PATIENT-CENTERED MEDICAL HOMES: PROGRESS, NOT PERFECTION
|
|
|
- Marshall Pearson
- 5 years ago
- Views:
Transcription
1 PATIENT-CENTERED MEDICAL HOMES: PROGRESS, NOT PERFECTION J O N AT H A N G R I F F I N, M D, M H A M M A P H Y S I C I A N L E A D E R S H I P E F F E C T I V E N E S S P R O G R A M J A N U A R Y 1 6,

2 WHY PATIENT CENTERED MEDICAL HOME
3 PCMH CREATES VISION FOR CHANGE
4 Yesterday s Care My patients are those who make appointments to see me Patients chief complaints or reasons for visit determines care Care is determined by today s problem and time available today Care varies by scheduled time and memory or skill of the doctor Patients are responsible for coordinating their own care I know I deliver high quality care because I m well trained Acute care is delivered in the next available appointment and walk-ins It s up to the patient to tell us what happened to them Clinic operations center on meeting the doctor s needs Medical Home Care Our patients are those who are registered in our medical home We systematically assess all our patients health needs to plan care Care is determined by a proactive plan to meet patient needs without visits Care is standardized according to evidence-based guidelines A prepared team of professionals coordinates all patients care We measure our quality and make rapid changes to improve it Acute care is delivered by open access and non-visit contacts We track tests & consultations, and follow-up after ED & hospital A multidisciplinary team works at the top of our licenses to serve patients Slide from Daniel Duffy MD School of Community Medicine Tulsa Oklahoma
5 Yesterday s Care Care is delivered to individual patients Quality is assumed by an absence of errors The team is organized to make things flow smoothly for providers Primary care treats medical problems and refers out everything else Patients make appointments when something is wrong and the provider treats the complaint Out of sight, out of mind Medical Home Care Care is delivered to individuals and to clinical populations Quality is measured and continually improved, care is monitored against national or regional benchmarks Everyone on the team has a role in making care flow smoothly for patients Primary care treats the whole person and coordinates all services that impact health The provider and team proactively partner with a panel of patients over time Anticipate and respond to needs for prevention, acute, chronic and palliative care Slide from Daniel Duffy MD School of Community Medicine Tulsa Oklahoma
6 DON T MISTAKE ACTIVITY FOR ACHIEVEMENT Increased access does not ensure increased quality of communication Quality of interaction = real achievement Patient trust Behavior change Outcomes Satisfaction Understanding where the patient is coming from Social relationships Living situation Quality of life Goals Beliefs Understanding and beliefs about health, disease, medications
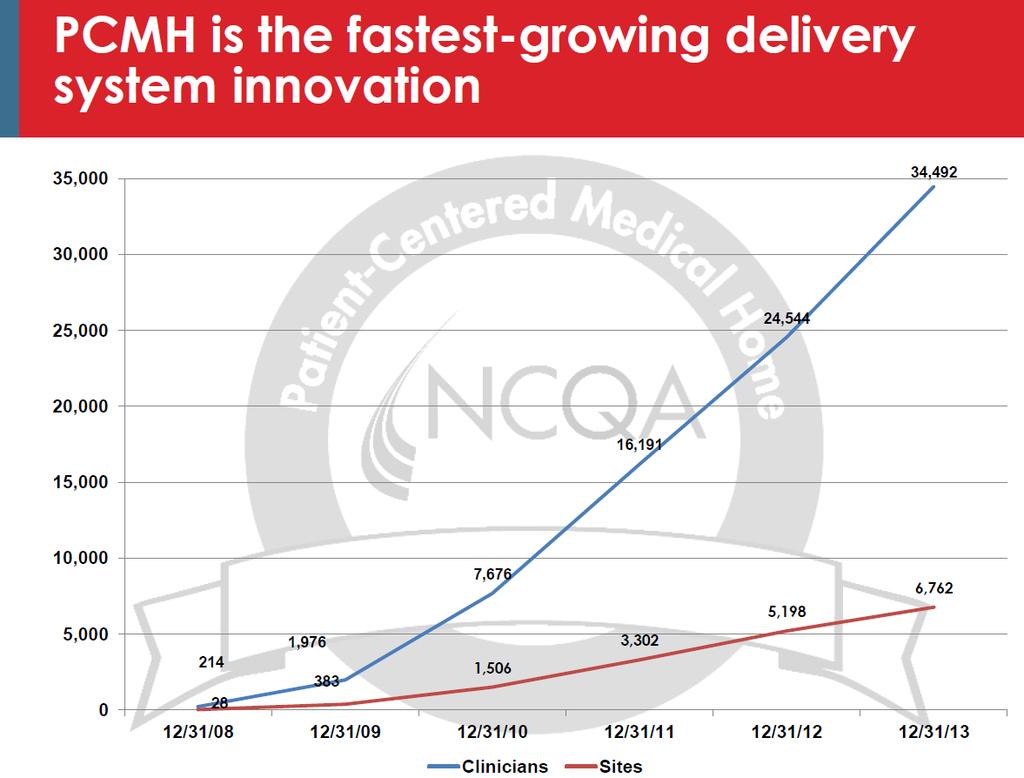
7 PCMH CREATES A FRAMEWORK FOR CHANGE

8 PCMH: FRAMEWORK FOR CHANGE
9
10

11
12 PCMH CREATES OPPORTUNITY FOR CHANGE
13
14
15
16
17
18 PCMH CREATES COMMON LANGUAGE FOR CHANGE
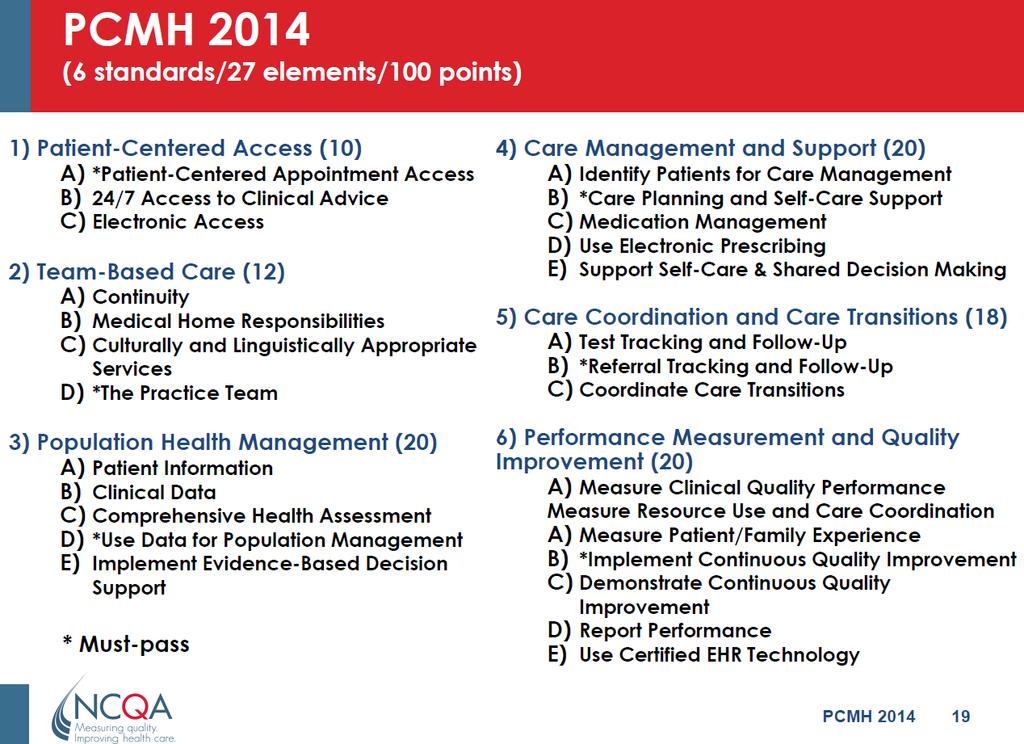
19 PCMH COMMON LANGUAGE Access to care: the ease with which a patient can initiate an interaction for any health problem with a clinician, such as through same-day appointments, clinicians answering patient s, etc. Patient engagement and self-management: the practice counsels patients to adopt healthier behaviors or learn how to better manage a chronic condition Team-based care: the primary care physician works with an interdisciplinary team to manage the patient s care, including collaboratively developing a treatment plan Comprehensiveness of care: the breadth of services the practice offers, to address any health problem at any given stage of a patient s life Continuity of care: policies that specify that patients are to be seen by the same clinician over time Coordination of care: interacting with other providers e.g., specialists and hospitals to coordinate all care delivered to the patient, including care transitions Care plan: developing an individualized treatment plan for a patient, basing this care plan on an individualized health risk assessment of the patient, etc.
20 PCMH COMMON LANGUAGE Population management: use of a registry to proactively manage care for patients with a given chronic condition Evidence-based care: use of evidence-based care guidelines, clinical decision support, etc. Quality measurement: quality is measured in some way Quality improvement: required to engage in quality improvement projects and/or set performance targets based on quality measure data collected Community resources: referrals to social services Medical records: specific types of information that should be recorded in patients medical records Health IT: when questions explicitly require the use of an electronic system, like electronic health records (EHRs), e-prescribing, an electronic patient registry, etc. Evidence-based care: very basic care processes that all clinicians should already engage in, such as physician speaks to the patient about his/her health problems and concerns
21 PCMH COMMON LANGUAGE Business practices: the financial and organizational management of the practice, such as having a business plan, analyzing the percentage of submitted claims that went unpaid, etc. Presence of policies: requiring a policy on after-hours care for patients, but not requiring that policy to provide patients with in-person access to care after-hours, sets standards for continuous quality improvement work. Empanelment/Attribution: appropriately matching patients with specific primary care physicians and organizations with implications in quality reporting and health plan PCMH payments. Compact between practice and patients: requiring practices to execute a written PCMH agreement and/or have a conversation and document it in a patient s medical record in which the practice commits to provide certain services such as care coordination and the patient agrees to some basic responsibilities Culturally competent communication: the practice provides information at an appropriate reading level for patients and in multiple languages; the practice makes available translation services, etc. Patient Centered Communication: implementing techniques such as motivational interviewing, cognitive behavioral therapy, activation and commitment therapy, etc. into everyday clinical interactions either through brief provider interventions or specialty behavioral health visits.
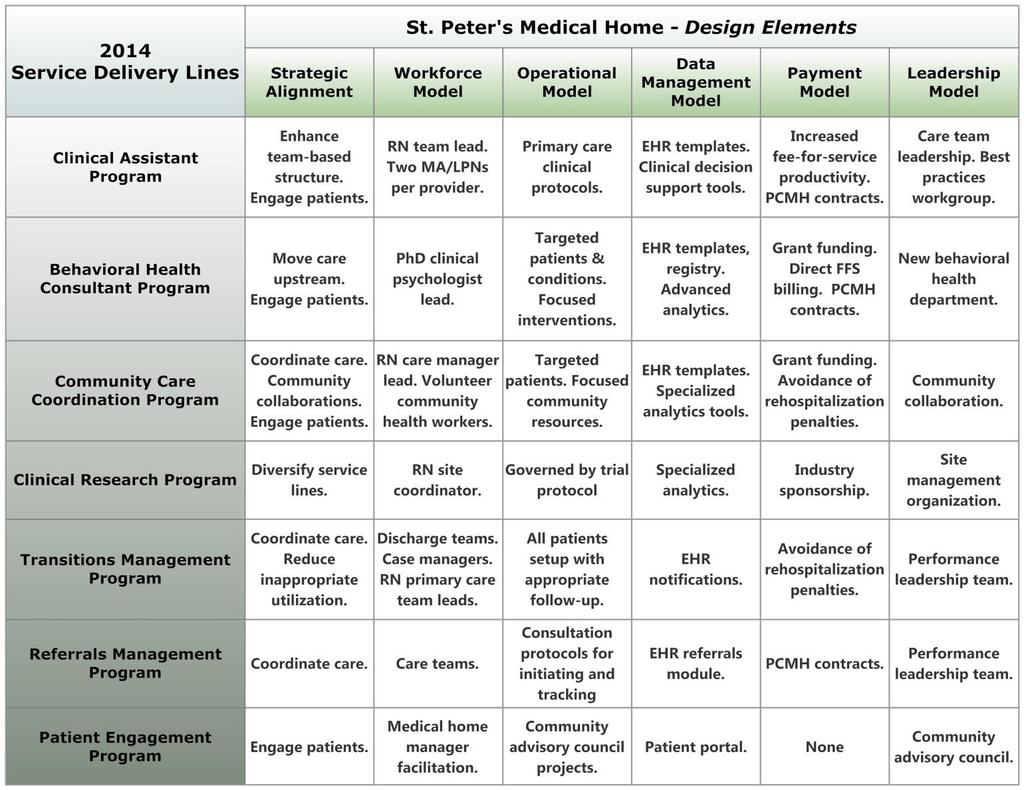
22 PATIENT CENTERED MEDICAL HOME (PCMH) A PROCESS NOT AN EVENT At both state and organizational levels

23 HOW DOES A PRACTICE BECOME A MEDICAL HOME? Change is hard enough; transformation to a PCMH requires epic whole-practice reimagination and redesign. The magnitude of stress and burden from the unrelenting, continual change required to implement components of the [PCMH] model was immense. Nutting et al. Ann Fam Med. 2009; 7: Nutting et al. Ann Fam Med. 2010; 8(Supp 1): S45-S56.
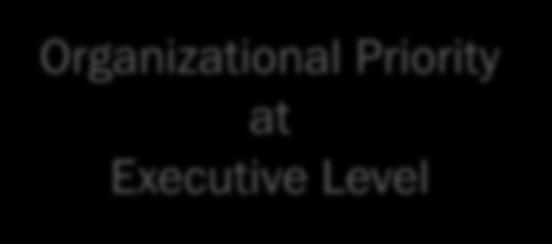
24 PCMH Critical Design Elements Making a business case Reforming payment Engaging providers Defining the medical home Supporting practice transformation TEXT TEXT Health data management & exchange Evaluating impact
25 PATIENT CENTERED PRIMARY CARE COLLABORATIVE OCT 2012 REVIEW OF 46 MEDICAL HOME INITIATIVES ACROSS THE US Alaska Native Medical Center, Anchorage, AK 50% fewer urgent care and emergency room (ER) visits 53% fewer hospital admissions 65% reduction in specialist utilization Capital Health Plan, Tallahassee, FL 40% fewer inpatient stays 37% fewer ER visits 18% lower health care claims costs Geisinger Health System, Danville, PA 25% fewer hospital admissions 50% fewer hospital readmissions 7% lower cumulative total spending Group Health of Washington, Seattle, WA 15% fewer inpatient stays 15% fewer hospital readmissions Estimated costs savings of $15 million ( ) 18-65% improvements in medication management HealthPartners, Bloomington, MN 39% fewer ER visits 40% fewer hospital readmissions Reduced appointment wait time from 26 days to 1 day Horizon Blue Cross Blue Shield of New Jersey 25% fewer hospital readmissions 21% fewer inpatient admissions 31% increase in self-management of blood sugar Maryland CareFirst Blue Cross Blue Shield 4.2% reduction in patients' overall health care costs Estimated cost savings of $40 million (2011) Vermont Medicaid 31% fewer ER visits 21% reduction in inpatient services 22% lower per member per month costs ( )
26 PATIENT CENTERED PRIMARY CARE COLLABORATIVE OCT 2012 REVIEW OF IMPROVED 46 MEDICAL HOME PATIENT INITIATIVES ACROSS EXPERIENCE THE US REDUCED CLINICIAN BURNOUT Alaska Native Medical Center, Anchorage, AK 50% fewer urgent care and emergency room (ER) visits 53% fewer hospital admissions 65% reduction in specialist utilization Capital Health Plan, Tallahassee, FL 40% fewer inpatient stays 37% fewer ER visits 18% lower health care claims costs Geisinger Health System, Danville, PA 25% fewer hospital admissions 50% fewer hospital readmissions 7% lower cumulative total spending Group Health of Washington, Seattle, WA 15% fewer inpatient stays 15% fewer hospital readmissions Estimated costs savings of $15 million ( ) 18-65% improvements in medication management HealthPartners, 39% fewer Bloomington, ER visits MN 40% fewer hospital readmissions Reduced appointment wait time from 26 days to 1 day REDUCED HOSPITALIZATION RATES REDUCED ER VISITS Horizon Blue Cross Blue Shield of New Jersey 25% fewer hospital readmissions 21% fewer inpatient admissions 31% increase in self-management of blood sugar Maryland CareFirst Blue Cross Blue Shield 4.2% reduction in patients' overall health care costs Estimated cost savings of $40 million (2011) INCREASED SAVINGS PER PATIENT HIGHER QUALITY OF CARE Vermont 31% Medicaid 21% fewer reduction ER visits in inpatient services 22% lower per member per month costs ( ) REDUCED COST OF CARE

27 PCMH LOWERS COSTS IN PENNSYLVANIA August 5 th % reduction in hospital costs 21% reduction in overall medical costs. 160 PCMH practices Pennsylvania from 2008 to 12 Number of patients with poorly controlled diabetes declined by 45%. Jeffrey Bendix modernmedicine.com/

28 PCMH LOWERS UTILIZATION IN MICHIGAN August 11 th % lower rate of adult hospitalization. 8.8% lower rate of adult ER visits. 17.7% lower rate ER visits (children under age 17) 7.3% lower rate of adult high-tech radiology usage VS non-pcmh designated PCPs 3,017 Physicians Medical home physicians help patients avoid ERs and admissions by evening hour appointments, weekend and same-day appointments

29
30 PCMH Critical Design Elements TEXT Making a business case Reforming payment Engaging providers Defining the medical home Supporting practice transformation TEXT Health data management & exchange Evaluating impact


31 ECONOMIC INCENTIVES S I G N I F I C A N T L Y I N F L U E N C E H E A L T H C A R E I N B A C K W A R D A N D C O M P L E T E L Y U N I N T E N D E D W A Y S. What s the use you learning to do right when it s troublesome to do right and ain t no trouble to do wrong, and the wages is just the same.

32 Healthcare transformation will require a step change in thinking and execution Meaningful change in clinical delivery includes the development of robust information systems, primary care platforms, adherence to clinical pathways, integrated networks, and reductions in variability.

33

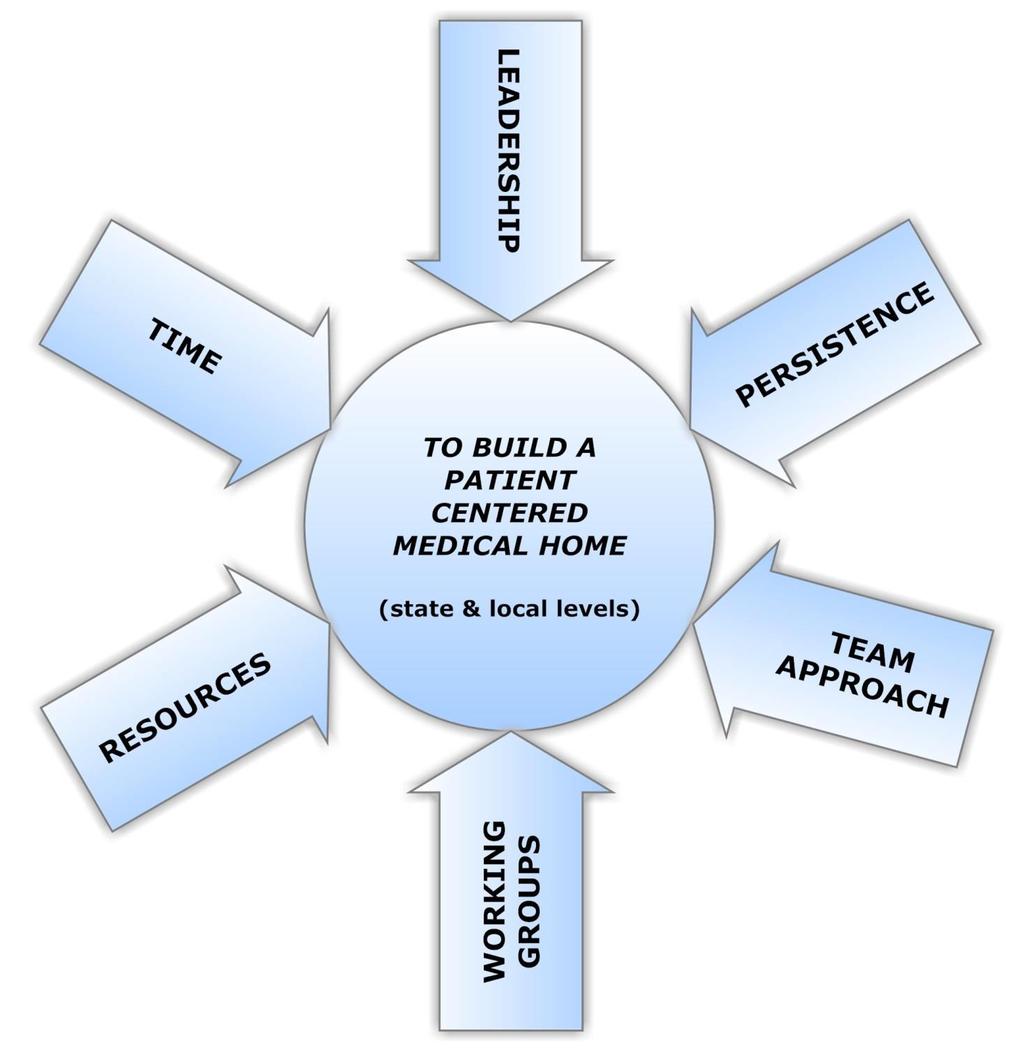
34 Managing Through the Payment Tipping Point
35
 Anti-trust protections Consistent standards Multi-stakeholder")
36 MONTANA PATIENT CENTERED MEDICAL HOME PROGRAM Legislation passed 2013 (SB-84) Anti-trust protections Consistent standards Multi-stakeholder involvement

37 WHAT DO NEW REIMBURSEMENT MODELS LOOK LIKE? Fee-for-service hybrid models Reimbursement rates declining Quality care incentivized Pay for performance Value-based purchasing Reduced cost of care incentivized Shared savings models Penalties for low quality Providers assume more risk Bundled payments Steerage Exclusivity Capitated models
38 APPROACHES TO PCMH PAYMENTS 1. Fee-for-service (FFS) with discrete new codes 2. FFS with higher payment levels 3. FFS with lump sum payments 4. FFS with PMPM fee 5. FFS with PMPM fee and with P4P 6. FFS with PMPY payment 7. FFS with PMPM fee and shared savings 8. FFS with PMPY payment and shared savings 9. FFS with at risk PMPM (per member per month) payment and shared savings 10. Comprehensive payment with P4P (pay for performance) 11. Grants

39 PAYMENT REFORM REQUIRES MORE THAN ONE METHOD. ADJUSTMENTS IN PROGRESS. fee for health fee for value fee for outcome fee for process fee for patient service fee for satisfaction Mix it up!

40 2015 *Numbers based on educated assumptions for demonstration purposes and are not precisely representative of the Montana healthcare market
41 PCMH - PAYMENT REFORM Rationale: Infrastructure support Incentive alignment Payers want to see: ROI Decreased costs Reduced utilization Ready, set, you go first
42 IN DEVELOPING OUR OWN STATE AND ORGANIZATIONAL MEDICAL HOMES, PHYSICIANS MUST BE AT THE TABLE WITH HEALTH PLANS HELPING GUIDE THE PROCESS OF PAYMENT REFORM. IT IS OUR RESPONSIBILITY TO BE ENGAGED AND TO ADVOCATE FOR OUR PATIENTS AND OUR PROFESSION.
43 PCMH Critical Design Elements TEXT Making a business case Reforming payment Engaging providers Defining the medical home Supporting practice transformation TEXT Health data management & exchange Evaluating impact
44 THE VALUE OF PHYSICIAN LEADERSHIP AT EVERY LEVEL OF THE HEALTHCARE SYSTEM I N T E R F A C E P R O F E S S I O N A L S T H E S O L E O F T H E B U S I N E S S M A T T E R S O F T R U S T R E S P E C T E D C H A N G E A G E N T S M U L T I D I S C I P L I N A R Y T E A M S T R A N S I T I O N A L H U R D L E S A D J U S T I N G T O A M B I G U I T Y P O W E R O F I N F L U E N C E N E W I N T E L L I G E N C E N E E D E D I N N O V A T I O N S I N E D U C A T I O N
45 PCMH Critical Design Elements Making a business case Reforming payment Engaging providers Defining the medical home Supporting practice transformation TEXT TEXT Health data management & exchange Evaluating impact
46

47 Organizational Priority at Executive Level

48 St. Peter s Strategic Framework and Pillars of Excellence

49 Engaged & organized Physician leadership

50 St. Peter s Provider Performance Leadership Team


51 Patientcentered interactions Expanded team roles New care team members New service lines

52 Provider Nurse MA/LPN Behavioral Health Care Manager Clinical pharmacist Social worker

53 Continuous quality improvement Patient-centered interactions Organized, evidence based care Continuous and team-based healing relationships Enhanced access Population management Care coordination

54 Data capture & aggregation Data integrity Reporting capabilities Dashboards


55 Sustainability model for all programs Creativity with payment models Active negotiations with health plans
56
57 PCMH Critical Design Elements Making a business case Reforming payment Engaging providers Defining the medical home Supporting practice transformation TEXT TEXT Health data management & exchange Evaluating impact
58
59 PRACTICE REDESIGN STRATEGIES LINKED TO RESULTS Pre-visit checklists Team huddles Using HIT to flag charts, build lists and use alerts in scheduling Bundling prevention with other visits Make it easy for the patient; reduce need to arrange multiple visits Standing orders/protocols -prevention services Create targeted quality improvement teams; for example; the Colorectal Health Team Streamline and improve process efficiency New workflows embedded in protocols, policies and new staff oriented to improved flows. New roles; navigators, population/panel management, health coaches. Regular, visible reporting of QI Transparent improvement cycles working the register aka scrubbing the list. New process for communication of lab results=standardized response to A1C abnormalities. Improving access/continuity of team.
60 SUCCESSFUL STRATEGIES Focus on real-life needs of patients nonclinical factors Transportation Social relationships Care outreach, in the home, in the community Physician engagement and change leadership Protocols for specific conditions Risk stratification focused services and resources Complex care coordination Chronic disease management
61 PCMH Critical Design Elements Making a business case TEXT Reforming payment Engaging providers Defining the medical home Supporting practice transformation TEXT Health data management & exchange Evaluating impact
62


 Care Gap")





63 PROACTIVE OUTCOMES AND PERFORMANCE IMPROVEMENT THROUGH METRICS AND REPORTING Patient Specific Data Evidence & Guideline-Based Clinical Decision Support (CDS) Care Gap Analysis Outcomes Improvements Patient Population Data Care Management Provider Reports Goal-Directed Outreach Population Management Provider Specific Data Care Team & Provider Quality Reports Operational & Financial Performance Improvement Quality Data Subsets MU, PQRS, PCMH, Metrics Reports EHR Incentive Payments & Medical Home Status
 Enhanced patient service")
64 MULTIPLE DEFINITIONS OF SUCCESS Improved chronic disease process and outcomes measures Need to allow 4 years to see differences Improved ability to capture data in EHR systems Workflow redesign to improve care of specific patient conditions or episodes of care Workflow redesign of comprehensive care planning (preventive care plus multiple chronic conditions management) Enhanced patient service manifest through experience reports, loyalty, retention Improved primary care team morale, quality of work life Increased primary care payment/revenue Patient engagement behavior change quality of life
65 A WORK IN PROGRESS THANK YOU! Jonathan Griffin, MD, MHA Family Physician VP of Medical Homes and Innovation St. Peter s Hospital & Medical Group 2550 Broadway Helena, MT O: F: C: jonsgriffin@gmail.com Chair, Montana State PCMH Advisory Council
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future
 Paul Grundy MD, MPH IBM Director, Healthcare Transformation Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future @Paul_PCPCC 2015 IBM Corporation 1 https://www.youtube.com/watch?v=uy088yyq6ua
Paul Grundy MD, MPH IBM Director, Healthcare Transformation Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future @Paul_PCPCC 2015 IBM Corporation 1 https://www.youtube.com/watch?v=uy088yyq6ua
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Building Coordinated, Patient Centered Care Management Teams
 Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Keith Salzman, M.D. Chief Medical Information Officer, IBM
 Keith Salzman, M.D. Chief Medical Information Officer, IBM Smarter Care through Transformation Keith L Salzman, MD, MPH CMIO-IBM GBS Federal keithsal@us.ibm.com USA 2012 Ogden UT IOM-The Healthcare Imperative:
Keith Salzman, M.D. Chief Medical Information Officer, IBM Smarter Care through Transformation Keith L Salzman, MD, MPH CMIO-IBM GBS Federal keithsal@us.ibm.com USA 2012 Ogden UT IOM-The Healthcare Imperative:
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
Health Care Evolution
 Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Health Information Technology
 ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services HANYS Solutions Patient-Centered Medical
 Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2015 HANYS Solutions Patient-Centered Medical Home Advisory Services Objectives After today s presentation, you will Understand how
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2015 HANYS Solutions Patient-Centered Medical Home Advisory Services Objectives After today s presentation, you will Understand how
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS
 UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Patient-Centered Medical Home Best Practices: Case Study Examples
 Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Prevea Health Automates Population Health Management and Improves Health Outcomes
 CASE STUDY Prevea Health Prevea Health Automates Population Health Management and Improves Health Outcomes After adopting the patient-centered medical home care delivery model to improve the health and
CASE STUDY Prevea Health Prevea Health Automates Population Health Management and Improves Health Outcomes After adopting the patient-centered medical home care delivery model to improve the health and
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
2014 Patient Centered Medical Home (PCMH) Recognition
 Recognition") Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A)
") SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
WELCOME. Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association
 WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Paying for Primary Care: Is There A Better Way?
 Paying for Primary Care: Is There A Better Way? Robert A. Berenson, M.D. Senior Fellow, The Urban Institute CHCS Regional Quality Improvement Initiative, Providence, R.I., July 25, 2007 1 Medicare Challenges
Paying for Primary Care: Is There A Better Way? Robert A. Berenson, M.D. Senior Fellow, The Urban Institute CHCS Regional Quality Improvement Initiative, Providence, R.I., July 25, 2007 1 Medicare Challenges
NCQA s Patient-Centered Medical Home Recognition and Beyond. Tricia Marine Barrett, VP Product Development
 NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
Population Health. Collaborative Care. One interoperable platform. NextGen Care
 Population Health. Collaborative Care. One interoperable platform. NextGen Care We ve become very proactive in identifying at-risk patients and getting them in our door before they get sick. Our physicians
Population Health. Collaborative Care. One interoperable platform. NextGen Care We ve become very proactive in identifying at-risk patients and getting them in our door before they get sick. Our physicians
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices
 Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
11/7/2016. Objectives. Patient-Centered Medical Home
 Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In?
 Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
IBM Watson Health Utica Park Clinic The need The solution The benefit
 Utica Park Clinic Population health management helps Utica Park Clinic ease the transition to value-based care Overview The need Utica Park Clinic needed to balance the challenging financial implications
Utica Park Clinic Population health management helps Utica Park Clinic ease the transition to value-based care Overview The need Utica Park Clinic needed to balance the challenging financial implications
Patient-Centered Primary Care
 Patient-Centered Primary Care Greg Moody, Director Office of Health Transformation July 30, 2014 www.healthtransformation.ohio.gov Agenda 1. Health System Challenges 2. Health System Trends in Primary
Patient-Centered Primary Care Greg Moody, Director Office of Health Transformation July 30, 2014 www.healthtransformation.ohio.gov Agenda 1. Health System Challenges 2. Health System Trends in Primary
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
Quality, Cost and Business Intelligence in Healthcare
 Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
Quality, Cost and Business Intelligence in Healthcare Maitri Vaidya Population Health Executive DBA, MHA, CPHQ May 2016 Where are we going? IHI Triple Aim Improve the patient experience of care Lower
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
WHITE PAPER. Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice
 WHITE PAPER Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice Maximizing Pay-for-Performance Opportunities In today s
WHITE PAPER Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice Maximizing Pay-for-Performance Opportunities In today s
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Transformational Payment Reform: How will FQHC s survive?
 Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study
 Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Mission Health Care Network. April 2017
 Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Transforming Primary Care in the Adirondack Region of New York State
 Transforming Primary Care in the Adirondack Region of New York State 2013 Southwind Institute October 22, 2013 Karen Ashline, Director Northern Adirondack Medical Home A Division of the Champlain Valley
Transforming Primary Care in the Adirondack Region of New York State 2013 Southwind Institute October 22, 2013 Karen Ashline, Director Northern Adirondack Medical Home A Division of the Champlain Valley
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Medical Home Renovations: A Patient-centered Medical Home Case Study
 Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Transforming Clinical Practice Initiative (TCPI) A Service Delivery Innovation Model. Better Health. Better Care. Lower Cost.
 A Service Delivery Innovation Model. Better Health. Better Care. Lower Cost.") Transforming Clinical Practice Initiative (TCPI) A Service Delivery Innovation Model Better Health. Better Care. Lower Cost. 1 Context for Transforming Clinical Practice With the passage of the Affordable
Transforming Clinical Practice Initiative (TCPI) A Service Delivery Innovation Model Better Health. Better Care. Lower Cost. 1 Context for Transforming Clinical Practice With the passage of the Affordable
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology
 Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
The influx of newly insured Californians through
 January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
Building the Universal Roadmap to Population Health Management
 Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
Product and Network Innovation: Strategies to Achieve Triple Aim Success. Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013
 Product and Network Innovation: Strategies to Achieve Triple Aim Success Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013 Agenda About Minnesota s Market Measurement building blocks
Product and Network Innovation: Strategies to Achieve Triple Aim Success Patrick Courneya, MD Medical Director, HealthPartners October 31, 2013 Agenda About Minnesota s Market Measurement building blocks
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
A Journey PCMH & Practice Transformation PCMH 101. Kentucky Primary Care Association Lexington Kentucky June 11, 2014
 A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Lessons Learned in Care Management. Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference
 Lessons Learned in Care Management Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference 1 Objectives: Rationale for team-based care model Lessons learned in implementing
Lessons Learned in Care Management Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference 1 Objectives: Rationale for team-based care model Lessons learned in implementing
Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS CMS support of Health Care Delivery System Reform (DSR) will result in better care, smarter spending, and healthier
Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS CMS support of Health Care Delivery System Reform (DSR) will result in better care, smarter spending, and healthier
CMS Quality Payment Program: Performance and Reporting Requirements
 CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
TABLE H: Finalized Improvement Activities Inventory
 TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
10/10/2017. Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP
 Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP") Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
MACRA & Implications for Telemedicine. June 20, 2016
 MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
All ACO materials are available at What are my network and plan design options?
 ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
New Models of Health Care: The Patient Centered Medical Home. Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013
 New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
21 st Century Health Care: The Promise and Potential of a Learning Health System
 21 st Century Health Care: The Promise and Potential of a Learning Health System Carolyn M. Clancy, MD Director Agency for Healthcare Research and Quality National Science Foundation Learning Health System
21 st Century Health Care: The Promise and Potential of a Learning Health System Carolyn M. Clancy, MD Director Agency for Healthcare Research and Quality National Science Foundation Learning Health System
MEDICAL HOMES Arkansas Hospital Association
 MEDICAL HOMES Arkansas Hospital Association Framing our discussion Environmental snapshot of health care Hospitals and the PCMH Arkansas Medical Homes Patients/Consumers 2 1 Health Policy is changing Budget
MEDICAL HOMES Arkansas Hospital Association Framing our discussion Environmental snapshot of health care Hospitals and the PCMH Arkansas Medical Homes Patients/Consumers 2 1 Health Policy is changing Budget
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Transforming to Value: One Way Forward
 Transforming to Value: One Way Forward Intermountain Healthcare s Value-Based Reimbursement and Change Management Strategy Mark Briesacher, MD Senior Administrative Medical Director Intermountain Medical
Transforming to Value: One Way Forward Intermountain Healthcare s Value-Based Reimbursement and Change Management Strategy Mark Briesacher, MD Senior Administrative Medical Director Intermountain Medical
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Payment Reform Strategies. Ann Thomas Burnett BlueCross BlueShield of South Carolina
 Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Adopting a Care Coordination Strategy
 Adopting a Care Coordination Strategy Authors: Henna Zaidi, Manager, and Catherine Castillo, Senior Consultant Current state of health care The traditional approach to health care delivery is quickly becoming
Adopting a Care Coordination Strategy Authors: Henna Zaidi, Manager, and Catherine Castillo, Senior Consultant Current state of health care The traditional approach to health care delivery is quickly becoming
Fast-Track PCMH Recognition
 Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP)
 & Patient-Centered Specialty Practice (PCSP)") Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP) Foundation for a Better Health Care System Presenter Jeanette Ikan, M.D., MHAI Objectives: Definition and benefits of PCMH,
Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP) Foundation for a Better Health Care System Presenter Jeanette Ikan, M.D., MHAI Objectives: Definition and benefits of PCMH,
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
Patient Centered Medical Home Foundation for Accountable Care
 Patient Centered Medical Home Foundation for Accountable Care Outline of Presentation History and tenants of the patient-centered care and PCMH model Defining, measuring, recognizing, and evaluating the
Patient Centered Medical Home Foundation for Accountable Care Outline of Presentation History and tenants of the patient-centered care and PCMH model Defining, measuring, recognizing, and evaluating the
Why Are We Doing This?
 ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
Overview. Patient Centered Medical Home. Demonstrations and Pilots: Judith Steinberg, MD, MPH March 6, 2009
 Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation