hospice Policies and Procedures: Patient Care are permitted to use and reproduce
Hospice Policies & Procedures PATIENT CARE Copyright 2017 by Weatherbee Resources, Inc. All rights reserved. Purchasers of Hospice Policies and Procedures: Patient Care are permitted to use and reproduce
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM
 The Harvard Pilgrim Independence Plan SM") Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
Getting Started in a Medicare Shared Savings Program Accountable Care Organization
 1 Getting Started in a Medicare Shared Savings Program Accountable Care Organization Tuesday, September 16 th Pam Maxwell, Chief Growth Officer What is an ACO? Accountable Care Organizations (ACOs) are
1 Getting Started in a Medicare Shared Savings Program Accountable Care Organization Tuesday, September 16 th Pam Maxwell, Chief Growth Officer What is an ACO? Accountable Care Organizations (ACOs) are
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
Outcomes Measurement in Long-Term Care (LTC)
") ASHA Short Course Outcomes Measurement in Long-Term Care (LTC) Bill Goulding, MS/CCC-SLP November 19, 2012 How Do We Show Value? Easy to measure! Not so easy! V $$$ A L Impact? Cost U Benefit E What do
ASHA Short Course Outcomes Measurement in Long-Term Care (LTC) Bill Goulding, MS/CCC-SLP November 19, 2012 How Do We Show Value? Easy to measure! Not so easy! V $$$ A L Impact? Cost U Benefit E What do
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care
 Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care January 19, 2017 Kimberly S. Hodge, MSN, RN, ACNS-BC, CCRN-K Learning Objectives After attending this presentation,
Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care January 19, 2017 Kimberly S. Hodge, MSN, RN, ACNS-BC, CCRN-K Learning Objectives After attending this presentation,
Hospital Readmissions
 Article Title Hospital Readmissions Published By Pramit Sengupta, Georgia Institute of Technology Hospital Readmissions Overview of Hospital Readmission A readmission is defined as a hospitalization that
Article Title Hospital Readmissions Published By Pramit Sengupta, Georgia Institute of Technology Hospital Readmissions Overview of Hospital Readmission A readmission is defined as a hospitalization that
Partnering with Hospice: Reducing Skilled Nursing Facility to Hospital Readmissions
 Partnering with Hospice: Reducing Skilled Nursing Facility to Hospital Readmissions Scott Lavis, LICSW, CT Community Liaison Kline Galland Hospice Objectives for Today Quick review of regulations that
Partnering with Hospice: Reducing Skilled Nursing Facility to Hospital Readmissions Scott Lavis, LICSW, CT Community Liaison Kline Galland Hospice Objectives for Today Quick review of regulations that
Care Coordination in the New CoP s. Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017
 Care Coordination in the New CoP s Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting,
Care Coordination in the New CoP s Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting,
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Organization. Hospital to SNF Communication. Care Coordination Goals. Chasing the Perfect Handoff The Missing Link to Interoperability 7/18/2016
 Organization Chasing the Perfect Handoff The Missing Link to Interoperability Annette Brown, BSN, RN Director, Clinical Informatics Eisenhower Medical Center abrown@emc.org Not for profit, academic, community
Organization Chasing the Perfect Handoff The Missing Link to Interoperability Annette Brown, BSN, RN Director, Clinical Informatics Eisenhower Medical Center abrown@emc.org Not for profit, academic, community
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
A Battelle White Paper. How Do You Turn Hospital Quality Data into Insight?
 A Battelle White Paper How Do You Turn Hospital Quality Data into Insight? Data-driven quality improvement is one of the cornerstones of modern healthcare. Hospitals and healthcare providers now record,
A Battelle White Paper How Do You Turn Hospital Quality Data into Insight? Data-driven quality improvement is one of the cornerstones of modern healthcare. Hospitals and healthcare providers now record,