Comprehensive Analysis Method
|
|
|
- Belinda Dean
- 5 years ago
- Views:
Transcription

1 Incident Analysis Learning Program - Module Four Comprehensive Analysis Method Jan. 10, 2013




2 Welcome Ioana Popescu Sandi Kossey Erin Pollock Tina Cullimore

3 Learning Program M3 WHAT WAS LEARNED? WHAT CAN BE DONE? HOW AND WHY? WHAT HAPPENED?

4 Analysis Methods Canadian Incident Analysis Framework Systematic Systems Analysis Local framework Other (VA, NPSA)
5 Learning Objectives The knowledge elements include an understanding of the: Steps to take when undertaking a comprehensive analysis Benefits and limitations of different diagramming tools Various considerations when writing statements of findings The performance elements include the ability to: Describe the steps to create a timeline of the event Perform the main steps to analyze information to identify contributing factors and relationships
6 Agenda 3-parts Knowledge expert Practice leader Facilitated discussion

7 Introducing: WebEx Be prepared to use: - Raise Hand & Checkmark - Chat & Q&A - Pointer & Text 7 11-Jan-13 7

8 About You M2
9 Presentation Wayne Miller

10 Has this ever happened in one of your facilities? 3:45 pm Call from Nurse manager Patient has been given the wrong medication. Patient is unconscious and has been moved to the ICU and assessment is ongoing.
11 Individual Perspectives to Leading Practices Key Features of Incident Analysis Timely, Thorough Objective and Impartial (avoid conflicts of interest or perceived conflicts) Credible Interdisciplinary, Including Frontline, Patient/Family, and Nonregulated staff Practise / Preparing Who, When, and How is the analysis conducted in your organization Build Teams - Quality, IT, Health Records, Bio Med Run simulations Just and trusting culture encourages, supports, and expects the reporting of safety and learning events. M2

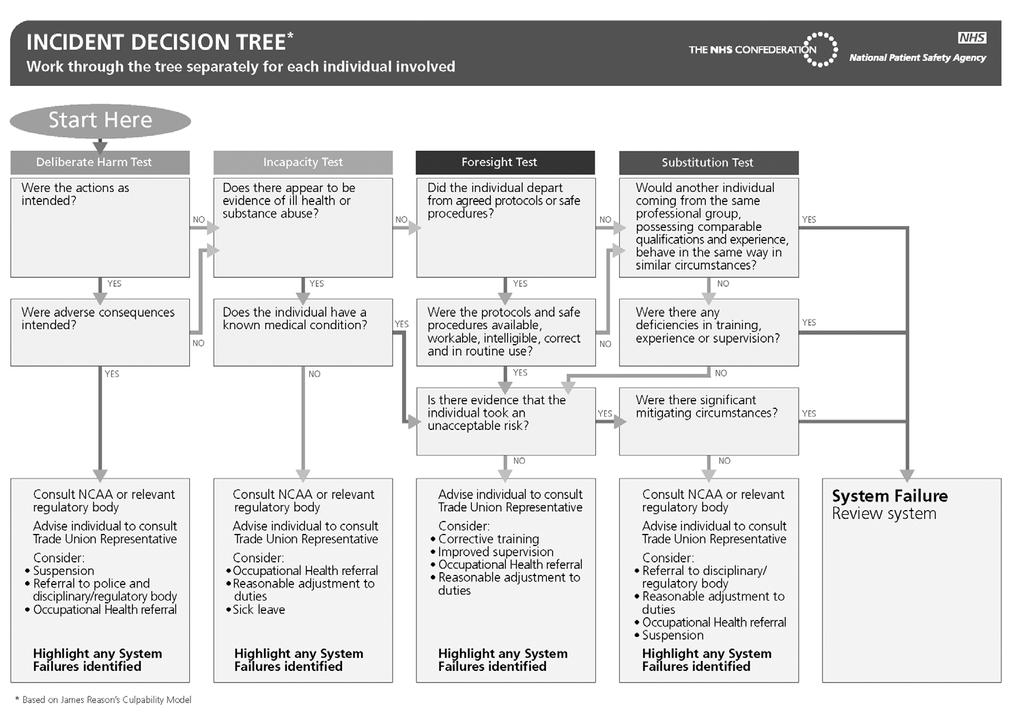
12 Page 39 Canadian Incident Analysis Framework

13
14 Gather Information Caution Do not jump to solutions, conclusions, and assumptions. Caution The team will not understand the contributing factors related to the incident if they do not understand the circumstances surrounding the incident. Caution The facilitator must have systematic processes for identifying the gaps in information and for accurately addressing those gaps.
 Report")
15 WHAT HAPPENED? Get a Game Plan Each Incident is different Gather Information Review the Incident (Occurrence) Report Review Additional information Create a Detailed Timeline Review Supporting Information
16 Review the Incident Report & Additional information Triggers for a comprehensive analysis Incident report is based on initial understanding Others Review the health record Conduct interviews Visit the location where the incident occurred Secure items OR look at similar items/devices to help build that understanding

17 Create a Detailed Timeline Example (p.104)
18 Review Supporting Information Includes: Review of Policies and Procedures Look at previously reported similar incidents Environmental Scan Literature Search Policies and Practices in leading organizations Consultation with colleagues or experts in the field.

19 HOW AND WHY IT HAPPENED? Analyze information to identify contributing factors and relationships Uses systems theory and human factors Uses diagramming Summarizes findings
20 Analyze Information Build on understanding by asking questions to determine contributing factors and relationships of factors to the event. Appendix G, Page 89, Guiding Questions Allows lens to focus on system issues which may have contributed to the event rather than focus on the person What was this influenced by? What else affected the circumstances?

21 Use Systems Theory and Human Factors Systems Theory Focuses on an assessment of the individual s action within the context of the circumstances at the time, NOT on the individual alone. Human Factors Interaction between the human and the system

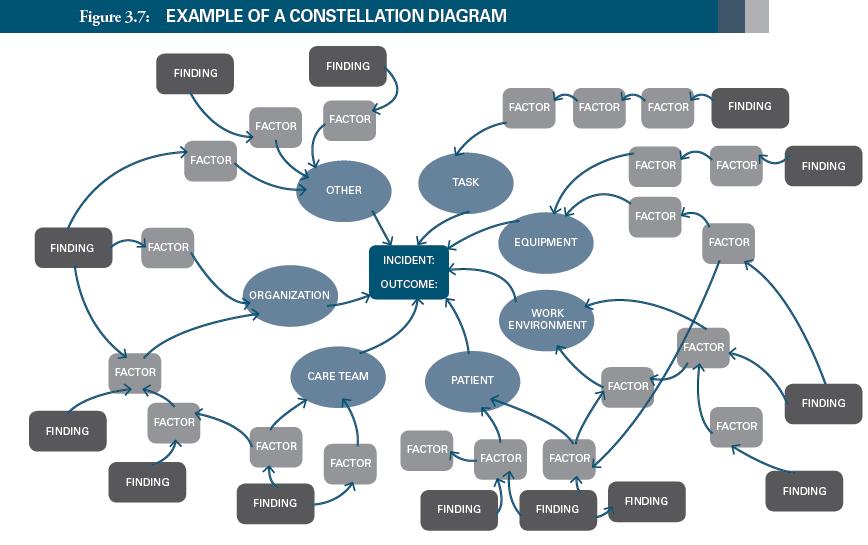
22 Use Diagramming Identify and understand inter-relationships between and among contributing factors Provides a map which, when used correctly, helps the team identify the route which was taken and why it was taken. Shifts the focus from the person to the system in which the person works.

23 Diagramming Ishikawa Diagram

24 Diagramming Tree Diagram
25
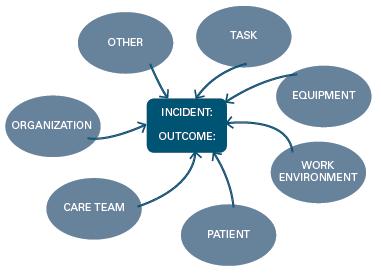
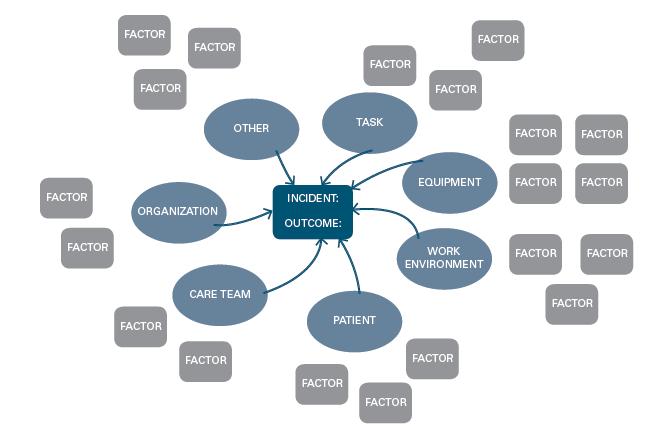
26 Constellation Diagramming 5 steps Step 1: Describe the incident Step 2: Identify potential contributing factors Step 3: Define inter-relationships between and among potential contributing factors. Step 4: Identify the findings Step 5: Confirm the findings with the team

27
28 Appendix G (p. 89) Guiding Questions Example
29 Summarize Findings Statements of findings Describe the relationships between the contributing factors and the incident and/or outcome. Three categories of findings: Factors that if corrected would likely have prevented the incident or mitigated the harm. Factors that if corrected, would NOT have prevented the incident or mitigated the harm, but are important for patient/staff safety or safe patient care in general Mitigating factors factors that didn t allow the incident to have more serious consequences and represent solid safeguards that should be kept in place
30 Statement of Findings Example The use of gravity intravenous infusion sets in the Emergency Department increased the likelihood that an intravenous narcotics infusion would be infused at a higher than intended rate when the patient changed his position on the stretcher
31 Confirm Findings Team should agree on the findings before developing recommended actions Work through disagreements to achieve consensus If key individuals who were involved in the event were not part of the analysis team, ask for their feedback on the findings. Include a Back-Checking Step


32 Ultimate Goal To WHAT CAN BE DONE TO REDUCE THE RISK OF RECURRENCE AND MAKE CARE SAFER

33 WHAT WAS LEARNED? Healthcare providers work very hard to provide safe care in the best way they know how. Let s not ask them to do this risky work without a net

34 Real-life Experience Dr. Chris Hayes

35 Incident Analysis Framework: Real-life Experience Module 4: Comprehensive analysis method January 10, 2013
36 What is critical incident (ie. a severe harmful patient safety incident) Any unintended event that occurs when a patient receives treatment in the hospital, that results in death, or serious disability, injury or harm to the patient, and does not result primarily from the patients' underlying medical condition or from a known risk inherent in providing the treatment
37 What is critical incident (ie. a severe harmful patient safety incident) Not Any factored unintended into event the definition that occurs at St. when a Michael s patient receives treatment in the hospital, perspective of patient outcome is considered that results in death, or serious disability, first.harm feels like harm!! injury or harm to the patient, and assumes inherent risks are fixed with no potential does not in result learning primarily or reducing eg from the patients' CLI data underlying supports medical inherent condition risk of or death from d/t a known adverse risk inherent events in providing = 1/116 the treatment
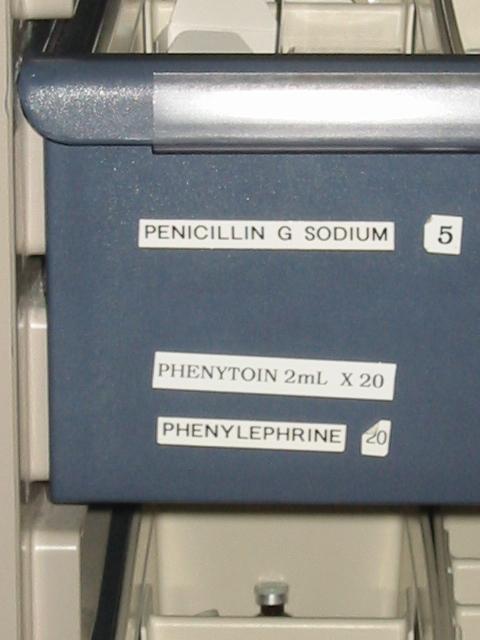
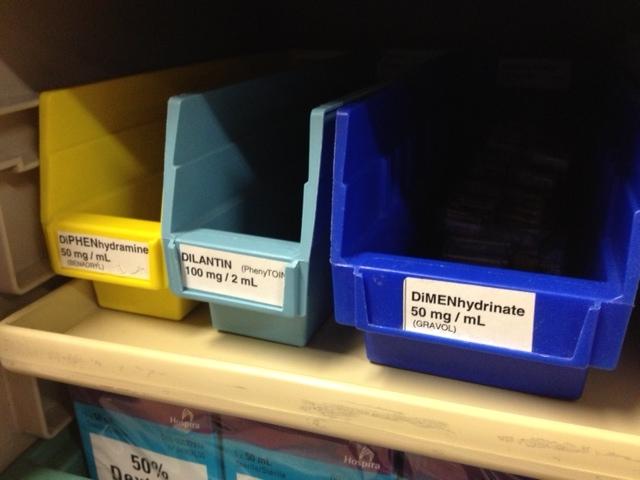
38 An example Patient admitted to the ICU following a large stroke. At approximately midnight the patient began having generalized seizures. She paged the resident on call. The resident came and asked for some Ativan. As the resident was giving the Ativan he asked the nurse to quickly get some Dilantin (phenytoin). The nurse left the bedside to prepare the medication in an IV minibag, returned to the bedside and began to hang the drug. Meanwhile the Ativan had stopped the seizure and the resident returned to his call room. 20 minutes later the patient s blood pressure rose to 230 over 120 mmhg. The patient began complaining of chest pain and was visibly short of breath. The nurse paged the resident to the bedside STAT. The resident on arrival asked for some IV metoprolol. He gave 20mg in total with little effect on the blood pressure.
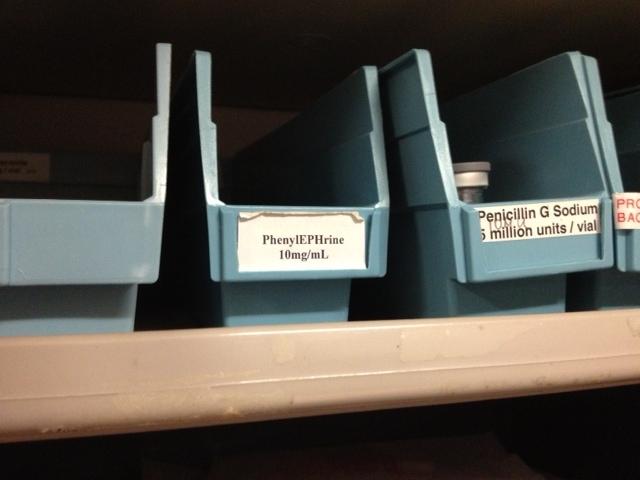
39 An example Eventually the patient was stabilized but had suffered a large heart attack and now had significant congestive heart failure. Later that evening the resident noticed a vial of phenylephrine at the patient s bedside. He showed this to the nurse who became immediately very upset and was later sent home. The Charge Nurse reported the incident later that evening, the family was informed of the incident and received an apology Risk Management & QI team reviewed the incident details and decided that a comprehensive review be conducted
40 So it s an adverse event The next phase is to analyze the event in order to know: What happened How and why it happened What can be done to reduce the likelihood of recurrence and make care safer What was learned

41 Conducting the analysis
42 Conducting the analysis Date / Time Information item Comment / Source Jan 1, 12 22:45 Patient admitted with stroke Patient record Jan 2, 12 00:20 23:35 Patient develops GTC seizure Nurses notes, confirmed by nurse interview 23:40 Resident assessed, gave Ativan and verbally ordered Dilantin 1g over 20 min 23:55 Nurse finished preparing, hung and administered Dilantin Patient blood pressure noted at 230/120, requring more oxygen Patient record, confirmed by resident interview Patient record, confirmed by nurse interview Patient record 00:50 Patient s BP resolved but requiring more oxygen Patient record ~01:20 Bottle of phenylephrine discovered at bedside Interview with resident ~01:50 Bedside nurse relieved of duty and went home Interview with charge nurse 10:30 Echo done and shows Grade 3 LV Patient record

43 Conducting the analysis

44 Conducting the analysis Verbal order given Acute issue, middle of night Double-check policy does not include anticonvulsants Sound-alike, look alike drugs stored together Nurse had to leave bedside to prepare med Patient suffers large MI and CHF following wrong drug administration


45


46 Swiss Cheese model Medication organization Manufacturer Hazards Sound-alike look-alike drug Purchasing Losses CHF/MI RN/MD Double-check
47

48 What did we do?

49 What did we do?
50 Recommendations / Actions Introduced TallMan lettering Removed multi-drug bins and reorganized med cabinets Moved phenytoin under D for dilantin Did the same for all other ICUs, then all wards Met with Clinical Services Committee and Pharmacy re purchasing of sound-alike, lookalike drugs Discussed the problem and the solution openly
51 Recommendations / Actions
52 Summary Incident analysis is a standard process to learn what, why and how an patient safety incident occurred An interprofessional, open and just approach fosters greater learning Requires gathering of material facts and interviews of those involved Requires open exploration of all contributing system factors Done right leads to effective recommendations and improvement in patient safety
53 Case Study Virtual Group Exercise


54 Breakout Session Most participants will move to breakout rooms Some participants will stay in the main room Those prompted: click YES to both pop-up screens to move
55 Small Group Discussion 0 Experience with comprehensive analysis 10 - Share your organization s comprehensive analysis process (what works well and what can be improved) - Point out the differences with the comprehensive method presented (4 objectives, steps, tools) - What would you need to do tomorrow to make the comprehensive analysis more effective
56 Large Group De-Briefing
57 Wrap-up
58 Next Steps End of session evaluation certificate of attendance Follow up survey we learn from you Incident Analysis Learning Program Concise analysis January 31, 2013 Multi-incident analysis February 21, 2013 Recommendations management March 7, 2013 Follow-through and share what was learned March 28, 2013
59 Resource slide Learning Program previous modules: rogram/pages/session-recordings-and-documents.aspx HQCA s Systematic Systems Analysis ews%20final%20june% pdf Incident Analysis Tools ysis/pages/tools.aspx

60 Mulţumesc Thank You
Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario A Teenager with Asthma
 Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario The purpose of interprofessional simulation is for students to participate in a simulated interprofessional experience
Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario The purpose of interprofessional simulation is for students to participate in a simulated interprofessional experience
Lesson 9: Medication Errors
 Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
A Systems Approach to Patient Safety at the VA
 BRIGHT IDEAS A Systems Approach to Patient Safety at the VA Erika Hatva The Department of Veterans Affairs (VA) operates the largest integrated healthcare system in the United States, serving 8.76 million
BRIGHT IDEAS A Systems Approach to Patient Safety at the VA Erika Hatva The Department of Veterans Affairs (VA) operates the largest integrated healthcare system in the United States, serving 8.76 million
Patient Safety and Incident Management
 Patient Safety and Incident Management Physiotherapy Alberta Webinar Sandi Kossey and Ioana Popescu, Canadian Patient Safety Institute October 22, 2015 Overview of Presentation About the Canadian Patient
Patient Safety and Incident Management Physiotherapy Alberta Webinar Sandi Kossey and Ioana Popescu, Canadian Patient Safety Institute October 22, 2015 Overview of Presentation About the Canadian Patient
Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home
 CANADIAN INCIDENT ANALYSIS FRAMEWORK Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home 2012 Canadian Patient Safety Institute All rights reserved. Permission is hereby granted to
CANADIAN INCIDENT ANALYSIS FRAMEWORK Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home 2012 Canadian Patient Safety Institute All rights reserved. Permission is hereby granted to
Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario A Postoperative Patient with Tachycardia
 Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario The purpose of interprofessional simulation is for students to participate in a simulated interprofessional experience
Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario The purpose of interprofessional simulation is for students to participate in a simulated interprofessional experience
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that
 Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Open Disclosure. Insert Logo Here. For more information, contact:
 Open Disclosure What s it about? Encouraging open and effective communication with patients. Acknowledging that adverse events causing harm occur. Saying sorry to the patient for any harm suffered during
Open Disclosure What s it about? Encouraging open and effective communication with patients. Acknowledging that adverse events causing harm occur. Saying sorry to the patient for any harm suffered during
Root Cause Analysis (Part I) event/rca_assisttool.doc
 event/rca_assisttool.doc") (Part I) http://www.jcaho.org/accredited+organizations/sentinel+ event/rca_assisttool.doc Edited by Dr. E. Terry DIO Dr. S.K. Oliver OME Examines the reasons an error occurred Suggests changes to the system
(Part I) http://www.jcaho.org/accredited+organizations/sentinel+ event/rca_assisttool.doc Edited by Dr. E. Terry DIO Dr. S.K. Oliver OME Examines the reasons an error occurred Suggests changes to the system
Management of Reported Medication Errors Policy
 Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Root Cause Analysis LITE (RCA Lite)
") Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Surgical Critical Care Sub I
 Course Goals Goals 1. Develop the attitude, skills, and knowledge to be able to recognize the impact of the global and local health care system and its impact on patient outcomes. 2. Develop the attitude,
Course Goals Goals 1. Develop the attitude, skills, and knowledge to be able to recognize the impact of the global and local health care system and its impact on patient outcomes. 2. Develop the attitude,
Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant
 Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant Today s presentation is an overview of the Investigating Workplace
Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant Today s presentation is an overview of the Investigating Workplace
Clinical Governance & Risk Management Awareness. Incl. investigation of accidents, complaints and claims. Unit 2
 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Nurse Orientation. Medication Management
 Nurse Orientation Medication Management Objectives Discuss basic principles/rights of medication administration, according to your site policy Describe principles of patient/family education related to
Nurse Orientation Medication Management Objectives Discuss basic principles/rights of medication administration, according to your site policy Describe principles of patient/family education related to
Medication errors and patient safety: tools for system improvement
 Medication errors and patient safety: tools for system improvement PHM 301 Julie Greenall ISMP Canada 2013 Institute for Safe Medication Practices Canada (ISMP Canada) 2013 Institute for Safe Medication
Medication errors and patient safety: tools for system improvement PHM 301 Julie Greenall ISMP Canada 2013 Institute for Safe Medication Practices Canada (ISMP Canada) 2013 Institute for Safe Medication
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
Guidance for Medication Reconciliation and System Integration Process
 Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
(10+ years since IOM)
") Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Storage, Labeling, Controlled Medications Instructor s Guide CFR (b)(2)(3)(d)(e) F431
(2)(3)(d)(e) F431") Centers for Medicare & Medicaid Services (CMS) Storage, Labeling, Controlled Medications Instructor s Guide CFR 483.60(b)(2)(3)(d)(e) F431 2006 Prepared by: American Institutes for Research 1000 Thomas
Centers for Medicare & Medicaid Services (CMS) Storage, Labeling, Controlled Medications Instructor s Guide CFR 483.60(b)(2)(3)(d)(e) F431 2006 Prepared by: American Institutes for Research 1000 Thomas
To prevent harm to patients from adverse medication events involving high-alert medications.
 TITLE MANAGEMENT OF HIGH-ALERT MEDICATIONS DOCUMENT # PS-46-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Management of High-alert Medications Policy APPROVAL LEVEL Alberta Health Services Executive
TITLE MANAGEMENT OF HIGH-ALERT MEDICATIONS DOCUMENT # PS-46-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Management of High-alert Medications Policy APPROVAL LEVEL Alberta Health Services Executive
National Patient Safety Agency Root Cause Analysis (RCA) Investigation
 Investigation") National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
Go! Guide: Adding Medication Administration History
 Go! Guide: Adding Medication Administration History Introduction Past medication administrations are often an integral part of a patient scenario. It may be important for students to review the patient
Go! Guide: Adding Medication Administration History Introduction Past medication administrations are often an integral part of a patient scenario. It may be important for students to review the patient
Participant WebEx Training. Jacob Auger Project Coordinator
 Participant WebEx Training Jacob Auger Project Coordinator WebEx Interaction Features Raise hand feature Yes/No feature Full screen view feature 2 Virtual Agreement Turn off cell phone and beepers. Avoid
Participant WebEx Training Jacob Auger Project Coordinator WebEx Interaction Features Raise hand feature Yes/No feature Full screen view feature 2 Virtual Agreement Turn off cell phone and beepers. Avoid
Practicum skills and competence expectation list Bachelor of Nursing students
 Practicum skills and competence expectation list Bachelor of Nursing students This practicum skills and competence expectation list has been developed in partnership by the 5 tertiary providers of BN programmes
Practicum skills and competence expectation list Bachelor of Nursing students This practicum skills and competence expectation list has been developed in partnership by the 5 tertiary providers of BN programmes
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND
TITLE CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND
TWH ED ACUTE & SUBACUTE BEDS UTILIZATION PROJECT
 TWH ED ACUTE & SUBACUTE BEDS UTILIZATION PROJECT PROJECT CHARTER Title: Toronto Western Hospital Emergency Department Acute & Sub-acute Beds Utilization Project Team: QI team: o Lucas Chartier MD, Director
TWH ED ACUTE & SUBACUTE BEDS UTILIZATION PROJECT PROJECT CHARTER Title: Toronto Western Hospital Emergency Department Acute & Sub-acute Beds Utilization Project Team: QI team: o Lucas Chartier MD, Director
Safer use of anticoagulants: the NPSA patient safety alert Steve Chaplin MSc, MRPharmS
 Safer use of anticoagulants: the NPSA patient safety alert Steve Chaplin MSc, MRPharmS Steve Chaplin describes the NPSA s anticoagulant patient safety alert and the measures it recommends for making the
Safer use of anticoagulants: the NPSA patient safety alert Steve Chaplin MSc, MRPharmS Steve Chaplin describes the NPSA s anticoagulant patient safety alert and the measures it recommends for making the
Profiles in CSP Insourcing: Tufts Medical Center
 Profiles in CSP Insourcing: Tufts Medical Center Melissa A. Ortega, Pharm.D., M.S. Director, Pediatrics and Inpatient Pharmacy Operations Tufts Medical Center Hospital Profile Tufts Medical Center (TMC)
Profiles in CSP Insourcing: Tufts Medical Center Melissa A. Ortega, Pharm.D., M.S. Director, Pediatrics and Inpatient Pharmacy Operations Tufts Medical Center Hospital Profile Tufts Medical Center (TMC)
Improving Care, Delivering Quality Reducing mortality & harm in Welsh Ambulance Services NHS Trust
 National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
National Learning Session - 10 th June 2011 Improving Care, Delivering Quality Reducing mortality & harm in Insert name of presentation on Master Slide Reducing Mortality & Harm in the Welsh Ambulance
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Pediatric Neonatology Sub I
 Course Goals Goals 1. Provide patient care that is compassionate, appropriate and effective for the treatment of health problems. 2. Recommend and interpret common diagnostic tests and vital signs. 3.
Course Goals Goals 1. Provide patient care that is compassionate, appropriate and effective for the treatment of health problems. 2. Recommend and interpret common diagnostic tests and vital signs. 3.
CARE OF THE PATIENT REQUIRING CONTINUOUS FLOLAN INFUSION GUIDELINE
 Page Number: 1 of 5 TITLE: CARE OF THE PATIENT REQUIRING CONTINUOUS FLOLAN INFUSION GUIDELINE PURPOSE: To provide guidelines for the nursing care of the patient with a Flolan infusion delivered thru continuous
Page Number: 1 of 5 TITLE: CARE OF THE PATIENT REQUIRING CONTINUOUS FLOLAN INFUSION GUIDELINE PURPOSE: To provide guidelines for the nursing care of the patient with a Flolan infusion delivered thru continuous
National Patient Safety Goals from The Joint Commission
 National Patient Safety Goals from The Joint Commission Objectives After completion of this module, participants will be able to: List at least five National Patient Safety Goals that are required in a
National Patient Safety Goals from The Joint Commission Objectives After completion of this module, participants will be able to: List at least five National Patient Safety Goals that are required in a
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
INPATIENT UNIT MEDICATIONS. Best Practice Guidelines
 INPATIENT UNIT MEDICATIONS Best Practice Guidelines Goals Standardize medication entry for narcotic medications Understand the function of IV and continuous medications including subcutaneous medications
INPATIENT UNIT MEDICATIONS Best Practice Guidelines Goals Standardize medication entry for narcotic medications Understand the function of IV and continuous medications including subcutaneous medications
To establish a consistent process for the activity of an independent double-check prior to medication administration, where appropriate.
 TITLE INDEPENDENT DOUBLE-CHECK SCOPE Provincial, Clinical DOCUMENT # PS-60-01 APPROVAL LEVEL Senior Operating Officer, Pharmacy Services SPONSOR Provincial Medication Management Committee CATEGORY Patient
TITLE INDEPENDENT DOUBLE-CHECK SCOPE Provincial, Clinical DOCUMENT # PS-60-01 APPROVAL LEVEL Senior Operating Officer, Pharmacy Services SPONSOR Provincial Medication Management Committee CATEGORY Patient
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
The CARE CERTIFICATE. Duty of Care. What you need to know. Standard THE CARE CERTIFICATE WORKBOOK
 The CARE CERTIFICATE Duty of Care What you need to know Standard THE CARE CERTIFICATE WORKBOOK Duty of care You have a duty of care to all those receiving care and support in your workplace. This means
The CARE CERTIFICATE Duty of Care What you need to know Standard THE CARE CERTIFICATE WORKBOOK Duty of care You have a duty of care to all those receiving care and support in your workplace. This means
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU. Change Package.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Impact of an Innovative ADC System on Medication Administration
 Impact of an Innovative ADC System on Medication Administration March 1, 2016 Nilesh Desai, BS, RPh, MBA Administrator Pharmacy and Clinical Operations Hackensack University Medical Center Conflict of
Impact of an Innovative ADC System on Medication Administration March 1, 2016 Nilesh Desai, BS, RPh, MBA Administrator Pharmacy and Clinical Operations Hackensack University Medical Center Conflict of
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
PATIENT RIGHTS, PRIVACY, AND PROTECTION
 REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
Root Cause Analysis Practicum Human Factors Engineering Short Course
 Learning Objectives Root Cause Analysis Practicum Human Factors Engineering Short Course 1. Identify human factors and other work system issues associated with an adverse event. 2. Develop a Cause-Effect
Learning Objectives Root Cause Analysis Practicum Human Factors Engineering Short Course 1. Identify human factors and other work system issues associated with an adverse event. 2. Develop a Cause-Effect
Monday, August 15, :00 p.m. Eastern
 Monday, August 15, 2016 2:00 p.m. Eastern Dial In: 888.863.0985 Conference ID: 34874161 Slide 1 Speakers Deb Kilday, MSN, RN Senior Performance Partner Performance Services Quality & Safety Premier, Inc.
Monday, August 15, 2016 2:00 p.m. Eastern Dial In: 888.863.0985 Conference ID: 34874161 Slide 1 Speakers Deb Kilday, MSN, RN Senior Performance Partner Performance Services Quality & Safety Premier, Inc.
How to Report Medication Safety Incidents from a GP Practice on the National Reporting and Learning System (NRLS)
") pecialist Pharmacy ervice Medicines Use and afety How to Report Medication afety Incidents from a GP Practice on the National Reporting and Learning ystem (NRL) This document provides a quick explanation
pecialist Pharmacy ervice Medicines Use and afety How to Report Medication afety Incidents from a GP Practice on the National Reporting and Learning ystem (NRL) This document provides a quick explanation
Required Organizational Practices Resources for 2016
 Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Drug Events. Adverse R EDUCING MEDICATION ERRORS. Survey Adapted from Information Developed by HealthInsight, 2000.
 Survey Adapted from Information Developed by HealthInsight, 2000. Adverse Drug Events R EDUCING MEDICATION ERRORS The Adverse Drug Events Survey will assist healthcare organizations evaluate the number
Survey Adapted from Information Developed by HealthInsight, 2000. Adverse Drug Events R EDUCING MEDICATION ERRORS The Adverse Drug Events Survey will assist healthcare organizations evaluate the number
Acute Care Workflow Solutions
 Acute Care Workflow Solutions 2016 North American General Acute Care Workflow Solutions Product Leadership Award The Philips IntelliVue Guardian solution provides general floor, medical-surgical units,
Acute Care Workflow Solutions 2016 North American General Acute Care Workflow Solutions Product Leadership Award The Philips IntelliVue Guardian solution provides general floor, medical-surgical units,
Foundations of Patient Safety and Interprofessional Practice Syllabus
 Foundations of Patient Safety and Interprofessional Practice Syllabus ACADEMIC YEAR 2015-2016 COURSE DESCRIPTION This 1 credit course is designed for early health care learners from all OHSU schools and
Foundations of Patient Safety and Interprofessional Practice Syllabus ACADEMIC YEAR 2015-2016 COURSE DESCRIPTION This 1 credit course is designed for early health care learners from all OHSU schools and
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
Anatomy of a Fatal Medication Error
 Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE DISCLOSURE OF HARM SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND NUMBER
TITLE DISCLOSURE OF HARM SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND NUMBER
POLICY NAME POLICY # Sentinel, Adverse Event and Near Miss. CSP Reporting and Investigation
 Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
Communicating with your patient about harm
 Communicating with your patient about harm DISCLOSURE OF ADVERSE EVENTS Suggestions to help CMPA members meet their patients clinical, information and emotional needs after an adverse event THE DISCLOSURE
Communicating with your patient about harm DISCLOSURE OF ADVERSE EVENTS Suggestions to help CMPA members meet their patients clinical, information and emotional needs after an adverse event THE DISCLOSURE
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Lesson 1: Introduction
 Lesson 1: Introduction Transcript Title Slide (no narration) Webcast Tips There are a few things that will assist you in navigating through the webcasts. At the bottom of the viewing pane are the play
Lesson 1: Introduction Transcript Title Slide (no narration) Webcast Tips There are a few things that will assist you in navigating through the webcasts. At the bottom of the viewing pane are the play
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
Safe Medication - Think Global, Act Local A global webinar series designed and facilitated by patient partners
 Safe Medication - Think Global, Act Local A global webinar series designed and facilitated by patient partners December 18, 2017 Theresa Malloy Miller Moderator Member Patients for Patient Safety Canada
Safe Medication - Think Global, Act Local A global webinar series designed and facilitated by patient partners December 18, 2017 Theresa Malloy Miller Moderator Member Patients for Patient Safety Canada
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Policies and Procedures. Title:
 Policies and Procedures Title: PATIENT CONTROLLED ANALGESIA (PCA) LPN Additional Competency: Patient Controlled Analgesia with an Established Plan of Care RN Entry-Level Competency Authorization: [X] Former
Policies and Procedures Title: PATIENT CONTROLLED ANALGESIA (PCA) LPN Additional Competency: Patient Controlled Analgesia with an Established Plan of Care RN Entry-Level Competency Authorization: [X] Former
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE IMMEDIATE MANAGEMENT OF CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT
TITLE IMMEDIATE MANAGEMENT OF CLINICAL ADVERSE EVENTS SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT
Improving the Safe Use of Multiple IV Infusions
 QUICK GUIDE Improving the Safe Use of Multiple IV Infusions The AAMI Foundation is grateful to its collaborating partners in the National Coalition for Infusion Therapy Safety: Acknowledgements The AAMI
QUICK GUIDE Improving the Safe Use of Multiple IV Infusions The AAMI Foundation is grateful to its collaborating partners in the National Coalition for Infusion Therapy Safety: Acknowledgements The AAMI
University of Wisconsin Hospital and Clinics Medication Reconciliation Education Packet
 Medication Reconciliation Education Objectives Purpose: The following learning objectives will be presented and evaluated with regard to the process of medication reconciliation. The goal is to provide
Medication Reconciliation Education Objectives Purpose: The following learning objectives will be presented and evaluated with regard to the process of medication reconciliation. The goal is to provide
The Knowledge Imperative Timothy B McDonald, MD JD September 7, 2012
 The Knowledge Imperative Timothy B McDonald, MD JD September 7, 2012 1 SESSION DESCRIPTION Interactive session on the role of science in patient safety that will address how knowledge, skills and behavioral
The Knowledge Imperative Timothy B McDonald, MD JD September 7, 2012 1 SESSION DESCRIPTION Interactive session on the role of science in patient safety that will address how knowledge, skills and behavioral
Kate Beaumont. Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign.
 Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
10/4/2012. Disclosure. Leading a Meaningful Event Investigation. Just Culture definition. Objectives. What we all have in common
 Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
Does patient engagement in patient safety and quality committees advance safe care or is it a myth?
 Does patient engagement in patient safety and quality committees advance safe care or is it a myth? February 24, 2016 Your line will be muted until the session begins. Interacting in WebEx Click the hand
Does patient engagement in patient safety and quality committees advance safe care or is it a myth? February 24, 2016 Your line will be muted until the session begins. Interacting in WebEx Click the hand
Seven steps to patient safety A guide for NHS staff
 Seven steps to patient safety A guide for NHS staff Seven steps to patient safety Step 1 Build a safety culture Step 2 Lead and support your staff Step 3 Integrate your risk management activity Step 4
Seven steps to patient safety A guide for NHS staff Seven steps to patient safety Step 1 Build a safety culture Step 2 Lead and support your staff Step 3 Integrate your risk management activity Step 4
Monitoring Medication Storage & Administration
 Monitoring Medication Storage & Administration Objectives Review F-Tags pertaining to medication management Discuss proper medication storage and administration Understand medication cart and medication
Monitoring Medication Storage & Administration Objectives Review F-Tags pertaining to medication management Discuss proper medication storage and administration Understand medication cart and medication
Comprehensive Outreach Education Certificate Program & Health Modules
 Comprehensive Outreach Education Certificate Program & Health Modules Community Health Education Center Lowell Community Health Center 161 Jackson Street Lowell, MA 01852 Tel: 978.452.0003 Email: CHEC@lchealth.org
Comprehensive Outreach Education Certificate Program & Health Modules Community Health Education Center Lowell Community Health Center 161 Jackson Street Lowell, MA 01852 Tel: 978.452.0003 Email: CHEC@lchealth.org
Clinical Research Proposal To the Jersey City Medical Center Institutional Review Board
 1 Clinical Research Proposal To the Jersey City Medical Center Institutional Review Board Principle Investigators: Erin Salmond BSN RN and Joanie Knuth RN BSN RN Date of Submission: Type of Proposal: Descriptive
1 Clinical Research Proposal To the Jersey City Medical Center Institutional Review Board Principle Investigators: Erin Salmond BSN RN and Joanie Knuth RN BSN RN Date of Submission: Type of Proposal: Descriptive
Handling Organisational Complaints
 Council meeting 12 January 2012 Public business Handling Organisational Complaints Purpose To report to the Council on the handling of organisational complaints for the period 27 September 2010 to 30 September
Council meeting 12 January 2012 Public business Handling Organisational Complaints Purpose To report to the Council on the handling of organisational complaints for the period 27 September 2010 to 30 September
1. He stated he had been treated with the utmost respect and professionalism by (b) (6)
 (6)") 13 OCT 17 NO. OF VETERAN BRIEF STATEMENT OF INFORMATION REQUESTED AND GIVEN: Task # T18-0146 - VA IQ Assignment--Parent Workflow ID 7845600/ Veteran s Inquiry: compliments: stated he is a Vietnam Veteran,
13 OCT 17 NO. OF VETERAN BRIEF STATEMENT OF INFORMATION REQUESTED AND GIVEN: Task # T18-0146 - VA IQ Assignment--Parent Workflow ID 7845600/ Veteran s Inquiry: compliments: stated he is a Vietnam Veteran,
The STEMI ALERT Packet
 The STEMI ALERT Packet (At a PCI-capable institution) Use of a STEMI ALERT Packet is a key step in optimizing treatment of the STEMI patient. Opening a STEMI ALERT Packet upon first recognition of STEMI
The STEMI ALERT Packet (At a PCI-capable institution) Use of a STEMI ALERT Packet is a key step in optimizing treatment of the STEMI patient. Opening a STEMI ALERT Packet upon first recognition of STEMI
Sample. A guide to development of a hospital blood transfusion Policy at the hospital level. Effective from April Hospital Transfusion Committee
 Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Using Patient and Family Centered Care Fundamentals in Establishing an Office of Patient Experience
 Using Patient and Family Centered Care Fundamentals in Establishing an Office of Patient Experience Presenters: Keith Gran, CPA, MBA, Chief Patient Experience Officer Molly Dwyer-White, MPH, Administrative
Using Patient and Family Centered Care Fundamentals in Establishing an Office of Patient Experience Presenters: Keith Gran, CPA, MBA, Chief Patient Experience Officer Molly Dwyer-White, MPH, Administrative
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Are National Indicators Useful for Improvement Work? Exercises & Worksheets
 Session L5 These presenters have nothing to disclose These presenters have nothing to disclose Are National Indicators Useful for Improvement Work? Exercises & Worksheets Robert Lloyd, PhD Göran Henriks,
Session L5 These presenters have nothing to disclose These presenters have nothing to disclose Are National Indicators Useful for Improvement Work? Exercises & Worksheets Robert Lloyd, PhD Göran Henriks,
Medication Management at Acme Medical Center
 2014 Medication Management at Acme Medical Center This patient might have died from complications related to her TPN infusion, said Dr. Isaac Johnson, Chief Medical Officer at Acme Medical Center (AMC).
2014 Medication Management at Acme Medical Center This patient might have died from complications related to her TPN infusion, said Dr. Isaac Johnson, Chief Medical Officer at Acme Medical Center (AMC).
Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003
 Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003 Susan M. Proulx, Pharm.D. President, Med-E.R.R.S. Subsidiary of ISMP (www.med-errs.com) Mission of ISMP Translate errors into education
Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003 Susan M. Proulx, Pharm.D. President, Med-E.R.R.S. Subsidiary of ISMP (www.med-errs.com) Mission of ISMP Translate errors into education
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Disclosure of Adverse Events and Medical Errors. Albert W. Wu, MD, MPH
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Organizational Overview
 0 Organizational Overview First All Digital Hospital in U.S. Fully integrated EMR across 2 Hospitals & 60 Clinics National Valve Center Five Star Hotel for; Patients, Physicians, Nurses & and all team
0 Organizational Overview First All Digital Hospital in U.S. Fully integrated EMR across 2 Hospitals & 60 Clinics National Valve Center Five Star Hotel for; Patients, Physicians, Nurses & and all team
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Root Cause Analysis A Necessary Evil? Dr Joseph Lui HA Convention 8 th May 2012
 Root Cause Analysis A Necessary Evil? Dr Joseph Lui HA Convention 8 th May 2012 Root Cause Analysis (RCA) The use of RCA as an organization learning tool first deployed by Veteran Affairs Hospitals in
Root Cause Analysis A Necessary Evil? Dr Joseph Lui HA Convention 8 th May 2012 Root Cause Analysis (RCA) The use of RCA as an organization learning tool first deployed by Veteran Affairs Hospitals in
Patient safety alert 06
 Immediate action Action Update Information request Correct site surgery Surgery performed at the incorrect anatomical site is rare. However, it can be devastating for patients. Correct site surgery (CSS)
Immediate action Action Update Information request Correct site surgery Surgery performed at the incorrect anatomical site is rare. However, it can be devastating for patients. Correct site surgery (CSS)
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
WHAT are medication errors?
 Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
NATIONAL PATIENT SAFETY AGENCY DRAFT PATIENT SAFETY ALERT. Safer Use of Injectable Medicines In Near-Patient Areas
 NATIONAL PATIENT SAFETY AGENCY DRAFT PATIENT SAFETY ALERT Safer Use of Injectable Medicines In Near-Patient Areas Wide Stake Holder Consultation January March 2006 The NPSA is undertaking a wide stake
NATIONAL PATIENT SAFETY AGENCY DRAFT PATIENT SAFETY ALERT Safer Use of Injectable Medicines In Near-Patient Areas Wide Stake Holder Consultation January March 2006 The NPSA is undertaking a wide stake