2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of
|
|
|
- Mark Greer
- 6 years ago
- Views:
Transcription


1 2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company names mentioned herein are the trademarks of their respective owners. No part of this copyrighted work may be reproduced, modified, or distributed in any form or manner without the prior written permission of Experian. Experian Public.


2 ACO Success through a 30-Day Transition of Care Process Jennifer Toms, Innovista Health Solutions
3 Agenda Introduction About Innovista Transition of Care (TOC) Overview TOC Program Goals & Benefits TOC Workflows Initial TOC Program Updated Program with CareCertainty Conclusion and Questions Patient/Physician/Hospital responses to new program Successes and Goals moving forward (5 mins) Conclusion/Q&A? (5 mins) 3
4 Innovista: Information & Company Goals Leading Population Health Management organization founded in October 2013 Locations in Illinois and Texas Enable physicians to manage all types of value based agreements that can enable independent physicians to stay independent Improve clinical quality, utilization/cost, value, physician satisfaction Lower the cost of care across the healthcare continuum by: Building and managing high-performing, quality, physician networks Combining information, technology and people to identify, communicate and manage physician behavior change and drive performance.ng support and tools necessary to manage population health a Delivering certified programs to exceed health plan requirements 4
5 Innovista: Background / Growth Employees 20 Networks 2 Members* 46,000/*All PCPs 200 Employees 60 Networks 6 Members* 187,000/*51,000 PCPs 700 Employees 115 Networks 18 Members* 300,000/*58,000 PCPs 1000 Employees TBD Networks 31+ Members* 400,000+/*??? PCPs ** *** Contracts/Plans 8 Contracts/Plans 15 Contracts/Plans: Fee for Service Pay for Performance Shared Savings Limited Risk Delegated * Medicare lives ** Innovista launched October Contracts/Plans 5
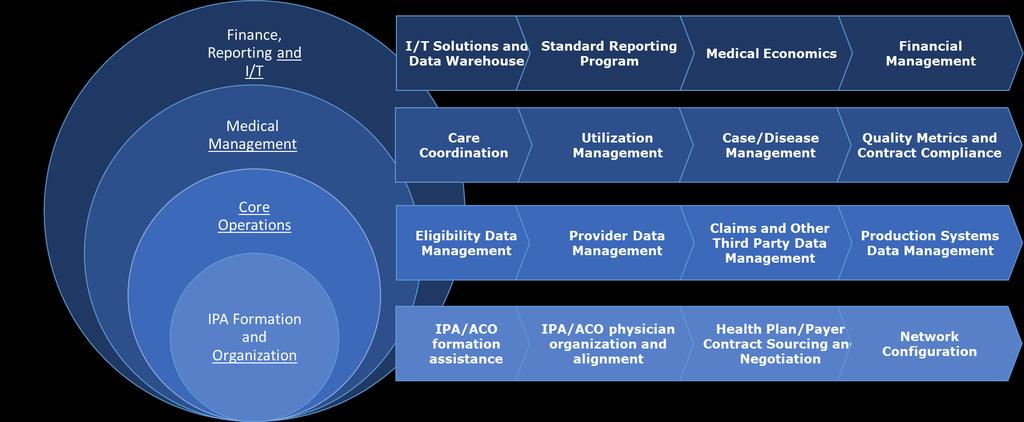

6 Innovista: Service Platforms 6

7 Care Coordination: The Transition of Care Program CMS started reimbursing providers on January 1, 2013 Provided to: Patient whose medical and/or psychosocial problems require moderate or high-complexity medical decision Patient making during transition from an inpatient hospital setting, partial hospital, observation status in a hospital, or skilled nursing facility/nursing facility, to the patient s community setting Estimated 80% of serious medical errors involve miscommunication during the hand-off between medical providers ~ 2.6 million seniors are readmitted within 30 days, at a cost of over $26 billion every year About 70% of all discharges qualify for Transition of Care Services 7

8 Transition of Care: Goals 8



9 Transition of Care: Cost Containment $2,640,000* $12,000,000* *Cost example specific to Innovista s IL Market 9
10 Transition of Care: Requirements 30-day period begins on the date the beneficiary is discharged from the inpatient hospital setting and continues for the next 29 days. During the 30 days beginning on the date the beneficiary is discharged from a hospital inpatient setting, you must furnish the following three components: Face-to-face visit Medical Complexity Determination Medication Reconciliation Completed within 7 or 14 days of discharge An interactive contact Two attempts made with 2 business days of discharge Telephone, , or face-to-face Additional non-face-to-face services 10


11 Transition of Care: Program Completion Must document the following information in the beneficiary s medical record: Date the beneficiary was discharged. Date you made an interactive contact with the beneficiary and/or caregiver. Date you furnished the face-to-face visit. The complexity of medical decision making (moderate or high) 11


12 Innovista s Transition of Care Workflow 12
13 Questionnaire: TOC Follow-Up: Completion: ED Notice: Adm. Notice: DC Notice: Transition of Care Program Notification sent to PCP alerting office of member ED encounter Notify PCP of Obsv/Inpatient Admissions based on ADT feed from facilities Notify PCP of discharge & engage with PCP office to ensure post-dc appointment has been scheduled. Message includes encouragement to schedule post-ed appointment with member Includes facility name & department, admission date, admitting diagnosis, admitting &m attending providers Includes facility name admit day & discharge day, LACE score, diagnosis, member contact info, and alert that 30- Day TOC Program has been initiated. TOC Questionnaire completed telephonically with member within TWO business days of discharge. Min. 2 attempts made. Completed Questionnaire immediately sent to PCP so it can be reviewed during the follow-up appointment Contact PCP Office to Verify that member kept appointment & that medical complexity was determined All additional requested calls & 30-Day TOC completion call made to member, as needed TOC Summary sent to PCP office detailing completed program components TOC Billing instructions included, if requested 13
14 Transition of Care Program: Initial Program Response Innovista Care Team: Tedious to record all program components in Excel Spreadsheet Time wasted entering information into notifications and records Nothing driving workflow or reminding team of deadlines Physicians: Patient cases missing or incomplete Low volume of cases managed Lack of customization for individual practices Hospital Staff Eager to participate Need to custom workflows based on facility 14
15 Transition of Care: CareCertainty Workflow Driven by System Auto-Generated Notifications Customizable by Facility, PCP, Internal Departments, Encounter/Task Type ED Encounter Notifications Observation/Inpatient Admission Notifications Observation/Inpatient Discharge Notifications Post-Discharge Member Services 15
16 Transition of Care: CareCertainty Notification Demo Demo of Test Patient %2fSuiteHome 16
17 Transition of Care: Responses to the Updated Program Innovista Care Team: Incomplete TOC Programs reduced from 45% to 0% Focus shifted from data entry to patient management Simplified team collaboration Early reports generated by CareCertainty system Physicians: Receive increased number of notification Information from wider variety of hospitals More patient detail provided to physicians prior to patient appointments Easy to customize notification type per practice Hospital Staff Positive response to notification system and demo Customized notifications based on facility has lead to increased hospital cooperation and eagerness to provide more/better patient information 17

18 Transition of Care: ACO Success First commercial ACO contract for an IPA saved over $250K with ~4K lives in 2015 Reduced loss for one client by 50% Went from $5M loss to $2.5M loss 18
19 Goals Moving Forward Train physicians and their staffs on the electronic messaging capabilities of CareCertainty Expand current program model to additional groups/contracts Work with Post Acute Care Facilities to implement admission, concurrent review, and discharge planning workflows Develop Chronic Disease Management and Clinical Escalation Programs Implement procedures for high risk readmission patients based on calculated LACE score 19
20 Conclusion Thank you! For more information on billing the PFS for TCM services, refer to Frequently Asked Questions about Billing the Medicare Physician Fee Schedule for Transitional Care Management Services. MLN/MLNProducts/Downloads/Transitional-Care-Management-Services-Fact-Sheet- ICN pdf 20


21
Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process. April 19, :00 PM
 and Chronic Care Management (CCM) Overview and Billing Process. April 19, :00 PM") Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process April 19, 2016 2:00 PM 2 Discussion Topics TCM Requirements TCM Services and C247 Process Medical Decision
Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process April 19, 2016 2:00 PM 2 Discussion Topics TCM Requirements TCM Services and C247 Process Medical Decision
Monday, October 24, :15 a.m. to 10:45 a.m. Great Halls 1 & 2
 Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Updates in Coding & Billing Strategies.
 Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
Clinically Focused. Outcomes Oriented. Technology Driven. Chronic Care Management. eqguide. (CPT Codes 99490, 99487, 99489)
") Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
improvement program to Electronic Health variety of reasons, experts suggest that up to
 Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018
 Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018 Revision Log See Important Reminder at the end of this policy for important regulatory
Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018 Revision Log See Important Reminder at the end of this policy for important regulatory
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: Problem Oriented Visits Billed with Preventative Visits
 Payment Policy: Problem Oriented Visits Billed with Preventative Visits Reference Number: CC.PP.052 Product Types: ALL Effective Date: 11/1/2017 Last Review Date: Coding Implications Revision Log See Important
Payment Policy: Problem Oriented Visits Billed with Preventative Visits Reference Number: CC.PP.052 Product Types: ALL Effective Date: 11/1/2017 Last Review Date: Coding Implications Revision Log See Important
Exploring the Possibilities with MIDAS+ SmartConnect
 June 1 3, 2009 Westin La Paloma Resort Tucson, Arizona Exploring the Possibilities with MIDAS+ SmartConnect Leverage your existing MIDAS+ Care Management tools and consider automating your transition planning
June 1 3, 2009 Westin La Paloma Resort Tucson, Arizona Exploring the Possibilities with MIDAS+ SmartConnect Leverage your existing MIDAS+ Care Management tools and consider automating your transition planning
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT
 1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
Standards of Practice & Scope of Services. for Health Care Delivery System Case Management and Transitions of Care (TOC) Professionals
 Professionals") A M E R I C A N C A S E M A N A G E M E N T A S S O C I A T I O N Standards of Practice & Scope of Services for Health Care Delivery System Case Management and Transitions of Care (TOC) Professionals O
A M E R I C A N C A S E M A N A G E M E N T A S S O C I A T I O N Standards of Practice & Scope of Services for Health Care Delivery System Case Management and Transitions of Care (TOC) Professionals O
Chronic Care Taking Disease Management Beyond Hospital Walls
 Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Multi-payer G and CPT Care Management Code Summary v7
 Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Accountable Care Collaborative: Transforming from Volume to Value
 Accountable Care Collaborative: Transforming from Volume to Value Risk Segmentation and Modeling American Medical Group Association Gary Piefer, MD, MS, FAAFP, FACPE Thursday June 14, 2010 WellMed Agenda
Accountable Care Collaborative: Transforming from Volume to Value Risk Segmentation and Modeling American Medical Group Association Gary Piefer, MD, MS, FAAFP, FACPE Thursday June 14, 2010 WellMed Agenda
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Chronic Care Management
 Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
PRIMARY PARTNERS, LLC. Our Journey with the State HIE
 PRIMARY PARTNERS, LLC Our Journey with the State HIE About Us As a 2012 starter, Primary Partners was one of the 1 st Medicare ACO s in the country Our 2 nd Medicare ACO was formed in 2013 In late 2014
PRIMARY PARTNERS, LLC Our Journey with the State HIE About Us As a 2012 starter, Primary Partners was one of the 1 st Medicare ACO s in the country Our 2 nd Medicare ACO was formed in 2013 In late 2014
A Regional Approach to HIE
 A Regional Approach to HIE Yvonne Hughes, CEO Small & Rural Hospital Conference November 12, 2014 Needs Assessment 2 Governance Structure Multi-Disciplinary Board Regional Hospitals (3 seats) Local Regional
A Regional Approach to HIE Yvonne Hughes, CEO Small & Rural Hospital Conference November 12, 2014 Needs Assessment 2 Governance Structure Multi-Disciplinary Board Regional Hospitals (3 seats) Local Regional
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT
 Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Chronic Care Management Services. Presented by Noridian Part B Medicare Provider Outreach and Education April 2015
 Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
CMS Quality Payment Program: Performance and Reporting Requirements
 CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
Provider-Based RHC Billing June 8, 2018
 Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Documentation for CCC Reimbursement
 Section 4.6 Implement Documentation for CCC Reimbursement This tool describes the importance of documentation and potential workflow changes to take advantage of any opportunity for reimbursement of services
Section 4.6 Implement Documentation for CCC Reimbursement This tool describes the importance of documentation and potential workflow changes to take advantage of any opportunity for reimbursement of services
Physician Estimate of Length of Services
 Physician Estimate of Length of Services Can the physician estimate of length of services be longer than 60 days? The physician estimate of length of service can be longer than 60 days. This estimate is
Physician Estimate of Length of Services Can the physician estimate of length of services be longer than 60 days? The physician estimate of length of service can be longer than 60 days. This estimate is
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM. November 20, 2015
 THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
Special Needs Plan (SNP) Model of Care Training 2018
 Model of Care Training 2018") Special Needs Plan (SNP) Model of Care Training 2018 Table of Contents Training Overview Pg. 1 Denver Health Medical Plan s (HMO SNP) MOC Annual Training Pg. 2 Special Needs Plans (SNPs) Pg. 2 Special
Special Needs Plan (SNP) Model of Care Training 2018 Table of Contents Training Overview Pg. 1 Denver Health Medical Plan s (HMO SNP) MOC Annual Training Pg. 2 Special Needs Plans (SNPs) Pg. 2 Special
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Unique Billing for PCMH Transition of Care/HCC Risk Management
 THE MEDICAL HOME SUMMIT MARCH 23, 2015 Unique Billing for PCMH Transition of Care/HCC Risk Management JAYNE BRYANT RN, BSN THERESA BAILEY, LVN JAMES L. HOLLY, MD MARCH 23, 2015 Criteria for New Codes 2
THE MEDICAL HOME SUMMIT MARCH 23, 2015 Unique Billing for PCMH Transition of Care/HCC Risk Management JAYNE BRYANT RN, BSN THERESA BAILEY, LVN JAMES L. HOLLY, MD MARCH 23, 2015 Criteria for New Codes 2
PAYMENT POLICY. Anesthesia
 IMPORTANT REMINDER This policy is current at the time of publication. Centene Corporation retains the right to change or amend this policy at any time. While this policy provides guidance regarding reimbursement,
IMPORTANT REMINDER This policy is current at the time of publication. Centene Corporation retains the right to change or amend this policy at any time. While this policy provides guidance regarding reimbursement,
Improving Patient Health Through Real-Time ADT Integration
 Improving Patient Health Through Real-Time ADT Integration Session 209, March 08, 2018 John Whitington, CIO, South Country Health Alliance Megan LaCanne, Sr Business Systems Analyst, South Country Health
Improving Patient Health Through Real-Time ADT Integration Session 209, March 08, 2018 John Whitington, CIO, South Country Health Alliance Megan LaCanne, Sr Business Systems Analyst, South Country Health
"Strategies for Enhancing Reimbursement " September 16, 2015
 "Strategies for Enhancing Reimbursement- 99080" September 16, 2015 Chat box feature Chat Box is available to you to ask questions or make comments anytime throughout today s webinar. Submit to Host and
"Strategies for Enhancing Reimbursement- 99080" September 16, 2015 Chat box feature Chat Box is available to you to ask questions or make comments anytime throughout today s webinar. Submit to Host and
Aetna Better Health of Illinois
 Aetna Better Health of Illinois Navigating Relationships in an Evolving Healthcare Environment: Community Health Centers and Managed Care Organizations Forum October 1, 2013 Sanjoy Musunuri Agenda Aetna
Aetna Better Health of Illinois Navigating Relationships in an Evolving Healthcare Environment: Community Health Centers and Managed Care Organizations Forum October 1, 2013 Sanjoy Musunuri Agenda Aetna
Third Party Payer Days. IMGMA February 25, 2015
 Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE (MOC) PROVIDER TRAINING
 MODEL OF CARE (MOC) PROVIDER TRAINING") SPECIAL NEEDS PLAN (SNP) MODEL OF CARE (MOC) PROVIDER TRAINING AlohaCare Advantage Plus (HMO SNP) Revised May 2018 HISTORY AlohaCare was formed by a network of Hawaii community health centers in 1994.
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE (MOC) PROVIDER TRAINING AlohaCare Advantage Plus (HMO SNP) Revised May 2018 HISTORY AlohaCare was formed by a network of Hawaii community health centers in 1994.
Hospice Policies & Procedures PATIENT CARE
 Hospice Policies & Procedures PATIENT CARE Copyright 2017 by Weatherbee Resources, Inc. All rights reserved. Purchasers of Hospice Policies and Procedures: Patient Care are permitted to use and reproduce
Hospice Policies & Procedures PATIENT CARE Copyright 2017 by Weatherbee Resources, Inc. All rights reserved. Purchasers of Hospice Policies and Procedures: Patient Care are permitted to use and reproduce
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL MEASURES REGISTRY ONLY
 Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
Transitional Care Management - Mistakes, CCM Interface, and the 2016 Fee Schedule Changes
 Transitional Care Management - Mistakes, CCM Interface, and the 2016 Fee Schedule Changes Stephen Canon, M.D. Program Director & Associate Professor UAMS Department of Urology Chief, Division of Pediatric
Transitional Care Management - Mistakes, CCM Interface, and the 2016 Fee Schedule Changes Stephen Canon, M.D. Program Director & Associate Professor UAMS Department of Urology Chief, Division of Pediatric
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
SUBMIT/RECEIVE STATEWIDE ADMISSION, DISCHARGE, TRANSFER (ADT) NOTIFICATIONS
 NOTIFICATIONS") Use Case Summary NAME OF UC: SUBMIT/RECEIVE STATEWIDE ADMISSION, DISCHARGE, TRANSFER (ADT) NOTIFICATIONS Sponsor(s): NJHIN / NJII NJDOH Date: 5/28/15 The purpose of this Use Case Summary is to allow Sponsors,
Use Case Summary NAME OF UC: SUBMIT/RECEIVE STATEWIDE ADMISSION, DISCHARGE, TRANSFER (ADT) NOTIFICATIONS Sponsor(s): NJHIN / NJII NJDOH Date: 5/28/15 The purpose of this Use Case Summary is to allow Sponsors,
Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL
 Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL Effective Date: 01/01/2015 Last Review Date: 04/28/2018 Coding Implications Revision Log See Important Reminder at the
Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL Effective Date: 01/01/2015 Last Review Date: 04/28/2018 Coding Implications Revision Log See Important Reminder at the
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Improving Transitions of Care
 Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
2) The percentage of discharges for which the patient received follow-up within 7 days after
 The percentage of discharges for which the patient received follow-up within 7 days after") Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Getting Started in a Medicare Shared Savings Program Accountable Care Organization
 1 Getting Started in a Medicare Shared Savings Program Accountable Care Organization Tuesday, September 16 th Pam Maxwell, Chief Growth Officer What is an ACO? Accountable Care Organizations (ACOs) are
1 Getting Started in a Medicare Shared Savings Program Accountable Care Organization Tuesday, September 16 th Pam Maxwell, Chief Growth Officer What is an ACO? Accountable Care Organizations (ACOs) are
Community Paramedicine Seminar Milbank Memorial Fund, Nov
 Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
Part 1: Central Fill Pharmacy - A Consolidated Services Center Part 2: A Review of CMS Initiatives That Involve Drug Therapy
 New Opportunities for Pharmacy Part 1: Central Fill Pharmacy - A Consolidated Services Center Part 2: A Review of CMS Initiatives That Involve Drug Therapy Presenters: Bonnie Kirschenbaum, MS, FASHP, FCSHP
New Opportunities for Pharmacy Part 1: Central Fill Pharmacy - A Consolidated Services Center Part 2: A Review of CMS Initiatives That Involve Drug Therapy Presenters: Bonnie Kirschenbaum, MS, FASHP, FCSHP
Medicare 2010 Hot Topics. About This Manual. Mary Jean Sage The Sage Associates 1/13/ Oak Park Blvd.
 Medicare 2010 Hot Topics Alameda Contra Costa Medical Association January 13, 2010 About This Manual Copyrighted 2010, The Sage Associates, Pismo Beach, California All rights reserved. All material contained
Medicare 2010 Hot Topics Alameda Contra Costa Medical Association January 13, 2010 About This Manual Copyrighted 2010, The Sage Associates, Pismo Beach, California All rights reserved. All material contained
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Transitional Care Management Services: New Codes, New Requirements
 Transitional Care Management Services: New Codes, New Requirements hospital 99496 99495 99496 family practice o n Jan. 1, 2013, the much anticipated transitional care management (TCM) Two new codes will
Transitional Care Management Services: New Codes, New Requirements hospital 99496 99495 99496 family practice o n Jan. 1, 2013, the much anticipated transitional care management (TCM) Two new codes will
Potential for an additional 5% PDCM-PCP BCBSM Value Based Reimbursement (VBR) onto your Patient Centered Medical Home designation VBR (estimated
 onto your Patient Centered Medical Home designation VBR (estimated") Revised 1/25/2018 1 Potential for an additional 5% PDCM-PCP BCBSM Value Based Reimbursement (VBR) onto your Patient Centered Medical Home designation VBR (estimated average of $4,000 per physician, varies
Revised 1/25/2018 1 Potential for an additional 5% PDCM-PCP BCBSM Value Based Reimbursement (VBR) onto your Patient Centered Medical Home designation VBR (estimated average of $4,000 per physician, varies
Alternative Payment Models for Behavioral Health Kim Cox VP, Provider Network
 Alternative Payment Models for Behavioral Health Kim Cox VP, Provider Network Kim Cox Vice President, Provider Network, Optum Kim Cox is Vice President of Provider Network. She joined Optum in February
Alternative Payment Models for Behavioral Health Kim Cox VP, Provider Network Kim Cox Vice President, Provider Network, Optum Kim Cox is Vice President of Provider Network. She joined Optum in February
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Planning a Course to Population Health Management
 Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Coding Guidance for HIV Clinical Practices: Care Management Services
 Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
Session Topic Question Answer 8-28 Action List
 8-28 Action List When do you accept, reject, or investigate an action? What if it is right in CROWNWeb but wrong on the other data base? Accept when you agree with the CMS value Reject when you do NOT
8-28 Action List When do you accept, reject, or investigate an action? What if it is right in CROWNWeb but wrong on the other data base? Accept when you agree with the CMS value Reject when you do NOT
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Review of the 2016 Annual Quality and Resource Use Reports. October 19, 2017
 Review of the 2016 Annual Quality and Resource Use Reports October 19, 2017 Acronyms in this presentation ACO: AF: AMA: CCN: CNS: CRNA: CPC: CPT: DOB: EIDM: EP: ESRD: FFS: GPRO: HCC: Accountable Care Organization
Review of the 2016 Annual Quality and Resource Use Reports October 19, 2017 Acronyms in this presentation ACO: AF: AMA: CCN: CNS: CRNA: CPC: CPT: DOB: EIDM: EP: ESRD: FFS: GPRO: HCC: Accountable Care Organization
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES
 2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES 2017 Physician Fee Schedule Impact on Medicare ACOs 1. Allowing ACO Participants to report PQRS separately from ACO 2. ACO Quality
2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES 2017 Physician Fee Schedule Impact on Medicare ACOs 1. Allowing ACO Participants to report PQRS separately from ACO 2. ACO Quality
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
reduce hospitalization
 Frail and Elderly Program Powered by CareSage Intelligence to reduce hospitalization Frail and Elderly Program powered by CareSage Multiple chronic conditions are becoming common among seniors, contributing
Frail and Elderly Program Powered by CareSage Intelligence to reduce hospitalization Frail and Elderly Program powered by CareSage Multiple chronic conditions are becoming common among seniors, contributing
Readmission Partnership Between Acute Care and Post-Acute Care
 Readmission Partnership Between Acute Care and Post-Acute Care Melissa Suzuki, MSW Regional UR Case Manager Specialist Commonwealth Care of Roanoke (CCR) Amanda Melvin, MSW Referral Development Coordinator
Readmission Partnership Between Acute Care and Post-Acute Care Melissa Suzuki, MSW Regional UR Case Manager Specialist Commonwealth Care of Roanoke (CCR) Amanda Melvin, MSW Referral Development Coordinator
The Business Case for Chronic Care Management in the Ambulatory Care Practice
 The Business Case for Chronic Care Management in the Ambulatory Care Practice Debbie Rozanski, CMC Practice Transformation Coach Michigan Rural Health Association Soaring Eagle Casino & Resort May 4-5,
The Business Case for Chronic Care Management in the Ambulatory Care Practice Debbie Rozanski, CMC Practice Transformation Coach Michigan Rural Health Association Soaring Eagle Casino & Resort May 4-5,
Reducing Readmissions Through Timely Post-Discharge Follow-Up:
 Reducing Readmissions Through Timely Post-Discharge Follow-Up: Best Practices from the Field March 18, 2015 Guest Presenters: JENNIFER DURST, Quality Assurance and Improvement Manager, Marin Community
Reducing Readmissions Through Timely Post-Discharge Follow-Up: Best Practices from the Field March 18, 2015 Guest Presenters: JENNIFER DURST, Quality Assurance and Improvement Manager, Marin Community
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
LTC User Guide for Nursing Facility Forms 3618/3619 and Minimum Data Set/ Long Term Care Medicaid Information (MDS/LTCMI)
") LTC User Guide for Nursing Facility Forms 3618/3619 and Minimum Data Set/ Long Term Care Medicaid Information (MDS/LTCMI) v 2018 0614 Contents Learning Objectives...1 Sequencing of Documents...2 Admission
LTC User Guide for Nursing Facility Forms 3618/3619 and Minimum Data Set/ Long Term Care Medicaid Information (MDS/LTCMI) v 2018 0614 Contents Learning Objectives...1 Sequencing of Documents...2 Admission
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
January 4, Dear Sir/Madam:
 January 4, 2016 U.S. Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-3317-P P.O. Box 8016 Baltimore, MD 21244-8016 Dear Sir/Madam: The Home Care Association
January 4, 2016 U.S. Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-3317-P P.O. Box 8016 Baltimore, MD 21244-8016 Dear Sir/Madam: The Home Care Association
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
COLLABORATING FOR VALUE. A Winning Strategy for Health Plans and Providers in a Shared Risk Environment
 COLLABORATING FOR VALUE A Winning Strategy for Health Plans and Providers in a Shared Risk Environment Collaborating for Value Executive Summary The shared-risk payment models central to health reform
COLLABORATING FOR VALUE A Winning Strategy for Health Plans and Providers in a Shared Risk Environment Collaborating for Value Executive Summary The shared-risk payment models central to health reform
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Presentation Overview
 RETROSPECTIVE PREPAYMENT REVIEW & BILLING ERRORS Presentation Overview eqhealth s Role as QIO What is Retrospective Review? Selection and notification process HFS Retrospective Review Requirements Scope
RETROSPECTIVE PREPAYMENT REVIEW & BILLING ERRORS Presentation Overview eqhealth s Role as QIO What is Retrospective Review? Selection and notification process HFS Retrospective Review Requirements Scope
Community Paramedicine Seminar July, 20th 2015
 Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
The Center for Medicare & Medicaid Innovations: Programs & Initiatives
 The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
Best Practices: Access Case Management
 Best Practices: Access Case Management Sarah M. Clark, RN-BC, BSN, MHA/INF, CCM Manager, Care Coordination Education Sentara Healthcare August 15, 2013 1 Objectives Identify key components of an effective
Best Practices: Access Case Management Sarah M. Clark, RN-BC, BSN, MHA/INF, CCM Manager, Care Coordination Education Sentara Healthcare August 15, 2013 1 Objectives Identify key components of an effective
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
23 rd Annual Health Sciences Tax Conference
 23 rd Annual Health Sciences Tax Conference December 9, 2013 Disclaimer This content is for educational and discussion purposes only, and is not intended, and should not be relied upon, as accounting advice.
23 rd Annual Health Sciences Tax Conference December 9, 2013 Disclaimer This content is for educational and discussion purposes only, and is not intended, and should not be relied upon, as accounting advice.
Accountable Care in Infusion Nursing. Hudson Health Plan. Mission Statement. for all people. INS National Academy of Infusion Therapy
 Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
Coordinated Care: Key to Successful Outcomes
 Coordinated Care: Key to Successful Outcomes Best practices in care coordination improve health, lower costs and increase patient satisfaction 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.continuumhealth.net
Coordinated Care: Key to Successful Outcomes Best practices in care coordination improve health, lower costs and increase patient satisfaction 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.continuumhealth.net
SWAN Alerts and Best Practices for Improved Care Coordination
 SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
CHRONIC CARE MANAGEMENT. A Guide to Medicare s New Move Toward Patient-Centric Care
 CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
Readmission Policy REIMBURSEMENT POLICY UB-04. Reimbursement Policy Oversight Committee
 Readmission Policy Policy Number 2018F7001A Annual Approval Date 11/11/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are responsible for submission
Readmission Policy Policy Number 2018F7001A Annual Approval Date 11/11/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are responsible for submission
The Telemedicine Train is Leaving the Station: Don t be left behind
 The heart and science of medicine. UVMHealth.org The Telemedicine Train is Leaving the Station: Don t be left behind Prepared by Norman Ward MD, Chief Medical Officer, OneCare Vermont Natasha Wither, DO,
The heart and science of medicine. UVMHealth.org The Telemedicine Train is Leaving the Station: Don t be left behind Prepared by Norman Ward MD, Chief Medical Officer, OneCare Vermont Natasha Wither, DO,
Streamlining care processes with a data-driven approach
 Streamlining care processes with a data-driven approach With Innovaccer s efficient and end-to-end care management solution Case Study Leading Iowa-based Mercy ACO deployed InCare to enable every member
Streamlining care processes with a data-driven approach With Innovaccer s efficient and end-to-end care management solution Case Study Leading Iowa-based Mercy ACO deployed InCare to enable every member
04/08/2015. Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists. Pharmacist Objectives. Technician Objectives
 1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
Medicaid Super-Utilizers: 1% of Members = 25% of Costs. Opportunities for Improvement
 Medicaid Super-Utilizers: 1% of Members = 25% of Costs Opportunities for Improvement Presenter: James A. Cooley Texas Health and Human Services Commission (HHSC) Medicaid/CHIP Super-Utilizers Program September
Medicaid Super-Utilizers: 1% of Members = 25% of Costs Opportunities for Improvement Presenter: James A. Cooley Texas Health and Human Services Commission (HHSC) Medicaid/CHIP Super-Utilizers Program September