High Reliability Organizations Healing Without Harm by 2014
|
|
|
- Earl Montgomery
- 5 years ago
- Views:
Transcription

1 Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by
2 Stand up if You have suffered harm as a patient at a hospital or other care facility (an infection, fall, a delayed diagnosis causing delay in treatment, other ) A family member has suffered harm in a hospital or other care facility A friend or colleague has suffered harm in a hospital or other care facility You have had to disclose harm or otherwise handle the situation when a patient was harmed in your hospital or other care facility 2
3 AGENDA Objectives Five Principles of HRO Facts about Errors How do Serious Safety Events Occur Anatomy of a Serious Safety Event Error Prevention Techniques Leadership Methods 3
4 Why we re here. Our mission calls us to deliver holistic care. For Ascension Health, holistic care means caring for the physical, emotional, social, and spiritual well-being of the whole person by: Attending to the spirit through compassionate relationships and empathetic, effective communication. Inviting shared decision making among patients, providers and care teams. Delivering safe, reliable, evidence-based, and interdisciplinary care consistent with individual preferences. 4
5 Healing without Harm by 2014 Timeline FY10: Foundation FY11: Immersion FY12: Accountability FY13: Sustainability FY14: Sustainable Achievement By the end of FY10, 100% of the targeted hospitals (N=66) will have established a baseline* for Serious Safety Events. By the end of FY11, 100% of the targeted hospitals will be reporting Serious Safety Event rates and 75% will have begun training (leaders/ Associates and/or active medical staff). By the end of FY12, 75% (50) of the 66 targeted hospitals will have completed training of leaders, Associates, and active medical staff. By the end of FY13, the overall Ascension Health Serious Safety Event rate is reduced by 15% from true baseline. By the end of FY14, the overall Ascension Health Serious Safety Event rate is reduced by 40% from true baseline.
6 Commercial Aviation 1935 Advent of the checklist 1945 Fitts & Jones study of cockpit design Source: Boeing, 2007 Statistical Summary, July 2008

7 Naval Aviation Mishap Rate aircraft destroyed in 1954 Mishap rates per 100,000 flight hours USN/USMC, FY aircraft destroyed in Source: ORM Flight Mishap Rate
 finding or performance indicator.")
8 Significant Events at US Nuclear Plants Annual Industry Average, Fiscal Year Significant Events are those events that the NRC staff identifies for the Performance Indicator Program as meeting one or more of the following criteria: A Yellow or Red Reactor Oversight Process (ROP) finding or performance indicator. An event with a Conditional Core Damage Probability (CCDP) or increase in core damage probability (ΔCDP) of 1x10-5 or higher. An Abnormal Occurrence as defined by Management Directive 8.1, Abnormal Occurrence Reporting Procedure. An event rated two or higher on the International Nuclear Event Scale. Source: Nuclear Regulatory Commission Information Digest (1988 is earliest year data is available) Updated: November 2007
 ISAR = Number of accidents resulting in lost work, restricted work, or fatalities per 200,000 worker hours.")
9 Industrial Safety Accident Rate One-Year Nuclear Utility Industry Values Healthcare = 7.1 (2007) ISAR = Number of accidents resulting in lost work, restricted work, or fatalities per 200,000 worker hours. Note: Starting in 2008, data includes supplemental personnel. Source: World Association of Nuclear Operators, Updated: 4/09
10 Nuclear-Powered Submarines 5,500 cumulative years of nuclear reactor operations. 127 million miles submerged (265 round trips to moon). Zero reactor accidents. Operated by 20 year olds.
 Ultra Safe (<1/100K) 10,000 Health Care (1 of ~600) Driving In US Total lives lost per year 1,000 100 10 Mountaineering Chartered Flights Scheduled")
11 How Safe is Healthcare? 100,000 Dangerous (>1/1,000) Ultra Safe (<1/100K) 10,000 Health Care (1 of ~600) Driving In US Total lives lost per year 1, Mountaineering Chartered Flights Scheduled Commercial Airlines European Railroads 1 Bungee Jumping Chemical Manufacturing Nuclear Power ,000 10, K 1M 10M Number of encounters for each fatality

12 Reliability from the patient s perspective Don't kill me (no needless deaths). Do help me and don't hurt me (no needless pain). Don't make me feel helpless. Don't keep me waiting. Don t waste resources - mine or anyone else's. SAFETY + Quality + Satisfaction = Exceptional Care Berwick, Donald. My Right Knee. Ann Intern Med, January 18, 2005, Volume142, no2,
13 Healing without Harm by 2014 Healing without Harm by 2014 is a destination in quality, safety, and experience for patients and caregivers. This destination is possible through the principles and practices of high reliability. 13
14 Five Principles of HROs Three Principles of Anticipation Preoccupation with Failure Remaining alert to small, inconsequential errors as a symptom that something s wrong. Sensitivity to Operations Paying attention to what s happening on the front-line. Reluctance to Simplify Interpretations Encouraging diversity in experience, perspective, and opinion. 14


15 Five Principles of HROs Two Principles of Containment Commitment to Resilience Developing capabilities to detect, contain, and bounce-back from events that do occur. Deference to Expertise Pushing decision making down and around to the person with the most directly related knowledge and expertise. 15

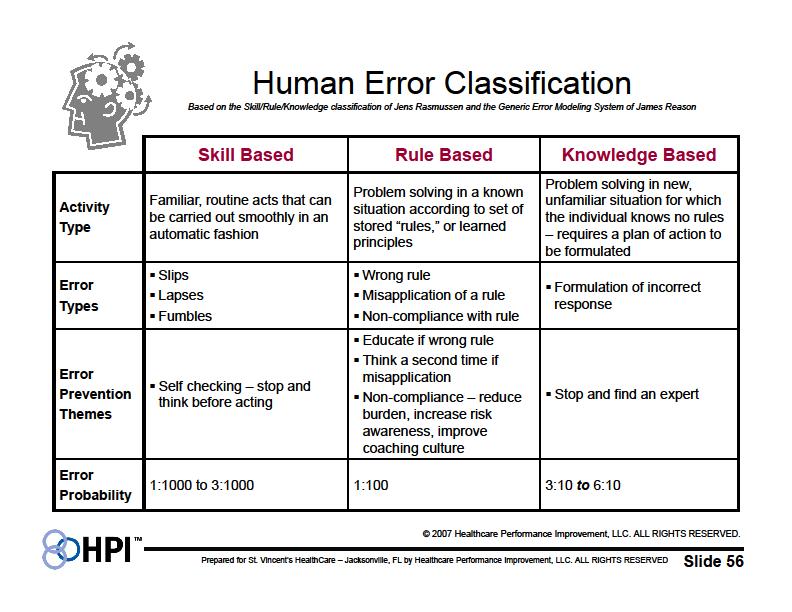
16 Facts about Errors 1. Everyone makes errors even very experienced people. 2. We work in high-risk situations that increase the chance we will make an error. 3. We can avoid most errors by practicing low-risk behaviors. 16 Source: Institute of Nuclear Power Operations
17 Facts about Errors 4. Culture affects how we behave, and our behaviors determine outcomes. 5. Most near-misses and significant events are due to system or process problems. System Failure Modes Ascension Health (67 hospital) % Structure 14% Culture 49% Process 21% Policy & Protocol Technology & Environment 11% 5% 17 Source: Institute of Nuclear Power Operations
18 Typical Improvement Curve
19 3.19
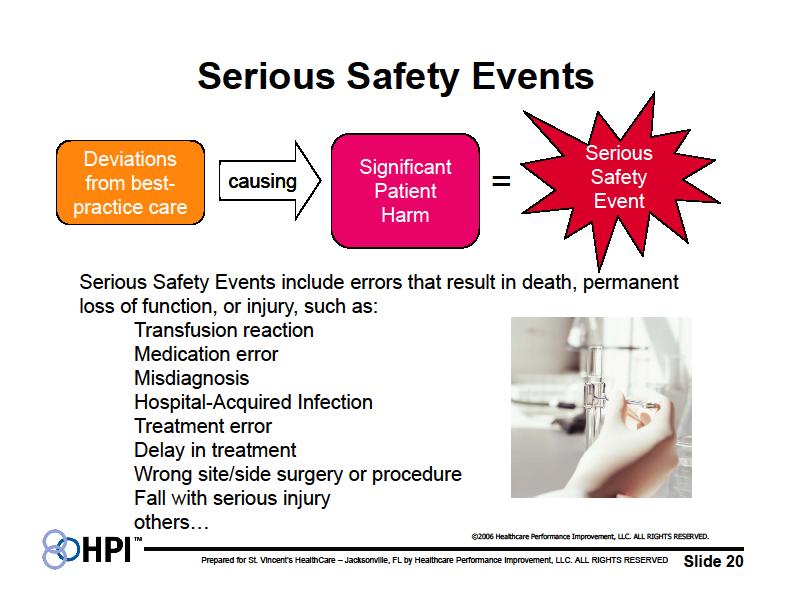
20 20



21 A deviation from generally accepted performance standards (GAPS) that Serious Safety Event Reaches the patient and Results in moderate harm to severe harm or death Precursor Safety Event Reaches the patient and Results in minimal harm or no detectable harm Serious Safety Events Precursor Safety Events Near Miss Safety Event Does not reach the patient Error is caught by a detection barrier or by chance Near Miss Safety Event 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED. 21
22 22

23 How do serious safety events occur? High Risk Situation High Risk + = Behavior Safety Event 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED. 23
24 24
25 25
26 26
27 27
28 28
29 29
30 30
31 31
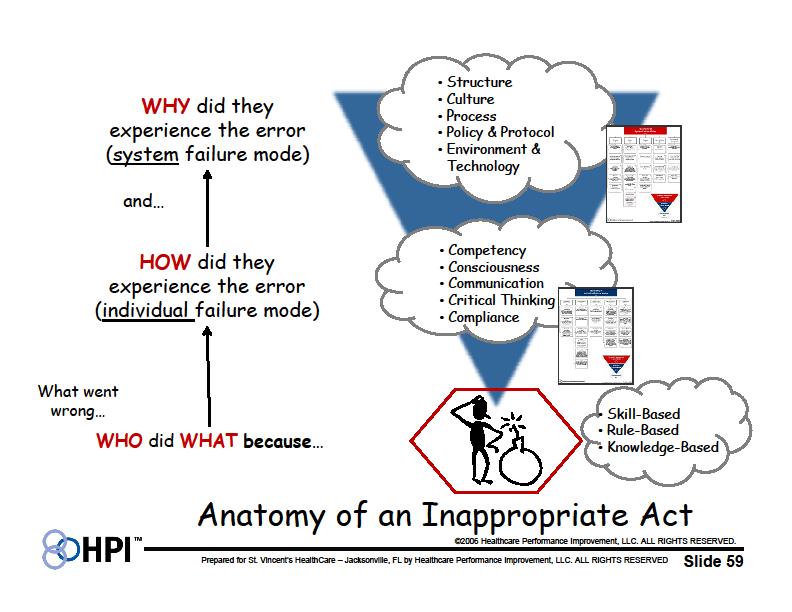
32 The Anatomy of an Event Multiple Barriers In technology, processes, and people - designed to stop active errors (our defense in depth ) Events of Harm Active Errors By individuals result in initiating action(s) Prevent The errors Detect & Correct The system weakness Latent Weakness In barriers 32 Adapted from James Reason, Managing the Risks of Organizational Accidents (1997)

33 Care Management Barriers to prevent event fall The patient requested privacy while up to BR; found unresponsive with fracture and permanent mental status changes. Fall with injury Nurse did not provide PCT with guidance on Patient being up with assistance. PCT did not assure visual of pt who was up to BR Physician wrote standard order (using order sheet) for pt at significant risk for falls Nurse did not further clarify physician order up to BR with assistance. Care team did not know the extent of patient s risk for falls falls assessment was documented post fall. 33




34 Three Things We Must Do to Eliminate or Reduce Unwanted Events Find holes by DETECTION 2 3 Reduce the size or eliminate the holes by CORRECTION STOP Reduce Initiating Actions by PREVENTION 1 STOP Detection and Correction 50% decrease in events every 2 years 34 Adapted from James Reason, Managing the Risks of Organizational Accidents (1997)
35 Error Prevention for Staff EXPECTATIONS I am accountable for : 1. Patient, Personal and Peer Safety I will demonstrate an open, personal and co-worker (200%) commitment to safety 2. Clear & Complete Communications I am personally responsible for professional, accurate, clear and timely verbal and written communications TECHNIQUES I will: 1. Practice peer checking & coaching using ARCC 2. Stop and resolve in the face of uncertainty 1. Include the "5P Handoff process when transferring & sharing patient care responsibility 2. Use SBAR to communicate patient concerns 3. Use Repeat-Backs and Read-backs with 1 or 2 Clarifying Questions 4. Document legibly 3. Paying Attention to Detail 1. Practice S.T.A.R. I will attend carefully to important details 35

36 What is a RED RULE? An act that has the highest level of risk or consequence to patient or employee safety if not performed exactly, each and every time Red designates the highest priority for exact compliance STOP action if you can t comply 36
37 Red Rules Defining red rules. Red rules are rules that cannot be broken. Example of a red rule in everyday life. The use of seatbelts while riding in an automobile could serve as an example of a red rule that everyone should follow in everyday life. Red rule criteria. It must be possible and desirable for everyone to follow a red rule every time in a process under all circumstances (red rules should not contain verbiage such as except when or each breach will be assessed for appropriateness ) Summary. Red rules have the potential to promote an organizational culture of safety that shares accountability for the safe delivery of patient care.
38 Patient Identifiers Specimen Labeling Red Rule Basis/Intent: To promote a culture of patient safety by ensuring individuals are reliably identified as the individual for whom the service or treatment is intended, also to match the service or treatment to the individual. Red Rule Expectations: Employees will use at least twopatient identifiers (Name and date of birth) Red Rule Basis/Intent: To promote a culture of patient safety by ensuring specimens are properly and accurately labeled. Red Rule Expectations: Employees will label all specimens at the bedside in front of the patient Red Rule Violations: Individuals found in breach of red rules will be disciplined in the following progression: 1st offence- Written-counseling to be placed in personnel file 2nd offence- Suspension of employment 3rd offence- Termination of employment
 Handoffs 5 Ps SBAR")

39 Error Prevention Techniques Recommended Techniques for All Team Checking/Team Coaching (ARCC) Handoffs 5 Ps SBAR Read-backs/Repeat-backs with Clarifying Questions Document Legibly and Accurately Stop and Resolve Self-Checking with STAR 39
40 Patient, Personal, and Peer Safety A responsibility to protect in a manner of mutual respect an assertion and escalation technique With ARCC use the lightest touch possible Ask a question Make a Request Voice a Concern If no success Use Chain of Command A Safety Phrase: I have a concern Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
41 Clear, Concise and Complete Communications The Five Ps A Simple Responsibility Change Checklist I own it until I hand it off to an appropriate person. An effective handoff includes the 5 Ps: Patient or Project what is to be handed off Plan what is to happen next Purpose (of the plan) the desired end state Problems what problems you have encountered with this patient or what is known to be different, unusual, or complicating about this patient or project Precautions what you are or would be concerned about or what could be expected to be different, unusual, or complicating about this patient or project Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
42 Techniques Practice - Instructions Work with a partner. Review the scenario (on next screen). Apply the 5 Ps technique. Partner A explains what they would say in this situation using the 5 P technique at the time of transfer assessment. Partner B suggests improvements. Share any best practices or examples you have that relate to this technique. 42
43 Practice Activity: 5 P Scenario A 55-year-old female with a very complex medical condition is admitted for a femoral artery bypass graft. Following this procedure, she is transferred to the ICU with an arterial line in place. Due to an incomplete transfer assessment, the patient s arterial line is not connected to a monitor as required. The arterial line remains disconnected from the monitoring device for more than 12 hours. At shift change, the nurse assuming care of the patient notices this. The patient remains unstable during much of the recovery period. Fortunately, no harm results from the 12 hour period that the arterial line was not attached to the monitor. 43

44 Leadership Methods Reinforce & Build Accountability Rounding to Influence Walking Rounds 5:1 Feedback Fair & Just Accountability Red Rules for Safety Daily Check-In Find & Fix Problems Pre-Task Brief After Action Review Rapid Response to Safety Critical Issues Top Ten Problem List with Problem Owners & Action Plans Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
45 Benefits of a Daily Check-In Leadership Awareness For the senior leader: awareness of what s happening at the front line by staying in touch with your people For operational leaders: awareness of what s going on in other areas and cross-department impact Mental organization a chance to plan your day Problem Identification & Resolution Early notification of issues Breaking down silos all directors to pool ideas and resources in solving problems and potential problems Accountability for Safety Talking about perfect care has become easier more aggressive in leadership for Zero events Dialogue about how we are at risk, how we can reduce our risk, and how we can support each other Transparency A patient fell on my unit last night and broke an ankle 45

46 START HERE Leadership Daily Check-In Happens every day 15 minutes Face-to-face or by phone Always led by senior leader Every leader comes prepared Problems are assigned owners EVOLVE OVER TIME Unit Daily Check-In Happens every day 15 minutes Face-to-face on unit Always led by unit leader Staff come prepared Problems are assigned owners 46
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
SafetyFirst: The Journey to High Reliability
 SafetyFirst: The Journey to High Reliability Course Audio Transcript Module 1: Navigating SafetyFirst: The Journey to High Reliability Welcome Welcome to SafetyFirst: The Journey to High Reliability. This
SafetyFirst: The Journey to High Reliability Course Audio Transcript Module 1: Navigating SafetyFirst: The Journey to High Reliability Welcome Welcome to SafetyFirst: The Journey to High Reliability. This
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Creating a Highly Reliable Health System: the Leadership Challenge. 6 th Annual Patient Safety Symposium Rick Foster, MD
 Creating a Highly Reliable Health System: the Leadership Challenge 6 th Annual Patient Safety Symposium Rick Foster, MD April 18, 2013 Moving Toward Zero It may seem a strange principle to enunciate as
Creating a Highly Reliable Health System: the Leadership Challenge 6 th Annual Patient Safety Symposium Rick Foster, MD April 18, 2013 Moving Toward Zero It may seem a strange principle to enunciate as
Patient Safety. Annual Accidental Deaths. Medical Errors in History. How Hazardous Is Health Care (Amalberti)
") Patient Safety Annual Accidental Deaths 100000 90000 80000 70000 60000 50000 40000 30000 20000 10000 0 Medical Auto Workplace Air Deaths Total lives lost per year How Hazardous Is Health Care (Amalberti)
Patient Safety Annual Accidental Deaths 100000 90000 80000 70000 60000 50000 40000 30000 20000 10000 0 Medical Auto Workplace Air Deaths Total lives lost per year How Hazardous Is Health Care (Amalberti)
CROSSING THE QUALITY CHASM: HEALTH CARE FOR THE 21 ST CENTURY
 CROSSING THE QUALITY CHASM: HEALTH CARE FOR THE 21 ST CENTURY May 10, 2002 Donald M. Berwick, M.D. President & CEO Institute for Healthcare Improvement The Foundation IOM Roundtable President s Advisory
CROSSING THE QUALITY CHASM: HEALTH CARE FOR THE 21 ST CENTURY May 10, 2002 Donald M. Berwick, M.D. President & CEO Institute for Healthcare Improvement The Foundation IOM Roundtable President s Advisory
Patient Safety in Resource Poor Settings
 Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
To Err is Human To Delay is Deadly Ten years later, a million lives lost, billions of dollars wasted
 1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
From Value to High-Reliability Organization
 From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
TIME OUT! A Patient Safety Strategy. Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service
 TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
SBAR Communication Tool. Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme
 Clinical Risk Advisor, Clinical Indemnity Scheme") SBAR Communication Tool Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme Background Communication Tools What is SBAR SBAR in action
SBAR Communication Tool Anne Marie Oglesby RGN., MSc. Health Care (Risk Management & Quality) Clinical Risk Advisor, Clinical Indemnity Scheme Background Communication Tools What is SBAR SBAR in action
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE IMMEDIATE MANAGEMENT OF CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT
TITLE IMMEDIATE MANAGEMENT OF CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT
Kate Beaumont. Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign.
 Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Leadership for Transforming Health Care
 Presenters have nothing to disclose. Leadership for Transforming Health Care Partnerships with Patients and Families Barbara Balik, RN, EdD Kris White, RN, MBA November 4, 2014 This presenter has nothing
Presenters have nothing to disclose. Leadership for Transforming Health Care Partnerships with Patients and Families Barbara Balik, RN, EdD Kris White, RN, MBA November 4, 2014 This presenter has nothing
High Reliability. How to Significantly Improve Safety Systems Using HRO Methodology
 High Reliability How to Significantly Improve Safety Systems Using HRO Methodology Tom Peterson, MD VP, Chief Safety Officer SCL Health April 15, 2015 Sisters of Charity of Leavenworth Health System, Inc.
High Reliability How to Significantly Improve Safety Systems Using HRO Methodology Tom Peterson, MD VP, Chief Safety Officer SCL Health April 15, 2015 Sisters of Charity of Leavenworth Health System, Inc.
COOK COUNTY HEALTH & HOSPITALS SYSTEM
 COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Nursing Documentation 101
 Nursing Documentation 101 Module 5: Applying Knowledge Part I Handout 2014 College of Licensed Practical Nurses of Alberta. All Rights Reserved. Nursing Documentation 101 Module 5: Applying Knowledge Part
Nursing Documentation 101 Module 5: Applying Knowledge Part I Handout 2014 College of Licensed Practical Nurses of Alberta. All Rights Reserved. Nursing Documentation 101 Module 5: Applying Knowledge Part
Sharp HealthCare s HRO Commitment
 Sharp HealthCare s HRO Commitment Daniel L. Gross, DNSc, RN Executive Vice President Amy Adome, MD, MPH Senior Vice President, Clinical Effectiveness November 3, 2016 Perfection is not attainable, but
Sharp HealthCare s HRO Commitment Daniel L. Gross, DNSc, RN Executive Vice President Amy Adome, MD, MPH Senior Vice President, Clinical Effectiveness November 3, 2016 Perfection is not attainable, but
Translational Safety Through Immersive Learning: Practice What you Preach
 Translational Safety Through Immersive Learning: Practice What you Preach Gregory Botz, MD, FCCM Professor, Department of Critical Care Division of Anesthesiology and Critical Care The University of Texas,
Translational Safety Through Immersive Learning: Practice What you Preach Gregory Botz, MD, FCCM Professor, Department of Critical Care Division of Anesthesiology and Critical Care The University of Texas,
Strange Strategy and Change. HRO High Reliability Organizing
 HRO High Reliability Organizing Program 14.00u Dialogue versus Discussion HRO condition 1: Informed culture 14.15u A real life situation: the Intensive Care Unit at the OLVG An introduction to all 4 HRO
HRO High Reliability Organizing Program 14.00u Dialogue versus Discussion HRO condition 1: Informed culture 14.15u A real life situation: the Intensive Care Unit at the OLVG An introduction to all 4 HRO
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM
 Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
ICT and ID Management in the health sector. Dr. Susann Roth Senior Social Development Specialist
 ICT and ID Management in the health sector Dr. Susann Roth Senior Social Development Specialist 19 September 2016 Key Points ICT investments need to be made beyond one sector. Strong business case in the
ICT and ID Management in the health sector Dr. Susann Roth Senior Social Development Specialist 19 September 2016 Key Points ICT investments need to be made beyond one sector. Strong business case in the
High Reliability Organizations The Key to Improving Quality and Safety
 High Reliability Organizations The Key to Improving Quality and Safety William B Munier, MD, MBA Acting Director Center for Quality Improvement and Patient Safety Agency for Healthcare Research and Quality
High Reliability Organizations The Key to Improving Quality and Safety William B Munier, MD, MBA Acting Director Center for Quality Improvement and Patient Safety Agency for Healthcare Research and Quality
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Background on NCH. 3
 1 2 Background on NCH. 3 Picture of where NCH sits in relation to the city of Columbus. 4 New replacement hospital being built with two floors opening in 2011 and the entire hospital opening in 2012. 5
1 2 Background on NCH. 3 Picture of where NCH sits in relation to the city of Columbus. 4 New replacement hospital being built with two floors opening in 2011 and the entire hospital opening in 2012. 5
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Table of Contents. TeamSTEPPS Framework and Competencies Key Principles. Team Structure Multi-Team System For Patient Care
 Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Fostering a Culture of Safety
 Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Checklist: What Can My Organization Do?
 Checklist: What Can My Organization Do? 2 Introduction About The Framework This is an evidence and consensus-based framework for successful clinical outcomes in long term and post-acute care. The framework
Checklist: What Can My Organization Do? 2 Introduction About The Framework This is an evidence and consensus-based framework for successful clinical outcomes in long term and post-acute care. The framework
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
Leadership Forum: Promoting a Culture of Safety
 Leadership Forum: Promoting a Culture of Safety Dates: 5/10, 5/13 and 5/14 (Note: All sessions at the InterContinental Hotel) Times: 4-hour sessions (Note: Participants only attend 1 session) o Morning
Leadership Forum: Promoting a Culture of Safety Dates: 5/10, 5/13 and 5/14 (Note: All sessions at the InterContinental Hotel) Times: 4-hour sessions (Note: Participants only attend 1 session) o Morning
TrainingABC Patient Rights Made Simple Support Materials
 TrainingABC 2017 Patient Rights Made Simple Support Materials Video Transcript The Patient Bill of Rights is a list of rights first developed in 1973 and then revised in 1992, by the American Hospital
TrainingABC 2017 Patient Rights Made Simple Support Materials Video Transcript The Patient Bill of Rights is a list of rights first developed in 1973 and then revised in 1992, by the American Hospital
STANDARDS Point-of-Care Testing
 STANDARDS Point-of-Care Testing For Surveys Starting After: January 1, 2018 Date Generated: January 12, 2017 Point-of-Care Testing Published by Accreditation Canada. All rights reserved. No part of this
STANDARDS Point-of-Care Testing For Surveys Starting After: January 1, 2018 Date Generated: January 12, 2017 Point-of-Care Testing Published by Accreditation Canada. All rights reserved. No part of this
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE DISCLOSURE OF HARM SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND NUMBER
TITLE DISCLOSURE OF HARM SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND NUMBER
Shifting from Blame-&-Shame to a Just-and-Safe Culture
 Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
The Milestones provide a framework for the assessment
 The Transitional Year Milestone Project The Milestones provide a framework for the assessment of the development of the resident physician in key dimensions of the elements of physician competency in a
The Transitional Year Milestone Project The Milestones provide a framework for the assessment of the development of the resident physician in key dimensions of the elements of physician competency in a
Creating a Culture in Support of Patient Safety
 Session: L11 Ms. Ching has nothing to disclose Ms. Derheimer is an employee of the Virginia Mason Institute; a not-for-profit organization that provides education and training in the Virginia Mason Production
Session: L11 Ms. Ching has nothing to disclose Ms. Derheimer is an employee of the Virginia Mason Institute; a not-for-profit organization that provides education and training in the Virginia Mason Production
Merced College Registered Nursing 34: Advanced Medical/Surgical Nursing and Pediatric Nursing
 Merced College Registered Nursing 34: Advanced Medical/Surgical Nursing and Pediatric Nursing Course Description, Student Learning Outcomes and Competencies, Clinical Evaluation Tool, and Clinical Activities
Merced College Registered Nursing 34: Advanced Medical/Surgical Nursing and Pediatric Nursing Course Description, Student Learning Outcomes and Competencies, Clinical Evaluation Tool, and Clinical Activities
COMMON FACTORS CHECKLIST
 COMMON FACTORS CHECKLIST For Identifying Causes and Contributory Factors When attempting to identify potential causes and contributory factors related to an incident or system failure review the following
COMMON FACTORS CHECKLIST For Identifying Causes and Contributory Factors When attempting to identify potential causes and contributory factors related to an incident or system failure review the following
10 Things To Know About
 10 Things To Know About Nurse Call 100% Nurse Approved 10 Things to Know About Nurse Call in 2016 Nurse call systems have evolved. Today s nurse call systems provide front-line nurses with critical communications
10 Things To Know About Nurse Call 100% Nurse Approved 10 Things to Know About Nurse Call in 2016 Nurse call systems have evolved. Today s nurse call systems provide front-line nurses with critical communications
What Every Patient Safety Officer Must Know:
 What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
9/8/2014. I have no conflicts of interest to disclose. Conflict of Interest Disclosure. Carrie Brunson: Except
 ENSURING OPIOID SAFETY: DO OUR NURSES POSSESS THE KNOWLEDGE Click to add subtitle TO RESCUE PATIENTS? Carrie Brunson MSN, APRN-BC, ACNS-BC Clinical Nurse Specialist Acute Pain Service September 2014 ASPMN
ENSURING OPIOID SAFETY: DO OUR NURSES POSSESS THE KNOWLEDGE Click to add subtitle TO RESCUE PATIENTS? Carrie Brunson MSN, APRN-BC, ACNS-BC Clinical Nurse Specialist Acute Pain Service September 2014 ASPMN
Patient Safety (PS) 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.
 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.") Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
PATIENT SERVICES POLICY AND PROCEDURE MANUAL
 SECTION Patient Services Manual Multidiscipline Section NAME Patient Rights and Responsibilities PATIENT SERVICES POLICY AND PROCEDURE MANUAL EFFECTIVE DATE 8-1-11 SUPERSEDES DATE 7-20-10 I. PURPOSE To
SECTION Patient Services Manual Multidiscipline Section NAME Patient Rights and Responsibilities PATIENT SERVICES POLICY AND PROCEDURE MANUAL EFFECTIVE DATE 8-1-11 SUPERSEDES DATE 7-20-10 I. PURPOSE To
8/10/2015. Module 1. A Fundamental Understanding of Quality. Management and its Application to Health Care
 Module 1 A Fundamental Understanding of Quality Management and its Application to Health Care Addressing Physician Uncertainty about Payment Reform: Skills for Success in Value-Based Delivery Systems The
Module 1 A Fundamental Understanding of Quality Management and its Application to Health Care Addressing Physician Uncertainty about Payment Reform: Skills for Success in Value-Based Delivery Systems The
HOSPICE CONTRACTING CHECKLIST FOR INPATIENT SERVICES, RESPITE CARE AND VENDOR AGREEMENTS
 HOSPICE CONTRACTING CHECKLIST FOR INPATIENT SERVICES, RESPITE CARE AND VENDOR AGREEMENTS The following checklist can be used to verify that the regulatory requirements are addressed in hospice contracts
HOSPICE CONTRACTING CHECKLIST FOR INPATIENT SERVICES, RESPITE CARE AND VENDOR AGREEMENTS The following checklist can be used to verify that the regulatory requirements are addressed in hospice contracts
Keeping Kids Safe TeamSTEPPS Essentials
 Keeping Kids Safe TeamSTEPPS Essentials TeamSTEPPS Leadership Team Michelle (Mickey) Ryerson, DNP, RN, NEA BC Glen Medellin, MD Michelle Arandes, MD Stacey Denver, DNP, FNP BC Rachael Bridwell, MSN, RN
Keeping Kids Safe TeamSTEPPS Essentials TeamSTEPPS Leadership Team Michelle (Mickey) Ryerson, DNP, RN, NEA BC Glen Medellin, MD Michelle Arandes, MD Stacey Denver, DNP, FNP BC Rachael Bridwell, MSN, RN
Practical Application of High Reliability Principles in Healthcare to Promote Clinical Quality and Safety Outcomes
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Culture. Safety. Process. Culture of Safety and Improvement
 Culture Safety Process Culture of Safety and Improvement Objectives Define key elements in a Culture of Safety Describe your role in the culture and process of safety Identify three personal actions to
Culture Safety Process Culture of Safety and Improvement Objectives Define key elements in a Culture of Safety Describe your role in the culture and process of safety Identify three personal actions to
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
BETHESDA HEALTH. Commitment to Care: Partnering with Care Logistics to Adopt a Patient-First System for Care
 BETHESDA HEALTH Commitment to Care: Partnering with Care Logistics to Adopt a Patient-First System for Care Success Snapshot Commitment to Care transformation initiative has driven $11 million in annual
BETHESDA HEALTH Commitment to Care: Partnering with Care Logistics to Adopt a Patient-First System for Care Success Snapshot Commitment to Care transformation initiative has driven $11 million in annual
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND
TITLE CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND
CUMBERLAND COUNTY COLLEGE
 CUMBERLAND COUNTY COLLEGE Course: HS 105 Introduction to Athletic Training Credits: 2 Prerequisites None Course Description This course is designed as an initial experience for students considering a career
CUMBERLAND COUNTY COLLEGE Course: HS 105 Introduction to Athletic Training Credits: 2 Prerequisites None Course Description This course is designed as an initial experience for students considering a career
Tufts Medical Center: Falls Prevention Education
 Tufts Medical Center: Falls Prevention Education Purpose of Tufts Medical Center s Fall Program Minimize the number of patient, visitor and employee falls Minimize injuries related to falls Promote an
Tufts Medical Center: Falls Prevention Education Purpose of Tufts Medical Center s Fall Program Minimize the number of patient, visitor and employee falls Minimize injuries related to falls Promote an
Root Cause Analysis Handbook A Guide To. Efficient And Effective Incident Investigation Pdf
 Root Cause Analysis Handbook A Guide To Efficient And Effective Incident Investigation Pdf Download: Root Cause Analysis Handbook: A Guide to Efficient and Effective Incident Investigation (Third Edition).
Root Cause Analysis Handbook A Guide To Efficient And Effective Incident Investigation Pdf Download: Root Cause Analysis Handbook: A Guide to Efficient and Effective Incident Investigation (Third Edition).
Are National Indicators Useful for Improvement Work? Exercises & Worksheets
 Session L5 These presenters have nothing to disclose These presenters have nothing to disclose Are National Indicators Useful for Improvement Work? Exercises & Worksheets Robert Lloyd, PhD Göran Henriks,
Session L5 These presenters have nothing to disclose These presenters have nothing to disclose Are National Indicators Useful for Improvement Work? Exercises & Worksheets Robert Lloyd, PhD Göran Henriks,
Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa
 Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa Developed by the Undergraduate Education and Training Subcommittee
Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa Developed by the Undergraduate Education and Training Subcommittee
Creating a Safe Day the science of safety and operational excellence
 Creating a Safe Day the science of safety and operational excellence August 21, 2015 2015 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED. This material is a proprietary document of Healthcare
Creating a Safe Day the science of safety and operational excellence August 21, 2015 2015 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED. This material is a proprietary document of Healthcare
Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project
 Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project Linda Cronenwett, PhD, RN, FAAN Principal Investigator, QSEN Gwen Sherwood, PhD, RN, FAAN Co-Investigator, QSEN
Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project Linda Cronenwett, PhD, RN, FAAN Principal Investigator, QSEN Gwen Sherwood, PhD, RN, FAAN Co-Investigator, QSEN
The Purpose of this Code of Conduct
 The Purpose of this Code of Conduct This Code of Conduct provides a framework to guide us in meeting our obligations as employees and volunteers of HPC Healthcare, Inc., and its current and future affiliates,
The Purpose of this Code of Conduct This Code of Conduct provides a framework to guide us in meeting our obligations as employees and volunteers of HPC Healthcare, Inc., and its current and future affiliates,
Clinical Governance & Risk Management Awareness. Incl. investigation of accidents, complaints and claims. Unit 2
 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
Unit 2 Clinical Governance & Risk Management Awareness
 Unit 2 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Unit 2 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
DOCUMENTATION BASIC PRINCIPLES FOR LONG TERM CARE
 DOCUMENTATION BASIC PRINCIPLES FOR LONG TERM CARE Speakers for this conference have disclosed that they do not have significant relationships or affiliations with any commercial organization that could
DOCUMENTATION BASIC PRINCIPLES FOR LONG TERM CARE Speakers for this conference have disclosed that they do not have significant relationships or affiliations with any commercial organization that could
Observations of Implementing the Nuclear Promise for CAP
 Jack Martin Vice President, Consulting BackPacker Jack, Inc.- F-11070 TX Observations of Implementing the Nuclear Promise for CAP A Pendulum Swing in CAP Objectives CAP Regulatory Requirement The evolution
Jack Martin Vice President, Consulting BackPacker Jack, Inc.- F-11070 TX Observations of Implementing the Nuclear Promise for CAP A Pendulum Swing in CAP Objectives CAP Regulatory Requirement The evolution
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Documentation and Release Forms Optional #8 2018
 McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Documentation and Release Forms Optional #8 2018 This month we will be looking at the medical report that we generate
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Documentation and Release Forms Optional #8 2018 This month we will be looking at the medical report that we generate
Human Factors Engineering in Health Care. Awatef O. Ergai, PhD Post-Doctoral Research Associate Healthcare Systems Engineering Institute
 Human Factors Engineering in Health Care Awatef O. Ergai, PhD Post-Doctoral Research Associate Outline 1. What s human factors engineering (HFE) 2. Why is human factors engineering important in health
Human Factors Engineering in Health Care Awatef O. Ergai, PhD Post-Doctoral Research Associate Outline 1. What s human factors engineering (HFE) 2. Why is human factors engineering important in health
Patient Safety in Neurosurgery and Neurology. Andrea Halliday, M.D. Oregon Neurosurgery Specialists
 in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Compliance Program Updated August 2017
 Compliance Program Updated August 2017 Table of Contents Section I. Purpose of the Compliance Program... 3 Section II. Elements of an Effective Compliance Program... 4 A. Written Policies and Procedures...
Compliance Program Updated August 2017 Table of Contents Section I. Purpose of the Compliance Program... 3 Section II. Elements of an Effective Compliance Program... 4 A. Written Policies and Procedures...
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
21 Questions. Key risks (other) 9. related to finances? related to leadership?
 9. related to finances? related to leadership?") 21 Questions Guidance for healthcare boards on what they should ask senior leaders about risk. Drawing on strong ethical and evidence-based principles, HIROC, in collaboration with subscribers, has developed
21 Questions Guidance for healthcare boards on what they should ask senior leaders about risk. Drawing on strong ethical and evidence-based principles, HIROC, in collaboration with subscribers, has developed
Accident and Incident Investigation
 Standard Operating Procedures Accident and Incident Investigation Last Modified: JAN 2013 1 of 8 Accident and Incident Investigation I Purpose To prevent the recurrence of Accidents and Incidents by ensuring
Standard Operating Procedures Accident and Incident Investigation Last Modified: JAN 2013 1 of 8 Accident and Incident Investigation I Purpose To prevent the recurrence of Accidents and Incidents by ensuring
M2 This presenter has nothing to disclose What is High Reliability and Why Does Healthcare Need it?
 M2 This presenter has nothing to disclose What is High Reliability and Why Does Healthcare Need it? Mark R. Chassin, MD, FACP, MPP, MPH President, The Joint Commission Institute for Healthcare Improvement
M2 This presenter has nothing to disclose What is High Reliability and Why Does Healthcare Need it? Mark R. Chassin, MD, FACP, MPP, MPH President, The Joint Commission Institute for Healthcare Improvement
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
A nurse s guide for successful care transition and handoff communication
 A nurse s guide for successful care transition and handoff communication August 2017 Contents A care transition story you may recognize 3 What to communicate and when 4 Pay extra-close attention to medication
A nurse s guide for successful care transition and handoff communication August 2017 Contents A care transition story you may recognize 3 What to communicate and when 4 Pay extra-close attention to medication
Returning to the Why: Patient and Caregiver Suffering and Care. Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer
 Returning to the Why: Patient and Caregiver Suffering and Care Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer What Do We Want To Accomplish? Quality does not mean the elimination of death
Returning to the Why: Patient and Caregiver Suffering and Care Christy Dempsey, MSN MBA CNOR CENP SVP, Chief Nursing Officer What Do We Want To Accomplish? Quality does not mean the elimination of death
AGGRESSIVE BEHAVIOR TOOLKIT WSHA & ASHNHA PARTNERSHIP FOR PATIENTS PRESENTED BY: COURTNEY ULRICH
 AGGRESSIVE BEHAVIOR TOOLKIT WSHA & ASHNHA PARTNERSHIP FOR PATIENTS PRESENTED BY: COURTNEY ULRICH HIIN AND PARTNERSHIP FOR PATIENTS The Partnership for Patients initiative is a public-private partnership
AGGRESSIVE BEHAVIOR TOOLKIT WSHA & ASHNHA PARTNERSHIP FOR PATIENTS PRESENTED BY: COURTNEY ULRICH HIIN AND PARTNERSHIP FOR PATIENTS The Partnership for Patients initiative is a public-private partnership
WORKING DRAFT. Standards of proficiency for nursing associates. Release 1. Page 1
 WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
Nursing Documentation 101
 Nursing Documentation 101 Module 3: Essential Elements Part I Handout 2014 College of Licensed Practical Nurses of Alberta. All Rights Reserved. Nursing Documentation 101 Module 3: Essentials Part I Page
Nursing Documentation 101 Module 3: Essential Elements Part I Handout 2014 College of Licensed Practical Nurses of Alberta. All Rights Reserved. Nursing Documentation 101 Module 3: Essentials Part I Page
Emergency Preparedness Near Nuclear Power Plants
 Emergency Preparedness Near Nuclear Power Plants January 2009 Key Facts Federal law requires that energy companies develop and exercise sophisticated emergency response plans to protect public health and
Emergency Preparedness Near Nuclear Power Plants January 2009 Key Facts Federal law requires that energy companies develop and exercise sophisticated emergency response plans to protect public health and
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor
 Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Safe Sharp Program: A Culture of Prevention
 Safe Sharp Program: A Culture of Prevention Ken Smith System Director of Safety kenneth.smith@sclhs.net Sisters of Charity of Leavenworth Health System, Inc. All rights reserved. 1 Safe Sharps: A Culture
Safe Sharp Program: A Culture of Prevention Ken Smith System Director of Safety kenneth.smith@sclhs.net Sisters of Charity of Leavenworth Health System, Inc. All rights reserved. 1 Safe Sharps: A Culture
Building a High-Performance team in the Pediatric Medical Home Xavier Sevilla M.D. FAAP Whole Child Pediatrics MCRHS Inc.
 Building a High-Performance team in the Pediatric Medical Home Xavier Sevilla M.D. FAAP Whole Child Pediatrics MCRHS Inc. Whole Child Pediatrics Whole Child Pediatrics Opened November 2007 Using the Principles
Building a High-Performance team in the Pediatric Medical Home Xavier Sevilla M.D. FAAP Whole Child Pediatrics MCRHS Inc. Whole Child Pediatrics Whole Child Pediatrics Opened November 2007 Using the Principles
14 th May Pharmacy Voice. 4 Bloomsbury Square London WC1A 2RP T E
 Consultation response Department of Health Rebalancing Medicines Legislation and Pharmacy Regulation: draft orders under section 60 of the Health Act 1999 14 th May 2015 Pharmacy Voice 4 Bloomsbury Square
Consultation response Department of Health Rebalancing Medicines Legislation and Pharmacy Regulation: draft orders under section 60 of the Health Act 1999 14 th May 2015 Pharmacy Voice 4 Bloomsbury Square
Guidelines for the Management of C. difficile Infections in. Healthcare Settings. Saskatchewan Infection Prevention and Control Program November 2015
 Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
A3/B3: Improvement in the Intensive Care Unit
 A3/B3: Improvement in the Intensive Care Unit Carol Peden, MD, MPH, FRCA, FFICM, Associate Medical Director for Quality Improvement, Consultant in Anesthesia and Intensive Care Session Objectives Structure
A3/B3: Improvement in the Intensive Care Unit Carol Peden, MD, MPH, FRCA, FFICM, Associate Medical Director for Quality Improvement, Consultant in Anesthesia and Intensive Care Session Objectives Structure
Health and Safety Policy and Managerial Responsibilities
 Health and Safety Policy and Managerial Responsibilities 1.0 Purpose This document outlines the policies, procedures and practices governing the manner in which the Royal Conservatoire of Scotland manages
Health and Safety Policy and Managerial Responsibilities 1.0 Purpose This document outlines the policies, procedures and practices governing the manner in which the Royal Conservatoire of Scotland manages
Dr. Ginette M. Collazo
 Human Error Reduction Model: Root Cause Determination, CAPA development and CAPA Effectiveness Measurement for Human Performance Related Deviations Dr. Ginette M. Collazo www.humanerror.com Regulation
Human Error Reduction Model: Root Cause Determination, CAPA development and CAPA Effectiveness Measurement for Human Performance Related Deviations Dr. Ginette M. Collazo www.humanerror.com Regulation
PATIENT BILL OF RIGHTS & NOTICE OF PRIVACY PRACTICES
 Helping People Perform Their Best PRIVACY, RIGHTS AND RESPONSIBILITIES NOTICE PATIENT BILL OF RIGHTS & NOTICE OF PRIVACY PRACTICES Request Additional Information or to Report a Problem If you have questions
Helping People Perform Their Best PRIVACY, RIGHTS AND RESPONSIBILITIES NOTICE PATIENT BILL OF RIGHTS & NOTICE OF PRIVACY PRACTICES Request Additional Information or to Report a Problem If you have questions
A9/B9: Integrating Patient Safety into Your System s DNA
 A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
Appendix G: The LFD Tool
 Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
HROs and the Role of Finance South Carolina HFMA Annual Institute
 HROs and the Role of Finance South Carolina HFMA Annual Institute Kari Cornicelli, FHFMA,CPA Vice President/CFO Sharp Metropolitan Medical Campus San Diego, CA 1 Reflection Perfection is not attainable.
HROs and the Role of Finance South Carolina HFMA Annual Institute Kari Cornicelli, FHFMA,CPA Vice President/CFO Sharp Metropolitan Medical Campus San Diego, CA 1 Reflection Perfection is not attainable.
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.