The Role & Challenges of Hospital Care Coordination in a POP HEALTH WORLD
|
|
|
- Alexia Stone
- 6 years ago
- Views:
Transcription


1 The Role & Challenges of Hospital Care Coordination in a POP HEALTH WORLD Presented by: Mary Jane Fellers, RN, BSN, MBA Senior Director, UM & Care Coordination OhioHealth Columbus, Ohio Replace text box with chapter logo (on all master slides)


2 Our mission To improve the health of those we serve. Replace text box with chapter logo





3 So who am I? RN RN Senior Director, UM & Care Coordination OhioHealth Replace text box with chapter logo

4 Care coordination means different Care coordination things to different people; no consensus definition has means fully evolved. different A recent systematic review identified over 40 definitions things to of different the term "care coordination." people; no "Care coordination is the deliberate consensus organization of patient care activities between two or more definition participants has fully (including the patient) involved in a patient's care evolved. to facilitate A recent the appropriate delivery of health care services. Organizing systematic care involves review the marshalling of personnel and other resources identified needed over to 40 carry out all required patient care activities and is definitions often managed of the by the exchange of information among participants term responsible "care for different aspects of care." coordination." Replace text box with chapter logo
5 Population health Plethora of definitions. From Wikipedia, the free encyclopedia Population health has been defined as "the health outcomes of a group of individuals, including the distribution of such outcomes within the group". [1] It is an approach to health that aims to improve the health of an entire human population. This concept does not refer to animal or plant populations. A priority considered important in achieving this aim is to reduce health inequities or disparities among different population groups due to, among other factors, the social determinants of health, SDOH. The SDOH include all the factors: social, environmental, cultural and physical the different populations are born into, grow up and function with throughout their lifetimes which potentially have a measurable impact on the health of human populations. [2] The Population Health concept represents a change in the focus from the individual-level, characteristic of most mainstream medicine. It also seeks to complement the classic efforts of public health agencies by addressing a broader range of factors shown to impact the health of different populations. The World Health Organization's Commission on Social Determinants of Health, reported in 2008, that the SDOH factors were responsible for the bulk of diseases and injuries and these were the major causes of health inequities in all countries. [3] In the US, SDOH were estimated to account for 70% of avoidable mortality. [4] From a population health perspective, health has been defined not simply as a state free from disease but as "the capacity of people to adapt to, respond to, or control life's challenges and changes". [5] The World Health Organization (WHO) defined health in its broader sense in 1946 as "a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity." [6][ 7] Replace text box with chapter logo
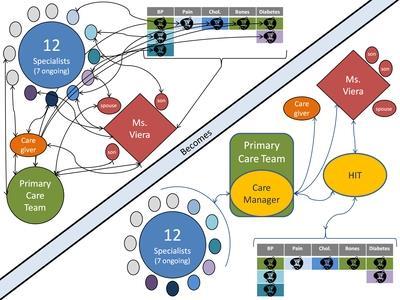
6 Moving on: Hospital Care Coordination 6


7 Medical Home now the key player! 7
8 The Care Coordination Puzzle As healthcare reform leads to a change from the fee-for-service payment model to value-based, quality-focused care, hospitals around the country must solve the care coordination puzzle. From admission to discharge and beyond, hospitals now take a more active role in improving patient engagement, patient navigation, physician engagement, medical monitoring technology and working with pharmacists and other specialists to align all the pieces to create more affordable, quality healthcare. One of the most important aspects of care coordination is a team-based approach between hospitals and post-acute care facilities to reduce readmissions and improve patient satisfaction,while emphasizing preventive healthcare, Janet Comrey, R.N., a senior consultant for population health at Geisinger Healthcare in Danville, Pennsylvania in interview with Fierce HealthCare. Replace text box with chapter logo
9 Hospital Care Coordination 9
10 5 PIECES OF THE CARE COORDINATION PUZZLE Physician Engagement Patient Engagement Pharmacy & Specialist Consults Remote Monitoring Technology Patient Navigators Replace text box with chapter logo

11 You can have all the systems in the world. but if you can t EXECUTE a strategy you re
12 Where /how do I know if the patient navigator has the patient on their list? How does a patient get on their list? How do I know if the pharmacist has been consulted? And if they have how do I know if they ve seen the patient..and what they have done? Remote monitoring who does that?... How do I know if its been done? Patient Engagement??? - Teachback?? How do I know if this has been done? And even more if patient was engaged? And do I have the resources to do this for everyone?? Replace text box with chapter logo

13 Replace text box with chapter logo

14 Replace text box with chapter logo
 Home Health Referral (coaching or visit) Follow up phone call.")
15 1234 Patient X 1235 patient Y 2134 Patient Z 1234 Patient A 1235 patient B 2134 Patient C Hospital Process Metrics Follow up phone call Teachback Pharmacy Consult (Mod/High Risk only) Home Health Referral (coaching or visit) Follow up phone call. Replace text box with chapter logo


16 Replace text box with chapter logo

17 Replace text box with chapter logo

18 Sometimes..its the little things that can throw a screw in the works Replace text box with chapter logo
19 EXAMPLE: Post Acute Referral important..but who do I make it to? Who s your primary physician Mr. Smith? Its Dr. Stan Bush Well I see at your last admission it was Dr. Dave Lubdub? Oh no, He s my cardiologist. So Dr. Stan Bush is your primary care physician and that s who you see on a regular basis? Oh no.. I usually see my pulmonologist for my COPD..that s Dr. Wheezer. Replace text box with chapter logo
20 So again who owns the patient? Starts with Hospital Visit WITH REFERRAL AT DISCHARGE TO Which of these players owns PATIENT the patient s CALL Care Coordination BACK after AFTER Discharge? DISCHARGE BUT ALSO POTENTIAL FOR.. AND VERY POSSIBLE THE PAYER IS CALLING PATIENT AS WELL Hospital Replace text box with chapter logo RN

21 POTENTIAL SOLUTION? ATTRIBUTION WORKFLOW Patient arrives at Hospital ADT or Creighton Report to PO * PO notifies Central UR: this one is ours Central UR tags member in MIDAS with Identified PO HOSPITAL CASE MGR FOLLOWS PO S GUIDELINE FOR COCURRENT &/or DISCHARGE PLAN & PLANS FOR A WARM HAND Hand off Receiver assumes responsibility for assuring: - post discharge followup call? - post discharge followup appt? - med rec? - other??, Medical Home Or PCP SNF or Patient Navigator *PO = patient owner the entity that has this member tagged in their system as an attributed member to follow either while in hospital or post discharge. Replace text box with chapter logo

22 Challenge #2: Lack of standardized handoff Industry Standards: Meaningful Use Stage II Care Coordination Interact Interim Electronic: Discharge instructions Discharge summary Others: Warm Handoff Replace text box with chapter logo
23 23


24 Prospective Payment System HOSPITAL REIMBURSEMENTRISK HERE NOW NOT WHEN STAGE 2 MEANINGFUL USE FINALLY ARRIVES? Replace text box with chapter logo


25 25 But no one interacts with the Interact
26 Electronic DI vs. Discharge Summary Discharge Instructions (the DI ) Pros: physician must sign prior to discharge Cons: limited info Diagnosis, Procedures, Appointment, Meds Discharge Summary Pros: contains the story course of hospital visit/what happened. Cons: Physicians may have up to 30 days to dictate/sign. 26

27 27
28 Challenge #3: No PING back. Multiple providers cite they will or are following the patient after discharge - scheduling appointments - providing transportation - making call backs, etc.. Hospital doesn t know & since we own the penalty, we don t let go. 28
29 Challenge #4: Complying with Compliance REIMBURSEMENT IS THERE FOR POP HEALTH WE JUST NEED TO COMPLY WITH PAYER REQUIREMENTS TO OBTAIN IT A few of the rules. 29



30 The 3 Day SNF Rule Currently, when Medicare beneficiaries are discharged to a skilled care facility for rehabilitation, Medicare s coverage only kicks in if beneficiaries have been coded as an in-patient at a hospital for at least three days, known as the three-day stay rule. But I don t want to be in Observation Status my doctor said I could be admitted and then go to a nursing home 30

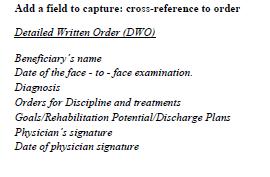
31 Home Health, PT/OT Face-to-Face Page 1 of 6
32 DME REQUIREMENTS F2F documentation will be required for the following frequently used items. (Actual list several pages long) 1.Wheelchairs 2.Hospital Beds and accessories 3.Portable Oxygen 4.Nebulizer 5.Cpap 6.Bipap 7.Ventilators What is documentation is needed prior to each delivery: Written Order Requirements: Order Prior to Delivery A F2F encounter must be documented as part of the medical record before the equipment is delivered to the patient. The encounter must have occurred no greater than 6 months prior to the order and delivery date. A written dispensing order is required prior to the delivery of equipment items that fall under the F2F requirement (see above items). The date of the written order must not be prior to the date of the F2F encounter. 1. The beneficiary's name 2. Detailed description of DME ordered 3. The prescribing practitioner's National Provider Identifier (NPI)- Must be noted above the Practitioner s signature. 4. The date of the order and the start date, if start date is different from the date of the order 5. The signature of the ordering Practitioner 6. Date order signed by Practitioner, must be located by signature 6. Ordering Practitioner's printed name (this is not in the regulation, but is always needed if the signature is not legible) The written dispensing order does not need to be signed by the same practitioner that completed the F2F encounter. The written dispensing order can be signed by a physician, CNP, CNS, PA, or Resident and does not need to be cosigned by physician. The FINE PRINT: Therapy notes can support the medical necessity, but can not be used in place of the F2F encounter. If the F2F encounter was completed by physician, CNP, CNS, PA, or Resident, a physician must document the occurrence of the F2F encounter by signing or cosigning the encounter that is documented in medical record. The requirement of the face-to-face is to document the need for the item that is being ordered. A practitioner can order equipment as long as there is a documented encounter within the last 6 months of the order date that supports the need. If there is no encounter within the last 6months prior to the written order, a new face-to-face encounter will be required for coverage. A face-to-face encounter for Oxygen can only be completed 30 days prior to the order. This is different than other F2F equipment, which is 6 months. A new face-to-face encounter is required when any of the participating equipment items need replaced.
33 Transition of Care Billing Codes 99495: Transitional Care Management Services with the following required elements Communication (direct contact, telephone, electronic) with the patient and/or caregiver within 2 business days of discharge Medical decision making of at least moderate* complexity during the service period Face-to-face visit, within 14 calendar days of discharge. Payment $135 to $163** : Transitional Care Management Services with the following required elements: Communication (direct contact, telephone, electronic) with the patient and/or caregiver within 2 business days of discharge. Medical decision making of at least high* complexity during the service period Face-to-face visit, within 7 calendar days of discharge. Payment $197 to $230**. Replace text box with chapter logo


34 Replace text box with chapter logo
35 35

36 Don t allow the environment to overwhelm.., Have a thorough understanding of your organizational culture From an IT perspective From an ACO Model From a who s who in your organization who are the leaders? The folks who can get things done? While advancing with strategic steps, there are hundreds of PROCESS steps that can be implemented, that will assure some work is getting done. But work as a team..have the right people at the table.. 36

37 Replace text box with chapter logo
The New Medicare DME Face-To- Face Rule: What Referral Sources Need to Know
 The New Medicare DME Face-To- Face Rule: What Referral Sources Need to Know What is the Face-to-Face Rule? Section 6407(b) of the 2009 Health Care Reform law (Affordable Care Act) mandates that there must
The New Medicare DME Face-To- Face Rule: What Referral Sources Need to Know What is the Face-to-Face Rule? Section 6407(b) of the 2009 Health Care Reform law (Affordable Care Act) mandates that there must
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Exploring the Possibilities with MIDAS+ SmartConnect
 June 1 3, 2009 Westin La Paloma Resort Tucson, Arizona Exploring the Possibilities with MIDAS+ SmartConnect Leverage your existing MIDAS+ Care Management tools and consider automating your transition planning
June 1 3, 2009 Westin La Paloma Resort Tucson, Arizona Exploring the Possibilities with MIDAS+ SmartConnect Leverage your existing MIDAS+ Care Management tools and consider automating your transition planning
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2013 [File Code CMS 1590 P]
![Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2013 [File Code CMS 1590 P]](/thumbs/79/80256172.jpg "Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2013 [File Code CMS 1590 P]") Centers for Medicare & Medicaid Services Attention: CMS 1590 P Mail Stop C4 26 05 7500 Security Boulevard Baltimore, MD 21244 1850 [Submitted online at: http://www.regulations.gov] Re: Medicare Program;
Centers for Medicare & Medicaid Services Attention: CMS 1590 P Mail Stop C4 26 05 7500 Security Boulevard Baltimore, MD 21244 1850 [Submitted online at: http://www.regulations.gov] Re: Medicare Program;
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Joint Statement on Ambulance Reform
 Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Joint Statement on Ambulance Reform Policymakers Should Examine Short- and Intermediate-Term Policies to Promote Innovation in the Delivery of Emergency and Non- Emergency Care Provided by Ambulance Services
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE)
") MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.0 October 10, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility, functionality,
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.0 October 10, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility, functionality,
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization. Quality Forum August 19, 2015
 The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model. The New Accountable Care Business Model
 Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
04/08/2015. Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists. Pharmacist Objectives. Technician Objectives
 1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Model Of Care: Care Coordination Interdisciplinary Care Team (ICT)
") Cal MediConnect 2017 Model Of Care: Care Coordination Interdisciplinary Care Team (ICT) 2017 CMC Annual Training Learning Objectives Define the L.A. Care Cal MediConnect (CMC) Model of Care Describe the
Cal MediConnect 2017 Model Of Care: Care Coordination Interdisciplinary Care Team (ICT) 2017 CMC Annual Training Learning Objectives Define the L.A. Care Cal MediConnect (CMC) Model of Care Describe the
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE)
") MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.2 November 13, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility,
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.2 November 13, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility,
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
HOME HEALTH CARE TABLE OF CONTENTS. OVERVIEW TRANSITIONAL... CARE... SERVICES . MEMBERS... MANAGED... BY... EVICORE
 TABLE OF CONTENTS. OVERVIEW............................................................................................. 452..... TRANSITIONAL................. CARE...... SERVICES......................................................................
TABLE OF CONTENTS. OVERVIEW............................................................................................. 452..... TRANSITIONAL................. CARE...... SERVICES......................................................................
Pharmacists Improve Care Through Team Collaboration
 Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab
 Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab (Required for all Rehab, SNF, LTAC admits) Providers must request authorization for initial admissions
Prior Authorization form for Post-Acute Care Admission and Recertification for SNF,LTAC and Rehab (Required for all Rehab, SNF, LTAC admits) Providers must request authorization for initial admissions
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
CMS Proposed Payment Rule FY Cheryl Phillips, MD Evvie Munley
 CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
Fundamentals of Medication Therapy Management (MTM) Services By Bruce R. Siecker, Ph.D., R.Ph.
 Services By Bruce R. Siecker, Ph.D., R.Ph.") Fundamentals of Medication Therapy Management (MTM) Services By Bruce R. Siecker, Ph.D., R.Ph. Bruce Siecker is president of Paradigm Research & Advisory Services, Inc. based in Stone Ridge, Virginia.
Fundamentals of Medication Therapy Management (MTM) Services By Bruce R. Siecker, Ph.D., R.Ph. Bruce Siecker is president of Paradigm Research & Advisory Services, Inc. based in Stone Ridge, Virginia.
Blue Cross Blue Shield of Michigan MiPCT/PDCM Reimbursement Policy and Billing Guidelines Commercial
 Purpose Beginning April 1, 2012 BCBSM began accepting and paying claims for Provider Delivered Care Management services delivered by qualified Primary Care Physicians to patients in physician practices
Purpose Beginning April 1, 2012 BCBSM began accepting and paying claims for Provider Delivered Care Management services delivered by qualified Primary Care Physicians to patients in physician practices
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
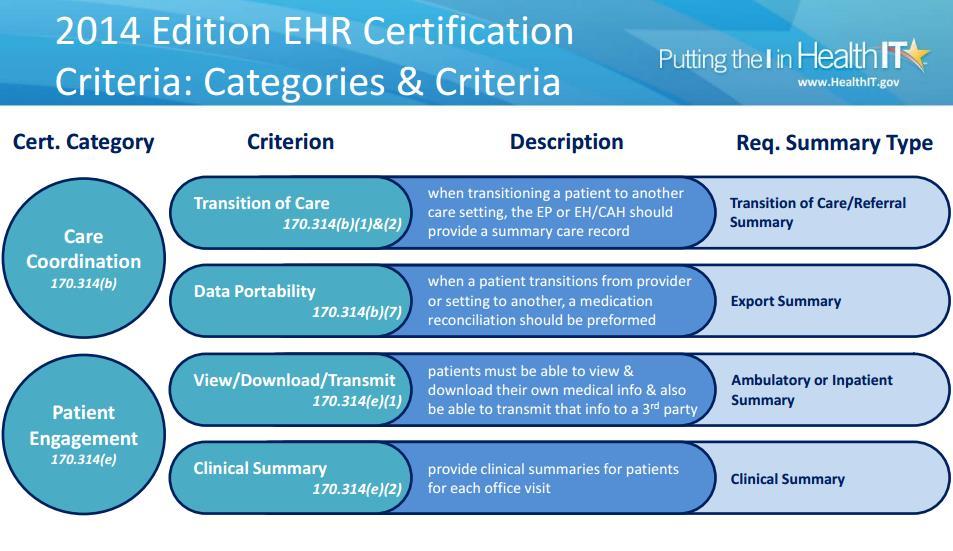
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Healthcare Reimbursement Change VBP -The Future is Now
 Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods
 A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
The Minnesota Accountable Health Model
 The Minnesota Accountable Health Model L E A R N I N G S F R O M S I M : I N T E G R AT I O N O F P R I M A R Y A N D B E H AV I O R A L H E A LT H R U R A L H E A LT H C O N F E R E N C E J U N E 2 0,
The Minnesota Accountable Health Model L E A R N I N G S F R O M S I M : I N T E G R AT I O N O F P R I M A R Y A N D B E H AV I O R A L H E A LT H R U R A L H E A LT H C O N F E R E N C E J U N E 2 0,
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Objectives. Medication Therapy Management: The Important Role of the Pharmacy Technician. Medication Therapy Management (MTM)
") Medication Therapy Management: The Important Role of the Pharmacy Technician Nancy Myers, PharmD, MBA, BCPS, CDE Katrina Harper, PharmD, MBA Objectives Define Medication Therapy Management () and its Core
Medication Therapy Management: The Important Role of the Pharmacy Technician Nancy Myers, PharmD, MBA, BCPS, CDE Katrina Harper, PharmD, MBA Objectives Define Medication Therapy Management () and its Core
MANAGED CARE IS HERE
 MANAGED CARE IS HERE Survive or Thrive Susie Mix CEO/President Mix Solutions Inc. 1 Nursing Home (NH) Industry Transformation Senior Care Industry Trends & Strategies Why do we care about change? Finances
MANAGED CARE IS HERE Survive or Thrive Susie Mix CEO/President Mix Solutions Inc. 1 Nursing Home (NH) Industry Transformation Senior Care Industry Trends & Strategies Why do we care about change? Finances
Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims
 Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims Skilled Nursing Facility Services Custodial Care, SLP and Hospice R&B
Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims Skilled Nursing Facility Services Custodial Care, SLP and Hospice R&B
Sharp HealthCare ACO. Presented by: Donald C. Balfour, M.D. President and Medical Director Sharp Rees-Stealy Medical Group
 Sharp HealthCare ACO Presented by: Donald C. Balfour, M.D. President and Medical Director Sharp Rees-Stealy Medical Group Institute for Quality Leadership Annual Conference October 4, 2012 Sharp ACO Collaborations
Sharp HealthCare ACO Presented by: Donald C. Balfour, M.D. President and Medical Director Sharp Rees-Stealy Medical Group Institute for Quality Leadership Annual Conference October 4, 2012 Sharp ACO Collaborations
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
POWER MOBILITY DEVICE REGULATION AND PAYMENT
 POWER MOBILITY DEVICE REGULATION AND PAYMENT Today s Actions: The Centers for Medicare & Medicaid Services (CMS) is issuing a final rule implementing provisions in the Medicare Modernization Act (MMA)
POWER MOBILITY DEVICE REGULATION AND PAYMENT Today s Actions: The Centers for Medicare & Medicaid Services (CMS) is issuing a final rule implementing provisions in the Medicare Modernization Act (MMA)
Medicare & Medicaid EHR Incentive Program. Betsy L. Thompson, MD, DrPH EHR Summit October 4, 2010
 Medicare & Medicaid EHR Incentive Program Betsy L. Thompson, MD, DrPH EHR Summit October 4, 2010 1 Overview Background and Policy Context EHR Incentive Program Basics Who is Eligible to Participate How
Medicare & Medicaid EHR Incentive Program Betsy L. Thompson, MD, DrPH EHR Summit October 4, 2010 1 Overview Background and Policy Context EHR Incentive Program Basics Who is Eligible to Participate How
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Physician-led ACOs: Opportunities & Challenges
 Physician-led ACOs: Opportunities & Challenges Farzad Mostashari, MD Founder/CEO, Aledade Inc, former National Coordinator for Health Information Technology May 13, 2015 Physician Webinar Series #16 Welcome
Physician-led ACOs: Opportunities & Challenges Farzad Mostashari, MD Founder/CEO, Aledade Inc, former National Coordinator for Health Information Technology May 13, 2015 Physician Webinar Series #16 Welcome
Finding a Faster Path to Value-Based Care
 Finding a Faster Path to Value-Based Care June 2016 Executive Summary The U.S. healthcare system is progressing along a continuum from volume- to valuebased care models where physicians and health systems
Finding a Faster Path to Value-Based Care June 2016 Executive Summary The U.S. healthcare system is progressing along a continuum from volume- to valuebased care models where physicians and health systems
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS. Amy Hancock, CEO Presented to: CPERI April 16, 2018
 DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Review Process. Introduction. InterQual Level of Care Criteria Subacute & SNF Criteria. Reference materials. Informational notes
 InterQual Level of Care Criteria Subacute & SNF Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
InterQual Level of Care Criteria Subacute & SNF Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
Readmission Partnership Between Acute Care and Post-Acute Care
 Readmission Partnership Between Acute Care and Post-Acute Care Melissa Suzuki, MSW Regional UR Case Manager Specialist Commonwealth Care of Roanoke (CCR) Amanda Melvin, MSW Referral Development Coordinator
Readmission Partnership Between Acute Care and Post-Acute Care Melissa Suzuki, MSW Regional UR Case Manager Specialist Commonwealth Care of Roanoke (CCR) Amanda Melvin, MSW Referral Development Coordinator
Wound Care Reimbursement. Things Are A-Changing!
 Wound Care Reimbursement Things Are A-Changing! Kathleen D. Schaum, MS President Kathleen D. Schaum & Assoc., Inc. kathleendschaum@bellsouth.net 561-964-2470 Disclosure No relevant financial relationships
Wound Care Reimbursement Things Are A-Changing! Kathleen D. Schaum, MS President Kathleen D. Schaum & Assoc., Inc. kathleendschaum@bellsouth.net 561-964-2470 Disclosure No relevant financial relationships
Episode Payment Models Final Rule & Analysis
 Episode Payment Models Final Rule & Analysis February 15, 2017 Agenda Overview Changes from Proposed Rule Categorization of Episodes Episode Attribution Reconciliation Quality Performance Cardiac Rehab
Episode Payment Models Final Rule & Analysis February 15, 2017 Agenda Overview Changes from Proposed Rule Categorization of Episodes Episode Attribution Reconciliation Quality Performance Cardiac Rehab
How to Improve the Discharge Process. Michelle Mourad, MD Ryan Greysen, MD
 How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
$traight Talk Hot Topics. Free Standing EDs. Free Standing EDs 11/6/2017. David A. McKenzie, CAE ACEP Reimbursement Director
 Free Standing EDs $traight Talk Hot Topics Free Standing EDs David A. McKenzie, CAE ACEP Reimbursement Director CPT Definition for the use of 99281-99285: Organized hospital-based facility for the provision
Free Standing EDs $traight Talk Hot Topics Free Standing EDs David A. McKenzie, CAE ACEP Reimbursement Director CPT Definition for the use of 99281-99285: Organized hospital-based facility for the provision
Comparison of Bundled Payment Models. Model 1 Model 2 Model 3 Model 4. hospitals, physicians, and post-acute care where
 Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Improving Emergency Department Transitions of Care Can It Help with ED Overcrowding? Stephen V. Cantrill, MD, FACEP Denver Health Medical Center
 Improving Emergency Department Transitions of Care Can It Help with ED Overcrowding? Stephen V. Cantrill, MD, FACEP Denver Health Medical Center Improving Emergency Department Transitions of Care: Can
Improving Emergency Department Transitions of Care Can It Help with ED Overcrowding? Stephen V. Cantrill, MD, FACEP Denver Health Medical Center Improving Emergency Department Transitions of Care: Can
Improving Transitions Across the Continuum of Care
 Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Home Health & HP Provider Relations
 Home Health & Hospice HP Provider Relations October 2010 Agenda Session Objectives Home Health Benefit Coverage Billing Overhead Multiple Visits Most Common Denials Hospice Benefit Coverage Election/Revocation/Discharge
Home Health & Hospice HP Provider Relations October 2010 Agenda Session Objectives Home Health Benefit Coverage Billing Overhead Multiple Visits Most Common Denials Hospice Benefit Coverage Election/Revocation/Discharge
Test bank PowerPoint slides for each chapter Instructor guides for each chapter (with answers for discussion questions and case studies)
") This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
Discharge Planning/ Transition of Care: What s Hot in the 20-teens CMSANJ - July 24, 2014
 Discharge Planning/ Transition of Care: What s Hot in the 20-teens CMSANJ - July 24, 2014 Jackie Birmingham, RN, BSN, MS VP, Emerita, Clinical Leadership Curaspan Health Group jbirmingham@curaspan.com
Discharge Planning/ Transition of Care: What s Hot in the 20-teens CMSANJ - July 24, 2014 Jackie Birmingham, RN, BSN, MS VP, Emerita, Clinical Leadership Curaspan Health Group jbirmingham@curaspan.com
Geisinger s Bundled Payments Experience for Better Clinical Integration to Drive Quality to Lower Cost
 Geisinger s Bundled Payments Experience for Better Clinical Integration to Drive Quality to Lower Cost Thomas Graf, MD Chief Medical Officer Population Health and Longitudinal Care Service Lines Let us
Geisinger s Bundled Payments Experience for Better Clinical Integration to Drive Quality to Lower Cost Thomas Graf, MD Chief Medical Officer Population Health and Longitudinal Care Service Lines Let us
What is Value-Based Care
 Genesis HealthCare Value-Based Care Initiatives and BPCI Model 3 Aug 4, 2017 Copyright 2017 by Genesis HealthCare LLC. All Rights Reserved. What is Value-Based Care 2 Value-based care delivery is an approach
Genesis HealthCare Value-Based Care Initiatives and BPCI Model 3 Aug 4, 2017 Copyright 2017 by Genesis HealthCare LLC. All Rights Reserved. What is Value-Based Care 2 Value-based care delivery is an approach
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Forces of Change- Seeing Stepping Stones Not Potholes
 May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
May 19, 2014 Forces of Change- Seeing Stepping Stones Not Potholes 2 3 4 Overview Demographics Long Term Care Financing Challenges Broad Health System Challenges Payment Reform Delivery System Reform Where
Personal Care Services (PCS): An Overview of PCS and The Request for Independent Assessment for PCS Attestation of Medical Need Form (DMA 3051)
: An Overview of PCS and The Request for Independent Assessment for PCS Attestation of Medical Need Form (DMA 3051)") Personal Care Services (PCS): An Overview of PCS and The Request for Independent Assessment for PCS Attestation of Medical Need Form (DMA 3051) January 2018 OBJECTIVES At the conclusion of this training,
Personal Care Services (PCS): An Overview of PCS and The Request for Independent Assessment for PCS Attestation of Medical Need Form (DMA 3051) January 2018 OBJECTIVES At the conclusion of this training,
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Guidance for Medication Reconciliation and System Integration Process
 Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Pitch Perfect: Selling Your Services to LTC Facilities
 Pitch Perfect: Selling Your Services to LTC Facilities Lou Ann Brubaker, President Brubaker Consulting www.brubakerconsulting.com 301 535 5449 brubak97@aol.com Linkedin Disclosure Lou Ann Brubaker is the
Pitch Perfect: Selling Your Services to LTC Facilities Lou Ann Brubaker, President Brubaker Consulting www.brubakerconsulting.com 301 535 5449 brubak97@aol.com Linkedin Disclosure Lou Ann Brubaker is the
Federal law does not require state Medicaid programs to cover specific substance use disorder interventions
 Federal law does not require state Medicaid programs to cover specific substance use disorder interventions States have the option Coverage differs state-by-state Prior authorizations are often necessary
Federal law does not require state Medicaid programs to cover specific substance use disorder interventions States have the option Coverage differs state-by-state Prior authorizations are often necessary
The Accountable Care Organization Specific Objectives
 Accountable Care Organizations and You E. Christopher h Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences CEO, OSU Faculty Group Practice Chair, Department of Surgery Ohio State
Accountable Care Organizations and You E. Christopher h Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences CEO, OSU Faculty Group Practice Chair, Department of Surgery Ohio State
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Risk Adjusted Diagnosis Coding:
 Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Improving Care Transitions
 Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow
 One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
Interoperability is Happening Now
 Interoperability is Happening Now Nick Knowlton and Tammy Ordoyne-Vial Brightree and Ochsner HME Interoperability - Better Business, Better Outcomes Shifts in the Healthcare Ecosystem impact our HME Space
Interoperability is Happening Now Nick Knowlton and Tammy Ordoyne-Vial Brightree and Ochsner HME Interoperability - Better Business, Better Outcomes Shifts in the Healthcare Ecosystem impact our HME Space
Topics for Today s Discussion
 MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion