Organization. Hospital to SNF Communication. Care Coordination Goals. Chasing the Perfect Handoff The Missing Link to Interoperability 7/18/2016
|
|
|
- Conrad Powell
- 5 years ago
- Views:
Transcription
1 Organization Chasing the Perfect Handoff The Missing Link to Interoperability Annette Brown, BSN, RN Director, Clinical Informatics Eisenhower Medical Center Not for profit, academic, community hospital 463 licensed beds with 71 clinics 3,500 employees; 496 affiliated physicians 2015 Awards & Recognition Most Wired Hospital since 2012 Magnet Recognition & NICHE Recognition LeapfrogHospital Safety Score A Ranked in Top 50 US Cardiovascular Hospitals (Truven Health Analytics) LGBT Healthcare Equality Leader since 2013 (Healthcare Equality Index) Care Coordination Goals The National Quality Strategy aims to promote effective communication and coordination of care across the healthcare system by focusing on three goals: Improve the quality of care transitions and communications across care settings. Improve the quality of life for patients with chronic illness and disability by following a current care plan that anticipates and addresses pain and symptom management, psychosocial needs, and functional status. Establish shared accountability and integration of communities and healthcare systems to improve quality of care and reduce health disparities. Hospital to SNF Communication Major communication problem Easily identified More difficult to solve Eisenhower Medical Center (EMC) Family Medicine Residency Program highlighted multiple physician concerns regarding the quality, adequacy, and timeliness of EMC SNF hand off information. Critical information insufficiently presented Not always timely Both major contributing factors to substandard hand offs Need for in depth gap analysis of hospital to post acute care transitions identified by patient safety review. National Quality Forum,

 and Meaningful Use Stage 2 Requirements mandated electronic interoperability and Summary of Care (SoCR)")

2 MU Stage 2 Summary of Care Report Too Lengthy Inefficient Interpretation Literacy Levels Incomplete Plan of Care & Progress to Goals Negative Impact to Clinical Workflow Clinicians Perceived Minimal Benefit to Care Technology Challenges Clinical Challenges Strategic Challenges Summary of Care Report EMC SNF Gap Analysis History Eisenhower Medical Center (EMC) and surrounding SNFs functioned as separate entities 2012 Center for Medicare and Medicaid Services (CMS) and Meaningful Use Stage 2 Requirements mandated electronic interoperability and Summary of Care (SoCR) report February 2014 EMC formed a SNF Collaborative Committee Aim: to align care providers in the EMC network Goal: to deliver more integrated patient care to the community EMC educated SNF staff to the SoCR Process Key elements of the report Establish SNF Internet Protocols Addresses (IPAs) 2


3 How Did We Get There Conduct Root Cause Analysis Identify SNF inbound critical information requirements Determine needed hospital outbound documents Evaluate clarity of hospital outbound documents Direct observations of the Hospital discharge and SNF admission process Develop modified e Develop standardization and accountability Identify physician champion & desired data elements Accomplishments IPAs e SNF Discharge Document Checklist Reconciliation of Medication Documents Training and Education Timeliness of Discharge Summary Enhanced SNF Discharge iform Risk Stratification ABILITY ILLUMINATE referral process lights up the care transition process to make faster, easier, more informed connections among patients, acute and post acute providers. Similar to Extended Care Information Network (ECIN) Ability Network.com, 2016 Situation 3

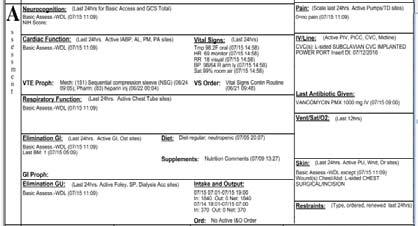
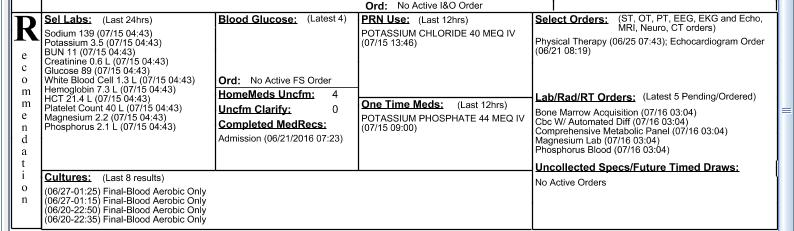
4 Background Assessment 2 2 Recommendations T R A N S F E R C H E C K L I S T 4







5 DISCHARGE I FORM DISCHARGE I FORM New EMC SNF Transfer Communication Process/Outcomes Created an environment for increased dialogue and positive cooperation between the organizations and among care team members Count of Responses Results SNF Survey Identified Continued Improvement Areas, January More effective communication & more efficient tools resulted in: Care providers more confident that information they share assures safe and secure transition of care for every patient Medication Clarity Discharge Summary Timeliness Contact Person at EMC Standard Paperwork Nurse to Nurse Communication Continued Collaborative Fully Electronic Handoff Family Education Risk Stratification 5


6 Hospital Unit Dashboard Ability Networks, 2016 Lessons Learned 1 Don t be afraid of change Identify a physician champion Relationship based care / patient engagement Transition of care pharmacist & Behavioral Health support Engage leadership Develop relationships Schedule routine meetings Monitor & measure the process Lessons Learned 2 Develop a SNF dashboard SNF designated case manager or color code SNF admissions Consider assigning a case manager with responsibility for SNF patients or color code SNF admissions To improve the transfers Create a transfer process to include policy and procedure for transfer accountabilities Determine the information to be sent for referral vs. discharge Put in place the tools, forms, and education for safe transfers Monitor and measure your process Communicate, communicate, and communicate! 6
 INTERACT a quality improvement program that focuses on the management of acute change in resident condition.")
7 Summary To close the loop for the Hospital and SNF relationship, SNFs will outbound patients to the hospital with a similar practice developed here with INTERACT (Interventions to Reduce Acute Care Transfers) INTERACT a quality improvement program that focuses on the management of acute change in resident condition. It includes clinical and educational tools and strategies for use in every day practice in long term care facilities. INTERACT Nursing Home to Hospital Transfer Form Interact, 2014 Potential Areas for Improvement Improve communications during transitions between providers, patients and caregivers Implement SNF electronic medical records that include standardized medication reconciliation and elements, assess interoperability of Ability & Interact tools Establish points of accountability for sending and receiving care, particularly for hospitalists and SNFists Increase the use of case management and professional care coordination Expand the role of the pharmacist in transitions of care Implement payment systems that align incentives and include performance measures to encourage better transitions of care Six Communication Best Practices for Transitional Care Management Lay The Groundwork Prior To Discharge Provide Constant Contact Capture Patient Preferences Be Persistent Automate the Outreach Implement Smart Reminder Messaging West Healthcare

. Improve the Transition of Care Process for Acute Providers. http://abilitynetwork.com/services/referral management transition ofcare/acute. Retrieved 1/25/16.")
8 Four High Impact Areas Linkages and Synchronization Individuals Progression Toward Goals Comprehensive Assessment Shared Accountability Acknowledgements EMC expresses it s appreciation to individuals and organizations that share their insights with us. Brookdale Eisenhower Family Medicine Residency The Fountains at the Carlotta Indio Nursing and Rehab HCR Manor Care Monterey Palms Premier Health Care Rancho Mirage Health Care References Ability Network. (n.d.). Improve the Transition of Care Process for Acute Providers. management transition ofcare/acute. Retrieved 1/25/16. That s Enough Thanks for listening! Ability Network. (n.d.) Ability/Illuminate Hospital View of Pending SNF Discharges. Retrieved 1/25/16. Interact2.net. (n.d.). Interventions to Reduce Acute Care Transfers. Retrieved 1/25/16. Interact2.net. (n.d.). Nursing Home to Hospital Transfer Form. Retrieved 1/25/16. National Quality Forum. (2012). Effective Communication and Care Coordination. Retrieved 1/25/16. West Healthcare. (2016). Six Communication Best Practices for Transitional Care Management. 8
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
URAC Patient Centered Medical Home
 URAC Patient Centered Medical Home Presented by: Cynthia Cook, RN, BSN Sr. Director Business Development Data Only 27% of U.S. adults can easily contact their primary care physicians by telephone, obtain
URAC Patient Centered Medical Home Presented by: Cynthia Cook, RN, BSN Sr. Director Business Development Data Only 27% of U.S. adults can easily contact their primary care physicians by telephone, obtain
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Leverage Information and Technology, Now and in the Future
 June 25, 2018 Ms. Seema Verma Administrator Centers for Medicare & Medicaid Services US Department of Health and Human Services Baltimore, MD 21244-1850 Donald Rucker, MD National Coordinator for Health
June 25, 2018 Ms. Seema Verma Administrator Centers for Medicare & Medicaid Services US Department of Health and Human Services Baltimore, MD 21244-1850 Donald Rucker, MD National Coordinator for Health
Fast-Track PCMH Recognition
 Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
NextGen Population Health TEN TEN TEN TEN TE. Prevent Patients from Falling Through the Cracks in 10 Easy Steps
 NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
Core Item: Hospital. Cover Page. Admissions and Readmissions. Executive Summary
 Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Exploring the challenges and possibilities of data. a guide to nursing and health care informatics
 Exploring the challenges and possibilities of data a guide to nursing and health care informatics why INFORMATICS? Health informatics drives changes in health care through the use of data. And these changes
Exploring the challenges and possibilities of data a guide to nursing and health care informatics why INFORMATICS? Health informatics drives changes in health care through the use of data. And these changes
Using Updox to Succeed with MIPS
 Using Updox to Succeed with MIPS Who is Updox? A Communications Platform built by physicians, for physicians 56,000+ providers and more than 300,000 users--and growing 100+ EMR integrations 72 million
Using Updox to Succeed with MIPS Who is Updox? A Communications Platform built by physicians, for physicians 56,000+ providers and more than 300,000 users--and growing 100+ EMR integrations 72 million
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
CMS Quality Payment Program: Performance and Reporting Requirements
 CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Promoting Interoperability (PI) Formerly Meaningful Use
 Formerly Meaningful Use") Promoting Interoperability (PI) Formerly Meaningful Use 1 What is Promoting Interoperability Formerly known as Meaningful Use In 2011 CMS established the Medicare and Medicaid EHR Incentive program to
Promoting Interoperability (PI) Formerly Meaningful Use 1 What is Promoting Interoperability Formerly known as Meaningful Use In 2011 CMS established the Medicare and Medicaid EHR Incentive program to
Table of Contents for CCC Toolkit
 Section 0.2 Overview Table of Contents for CCC Toolkit This document lists and briefly describes all the tools in the CCC Toolkit in alphabetic order. Time needed: As needed Suggested other tools: How
Section 0.2 Overview Table of Contents for CCC Toolkit This document lists and briefly describes all the tools in the CCC Toolkit in alphabetic order. Time needed: As needed Suggested other tools: How
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care
 Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care Peggi M. Czinger MPH Director, Network Care Management COE The Care Management Company of Montefiore The Bronx:
Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care Peggi M. Czinger MPH Director, Network Care Management COE The Care Management Company of Montefiore The Bronx:
Meaningful Use Update: Stage 3 and Beyond. Carla McCorkle, Midas+ Solutions CQM Product Lead
 Meaningful Use Update: Stage 3 and Beyond Carla McCorkle, Midas+ Solutions CQM Product Lead Objectives Discuss major changes to Meaningful Use program for Stage 3 and impact on hospitals Identify steps
Meaningful Use Update: Stage 3 and Beyond Carla McCorkle, Midas+ Solutions CQM Product Lead Objectives Discuss major changes to Meaningful Use program for Stage 3 and impact on hospitals Identify steps
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Abstract. Are eligible providers participating? AdvancedMD EHR features streamline meaningful use processes: Complete & accurate information
 Abstract As part of the American Recovery and Reinvestment Act of 2009, the Federal Government laid the groundwork for the nationwide implementation of electronic health records (EHR) systems as a measure
Abstract As part of the American Recovery and Reinvestment Act of 2009, the Federal Government laid the groundwork for the nationwide implementation of electronic health records (EHR) systems as a measure
Meaningful Use Stage 2
 Meaningful Use Stage 2 Objectives Gain understanding of the changes Focus on Transitions in Care and Patient Engagement Recognize the increasing HIE role Who Are You? What is YOUR Need Today? A. Office
Meaningful Use Stage 2 Objectives Gain understanding of the changes Focus on Transitions in Care and Patient Engagement Recognize the increasing HIE role Who Are You? What is YOUR Need Today? A. Office
PointRight: Your Partner in QAPI
 A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
QUALITY MEASURES WHAT S ON THE HORIZON
 QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
January 2017 A GUIDE TO HOME HEALTH VALUE-BASED PURCHASING
 January 2017 A GUIDE TO HOME HEALTH VALUE-BASED PURCHASING Copyright 2017 HEALTHCAREfirst. All rights reserved. 01/13/2017 2 A Guide to Home Health Value-Based Purchasing BACKGROUND In recent years, the
January 2017 A GUIDE TO HOME HEALTH VALUE-BASED PURCHASING Copyright 2017 HEALTHCAREfirst. All rights reserved. 01/13/2017 2 A Guide to Home Health Value-Based Purchasing BACKGROUND In recent years, the
Chronic Care Management Coding Guidelines Effective January 1, 2017
 Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Michigan s Statewide Health Information Network
 Michigan s Statewide Health Information Network November 9, 2017 Marty Woodruff Associate Director Marty.Woodruff@mihin.org Today s Agenda Introduction to MiHIN Data-Sharing Use Cases Shared Services Working
Michigan s Statewide Health Information Network November 9, 2017 Marty Woodruff Associate Director Marty.Woodruff@mihin.org Today s Agenda Introduction to MiHIN Data-Sharing Use Cases Shared Services Working
CMS Proposed Payment Rule FY Cheryl Phillips, MD Evvie Munley
 CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
Accountable Care Organizations. What the Nurse Executive Needs to Know. Rebecca F. Cady, Esq., RNC, BSN, JD, CPHRM
 JONA S Healthcare Law, Ethics, and Regulation / Volume 13, Number 2 / Copyright B 2011 Wolters Kluwer Health Lippincott Williams & Wilkins Accountable Care Organizations What the Nurse Executive Needs
JONA S Healthcare Law, Ethics, and Regulation / Volume 13, Number 2 / Copyright B 2011 Wolters Kluwer Health Lippincott Williams & Wilkins Accountable Care Organizations What the Nurse Executive Needs
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 2. Expedition Coordinator
 Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Value-Based Models: Two Successful Payer-Provider Approaches March 1, 2016
 Value-Based Models: Two Successful Payer-Provider Approaches March 1, 2016 Clifford T. Fullerton, MD, MSc President, Baylor Scott & White Quality Alliance Chief Population Health Officer, Baylor Scott
Value-Based Models: Two Successful Payer-Provider Approaches March 1, 2016 Clifford T. Fullerton, MD, MSc President, Baylor Scott & White Quality Alliance Chief Population Health Officer, Baylor Scott
Lessons Learned from the Dual Eligibles Demonstrations. Real-Life Takeaways from California and Other States
 Lessons Learned from the Dual Eligibles Demonstrations 1 May 28, 2015 Real-Life Takeaways from California and Other States Introductions Toby Douglas Consultant, MAXIMUS Former Director of California Department
Lessons Learned from the Dual Eligibles Demonstrations 1 May 28, 2015 Real-Life Takeaways from California and Other States Introductions Toby Douglas Consultant, MAXIMUS Former Director of California Department
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow
 One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
Re: CMS Code 3310-P. May 29, 2015
 May 29, 2015 Centers for Medicare & Medicaid Services Department of Health and Human Services P.O. Box 8013 Baltimore, MD 21244-8013 Attention: CMS-3310-P Re: The Centers for Medicare Medicaid Services
May 29, 2015 Centers for Medicare & Medicaid Services Department of Health and Human Services P.O. Box 8013 Baltimore, MD 21244-8013 Attention: CMS-3310-P Re: The Centers for Medicare Medicaid Services
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
CMS Modifications to Meaningful Use in Final Rule. Slide materials and recording will be available after the webinar
 CMS Modifications to Meaningful Use in 2015-2017 Final Rule Denise Satterfield Practice Solutions Advisor December 2015 Welcome Slide materials and recording will be available after the webinar Submit
CMS Modifications to Meaningful Use in 2015-2017 Final Rule Denise Satterfield Practice Solutions Advisor December 2015 Welcome Slide materials and recording will be available after the webinar Submit
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Preparing for the 2018 EHR Medicaid Incentive Payment Program
 Preparing for the 2018 EHR Medicaid Incentive Payment Program 1 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois Health Information
Preparing for the 2018 EHR Medicaid Incentive Payment Program 1 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois Health Information
Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees
 TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
Summer Institute of Nursing Informatics (SINI) 2012
 2012") Moving Nursing from the Sidelines to the Playing Field: Patient-Centered Interdisciplinary Care Planning and Outcomes Measurements Summer Institute of Nursing Informatics (SINI) 2012 Stephanie Lambrecht,
Moving Nursing from the Sidelines to the Playing Field: Patient-Centered Interdisciplinary Care Planning and Outcomes Measurements Summer Institute of Nursing Informatics (SINI) 2012 Stephanie Lambrecht,
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care
 Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care January 19, 2017 Kimberly S. Hodge, MSN, RN, ACNS-BC, CCRN-K Learning Objectives After attending this presentation,
Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care January 19, 2017 Kimberly S. Hodge, MSN, RN, ACNS-BC, CCRN-K Learning Objectives After attending this presentation,
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor
 Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
SECTION 9 Referrals and Authorizations
 SECTION 9 Referrals and Authorizations General Information The PAMF Utilization Management (UM) Program is carried out by the Managed Care department. The UM Program is designed to ensure that all Members
SECTION 9 Referrals and Authorizations General Information The PAMF Utilization Management (UM) Program is carried out by the Managed Care department. The UM Program is designed to ensure that all Members
Technology Fundamentals for Realizing ACO Success
 Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
HCAHPS: Background and Significance Evidenced Based Recommendations
 HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12
 New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
U.S. Healthcare Problem
 U.S. Healthcare Problem U.S. Federal Spending GDP (%) Source: Congressional Budget Office This graph shows that government has to spend a lot of more money in healthcare in the future and it is growing
U.S. Healthcare Problem U.S. Federal Spending GDP (%) Source: Congressional Budget Office This graph shows that government has to spend a lot of more money in healthcare in the future and it is growing
2017 Edition. MIPS Guide. The rule is in and Medicare physician payments are changing. What does that mean for you?
 2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
Primary goal of Administration Patients Over Paperwork
 Meaningful Measures Presented by: Maria Durham, Director, Kevin Larsen, MD, Director Continuous Improvement and Strategic Planning, Centers for Medicare & Medicaid Services Discussion Topics Introduction
Meaningful Measures Presented by: Maria Durham, Director, Kevin Larsen, MD, Director Continuous Improvement and Strategic Planning, Centers for Medicare & Medicaid Services Discussion Topics Introduction
The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management
 The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management By Jim Hansen, Vice President, Health Policy, Lumeris November 19, 2013 EXECUTIVE SUMMARY When EMR data
The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management By Jim Hansen, Vice President, Health Policy, Lumeris November 19, 2013 EXECUTIVE SUMMARY When EMR data
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION
 UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
Tool: Discharge Planning Process (c)(1)
(1)") Purpose & Intent 483.21(c)(1): To develop a discharge plan to help as many residents who want to return back to the community, to be effectively discharged from the nursing center back to the community.
Purpose & Intent 483.21(c)(1): To develop a discharge plan to help as many residents who want to return back to the community, to be effectively discharged from the nursing center back to the community.
Tribal Health. Integrated Tribal Health Center Solutions Five Steps to Better Tribal Health Outcomes
 Tribal Health Integrated Tribal Health Center Solutions Five Steps to Better Tribal Health Outcomes Join the Tribal Health leader Tap into the single, shared database of our EHR and practice management
Tribal Health Integrated Tribal Health Center Solutions Five Steps to Better Tribal Health Outcomes Join the Tribal Health leader Tap into the single, shared database of our EHR and practice management
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Park Nicollet Health Services Community Health Needs Assessment 2016 Implementation Update
 Park Nicollet Health Services Community Health Needs Assessment 2016 Implementation Update Priority #1: Mental and Behavioral Health Objective Action Steps Responsible Leader(s) Improve education about
Park Nicollet Health Services Community Health Needs Assessment 2016 Implementation Update Priority #1: Mental and Behavioral Health Objective Action Steps Responsible Leader(s) Improve education about
Special Needs Program Training. Quality Management Department
 10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Clinically Focused. Outcomes Oriented. Technology Driven. Chronic Care Management. eqguide. (CPT Codes 99490, 99487, 99489)
") Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
WHITE PAPER. Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice
 WHITE PAPER Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice Maximizing Pay-for-Performance Opportunities In today s
WHITE PAPER Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice Maximizing Pay-for-Performance Opportunities In today s
PATH Program. Getting Started Guide
 PATH Program Getting Started Guide We have a BIG opportunity. Together, we can empower and encourage people to take an active role in their health. Preventive health care services help people find and
PATH Program Getting Started Guide We have a BIG opportunity. Together, we can empower and encourage people to take an active role in their health. Preventive health care services help people find and
Improvement Activities: What You Have To Do
 Learning Forum Fridays Countdown to MIPS Data Submission Webinar Series Improvement Activities: What You Have To Do Merit-based Incentive Payment System = MIPS Liem Tran Health Informatics Specialist Health
Learning Forum Fridays Countdown to MIPS Data Submission Webinar Series Improvement Activities: What You Have To Do Merit-based Incentive Payment System = MIPS Liem Tran Health Informatics Specialist Health
Centers for Medicare and Medicaid CMS Updates. Christol Green, Anthem Inc.
 Centers for Medicare and Medicaid CMS 2016-2017 Updates Christol Green, Anthem Inc. Agenda Topic Page Payment Models - BPCI 3 Sequestration 5 CPC+ Initiative 7 What is MACRA? 12 CMS Social Security Number
Centers for Medicare and Medicaid CMS 2016-2017 Updates Christol Green, Anthem Inc. Agenda Topic Page Payment Models - BPCI 3 Sequestration 5 CPC+ Initiative 7 What is MACRA? 12 CMS Social Security Number
Model Of Care: Care Coordination Interdisciplinary Care Team (ICT)
") Cal MediConnect 2017 Model Of Care: Care Coordination Interdisciplinary Care Team (ICT) 2017 CMC Annual Training Learning Objectives Define the L.A. Care Cal MediConnect (CMC) Model of Care Describe the
Cal MediConnect 2017 Model Of Care: Care Coordination Interdisciplinary Care Team (ICT) 2017 CMC Annual Training Learning Objectives Define the L.A. Care Cal MediConnect (CMC) Model of Care Describe the
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Cutting Avoidable Readmissions Starts in the Emergency Department
 WHITE PAPER Cutting Avoidable Readmissions Starts in the Emergency Department SMARTER EMERGENCY CARE: EVERYWHERE, EVERY TIME. Our experience and innovative approach offers smarter solutions for emergency
WHITE PAPER Cutting Avoidable Readmissions Starts in the Emergency Department SMARTER EMERGENCY CARE: EVERYWHERE, EVERY TIME. Our experience and innovative approach offers smarter solutions for emergency
Measures Reporting for Eligible Providers
 Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Population Health. Collaborative Care. One interoperable platform. NextGen Care
 Population Health. Collaborative Care. One interoperable platform. NextGen Care We ve become very proactive in identifying at-risk patients and getting them in our door before they get sick. Our physicians
Population Health. Collaborative Care. One interoperable platform. NextGen Care We ve become very proactive in identifying at-risk patients and getting them in our door before they get sick. Our physicians
RESPITE CARE LEGACY HOSPICE
 RESPITE CARE LEGACY HOSPICE THE BASICS OF RESPITE CARE WHAT IS RESPITE? Short-term inpatient care provided only when necessary to relieve the family members or other persons caring for the individual at
RESPITE CARE LEGACY HOSPICE THE BASICS OF RESPITE CARE WHAT IS RESPITE? Short-term inpatient care provided only when necessary to relieve the family members or other persons caring for the individual at
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Creating Data-driven Strategies to Improve Hospital Outcomes
 Annual National Institute October 16, 2014 Creating Data-driven Strategies to Improve Hospital Outcomes A Case Manager s Guide Information Data Knowledge 1 2014 Conifer Health Solutions, LLC. All Rights
Annual National Institute October 16, 2014 Creating Data-driven Strategies to Improve Hospital Outcomes A Case Manager s Guide Information Data Knowledge 1 2014 Conifer Health Solutions, LLC. All Rights
At EmblemHealth, we believe in helping people stay healthy, get well and live better.
 At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
Iatric Systems Supports the Achievement of Meaningful Use
 Iatric Systems Supports the Achievement of Meaningful Use Iatric Systems offers a wide variety of solutions to assist with today s business challenges and support hospitals in providing superior patient
Iatric Systems Supports the Achievement of Meaningful Use Iatric Systems offers a wide variety of solutions to assist with today s business challenges and support hospitals in providing superior patient
Care Transitions Success Stories and Lessons Learned
 Care Transitions Success Stories and Lessons Learned April 30, 2015 Stratis Health, based in Bloomington, Minnesota, is a nonprofit organization that leads collaboration and innovation in health care quality
Care Transitions Success Stories and Lessons Learned April 30, 2015 Stratis Health, based in Bloomington, Minnesota, is a nonprofit organization that leads collaboration and innovation in health care quality
Meaningful Use Overview for Program Year 2017 Massachusetts Medicaid EHR Incentive Program
 Meaningful Use Overview for Program Year 2017 Massachusetts Medicaid EHR Incentive Program October 23 & 24, 2017 Presenters: Elisabeth Renczkowski, Al Wroblewski, and Thomas Bennett Agenda 2017 Meaningful
Meaningful Use Overview for Program Year 2017 Massachusetts Medicaid EHR Incentive Program October 23 & 24, 2017 Presenters: Elisabeth Renczkowski, Al Wroblewski, and Thomas Bennett Agenda 2017 Meaningful
INTERMACS has a Key Role in Reporting on Quality Metrics
 INTERMACS has a Key Role in Reporting on Quality Metrics Robert L Kormos MD FACS, FAHA FRCS(C) Director Artificial Heart Program University of Pittsburgh Medical Center The Patient Protection and Affordable
INTERMACS has a Key Role in Reporting on Quality Metrics Robert L Kormos MD FACS, FAHA FRCS(C) Director Artificial Heart Program University of Pittsburgh Medical Center The Patient Protection and Affordable