Reducing Hospital Readmissions and The Critical Role of Physician Leadership
|
|
|
- Maximillian Wilcox
- 6 years ago
- Views:
Transcription

1
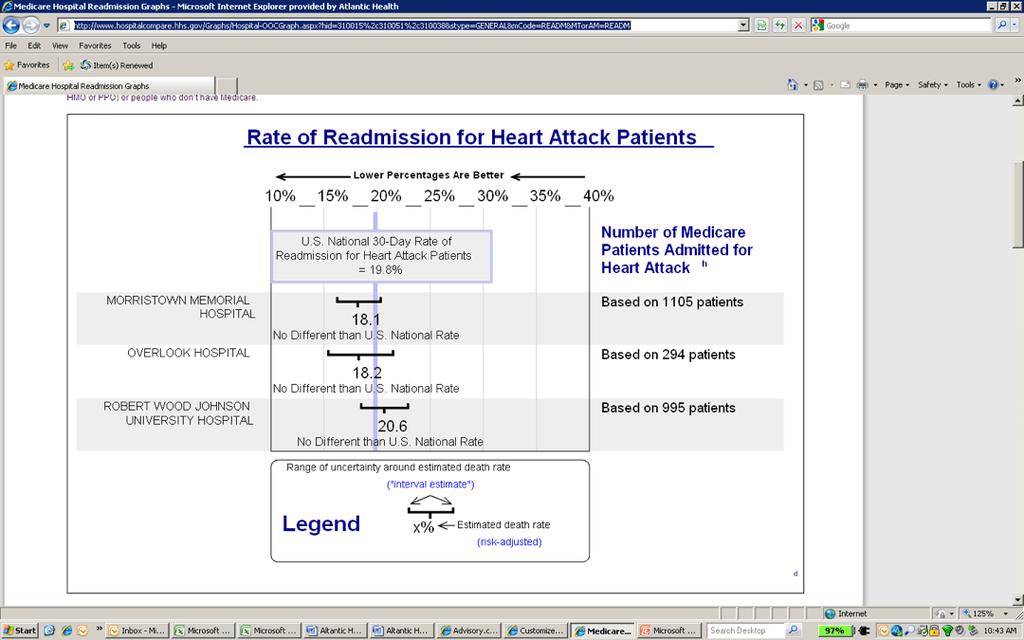
2 Reducing Hospital Readmissions and The Critical Role of Physician Leadership The Process of Designing our Readmission Reduction Plan, the Final Plan and the Critical Role of Physician Leadership Jeffrey E. Epstein, MD Medical Director, Continuum of Care Department Morristown Medical Center, Atlantic Health System Morristown, NJ


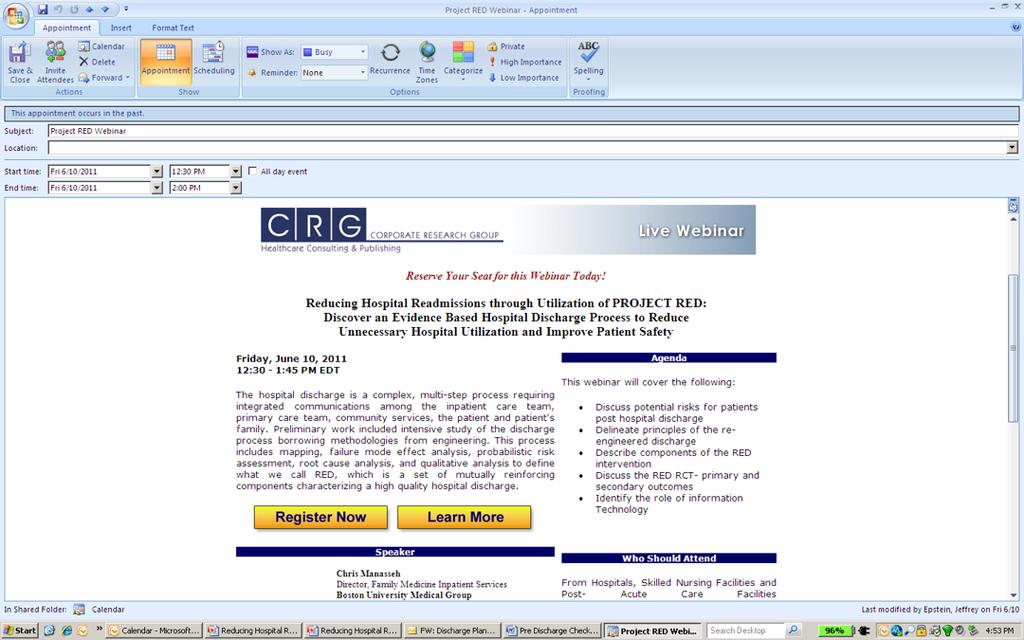
3 Presentation Outline Morristown Medical Center Where I come from What we are doing Our Discharge Checklist and our Discharge Planning Meetings What we have done How we have done it What are the problems that could lead to high Readmission rates The Audience Participation Part of our Presentation What is Wrong with Post Discharge Care Post Discharge Planning in the Perfect World The Critical Importance of strong Physician Leadership Will we seriously address the readmission problem anytime soon Medicare Incentives to Reduce Readmissions by October 2012 Our Commercial Insurance Contracts with Regards to Readmissions Should we work hard to reduce readmissions now? Project RED Project RED Plus




4 Morristown Medical Center
5 Morristown Medical Center Beds: 650 ED Visits per Year: 80,000 Admissions per Year: 38,000 Residency Programs: Medicine, Surgery, OB/GYN, Pediatrics, ER, Radiology Level One Trauma, Cardiac Surgery, Interventional Cardiology Cancer Center, Children s Hospital, Cardiac Center United Healthcare Consortium Affiliated with Mt. Sinai Medical School
6


7 The Answer to our Readmission Problem is not Magical It is really pretty Simple!
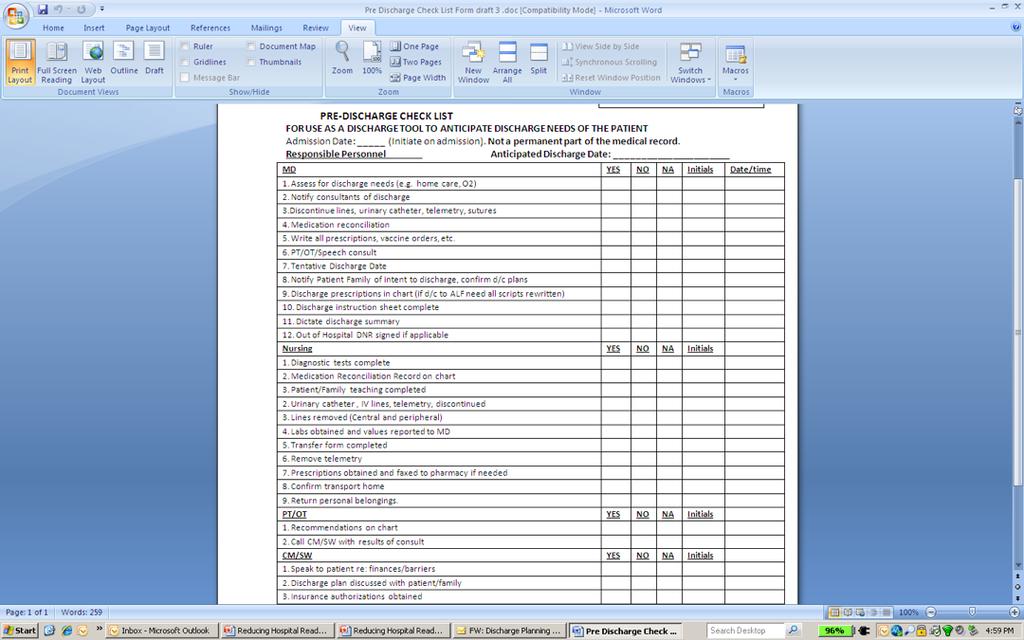
8 Discharge Process Planning Meetings & Initiative Chief Nursing Officer, Nurse Manager of Nursing Education, Director of the Continuum of Care Department, Medical Director of Continuum of Care Purpose: Reduce Delays in Discharge and Improve the Quality of our Discharges Safe and Effective Discharges: Coordination of Care The Reason this Process Improvement Initiative Was Put in Place: Delays in Discharge National Attention on Readmissions and Post Discharge Coordination of Care Specific Problems: Waiting until Discharge Order Written before beginning Discharge Process Suboptimal Patient and Family Education at the time of Discharge Discharge Process Lacked Quality Improvement Process Our Plan to Address the Issues and Problems Above: Pre-Discharge Checklist Project RED: Re-Engineering Discharge Post Discharge Care Oversight and Coordination Readmission Reduction
9 The Work Group and Schedule Weekly Meetings Leadership: Nurse Manager of Nursing Education Director of the Continuum of Care Department Medical Director of the Continuum of Care Department Work Group: MD/DO Hospitalist Chief of Family Practice Nurse Manager Information Technology/EMR Leadership Coordinator of Social Workers Coordinator of Case Managers Manager of Physical Therapy Manager of Quality
10 Initial Work Done by the Group 1. Pre-Discharge Checklist 1. Reminder Cues for Care Team 2. Communication Tool 2. Study and Learn about Project RED 3. Identify Key Players in Initiative 1. Nurses, Care Managers, Social Workers, PT/OT 2. Patients and their Families 3. Hospitalists 4. Receiving Physicians 5. Home Health Agencies 6. Post Discharge Facilities 4. Identify Possible Pilot Populations of Patients 1. CHF, Pneumonia, COPD, MI 2. Specific Commercial Plans 3. Medicare and Elderly 5. Develop Plan of Implementation
11
12
13 Initial Work Done by the Group 1. Pre-Discharge Checklist 1. Reminder Cues for Care Team 2. Communication Tool 2. Study and Learn about Project RED 3. Identify Key Players in Initiative 1. Nurses, Care Managers, Social Workers, PT/OT 2. Patients and their Families 3. Hospitalists 4. Receiving Physicians 5. Home Health Agencies 6. Post Discharge Facilities 4. Identify Possible Pilot Populations of Patients 1. CHF, Pneumonia, COPD, MI 2. Specific Commercial Plans 3. Medicare and Elderly 5. Develop Plan of Implementation
14
15
16
17 Initial Work Done by the Group 1. Pre-Discharge Checklist 1. Reminder Cues for Care Team 2. Communication Tool 2. Study and Learn about Project RED 3. Identify Key Players in Initiative 1. Nurses, Care Managers, Social Workers, PT/OT 2. Patients and their Families 3. Hospitalists 4. Receiving Physicians 5. Home Health Agencies 6. Post Discharge Facilities 4. Identify Possible Pilot Populations of Patients 1. CHF, Pneumonia, COPD, MI 2. Specific Commercial Plans 3. Medicare and Elderly 5. Develop Plan of Implementation
18
19 Initial Work Done by the Group 1. Pre-Discharge Checklist 1. Reminder Cues for Care Team 2. Communication Tool 2. Study and Learn about Project RED 3. Identify Key Players in Initiative 1. Nurses, Care Managers, Social Workers, PT/OT 2. Patients and their Families 3. Hospitalists 4. Receiving Physicians 5. Home Health Agencies 6. Post Discharge Facilities 4. Identify Possible Pilot Populations of Patients 1. CHF, Pneumonia, COPD, MI 2. Specific Commercial Plans 3. Medicare and Elderly 5. Develop Plan of Implementation

20 Possible Pilot Populations Acute MI, CHF, Pneumonia: The Initial Focus of CMS Horizon Patients with CHF: Horizon, our largest Insurer has a CHF Readmission Reduction Pilot Project Our Elderly Population is at high risk for Readmissions within 30 days Medicare Patients and the Elderly are high risk More Opportunity for Improvement No need to expend resources on 28 year old in for knee injury repair
21 Initial Work Done by the Group 1. Pre-Discharge Checklist 1. Reminder Cues for Care Team 2. Communication Tool 2. Study and Learn about Project RED 3. Identify Key Players in Initiative 1. Nurses, Care Managers, Social Workers, PT/OT 2. Patients and their Families 3. Hospitalists 4. Receiving Physicians 5. Home Health Agencies 6. Post Discharge Facilities 4. Identify Possible Pilot Populations of Patients 1. CHF, Pneumonia, COPD, MI 2. Specific Commercial Plans 3. Medicare and Elderly 5. Develop Plan of Implementation

22 Reducing Readmissions is Simple but NOT Easy! Come up with a plan that will work in your institution Get buy-in from all Essential Parties Measure Outcomes and Improve the Process Better patient care Higher Patient Satisfaction Extra Work for all Involved Improved Communication between Providers More Educated and Involved Patients Better Patient Outcomes

23 What are some problems that could lead to the readmission rate being so high?
24 What is Wrong with our Post Hospitalization Care 1. Patients do not see their primary care physician within days of their discharge 1. They are not told to see their doctor within days of discharge 2. Appointments are not made at the time of discharge 3. Primary Care Doctors are too busy to see these patients within days of discharge 2. Patients are sent to facilities where the quality of care is not optimal 1. The quality of Long Term Care Facilities or Rehabilitation Facilities has a great deal of variation 2. Patients cannot be evaluated adequately at these facilities 1. No exam rooms, equipment, labs or x-ray 3. Doctors are not always available on a daily basis to evaluate patients in the facility if they develop an acute problem 3. The hospital care team does not communicate well with the post hospital care team 1. No phone calls 2. Discharge Summaries are not dictated or available 3. Discharge Notes are short, incomplete and inadequate 4. The hospital care team does not communicate well and effectively with the patient and the patient s family 1. Patients and their care givers are not adequately educated 2. If they are educated, they are not predisposed to learn at the time of the acute admission 3. There is no follow up education and reinforcement after discharge 4. Inadequate resources are available to the patient and their family after discharge
25 The Post Discharge Plan in the Perfect World 1. Patients and Families are smart and educable 2. Education and information is provided during the hospital stay and after the hospital stay 3. Patients and families are highly motivated to get well and stay well 4. The hospital team communicates clearly and extensively with the post hospitalization team via phone calls and written material (dictated discharge summaries and detailed written discharge forms) 1. Doctor to Doctor 2. Nurse to Nurse 3. Physical Therapist to Physical Therapist 4. Wound Care Specialist to Wound Care Specialist 5. The care is Patient Centered so the patient and family are in control and their doctors are helping them by providing advice and guidance 1. The patient knows all their problems and the plan for each problem 2. The patient knows all their medications and which problem the medication is intended to help 3. Their doctors know all their problems and the plan for each problem 4. Their doctors know all their medications and the reason for each medication 5. All consultants as well as their Primary Care Doctor knows all of this 6. The patient is seen by the post discharge team within a day or two of discharge and is seen as frequently as needed to keep the patient tuned up and doing well
26 The Critical Role of Physician Leadership As you work with the Task force, certain key critical decisions have to be made and advocated for very strongly. You need a Physician Champion to get all doctors to buy-in to the program Dictate Quality Discharge Summaries with Critical Elements in a Problem-Oriented Fashion Dictate with 24 hours PCP s see their patients within 48 hours of Discharge Hospitalists call the PCP to discuss the Patient Post Discharge Facilities Improve the Quality of their Care and the Quality of the Patient Evaluations in their facilities Complete Paperwork prior to Discharge so patients can carry with them to their PCP You need a doctor who knows what doctors are really capable of so they can t say no when the answer can be and should be yes You need a doctor who can advocate as the Hospitalist, the PCP in the office and the Receiving Physician in the Post Discharge Facility
27 The Future Will This Happen?
28
29

30 When will there be a serious Effort to Reduce Readmissions? When the financial incentives are made perfectly clear to all parties!
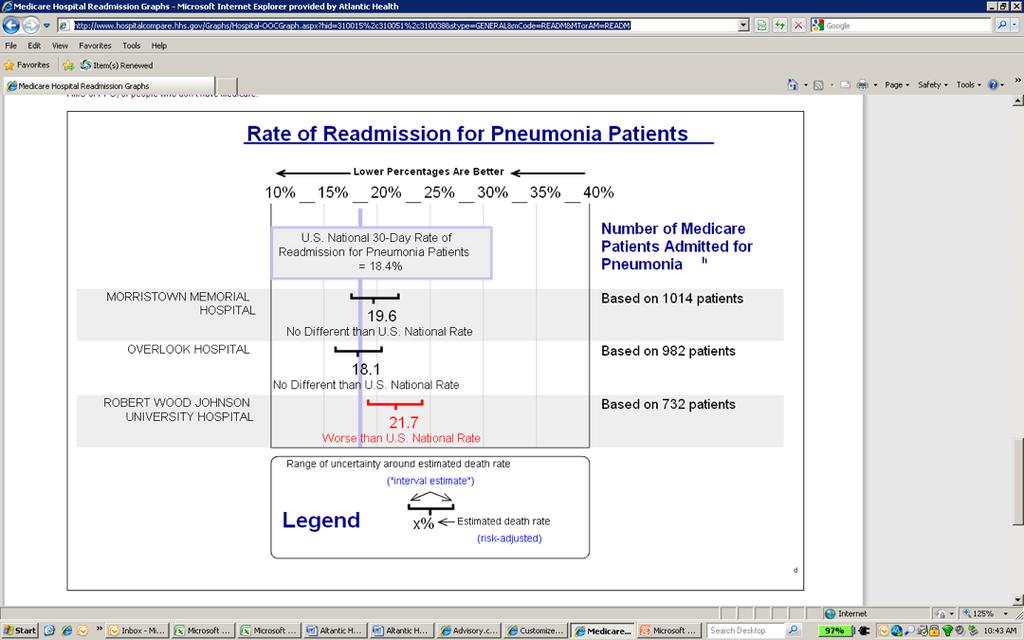
31 The Currently Planned Medicare Changes to take Effect October 1, 2012 Excessive Readmissions The health reform legislation introduces a Hospital Readmissions Reduction Program that will affect hospitals' Medicare inpatient payments. For fiscal years beginning on or after October 1, 2012, inpatient payments to hospitals will be reduced if a hospital experiences "excessive" readmissions, which will be defined by HHS, within a specified period following discharge for a heart attack, heart failure, or pneumonia. Certain planned readmissions will be exempted under this program. The health reform legislation authorizes HHS to designate additional conditions to the readmission list beginning in fiscal year Hospitals with excessive readmissions for these conditions will receive reduced payments for all inpatient discharges, not just discharges relating to readmissions deemed excessive. In addition, hospitals' performance with respect to these readmissions will be publicly reported by HHS, which will include publication on the Hospital Compare Web site. The amount of the payment reduction and other terms and conditions of this program will be established by HHS at a later date.

32 August 2011, Volume 8, No. 8. Case Management Monthly. "Is improper billing inflating your readmission rate?". In this article it states, "The Readmission Reduction Program will penalize hospitals with high readmission rates. Essentially CMS will assess the ratio of each hospital's readmission rate in comparison to the national average for three target conditions: acute MI, heart failure and pneumonia. If the ratio is greater than one, CMS will reduce the facilities aggregate Medicare payment."
33 Background As mandated under PPACA and detailed in the FY12 Inpatient Prospective Payment System (IPPS) Proposed Rule, short-term acute care hospitals with higher than expected 30-day risk-adjusted readmission rates for heart failure, acute myocardial infarction (heart attack) and pneumonia discharges between July 1, 2008 through June 30, 2011 will receive reduced Medicare payments starting in FY2013, capped at a maximum of 1% of inpatient payments. These penalties will increase in subsequent years to a maximum of 2% in FY2014 and 3% from FY2015 onwards. Additionally, the program will expand the list of targeted conditions beyond the initial three in FY2015. The first-year impact estimated in this report incorporates details from the PPACA, the FY12 IPPS Proposed Rule and CMS's QualityNet website, along with assumptions for certain provisions not addressed in the legislation. Please note that unlike CMS s other high profile quality initiative, the Hospital Inpatient Value Based Purchasing Program, which allows high performing hospital to earn a bonus payment, the Hospital Readmissions Reduction Program is a penalty-only plan designed to recover payments from hospitals that have received additional revenue associated with readmitted patients. As such, this program will have no financial impact for hospitals with risk-adjusted readmission rates below the national average on all applicable conditions. --- The Advisor Board Company Website, August 8, 2011
34
35
36
37 Why is this Being Looked At 4.4 Million Hospital Stays that are the Result of Potentially Preventable Re- Admissions $30 Billion per year 10% of all money spent to Hospital Care
38 Readmission Contract Language with Commercial Payers Here are the contracts with specific readmission language (DRG case rate contracts). Call me anytime today if you need further info/want to discuss. I m in all day. Aetna: Patients readmitted within 7 days shall be considered to included I the previous admission if the MS DRG assignment is identical and the reason for the readmission is due to improper discharge. (This is not defined) The intent is to insure the hospital only discharges patients at the appropriate time and not prematurely. Furthermore the following exceptions to the rule shall apply for patient readmitted within 7 days from the previous discharge (PTCI patients undergoing procedure for multiple stent insertion, CHF, chronic chemical dependency and alcoholism). Cigna: Cigna s Ms DRG Case Rate includes all care provided for a Participant s readmission with the same discharge diagnosis if the readmission occurs within 72 hours of the Participant s discharge, and Payor will not provide additional reimbursement to Hospital for such readmission. Horizon: Readmissions within 15 days for the same DRG and or any complications resulting from the initial admission will not be separately reimbursed whether or not he admission is considered medically necessary. The reimbursement for the first admission will be considered payment in full for both admissions. Oxford/United: United will not deny payment for re admissions. United and facility will establish a review process whereby at the discretion of United potentially all re admissions United believes were the result of a premature discharge. This review will be conducted by Facility s Medical Director or their designee with United s Medical Director or their designee. Those re-admissions where it is agreed by both Medical Directors the cause of the readmission was a result of a premature discharge will be subject to the recovery of the DRG payment for the second admission. In instances where the Medical Directors cannot agree on whether a re-admission was result of a pre mature discharge, the case will be referred to an external peer review organization for resolution.
39 Should we do it now? Revenue Cycle concerns: We get paid for readmissions Bad for Revenue Quality of Care Issues Better Quality Cost of Care Issues: Medicare and other Payers Tax Payers, Premiums, Employers Clearly better for Payers and Cost of Care What is best for the patient? Clearly better for Patients What is best for the hospital? Not Clear at this time in terms of revenue cycle What is best for the doctors? Financially, Job Satisfaction Conflicting Incentives
40 5 Questions to Determine Readmission Rate Effectiveness Joan Moss, RN, MSN, Senior Vice President, Sg2, for HealthLeaders Media, June 30, 2011 Question 1: What is our business exposure based on CMS penalties and future accountable care organization (ACO) quality reporting requirements? Question 2: How can we reduce readmissions without adversely affecting our current financial goals? Question 3: How can we better manage AMI, CHF and pneumonia patients? Question 4: What post-acute referral locations create our greatest readmission risks? Question 5: How can we more effectively manage readmissions
41
42 What to do when you are ready to get serious of Readmission Reduction
43 How do you reduce Readmissions? Prepare Patients and Families better for Discharge and Post Hospitalization Care More Effective Transfer of Information from Hospitalists to Receiving Doctors Improve your Post Hospitalization Care! Improve Care in Post Hospitalization Facilities Get Informed Patients to Informed Primary Care Doctors Sooner Will this eliminate the problem? No because some patients relapse within 30 days no matter how well they are cared for. Will this reduce the number of readmissions? Yes, absolutely because we generally do a poor job when it comes to Post Hospitalization Care!
44 RED: Why it was done, its drawbacks, the results and how it can be improved 1. Why it was done 1. 25% of patient required outpatient workup and 1/3 did not get that workup 2. 41% of patients had tests pending. 2/3 of time receiving doctor was not aware 3. Discharge Summary was not available to receiving doctor 1/3 of the time 4. 23% of patients had an adverse event after discharge. 2/3 could have been prevented or ameliorated 5. Only 40% of patients knew their discharge diagnoses or their medications at the time of discharge 6. An average of 8 minutes is spent preparing patients for discharge and patients only have an average of 2 questions 2. It s Drawbacks 1. Patient s average age was 49 years old 2. 50% of patients were Medicaid 3. The Results 1. Readmissions reduced from 21% to 15% 2. ED Visits reduced from 24% to 16% 3. Total Readmissions plus ED Visits reduced from 45% to 31% 4. Follow up visits increased from 44% to 62%
45 Project RED (Re-Engineering Discharge) Mutually Reinforcing Components 1. Educate patient during stay. Educate every day. 2. Make Follow up Appointment with Receiving Doctor within 2 weeks of Discharge 3. Make sure Tests and Studies have appropriate follow up (Discharge Advocate). Organized Post Discharge Plan with Tasks. 4. After Hospital Discharge Plan (AHDP) and Discharge Summary to Receiving Doctor at Follow up Visit 5. Make sure post discharge plan is consistent with Clinical Guidelines and Pathways 6. Medication Reconciliation 7. Make sure patients understand their diagnoses and plan of care (Teach Back Method) 1. Confirm Medication Plan and make sure Patients know why they are taking each Medication 2. Make sure patients know what to do if certain problems arise 3. Have a written Discharge Plan for the Patient (Diagnoses, Medications, Follow up plan, Pending tests and labs, Tests to be done hour phone call to patient
46 How can we do better than Project RED 1. Patients should be seen within 72 hours of discharge 2. Appointments should be made by hospital prior to discharge 3. All Discharge Summaries should be dictated within 24 hours of discharge 4. Every Problem on the Problem List should be addressed in the Discharge Summary 5. Discharge Summaries MUST be Dictated (not written) 6. Hospitalist calls the Receiving Doctor to have a real time conversation about the patient (sign out or hand off ) 7. Patients should get a copy of their Medical Record to Read and Take to their Receiving Physician 1. Admission H&P, ED Evaluation, Consultations, Discharge Summary, Radiology, Labs, Operative Reports, Anesthesia Reports, Procedure Reports
47 What Physicians and Hospital Systems have to do together Dictate within 24 Hours of Discharge Dictate a Quality Discharge Summary with is Problem Oriented Get this Dictation to the Receiving Provider within 24 Hours Make sure Patients are Seen Within 48 Hours of Discharge Make Sure Post Discharge Care is High Quality From Home From the Post Discharge Facility Make Sure Patients and Their Families are Informed and Educated Make Sure Patients Have a Copy of their Medical Record which is Organized
48 What some Hospital Systems and Insurance Companies are Doing 1. Horizon of New Jersey: Scale and BP cuff for CHF patients 2. Grove City Hospital: Home with Meds Program. 1. Discharged patients leave with a month s worth of discharge medications arranged by morning, noon and bedtime 2. A local pharmacist visits the hospital to counsel patients on medications 3. That pharmacist also makes house calls if concerns arise with homebound patients 3. Health First: Discharge Advocates make sure patients are seen within 7 days of Discharge 4. Independence Blue Cross in Philadelphia: Providing $5 million to a patientsafety initiative involving more than 70 hospitals and aiming to reduce readmissions by 10%.

49
50 Francisco's 'Money' Speech from "Atlas Shrugged" "So you think that money is the root of all evil?" said Francisco d'aconia. "Have you ever asked what is the root of money? Money is a tool of exchange, which can't exist unless there are goods produced and men able to produce them. Money is the material shape of the principle that men who wish to deal with one another must deal by trade and give value for value. Money is not the tool of the moochers, who claim your product by tears, or of the looters, who take it from you by force. Money is made possible only by the men who produce When you accept money in payment for your effort, you do so only on the conviction that you will exchange it for the product of the effort of others Those pieces of paper, which should have been gold, are a token of honor your claim upon the energy of the men who produce Try to obtain your food by means of nothing but physical motions and you'll learn that man's mind is the root of all the goods produced and of all the wealth that has ever existed on earth Wealth is the product of man's capacity to think Money is made before it can be looted or mooched made by the effort of every honest man, each to the extent of his ability. An honest man is one who knows that he can't consume more than he has produced To trade by means of money is the code of the men of good will. Money rests on the axiom that every man is the owner of his mind and his effort. Money allows no power to prescribe the value of your effort except by the voluntary choice of the man who is willing to trade you his effort in return. Money permits you to obtain for your goods and your labor that which they are worth to the men who buy them, but no more. Money permits no deals except those to mutual benefit by the unforced judgment of the traders. Money demands of you the recognition that men must work for their own benefit, not for their own injury, for their gain, not their loss the recognition that they are not beasts of burden, born to carry the weight of your misery that you must offer them values, not wounds that the common bond among men is not the exchange of suffering, but the exchange of goods. Money demands that you sell, not your weakness to men's stupidity, but your talent to their reason; it demands that you buy, not the shoddiest they offer, but the best your money can find. And when men live by trade with reason, not force, as their final arbiter it is the best product that wins, the best performance, then man of best judgment and highest ability and the degree of a man's productiveness is the degree of his reward. This is the code of existence whose tool and symbol is money Until and unless you discover that money is the root of all good, you ask for your own destruction. When money ceases to be the tool by which men deal with one another, then men become the tools of men Blood, whips and guns or dollars Take your choice there is no other

51 Money Quality of Care Do the right thing Be better at what you do Help others

52

53 In summing up, I wish I had some kind of affirmative message to leave you with, I don't. Would you take two negative messages? Woody Allen, The Comedy Years
54 Actually there is a Very Positive Message Reducing Readmissions and Providing Better Care is Simple but Not Easy! When Providers are Financially Rewarded for Taking Better Care of Patient, They Will Do It! Get Ready because It is Coming Even if it is Not in Your Financial Interest To Reduce Readmissions and Provide Better Post Hospitalization Care the Time Will Come and You Had Better Be Ready with A Robust and Effective Plan Why Do It NOW? Because if it the Right Thing To Do!
55
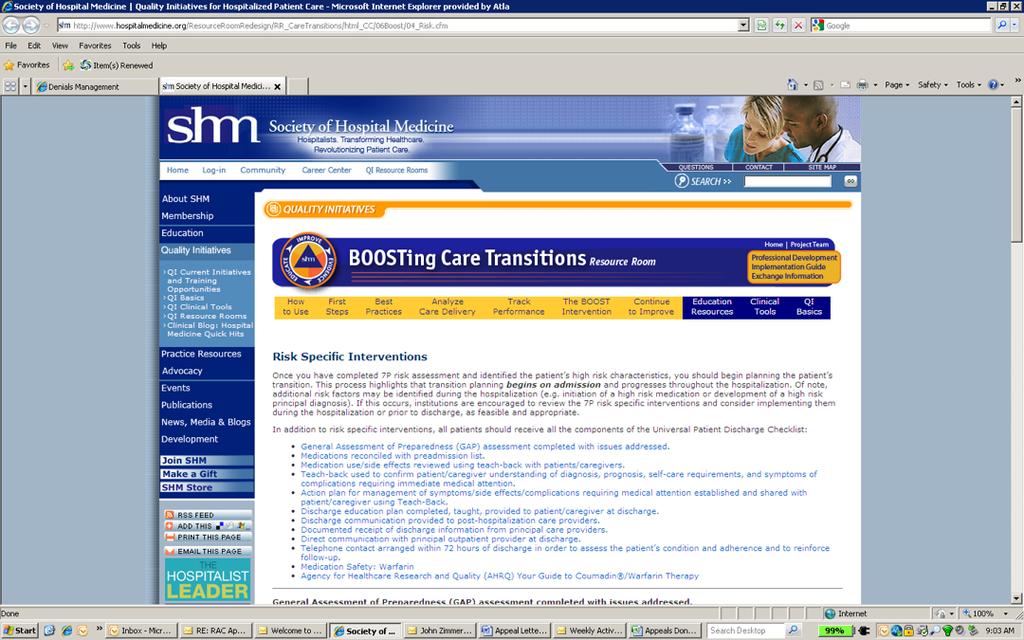
56 Additional Resources: Your Discharge Planning Checklist: For patients and their caregivers preparing to leave a hospital, nursing home, or other health care setting. CMS. CMS Product No Revised April Innovating on teach-back to prevent avoidable readmissions. Preventing Avoidable Hospital Admissions: Strategic Considerations for Nurse Executives. Nursing Executive Center. The Advisory Board Company
57 Meeting Two: Involve Chief of Family Practice Get information about their patients before seeing them in their office Have the opportunity to take care of their patients in the post discharge facilities Medication Reconsiliation Don t send their patient home on all new meds when they have meds they can use at home Meaningful Use Requirement for Electronic Discharge Summary Form being developed by the Internal Medicine Department Teaching Service Tools and Resources Already Available that people don t know about Paper Pads which encourage patients and families to write down their questions and concerns MyAtlanticHealth.org: My Medical Profile Wallet Card Pilot the Pre-Discharge Checklist on Unit F5W with involvement of Hospitalist Group and Nurse Manager and her Nursing Staff Looking to improve Patient Satisfaction Discussed making it a general practice to make follow up appointments for patients before they left hospital. This would ensure that they would be seen soon after discharge
58 Meeting Three: Boston Medical Center: Project RED After Hospital Care Plan Medications What is my main medical problem When are my appointments (date, time, place, doctor, address, phone) What exercises are good for me What should I eat What are my medication allergies Where is my pharmacy (address and phone number) Questions for the doctor Calendar with Appointments Patient Educational Information Should Core Quality Measures be part of our Pre Discharge Checklist? No as this will distract from the main purpose of this checklist Physicians should be dictating their Discharge Summaries at the time of Discharge The summary is better when the doctor remembers more The summary can be typed and sent to the Primary Care Doctor Problem Oriented Discharge Summary Essential Elements of a Quality Discharge Summaryd Avoid duplication of Effort Are other departments working on this project Are other hospitals in our System working on this project?
Readmission Reduction and the ACO
 Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
1. The new state-based insurance exchange for small businesses (SHOP) stands for:
 stands for:") Chapter 5 Review Questions 1. The new state-based insurance exchange for small businesses (SHOP) stands for: a. Small Business Health Options Program b. Small Business Health Option Plans c. State Health
Chapter 5 Review Questions 1. The new state-based insurance exchange for small businesses (SHOP) stands for: a. Small Business Health Options Program b. Small Business Health Option Plans c. State Health
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform. Summary
 Reform. Summary") Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Regulatory Advisor Volume Eight
 Regulatory Advisor Volume Eight 2018 Final Inpatient Prospective Payment System (IPPS) Rule Focused on Quality by Steve Kowske WEALTH ADVISORY OUTSOURCING AUDIT, TAX, AND CONSULTING 2017 CliftonLarsonAllen
Regulatory Advisor Volume Eight 2018 Final Inpatient Prospective Payment System (IPPS) Rule Focused on Quality by Steve Kowske WEALTH ADVISORY OUTSOURCING AUDIT, TAX, AND CONSULTING 2017 CliftonLarsonAllen
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs
 Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM
 The Harvard Pilgrim Independence Plan SM") Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
Integrated Health System
 Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Intro to Global Budgeting
 Intro to Global Budgeting Jim Hester House Health Care Committee & Senate Health & Welfare Committee 1/21/10 Agenda Goal of global budgeting Global budget models and examples Global payment model and examples
Intro to Global Budgeting Jim Hester House Health Care Committee & Senate Health & Welfare Committee 1/21/10 Agenda Goal of global budgeting Global budget models and examples Global payment model and examples
Summary of U.S. Senate Finance Committee Health Reform Bill
 Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
UPDATE ON MEANINGFUL USE. HITECH Stimulus Act of 2009: CSC Point of View
 HITECH Stimulus Act of 2009: CSC Point of View UPDATE ON MEANINGFUL USE Introduction The HITECH provisions of the American Recovery and Reinvestment Act of 2009 provide a commanding $36 billion dollars
HITECH Stimulus Act of 2009: CSC Point of View UPDATE ON MEANINGFUL USE Introduction The HITECH provisions of the American Recovery and Reinvestment Act of 2009 provide a commanding $36 billion dollars
A Care Transitions Project
 Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Health Reform and IRFs
 American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
Physician Compensation in an Era of New Reimbursement Models
 2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
Chronic Care Taking Disease Management Beyond Hospital Walls
 Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Re: Medicare Program; Medicare Shared Savings Program: Accountable Care Organizations, Proposed rule.
 June 3, 2011 Donald Berwick, MD Administrator Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1345-P, Mail Stop C4-26-05, 7500 Security Boulevard, Baltimore,
June 3, 2011 Donald Berwick, MD Administrator Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1345-P, Mail Stop C4-26-05, 7500 Security Boulevard, Baltimore,
Readmission Partnership Between Acute Care and Post-Acute Care
 Readmission Partnership Between Acute Care and Post-Acute Care Melissa Suzuki, MSW Regional UR Case Manager Specialist Commonwealth Care of Roanoke (CCR) Amanda Melvin, MSW Referral Development Coordinator
Readmission Partnership Between Acute Care and Post-Acute Care Melissa Suzuki, MSW Regional UR Case Manager Specialist Commonwealth Care of Roanoke (CCR) Amanda Melvin, MSW Referral Development Coordinator
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
AGENDA. QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, /21/2014
 QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, 2014 04 AGENDA Speaker Background Re Admissions Home Health Hospice Economic Incentivized Situations
QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, 2014 04 AGENDA Speaker Background Re Admissions Home Health Hospice Economic Incentivized Situations
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Re: Rewarding Provider Performance: Aligning Incentives in Medicare
 September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
Case managers are consummate team players, working with. IssueBrief
 IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
Community Paramedicine Seminar July, 20th 2015
 Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
ramping up for bundled payments fostering hospital-physician alignment
 REPRINT May 2016 Angie Curry James P. Fee healthcare financial management association hfma.org ramping up for bundled payments fostering hospital-physician alignment AT A GLANCE When hospitals embark on
REPRINT May 2016 Angie Curry James P. Fee healthcare financial management association hfma.org ramping up for bundled payments fostering hospital-physician alignment AT A GLANCE When hospitals embark on
Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
 Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Overview of Alaska s Hospitals and Nursing Homes. House HSS Committee March 1, 2012
 Overview of Alaska s Hospitals and Nursing Homes House HSS Committee March 1, 2012 Alaska Hospital and Nursing Homes Testifying Today Fairbanks Memorial Hospital Mike Powers Central Peninsula Hospital
Overview of Alaska s Hospitals and Nursing Homes House HSS Committee March 1, 2012 Alaska Hospital and Nursing Homes Testifying Today Fairbanks Memorial Hospital Mike Powers Central Peninsula Hospital
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Community Paramedicine Seminar Milbank Memorial Fund, Nov
 Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
The Role of Analytics in the Development of a Successful Readmissions Program
 The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM
 THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
2013 Health Care Regulatory Update. January 8, 2013
 2013 Health Care Regulatory Update January 8, 2013 Quality-Based Payment Reform, ACOs and Clinical Integration Bruce Johnson and Tom Donohoe Overview Quality-based payment reform programs Major programs
2013 Health Care Regulatory Update January 8, 2013 Quality-Based Payment Reform, ACOs and Clinical Integration Bruce Johnson and Tom Donohoe Overview Quality-based payment reform programs Major programs
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Paying for Outcomes not Performance
 Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
STRATEGIES TO REDUCE READMISSIONS
 STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
OMC Strategic Plan Final Draft. Dear Community, Working together to provide excellence in health care.
 Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Care Redesign: An Essential Feature of Bundled Payment
 Issue Brief No. 11 September 2013 Care Redesign: An Essential Feature of Bundled Payment Jett Stansbury Director, New Payment Strategies, Integrated Healthcare Association Gabrielle White, RN, CASC Executive
Issue Brief No. 11 September 2013 Care Redesign: An Essential Feature of Bundled Payment Jett Stansbury Director, New Payment Strategies, Integrated Healthcare Association Gabrielle White, RN, CASC Executive
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
Overview of Meaningful Use Medicare and Medicaid EHR Incentive Programs
 Contents Page # I. Background 1 FR 1846 Regulation Language Summary: This proposed rule would implement the provisions of the American Recovery and Reinvestment Act of 2009 (ARRA) (Pub. L. 111-5) that
Contents Page # I. Background 1 FR 1846 Regulation Language Summary: This proposed rule would implement the provisions of the American Recovery and Reinvestment Act of 2009 (ARRA) (Pub. L. 111-5) that
Value-Based Reimbursements are Here: Are you Ready?
 Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
Executing a Patient Experience Measurement Initiative
 Executing a Patient Experience Measurement Initiative Cathy Gorman Klug RN, MSN Director, Quality Service Line Nuance 2015 Nuance Communications, Inc. All rights reserved. Patient Experience Defined-The
Executing a Patient Experience Measurement Initiative Cathy Gorman Klug RN, MSN Director, Quality Service Line Nuance 2015 Nuance Communications, Inc. All rights reserved. Patient Experience Defined-The
Introduction to Value-Based Health Care Delivery
 Introduction to Value-Based Health Care Delivery Prof. Michael E. Porter Harvard Business School January 6, 2009 This presentation draws on Michael E. Porter and Elizabeth Olmsted Teisberg: Redefining
Introduction to Value-Based Health Care Delivery Prof. Michael E. Porter Harvard Business School January 6, 2009 This presentation draws on Michael E. Porter and Elizabeth Olmsted Teisberg: Redefining
Central Ohio Primary Care (COPC) Spotlight on Innovation
 Spotlight on Innovation") Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Chapter 02 Hospital Based Care
 Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
The Law and EHRs in Medical Education: The ARRA World. Overview
 The Law and EHRs in Medical Education: The ARRA World David Donnersberger MD, JD Clinical Assistant Professor of Medicine MS3 Site Director University of Chicago Pritzker School of Medicine Overview American
The Law and EHRs in Medical Education: The ARRA World David Donnersberger MD, JD Clinical Assistant Professor of Medicine MS3 Site Director University of Chicago Pritzker School of Medicine Overview American
04/08/2015. Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists. Pharmacist Objectives. Technician Objectives
 1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
Preventable Readmissions
 Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
snapshot Improving Experience of Care Scores Alone is NOT the Answer: Hospitals Need a Patient-Centric Foundation
 SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
Molina Healthcare Michigan Health Care Services Department Phone: (855) Fax: (800)
 Fax: (800)") Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
The Impact of Health Care Reform on Long- Term Care
 The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
Meaningful Use of EHR Technology:
 Meaningful Use of EHR Technology: What Do the New Standards and Certification Criteria Mean for Your Organization? January 20, 2010 Mitchell J. Olejko Ropes & Gray LLP mitchell.olejko@ropesgray.com 415-315-6328
Meaningful Use of EHR Technology: What Do the New Standards and Certification Criteria Mean for Your Organization? January 20, 2010 Mitchell J. Olejko Ropes & Gray LLP mitchell.olejko@ropesgray.com 415-315-6328
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A
 Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A Sec. 15001. Development of Medicare study for HCPCS versions of MS-DRG codes
Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A Sec. 15001. Development of Medicare study for HCPCS versions of MS-DRG codes
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods
 A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
Prepared for North Gunther Hospital Medicare ID August 06, 2012
 Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
ALTERNATIVE PAYMENT MODEL CONTRACTING GUIDE
 ALTERNATIVE PAYMENT MODEL CONTRACTING GUIDE June 2017 INTRODUCTION Alternative, collaborative health care delivery systems are the wave of the future. The Centers for Medicare and Medicaid Services (CMS),
ALTERNATIVE PAYMENT MODEL CONTRACTING GUIDE June 2017 INTRODUCTION Alternative, collaborative health care delivery systems are the wave of the future. The Centers for Medicare and Medicaid Services (CMS),
Increase Your Bottom Line by Eliminating Physician Driven Denials. Olakunle Olaniyan MD President Case Management Covenants
 Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Quality Circles. Nursing as a Revenue Center NDNQI
 IS YOUR ORGANIZATION ACCOUNTABLE? 2011 NDNQI Conference Miami, FL Victoria L. Rich, PhD, RN, FAAN Chief Nurse Executive, University of Pennsylvania Medical Center Associate Executive Director, Hospital
IS YOUR ORGANIZATION ACCOUNTABLE? 2011 NDNQI Conference Miami, FL Victoria L. Rich, PhD, RN, FAAN Chief Nurse Executive, University of Pennsylvania Medical Center Associate Executive Director, Hospital
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees
 TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
FY 2014 Inpatient Prospective Payment System Proposed Rule
 FY 2014 Inpatient Prospective Payment System Proposed Rule Summary of Provisions Potentially Impacting EPs On April 26, 2013, the Centers for Medicare and Medicaid Services (CMS) released its Fiscal Year
FY 2014 Inpatient Prospective Payment System Proposed Rule Summary of Provisions Potentially Impacting EPs On April 26, 2013, the Centers for Medicare and Medicaid Services (CMS) released its Fiscal Year
Patient Navigator Program
 Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model
 Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
How to Win Under Bundled Payments
 How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services