ASSESSING AND ADDRESSING THE SOCIAL DETERMINANTS OF HEALTH USING PRAPARE:
|
|
|
- Emily Washington
- 5 years ago
- Views:
Transcription




1 ASSESSING AND ADDRESSING THE SOCIAL DETERMINANTS OF HEALTH USING PRAPARE: PROTOCOL FOR RESPONDING TO AND ASSESSING PATIENTS ASSETS, RISKS, AND EXPERIENCES This project was made possible with funding from: 1
2 WEBINAR OBJECTIVES Strategize the PRAPARE implementation process Introduce EHR template for data collection/patient engagement Describe health center implementation experience, including workflow Previous webinars located in the Social Determinants of Health Resources folder at 2
3 IN DEVELOPMENT: IMPLEMENTATION AND ACTION TOOLKIT Categories Step 1: Understand the Project Step 2: Engage Key Stakeholders Step 3: Strategize the Implementation Plan Step 4: Technical Implementation Step 5: Workflow Implementation Step 6: Understand and Report Your Data Step 7: Act on Your Data Step 8: Use Your Data to Drive Payment and Policy Transformation Examples of Potential Resources to Include Project overview, project framework, defining risk, case studies, FAQs Messaging materials, change management guidance Readiness assessment, PDSA materials, 5 Rights Framework, Implementation timeline, progress reports, legal documents PRAPARE paper assessment, data documentation, EHR templates, sample data dictionaries, data specifications, data warehouse and retrieval strategies, guidelines for using design and requirements documents Workflow diagrams, data collection training curriculum, lessons learned and best practices Reporting requirements, sample database, sample data outputs, sample data analyses and reports, cross-tabulating data, evaluation protocol, populationlevel planning, guidelines for data integration Strategy for detecting risk, report on best practices and processes for using SDH data, examples of SDH interventions, SDH response codes, linking to enabling services codes Strategy to engage payers, funding SDH efforts, data visualization templates 3
4 IN DEVELOPMENT: IMPLEMENTATION AND ACTION TOOLKIT Categories Step 1: Understand the Project Step 2: Engage Key Stakeholders Step 3: Strategize the Implementation Plan Step 4: Technical Implementation Step 5: Workflow Implementation Step 6: Understand and Report Your Data Step 7: Act on Your Data Step 8: Use Your Data to Drive Payment and Policy Transformation Examples of Potential Resources to Include Project overview, project framework, defining risk, case studies, FAQs Messaging materials, change management guidance Readiness assessment, PDSA materials, 5 Rights Framework, Implementation timeline, progress reports, legal documents PRAPARE paper assessment, data documentation, EHR templates, sample data dictionaries, data specifications, data warehouse and retrieval strategies, guidelines for using design and requirements documents Workflow diagrams, data collection training curriculum, lessons learned and best practices Reporting requirements, sample database, sample data outputs, sample data analyses and reports, cross-tabulating Available data, in August evaluation protocol, populationlevel planning, guidelines for data integration through an End User License Agreement Strategy for detecting risk, report on best practices and processes for using SDH data, examples of SDH interventions, SDH response codes, linking to enabling services codes Strategy to engage payers, funding SDH efforts, data visualization templates 4

5 CHAT FEATURE The chat feature is available to ask questions or make comments anytime throughout today s webinar. We will answer as many questions as possible. Submit to All Panelists and click the send button.
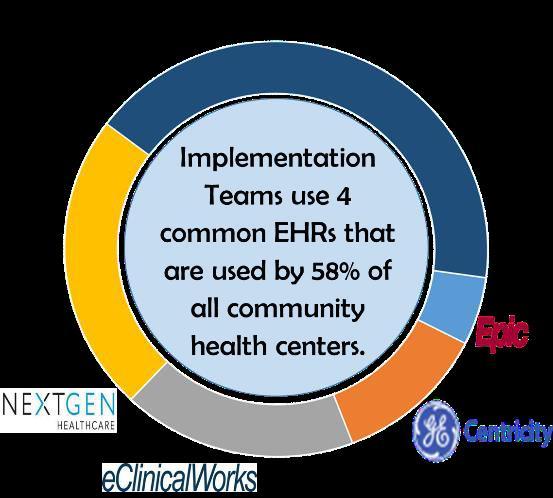
6 in GE Centricity Webinar Dave Faldmo (Siouxland Community Health Center) Christina Kim (Alliance of Chicago) Kyle Pedersen (Iowa Primary Care Association)
7 Why do CHCs need to document and address SDH? Research demonstrates SDH: Contribute to poorer health outcomes Lead to health disparities Impact on health centers and population served: Increasingly difficult to improve health outcomes for complex patients Possible negative impacts under: -Value-based pay, such as incentive payments, shared shavings, and pay for performance -Public Reporting Insufficient funds to provide comprehensive care HRSA s goal is to have providers screen for and address SDH within the EMR

8
9
10 Why We Participated: Provide better care to patients Collect more robust data about other factors impacting health Begin to match identified issues with solutions with the health center Use data to establish or grow partnerships with other community resources Leverage data and accompanying interventions to provide evidence to payors and policymakers about the needs of patients, a broader definition of patient risk, and to ensure adequate reimbursement for safety net providers
11 Overall Project Goals To create, implement/test, and promote a national standardized patient risk assessment protocol to assess and address patients social determinants of health (SDH). Document the extent to which each patient and total patient populations are complex. Use that data to: improve patient health, affect change at the community/population level sustain resources and create community partnerships necessary to improve health.





12 Timeline of the project We have just finished year 2 and are now in year 3 of the 3 year project. Year 1 Year 2 Year 3 Develop paper based tool Develop EMR template and test tool in health center workflow with CHCs and HCCNs Disseminate tool widely and release final report
13 was designed specifically to aid health centers in gathering data that informs and addresses individual patient care and population health management, while capturing what makes health center populations unique. Individuallevel Local-level State and nationallevel Patient and Family Care Team Members Health Center Community Policies Local Health System Payment Negotiation State and National Policies Improve health Better manage patient needs with services Better understand patient population Inform advocacy efforts related to local policies around SDH Provide comparison data for other local clinics and to inform partnerships Demonstrate the relationship between patient SDH and cost of care for fair provider comparisons (risk adjustment) Improve health center capacity for serving complex patients (payment reform) 13

14 SDH Impact the Ability to Achieve Triple Aim
15 SDH Impact Ability to Achieve Triple Aim Complex patients must be treated in new and innovative ways to achieve the Triple Aim Complex patients usually have multiple needs that must be addressed to produce the desired clinical results. Health centers are held accountable for patient health and cost outcomes. Complexity results when multiple risks converge to interfere with the Triple Aim of improving patient health and experience of care, while lowering cost. In order to assess and address patient complexity, care teams need data on patient SDH assets, risks, and experiences to inform care. Complex patients require complex solutions
16 Our journey with PRAPARE Siouxland Community Health Center Sioux City, IA and South Sioux City, NE
17 Steps needed to develop readiness: 1. Educate staff and leadership of the value of PRAPARE Educate everyone in the organization at a high level. Educate key players at a detailed level Get the right people on the bus!
18 Steps needed to develop readiness: 2. Be prepared to address concerns and questions from staff and administration We have too much going on right now to add another project. We already screen for and address social determinants of health. Once we identify a social determinant of health, are we accountable to provide help to overcome the determinant? Who is going to be responsible for addressing the need?
19 Steps needed to develop readiness: 3. Be prepared to address questions and concerns of patients. Why are you asking me these questions? Who will have access to this information? Will providing this information impact my ability to receive care?
20 Steps needed to develop readiness: 4. Catalog current countermeasure/resources available, both inhouse and in the community, for each social determinants of health surveyed on the tool. Identify resources that need to be developed or improved. Identify community partnerships that need to be initiated or strengthened.
21 Steps needed to develop readiness: 5. Use 5 Rights and PDSA cycle to develop workflow for administering and responding to PRAPARE tool. The 5 Rights include: the right information, to the right person, in the right intervention format, through the right channel, at the right time in workflow.
22 Steps needed to develop readiness: 5. Use 5 Rights and PDSA cycle to develop workflow for administering and responding to PRAPARE tool. How will tool be administered to the patient to ensure that it accurately identifies the SDH the patient may have? (obtain right information) Who will address social determinants identified? (right person) How will resource information be organized so that it is readily available and standardized for all? (right intervention format) How is the appropriate care team member notified to address the SDH identified? (right channel) When in the patient visit does it make sense to administer the tool and when is the best time to address identified SDH? (right workflow)
23 Implementation at SCHC: How we prepared for this change? - Invitation to all employees to join the project. - Planning meeting which included employees from various departments at all levels. - Determined initial teams to try out survey with patients and identify workflow issues before it is rolled out to all the provider teams.
24 Implementation at SCHC: Who would survey the patients? -PDSA 1 Behavioral Health/Social Services and PCMH Case Managers complete face to face interview with patients. -PDSA 2 Paper copies were developed in 4 languages for provider teams to handout to the patients while waiting in the exam room. -Questions were added to identify if the patient would like to visit with behavioral health staff.
25 Implementation at SCHC: How did we roll out to all the provider teams? - Educating all provider teams one on one. - Developed instructions in writing for employees to refer back to and to educate new employees. -purpose of the survey -how to locate appropriate community resource -what to do with difficult questions
26
27
28
29
30 Implementation at SCHC: How does this help medical providers, behavioral health, and nurse case managers work with patients? - Survey allows for behavioral health to have an initial meeting with patients and build rapport. - We don t know what we don t ask. - Opportunity to engage the patient in their psychosocial health and discuss how these things could affect their overall health.
31 Challenges/Impacts Need to account for data collection overload among staff and share how the data will be used and why it is valuable ROI when this adds time to the patient visit Don t treat as a project, but instead part of providing care The data captured as part of the pilot project has multiple uses endless number of case statements possible More discussion about how the data will be used, i.e. is it most important to impact point of care or policy or something else? Where can the easiest customization and marrying of data occur? Need to consider what interventions are internal versus require community partnerships
32 Template
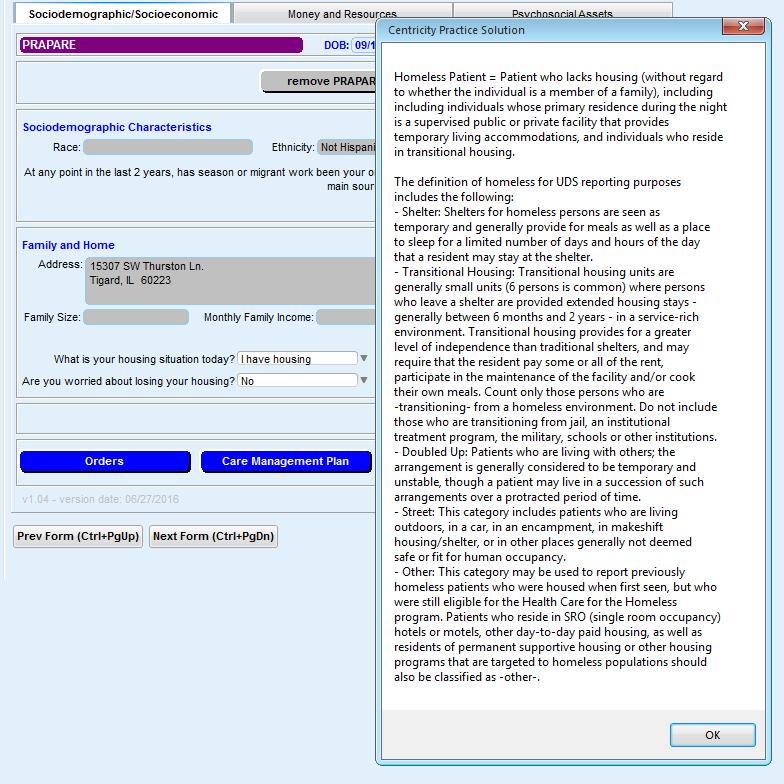
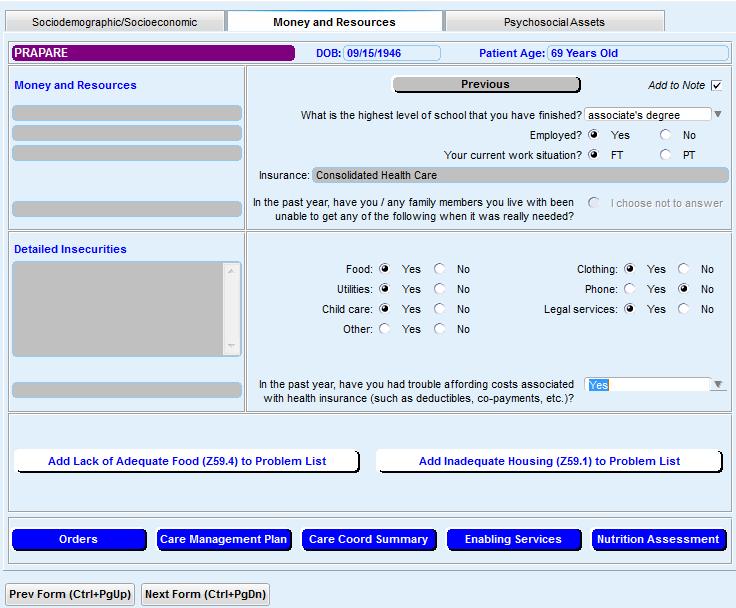
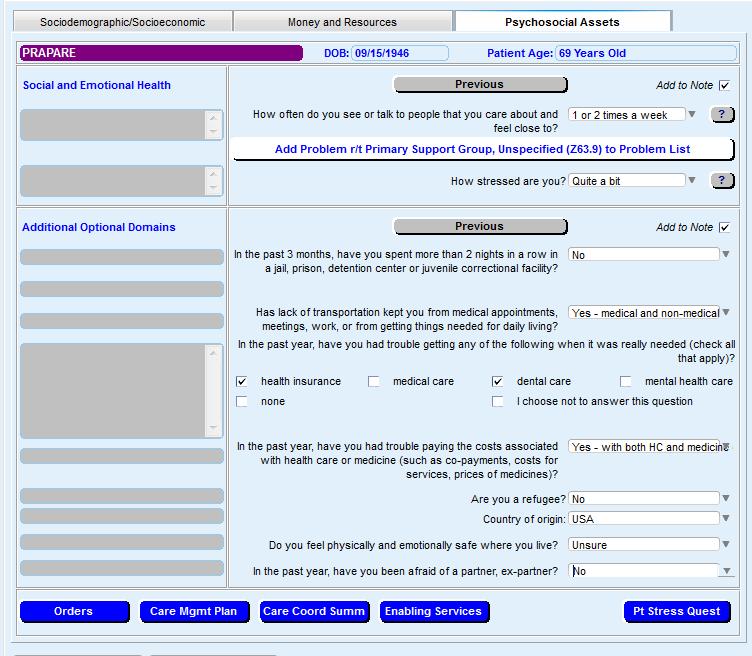
33 Unique Features: 3 Tabs: 1. Sociodemographic/Socioeconomic 2. Money & Resources 3. Psychosocial Assets User friendly look & feel Pulls fields from registration ICD-10 codes populate depending on how the patient responds Blue jump buttons > brings you to additional forms/assessments Ability to show previously captured information Remove from note option for patient sensitive information
34 How to Implement PRAPARE: How to Install into CPS: 1. Save the PRAPARE zip folder to your computer 2. Log in to CPS 3. Administration Module 4. System Folder > Import Clinical Kits 5. Click Import Clinical Kit 6. If the file is saved to the local PC, chose the location & double click on the source drive 7. Double click on the PRAPARE folder > Double click on the text file 1. Select YES TO ALL if a pop up display appears 8. Return to Chart Documents > Start a new encounter > Select Add > Locate the PRAPARE form to add

35 Greyed out fields will pull from PM if documented
36

37
38
39
40 Reporting / Future Plans
41 PRAPARE Data Over 25,000 patients 3,842 surveys completed 13% do not have housing (483) 18% indicate they only have social interactions 1 2 per week (696) 38% indicate quite a bit, somewhat, very much stress (1,463) * Data report pulled 6/9/2016
42 Unmet Materials Needs Child care (104) Clothing (328) Food (463) Medicine/Medical Care (538) Phone (316) Rent/Mortgage (369) Transportation (443) Utilities (369) * Data report pulled 6/9/2016
43 Insights from Data Staff not surprised by the issues identified through the tool Data changed the way the care teams communicated with patients (education question) Lots of discussion about possible interventions if incarceration identified as an issue Changed the way Siouxland approached community partners transportation example
44 Reporting: PRAPARE Alliance of Chicago is working on enhancing the reporting capabilities Health Center friendly Data Warehouse Adding obs terms behind each question response to enabling services to document interventions *Work in progress
45 Future plans: Risk coding/stratification as a hot topic Need for consideration of non-clinical factors to be included Payors need providers to come to the table with data Providers need payors to recognize these factors Together we need to develop new models Documenting Enabling Services to validate to payers and policy makers need for CHC funding and for internal justification Identifying most common determinants and determining best ways to address Bolster or create in-house services Develop or strengthen and external partnerships Partner with others to create Coordinate with policymakers and community stake holders to address social and environmental conditions
46 More future plans Cross tab survey results with clinical indicators such as chronic diseases Think about staffing needs at the health center and further community partnerships needed to connect patients to necessary interventions Build these necessary interventions into the overall care coordination approach at health centers Using the data as part of PCMH re-recognition process
47 Opportunities with Payors in Iowa Some alignment with largest commercial payor and Medicaid around a 3M product and overall approach through CMS SIM Model Testing funding Interest in better understanding SDOH data at patient level, community level, and state level Exploration of interest in different payment methodologies with new managed care plans Likely need more health centers to implement the tool to reach critical mass, but believe providers need to collect this data
48 Final Thoughts Matthew Nagato, HI PCA Data is the currency of advocacy. Trust is the currency of medicine. This project brings both of these issues to the forefront We believe this project is the first step in a long journey to figure out how the marrying of health care and social determinant data can lead to better individual health (via more individualized and higher quality care) and community health (via advocacy and policy change)



49 Questions & Thoughts David Faldmo PA-C, MPAS Siouxland Community Health Center Sioux City, Iowa
Assessing Social Determinant of Health Data and Raising Awareness of Patient Needs
 Assessing Social Determinant of Health Data and Raising Awareness of Patient Needs Iowa Primary Care Association 2015 Annual Conference October 21, 2015 Presentation Goals Share the experience of two health
Assessing Social Determinant of Health Data and Raising Awareness of Patient Needs Iowa Primary Care Association 2015 Annual Conference October 21, 2015 Presentation Goals Share the experience of two health
COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE
 COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 BACKGROUND ON PRAPARE 2 HEALTH,
COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 BACKGROUND ON PRAPARE 2 HEALTH,
WHAT IS PRAPARE ADDRESSING SOCIAL DETERMINANTS OF HEALTH USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE
 ADDRESSING SOCIAL DETERMINANTS OF HEALTH USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 WHAT IS PRAPARE 2 PRAPARE: PROTOCOL
ADDRESSING SOCIAL DETERMINANTS OF HEALTH USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 WHAT IS PRAPARE 2 PRAPARE: PROTOCOL
COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE
 COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 BACKGROUND ON PRAPARE 2 HEALTH,
COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA USING PRAPARE TO REDUCE DISPARITIES, IMPROVE OUTCOMES, AND TRANSFORM CARE This project was made possible with funding from: 1 BACKGROUND ON PRAPARE 2 HEALTH,
Massachusetts League of Community Health Centers CHI Conference May 3, 2017 AGENDA. Overview of PRAPARE
 GETTING STARTED IN USING PRAPARE TO ASSESS AND ADDRESS THE SOCIAL DETERMINANTS OF HEALTH Michelle Jester, Research Manager National Association of Community Health Centers This project was made possible
GETTING STARTED IN USING PRAPARE TO ASSESS AND ADDRESS THE SOCIAL DETERMINANTS OF HEALTH Michelle Jester, Research Manager National Association of Community Health Centers This project was made possible
COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA TO REDUCE DISPARITIES AND IMPROVE OUTCOMES
 COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA TO REDUCE DISPARITIES AND IMPROVE OUTCOMES Roger Chaufournier President and CEO, CSI Solutions, LLC Michelle Proser Director of Research, National Association
COLLECTING SOCIAL DETERMINANTS OF HEALTH DATA TO REDUCE DISPARITIES AND IMPROVE OUTCOMES Roger Chaufournier President and CEO, CSI Solutions, LLC Michelle Proser Director of Research, National Association
Health Coaching in Team-Based Care. Recipes for Success
 Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
WHITE PAPER. Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice
 WHITE PAPER Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice Maximizing Pay-for-Performance Opportunities In today s
WHITE PAPER Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice Maximizing Pay-for-Performance Opportunities In today s
Lessons from the States: Oregon s APM Model
 Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Value-based Care and the Role of Health Information Technology. Andrew Hamilton, RN, BS, MS, Chief Informatics Officer
 Value-based Care and the Role of Health Information Technology Andrew Hamilton, RN, BS, MS, Chief Informatics Officer HHS Core Strategies 1. Improving payment process to incentivize quality and value of
Value-based Care and the Role of Health Information Technology Andrew Hamilton, RN, BS, MS, Chief Informatics Officer HHS Core Strategies 1. Improving payment process to incentivize quality and value of
Assessing and Addressing the Social Determinants of Health Using PRAPARE: Experiences in California
 Assessing and Addressing the Social Determinants of Health Using PRAPARE: Experiences in California This project was made possible with funding from: December 7, 2017 Copyright Notice 2017. National Association
Assessing and Addressing the Social Determinants of Health Using PRAPARE: Experiences in California This project was made possible with funding from: December 7, 2017 Copyright Notice 2017. National Association
A Journey PCMH & Practice Transformation PCMH 101. Kentucky Primary Care Association Lexington Kentucky June 11, 2014
 A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
Guide to Population Health Management
 Guide to Population Health Management presented by the Healthcare Intelligence Network Note: This is an authorized excerpt from the Guide to Population Health Management. To download the entire guide,
Guide to Population Health Management presented by the Healthcare Intelligence Network Note: This is an authorized excerpt from the Guide to Population Health Management. To download the entire guide,
Documenting Your Impact: Tools For Addressing Social Determinants Of Health And Demonstrating Value
 Documenting Your Impact: Tools For Addressing Social Determinants Of Health And Demonstrating Value Leinaala Kanana, Director of Community Health AANHPI Summit May 26, 2017 ~ San Francisco, California
Documenting Your Impact: Tools For Addressing Social Determinants Of Health And Demonstrating Value Leinaala Kanana, Director of Community Health AANHPI Summit May 26, 2017 ~ San Francisco, California
Unit 1 Introduction to the Medical Home JumpStart Program
 Objectives Overview of the Medical Home model of care and its benefits Introducing the National Committee for Quality Assurance (NCQA) recognition process Overview of the Medical Home JumpStart approach
Objectives Overview of the Medical Home model of care and its benefits Introducing the National Committee for Quality Assurance (NCQA) recognition process Overview of the Medical Home JumpStart approach
Michigan Primary Care Association
 Michigan Primary Care Association Improving Outcomes Finance & Quality through Integrated Information Conference June 2-3, 2016 Shanty Creek Resorts Bellaire, MI Definition and Purpose HRSA s Health Center
Michigan Primary Care Association Improving Outcomes Finance & Quality through Integrated Information Conference June 2-3, 2016 Shanty Creek Resorts Bellaire, MI Definition and Purpose HRSA s Health Center
ICD-10 Frequently Asked Questions
 ICD-10 Frequently Asked Questions September 2015 pulseinc.com + 1.800.444.0882 We care for your practice, as if it were our own. Acknowledgments Document Number: 01 Date: September 7, 2015 Pulse Systems
ICD-10 Frequently Asked Questions September 2015 pulseinc.com + 1.800.444.0882 We care for your practice, as if it were our own. Acknowledgments Document Number: 01 Date: September 7, 2015 Pulse Systems
Why Are We Doing This?
 ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition
 What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
The SoonerCare Health Management Program
 The SoonerCare Health Management Program National Medicaid Congress June 13, 2011 Washington, DC Dr. Michael Herndon Oklahoma Health Care Authority Mike Speight Iowa Foundation for Medical Care Why did
The SoonerCare Health Management Program National Medicaid Congress June 13, 2011 Washington, DC Dr. Michael Herndon Oklahoma Health Care Authority Mike Speight Iowa Foundation for Medical Care Why did
PCORI Funding Announcement (PFA):
:") Patient-Centered Outcomes Research Institute PCORI Funding Announcement (PFA): Registration & Letter of Intent June 2012 1 Today s Agenda Introduction to PCORI About PCORI, National Priorities and the
Patient-Centered Outcomes Research Institute PCORI Funding Announcement (PFA): Registration & Letter of Intent June 2012 1 Today s Agenda Introduction to PCORI About PCORI, National Priorities and the
Training Quick Steps Front Office Workflow. Using the PrognoCIS Schedule
 Using the PrognoCIS Schedule The primary screen front office personnel will use within the PrognoCIS EMR module is the Schedule tab. The user may alter the presentation of the data according to local preferences.
Using the PrognoCIS Schedule The primary screen front office personnel will use within the PrognoCIS EMR module is the Schedule tab. The user may alter the presentation of the data according to local preferences.
Health Center Controlled Networks Overview and Resources
 Health Center Controlled Networks Overview and Resources BPHC/OQI/SPD Colleen Morris, MS,RN February 15, 2018 Agenda Health Center Program Health Center Controlled Networks and SPD Partners NACHC Network
Health Center Controlled Networks Overview and Resources BPHC/OQI/SPD Colleen Morris, MS,RN February 15, 2018 Agenda Health Center Program Health Center Controlled Networks and SPD Partners NACHC Network
Payment Reform Strategies. Ann Thomas Burnett BlueCross BlueShield of South Carolina
 Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013
 State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013 The National Association of Medicaid Directors (NAMD) is engaging states in shared learning on how Medicaid
State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013 The National Association of Medicaid Directors (NAMD) is engaging states in shared learning on how Medicaid
Core Item: Hospital. Cover Page. Admissions and Readmissions. Executive Summary
 Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Creating Quality Improvement and Incentive Platforms in the Safety Net 2009 Pay for Performance Summit
 Creating Quality Improvement and Incentive Platforms in the Safety Net 2009 Pay for Performance Summit Presented by: Julie Murchinson, Manatt Health Solutions Jonah Frohlich, California HealthCare Foundation
Creating Quality Improvement and Incentive Platforms in the Safety Net 2009 Pay for Performance Summit Presented by: Julie Murchinson, Manatt Health Solutions Jonah Frohlich, California HealthCare Foundation
Toward the Electronic Patient Record:
 June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
Essentia Health. A View on Information Technology. ND HIMS Conference April 12, Tim Sayler, COO Essentia Health - West
 Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Succeeding with Accountable Care Organizations
 Succeeding with Accountable Care Organizations The Point B Webinar Series October 25, 2011 Today s Discussion Key ACO trends and emerging models Critical success factors for building an ACO Developing
Succeeding with Accountable Care Organizations The Point B Webinar Series October 25, 2011 Today s Discussion Key ACO trends and emerging models Critical success factors for building an ACO Developing
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
The Transition to Version 5010 and ICD-10
 The Transition to Version 5010 and ICD-10 An Overview Denise M. Buenning, MsM Director, Administrative Simplification Group Office of E-Health Standards and Services Centers for Medicare & Medicaid Services
The Transition to Version 5010 and ICD-10 An Overview Denise M. Buenning, MsM Director, Administrative Simplification Group Office of E-Health Standards and Services Centers for Medicare & Medicaid Services
Transformational Payment Reform: How will FQHC s survive?
 Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
New Problem List Dictionary (IMO) Workflow Recommendations
 Workflow Recommendations") Catherine Hill, RN May 15, 2014 The Problem List Overview What is SNOMED-CT? Mapping ICD SNOMED One-to-one (Bulk mapping) One-to-many (Manual mapping) Mapping Required Basic Navigation Data Display Grid
Catherine Hill, RN May 15, 2014 The Problem List Overview What is SNOMED-CT? Mapping ICD SNOMED One-to-one (Bulk mapping) One-to-many (Manual mapping) Mapping Required Basic Navigation Data Display Grid
Care360 EHR Frequently Asked Questions
 Care360 EHR Frequently Asked Questions Table of Contents Care360 EHR... 4 What is Care360 EHR?... 4 What are the current capabilities of Care 360 EHR?... 4 Is Care 360 EHR an EMR?... 5 Can I have Care360
Care360 EHR Frequently Asked Questions Table of Contents Care360 EHR... 4 What is Care360 EHR?... 4 What are the current capabilities of Care 360 EHR?... 4 Is Care 360 EHR an EMR?... 5 Can I have Care360
Quality, Cost and Business Intelligence in Healthcare
 Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
College-wide Patient-Centered Medical Home Program Meharry Medical College
 + The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
+ The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
Seamless Clinical Data Integration
 Seamless Clinical Data Integration Key to Efficiently Increasing the Value of Care Delivered The value of patient care is the single most important factor of success for healthcare organizations transitioning
Seamless Clinical Data Integration Key to Efficiently Increasing the Value of Care Delivered The value of patient care is the single most important factor of success for healthcare organizations transitioning
Leverage Information and Technology, Now and in the Future
 June 25, 2018 Ms. Seema Verma Administrator Centers for Medicare & Medicaid Services US Department of Health and Human Services Baltimore, MD 21244-1850 Donald Rucker, MD National Coordinator for Health
June 25, 2018 Ms. Seema Verma Administrator Centers for Medicare & Medicaid Services US Department of Health and Human Services Baltimore, MD 21244-1850 Donald Rucker, MD National Coordinator for Health
Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts
 Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts May 9, 2018 www.hcttf.org 1 Speakers Jeff Micklos Executive Director HCTTF Kelly McCracken National
Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts May 9, 2018 www.hcttf.org 1 Speakers Jeff Micklos Executive Director HCTTF Kelly McCracken National
Connecting Care Across the Continuum
 Connecting Care Across the Continuum A Guide for Providers > Discharging patients should be quick, easy, and painless for everyone including patients, families and the hospital. That s why a hospital that
Connecting Care Across the Continuum A Guide for Providers > Discharging patients should be quick, easy, and painless for everyone including patients, families and the hospital. That s why a hospital that
Care Redesign and Population Health
 Care Redesign and Population Health Care Redesign Amendment At stakeholder request, we asked CMS to approve an amendment to our All-Payer Model (Model) to obtain comprehensive patient level Medicare data
Care Redesign and Population Health Care Redesign Amendment At stakeholder request, we asked CMS to approve an amendment to our All-Payer Model (Model) to obtain comprehensive patient level Medicare data
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12
 New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
2017 TPCA Conference Schedule (subject to change)
") Day 1: Wednesday, Boot Camps 2017 TPCA Conference Schedule (subject to change) Time Session Title Speaker(s) Description 9:00am 3:00pm Boot Camp 1: HR Boot Camp Ann Hogan This 3hour interactive facilitated
Day 1: Wednesday, Boot Camps 2017 TPCA Conference Schedule (subject to change) Time Session Title Speaker(s) Description 9:00am 3:00pm Boot Camp 1: HR Boot Camp Ann Hogan This 3hour interactive facilitated
DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request
 DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request Webinar: Monday, October 5, 2015 Time: 1:30pm-3:00pm Presented by Suffolk Care Collaborative (SCC) Suffolk County Performing
DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request Webinar: Monday, October 5, 2015 Time: 1:30pm-3:00pm Presented by Suffolk Care Collaborative (SCC) Suffolk County Performing
Quanum Electronic Health Record Frequently Asked Questions
 Quanum Electronic Health Record Frequently Asked Questions Table of Contents... 4 What is Quanum EHR?... 4 What are the current capabilities of Quanum EHR?... 4 Is Quanum EHR an EMR?... 5 Can I have Quanum
Quanum Electronic Health Record Frequently Asked Questions Table of Contents... 4 What is Quanum EHR?... 4 What are the current capabilities of Quanum EHR?... 4 Is Quanum EHR an EMR?... 5 Can I have Quanum
Market Trends and Practical Examples
 Market Trends and Practical Examples Disclaimer 2017 General Electric Company The results expressed in this document may not be applicable to a particular site or installation and individual results may
Market Trends and Practical Examples Disclaimer 2017 General Electric Company The results expressed in this document may not be applicable to a particular site or installation and individual results may
How to Improve HEDIS Reporting Among Providers and Improve Your Health Plan Rankings
 How to Improve HEDIS Reporting Among Providers and Improve Your Health Plan Rankings Introduction In today s value-focused market, health plan rankings, such as those calculated by the National Committee
How to Improve HEDIS Reporting Among Providers and Improve Your Health Plan Rankings Introduction In today s value-focused market, health plan rankings, such as those calculated by the National Committee
AccessHealth Spartanburg
 TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
producing an ROI with a PCMH
 REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
Care Compact Guide Patient-Centered Specialty Care (PCSC) A Component of Medical Neighborhood Initiatives
 A Component of Medical Neighborhood Initiatives") Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013
 GE Healthcare Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013 Centricity Electronic Medical Record DOC0886165 Rev 13 2013 General Electric Company - All rights
GE Healthcare Using Centricity Electronic Medical Record Meaningful Use Reports Version 9.5 January 2013 Centricity Electronic Medical Record DOC0886165 Rev 13 2013 General Electric Company - All rights
Moving HIT and Meaningful Use
 Moving HIT and Meaningful Use Tim Gutshall, MD March 30, 2011 EHR Adoption in Iowa Less than 50 percent of Iowa physicians have adopted EHRs As late as 2009, 89 percent of Iowa s hospitals still used some
Moving HIT and Meaningful Use Tim Gutshall, MD March 30, 2011 EHR Adoption in Iowa Less than 50 percent of Iowa physicians have adopted EHRs As late as 2009, 89 percent of Iowa s hospitals still used some
2014, Healthcare Intelligence Network
 Note: This is an authorized excerpt from 2014 Healthcare Benchmarks: The Patient-Centered Medical Home. To download the entire report, go to http://store.hin.com/product.asp?itemid=4832 or call 888-446-3530.
Note: This is an authorized excerpt from 2014 Healthcare Benchmarks: The Patient-Centered Medical Home. To download the entire report, go to http://store.hin.com/product.asp?itemid=4832 or call 888-446-3530.
Medicare Total Cost of Care Reporting
 Issue Brief Medicare Total Cost of Care Reporting True health care transformation requires access to clear and consistent data. Three regions are working together to develop reporting that is as consistent
Issue Brief Medicare Total Cost of Care Reporting True health care transformation requires access to clear and consistent data. Three regions are working together to develop reporting that is as consistent
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination
 Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
MIPS Improvement Activities:
 MIPS Improvement Activities: Quality Insights Tips, Tools & Support March 14, 2017 Maureen Kelsey, MA, Quality Insights, Practice Integration Task Lead MIPS in 2017 A MIPS score is calculated by adding
MIPS Improvement Activities: Quality Insights Tips, Tools & Support March 14, 2017 Maureen Kelsey, MA, Quality Insights, Practice Integration Task Lead MIPS in 2017 A MIPS score is calculated by adding
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards
 and the NCQA PCMH 2011 Standards") Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
How to Approach Data Collection and Evaluation in SBHCs
 How to Approach Data Collection and Evaluation in SBHCs California School Health Centers Association Annual Conference March 15, 2013 Presenters: Serena Clayton PhD, Executive Director, California School
How to Approach Data Collection and Evaluation in SBHCs California School Health Centers Association Annual Conference March 15, 2013 Presenters: Serena Clayton PhD, Executive Director, California School
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework
 The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
August 8, :00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell
 August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
How an ACO Provides and Arranges for the Best Patient Care Using Clinical and Operational Analytics
 Success Story How an ACO Provides and Arranges for the Best Patient Care Using Clinical and Operational Analytics HEALTHCARE ORGANIZATION Accountable Care Organization (ACO) TOP RESULTS Clinical and operational
Success Story How an ACO Provides and Arranges for the Best Patient Care Using Clinical and Operational Analytics HEALTHCARE ORGANIZATION Accountable Care Organization (ACO) TOP RESULTS Clinical and operational
ACCOUNTABLE CARE: ROADMAP TO VALUE
 ACCOUNTABLE CARE: ROADMAP TO VALUE Perspective The adoption of Accountable Care and value-based reimbursement has dramatically increased these past several years. New organizations are being established
ACCOUNTABLE CARE: ROADMAP TO VALUE Perspective The adoption of Accountable Care and value-based reimbursement has dramatically increased these past several years. New organizations are being established
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
Learning Objectives INDUSTRY BEST PRACTICES 3/5/2014. Be Ready for ICD-10 Best Practices for Educating Coders. Learn industry best practices for:
 Be Ready for ICD-10 Best Practices for Educating Coders Mary Pat Jackey BSN, RN Clinical Educator Commonwealth Health Corporation Bowling Green, KY Michelle Leavitt Director, Learning Solutions HealthcareSource
Be Ready for ICD-10 Best Practices for Educating Coders Mary Pat Jackey BSN, RN Clinical Educator Commonwealth Health Corporation Bowling Green, KY Michelle Leavitt Director, Learning Solutions HealthcareSource
Mary Pat Jackey BSN, RN Clinical Educator Commonwealth Health Corporation Bowling Green, KY. Learning Objectives. Learn industry best practices for:
 Be Ready for ICD-10 Best Practices for Educating Coders Mary Pat Jackey BSN, RN Clinical Educator Commonwealth Health Corporation Bowling Green, KY Michelle Leavitt Director, Learning Solutions HealthcareSource
Be Ready for ICD-10 Best Practices for Educating Coders Mary Pat Jackey BSN, RN Clinical Educator Commonwealth Health Corporation Bowling Green, KY Michelle Leavitt Director, Learning Solutions HealthcareSource
Patient-Centered. Medical Homes (Presentation Handout)
") Patient-Centered Medical Homes (Presentation Handout) Presented to AFC SPC, 3/14/13 by Barbara Schechtman, MPH 1 What is a PCMH? From the March 2007 Joint Principles of the PCMH: AAP, American Academy
Patient-Centered Medical Homes (Presentation Handout) Presented to AFC SPC, 3/14/13 by Barbara Schechtman, MPH 1 What is a PCMH? From the March 2007 Joint Principles of the PCMH: AAP, American Academy
An Overview of Eligibility, Registration, and Attestation for the Medicare & Medicaid EHR Incentive Programs Eligible Professionals
 An Overview of Eligibility, Registration, and Attestation for the Medicare & Medicaid EHR Incentive Programs Eligible Professionals Jon Langmead 10/31/2011 Centers for Medicare & Medicaid Services 1 Eligible
An Overview of Eligibility, Registration, and Attestation for the Medicare & Medicaid EHR Incentive Programs Eligible Professionals Jon Langmead 10/31/2011 Centers for Medicare & Medicaid Services 1 Eligible
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
State Innovation Model
 State Innovation Model 1 Context: Centers for Medicare and Medicaid Services Payment Reform Targets Planned percentage of Medicare FFS payments linked to quality and alternative payment models 2016 2018
State Innovation Model 1 Context: Centers for Medicare and Medicaid Services Payment Reform Targets Planned percentage of Medicare FFS payments linked to quality and alternative payment models 2016 2018
EHR for the PCMH A Doctor s Perspective. Medical Home Summit
 EHR for the PCMH A Doctor s Perspective Medical Home Summit Salvatore Volpe MD FAAP FACP CHCQM www.svolpemd.com March 15, 2011 Learning Objectives Why I adopted an EHR My experience: what I needed to do
EHR for the PCMH A Doctor s Perspective Medical Home Summit Salvatore Volpe MD FAAP FACP CHCQM www.svolpemd.com March 15, 2011 Learning Objectives Why I adopted an EHR My experience: what I needed to do
Catalog of Value-Based Payment (VBP) Resources July 2017
 Resources July 2017") Catalog of Value-Based Payment (VBP) Resources July 2017 Table of Contents I. Overview: Defining VBP and the Rationale for Moving to VBP (p. 2) a. Health Care Payment Learning and Action Network Website
Catalog of Value-Based Payment (VBP) Resources July 2017 Table of Contents I. Overview: Defining VBP and the Rationale for Moving to VBP (p. 2) a. Health Care Payment Learning and Action Network Website
Quality of Life Conversation On Advance Care Planning
 Quality of Life Conversation On Advance Care Planning Information Packet Page 1 About the Integrated Healthcare Association The nonprofit Integrated Healthcare Association (IHA) convenes diverse stakeholders,
Quality of Life Conversation On Advance Care Planning Information Packet Page 1 About the Integrated Healthcare Association The nonprofit Integrated Healthcare Association (IHA) convenes diverse stakeholders,
NY State initiatives for Primary Care Practices: CPC plus - Webinar
 NY State initiatives for Primary Care Practices: CPC plus - Webinar Marcus Friedrich, MD, MBA, FACP Medical Director NYSDOH - Office of Quality and Patient Safety August 30, 2016 August 30, 2016 2 Primary
NY State initiatives for Primary Care Practices: CPC plus - Webinar Marcus Friedrich, MD, MBA, FACP Medical Director NYSDOH - Office of Quality and Patient Safety August 30, 2016 August 30, 2016 2 Primary
Adirondack Medical Home Pilot Overview. Dennis Weaver MD MBA November 2, 2010
 Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Population Health. Collaborative Care. One interoperable platform. NextGen Care
 Population Health. Collaborative Care. One interoperable platform. NextGen Care We ve become very proactive in identifying at-risk patients and getting them in our door before they get sick. Our physicians
Population Health. Collaborative Care. One interoperable platform. NextGen Care We ve become very proactive in identifying at-risk patients and getting them in our door before they get sick. Our physicians
INNAUGURAL LAUNCH MAIN SOURCE OF PHILOSOPHY, APPROACH, VALUES FOR FOUNDATION
 FOUNDATION PHILOSOPHY DOCUMENT SEPTEMBER 29, 2015 INNAUGURAL LAUNCH MAIN SOURCE OF PHILOSOPHY, APPROACH, VALUES FOR FOUNDATION Foundation Philosophy TABLE OF CONTENTS 1) Introduction a. Foundation Approach
FOUNDATION PHILOSOPHY DOCUMENT SEPTEMBER 29, 2015 INNAUGURAL LAUNCH MAIN SOURCE OF PHILOSOPHY, APPROACH, VALUES FOR FOUNDATION Foundation Philosophy TABLE OF CONTENTS 1) Introduction a. Foundation Approach
What is a Pathways HUB?
 What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
The Michigan Primary Care Transformation (MiPCT) Project: December PGIP Meeting Update. MiPCT Team December 2, 2011
 Project: December PGIP Meeting Update. MiPCT Team December 2, 2011") 1 The Michigan Primary Care Transformation (MiPCT) Project: December PGIP Meeting Update MiPCT Team December 2, 2011 2 Agenda Introduction MiPCT Participation Care Management Update Funding Update MiPCT
1 The Michigan Primary Care Transformation (MiPCT) Project: December PGIP Meeting Update MiPCT Team December 2, 2011 2 Agenda Introduction MiPCT Participation Care Management Update Funding Update MiPCT
MACRA, MIPS, and APMs What to Expect from all these Acronyms?!
 MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
Practice Transformation Networks
 Practice Transformation Networks The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U. S. Department of Health & Human Services, Centers for Medicare and Medicaid
Practice Transformation Networks The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U. S. Department of Health & Human Services, Centers for Medicare and Medicaid
elearning 5.6 Curriculum Guide >> Knowledge Base Module (KBM) Workflows - 7.8
 Workflows - 7.8") elearning 5.6 Curriculum Guide >> Knowledge Base Module (KBM) Workflows - 7.8 Table of Contents This document is for informational purposes only. You cannot launch elearning courses from this page. v5.6
elearning 5.6 Curriculum Guide >> Knowledge Base Module (KBM) Workflows - 7.8 Table of Contents This document is for informational purposes only. You cannot launch elearning courses from this page. v5.6
Health System Transformation Overview of Health Systems Transformation in New York State. July 23, 2015
 Health System Transformation Overview of Health Systems Transformation in New York State July 23, 2015 2 The Vision Healthier New Yorkers (population health) Lower costs Engaged consumers Systems, programs,
Health System Transformation Overview of Health Systems Transformation in New York State July 23, 2015 2 The Vision Healthier New Yorkers (population health) Lower costs Engaged consumers Systems, programs,
OPNS Suite of Products Opportunities Contact OPNS Informatics Department
 EMR/e-Rx Practice Fusion EMR/e-Rx Advanced MD Health Connect Health Connect OPNS Preferred Suite of Products OPNS Suite of Products Opportunities Contact OPNS Informatics Department OPNS Middle Range Suite
EMR/e-Rx Practice Fusion EMR/e-Rx Advanced MD Health Connect Health Connect OPNS Preferred Suite of Products OPNS Suite of Products Opportunities Contact OPNS Informatics Department OPNS Middle Range Suite
Integrated Leadership for Hospitals and Health Systems: Principles for Success
 Integrated Leadership for Hospitals and Health Systems: Principles for Success In the current healthcare environment, there are many forces, both internal and external, that require some physicians and
Integrated Leadership for Hospitals and Health Systems: Principles for Success In the current healthcare environment, there are many forces, both internal and external, that require some physicians and
Advisory Board Fellows
 Talent Development Advisory Board Fellows Delivering impact through a signature initiative Talent Development s marquee leadership program, the Advisory Board Fellowship, is an accelerated two-year, MBA-like
Talent Development Advisory Board Fellows Delivering impact through a signature initiative Talent Development s marquee leadership program, the Advisory Board Fellowship, is an accelerated two-year, MBA-like
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
SUCCESSES OF VIRGINIA S SIM DESIGN
 SUCCESSES OF VIRGINIA S SIM DESIGN SIM Structure Process + Strategy Convened hundreds of stakeholders from all regions and constituencies to develop solutions to some of our most complex health care challenges.
SUCCESSES OF VIRGINIA S SIM DESIGN SIM Structure Process + Strategy Convened hundreds of stakeholders from all regions and constituencies to develop solutions to some of our most complex health care challenges.
Medicaid Electronic Health Record (EHR) Incentive Program: A Webinar for Eligible Professionals
 Incentive Program: A Webinar for Eligible Professionals") Medicaid Electronic Health Record (EHR) Incentive Program: A Webinar for Eligible Professionals Presenters Ivy Bela, HHSC Leo Gutierrez, TMHP Craig Earls, CGI Wendy Wacasey, NTREC February 3, 2011 1 Overview
Medicaid Electronic Health Record (EHR) Incentive Program: A Webinar for Eligible Professionals Presenters Ivy Bela, HHSC Leo Gutierrez, TMHP Craig Earls, CGI Wendy Wacasey, NTREC February 3, 2011 1 Overview
IMPORTANT! Some sections of this article require you have appropriate security clearance to things like the System Manger.
 Author: Joel Kristenson Last Updated: 2015-09-04 Overview This article is primarily for our nonprofit customers, but does contain useful information related to log notes and pivot reports for political
Author: Joel Kristenson Last Updated: 2015-09-04 Overview This article is primarily for our nonprofit customers, but does contain useful information related to log notes and pivot reports for political
DY3 PP1 Contracting Webinar. Mount Sinai PPS (DSRIP) August 2017
 August 2017") DY3 PP1 Contracting Webinar Mount Sinai PPS (DSRIP) August 2017 Introductions Nina Bastian Associate Director, Operations Mount Sinai Ashley Fitch Senior Project Manager Mount Sinai Jocelyn Levine Data
DY3 PP1 Contracting Webinar Mount Sinai PPS (DSRIP) August 2017 Introductions Nina Bastian Associate Director, Operations Mount Sinai Ashley Fitch Senior Project Manager Mount Sinai Jocelyn Levine Data
Meaningful Use for Eligible Providers. Session Four: ARRA Meaningful Use Reporting, Registration, and Attestation
 Meaningful Use for Eligible Providers Session Four: ARRA Meaningful Use Reporting, Registration, and Attestation Session Revisions April 21, 2011 Slide 10: Updated to reflect clarification on number of
Meaningful Use for Eligible Providers Session Four: ARRA Meaningful Use Reporting, Registration, and Attestation Session Revisions April 21, 2011 Slide 10: Updated to reflect clarification on number of
Chapter 11. Expanding Roles and Functions of the Health Information Management and Health Informatics Professional
 Chapter 11 Expanding Roles and Functions of the Health Information Management and Health Informatics Professional 11-2 Learning Outcomes When you finish this chapter, you will be able to: 11.1 Discuss
Chapter 11 Expanding Roles and Functions of the Health Information Management and Health Informatics Professional 11-2 Learning Outcomes When you finish this chapter, you will be able to: 11.1 Discuss