MA Medical Society Boston, MA May 6, Christine A. Sinsky, MD, FACP Vice President, Professional Satisfaction American Medical Association
|
|
|
- Roderick Jayson Bell
- 6 years ago
- Views:
Transcription


1 In Search of Joy in Practice MA Medical Society Boston, MA May 6, 2016 Christine A. Sinsky, MD, FACP Vice President, Professional Satisfaction American Medical Association Prescription for Reducing Physician Burnout MA Medical Society Boston, MA May 6, 2016 Christine A. Sinsky, MD, FACP Vice President, Professional Satisfaction American Medical Association 1
 They are trying to apply Joy in Practice to their dept practices ACP Shattuck lecture: sponsored by NEJM at lunch; Sustaining Joy in the")
2 Agenda Introduction: Framing thoughts burnout Studies AMA Rand: Physician Career Satisfaction ABIMF: In Search of Joy in Practice Notes Dr. Dennis Dimitri, president MMS (family physician, U Mass) They are trying to apply Joy in Practice to their dept practices ACP Shattuck lecture: sponsored by NEJM at lunch; Sustaining Joy in the Practice of Medicine 8-12:15 Bridget Duffy Kavita Patel, Brookings: research on efforts to create systems for pt care; CEO of Hitachi Fnd rec d her, working on teams and workforce; for neighborhood health centers to provide entry level work for residents Jeff Cain, Chair AAFP; Chair of Fam Med at Denver Childrens; speak of patients experience from his own severe illness Presentation Synergy without overlap 2
3 Agenda Introduction: Framing thoughts burnout Studies AMA Rand: Physician Career Satisfaction ABIMF: In Search of Joy in Practice Discussion Quadruple Aim 3

4 On a recent visit to a new doctor I believe we made eye contact twice upon her arriving and leaving. And yet, I am much more able to receive advice From people I feel are thinking of me as a person rather than just the next patient. and Andie Dominick in Patient Listening: A Doctor s Guide, Loreen Herwaldt 4


5 Mayo Clin Proceed 2015 Over ½ of MDs Burned Out EHR Mayo Clin Proc 2015 More than ½ of MDs Burned Out General Internal Medicine Family Medicine Work induced syndrome Chaos Lack of control Reg burdens Unsupportive leadership 5
6 Mayo Clin Proc 2015 Physician Burnout Rising 46 54% Mayo Clin Proc 2015 Physician Burnout Rising 46 54% 28% gen l pop Students start med school w/stronger mental health profiles 6
7 Mayo Clin Proc 2015 Physician Burnout Rising 46 54% Mayo Clin Proc 2015 Physician Burnout Rising 46 54% 28% gen l pop Students start med school w/stronger mental health profiles 7


8 Arch Intern Med 2012; E1-9 WLB Gen l Pop, MDs 8

9 By Specialty By Specialty High WLB, Low Burnout GIM Low WLB, High Burnout Burnout affects Patients Physician burnout is associated with o Mistakes o Adherence o Less empathy o Patient satisfaction Sources: Dyrbye. JAMA 2011;305: ; Murray, Montgomery, Chang, et al. J Gen Intern Med 2001;16: ; Landon, Reschovsky, Pham, Blumenthal. Med Care 2006;44:
10 Why does burnout matter? Burnout Costs Organizations Physician burnout is associated with o Malpractice risk o Part time o MD and staff turnover Replace PCP costs $250,000 o (1999) Am J Man Care Nov 1999:5(11): Am J Man Care Jul 2001;7(7): Health Serv. Res. Oct 2004;39(5): Med. Care Mar 2006;44(3): Journal of Applied Psychology, Vol 73(4) Nov 1988, Burnout May Cost US Healthcare Physician burnout is associated with o Referrals o Fewer PCPs Bright Spotters: PCPs o 58% total expenditures o $300 billion/yr savings rson%20center%20on%20healthcare_stanford%20overview.pdf Social Science and Medicine 1999; (48): Family Practice doi: /fampra/cmt060. Arch Intern Med. 2011;171(17):
11 Satisfied clinicians work longer, retire later, are more productive, have better quality ratings, and have high quality metrics. Burnout Costs Physicians Physician burnout is associated with o Disruptive behavior o Divorce o CAD o Substance abuse/addiction o Suicide (2-4 x) 11
:547-557 Family Practice doi:10.1093/fampra/cmt060.")
12 Burnout May Cost US Healthcare o Referrals o Fewer PCPs Milstein:Exemplar Primary Care o 58% total expenditures o $300 billion/yr savings rson%20center%20on%20healthcare_stanford%20overview.pdf Social Science and Medicine 1999; (48): Family Practice doi: /fampra/cmt060. Arch Intern Med. 2011;171(17): in 2 US physicians burned out implies origins are rooted in the environment and care delivery system rather than in the personal characteristics of a few susceptible individuals. 12
13 Physician Career Satisfaction Quality: Major Driver of Satisfaction Physician Career Satisfaction EHR: Major Driver of Dissatisfaction Too much time per task, clerical Face-to-face time Quality of visit note Burnout: Work induced syndrome Environmental barriers Q Reg burdens Insurers don t cover necessary care Unsupportive leadership 13


14 CMS Andy Slavitt, says MU will be over in /11/16 We have to get the hearts and minds of physicians back. I think we ve lost them. Receptionist Billing Clerk Transcriptionist Medical Records Clerk Pharmacist 14

15 Pajama Time 1-2 hr/nig ht Weekend nights Week nights In Search of Joy in Practice Co-Investigators Christine Sinsky- PI Tom Bodenheimer-PI Rachel Willard Tom Sinsky Andrew Schutzbank David Margolius 15


16 Places Where PC Physicians & Staff are Thriving? Where the work of primary care is do-able Enjoyable as a life s vocation 16
17 Group Health Olympia Joy in Practice Martin s Point- Evergreen Woods Multnomah County Health Dept Allina Fairview Rosemont Clinic Mayo Red Cedar ThedaCare Harvard Vanguard Medford Brigham and Women s Hospital Clinic Ole Sebastopol Community Health La Clinica la Raza de Univ of Utah- Redstone Clinica Family Health Services Medical Center Medical Associates Clinic Mercy Clinics Quincy, Office of the Future Cleveland Clinic- Strongsville North Shore Physicians Group Mass. General Hospital Newport News Family Practice West Los Angeles- VA South Central Foundation Site visits to 23 highperforming practices (most PCMHs) Workflow Task distribution Physical space Technology Challenges Chaotic visits EHR work to MD Inadequate support Teams function poorly Time documentation 17
 61% additional visits (p<0.001) 21% tests ordered (p<0.0001) patient satisfaction Saved $26/visit Crocker B, Lewandrowski E, Lewandrowski N, Gregory K, Lewandrowski K.")
18 Challenges Innovations 1. Chaotic visits with overfull agendas Pre-visit planning Pre-appt labs Systematic Prescriptions Pre-visit Labs 89% phone calls (p<0.001) 85% letters (p<0.0001) 61% additional visits (p<0.001) 21% tests ordered (p<0.0001) patient satisfaction Saved $26/visit Crocker B, Lewandrowski E, Lewandrowski N, Gregory K, Lewandrowski K. Patient Satisfaction With Point-of-Care Laboratory Testing: Report of a Quality Improvement Program in an Ambulatory Practice of an Academic Medical Center. Clin Chem Acta 2013; 424:8-12.; and personal communication/poster
19 Annual Prescription Renewals Physician time 0.5 hr/d Nursing time 1 hr/d per physician Annual Prescription Renewals Physician time 0.5 hr/d Nursing time 1 hr/d per physician 40 million PC visits/yr 200,000 PCPs x 220d/yr x1 visit/d 19
20 Script Renewal Calls $10,000/yr per MD Surescripts estimate as reported in WSJ (Similar to our observation of 1 RN: 6-8 MDs) Each call costs $15-20 Challenges Action Innovations Steps 1. Chaotic visits with overfull agendas Insurers Single co-pay lab/visit Institutions Hold future orders Regulatory Prescription 15 mo 20

21 Challenges 2. Inadequate support to meet the patient demand for care Innovations Sharing the care among the team 2:1 or 3:1 Rooming protocol Between visit Challenges 2. Inadequate support to meet the patient demand for care Health coaching Care coordination Panel mgm t Innovations Action Steps Educators MA, nurse: MI, SMS Institutions/Regulators Staffing Scope of practice Payers Fund non-md services 21

22 Challenges Innovations 3. Vast amounts of time spent documenting care Team documentation Assistant order entry I used to be a doctor. Now I am a typist. Personal communication. Beth Kohnen, MD, internist Fairbanks, AK

23 I am no longer a physician but the data manager, data entry clerk and steno girl. I am frustrated, unhappy and I am unable to do my best in caring for my patients. I became a doctor to take care of patients. I have become the typist. physician, Boston 2013 Challenges Innovations 3. Vast amounts of time spent documenting care Team documentation Assistant order entry 23

24 Team Documentation Newport News What we all hoped for Team: 3:1 I used to spend an hour or two in the evening after my family went to bed completing my charts for the day. I haven t logged on from home in so long, I ve forgotten how to use the remote access system. Kevin Hopkins M.D. 24
25 Pre-visit (nurse) Med Rec Agenda, HPI Visit (nurse + MD) Team Documentation Cleveland Clinic med,lab, x-ray orders followup Post-visit (nurse) Reviews visit summary Health coaching MD next patient Team Documentation Cleveland Clinic New Model 2 MA: 1 MD 2 pt/d cover cost visits/d 30% revenue Spread to others We re having FUN 25
26 The MA s are more fully engaged in patient care than they have ever been and they enjoy their work They have increased knowledge about medical care in general and about their individual patients in particular. Kevin Hopkins M.D. We have turned the EHR into an ally rather that an adversary. James Jerzak, M.D. Bellin Health personal communication
27 Our CMAs and LPNs do the computer work, including order entry, refills, care gap closures, and team documentation. The physicians and advanced practice clinicians are able to focus totally on the patient during the entire visit. James Jerzak, M.D. Bellin Health personal communication OLD MODEL OF PATIENT CARE Paper Work Medication Refill Chronic Disease Management Test Results Acute Visits Preventative Visits Patient Orders/Triage PROVIDER Referral to Ancillary Services CMA/ LPN RN Referral to Specialist Managing Messages, Test Results, Calling Patients 54 27
 Breast Screening Baseline 55.37% Goal (6 months) 58.13% Actual 59.51% Financial Metrics (operating margin for Dr.")
28 Team Documentation Bellin Health Green Bay New Model 2 MA: 1 RN: 1 MD Extended care team prevention metrics chronic ill. metrics in margin staff/md satisfaction Bellin Results Quality Metrics (screenings) Breast Screening Baseline 55.37% Goal (6 months) 58.13% Actual 59.51% Financial Metrics (operating margin for Dr. Jerzak) Baseline negative 2.2% Goal negative 1.2% YTD Actual positive 6.1% Cervical Screening Baseline 69.61% Goal (6 months) 73.09% Actual 78.64% Colorectal Screening Baseline 79.41% Goal (6 months) % Actual- 83.5% 28
29 Team Documentation Bellin Health Green Bay How satisfied are you in your role? Pre Post Very 42% 0% Dissatisfied/D issatisfied Neutral 24% 14% Satisfied/Very Satisfied 34% 86% Google Glass Pilot Palo Alto Medical Foundation 10 internists x 1 yr video (wear glasses) or audio (around neck) Physicians are delighted as takes away an average of 2 hours of documentation time per day 95% charts closed 2-5 minutes after visit 97% patient acceptance Cost: $25,000/MD/yr (1/3 cost of MA) Source: GPIN newsletter


30 I get to look at my patients and talk with them again. We re reconnecting. Our patient satisfaction numbers are up, our quality metrics have improved, our nurses are contributing more, and I am going home an hour earlier to be with my family.. Amy Haupert MD, family physician, Allina-Cambridge personal communication Team Documentation Kaukauna, WI 4 weeks/year 2 MA: 1LPN: 1 MD 2 pt/d cover cost visits/d 30% revenue 30

31 I have seen 235 more patients in the first 6 months (the equivalent of 4 additional weeks of patient care), I have more that paid for the additional RN...and I have actually had time to do some fun reading. In brief, I have done more, billed more, dictated less, have more face time with patients, and my family gets to see me. a great change for me. Michael Werner M.D family physician, Kaukauna WI, personal communication Team Documentation UCLA UCLA: saves 3 hr/d JAMA IM


32 Innovation Team Documentation UCLA Physician Partners Scripts/COE Charting/Charge JAMA IM 5.14 Pt satisfaction w/md time Save 1.5 hr/4hr Training Academy Team Documentation Six sites Similar results Access 20-30% Costs covered Satisfaction Quality metrics Physician home hour earlier no work at home 32
33 Business Case Panel 4000 patients Clinic A 1:1 4 $250k $1,000,000 4 $50k 200,000 $1,200,000 Clinic B 3:1 2 MDs = 500,000 6 MAs 300,000 $ 800,000 Save $400,000 per 4000 patients (+ Happier docs, staff, pts, better recruitment, retention) Business Case Panel 4000 patients Clinic A 1:1 4 $250k $1,000,000 4 $50k 200,000 $1,200,000 Clinic B 3:1 2 MDs = 500,000 6 $75k 450,000 $ 950,000 Save $250,000 per 4000 patients (+ Happier docs, staff, pts, better recruitment, retention) 33


34 Assistant Order Entry U Alabama GIM Positive deviant 2015 ACGLIM survey of 20 GIM depts Productivity 16% wrvu/session Work-life balance Notes completed in clinic 0% 43% Weekend charting 86% 57% Marked reduction in burnout 34

35 I feel like I m taking better care of my patients because I m not doing everything. 35

36 The miracle of scribes is that I rediscovered what I didn t even know I had lost the beauty of reconnection with my patients. It is so much fun. I haven t had fun in the clinic in years. Mark Linzer, MD General internist, Hennepin County, MN personal communication 36


37 Challenges Action Innovations Steps 3. Vast amounts of time spent documenting care Regulatory Team log-in Meaningful Use Stage 2 Institutions Staffing ratios Assistant order entry Technology Seamless transitions between users Guidance/Legislation/EHRIncentivePrograms/downloads/Stage2_EPCore_1_CPOE_Medicatio norders.pdf 37
38 Challenges Innovations 4. Computerized technology that pushes more work to the clinician Verbal messages In-box management The worklist is unbearable. I spend 1.5 hours clearing out my worklist before leaving and another 1.5 hours at home after the kids go to bed. Primary Care Physician, Des Moines, IA;

39 Challenges Innovations 4. Computerized technology that pushes more work to the clinician Verbal messages Inbox management Dean Clinic RFID Sign On Tap and Go 73 signs to 2 sign ins per day Saved 14 min/d 39
40 Challenges Action Innovations Steps 4. Computerized technology that pushes more work to the clinician Institutions message generation Nurses filter inbox Regulators Modifications to accommodate teamwork Technology Improved usability Team-based design Challenges Innovations 5. Teams that function poorly and complicate rather than simplify the work Co-location Huddles Team meetings Workflow mapping 40
41 Dean Clinic RFID Sign On Tap and Go 73 signs to 2 sign ins per day Saved 14 min/d Challenges Action Innovations Steps 5. Teams that function poorly and complicate rather than simplify the work Institutions Co-location Line of sight Space for huddles Time for meetings 41
 2 wk family")

42 Observations from 23 Teaching Practices Across the US Clinic First Small 23 core primary faculty (40 10 care MDs for 4 FTE) 2 wk family scheduling medicine, blocks Stable internal team pairings medicine, Sufficient staff and pediatric Engage residents in transformation residency practices 42




43 Transformation Toolkits Teams Expanded rooming Team documentation Prescription management Pre-visit planning/lab Team meetings Daily huddles Value Panel management Medication adherence Burnout Prevention Diabetes prevention Hypertension Culture Preventing Burnout Resiliency Wellness in Residency Transforming culture Technology Telemedicine EHR implementation 43


44 44

45 45



46 QI Metrics 91 PROCESS MAP TOOLKIT 46
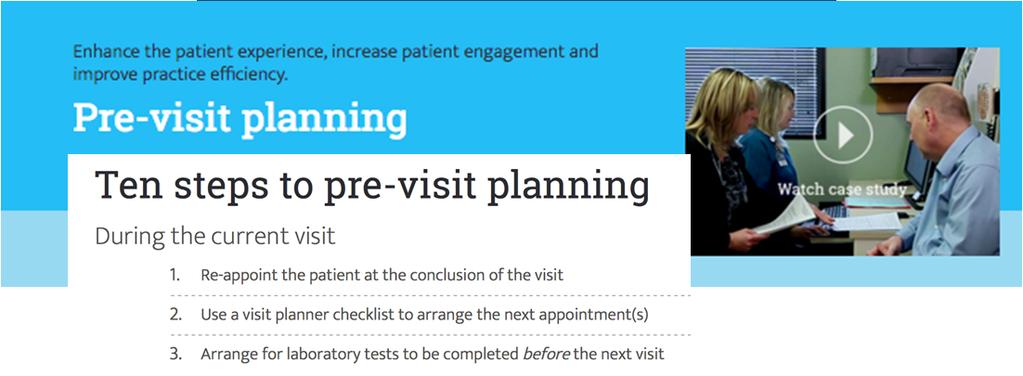
47 PRE-VISIT PLANNING DURING THE CURRENT VISIT Patient is at the office for their current visit Receptionist schedules followup appointment(s) for the patient before they leave the office Does the patient need to have any lab work or other diagnostics done before their next appointment? Yes Use a visit planner checklist to arrange next appointment(s) Medical assistant orders labs based on standing orders Medical assistant schedules labs to be completed before the next appointment No BEFORE THE NEXT VISIT Medical assistant performs visit preparations: Reviews notes from prior visit and confirms that documentation from interval care or hospitalizations has been obtained Prints copies of lab results and other important results to discuss at visit Use a visit prep checklist to identify gaps in care, such as immunizations or cancer screenings. If something needs to be scheduled before the upcoming visit, contact the patient to schedule the appointment Send patients appointment reminders, either automatically or manually Is the patient considered complex? Yes Consider a pre-visit phone call or to begin medication reconciliation, set the patient agenda and perform other preparations to ensure that the visit is thorough and efficient Patient has pre-visit labs completed No DURING THE NEXT VISIT Hold a pre-clinic care team huddle to prepare the team for the day ahead and anticipate any patient needs Receptionist hands out a pre-appointment questionnaire to each patient at check-in Medical assistant rooms patient and updates patient record based on information on pre-visit questionnaire, conducts medication reconciliation and sets visit agenda with patient Hand off the patient to the physician, informing them of the purpose of the patient s visit as well as any important information learned during rooming Physician portion of visit begins. Pre-visit planning commences at the current visit Terminal point Process Decision WAIT TIME PROCESS Patient arrives at FLOW clinic Are additional diagnostics required in the office? No Patient services representative (PSR) gives patient paperwork for review & signature and takes patient s insurance card & ID After completing paperwork, patient waits for available PSR to complete check-in Patient waits while physician works with medical assistants & nurses to obtain information Yes Patient leaves clinic PSR collects copay and returns cards to patient, completing check-in Medical assistant takes patient back on first ready basis, takes vitals & updates history and completes medication reconciliation Patient waits for medical assistant Patient waits for physician to enter & start visit Yes No Patient waits while physician works with medical assistants & nurses to place and validate orders Diagnostic test is completed Patient receives referrals, orders, after-visit summary and instructions, schedules follow-up appointments as necessary and completes check-out Patient has encounter with physician Additional documents required? Diagnostic tests, labs and/or outside records? Patient waits for physician to return with results Patient waits for available PSR in check-out area Patient discusses plan of care with physician Terminal point Process Delay Decision Improvement opportunities 47

48 MOST COMMON PROCESS MAP SYMBOLS Which symbols should you use? Most process maps can be created using a few basic flowchart symbols. Here are some common symbols and their meanings. To create your own map, copy and paste these symbols into a new slide. Process represents a step or activity in your process. Terminal points indicate the starting or ending points of a process. Delay represents a waiting period where no value-added activity takes place. Decision indicates a point where the outcome of a decision dictates the next step. There can be multiple outcomes, but often there are just two - yes and no. Document represents a step that requires or results in a document. Kaizen bursts indicate improvement opportunities. Preparation indicates an action that helps prepare for the next step in the process. Manual operation indicates an operation or adjustment to the process that can be made manually. CONNECTORS Connectors are lines that link different flowchart symbols. Once placed, connectors will stay connected to the symbols they are linked to. Move linked symbols and their connecters will automatically reorient with them. Solid lines are used to connect the flowchart symbols. Dotted lines indicate an alternate process. Arrow on both ends indicates that the process flow can move in either direction between the two steps. Arrow on one end indicates the direction of the process flow. Swim lanes can be used to delineate roles and responsibilities within your practice. Lanes can be arranged horizontally or vertically. See EXAMPLE 2 for swim lane element. 48


49 Rooming Checklist 98 49


50 Making the business case 50


51 Team Documentation Checkback 2011 APF: pt centered, team-based and mindful of care team well being. The biggest difference -- is team, culture and time. Time with patients to better understand who they are, their story Ben Crocker, MD Internist MGH I wouldn't trade that for anything. I'm loving it. 51



52 Our Work Going Forward How can we contribute to transformation Working in clinic is unbearable Entrusted and empowered by tech, team, policy I m loving it Quadruple Aim 52

53 What patients want is that deep relationship with a healer; this is the foundation upon which we need to build healthcare. Paul Grundy, MD IBM, PCPCC personal communication The Map is not the Territory "If you didn't document it, it didn't happen," Fresh ears are told in medical school. But then one day we realize that documenting doing doesn t make it so, Experiencing makes it so. 53


54 "Visited patient in her basement. Ascites worsening as she drinks more after death of son in motor vehicle accident." What more should I write? How do you document bearing witness? The Code is not the Care The Pocket Guide: It folds like origami and reads like computer code, this item we received early in residency. In small font and syllogism, It tells us what our time with a patient is worth. It sustains anachronisms like the review of systems. Three chronic conditions is the key that opens a Level 4 lock. 54

55 Now we hear these notes are being poorly done. They have too much. They have too little. They don t have the right elements. Doctors need better education. They need more detailed notes. We also hear there is burnout. Access problems for patients. People leaving primary care or not entering it. We hear EHRs are good. We hear they are bad. Why don t we start at the beginning? The care of the patient is what matters most. The map is not the terrain. The code is not the care. Colleagues have left practice Unable to keep up with the note-production complex. Charting encroaches on caring. This is what happens when a means for recording meaning is alchemized into a tool for billing, a means for monitoring, a line of defense. 55


56 The patient-doctor conversation becomes an act of distraction, lapsed eye-contact, and keyboard tapping. This is pawn activity. Finishing a patient session becomes prelude to converting it into billable accounts. We rush. Patients notice. The map is not the territory. The code is not the care. Doctors got to where we are because we follow rules well. What to do then, when the rules erode our doctoring? The map is not the territory. The code is not the care. 56
57

58 Quadruple Aim the most refine, most expensive and most important clinical instrument in our health system continues to be the physician. 58
59 The most refined, most expensive, and most important clinical instrument in our health system continues to be the physician. Stanford Dean s report 2015 Business Case Burnout doubles likelihood MD leave (Stanford) ( may cost $1 million ) 59

 Worker is over trained for the")



60 Calculus: wrong work burnout Conceptual Model: Matching Work to Worker Y Worker is under trained for the work Unsafe Complexity of work Sweet spot: worker and work are well matched Inefficient (Waste) Worker is over trained for the task X Modified from A. Mulley Training Current Work Distribution in PC High value Good match Solution Shop Dx and Rx plan Complex chronic Relationship bldg Shared decision making Complexity of work PAs Vitals Script renewals Production Line MA RN RN NP PA MD Training Inbox mgmt Med rec Script renewals Data entry Data gathering Prior authorization Sign for hearing aid battery 60





61 In few other sectors of the economy is the highest-level professional responsible for the majority of production, customer service, and clerical work. SGIM Blue Ribbon Panel Report. Redesigning the Practice Model for General Internal Medicine: A Proposal for Coordinated Care. J Gen Intern Med 2007;22: Matching Work to Worker Bio/psycho/social Shared decision m Chronic illness ca E/M acute sx Complexity of work Vitals Allows greater MD focus on high complexity Inbox mgmt tasks Med rec Script renewals Data entry Data gathering Prior authorization Sign for hearing a MA RN RN NP PA MD Training 61
62 4000 Clicks 6 clicks to order an aspirin 8 clicks to order a CXR 15 clicks for one prescription 40 clicks to record hand and wrist exam >40% of ER shift on data entry Am J Emerg Med 2014;31(11): data EHR actions per visit Impact-of-Electronic-Health-Record-Use-on-Physician-Productivity Higher level of EHR use over time did not reflect doing more work, but doing more documentation of the work done. 62

63 10 hours of charting for 6.8 hours of scheduled 63


64 A Day in the Life of Dr. Jones Blue: MA computer time Green: MD computer time Each row is a patient 2.5 hours of after hours charting PCP: Paperwork Completing Physician? The Doctor must be the one to fill out the entire 7 Element order, a member of the staff can no longer fill out any portion. 64
65 Why does burnout matter? Burnout Costs Organizations Physician burnout is associated with o Malpractice risk o Part time o MD and staff turnover Replace PCP costs $250,000 o (1999) Am J Man Care Nov 1999:5(11): Am J Man Care Jul 2001;7(7): Health Serv. Res. Oct 2004;39(5): Med. Care Mar 2006;44(3): Journal of Applied Psychology, Vol 73(4) Nov 1988,
Joy in Practice: Innovations in Patient Centered Care. Association of Chiefs and Leaders of GIM Christine A Sinsky, MD, FACP Feb 17, :40-4:40
 Joy in Practice: Innovations in Patient Centered Care Association of Chiefs and Leaders of GIM Christine A Sinsky, MD, FACP Feb 17, 2016 3:40-4:40 Agenda Introduction: Framing thoughts burnout Studies
Joy in Practice: Innovations in Patient Centered Care Association of Chiefs and Leaders of GIM Christine A Sinsky, MD, FACP Feb 17, 2016 3:40-4:40 Agenda Introduction: Framing thoughts burnout Studies
In Search of Joy in Practice: Innovations in Patient Centered Care
 In Search of Joy in Practice: Innovations in Patient Centered Care Pri-Med Annual Conference Rosemont, IL Christine A Sinsky, MD, FACP Thomas A Sinsky, MD, FACP Oct 18, 2013 Agenda Introduction: Framing
In Search of Joy in Practice: Innovations in Patient Centered Care Pri-Med Annual Conference Rosemont, IL Christine A Sinsky, MD, FACP Thomas A Sinsky, MD, FACP Oct 18, 2013 Agenda Introduction: Framing
Primary Care Innovations: Stories from the Field. PCPCC Webinar Christine A Sinsky, MD Thomas A. Sinsky, MD June 29, 2012
 Primary Care Innovations: Stories from the Field PCPCC Webinar Christine A Sinsky, MD Thomas A. Sinsky, MD June 29, 2012 In Search of Joy in Practice Co-Investigators Christine Sinsky- PI Tom Bodenheimer-PI
Primary Care Innovations: Stories from the Field PCPCC Webinar Christine A Sinsky, MD Thomas A. Sinsky, MD June 29, 2012 In Search of Joy in Practice Co-Investigators Christine Sinsky- PI Tom Bodenheimer-PI
Solving the adult primary care crisis: it s time to think differently
 Solving the adult primary care crisis: it s time to think differently Thomas Bodenheimer MD, MPH Center for Excellence in Primary Care (CEPC) UCSF Department of Family and Community Medicine Presenter
Solving the adult primary care crisis: it s time to think differently Thomas Bodenheimer MD, MPH Center for Excellence in Primary Care (CEPC) UCSF Department of Family and Community Medicine Presenter
Effective Strategies for Engaging and Retaining Clients in HIV Care and Treatment. Lessons Learned from Teams in Primary Care Settings
 Effective Strategies for Engaging and Retaining Clients in HIV Care and Treatment Lessons Learned from Teams in Primary Care Settings Effective Strategies for Engaging and Retaining Clients in HIV Care
Effective Strategies for Engaging and Retaining Clients in HIV Care and Treatment Lessons Learned from Teams in Primary Care Settings Effective Strategies for Engaging and Retaining Clients in HIV Care
Family Physician Well-Being: Update for the North Dakota AFP
 Family Physician Well-Being: Update for the North Dakota AFP November 11, 2017 Clif Knight, MD, CPE, FAAFP Senior Vice President for Education Cknight@AAFP.org @ClifKnight @4FPWB The AAFP will assist members
Family Physician Well-Being: Update for the North Dakota AFP November 11, 2017 Clif Knight, MD, CPE, FAAFP Senior Vice President for Education Cknight@AAFP.org @ClifKnight @4FPWB The AAFP will assist members
Resilience Strategies for Team Care THOMAS BODENHEIMER MD, MPH CENTER FOR EXCELLENCE IN PRIMARY CARE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO
 Resilience Strategies for Team Care THOMAS BODENHEIMER MD, MPH CENTER FOR EXCELLENCE IN PRIMARY CARE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Upon completion of this educational activity, participants will
Resilience Strategies for Team Care THOMAS BODENHEIMER MD, MPH CENTER FOR EXCELLENCE IN PRIMARY CARE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Upon completion of this educational activity, participants will
Why pay attention to burnout. The ACLGIM Worklife and Wellness Survey. Strategies for reducing burnout and promoting wellness in GIM
 Mark Linzer, MD Office of Professional Worklife Hennepin County Medical Center Why pay attention to burnout Burnout research The ACLGIM Worklife and Wellness Survey Review of the data Strategies for reducing
Mark Linzer, MD Office of Professional Worklife Hennepin County Medical Center Why pay attention to burnout Burnout research The ACLGIM Worklife and Wellness Survey Review of the data Strategies for reducing
Mark Linzer MD General Internal Medicine Office of Professional Worklife Hennepin County Medical Center
 Mark Linzer MD General Internal Medicine Office of Professional Worklife Hennepin County Medical Center No financial conflicts Research supported by Agency for Healthcare Research and Quality Partnering
Mark Linzer MD General Internal Medicine Office of Professional Worklife Hennepin County Medical Center No financial conflicts Research supported by Agency for Healthcare Research and Quality Partnering
Joy At Work - BellinHealth and HealthPartners
 Joy At Work - BellinHealth and HealthPartners Restoring Joy in Practice through Team Based Care IHI December 2016 James Jerzak M.D. Kathy Kerscher Bellin Health Green Bay, Wisconsin 1 Agenda Crisis Emerging
Joy At Work - BellinHealth and HealthPartners Restoring Joy in Practice through Team Based Care IHI December 2016 James Jerzak M.D. Kathy Kerscher Bellin Health Green Bay, Wisconsin 1 Agenda Crisis Emerging
Team-based Care: Answering the Call in Academic Medicine. Scott Shipman, MD, MPH Director of Primary Care Affairs and Workforce Analysis
 Team-based Care: Answering the Call in Academic Medicine Scott Shipman, MD, MPH Director of Primary Care Affairs and Workforce Analysis West Michigan Interprofessional Education Initiative, Sept 19, 2014
Team-based Care: Answering the Call in Academic Medicine Scott Shipman, MD, MPH Director of Primary Care Affairs and Workforce Analysis West Michigan Interprofessional Education Initiative, Sept 19, 2014
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
The True Cost of the Burnt Out Physician. Lisa Ellis, MD, FACP Chief Medical Officer- VCU Health Ambulatory Clinics
 The True Cost of the Burnt Out Physician Lisa Ellis, MD, FACP Chief Medical Officer- VCU Health Ambulatory Clinics DISCLOSURES/DISCLAIMERS I have no conflicts of interest 2 The True Cost a Burnt Out Physician
The True Cost of the Burnt Out Physician Lisa Ellis, MD, FACP Chief Medical Officer- VCU Health Ambulatory Clinics DISCLOSURES/DISCLAIMERS I have no conflicts of interest 2 The True Cost a Burnt Out Physician
Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP)
 & Patient-Centered Specialty Practice (PCSP)") Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP) Foundation for a Better Health Care System Presenter Jeanette Ikan, M.D., MHAI Objectives: Definition and benefits of PCMH,
Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP) Foundation for a Better Health Care System Presenter Jeanette Ikan, M.D., MHAI Objectives: Definition and benefits of PCMH,
Rethinking the model of primary care. Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine
 Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
The Quadruple Aim: Enduring Values for Changing Times. Kathleen Blake, MD, MPH Vice President, Healthcare Quality May 5, 2017
 The Quadruple Aim: Enduring Values for Changing Times Kathleen Blake, MD, MPH Vice President, Healthcare Quality May 5, 2017 AMA s Mission Promote the art and science of medicine and the betterment of
The Quadruple Aim: Enduring Values for Changing Times Kathleen Blake, MD, MPH Vice President, Healthcare Quality May 5, 2017 AMA s Mission Promote the art and science of medicine and the betterment of
Optimizing the Workforce: The Intersection of Healthcare Reform, Delivery Innovation, and Training
 Optimizing the Workforce: The Intersection of Healthcare Reform, Delivery Innovation, and Training Scott Shipman, MD, MPH Director of Primary Care Affairs Baldwin Series Lecture November 2017 Scott Shipman,
Optimizing the Workforce: The Intersection of Healthcare Reform, Delivery Innovation, and Training Scott Shipman, MD, MPH Director of Primary Care Affairs Baldwin Series Lecture November 2017 Scott Shipman,
Oregon Medical Group Team Medicine 3 April 2014
 Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Overview of The Joint Commission s Primary Care Medical Home (PCMH) Certification
 Certification") Overview of The Joint Commission s Primary Care Medical Home (PCMH) Certification Joyce Webb, RN, MBA Project Director, Standards and Survey Methods Program Lead, The Joint Commission s PCMH Initiative
Overview of The Joint Commission s Primary Care Medical Home (PCMH) Certification Joyce Webb, RN, MBA Project Director, Standards and Survey Methods Program Lead, The Joint Commission s PCMH Initiative
Joy in Medicine Physician well-being: A discussion on burnout and achieving joy in practice
 Joy in Medicine Physician well-being: A discussion on burnout and achieving joy in practice AMA s SL2 (Share, Listen, Speak, Learn) Series December 2017 Share, Listen, Speak, Learn (SL2) Series Share existing
Joy in Medicine Physician well-being: A discussion on burnout and achieving joy in practice AMA s SL2 (Share, Listen, Speak, Learn) Series December 2017 Share, Listen, Speak, Learn (SL2) Series Share existing
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Implementation and Impact of Lean Redesigns in Primary Care
 Implementation and Impact of Lean Redesigns in Primary Care June 6, 2017 Lean Healthcare Research Symposium Lean Transformation in Health Care Summit Dorothy Hung, Ph.D., M.A., M.P..H. Palo Alto Medical
Implementation and Impact of Lean Redesigns in Primary Care June 6, 2017 Lean Healthcare Research Symposium Lean Transformation in Health Care Summit Dorothy Hung, Ph.D., M.A., M.P..H. Palo Alto Medical
Bright Spots in primary care
 Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
University of California, Davis Family Practice Center: Update 2014
 University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
NCQA s Patient-Centered Medical Home Recognition and Beyond. Tricia Marine Barrett, VP Product Development
 NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Achieving Population Health through Team Based Care
 Achieving Population Health through Team Based Care Wisconsin Council on Medical Education and Workforce Conference November 12, 2015 Kathy Kerscher, Bellin Health Overview of Bellin Health 3 MISSION Bellin
Achieving Population Health through Team Based Care Wisconsin Council on Medical Education and Workforce Conference November 12, 2015 Kathy Kerscher, Bellin Health Overview of Bellin Health 3 MISSION Bellin
Presbyterian Healthcare Services Care Management
 Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Expanded Rooming and Discharge Protocols
 Expanded Rooming and Discharge Protocols Empower staff to make patient visits more meaningful and efficient. AMA IN PARTNERSHIP WITH CME CREDITS: 0.5 Christine Sinsky, MD Vice President, Professional Satisfaction,
Expanded Rooming and Discharge Protocols Empower staff to make patient visits more meaningful and efficient. AMA IN PARTNERSHIP WITH CME CREDITS: 0.5 Christine Sinsky, MD Vice President, Professional Satisfaction,
Monthly PCMH/HH Webinar. The Use of Scribes in the Patient Centered Medical Home
 Monthly PCMH/HH Webinar The Use of Scribes in the Patient Centered Medical Home Wednesday, March 26, 2014 7:30AM & 4:30PM Tel. 866.740.1260, ID: 2520060# Important Webinar Notes To minimize background
Monthly PCMH/HH Webinar The Use of Scribes in the Patient Centered Medical Home Wednesday, March 26, 2014 7:30AM & 4:30PM Tel. 866.740.1260, ID: 2520060# Important Webinar Notes To minimize background
August 8, :00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell
 August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
11/7/2016. Objectives. Patient-Centered Medical Home
 Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Future of the Health Care Workforce: Where are we going? May 23, 2018
 Future of the Health Care Workforce: Where are we going? May 23, 2018 Setting the Context Source: Various, AMA 2 Projected physician shortfall of between 42,600 and 121,300 Source: 2018 Update - The Complexities
Future of the Health Care Workforce: Where are we going? May 23, 2018 Setting the Context Source: Various, AMA 2 Projected physician shortfall of between 42,600 and 121,300 Source: 2018 Update - The Complexities
Empowering Medical Assistants Improves Primary Care
 Empowering Medical Assistants Improves Primary Care By: Jessica Langley, MS, Executive Director of Education and Provider Markets, National Healthcareer Association Running a healthcare practice presents
Empowering Medical Assistants Improves Primary Care By: Jessica Langley, MS, Executive Director of Education and Provider Markets, National Healthcareer Association Running a healthcare practice presents
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
VENICE FAMILY CLINIC: Improving capacity and managing patient lead times
 CASE STUDY, 4/12 VENICE FAMILY CLINIC: Improving capacity and managing patient lead times PREPARED BY Professor Kumar Rajaram, UCLA Anderson School of Management Karen Conner, MD, UCLA David Geffen School
CASE STUDY, 4/12 VENICE FAMILY CLINIC: Improving capacity and managing patient lead times PREPARED BY Professor Kumar Rajaram, UCLA Anderson School of Management Karen Conner, MD, UCLA David Geffen School
PALLIATIVE CARE NURSE PRACTITIONER
 PALLIATIVE CARE NURSE PRACTITIONER Responsible to Regional Director of Palliative Care with dotted line to Medical Director Description The Nurse Practitioner (NP) works independently and in collaboration
PALLIATIVE CARE NURSE PRACTITIONER Responsible to Regional Director of Palliative Care with dotted line to Medical Director Description The Nurse Practitioner (NP) works independently and in collaboration
Deeper Dive on Team Roles: Part 2
 Deeper Dive on Team Roles: Part 2 Moderator: Nicole Van Borkulo, MEd, Qualis Health Speakers: Catherine Dower, JD, Associate Director of Research, Susan Chapman, PhD, RN, and Lisel Blash, Senior Research
Deeper Dive on Team Roles: Part 2 Moderator: Nicole Van Borkulo, MEd, Qualis Health Speakers: Catherine Dower, JD, Associate Director of Research, Susan Chapman, PhD, RN, and Lisel Blash, Senior Research
Adopting a patient pre-registration process
 Adopting a patient pre-registration process Learn how a streamlined pre-registration process can save time for your patients and your practice. CME CREDITS: 0.5 Douglas K. Diehl, MD Asante Physician Brandon
Adopting a patient pre-registration process Learn how a streamlined pre-registration process can save time for your patients and your practice. CME CREDITS: 0.5 Douglas K. Diehl, MD Asante Physician Brandon
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff
 Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Presentation Outline
 Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Advanced Medical Homes: Bending the Trend. Alan Glaseroff, MD Co-Director Stanford Coordinated Care
 Advanced Medical Homes: Bending the Trend Alan Glaseroff, MD Co-Director Stanford Coordinated Care aglasero@stanford.edu 1 Hot Spotting in Employed Populations 1. Humboldt County, CA : Priority Care Partnered
Advanced Medical Homes: Bending the Trend Alan Glaseroff, MD Co-Director Stanford Coordinated Care aglasero@stanford.edu 1 Hot Spotting in Employed Populations 1. Humboldt County, CA : Priority Care Partnered
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Please stand by. There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1
 Please stand by There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1 Webinar Tips Today s webinar is a one-way audio broadcast through
Please stand by There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1 Webinar Tips Today s webinar is a one-way audio broadcast through
Using a Patient-Centered Care Plan and Teamwork to Support Self-Management
 Using a Patient-Centered Care Plan and Teamwork to Support Self-Management Speakers: Larry Mauksch, MEd, Senior lecturer and licensed mental health counselor, UW Department of Family Medicine; and Berdi
Using a Patient-Centered Care Plan and Teamwork to Support Self-Management Speakers: Larry Mauksch, MEd, Senior lecturer and licensed mental health counselor, UW Department of Family Medicine; and Berdi
Health Reform and The Patient-Centered Medical Home
 THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
Welcome to BCHC Your Medical Home
 START HERE 1 Welcome to BCHC Your Medical Home Thank you for choosing Berks Community Health Center (BCHC) as your medical home. This booklet gives you information about being a patient at BCHC and what
START HERE 1 Welcome to BCHC Your Medical Home Thank you for choosing Berks Community Health Center (BCHC) as your medical home. This booklet gives you information about being a patient at BCHC and what
Topic 4A: Foundational Changes Reducing Barriers to Care Webinar
 The Patient-centered Medical Home Webinar #4 Topic 4A: Foundational Changes Reducing Barriers to Care Webinar Ed Wagner, MD, MPH, MACP MacColl Center for Health Care Innovation Group Health Research Institute
The Patient-centered Medical Home Webinar #4 Topic 4A: Foundational Changes Reducing Barriers to Care Webinar Ed Wagner, MD, MPH, MACP MacColl Center for Health Care Innovation Group Health Research Institute
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION
 UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
New Models of Care: Diabetes and the Triple Aim
 Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Primary Care Meets Population Health: The Parable of Preventable Hospitalizations
 Department of Family & Community Medicine University of California, San Francisco Primary Care Meets Population Health: The Parable of Preventable Hospitalizations Kevin Grumbach, MD Duke Department of
Department of Family & Community Medicine University of California, San Francisco Primary Care Meets Population Health: The Parable of Preventable Hospitalizations Kevin Grumbach, MD Duke Department of
MAKING PROGRESS, SEEING RESULTS
 MAKING PROGRESS, SEEING RESULTS VALUE-BASED CARE REPORT HUMANA.COM/VALUEBASEDCARE Y0040_GCHK4DYEN 1117 Accepted 2 Americans are sick and getting sicker, with millions of us living with chronic conditions
MAKING PROGRESS, SEEING RESULTS VALUE-BASED CARE REPORT HUMANA.COM/VALUEBASEDCARE Y0040_GCHK4DYEN 1117 Accepted 2 Americans are sick and getting sicker, with millions of us living with chronic conditions
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases?
 Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases? Providing care for long-term cancer survivors? Managing depression?
Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases? Providing care for long-term cancer survivors? Managing depression?
Driving Business Value for Healthcare Through Unified Communications
 Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
Appendix 6. PCMH 2014 Summary of Changes
 Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Moving beyond burnout to professional engagement and joy. Martina Schulte, MD February 10, 2018
 Moving beyond burnout to professional engagement and joy Martina Schulte, MD February 10, 2018 Disclosures: None Can we use the word joy? Don Berwick, MD 2017 Perlo. IHI Framework for Improving Joy in
Moving beyond burnout to professional engagement and joy Martina Schulte, MD February 10, 2018 Disclosures: None Can we use the word joy? Don Berwick, MD 2017 Perlo. IHI Framework for Improving Joy in
Care Coordination Overview. Janet Tennison, PhD UPV Standards October 8, 2013
 Care Coordination Overview Janet Tennison, PhD UPV Standards October 8, 2013 What IS Care Coordination? The deliberate, proactive organization of patient care activities between two or more participants
Care Coordination Overview Janet Tennison, PhD UPV Standards October 8, 2013 What IS Care Coordination? The deliberate, proactive organization of patient care activities between two or more participants
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project
 Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
Team Integration Strategies
 Team Integration Strategies Making the Change to Team-Based Care Melissa Schoen, Schoen Consulting Cindy Barr, Capital Link Advancing the Financial Strength of L.A. County Clinics February 10, 2017 1 Dividing
Team Integration Strategies Making the Change to Team-Based Care Melissa Schoen, Schoen Consulting Cindy Barr, Capital Link Advancing the Financial Strength of L.A. County Clinics February 10, 2017 1 Dividing
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016
 ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
An Implementation Framework for Patient Safety in Ambulatory Care. To disseminate key findings from IHI s work on ambulatory safety
 An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Primary Care Redesign Updates to DFM
 Primary Care Redesign Updates to DFM Overview of Care Model Package 2 Care of the Complicated Patient March 5, 2014 Dr. Rich Welnick Susan Marks, Director of Population Health Lori Hauschild, Clinic Operations
Primary Care Redesign Updates to DFM Overview of Care Model Package 2 Care of the Complicated Patient March 5, 2014 Dr. Rich Welnick Susan Marks, Director of Population Health Lori Hauschild, Clinic Operations
Health Information Technology
 ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
Achieving Operational Excellence with an EHR a CIO s Perspective
 Achieving Operational Excellence with an EHR a CIO s Perspective Phyllis Schuck, SPHR CIO of Pinehurst Surgical HIT Session 6.02 Thursday, March 29, 2007 Pinehurst Surgical Organization Overview Founded
Achieving Operational Excellence with an EHR a CIO s Perspective Phyllis Schuck, SPHR CIO of Pinehurst Surgical HIT Session 6.02 Thursday, March 29, 2007 Pinehurst Surgical Organization Overview Founded
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
The Medical Neighborhood: Ensuring Continuity of Care with Hospital and Specialist Neighborhoods
 The Medical Neighborhood: Ensuring Continuity of Care with Hospital and Specialist Neighborhoods R. Scott Hammond MD, FAAFP Chair, CAFP PCMH Task Force Medical Director, SOC-PCMH Initiative, Colorado Associate
The Medical Neighborhood: Ensuring Continuity of Care with Hospital and Specialist Neighborhoods R. Scott Hammond MD, FAAFP Chair, CAFP PCMH Task Force Medical Director, SOC-PCMH Initiative, Colorado Associate
The Role of Medication Management in a Patient-Centered Medical Home
 The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
SCRIBES, SMAS AND INCIDENT T0
 SCRIBES, SMAS AND INCIDENT T0 Andrew R. McCulllough, MD In Transit Objectives Convince you to: Use Scribes Use Shared Medical Appointments Stop using Incident To The Facts of Life as a Physician Burnout
SCRIBES, SMAS AND INCIDENT T0 Andrew R. McCulllough, MD In Transit Objectives Convince you to: Use Scribes Use Shared Medical Appointments Stop using Incident To The Facts of Life as a Physician Burnout
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Burnout Among Health Care Professionals
 Burnout Among Health Care Professionals NAM Action Collaborative on Clinician Well-being and Resilience Research, Data, and Metrics Taskforce Lotte Dyrbye, MD, MHPE, FACP Professor of Medicine & Medical
Burnout Among Health Care Professionals NAM Action Collaborative on Clinician Well-being and Resilience Research, Data, and Metrics Taskforce Lotte Dyrbye, MD, MHPE, FACP Professor of Medicine & Medical
Patient Centered Medical Home
 Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Patient Care Coordination Variance Reporting
 Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
PCMH Recognition Redesign: Annual Reporting Requirements to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018
 PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
An Implementation Framework for Patient Safety in Ambulatory Care
 An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
Meaningful Use and PCC EHR. Tim Proctor Users Conference 2017
 Meaningful Use and PCC EHR Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda MU basics and eligibility How to participate in MU What s Next for MU? Meeting MU measures in PCC EHR Takeaways An understanding
Meaningful Use and PCC EHR Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda MU basics and eligibility How to participate in MU What s Next for MU? Meeting MU measures in PCC EHR Takeaways An understanding
How will this module help me successfully put team documentation in place?
 Team Documentation Spend more time caring for patients by sharing responsibilities with staff. AMA IN PARTNERSHIP WITH CME CREDITS: 0.5 Christine Sinsky, MD Vice President, Professional Satisfaction, American
Team Documentation Spend more time caring for patients by sharing responsibilities with staff. AMA IN PARTNERSHIP WITH CME CREDITS: 0.5 Christine Sinsky, MD Vice President, Professional Satisfaction, American
Physician Burnout and Distress: Causes, Consequences, and a Structure For Solutions
 Physician Burnout and Distress: Causes, Consequences, and a Structure For Solutions January 5, 2017 Presenter: Colin P. West, MD, PhD Professor of Medicine, Medical Education, and Biostatistics Division
Physician Burnout and Distress: Causes, Consequences, and a Structure For Solutions January 5, 2017 Presenter: Colin P. West, MD, PhD Professor of Medicine, Medical Education, and Biostatistics Division
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale