Catholic Medical Partners
|
|
|
- Albert Sutton
- 6 years ago
- Views:
Transcription


1 Improving Health Outcomes Patricia Podkulski, MS,RN October 13, 2011 Catholic Medical Partners 2 Independent Practice Association WNY: Erie/Niagara counties 900 physicians Four (4) Acute Care Hospitals Certified Home Care/Continuing Care Governing Board -23 members -16 physicians -7 hospital leaders 1





2 Clinical Integration Progression & Office Based Programs Prompt reporting of consults Rx Utilization In network Utilization Hospital Based Programs LOS Core Measure Prompt Discharge Reporting Physician Educational Seminars Registry Diabetes CAD CHF Asthma Non FFS population based payments Electronic Medical Records Financial support to offset implementation PCP/SCP at risk for Hospital based measures Care Coordination Adult PCPs CAD, CHF and Diabetic patients Disease Management Advanced training and support for selected Care coordination practices PCMH Technical assistance towards NCQA Recognition Pediatric nutrition referral program Care Coordination Expansion to the full continuum of care Specialists Pediatrics On line tools and assessment of patient knowledge and willing to change Development of Care Transition program Reduce readmission with a home assessment and pharmacist support FQHC Specialty Services Meaningful Use and Interoperability CCD Exchange Host EHR for practices Support and training for MU Patient Education Embed Nutritionists and Pharmacists in the practice offices Practice Re design Program Patient Experience Surveys High Performing Health Care System Payment Reform Enhancement of population based payment programs Bundled payments proposed to Health Plans NCQA Accreditation for Disease Management The Role of Catholic Medical Partners is to provide all the necessary resources for successful Clinical Integration Office Processes, Technology, Human Resources Registry Program Identify Gaps Measurement CIPA Office Based Clinical Integration Program Physician Engagement Patient Activation Clinical Integration Programs Disease Management, PCMH Educational Programs: Emmi, PAM, Nutrition 2


3 Population Health and Risk Reduction Model 10/12/ Program Goals To expand upon the fundamentals of office based care management by intensifying efforts on the identified population with disease management strategies. To transform the practice through care coordination, team development, PCMH implementation, Disease Management and then contracted delegated Disease Management as part of Catholic Medical Partners Patient Oriented NCQA Accredited Disease Management Program Focus is on Diabetes, CHF, CAD 3
4 Care Coordination and Disease Management Principles 1. Promotes evidence based medicine 2. Population based management/measurement with stratification of patients based on NEED 3. Supports physician-patient relationship 4. Promotes quality interaction between disease management program and physicians/patients 5. Stresses continuous quality improvement process 6. Create organized linkage from physician office to CHS service lines 10/12/ Program Objectives Understand the burden of illness for patient and provider Assess patient care vs. best practice guidelines Registry review sorting through low, medium and high risk Review of tool kit (EMMI, Health buddy, Care Connections, Health Connections, Health plans, Community resources, PAM tool) Understand disease management and Patient Centered Medical Home Managing the population data at your fingertips Refining coaching skills and promotion of self management 4




5 Care Coordination Engagement and trust are the cornerstones of care coordination The Care Management Cycle Follow-up Registry Review Interventions Patients in Need 5



6 Care Coordination and Disease Management System a. Patients with disease b. Patients at risk 1. High 2. Medium 3. Low a. Office interventions b. Referrals to service Line Diagnostic Services Consultations Treatment 1. Acute 2. Rehab 3. PACE 4. HHC 5. Sub-acute 6. LTC Care Coordination and Disease Management System 6




7 Care Coordination Numbers Total Care Coordinators Trained *Does not reflect year end total. Care Coordination Numbers Total Practices Trained 7



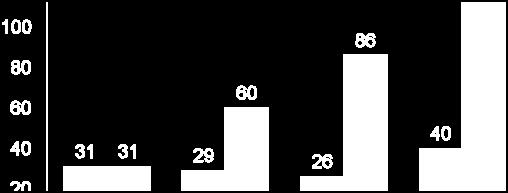
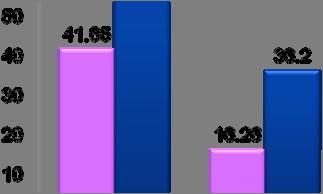
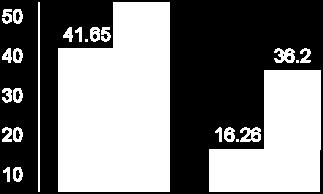
8 CI Resources Facilitate Meaningful Improvements 15 Control of Three Diabetes Indicators Among CMP Patients Uptick in Perfect Diabetes Care Follows Investment Measured Indicators and Goals 1 %age of Patients in Category Source: Catholic Medical Partners Time Since Baseline All three indicators in control No indicators in control HbA1c : Less than 7% LDL cholesterol: Less than or equal to 100 mg/dl Blood pressure: Less than 130/80 mm Hg Diabetes Results Comparison: Chart review process to EMR extracts * Measure HbA1c Measured Chart Review Practices (sample) EMR Practices ( all patients) 73.66% 89.94% HbA1c < % 59.62% B.P. Measured 71.61% 92.77% B.P. < 130/ % 36.20% * Cebul, Randall,MD, Love, Thomas,E, et al, Electronic Health Records and Quality of Diabetes Care, NEJM, 365;9, Sept 1, 2011, pp



9 Quality Outcomes Diabetes Quality Outcomes Congestive Heart Failure (CHF) 9

")
10 Quality Outcomes Coronary Artery Disease (CAD) Questions??? 10
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012
 Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home Domains of Function. Interpretive Guidelines
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home Domains of Function Interpretive Guidelines October 2009 Table of Contents Page 1.0 PATIENT-PROVIDER PARTNERSHIP 1 2.0 PATIENT REGISTRY
BCBSM Physician Group Incentive Program Patient-Centered Medical Home Domains of Function Interpretive Guidelines October 2009 Table of Contents Page 1.0 PATIENT-PROVIDER PARTNERSHIP 1 2.0 PATIENT REGISTRY
Market Mover? The Emerging Role of CMS in P4P. Linda Magno Director, Medicare Demonstrations Group August 24, 2004
 Market Mover? The Emerging Role of CMS in P4P Linda Magno Director, Medicare Demonstrations Group August 24, 2004 Why Medicare P4P? Quality & Patient Safety Significant room for improvement Significant
Market Mover? The Emerging Role of CMS in P4P Linda Magno Director, Medicare Demonstrations Group August 24, 2004 Why Medicare P4P? Quality & Patient Safety Significant room for improvement Significant
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Blueprint Integrated Pilot Programs
 Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
September, James Misak, M.D. Linda Stokes, MSPH The MetroHealth System
 Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Medicare Physician Group Practice Demonstration
 Medicare Physician Group Practice Demonstration Disease Management Colloquium Philadelphia, Pennsylvania June 23, 2005 John Pilotte Senior Research Analyst Medicare Demonstrations Program Group Centers
Medicare Physician Group Practice Demonstration Disease Management Colloquium Philadelphia, Pennsylvania June 23, 2005 John Pilotte Senior Research Analyst Medicare Demonstrations Program Group Centers
Prevea Health Automates Population Health Management and Improves Health Outcomes
 CASE STUDY Prevea Health Prevea Health Automates Population Health Management and Improves Health Outcomes After adopting the patient-centered medical home care delivery model to improve the health and
CASE STUDY Prevea Health Prevea Health Automates Population Health Management and Improves Health Outcomes After adopting the patient-centered medical home care delivery model to improve the health and
Referrals, Prior Authorizations, Medical Management, and Appeals
 Referrals, Prior Authorizations, Medical Management, and Appeals 1 An Independent Licensee of the Blue Cross Blue Shield Association 044506 (12-21-2017) 2017 Premera. Proprietary and Confidential. Referrals
Referrals, Prior Authorizations, Medical Management, and Appeals 1 An Independent Licensee of the Blue Cross Blue Shield Association 044506 (12-21-2017) 2017 Premera. Proprietary and Confidential. Referrals
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
IT Enabled Care: Connecting the Dots EMR Validated Data - Driving Quality and Clinical Performance Improvement
 5 th National Pay for Performance Summit March 9, 2010 San Francisco, CA IT Enabled Care: Connecting the Dots EMR Validated Data - Driving Quality and Clinical Performance Improvement The Melting Pot Accountable
5 th National Pay for Performance Summit March 9, 2010 San Francisco, CA IT Enabled Care: Connecting the Dots EMR Validated Data - Driving Quality and Clinical Performance Improvement The Melting Pot Accountable
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model
 Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Medicare Shared Savings ACOs: One Organization s Lessons Learned. Gregory A. Spencer MD FACP Chief Medical Officer Crystal Run Healthcare LLP
 Medicare Shared Savings ACOs: One Organization s Lessons Learned Gregory A. Spencer MD FACP Chief Medical Officer Crystal Run Healthcare LLP Learning Objectives Identify organizational strengths and weaknesses
Medicare Shared Savings ACOs: One Organization s Lessons Learned Gregory A. Spencer MD FACP Chief Medical Officer Crystal Run Healthcare LLP Learning Objectives Identify organizational strengths and weaknesses
Accelerating the Impact of Performance Measures: Role of Core Measures
 Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Ambulatory Care Delivery Strategy: The Key to Successful Population Health Management
 Ambulatory Care Delivery Strategy: The Key to Successful Population Health Management Christopher T. Olivia, MD, President Michael Renzi, DO, Chief Medical Officer March 18, 2014 2014, Continuum Health
Ambulatory Care Delivery Strategy: The Key to Successful Population Health Management Christopher T. Olivia, MD, President Michael Renzi, DO, Chief Medical Officer March 18, 2014 2014, Continuum Health
A. DIABETES AND HEART/STROKE Data Detail
 A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model. The New Accountable Care Business Model
 Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Building an Ambulatory System of Care: Using Population Health to Combat Secular Trends & Achieve the Triple Aim
 Building an Ambulatory System of Care: Using Population Health to Combat Secular Trends & Achieve the Triple Aim Christopher T. Olivia, MD, President June 11, 2014, All Rights Reserved and CONTINUUM HEALTH
Building an Ambulatory System of Care: Using Population Health to Combat Secular Trends & Achieve the Triple Aim Christopher T. Olivia, MD, President June 11, 2014, All Rights Reserved and CONTINUUM HEALTH
BCBSRI & Delivery System Transformation. Gus Manocchia, MD Senior Vice President & Chief Medical Officer March 11, 2016
 BCBSRI & Delivery System Transformation Gus Manocchia, MD Senior Vice President & Chief Medical Officer March 11, 2016 1 Overview Systems of Care Overview & Highlights Primary Care to Risk Arrangements
BCBSRI & Delivery System Transformation Gus Manocchia, MD Senior Vice President & Chief Medical Officer March 11, 2016 1 Overview Systems of Care Overview & Highlights Primary Care to Risk Arrangements
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Weaving Expanded Roles of the RN into Population Management
 Weaving Expanded Roles of the RN into Population Management Lois K. Andrews, DNP, RN-BC, CNS, ACNS-BC, CCRN Sentara Quality Care Network (SQCN), Norfolk, Va. Objectives: Explore the evolution of healthcare
Weaving Expanded Roles of the RN into Population Management Lois K. Andrews, DNP, RN-BC, CNS, ACNS-BC, CCRN Sentara Quality Care Network (SQCN), Norfolk, Va. Objectives: Explore the evolution of healthcare
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Our Response to Health Reform: Collaborative Initiatives for Success
 Our Response to Health Reform: Collaborative Initiatives for Success February 11, 2012 Joseph R Swedish, FACHE President and CEO Trinity Health Trinity Health: Unified Enterprise Ministry Serving Ten States
Our Response to Health Reform: Collaborative Initiatives for Success February 11, 2012 Joseph R Swedish, FACHE President and CEO Trinity Health Trinity Health: Unified Enterprise Ministry Serving Ten States
2012 QUEST Primary Care HMSA. Patient-Centered Medical Home. and. Pay-for-Quality. Getting Started and Ongoing Management
 2012 QUEST Primary Care HMSA Patient-Centered Medical Home and Pay-for-Quality Getting Started and Ongoing Management P r o g r a m G u i d e Table of Contents Overview....2 Introduction....4 Basic Requirements,
2012 QUEST Primary Care HMSA Patient-Centered Medical Home and Pay-for-Quality Getting Started and Ongoing Management P r o g r a m G u i d e Table of Contents Overview....2 Introduction....4 Basic Requirements,
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
A Clinically Integrated Network Approach
 Duke Medicine ACO Preparedness A Clinically Integrated Network Approach Bill Schiff, MHA Duke Medicine Private Diagnostic Clinic, PLLC. (PDC) Duke Faculty Practice 1 A. Duke Medicine Organizing for HealthCare
Duke Medicine ACO Preparedness A Clinically Integrated Network Approach Bill Schiff, MHA Duke Medicine Private Diagnostic Clinic, PLLC. (PDC) Duke Faculty Practice 1 A. Duke Medicine Organizing for HealthCare
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Health Information Technology
 ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
Informatics, PCMHs and ACOs: A Brave New World
 Informatics, PCMHs and ACOs: A Brave New World R. Clark Campbell, MSN, RN-BC, CPHIMS, FHIMSS Kathleen Kimmel, RN, BSN, MHA, CPHIMS, FHIMSS Engagement Executive with Health Catalyst Objectives - Define
Informatics, PCMHs and ACOs: A Brave New World R. Clark Campbell, MSN, RN-BC, CPHIMS, FHIMSS Kathleen Kimmel, RN, BSN, MHA, CPHIMS, FHIMSS Engagement Executive with Health Catalyst Objectives - Define
Patient-Centered Medical Home
 2014 Primary Care HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E HMSA, an Independent Licensee of the Blue Cross and Blue Shield Association Progressing
2014 Primary Care HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E HMSA, an Independent Licensee of the Blue Cross and Blue Shield Association Progressing
Building the Oncology Medical Home. Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc.
 Building the Oncology Medical Home Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc. Quality, Performance Improvement, Certification / Recognition Keep the doors
Building the Oncology Medical Home Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc. Quality, Performance Improvement, Certification / Recognition Keep the doors
Saint Francis Care and Cigna CAC Meeting the Triple Aim Together
 Saint Francis Care and Cigna CAC Meeting the Triple Aim Together Christopher M. Dadlez, President and CEO Saint Francis Care Jess Kupec, President and CEO Saint Francis HealthCare Partners 22 nd Annual
Saint Francis Care and Cigna CAC Meeting the Triple Aim Together Christopher M. Dadlez, President and CEO Saint Francis Care Jess Kupec, President and CEO Saint Francis HealthCare Partners 22 nd Annual
Exhibit A.11.DY3. DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements
 Requirements") Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Presbyterian Healthcare Services Care Management
 Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Developmental Screening Focus Study Results
 Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
PATIENT CENTERED. Medical Home. Attestation. Facility Compliance
 2 0 1 7 Attestation PATIENT CENTERED Medical Home of Facility Compliance State of Wyoming, Department of Health, Division of Healthcare Financing Check the Patient Centered Medical Home (PCMH) Programs
2 0 1 7 Attestation PATIENT CENTERED Medical Home of Facility Compliance State of Wyoming, Department of Health, Division of Healthcare Financing Check the Patient Centered Medical Home (PCMH) Programs
Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1)
") Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1) Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Professor and Chair Titus Family Department of Clinical
Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1) Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Professor and Chair Titus Family Department of Clinical
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration
 The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration January 26, 2012 1 Session Overview Partners in Innovation and Service
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration January 26, 2012 1 Session Overview Partners in Innovation and Service
Employer Breakout Session Payment Change in Ohio: What it Means for Employers
 Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community. Stewards of Change June 11, 2013
 An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
Healthy Patients/Engaged Patients
 Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Health Care that revolves around you.
 Health Care that revolves around you. MISSION STATEMENT Lone Star Circle of Care is committed to the pursuit of community-wide access to a behaviorally enhanced, patient-centered health care home that
Health Care that revolves around you. MISSION STATEMENT Lone Star Circle of Care is committed to the pursuit of community-wide access to a behaviorally enhanced, patient-centered health care home that
Adirondack Medical Home Pilot Overview. Dennis Weaver MD MBA November 2, 2010
 Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
N.E.W.T. Level Measurement:
 N.E.W.T. Level Measurement: Voldemort or Dumbledore? Nathan Spell, MD, FACP Chief Quality Officer, Emory University Hospital Georgia Chapter Scientific Meeting American College of Physicians Savannah,
N.E.W.T. Level Measurement: Voldemort or Dumbledore? Nathan Spell, MD, FACP Chief Quality Officer, Emory University Hospital Georgia Chapter Scientific Meeting American College of Physicians Savannah,
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM. Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017
 ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
The Patient Centered Medical Home: 2011 Status and Needs Study
 The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
Maximizing the Financial Performance of Employed Physicians
 Maximizing the Financial Performance of Employed Physicians Presented by: Health Directions, LLC Sabrina Burnett, Vice President HFMA Kentucky Chapter Summer Institute, July 24, 2014 About Health Directions,
Maximizing the Financial Performance of Employed Physicians Presented by: Health Directions, LLC Sabrina Burnett, Vice President HFMA Kentucky Chapter Summer Institute, July 24, 2014 About Health Directions,
Building the Universal Roadmap to Population Health Management
 Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
PPMI in a Community Teaching Hospital
 Presentation Objectives PPMI in a Community Teaching Targeting VBP and ACO metrics Pharmacist Objective: List ACO metrics that pharmacists can share accountability to achieve targets Technician Objective:
Presentation Objectives PPMI in a Community Teaching Targeting VBP and ACO metrics Pharmacist Objective: List ACO metrics that pharmacists can share accountability to achieve targets Technician Objective:
Patient-Centered Medical Home
 2015 QUEST Integration HMSA QUEST Integration Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent Licensee of the Blue Cross and Blue Shield Association
2015 QUEST Integration HMSA QUEST Integration Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent Licensee of the Blue Cross and Blue Shield Association
PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health
 PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health Spring Retreat March 19, 2010 Ashland, MA A PCMH provides Easy access to a PCP Who is working with a high-functioning team And a
PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health Spring Retreat March 19, 2010 Ashland, MA A PCMH provides Easy access to a PCP Who is working with a high-functioning team And a
Improving Care for the Chronically Ill. Linda Magno Director, Medicare Demonstrations
 Improving Care for the Chronically Ill Linda Magno Director, Medicare Demonstrations Medicare Spending for Beneficiaries with Chronic Conditions The 20 percent of beneficiaries with 5+ chronic conditions
Improving Care for the Chronically Ill Linda Magno Director, Medicare Demonstrations Medicare Spending for Beneficiaries with Chronic Conditions The 20 percent of beneficiaries with 5+ chronic conditions
Restructuring Healthcare The Role of Technology
 Restructuring Healthcare The Role of Technology Philip Gaziano, MD October 11, 2012 2 Physician Owned & Lead Organizations Accountable Care Associates, LLC (ACA): Founded in 2010, it is physician owned
Restructuring Healthcare The Role of Technology Philip Gaziano, MD October 11, 2012 2 Physician Owned & Lead Organizations Accountable Care Associates, LLC (ACA): Founded in 2010, it is physician owned
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Care Coordination (CC) assists members and their families with complex needs
 assists members and their families with complex needs") Care Coordination (CC) assists members and their families with complex needs Care is member-centered, family-focused, and culturally competent. CC assists in locating services to meet the health and social
Care Coordination (CC) assists members and their families with complex needs Care is member-centered, family-focused, and culturally competent. CC assists in locating services to meet the health and social
Effects of Patient Navigation on Chronic Disease Self Management
 Effects of Patient Navigation on Chronic Disease Self Management M. Christina R. Esperat, RN, PhD, FAAN, Professor and Associate Dean for Clinical Services, Texas Tech University Health Sciences Center
Effects of Patient Navigation on Chronic Disease Self Management M. Christina R. Esperat, RN, PhD, FAAN, Professor and Associate Dean for Clinical Services, Texas Tech University Health Sciences Center
Using Data to Promote Continuity of Care and Increase Accountability
 Using Data to Promote Continuity of Care and Increase Accountability USING DATA TO PROMOTE CONTINUITY OF CARE AND INCREASE ACCOUNTABILITY KAREN WOLK FEINSTEIN, PHD PRESIDENT AND CHIEF EXECUTIVE OFFICER
Using Data to Promote Continuity of Care and Increase Accountability USING DATA TO PROMOTE CONTINUITY OF CARE AND INCREASE ACCOUNTABILITY KAREN WOLK FEINSTEIN, PHD PRESIDENT AND CHIEF EXECUTIVE OFFICER
Provider Information Guide Complex Care and Condition Care Overview
 Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
WELCOME. Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association
 WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
2.b.iii ED Care Triage for At-Risk Populations
 2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
THE MISSISSIPPI QUALITY IMPROVEMENT INITIATIVE II MSQII-2
 THE MISSISSIPPI QUALITY IMPROVEMENT INITIATIVE II MSQII-2 To improve blood pressure and diabetes control in Mississippi, the MSDH Heart Disease and Stroke Prevention Program has established the Mississippi
THE MISSISSIPPI QUALITY IMPROVEMENT INITIATIVE II MSQII-2 To improve blood pressure and diabetes control in Mississippi, the MSDH Heart Disease and Stroke Prevention Program has established the Mississippi
Disease Management at Anthem West Or: what have we learned in trying to design these programs?
 Disease Management at Anthem West Or: what have we learned in trying to design these programs? Lisa M. Latts, MD, MSPH Regional Medical Director May 12, 2003 Anthem Inc. Anthem Inc. Headquarters: Indianapolis
Disease Management at Anthem West Or: what have we learned in trying to design these programs? Lisa M. Latts, MD, MSPH Regional Medical Director May 12, 2003 Anthem Inc. Anthem Inc. Headquarters: Indianapolis
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
MassHealth Initiatives:
 MassHealth Initiatives: PCMHI, DUALS, PCC/BH Integration, PCPR Dr. Julian Harris CBHI and CYF Advisory Committee Joint Meeting November 5, 2012 Our Mission To improve the health outcomes of our diverse
MassHealth Initiatives: PCMHI, DUALS, PCC/BH Integration, PCPR Dr. Julian Harris CBHI and CYF Advisory Committee Joint Meeting November 5, 2012 Our Mission To improve the health outcomes of our diverse
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2017-2018 V12.0 Blue Cross Blue Shield of Michigan is a nonprofit
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2017-2018 V12.0 Blue Cross Blue Shield of Michigan is a nonprofit
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
A Clinically Integrated Network. R.W. Chip Watkins, MD, MPH, FAAFP Independent Affinity Group 3 March 2015
 A Clinically Integrated Network R.W. Chip Watkins, MD, MPH, FAAFP Independent Affinity Group 3 March 2015 HHS has set a goal of tying 30 percent of traditional, or fee-for-service, Medicare payments to
A Clinically Integrated Network R.W. Chip Watkins, MD, MPH, FAAFP Independent Affinity Group 3 March 2015 HHS has set a goal of tying 30 percent of traditional, or fee-for-service, Medicare payments to
10/10/2017. Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP
 Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP") Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Medical Assistance Program Oversight Council. January 10, 2014
 Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Risk Stratification for Population Health Management
 STEPS FOR SUCCESS IN Risk Stratification for Population Health Management EVERY DOCTOR HAS EXPERIENCED THE 80/20 RULE WHEN IT COMES TO TREATING THEIR SICKEST PATIENTS, says Leonard Fromer, MD, FAAFP, Executive
STEPS FOR SUCCESS IN Risk Stratification for Population Health Management EVERY DOCTOR HAS EXPERIENCED THE 80/20 RULE WHEN IT COMES TO TREATING THEIR SICKEST PATIENTS, says Leonard Fromer, MD, FAAFP, Executive