High Reliability. How to Significantly Improve Safety Systems Using HRO Methodology
|
|
|
- Dominic Sutton
- 6 years ago
- Views:
Transcription


1 High Reliability How to Significantly Improve Safety Systems Using HRO Methodology Tom Peterson, MD VP, Chief Safety Officer SCL Health April 15, 2015 Sisters of Charity of Leavenworth Health System, Inc. All rights reserved.
2 No Conflicts of Interest



3 The Journey to High Reliability in Healthcare High Reliability Process improvement - Mandated measures -NPSG s,hac s, Never events, VBP, MU Generative Safety is how we do business around here Proactive Safety leadership and values drive continuous improvement Evidence Based Guidelines Clinical Protocols Core Measures IOM Report Calculative We have safety systems in place to manage all harm events Regulations Compliance Malpractice - Captive insurance boom Reactive Safety is important, we do a lot every time we have an accident <1980 s Pathological Who cares as long as we re not caught

4 Naval Aviation Mishap Rate Class A Mishaps/100,000 Flight Hours aircraft destroyed in Angled Carrier Decks Naval Aviation Safety Center NAMP est RAG concept initiated NATOPS initiated aircraft destroyed in 2008 Squadron Safety program System Safety Designated Aircraft ACT HFC s Fiscal Year Source: ORM Flight Mishap Rate 4
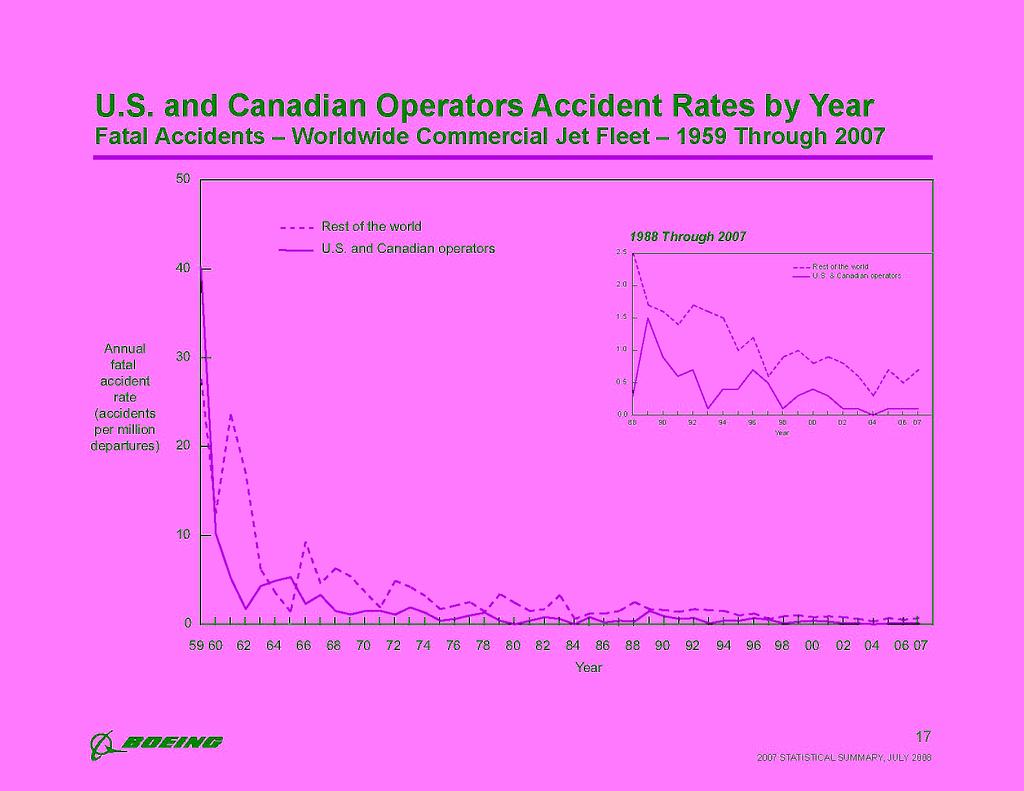
5 Commercial Aviation
 finding or performance indicator An event with a Conditional Core Damage Probability (CCDP) or increase")
6 Significant Events at US Nuclear Plants Annual Industry Average, Fiscal Year Significant Events are those events that the NRC staff identifies for the Performance Indicator Program as meeting one or more of the following criteria: A Yellow or Red Reactor Oversight Process (ROP) finding or performance indicator An event with a Conditional Core Damage Probability (CCDP) or increase in core damage probability (ΔCDP) of 1x10-5 or higher An Abnormal Occurrence as defined by Management Directive 8.1, Abnormal Occurrence Reporting Procedure An event rated two or higher on the International Nuclear Event Scale Source: Nuclear Regulatory Commission Information Digest (1988 is earliest year data is available) Updated: November
7 American Construction Company Worker Injury Rates Mortenson RIR BLS RIR BLS DART Mortenson DART
8 Healthcare? We lead in both preventable deaths to our customers (patients) as well as injuries to our employees. Our time is far overdue.. Sisters of Charity of Leavenworth Health System, Inc. All rights reserved.

9 The Numbers Today Are Daunting ,000 deaths caused each year to patients in American Hospitals¹ 3 rd leading cause of death in the US 670,000 injuries every year to healthcare workers² Healthcare leads all industries in workers injuries Up to times higher than such industries as high rise construction and aluminum plants BLS average RIR for American Hospitals = 6.4, Alcoa Aluminum in 2014 =.98! 1- Jour Patient Saf, 2013;9: Janocha JA, Smith RT. Workplace Safety and Health in the Health Care and Social Assistance Industry, Washington, DC: US Bureau of Labor Statistics; 2012
10 Do We Really Want To Be Ultra Safe? Total Lives Lost Per Year Dangerous >1/1, ,000 10, Healthcare (1 of ~ 600) Mountain Climbing Bungee Jumping Driving in the US Chartered Flights Chemical Manufacturing ,000 Number of Encounters 100K 1M Ultra-safe <1/100,000 Scheduled Commercial Airlines European Railroads Nuclear Power 10M
 To Err is Human, Institute of Medicine (1999) Created A Lot of Talk Patient safety publications before and after the IOM")

11 Healthcare s Wake Up Call 44,000 to 98,000 patient deaths per year from medical errors ( dead every day) (1 death per every 378 admissions) To Err is Human, Institute of Medicine (1999) Created A Lot of Talk Patient safety publications before and after the IOM report, To Err is Human Quality & Safety in Health Care (2006) Each month,134,00 hospitalized Medicare patients suffer from harm from medical care, while 15,000 of these patients die due to medical mistakes; 44% of all events rendered as preventable. Landrigan, New Eng Jour Med, (2010)

12 Frankly, there is little guidance in the high reliability science and in the case studies. There s very little guidance on how you get from our pretty mediocre state with quality, with respect to quality and safety. How do you get from low reliability to high reliability? So we have considered that problem and asked the question, how do we create blueprints, roadmaps, assistive devices that allow health care organizations to build toward high reliability? What would it take? Mark Chassin, M.D., President, The Joint Commission 2011







13 What is an HRO?

14 HRO Descriptions Can Be Confusing Sutcliffe and Weicke The 5 Principles Mindfulness TJC Chassin and Loeb Leadership Culture Process improvement Amalberti Accepting limits Abandon autonomy Craftsman to equivalent actors Sharing risk vertically Managing visible risk Health and Safety Executive The 5 Principles Anticipation and Containment Leadership Safety culture Continuous learning Admiral Hyman Rickover Rising standards over time (more than the minimum) Highly capable people trained over a wide range Leaders face bad news (mobilize effort, report up) Healthy respect for dangers Training is constant and rigorous All functions fit together Learning from the past

15 Journey From Improvement to High Reliability Design to Optimize Human Performance at the point of people interface: Easy to do the right thing impossible to do the wrong thing Mistake proofing/human factors Industry standards The occurrence is viewed as a failure Reliability Culture Mindfulness The Mindset of Failures, Accountability Safety as the core value, Leadership commitment A 1000 safety champions Behavior expectations for error prevention Collaborative Interactive Teams 10-2 Process, Protocol 10-1 &Technology Resource allocation Evidence-based practice (e.g. bundles) Technology enablers The blunt end barriers Reference: HPI, Inc, Sutcliffe and Weick
16 Things Done Right 99.9% of the Time Means.. Two unsafe landings at O Hare Airport every day 16,000 lost pieces of mail every hour 20,000 wrong drug prescriptions every year 500 incorrect surgical operations a month 50 newborn babies dropped by a doctor every day 32,000 missed heart beats a year 22,000 checks deducted from the wrong account every hour
17 Quality Improvement is Getting to 99.9% High Reliability is going from the 99.9% to 100%
18 Safety is One There are not two safety s in HRO s
19 In An HRO It Does Not Matter If It Is. MSK injuries Sharps/needlesticks CAUTI s Patient falls Employee slips and falls Pressure ulcers Admissions Pressure ulcers Combative patients Hand washing CLABSI s
20 It Sounds Simple. Do everything you can to prevent it from happening. If it happens, do everything you can to contain the process.. Then do everything you can to correct it, or keep it from happening again. The key is the failure(s) identified are precursors to an actual event.
21 Safe Patient Handling An unsafe handling is a failure Do Everything to Prevent It From Happening How do you hire? How much training did they get, and do they get? How strict is your screening and policies? Do they all learn error prevention behaviors? Do they all know it is a safe culture they are entering? Do they know safety is a core value? Is there peer checking always? Is there 200% accountability? Can they speak up and question, stop when we see a potential hazard? Are we rewarded for that? Do they report all near miss events and safety hazards? Are they rewarded for reporting? Do they work as a team? Are you always looking for a new way to make it better?
22 Safe Patient Handling If a failure almost occurs. Do everything you can to contain it if it happens. Did they get the proper equipment? Are you reporting the latent weaknesses always? Did we use leading indicators? Is there continuous training, a need to retrain? Are structures designed appropriately? Did they use the safe behaviors? Is the process standardized? Are you trending the failures? Was there an immediate shared learning? Was there peer checking, where was the team?
23 Safe Patient Handling If a failure caused an event. Do everything you can to correct the defect and keep it from happening again without missing a beat Did you do an immediate ACA on the event? Did you common cause the multiple events to identify a common process? Did you correct the root cause? Was it a system or individual failure, or both? Did you do an immediate huddle (SWARM), with senior execs, to de-brief the event and show your care for the employee and identify the most beneficial information? Have you audited your process recently? Was there an immediate shared learning with everyone? Was the event shared system wide? Was the action plan followed through on? Systems changes implemented?
24 An HRO High reliability is a mindset Strong responses to all weak signals The occurrence is viewed as a failure High reliability is always learning new ways, new skills. One is always one too many, no excuses Refuses to follow simplified processes High reliability exists only when leadership owns the process, all staff believe in the commitment.. High reliability requires a robust safety culture. There is not one safety officer, there are 2000 of them High reliability is being resilient, and strong infrastructures exist to respond to the needed changes The responses and shared learnings are immediate, and do not alter operations Committed to resilience High reliability is a journey
25 The High Reliability Mindset - Mindfulness First, we have to view previous norms as failures, or at least extremely dangerous, and be totally preoccupied with preventing it from happening Near misses are highly valued The weak signals are the most important Leading indicators become the norm Not an external mandate, but an internal value Mindfulness is horizontal and vertical The vertical processes are perfected with no defects, while the horizontal culture is always aware if deviations Always new appreciation of current context
26 CAUTI HAI/HAC Experience 45 The Lean/QI project began here CAUTI HAI/HAC Annual Comparison Number of CAUTI Events The new mindset began here CAUTI HAC still in 2015!

27 The Near Miss Reporting Strong Responses to Weak Signals Many industries use this as accepted practice Airlines, construction, nuclear power, steel, mining, military, petrochemical Near miss reporting has been used in several industries for the last 40 years Near misses, leading indicators, need to be valued by all in the organization Data and skills need to exist to trend, analyze and act on near misses
28 Leadership Must Own the Process Leadership walks the walk Resources are supported The leader knows every harm event, defect Structures are developed The leader drives accountabilities Safety is a core value

29 If you want to understand how is doing, you need to look at our workplace safety figures. If we bring our injury rates down, it won t be because of cheerleading or the nonsense you sometimes hear from other CEO s, or some training or new program. It will be because the individuals at this company have agreed to become part of something important: They ve devoted themselves to creating a habit of excellence. Safety will be an indicator that we re making progress in changing our habits across the entire institution. That s how we should be judged. Paul O Neill CEO of Alcoa years later injury rates are their lowest in history!
30 Always Learning New Ways One is one too many A commitment to zero Always training for new skills Shared learnings Question existing standards, assumptions Continuously changing based on new experiences Willingness to invent new processes
31 A Robust Safety and Learning Culture Everyone is engaged Clinical and non-clinical A 1000 safety champions Flexible, just, learning, informed and reporting Continuous training and skill building for all Full transparency Physician champions, the hierarchy is flat Stories, awareness, rewards
32 The Journey The culture and mindsets take years to develop Sustainable commitment is required Not a flavor of the month or a training It should not matter who the leadership is While it can be hard to measure, it is easy to experience when it exists
33 The Big Questions 1. Structures for culture change 2. Our behaviors are we serious? 3. Are we really reporting everything? 4. Our leaders? 5. Education of staff and physicians 6. Are we really committed? 7. Can we measure our progress? 8. How do we sustain progress?
34 SCL HRO Program Processes Sharps, SPH, Violence and STF s programs Cause analysis and HRO training - > 400 trained Human error prevention trainings 6,000 trained, > 250 trainers Core value Site assessments, apology and disclosure program Safety coach program 100 to train Safety and Physician Safety Committees Lessons learned program Daily huddles unit and hospital wide, executive rounding, Event reporting teams, Regular audits Safety Officers, System Directors Patient and Associate Outcomes Event reporting increased > 100% in 1 year System RIR - 40% in the past 4 years, sharps 25% in past year Current RIR 2.97 Serious safety event rate 20% Workers comp and litigation claims costs decreased over 4 years both by 30%
35 Questions?
36 Implementing the HRO Mindset in Healthcare 1/1,000,000 Drive Continuous Learning and Training the Accountabilities View the occurrence as a FAILURE! Human factors Error proofing Industry standards Hire to Fit Leadership accountabilities Leading indicators Performance reviews Create the Reliability Culture Safety stories - Awareness Campaigns Awards/positive feedback Safety Champions Safe environments Videos Increased reporting Safety coaches Unit based expertise - Physician safety champions Safety as a Core Value - Leadership behaviors Build the Foundation Swarms- (Executive) -Weekly Call ins Leadership Commitment - Safety Officers - Daily huddles (hospital and units) Safety Leadership Teams (council) The Right Equipment - Physician Safety Teams Error Behavior Prevention Trainings - Shared Learnings Leadership Ownership 1/100,000 1/10,000 1/1,000 1/100 1/10
37 . The Vertical Reliability establishes the needed structures and processes to prevent the failures from occurring, while Horizontal Reliability creates the culture for the safety behaviors to prevail... Central Line Infections Questioning attitude Focusing Slips and Falls Safe Patient Handling Bundles Rapid cycle Lean/PI Readmissions Trainings Critical thinking Needle stick injuries High Reliability Safety Culture Speaking up Evidence Based Protocols CAUTI s PDCA Peer checking and on, and on, and on Clear communication..but it only can happen if the mindset exists! 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.


38 We are what we repeatedly do. Excellence, then, is not an act, but a habit. Ἀριστοτέλης 384 BC 322 BC Student of Plato, Tutor to Alexander
39 High Reliability Patient Safety = Employee Safety Concepts directly apply to caregiver safety Shared values, tools and goals Institutional system for HRO creates framework for all safety initiatives Safe patient handling and mobility directly impacts both patient and caregiver Safety

40 Entirely In The Same Net Patient Handling Medication Errors Falls Wrong Surgery Site Delay in Diagnosis or Treatment Sharps
41 HRO Elements = Safe Patient Handling Success Near Miss Reporting Safety Event Follow Up Engaging Leaders about Every Injury Daily Safety Huddles Safety Awareness of each Employee Error Detection & Prevention Skills



42 Tools to Improve Reliability Crew Resource Management airline industry TeamSTEPPS department of defense Brief execute de-briefs naval aviation Daily Check ins nuclear power Lean Henry Ford, Toyota 42
43 Obsession With Failure Current Practice: We learn about patient handling issues AFTER an injury has occurred. HRO Practice: Learn about every near miss BEFORE an injury occurs.



44 Child Proof Your Safe Patient Handling Program and Your Hospital!

45 Be Prepared for Work Arounds Lets you learn about work-arounds to truly create a successful program!
46 Near Miss Reporting System Non-Punitive Fast and Easy Meaningful Categories Encourage Reporting! Immediate Management Follow Up
47 RL6 Reports There is no repositioning/highback slings in the supply room. Linen called and only had two slings available. Pt. needs frequent repositioning in bed, lift room would be safer for pt and staff. Patient unable to do 75% of his own repositioning in bed in a lift room, with a reposition sling underneath him asked me to "boost him up in bed" and requested that his wife help me. I explained to him that we use the overhead lift system with the reposition sling if he is unable to get himself back up in bed.

48 Are slings available? Is there enough equipment? Do we need different slings or tools? Is everyone adequately trained? Are there clinicians who need specific education? Are assessments accurate?


49 Cover Holes in the Swiss Cheese C.N.A. is develops a back injury. Other Caregivers Do Not Speak Up & Suggest Using Lift Patient Develops Deep Tissue Injury and Stage 4 Pressure Ulcer Caregivers Not Using Available Lift To Reposition Patient Sling is not under patient, training inadequate, low par levels


50 Lift Team Safe Patient Handling Committee Super Users, Coaches, Champions Simple Policy & Procedure with Concise Language Organization support for caregiver safety when moving patients. Access to Equipment Sling Flow Super Users, Coaches, Champions Equipment that meets needs Easy access to equipment Correct amount of equipment Distraction Critical Thinking Time pressure Assumptions The blunt end structures cannot prevent all errors, so the sharp end behaviors must exist always Correct Equipment is used to reduce injury and improve patient outcomes every time. Adapted from R. Cook and D. Woods, Operating at the Sharp End: The Complexity of Human Error (1994)




51 3 Ways We Learn 30 in 10,000 errors per day 0.3% forget to hook up one sling loop 1% Error Rate choose to boost and not use lift 30% Error Rate do not know how to use new equipment but try without asking for help
52 Type of Error: Skill Based- Auto Pilot Rule Based- Performance How we re taught or noncompliance Knowledge Based- Lack of knowledge Action Error Prevention Strategy: Focus Stop on proper and Think technique for sling loop placement Education, risk or burden reduction Create better location for slings Enforce management expectations Stop and find an expert Find Lift Champion or Site Safe Patient Handling Coordinator
53 Near Miss Follow Up Pertinent Information From Reporting System February 9, 2015 Specific Event Type: Patient Handling Type of Person Affected: Associate Injury Incurred? No Equipment Involved/Malfunctioned? No Was lift equipment used? No If no, why wasn't this used? (Explain): the nurse didn't seem to think it mattered. As i used my voice about concern, she again didn't seem to think it matter. Brief Factual Description: I went up to image the patient in room ####. the patient was in a room with a lift however there was no sling under the patient. The patient could not move at all. I told the nurse the patient need a sling and she didn't seem to care. Again i spoke up when the nurse asked me to help boost the patient up that this patient needs a sling. No one was injured today but this patient cant move and someone will eventually get injured or injury to the patient. Immediate Actions Taken: I voiced my concern about this patient not having a lift, she didn't seem to think it mattered. again i voiced my concern about this situation. I asked the nurse. i used CUS but it didn't matter.
54 Goal = 24 Hours Follow Up (All occurred in first 24 hours following near miss) to Unit Manager Unit Manager investigated and learned nurse involved was in float pool to float pool educator Float pool educator met with nurse and ed all involved managers Lesson Learned: Float pool education was needed Lesson Learned: Processes and tools need to be better utilized Lesson Learned: Policy was not followed and chain of command not utilized
55 Meeting Attendance Meeting Scheduled February 11, 2015 Attendance: 1. On-Site SPH Leader 2. System SPH Leader 3. Imaging Director 4. Float Pool Educator 5. Float Pool Manager 6. Wound Care Nurse 7. Department Manager of Unit where event occurred Agenda: 1. Review of incident focusing on patient mobility status 2. Identify best practice 3. Plan training and follow up
56 Near Miss Reporting System Example Meeting Scheduled February 11, 2015 Outcome: Patient had been on unit 3 days so sling should have been placed prior to this incident. Lack of mobility may be a contributing factor to patient s pain and low grade fever. SBAR written by unit manager. PM&R manager, Float manager and Surgical manager will review incident with all staff. Work is being done with PACU for sling placement on patients prior to transfer to the floor. Incident also discussed in Daily Safety Huddle, SPH committee, , Department huddles Results: 1.Employee who spoke up was rewarded and supported 2.Departmental issue learned and addressed from a near miss event with no harm 3.Late adopters are held accountable after initial attempt to ignore incident 4.Closed some holes in the Swiss cheese 5.SSC on Unit understands proper practice and support 6.Blunt End strategies were developed and implemented to support sharp end Long Term: 1.Culture is changed from bottom up and top down with each incident properly addressed.
57 A bad system will DEFEAT a good person every time. W. Edwards Deming Every system is perfectly designed to get the results it gets. Dr. Paul Batalden

58 Culture Will Not Change Without Manager Knowledge and Accountability

59 Rapid reporting directly to front line managers. Follow up meetings with leadership Ideally, there is personal knowledge of each employee injury by CEO! Written leadership follow up with details of corrective actions
60 Power Distance in Health Care Large Distance Relations are autocratic and paternalistic Power acknowledged based on formal, hierarchical positions Small Distance Relations are consultative and democratic Relate as equals regardless of formal positions The perceived distance not necessarily the real difference as seen by the subordinate Safety Culture Goal: Use organizational culture to reduce the power distance between groups Adapted from G. Hofstede s Culture s Consequences (2001)





61
62 Daily Check-in for Safety Patient Handling Examples Chair removed from patient room contributed to fall Sling loops need to be tucked in No lift room available during high census Report out standard patient handling metrics Report that nurse was asked to boost patient with sling under them Sling par issue poorly managed


63 Associate Safety Tip: What Should I do if no Blue Reposition Slings are available? 1.Call Materials Management and request a disposable sling. 2.Call Materials Management and request a Gold reposition sling if leg support is not needed. Follow up promotes more reporting!! 3.Please let your manager know there was a par issue so that our Safe Patient Handling Committee can work to solve this issue. 4.Consider using a limb lifter
64 Announcing a Good Catch for Safety! We re celebrating those who identify, correct and report potential safety issues before harm reaches a patient, associate or other staff person. Thank you for keeping our patients and each other safe from harm. Good Catch for Safety!
65
66
67
68
69
70
71
High Reliability Organizations Healing Without Harm by 2014
 Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by 2014 1.1 Stand up if You have suffered harm as a patient at a hospital
Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by 2014 1.1 Stand up if You have suffered harm as a patient at a hospital
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Safe Sharp Program: A Culture of Prevention
 Safe Sharp Program: A Culture of Prevention Ken Smith System Director of Safety kenneth.smith@sclhs.net Sisters of Charity of Leavenworth Health System, Inc. All rights reserved. 1 Safe Sharps: A Culture
Safe Sharp Program: A Culture of Prevention Ken Smith System Director of Safety kenneth.smith@sclhs.net Sisters of Charity of Leavenworth Health System, Inc. All rights reserved. 1 Safe Sharps: A Culture
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
From Value to High-Reliability Organization
 From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
TIME OUT! A Patient Safety Strategy. Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service
 TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
Creating a Highly Reliable Health System: the Leadership Challenge. 6 th Annual Patient Safety Symposium Rick Foster, MD
 Creating a Highly Reliable Health System: the Leadership Challenge 6 th Annual Patient Safety Symposium Rick Foster, MD April 18, 2013 Moving Toward Zero It may seem a strange principle to enunciate as
Creating a Highly Reliable Health System: the Leadership Challenge 6 th Annual Patient Safety Symposium Rick Foster, MD April 18, 2013 Moving Toward Zero It may seem a strange principle to enunciate as
Patient Safety. Annual Accidental Deaths. Medical Errors in History. How Hazardous Is Health Care (Amalberti)
") Patient Safety Annual Accidental Deaths 100000 90000 80000 70000 60000 50000 40000 30000 20000 10000 0 Medical Auto Workplace Air Deaths Total lives lost per year How Hazardous Is Health Care (Amalberti)
Patient Safety Annual Accidental Deaths 100000 90000 80000 70000 60000 50000 40000 30000 20000 10000 0 Medical Auto Workplace Air Deaths Total lives lost per year How Hazardous Is Health Care (Amalberti)
COOK COUNTY HEALTH & HOSPITALS SYSTEM
 COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
Fostering a Culture of Safety
 Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Understanding the High Reliability Organization and Why It's Important to Your Lab
 Understanding the High Reliability Organization and Why It's Important to Your Lab Jennifer Rhamy MBA, MA, MT(ASCP)SBB, HP Executive Director, Laboratory Accreditation High Reliability Organization (HRO)
Understanding the High Reliability Organization and Why It's Important to Your Lab Jennifer Rhamy MBA, MA, MT(ASCP)SBB, HP Executive Director, Laboratory Accreditation High Reliability Organization (HRO)
What Every Patient Safety Officer Must Know:
 What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
HROs and the Role of Finance South Carolina HFMA Annual Institute
 HROs and the Role of Finance South Carolina HFMA Annual Institute Kari Cornicelli, FHFMA,CPA Vice President/CFO Sharp Metropolitan Medical Campus San Diego, CA 1 Reflection Perfection is not attainable.
HROs and the Role of Finance South Carolina HFMA Annual Institute Kari Cornicelli, FHFMA,CPA Vice President/CFO Sharp Metropolitan Medical Campus San Diego, CA 1 Reflection Perfection is not attainable.
To Err is Human To Delay is Deadly Ten years later, a million lives lost, billions of dollars wasted
 1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
Kate Beaumont. Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign.
 Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Shifting from Blame-&-Shame to a Just-and-Safe Culture
 Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
High Reliability Organizing (HRO) in the Ambulatory Setting
 in the Ambulatory Setting") High Reliability Organizing (HRO) in the Ambulatory Setting High Reliability Training Sisters of Charity Leavenworth Health System 25 May 2016 2014 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
High Reliability Organizing (HRO) in the Ambulatory Setting High Reliability Training Sisters of Charity Leavenworth Health System 25 May 2016 2014 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
A26/B26: Goal Zero: South Carolina s Commitment to Safety
 A26/B26: Goal Zero: South Carolina s Commitment to Safety Coleen Smith, RN, MBA, CPHQ, High Reliability Initiatives Director Joint Commission Center for Transforming Healthcare Thornton Kirby, FACHE, President
A26/B26: Goal Zero: South Carolina s Commitment to Safety Coleen Smith, RN, MBA, CPHQ, High Reliability Initiatives Director Joint Commission Center for Transforming Healthcare Thornton Kirby, FACHE, President
Translational Safety Through Immersive Learning: Practice What you Preach
 Translational Safety Through Immersive Learning: Practice What you Preach Gregory Botz, MD, FCCM Professor, Department of Critical Care Division of Anesthesiology and Critical Care The University of Texas,
Translational Safety Through Immersive Learning: Practice What you Preach Gregory Botz, MD, FCCM Professor, Department of Critical Care Division of Anesthesiology and Critical Care The University of Texas,
Overcoming Common Barriers to Successful Safe Patient Handling Programs
 Overcoming Common Barriers to Successful Safe Patient Handling Programs Strategies for Gaining Support with Leadership at All Levels Ed Hall, Chief Operating Officer, The Risk Authority Strategies for
Overcoming Common Barriers to Successful Safe Patient Handling Programs Strategies for Gaining Support with Leadership at All Levels Ed Hall, Chief Operating Officer, The Risk Authority Strategies for
ECRI Patient Safety Organization HFACS and Healthcare
 October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Lab Quality Confab Process Improvement Institute. New Orleans, LA. John Waugh 11/3/2015
 Implementing a Single Quality Management System Across Multiple Hospitals of the Henry Ford Health System: Combining ISO 15189 with Lean to Deliver More Value Lab Quality Confab Process Improvement Institute
Implementing a Single Quality Management System Across Multiple Hospitals of the Henry Ford Health System: Combining ISO 15189 with Lean to Deliver More Value Lab Quality Confab Process Improvement Institute
Building a High-Performance team in the Pediatric Medical Home Xavier Sevilla M.D. FAAP Whole Child Pediatrics MCRHS Inc.
 Building a High-Performance team in the Pediatric Medical Home Xavier Sevilla M.D. FAAP Whole Child Pediatrics MCRHS Inc. Whole Child Pediatrics Whole Child Pediatrics Opened November 2007 Using the Principles
Building a High-Performance team in the Pediatric Medical Home Xavier Sevilla M.D. FAAP Whole Child Pediatrics MCRHS Inc. Whole Child Pediatrics Whole Child Pediatrics Opened November 2007 Using the Principles
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
 BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
Sharp HealthCare s HRO Commitment
 Sharp HealthCare s HRO Commitment Daniel L. Gross, DNSc, RN Executive Vice President Amy Adome, MD, MPH Senior Vice President, Clinical Effectiveness November 3, 2016 Perfection is not attainable, but
Sharp HealthCare s HRO Commitment Daniel L. Gross, DNSc, RN Executive Vice President Amy Adome, MD, MPH Senior Vice President, Clinical Effectiveness November 3, 2016 Perfection is not attainable, but
A9/B9: Integrating Patient Safety into Your System s DNA
 A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
High Reliability Organizing (HRO) and the Patient Experience
 and the Patient Experience") High Reliability Organizing (HRO) and the Patient Experience High Reliability Training Sisters of Charity Leavenworth Health System 25 May 206 204 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
High Reliability Organizing (HRO) and the Patient Experience High Reliability Training Sisters of Charity Leavenworth Health System 25 May 206 204 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
University of Washington School of Nursing - Continuing Nursing Education 1
 A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
High Reliability Healthcare: A Journey to Zero
 High Reliability Healthcare: A Journey to Zero Arizona Organization of Nurse Executives August 19, 2016 Coleen Smith, RN, MBA, CPHQ, CPPS Objectives Discuss the importance of leaders as agents of change
High Reliability Healthcare: A Journey to Zero Arizona Organization of Nurse Executives August 19, 2016 Coleen Smith, RN, MBA, CPHQ, CPPS Objectives Discuss the importance of leaders as agents of change
CROSSING THE QUALITY CHASM: HEALTH CARE FOR THE 21 ST CENTURY
 CROSSING THE QUALITY CHASM: HEALTH CARE FOR THE 21 ST CENTURY May 10, 2002 Donald M. Berwick, M.D. President & CEO Institute for Healthcare Improvement The Foundation IOM Roundtable President s Advisory
CROSSING THE QUALITY CHASM: HEALTH CARE FOR THE 21 ST CENTURY May 10, 2002 Donald M. Berwick, M.D. President & CEO Institute for Healthcare Improvement The Foundation IOM Roundtable President s Advisory
Barriers to a Positive Safety Culture. Donna Zankowski MPH RN
 Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Extract from Managing Infection Control
 TOPIC ONE: CONDUCTING AN INFECTION CONTROL RISK AUDIT The aims and objectives of this topic are to: state the rationale for conducting a risk audit detail the occasions when a risk audit should be conducted
TOPIC ONE: CONDUCTING AN INFECTION CONTROL RISK AUDIT The aims and objectives of this topic are to: state the rationale for conducting a risk audit detail the occasions when a risk audit should be conducted
VA Radiotherapy Incident Reporting and Analysis System (RIRAS)
") VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
Perfect Depression Care. M. Justin Coffey, MD Henry Ford Health System IBHI Webinar Series 2011
 Perfect Depression Care M. Justin Coffey, MD Henry Ford Health System IBHI Webinar Series 2011 M. Justin Coffey, MD Behavioral Health Services Henry Ford Hospitals & Health System jcoffey1@hfhs.org 313.874.6887
Perfect Depression Care M. Justin Coffey, MD Henry Ford Health System IBHI Webinar Series 2011 M. Justin Coffey, MD Behavioral Health Services Henry Ford Hospitals & Health System jcoffey1@hfhs.org 313.874.6887
DEALING WITH OPERATIONAL RISK AN INFORMAL CASE STUDY DRAWN FROM REAL LIFE
 DEALING WITH OPERATIONAL RISK AN INFORMAL CASE STUDY DRAWN FROM REAL LIFE JIM ELLIS APRIL 8, 2016 A BIT OF HISTORY OVER 100 YEARS OF OPERATING EXPERIENCE BEGINNING JANUARY 18, 1911 SAN FRANCISCO BAY RISK
DEALING WITH OPERATIONAL RISK AN INFORMAL CASE STUDY DRAWN FROM REAL LIFE JIM ELLIS APRIL 8, 2016 A BIT OF HISTORY OVER 100 YEARS OF OPERATING EXPERIENCE BEGINNING JANUARY 18, 1911 SAN FRANCISCO BAY RISK
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM
 Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Creating a Culture in Support of Patient Safety
 Session: L11 Ms. Ching has nothing to disclose Ms. Derheimer is an employee of the Virginia Mason Institute; a not-for-profit organization that provides education and training in the Virginia Mason Production
Session: L11 Ms. Ching has nothing to disclose Ms. Derheimer is an employee of the Virginia Mason Institute; a not-for-profit organization that provides education and training in the Virginia Mason Production
Pursuing Perfect Depression Care: A Model for Eliminating Suicide and Transforming Mental Healthcare
 A Model for Eliminating Suicide and Transforming Mental Healthcare C. Edward Coffey, M.D. Henry Ford Health System Detroit, MI Outline of Presentation Case Presentation A Health Care System in Shambles
A Model for Eliminating Suicide and Transforming Mental Healthcare C. Edward Coffey, M.D. Henry Ford Health System Detroit, MI Outline of Presentation Case Presentation A Health Care System in Shambles
The Clinician s Impact on the Patient Experience
 The Clinician s Impact on the Patient Experience Michelle George MSN RN CASC 1 Objectives Achieving desired clinical outcomes through safety initiatives and clinical best practices Communication and engagement
The Clinician s Impact on the Patient Experience Michelle George MSN RN CASC 1 Objectives Achieving desired clinical outcomes through safety initiatives and clinical best practices Communication and engagement
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
What is High Reliability and Why Does Healthcare Need it?
 What is High Reliability and Why Does Healthcare Need it? Mark R. Chassin, MD, FACP, MPP, MPH President, The Joint Commission Institute for Healthcare Improvement 25th Annual Forum Orlando, FL December
What is High Reliability and Why Does Healthcare Need it? Mark R. Chassin, MD, FACP, MPP, MPH President, The Joint Commission Institute for Healthcare Improvement 25th Annual Forum Orlando, FL December
A 21 st Century System of Patient Safety and Medical Injury Compensation
 A 21 st Century System of Patient Safety and Medical Injury Compensation Overview Our goal is to promote patient safety and reduce preventable errors and injuries. We want to replace our fault-based medical
A 21 st Century System of Patient Safety and Medical Injury Compensation Overview Our goal is to promote patient safety and reduce preventable errors and injuries. We want to replace our fault-based medical
Practical Application of High Reliability Principles in Healthcare to Promote Clinical Quality and Safety Outcomes
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
A culture of safety is a culture of compassion
 A culture of safety is a culture of compassion Compassion in Action Webinar Series March 21, 2017 1 Moderator Andrea Greenberg Communications and Partnerships Associate The Schwartz Center for Compassionate
A culture of safety is a culture of compassion Compassion in Action Webinar Series March 21, 2017 1 Moderator Andrea Greenberg Communications and Partnerships Associate The Schwartz Center for Compassionate
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM
 CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Patient Safety. At the heart of all we do
 Patient Safety At the heart of all we do Introduction from our Medical Director Over the last 15 years it has been recognised that patient safety problems exist throughout the NHS as they do in every health
Patient Safety At the heart of all we do Introduction from our Medical Director Over the last 15 years it has been recognised that patient safety problems exist throughout the NHS as they do in every health
Yoder-Wise: Leading and Managing in Nursing, 5th Edition
 Yoder-Wise: Leading and Managing in Nursing, 5th Edition Chapter 02: Patient Safety Test Bank MULTIPLE CHOICE 1. In an effort to control costs and maximize revenues, the Rehabilitation Unit at Cross Hospital
Yoder-Wise: Leading and Managing in Nursing, 5th Edition Chapter 02: Patient Safety Test Bank MULTIPLE CHOICE 1. In an effort to control costs and maximize revenues, the Rehabilitation Unit at Cross Hospital
1875 Connecticut Ave. NW / Suite 650 / Washington, D.C / / fax /
 Testimony of Jane Loewenson Director of Health Policy, National Partnership for Women & Families Before the U.S. House of Representatives Energy & Commerce Subcommittee on Health Hearing on Patient Safety
Testimony of Jane Loewenson Director of Health Policy, National Partnership for Women & Families Before the U.S. House of Representatives Energy & Commerce Subcommittee on Health Hearing on Patient Safety
Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians
 Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians Edna Rensing, RN, M.S.H.A., CPHQ This material was prepared by the Virginia Health Quality Center, the Medicare Quality
Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians Edna Rensing, RN, M.S.H.A., CPHQ This material was prepared by the Virginia Health Quality Center, the Medicare Quality
CCHS: Quality and Patient Safety. J Michael Henderson, MD Guido Bergomi
 CCHS: Quality and Patient Safety J Michael Henderson, MD Guido Bergomi Outline Integrated Quality & Safety structure Quality Goals and Performance Improvement Quality data sources Quality Reporting The
CCHS: Quality and Patient Safety J Michael Henderson, MD Guido Bergomi Outline Integrated Quality & Safety structure Quality Goals and Performance Improvement Quality data sources Quality Reporting The
Leadership and Culture: Building Highly Reliable Systems of Care
 Learning Objectives Leadership and Culture: Building Highly Reliable Systems of Care Michael Batchelor, CEO Baptist Easley Hospital Easley, South Carolina Discuss recent developments in health systems
Learning Objectives Leadership and Culture: Building Highly Reliable Systems of Care Michael Batchelor, CEO Baptist Easley Hospital Easley, South Carolina Discuss recent developments in health systems
TeamSTEPPS Introductory Webinar. July 19, 2018
 TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
L5: Getting to Always! Using Teach-back to Maximize Patient Learning
 Disclaimers: None L5: Getting to Always! Using Teach-back to Maximize Patient Learning March 21, 2016 Peg Bradke Gail Nielsen Objectives Identify opportunities across the continuum to engage patients and
Disclaimers: None L5: Getting to Always! Using Teach-back to Maximize Patient Learning March 21, 2016 Peg Bradke Gail Nielsen Objectives Identify opportunities across the continuum to engage patients and
Chasing Zero The Journey to Rural Hospital High Reliability
 1 Chasing Zero The Journey to Rural Hospital High Reliability Clint MacKinney, MD, MS Clinical Associate Professor College of Public Health University of Iowa clint-mackinney@uiowa.edu 2 Chasing Zero A
1 Chasing Zero The Journey to Rural Hospital High Reliability Clint MacKinney, MD, MS Clinical Associate Professor College of Public Health University of Iowa clint-mackinney@uiowa.edu 2 Chasing Zero A
Financial Disclosure. Learning Objectives: Preventing and Responding to Sentinel Events in Surgery 10/13/2015
 Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
AF4Q and TCAB: An Introduction
 AF4Q and TCAB: An Introduction July 13, 2011 Ellen Interlandi, MHM, RN, NE-BC Patricia Montoya, MPA, BSN 1 What is Aligning Forces for Quality? An unprecedented commitment by the Robert Wood Johnson Foundation
AF4Q and TCAB: An Introduction July 13, 2011 Ellen Interlandi, MHM, RN, NE-BC Patricia Montoya, MPA, BSN 1 What is Aligning Forces for Quality? An unprecedented commitment by the Robert Wood Johnson Foundation
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Employee Safety: Leveraging Lessons from Patient Harm Reduction to Create a Safer Work Environment
 Employee Safety: Leveraging Lessons from Patient Harm Reduction to Create a Safer Work Environment AJ Principe, MBA, CSSBB Senior Process Improvement Specialist Employee Safety Project Manager Nationwide
Employee Safety: Leveraging Lessons from Patient Harm Reduction to Create a Safer Work Environment AJ Principe, MBA, CSSBB Senior Process Improvement Specialist Employee Safety Project Manager Nationwide
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Delivering Great Care with High Reliability The Orlando Health Journey
 FE5 These presenters have nothing to disclose Delivering Great Care with High Reliability The Orlando Health Journey December 11, 2017 Frank Federico, RPh Vice President Patricia McGaffigan, RN, MS, CPPS
FE5 These presenters have nothing to disclose Delivering Great Care with High Reliability The Orlando Health Journey December 11, 2017 Frank Federico, RPh Vice President Patricia McGaffigan, RN, MS, CPPS
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Healthcare Solutions Nuance Clintegrity Quality Management Solutions. Quality. The Discipline to Win.
 Quality. The Discipline to Win. Brochure 2 It s not wanting to win that makes you a winner; it s refusing to fail. Peyton Manning, the first NFL quarterback to achieve 200 career wins (regular and post-season)
Quality. The Discipline to Win. Brochure 2 It s not wanting to win that makes you a winner; it s refusing to fail. Peyton Manning, the first NFL quarterback to achieve 200 career wins (regular and post-season)
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Never Events (Including Retained Foreign Objects) The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI
 The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI") Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Doctor in the Cockpit
 Doctor in the Cockpit Diffusion of aviation innovations in hospitals Dirk F. de Korne, PhD MSc Deputy Director, Health Innovation Assistant Professor, Health Services Management & Organisation Singapore
Doctor in the Cockpit Diffusion of aviation innovations in hospitals Dirk F. de Korne, PhD MSc Deputy Director, Health Innovation Assistant Professor, Health Services Management & Organisation Singapore
Patient Safety in Resource Poor Settings
 Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Lesson 9: Medication Errors
 Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
2. Why Applying Human Factors Is Important For Patient Safety
 PATIENT SAFETY 436 TEAM 2. Why Applying Human Factors Is Important For Patient Safety Objectives: Understand Human Factors And Its Relationship To Patient Safety Define The Meaning Of The Term Human Factors
PATIENT SAFETY 436 TEAM 2. Why Applying Human Factors Is Important For Patient Safety Objectives: Understand Human Factors And Its Relationship To Patient Safety Define The Meaning Of The Term Human Factors
Measurability of Patient Safety
 Measurability of Patient Safety Marsha Fleischer IMPO Conference, November 17, 2016 External requirements in Germany lead to a higher need for safety and risk management, among others arising from the:
Measurability of Patient Safety Marsha Fleischer IMPO Conference, November 17, 2016 External requirements in Germany lead to a higher need for safety and risk management, among others arising from the:
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement. Patty Austin, RN, CPHQ Project Coordinator
 QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement Patty Austin, RN, CPHQ Project Coordinator QA + PI = QAPI QAPI takes a systematic, comprehensive, and data-driven
QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement Patty Austin, RN, CPHQ Project Coordinator QA + PI = QAPI QAPI takes a systematic, comprehensive, and data-driven
Crane Bashes Pipes. Lessons Learned. Volume 03 Issue USW
 Crane Bashes Pipes Lessons Learned Volume 03 Issue 13 2004 USW Crane Bashes Pipes Purpose To conduct a small group lessons learned activity to share information gained from incident investigations. To
Crane Bashes Pipes Lessons Learned Volume 03 Issue 13 2004 USW Crane Bashes Pipes Purpose To conduct a small group lessons learned activity to share information gained from incident investigations. To
Leadership for Quality A Strategy for Marketplace Success. Requirements for Transformation. Typical State of Shared Vision. It All Starts With Urgency
 Virginia Mason Medical Center Leadership for Quality A Strategy for Marketplace Success Estes Park Institute January 2012 Gary S. Kaplan, MD, Chairman and CEO Virginia Mason Medical Center Seattle, Washington
Virginia Mason Medical Center Leadership for Quality A Strategy for Marketplace Success Estes Park Institute January 2012 Gary S. Kaplan, MD, Chairman and CEO Virginia Mason Medical Center Seattle, Washington
Measure what you treasure: Safety culture mixed methods assessment in healthcare
 BUSINESS ASSURANCE Measure what you treasure: Safety culture mixed methods assessment in healthcare DNV GL Healthcare Presenter: Tita A. Listyowardojo 1 SAFER, SMARTER, GREENER Declaration of interest
BUSINESS ASSURANCE Measure what you treasure: Safety culture mixed methods assessment in healthcare DNV GL Healthcare Presenter: Tita A. Listyowardojo 1 SAFER, SMARTER, GREENER Declaration of interest
Practical Approaches to Establishing a Culture of Safety*
 Practical Approaches to Establishing a Culture of Safety* Leading the Transformation to High-Reliability Care IHI National Forum 8 December 2014 Gregg S. Meyer, MD, MSc Chief Clinical Officer, Partners
Practical Approaches to Establishing a Culture of Safety* Leading the Transformation to High-Reliability Care IHI National Forum 8 December 2014 Gregg S. Meyer, MD, MSc Chief Clinical Officer, Partners
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Commonwealth Nurses Federation. A Safe Patient. Jill ILIFFE Executive Secretary. Commonwealth Nurses Federation
 A Safe Patient Jill ILIFFE Executive Secretary Commonwealth Nurses Federation INFECTION CONTROL Every patient encounter should be viewed as potentially infectious Standard Precautions 1. Hand hygiene 2.!
A Safe Patient Jill ILIFFE Executive Secretary Commonwealth Nurses Federation INFECTION CONTROL Every patient encounter should be viewed as potentially infectious Standard Precautions 1. Hand hygiene 2.!
Text-based Document. Building a Culture of Safety: Aligning innovative leadership rounding and staff driven hourly rounding strategies
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Section 5 General Policies Work, Health and Safety Policy. The Gums Childcare Centre Policies
 The Gums Childcare Centre Policies Section 5 General Policies 3.14 Work, Health and Safety Policy Background 1. The Gums Childcare Centre is committed to ensuring a safe and healthy working and learning
The Gums Childcare Centre Policies Section 5 General Policies 3.14 Work, Health and Safety Policy Background 1. The Gums Childcare Centre is committed to ensuring a safe and healthy working and learning
Pars Oil & Gas Company HEALTH, SAFETY AND ENVIRONMENT PROCEDURE. HSE Anomaly Reporting Procedure DOCUMENT ID - PR-74-POGC-002 REVISION 0.
 Pars Oil & Gas Company HSE Anomaly Reporting Procedure HEALTH, SAFETY AND ENVIRONMENT PROCEDURE HSE Anomaly Reporting Procedure DOCUMENT ID - PR-74-POGC-002 REVISION 0.0 Pars Oil & Gas Company Pages 14
Pars Oil & Gas Company HSE Anomaly Reporting Procedure HEALTH, SAFETY AND ENVIRONMENT PROCEDURE HSE Anomaly Reporting Procedure DOCUMENT ID - PR-74-POGC-002 REVISION 0.0 Pars Oil & Gas Company Pages 14
Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant
 Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant Today s presentation is an overview of the Investigating Workplace
Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant Today s presentation is an overview of the Investigating Workplace
Delivering Great Care with High Reliability
 FE4 These presenters have nothing to disclose Delivering Great Care with High Reliability The Orlando Health Journey December 5, 2016 Joelle Baehrend, MA Director, Institute of Healthcare Improvement 1
FE4 These presenters have nothing to disclose Delivering Great Care with High Reliability The Orlando Health Journey December 5, 2016 Joelle Baehrend, MA Director, Institute of Healthcare Improvement 1
BETHESDA HEALTH. Commitment to Care: Partnering with Care Logistics to Adopt a Patient-First System for Care
 BETHESDA HEALTH Commitment to Care: Partnering with Care Logistics to Adopt a Patient-First System for Care Success Snapshot Commitment to Care transformation initiative has driven $11 million in annual
BETHESDA HEALTH Commitment to Care: Partnering with Care Logistics to Adopt a Patient-First System for Care Success Snapshot Commitment to Care transformation initiative has driven $11 million in annual
Text-based Document. The Culture of Incident Reporting Among Filipino Nurses. de Guzman, Barbara Michelle. Downloaded 28-Apr :54:41
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Frequently Asked Questions from New Authors
 Frequently Asked Questions from New Authors As the official journal of the Infusion Nurses Society, the Journal of Infusion Nursing is committed to advancing the specialty of infusion therapy by publishing
Frequently Asked Questions from New Authors As the official journal of the Infusion Nurses Society, the Journal of Infusion Nursing is committed to advancing the specialty of infusion therapy by publishing
RCA in Healthcare 3/23/2017. Why Root Cause Analysis is Performed. Root Cause Analysis in Healthcare Part - 1. Contd. Contd.
 Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis