CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM
|
|
|
- Randall Baldwin
- 5 years ago
- Views:
Transcription


1 CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress of The Lebanese Urology Society Sep.29 - Oct.1, 2016
2 Outlines (Where) The OR: A Special Hazardous Place What Risks in OR? Why do errors happen in OR? What about medical errors in the US? How do others do to reduce errors? And you What will you do to reduce errors In your everyday work? The 9th Congress of The Lebanese Urology Society Sep.29 - Oct.1, 2016
3 The OR: A Special Hazardous Place Many Risks Many Predefined Risks Many unexpected Events Many Caregivers Many Interactions Many Relative Sub Processes A complex System A lot of Stress Unique Specific Patient

4 What Risks in OR? Identification errors Site errors Retained sponges & instruments Surgical site Infections Unanticipated major bleedings Failure of equipment Anesthesiology mishaps & medication errors Burns due to cautery misuse Neuropathies due to bad positioning
5 Why do errors happen in OR? Risky behaviors in OR: No pre op checking of equipment's Surgeon running two rooms Surgeon entering room after draping Not checking radiology procedures and pathology reports Lack of learning how new equipment functions Many intra op verbal orders Unlabeled clear solutions Use of cautery in O2 rich environment Continuing to close during sponge count
6 What about Medical errors in US IOM 1999: deaths per year. AHRQ 2004 report (Agency for Healthcare Quality and Research): deaths a year. BMJ 2016 (the 3rd leading cause of death): deaths per year in US (after heart disease and cancer)
7 IOM report: 2001 Safety problems occurs because of: Inability to translate knowledge into practice Inability to apply new technology safely and appropriately Inability to make the best use of resources (financial and human) Blaming health providers is not the answer! We must address the system flaws Crossing the Quality Chasm: A New Health System for the 21 st Century
8 NO CHANGE!!!! Still focusing on individuals Weak Team dynamics Weak Communication Hierarchical structure Culture of Blame

9 Strategies used to reduce errors WE CANNOT CHANGE THE HUMAN CONDITION WE CAN CHANGE THE CONDITIONS UNDER WHICH PEOPLE WORK. James Reason


10 A Surgical quality improvement program is so effective that each year a hospital uses it, on average, it has the opportunity to: o Prevent complications o Save lives o Reduce costs by millions of dollars

11 A five-skill model Designed to help change an organization s culture for better outcomes by: o placing less focus on events, errors and outcomes, and more focus on risk, o managing the behavioral choices focused on a juste and accountable system o Integrating the Learnings in the system design
 4.")
12 Focus on the risk Why do errors happen? Rarely due to lack of knowledge of care givers 1. Lack of organisation (time, resources) 2. Lack of verification 3. Lack of coordination (Human Machine interface) 4. Lack of communication Risky behaviors =LACK of SAFETY CULTURE
13 Focus on the risk Build a safety culture Build a culture which encourages coaching and honesty at all levels, in order to bring about the best possible outcomes Encourage the creation of an environment of free and open reporting within process systems VALUES. LEARNING






14 Management of behavioral choices The Three Behaviors we can expect Human Error At-Risk Behavior Reckless Behavior Inadvert action : Slip, lapse, mistake opportunity to learn and to improve systems Manage through changes in : - Processes / Procedures - Training - Design / Environment Console A choice : Risk is not recognized or Believed Insignificant or Justified Manage through : - Removing incentives for at-risk behaviors - Creating incentives for healthy behaviors - Increasing situational awareness Coach Conscious Disregard of unreassonable Risk Manage Through: - Remedial action - Punitive action Punish

15 Focus on the risk Matrix for Risk Management Calculation

16 Design the system Learn about the processes of Error Error Policy Team Protocols Work Conditions Organization Patient Frontline staff Reason Model, 1993 Swiss cheese model
17 Learn about the processes of Error- The 5 Why s

18 Learn about the processes of Error- WHO s 10 Objectives for Safe Surgery 1. Operate on the correct patient &correct site. 2. Prevent harm from administration of Anesthesia 3. Effectively prepare for life-threatening loss of airways 4. Prepare for risk of high blood loss. 5. Avoid inducing an allergic or ADR for patients at risk 6. Minimize the risk for Surgical Site Infection. 7. Prevent inadvertent retention of instruments or sponges in surgical wounds. 8. Accurately identify all surgical specimens 9. Effectively Surgical Team communication 10. Routine surveillance of surgical capacity, volume and results.
19 Learn about the processes of Error- Better outcomes Stanford University, United States Mortality declined from.88 to.80 Reported Patient Safety Never Events (PSN) rose from 559 to 637 Reported events due to errors/complications decreased from 35.2% to 24.3% Mean OR start to incision time was shorter There was improvement in the belief (SAQ) that all personnel take responsibility for patient safety Tsai Thomas, Boussard Tinna, Welton, Mark, Morton, John. Does a surgical safety checklist improve patient safety culture and outcomes? [Abstract]. In: American College of Surgeons Annual Clinical Congress October 3-7; Washington D.C. Journal of American College of Surgeons. (N=12,247)
20 Strategy for highly performed Systems 1. Process review 2. Communication 3. Training and education 4. Teamwork 5. Coordination Crossing the Quality Chasm: A New Health System for the 21 st Century

21 1. Standardization to improve processes AAOS : 1998 Orthopedic surgeons have 25% chance of performing a wrong site surgery during a 35 years career: Wrong knee arthroscopies Wrong level spine fusions ACS: 2002: Recommends the development of guidelines to ensure correct patient, correct site surgery
22

23 2. Improve communication IOM 2011 report: Process review Communication Training and education Teamwork Reviews, Coordination Safety is not residing in a piece of equipment, it is a collaboration between members, and can be achieved by better communication and full adherence to system



24 Standardized Communication Pilots are committed to standardized communication Speak-repeat Read-repeat

25 Barriers to effective communication PROVIDER-PROVIDER Bad dynamics Not listening/not asking questions Poor sharing of patient info Not using standard comms Blame and Shame PROVIDER-PATIENT Provider: lack of cultural competency, busy, non-respectful, patronising, discriminating, stressed, tired, ill Patient: Illiterate, confused, not same language or culture as provider INSTITUTIONAL Lack of standardization communication policies Not sharing information Conflicting agendas (leaders, providers, patients) World Health Organization, 2014
26 Barriers to effective team communication in the OR OR setting : masks, noise, Hierarchical structure Work overload Distracting communication Communication plan Accountability

27 Improving communication Operating Rooms briefing and debriefing Also called a team checklist Addressed safety issues by: o Decreasing reliance on memory o Standardizing processes o Increasing access to information o Providing feedback

28 IOM 2011 report: Process review Communication Training and education Teamwork Reviews, Coordination 3. Training and Education
29 Approaches to Team Training CLASS-ROOM BASED TEACHING MEDICAL SIMULATION Lectures Videos Case-reviews Problem-solving Exams High-fidelity simulated OR Practice new protocols in work setting

30 4. Teamwork Learn and use people s names Be assertive when required If something doesn t make sense, find out the other person s perspective Always do a team briefing before starting a team activity and a debrief afterwards When conflict occurs, concentrate on what is right for the patient, not who is right or wrong IOM 2011 report: Process review Communication Training and education Teamwork Reviews, Coordination


31 Leadership Roadmap White Coat Leadership All knowing In charge Autocratic Buck stops here Impatient Blaming Controlling Lean Improvement Leadership Patient Knowledgeable Facilitator Helper Teacher / Student Communicator Guide (Respect, Challenge, and Grow people and partners)
32 What makes an effective team leader Setting priorities and delegating tasks Conducting briefs and debriefs Empowering team members to speak freely and ask questions Organizing training activities for the team Inspiring team members and maintain a positive group culture Utilizing resources to maximize performance Resolving team conflicts Accepting patients as members of the team? 32

33 5. Reviews, Coordination IOM 2011 report: Process review Communication Training and education Teamwork Reviews, Coordination The 9th Congress of The Lebanese Urology Society Sep.29 - Oct.1, 2016







34 Dr. Rabab Rassi El-Khoury President Dr. Paula Rizkallah Founding Member Vice President Dr. Rola Hammoud Founding Member Ex-President Treasurer Maysaa Jaafar Secretary Nadia Chbeir Deek Dr. Boutros Assaf Dr. Jamal Hoballah Governing Board Members Quality is a journey not a destination

35 THANK YOU
Just and Accountable Culture (JAC): An Introduction
: An Introduction") Just and Accountable Culture (JAC): An Introduction Maureen S Padilla, DNP, RN, NEA-BC Sr. VP and Chief Nurse Executive Co-Chair, Just & Accountable Steering Committee Yvonne Chu, MD, MBA Chief, Ophthalmology
Just and Accountable Culture (JAC): An Introduction Maureen S Padilla, DNP, RN, NEA-BC Sr. VP and Chief Nurse Executive Co-Chair, Just & Accountable Steering Committee Yvonne Chu, MD, MBA Chief, Ophthalmology
JUST CULTURE FEBRUARY 20, 2013 KAREN ZANIN RN CNOR
 JUST CULTURE FEBRUARY 20, 2013 KAREN ZANIN RN CNOR Balance A Just Culture balances the need to learn from mistakes with the need to take corrective action against an individual if the individual s conduct
JUST CULTURE FEBRUARY 20, 2013 KAREN ZANIN RN CNOR Balance A Just Culture balances the need to learn from mistakes with the need to take corrective action against an individual if the individual s conduct
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Shifting from Blame-&-Shame to a Just-and-Safe Culture
 Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
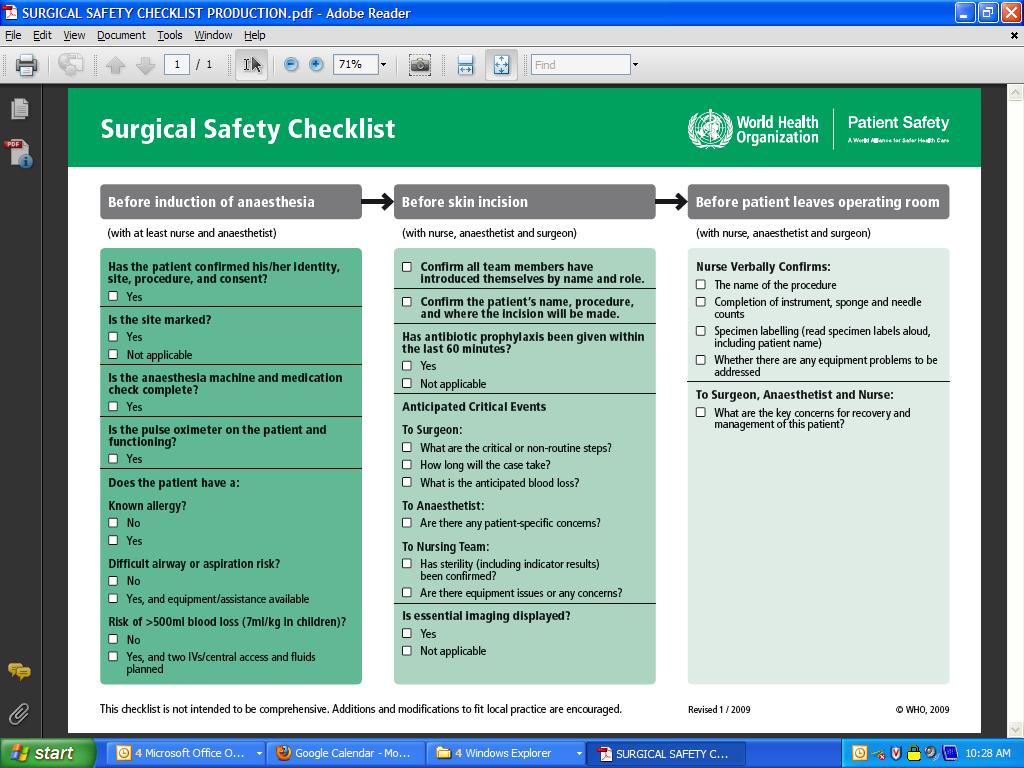
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Protecting the Public through Disciplinary Action. Maryann Alexander, PhD, RN, FAAN Kathleen Russell, JD, RN
 Protecting the Public through Disciplinary Action Maryann Alexander, PhD, RN, FAAN Kathleen Russell, JD, RN The Board s Duty Is To Protect The Public Not Punish The Licensee Criminal Justice System Punishment
Protecting the Public through Disciplinary Action Maryann Alexander, PhD, RN, FAAN Kathleen Russell, JD, RN The Board s Duty Is To Protect The Public Not Punish The Licensee Criminal Justice System Punishment
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Patient Safety (PS) 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.
 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.") Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Never Events (Including Retained Foreign Objects) The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI
 The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI") Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
How Should Policy Reflect a Culture of Safety?
 How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
Washington Patient Safety Coalition December 10, 2014
 Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009
 The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
10/4/2012. Disclosure. Leading a Meaningful Event Investigation. Just Culture definition. Objectives. What we all have in common
 Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Implementation of Surgical Safety Checklist
 Implementation of Surgical Safety Checklist The World Health Organisation has identified through consultation with surgeons, anaesthetists and nurses a checklist of critical steps that are common to all
Implementation of Surgical Safety Checklist The World Health Organisation has identified through consultation with surgeons, anaesthetists and nurses a checklist of critical steps that are common to all
Table of Contents. TeamSTEPPS Framework and Competencies Key Principles. Team Structure Multi-Team System For Patient Care
 Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Ruth Melville - QLD ACORN Director & Chair Standards Committee NUM ORS Clinical Services NGH
 Perioperative Documentation? Surgical Safety Checklist? Tray Checklists? Count sheets? What are they and how do they fit with current standards/practice? Ruth Melville - QLD ACORN Director & Chair Standards
Perioperative Documentation? Surgical Safety Checklist? Tray Checklists? Count sheets? What are they and how do they fit with current standards/practice? Ruth Melville - QLD ACORN Director & Chair Standards
Meeting Minutes Perioperative Quality Improvement Committee Meeting
 Meeting Minutes Perioperative Quality Improvement Committee Meeting Aim: To review systems issues uncovered by the morbidity and mortality process related to surgical patients with the goal to identify
Meeting Minutes Perioperative Quality Improvement Committee Meeting Aim: To review systems issues uncovered by the morbidity and mortality process related to surgical patients with the goal to identify
What we have learned:
 What we have learned: Perception Nursing Process Observations Nurses place undue reliance and trust in the count. Each individual nurse is sure that his/her count is correct yet there are retained sponges.
What we have learned: Perception Nursing Process Observations Nurses place undue reliance and trust in the count. Each individual nurse is sure that his/her count is correct yet there are retained sponges.
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers
 Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Leadership Forum: Promoting a Culture of Safety
 Leadership Forum: Promoting a Culture of Safety Dates: 5/10, 5/13 and 5/14 (Note: All sessions at the InterContinental Hotel) Times: 4-hour sessions (Note: Participants only attend 1 session) o Morning
Leadership Forum: Promoting a Culture of Safety Dates: 5/10, 5/13 and 5/14 (Note: All sessions at the InterContinental Hotel) Times: 4-hour sessions (Note: Participants only attend 1 session) o Morning
Reducing the risk of serious medication errors in community pharmacy practice
 Reducing the risk of serious medication errors in community pharmacy practice Eastern Medicaid Pharmacy Administrators Association (EMPAA) November 1, 2017 Newport, Rhode Island Michael R. Cohen, RPh,
Reducing the risk of serious medication errors in community pharmacy practice Eastern Medicaid Pharmacy Administrators Association (EMPAA) November 1, 2017 Newport, Rhode Island Michael R. Cohen, RPh,
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10
 Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB
 Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient Safety
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient Safety
Learning from Actual & Near Miss Events
 POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
TREATMENT OF MEDICAL ERROR ISSUES AT SURGICAL M&M CONFERENCE. Prof. Alberto R. Ferreres, MD, FACS
 TREATMENT OF MEDICAL ERROR ISSUES AT SURGICAL M&M CONFERENCE Prof. Alberto R. Ferreres, MD, FACS MEDICAL ERROR IN M&M CONFERENCE MEDICAL ERROR AT M&M CONFERENCE LA RESPONSABILIDAD MEDICA Y LA PRACTICA
TREATMENT OF MEDICAL ERROR ISSUES AT SURGICAL M&M CONFERENCE Prof. Alberto R. Ferreres, MD, FACS MEDICAL ERROR IN M&M CONFERENCE MEDICAL ERROR AT M&M CONFERENCE LA RESPONSABILIDAD MEDICA Y LA PRACTICA
Medication Safety in LTC. Objectives. About ISMP Canada
 Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Teamwork, Communication, O.R. Safety & SSI Reduction
 2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
JUST CULTURE DECEMBER 12,2012
 JUST CULTURE DECEMBER 12,2012 P R E S E N T E D B Y : K A T H Y F O W L E R : Q I P R O J E C T M A N A G E R M A R G R E T T U C K E R : W O U N D C A R E N U R S E P A U L L E V Y : N U R S E E D U C
JUST CULTURE DECEMBER 12,2012 P R E S E N T E D B Y : K A T H Y F O W L E R : Q I P R O J E C T M A N A G E R M A R G R E T T U C K E R : W O U N D C A R E N U R S E P A U L L E V Y : N U R S E E D U C
Invigorating Nursing Peer Review through Integration of Just Culture Human Factors and Principles
 Invigorating Nursing Peer Review through Integration of Just Culture Human Factors and Principles Jane S. Braaten, PhD, RN, CNS/ANP, CPPS Castle Rock Adventist Hospital Castle Rock, CO Cynthia Oster PhD,
Invigorating Nursing Peer Review through Integration of Just Culture Human Factors and Principles Jane S. Braaten, PhD, RN, CNS/ANP, CPPS Castle Rock Adventist Hospital Castle Rock, CO Cynthia Oster PhD,
Surgery Road Map. General practices. Road map sections
 Surgery Road Map MHA s road maps provide hospitals and health systems with evidence-based recommendations and standards for the development of topic-specific prevention and quality improvement programs,
Surgery Road Map MHA s road maps provide hospitals and health systems with evidence-based recommendations and standards for the development of topic-specific prevention and quality improvement programs,
Patient Safety Hazard Risk Assessment FY 2018
 Completed by: Patient Safety Committee Date Completed: Ocber 31, 2017 Methodology: Information utilized complete this Patient Safety Hazard Assessment included availa patterns/trends, high risk, prom prone
Completed by: Patient Safety Committee Date Completed: Ocber 31, 2017 Methodology: Information utilized complete this Patient Safety Hazard Assessment included availa patterns/trends, high risk, prom prone
Ambulatory Patient Safety
 We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
The Newcastle upon Tyne Hospitals NHS Foundation Trust
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Incidents, Accidents and the Trust Disciplinary Process - Guidelines for Managers, Clinical Directors and Employees Version.: 4.1 Effective From:
The Newcastle upon Tyne Hospitals NHS Foundation Trust Incidents, Accidents and the Trust Disciplinary Process - Guidelines for Managers, Clinical Directors and Employees Version.: 4.1 Effective From:
1875 Connecticut Ave. NW / Suite 650 / Washington, D.C / / fax /
 Testimony of Jane Loewenson Director of Health Policy, National Partnership for Women & Families Before the U.S. House of Representatives Energy & Commerce Subcommittee on Health Hearing on Patient Safety
Testimony of Jane Loewenson Director of Health Policy, National Partnership for Women & Families Before the U.S. House of Representatives Energy & Commerce Subcommittee on Health Hearing on Patient Safety
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Osteopathic and Medical Student Education Joseph C. Gambone, DO, MPH. Preparing Graduates for the 21 st Century Health Care System
 Osteopathic and Medical Student Education Joseph C. Gambone, DO, MPH Preparing Graduates for the 21 st Century Health Care System Interest in Method and Content: 20 years ago at UCLA -- We observed Students
Osteopathic and Medical Student Education Joseph C. Gambone, DO, MPH Preparing Graduates for the 21 st Century Health Care System Interest in Method and Content: 20 years ago at UCLA -- We observed Students
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Yoder-Wise: Leading and Managing in Nursing, 5th Edition
 Yoder-Wise: Leading and Managing in Nursing, 5th Edition Chapter 02: Patient Safety Test Bank MULTIPLE CHOICE 1. In an effort to control costs and maximize revenues, the Rehabilitation Unit at Cross Hospital
Yoder-Wise: Leading and Managing in Nursing, 5th Edition Chapter 02: Patient Safety Test Bank MULTIPLE CHOICE 1. In an effort to control costs and maximize revenues, the Rehabilitation Unit at Cross Hospital
Safe Surgery The Checklist Experience
 Safe Surgery The Checklist Experience Modificirana prezentacija uz suglasnost Gerald Dziekan, WHO Patient Safety The Surgical burden Estimated 234 million major operations performed worldwide each year
Safe Surgery The Checklist Experience Modificirana prezentacija uz suglasnost Gerald Dziekan, WHO Patient Safety The Surgical burden Estimated 234 million major operations performed worldwide each year
Leadership: Simple Strategies to Engage and Sustain
 Leadership: Simple Strategies to Engage and Sustain Susan Moffatt-Bruce, MD, PhD, FACS Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs, Quality and Patient Safety Associate
Leadership: Simple Strategies to Engage and Sustain Susan Moffatt-Bruce, MD, PhD, FACS Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs, Quality and Patient Safety Associate
(10+ years since IOM)
") Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Expedition: Improving Safety and Reliability for Surgical Procedures
 These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
Patient Safety Overview
 Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH, LSSBB Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH, LSSBB Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient
Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD
 Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Disclosure. Institute of Medicine (IOM) 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL
 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL") Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
NEUROSURGERY COMMUNICATION INITIATIVE STUDY
 MQP-BIO-DSA-4183 NEUROSURGERY COMMUNICATION INITIATIVE STUDY A Major Qualifying Project Report Submitted to the Faculty of the WORCESTER POLYTECHNIC INSTITUTE in partial fulfillment of the requirements
MQP-BIO-DSA-4183 NEUROSURGERY COMMUNICATION INITIATIVE STUDY A Major Qualifying Project Report Submitted to the Faculty of the WORCESTER POLYTECHNIC INSTITUTE in partial fulfillment of the requirements
How do we know the surgical checklist is making a meaningful. impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010
 How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
General OR-Stanford-CA-1 revised: Tuesday, February 02, 2016
 Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
Wrong Site, Wrong Procedure, Wrong Person Surgery
 Back to Basics Seventh in a Series Patient Safety Wrong Site, Wrong Procedure, Wrong Person Surgery By Alecia Cooper, RN, BS, MBA, CNOR An alarming occurrence affecting perioperative patient safety: According
Back to Basics Seventh in a Series Patient Safety Wrong Site, Wrong Procedure, Wrong Person Surgery By Alecia Cooper, RN, BS, MBA, CNOR An alarming occurrence affecting perioperative patient safety: According
Designing for Safety
 2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
Application of Simulation to Improve Clinical Efficiency Systems Integration
 Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Assessing Non-Technical Skills. A Guide to the NOTSS Tool Adapted for the Labour Ward
 Assessing Non-Technical Skills A Guide to the NOTSS Tool Adapted for the Labour Ward Acknowledgements The original NOTSS system was developed and evaluated in a multi-disciplinary project comprising surgeons,
Assessing Non-Technical Skills A Guide to the NOTSS Tool Adapted for the Labour Ward Acknowledgements The original NOTSS system was developed and evaluated in a multi-disciplinary project comprising surgeons,
The Journey To Ariadne Labs. Bill Berry, MD, MPH Chief Medical Officer Principle Research Scientist
 The Journey To Ariadne Labs Bill Berry, MD, MPH Chief Medical Officer Principle Research Scientist A Little History Flight Controls FREE & CORRECT The Problem The 3 Central Problems in Surgical Safety
The Journey To Ariadne Labs Bill Berry, MD, MPH Chief Medical Officer Principle Research Scientist A Little History Flight Controls FREE & CORRECT The Problem The 3 Central Problems in Surgical Safety
VERNON COLLEGE SYLLABUS. DIVISION: Allied Health and Human Services DATE:
 VERNON COLLEGE SYLLABUS DIVISION: Allied Health and Human Services DATE: 2011-2012 CREDITS HRS: 4 HRS/WK LEC: 2 HRS/WK LAB: 6 LEC/LAB COMB: 8 I. VERNON COLLEGE GENERAL EDUCATION PHILOSOPHY STATEMENT General
VERNON COLLEGE SYLLABUS DIVISION: Allied Health and Human Services DATE: 2011-2012 CREDITS HRS: 4 HRS/WK LEC: 2 HRS/WK LAB: 6 LEC/LAB COMB: 8 I. VERNON COLLEGE GENERAL EDUCATION PHILOSOPHY STATEMENT General
SafeStart & Patient Safety
 SafeStart & Patient Safety NS Safety Council Conference Halifax NS March 23, 2006 Allison Townsend, Electrolab Training Systems Belleville ON allison@electrolab.ca Electrolab Training Systems Belleville
SafeStart & Patient Safety NS Safety Council Conference Halifax NS March 23, 2006 Allison Townsend, Electrolab Training Systems Belleville ON allison@electrolab.ca Electrolab Training Systems Belleville
Enhancing Patient Safety through Team Work and Communication Strategies
 Enhancing Patient Safety through Team Work and Communication Strategies St. Joseph Medical Center- Towson Maryland Program/Project Description. In July 2009, Catholic Health Initiatives, of which St Joseph
Enhancing Patient Safety through Team Work and Communication Strategies St. Joseph Medical Center- Towson Maryland Program/Project Description. In July 2009, Catholic Health Initiatives, of which St Joseph
Accreditation Program: Office-Based Surgery
 ccreditation Program: Office-Based Surgery National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
ccreditation Program: Office-Based Surgery National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
A9/B9: Integrating Patient Safety into Your System s DNA
 A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
Take ACTION: A Collaborative Approach to Creating a Culture of Safety
 Take ACTION: A Collaborative Approach to Creating a Culture of Safety Heidi Boehm, MSN, RN-BC, Unit Educator Steven P. Kellar, BSN, RN, Unit Educator Joann L. Moore, RPh, Medication Safety Coordinator
Take ACTION: A Collaborative Approach to Creating a Culture of Safety Heidi Boehm, MSN, RN-BC, Unit Educator Steven P. Kellar, BSN, RN, Unit Educator Joann L. Moore, RPh, Medication Safety Coordinator
Patient Safety in Neurosurgery and Neurology. Andrea Halliday, M.D. Oregon Neurosurgery Specialists
 in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
When words and actions matter most: The Case for CANDOR
 January 20, 2017 When words and actions matter most: The Case for CANDOR Timothy B McDonald, MD Director, Center for Open and Honest Communication in Healthcare MedStar Health, Institute for Quality and
January 20, 2017 When words and actions matter most: The Case for CANDOR Timothy B McDonald, MD Director, Center for Open and Honest Communication in Healthcare MedStar Health, Institute for Quality and
Surgical Fires: Reducing the Risk of Patient Injury
 Surgical Fires: Reducing the Risk of Patient Injury By Georgette A. Samaritan, RN, BSN, CPHRM November 30, 2015 Surgical fires, fires that occur on or in a surgical patient, have consequences that can
Surgical Fires: Reducing the Risk of Patient Injury By Georgette A. Samaritan, RN, BSN, CPHRM November 30, 2015 Surgical fires, fires that occur on or in a surgical patient, have consequences that can
POLICY. The purpose of this policy is to establish Saskatoon Health Region s (SHR s) communication requirements for all surgical patients.
 communication requirements for all surgical patients.") POLICY Number: 7311-60-026 Title: Surgical Safety Checklist Authorization [ ] President and CEO [ X] Vice President, Finance and Corporate Services Source: Chair(s), Surgical Operations Committee Cross
POLICY Number: 7311-60-026 Title: Surgical Safety Checklist Authorization [ ] President and CEO [ X] Vice President, Finance and Corporate Services Source: Chair(s), Surgical Operations Committee Cross
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
TeamSTEPPS TM National Implementation
 TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
Perioperative Learning Center Mission Statement: The mission of the Perioperative Learning Center is to provide excellence in the education and
 Perioperative Learning Center Mission Statement: The mission of the Perioperative Learning Center is to provide excellence in the education and training of team members in an effort to deliver safe, competent
Perioperative Learning Center Mission Statement: The mission of the Perioperative Learning Center is to provide excellence in the education and training of team members in an effort to deliver safe, competent
Improved Patient Care and Safety
 Improved Patient Care and Safety David Fitzgerald, CCP, LP Division of Cardiovascular Perfusion College of Health Professions Medical University of South Carolina ARS Question #1 In my department/unit,
Improved Patient Care and Safety David Fitzgerald, CCP, LP Division of Cardiovascular Perfusion College of Health Professions Medical University of South Carolina ARS Question #1 In my department/unit,
UNIT TITLE: PERFORM BASIC FIRST AID PROCEDURES NOMINAL HOURS: 25 hours
 UNIT TITLE: PERFORM BASIC FIRST AID PROCEDURES NOMINAL HOURS: 25 hours UNIT NUMBER: D1.HRS.CL1.12 D1.HOT.CL1.12 D2.TCC.CL1.15 UNIT DESCRIPTOR: This unit deals with the skills and knowledge required to
UNIT TITLE: PERFORM BASIC FIRST AID PROCEDURES NOMINAL HOURS: 25 hours UNIT NUMBER: D1.HRS.CL1.12 D1.HOT.CL1.12 D2.TCC.CL1.15 UNIT DESCRIPTOR: This unit deals with the skills and knowledge required to
PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS
 PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS Active Error An error that occurs at the point of contact. Active errors are generally readily apparent (e.g., pushing an incorrect button, ignoring
PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS Active Error An error that occurs at the point of contact. Active errors are generally readily apparent (e.g., pushing an incorrect button, ignoring
Prevention of Retained Foreign Objects
 Prevention of Retained Foreign Objects Jane Kennedy RN, BSN, MBA, CNOR Senior Consultant Cardinal Health Objectives Discuss the impact, consequences, and contributing factors of retained foreign objects
Prevention of Retained Foreign Objects Jane Kennedy RN, BSN, MBA, CNOR Senior Consultant Cardinal Health Objectives Discuss the impact, consequences, and contributing factors of retained foreign objects
Text-based Document. The Culture of Incident Reporting Among Filipino Nurses. de Guzman, Barbara Michelle. Downloaded 28-Apr :54:41
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Statewide Patient Safety Culture: North Carolina HSOPS and Medical Office SOPS
 Statewide Patient Safety Culture: North Carolina HSOPS and Medical Office SOPS What is safety culture? The safety culture of an organization is the product of individual and group values, attitudes, perceptions,
Statewide Patient Safety Culture: North Carolina HSOPS and Medical Office SOPS What is safety culture? The safety culture of an organization is the product of individual and group values, attitudes, perceptions,
The CARE CERTIFICATE. Duty of Care. What you need to know. Standard THE CARE CERTIFICATE WORKBOOK
 The CARE CERTIFICATE Duty of Care What you need to know Standard THE CARE CERTIFICATE WORKBOOK Duty of care You have a duty of care to all those receiving care and support in your workplace. This means
The CARE CERTIFICATE Duty of Care What you need to know Standard THE CARE CERTIFICATE WORKBOOK Duty of care You have a duty of care to all those receiving care and support in your workplace. This means
7-8 September 2016 Sheraton Hotel & Towers Ho Chi Minh City, Vietnam
 7-8 September 2016 Sheraton Hotel & Towers Ho Chi Minh City, Vietnam www.hospitalmanagementasia.com 2 Empower Hospital Quality Culture through Accreditation About Vinmec Mission To deliver world class
7-8 September 2016 Sheraton Hotel & Towers Ho Chi Minh City, Vietnam www.hospitalmanagementasia.com 2 Empower Hospital Quality Culture through Accreditation About Vinmec Mission To deliver world class
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
TIME OUT! A Patient Safety Strategy. Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service
 TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations.
 ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations. 1 Thornton Kirby, President & CEO South Carolina Hospital Association Lorri Gibbons, RN, MSHL Vice President
ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations. 1 Thornton Kirby, President & CEO South Carolina Hospital Association Lorri Gibbons, RN, MSHL Vice President
Building and Sustaining a Culture of Safety
 Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Perioperative Nurse Coordinator Lead [Surgical]
![Perioperative Nurse Coordinator Lead [Surgical]](/thumbs/80/80543803.jpg "Perioperative Nurse Coordinator Lead [Surgical]") Date : July 2017 Job Title : Perioperative Nurse Coordinator Lead Note: Lead role is equivalent to Associate Clinical Charge Nurse Level [SN 4] Department : Surgical and Ambulatory Services Otorhinolaryngology
Date : July 2017 Job Title : Perioperative Nurse Coordinator Lead Note: Lead role is equivalent to Associate Clinical Charge Nurse Level [SN 4] Department : Surgical and Ambulatory Services Otorhinolaryngology
Creating and Using a Safe Surgery Checklist
 Creating and Using a Safe Surgery Checklist Michelle George, Vice President of Clinical Services Lisa Sinsel, Group Director of Clinical Services Surgical Care Affiliates 1 Agenda 1 2 3 4 5 6 7 Welcome
Creating and Using a Safe Surgery Checklist Michelle George, Vice President of Clinical Services Lisa Sinsel, Group Director of Clinical Services Surgical Care Affiliates 1 Agenda 1 2 3 4 5 6 7 Welcome
Physician Executive Council. Using the Perioperative Surgical Home to Improve Joint Replacement
 Physician Executive Council Using the Perioperative Surgical Home to Improve Joint Replacement 9 Today s Presenters Julie Riley Physician Executive Council Senior Consultant 202-266-5628 RileyJu@advisory.com
Physician Executive Council Using the Perioperative Surgical Home to Improve Joint Replacement 9 Today s Presenters Julie Riley Physician Executive Council Senior Consultant 202-266-5628 RileyJu@advisory.com
The Human Factor: Applying Safety Science in Health Care
 The Human Factor: Applying Safety Science in Health Care Sarah Henrickson Parker, PhD Director of Education and Academic Affairs, Research Scientist National Center for Human Factors Engineering in Healthcare
The Human Factor: Applying Safety Science in Health Care Sarah Henrickson Parker, PhD Director of Education and Academic Affairs, Research Scientist National Center for Human Factors Engineering in Healthcare
EL DORADO UNION HIGH SCHOOL DISTRICT Educational Services. Course of Study Information Page
 Course of Study Information Page Course Title:Medical Arts and Science, Level II #284 (Equivalent to Core Class ROP Health Occupations 101. One year course Block schedule, semester long.) Rationale: This
Course of Study Information Page Course Title:Medical Arts and Science, Level II #284 (Equivalent to Core Class ROP Health Occupations 101. One year course Block schedule, semester long.) Rationale: This
To Err is Human To Delay is Deadly Ten years later, a million lives lost, billions of dollars wasted
 1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
Waiting for a family member who is having surgery
 Waiting for a family member who is having surgery UHN Information for families, friends and caregivers in the Surgical Family Waiting Room Your family member, friend or loved one is having surgery. We
Waiting for a family member who is having surgery UHN Information for families, friends and caregivers in the Surgical Family Waiting Room Your family member, friend or loved one is having surgery. We
A Just Culture: Accountability for Patient Safety. Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012
 A Just Culture: Accountability for Patient Safety Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012 A Just Culture: Accountability for Patient Safety Today s Presenters:
A Just Culture: Accountability for Patient Safety Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012 A Just Culture: Accountability for Patient Safety Today s Presenters:
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
Welcome to Scott & White Memorial Hospital. Perioperative Services
 Welcome to Scott & White Memorial Hospital Perioperative Services What is a Perioperative Nurse? A perioperative nurse is a nurse who provides patient care, manages, teaches, and studies the care of patients
Welcome to Scott & White Memorial Hospital Perioperative Services What is a Perioperative Nurse? A perioperative nurse is a nurse who provides patient care, manages, teaches, and studies the care of patients
A 21 st Century System of Patient Safety and Medical Injury Compensation
 A 21 st Century System of Patient Safety and Medical Injury Compensation Overview Our goal is to promote patient safety and reduce preventable errors and injuries. We want to replace our fault-based medical
A 21 st Century System of Patient Safety and Medical Injury Compensation Overview Our goal is to promote patient safety and reduce preventable errors and injuries. We want to replace our fault-based medical