National Patient Safety Agency Root Cause Analysis (RCA) Investigation
|
|
|
- Patricia Short
- 6 years ago
- Views:
Transcription
1 National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services
2 Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural violations Latent Conditions - can translate into error provoking conditions eg time, pressure, poor equipment, staffing problems - provide longstanding weakness in defences eg unworkable procedures, construction deficiencies Reason BMJ 2000;320:
3 Reason s Swiss cheese model Some holes due to active failures Hazards Losses Other holes due to latent conditions DEFENCES, BARRIERS AND SAFEGUARDS James Reason 1990
4 Why RCA? In-depth analysis of a small number of incidents will bring greater dividends than a cursory examination of a large number Vincent and Adams, 1999
5 When to use RCA After a Patient Safety Incident has occurred Unpacks the whys The contributory factors which set people up to fail including workload, design, lack of procedures, poor training and supervision, incompatible goals etc..
6 timeline patient admitted event 1 event 2 event 3 adverse event additional information additional information additional information
7 basic elements of a good RCA investigation WHAT happened HOW it happened WHY it happened performance problem human behaviour influences control failure

8
9 Basic RCA method Identify and report Patient Safety Incident Select multi-disciplinary team Gather data Develop an incident chronology Identify the detail of what happened Explore the issues in depth Identify root causes and develop an action plan Test failsafe solutions Implementation and monitoring strategy
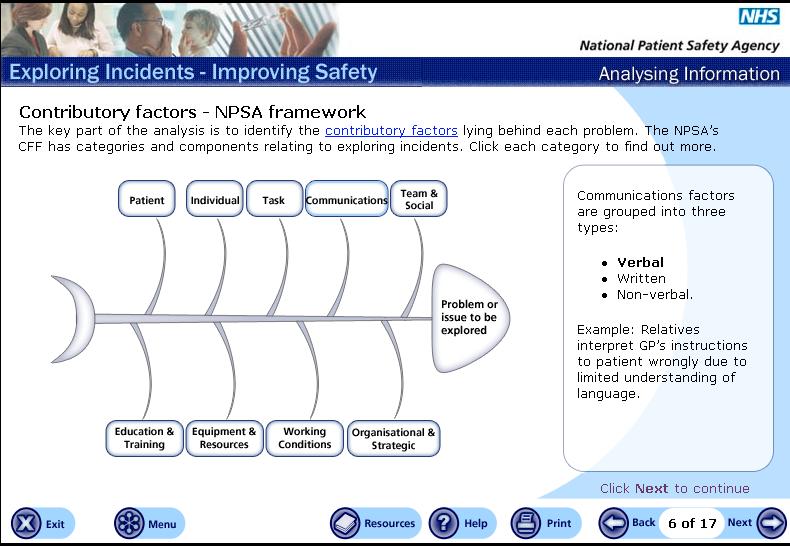
10 RCA Tools to identify and analyse Contributory Factors Brainstorming CRU/ALARM Protocol Cause and Effect Charting Five Why s Brain-writing Fishbone Diagrams Fault and Event Trees Nominal Group Technique
11
12 Identifying the Root Causes Identify the contributory factors having the biggest impact on system failure = ROOT CAUSE A Root Cause is a fundamental cause which if resolved will eradicate, or significantly contribute to the resolution, of the identified problem to which it is attached both within the local department and more widely across the organisation
13 Types of Barrier Human Action Barriers Checking the blood unit before administering Administrative Barriers Training Supervision Policies and procedures Physical Barriers insulation on pipes colour coding electrical flexes Natural Barriers place, time or distance
14 Performing a barrier analysis Choose an activity to be analysed (e.g. preparing a patient for theatre, giving blood) List, using Brainstorming techniques with relevant experts / others TARGETS Giving blood to patient HAZARDS wrong pt wrong blood BARRIERS checks protocols
15 Barrier Analysis Cont d Evaluate the list of barriers as strong, average or weak - any barrier involving human action is marked down Record the findings Remember barrier analysis can be used proactively or reactively!
16 Solution Ranking Matrix, New Zealand Ministry of Health 2001 Proposed Action Plan Summary Document Root Cause Actions to Address Root Cause Level of Recommenda tion (Individual Team, Directorate, Organisation) By Whom By When Resource Requirements Signoff Evidence of Compl -etion
17 Retrospective Study using root cause analysis (RCA) investigation into two incorrect blood component transfusion cases Hypothesis: RCA investigation would prove more useful in eliciting the latent conditions that lead to a patient safety incident Background: Review of SHOT s Annual Report 2000/01 stated that few cases were investigated thoroughly to get to the root cause that lead to incorrect blood transfusion
18 Methodology Participants: SHOT suggested 2 x Trusts who were deemed to be good reporters to SHOT who used old cases from the latter part of last year Training: Half day training to participants Follow up support: Appointment of ECRI to evaluate participants learning of RCA and to provide support with application of the process to past cases
19 Case Scenarios Trust 1 Background: 1991 and 1997: Patient previously known to have had red cell antibodies (anit-k and ant-fy(b)) by neighbouring hospital A (hospital A&B since merged in 1998). 3/1/03 received cross matched blood at hospital B. The transfused units were not selected as antigen negative (K-, Fy(b-1)) as per national guidelines and good transfusion practice. 13/1/03 This discovery was made on and subsequently reported to SHOT
20 Trust 1 - Methodology Incident Grading using 5 x 5 matrix risk scoring chart Timeline to track events occurring prior to, during and after the incident to discover all parts of the process where problems or errors occurred. Gathering of relevant documents: Patient s healthcare records Access to neighbouring hospital s Blood Bank computer and local hospital s computer, local Chemistry/Haematology computer PAS NBS reference laboratory report IRI incident report
21 1. Apparent outcome of incident in terms of harm B: Potential future risk to patients and to the organisation None Minor Moderate Major Catastrophic 3. Most likely consequences (if in doubt grade up, not down ) 2. Likelihood of recurrence None Minor Moderate Major Catastrophic Almost certain Likely Possible Unlikely Rare RIS K Very low Low Moderat e A: Impact on Patient: 1. Apparent harm to patient: none B: Potential future risk 2. Likelihood of recurrence of this type of incident: Likely 3. Most likely consequences of recurrence: Major Risk level: High High
22 Results Analysis & findings Lack of single Blood Bank computer system between hospital A & B Failure to pass on relevant patient information during transfer between hospital A & B Potential for access to hospital B laboratory system for all patients historical antibodies deemed impractical to look up for all patients due to time factors involved Failure of NBS reference lab staff to alert Trust 1 to the incorrect blood selection for transfusion The raise in bilirubin levels seems likely to have been caused by the biliary obstruction rather than red cell destruction as a probable result of this transfusion
23 Trust 1 - Key Learning Points A single Blood Bank system is needed between hospital A and hospital B Staff awareness of importance of passing on red cell antibody information during transfer of patients between hospitals When incompatibilities are detected all available hospital transfusion systems should be checked for historical antibodies When issuing verbal reports, it is important to pass on all relevant historical information
24 Trust 2 Background A 62 year old female patient received a unit of platelets which were not her ABO group Methodology Gathering of relevant records: Original telephone request form The blood bank register Relevant SOP Attempts were made to locate the Safecode IR form
25 Staff Informally Interviewed Purpose of interview- To establish not only the witnesses to the event, but underlying working practices also Staff interviewed: Blood Bank BMS Senior BMS involved in the incident Ward Manager involved in the incident and its reporting Senior Nurse
26 Findings & Analysis The computer system that supports the work in the blood bank failed to alert when the wrong ABO group of platelets was issued to the patient 1 member of staff operating in Blood Bank due to staff shortage Single person checking of products other than red cell transfusion appeared to be indicative of a task contributory factor A deficit related to education and training in the staff in HDU did not question the ABO group at the time of collection Patient factors were also to play very unwell, had been transferred as an emergency.
27 Other findings: Deficit related to laboratory working conditions The platelet transfusion was prescribed on the treatment chart in use on the ward. No record of any signature on this, fluid prescription chart used in HDU No record of the adverse event, or the completion of the Safecode, in the nursing notes
28 Key Learning: The computer system had a large part to play with highlighting both staffing issues an the shortcomings of the system. New system due to be installed this year Although difficulty in recruitment, now 2 members of staff are the norm in the laboratory Practice now changed - a second BMS should check and sign against the units for platelets Education deficits are currently being addressed by the Transfusion Nurse Specialist with the HDU staff re ABO compatibility and record keeping
29 Benefits of using RCA highlighted by Trust 1 & 2 Original investigation focussed on completing the questions raised by the SHOT reporting form- looked at immediate cause of the incident, e.g., in Trust 1, the incorrect verbal report by the NBS The true root causes were identified beyond the immediate obvious errors Use of the time line meant that a chronology of the patient s healthcare records was carried out, ensuring that questions were raised around any gaps in information A comprehensive process to follow when carrying out an RCA. Well structured report at the end of the RCA investigation
30 Other benefits Impressed by RCA investigation approach setting up with Transfusion Nurse Specialist, a framework for investigating future blood transfusion errors Although the incident had been key in influencing the purchase of a single database, key learning re patient transfer between hospitals will be a main feature of the education programme Greater understanding of the how and why the incident occurred. Showed that there was more than one issue that needed addressing
31 Further RCA Training The NPSA will be providing a RCA training in the following ways, commending its programme in November: RCA 1 day foundation course for any type/level of staff 3 day RCA course for Trust RCA facilitators in 800 Trusts Master Classes in RCA
Lessons for Transfusion Laboratory Staff. from the 2007 SHOT Report SHOT SERIOUS HAZARDS OF TRANSFUSION
 Lessons for Transfusion Laboratory Staff from the 2007 SHOT Report SERIOUS HAZARDS OF TRANSFUSION SHOT The Serious Hazards of Transfusion Scheme (SHOT) is a UK-wide confidential enquiry that collects data
Lessons for Transfusion Laboratory Staff from the 2007 SHOT Report SERIOUS HAZARDS OF TRANSFUSION SHOT The Serious Hazards of Transfusion Scheme (SHOT) is a UK-wide confidential enquiry that collects data
Sample. A guide to development of a hospital blood transfusion Policy at the hospital level. Effective from April Hospital Transfusion Committee
 Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
UK TRANSFUSION LABORATORY COLLABORATIVE
 UK TRANSFUSION LABORATORY COLLABORATIVE 2017 survey indicates that staff shortages are not being addressed Authors: Hema Mistry, Rashmi Rook and Paula HB Bolton-Maggs No Disclosures Introduction UK transfusion
UK TRANSFUSION LABORATORY COLLABORATIVE 2017 survey indicates that staff shortages are not being addressed Authors: Hema Mistry, Rashmi Rook and Paula HB Bolton-Maggs No Disclosures Introduction UK transfusion
Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE
 Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE Acknowledgement and disclaimer Funding acknowledgement: This project is funded by the National Institute for Health Research Health
Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE Acknowledgement and disclaimer Funding acknowledgement: This project is funded by the National Institute for Health Research Health
Why do we make mistakes? Human factors in transfusion practice
 Why do we make mistakes? Human factors in transfusion practice East of England Regional Transfusion Committee Blood transfusion: What now? What if? What next? Alison Watt SHOT Operations Manager Paula
Why do we make mistakes? Human factors in transfusion practice East of England Regional Transfusion Committee Blood transfusion: What now? What if? What next? Alison Watt SHOT Operations Manager Paula
Root Cause Analysis of Transfusion Incidents The Leeds Experience
 Root Cause Analysis of Transfusion Incidents The Leeds Experience Richard Haggas Quality Manager, Blood Transfusion Lab Claire Thompson Transfusion Nurse Practitioner, Hospital Transfusion Team LTH Transfusion
Root Cause Analysis of Transfusion Incidents The Leeds Experience Richard Haggas Quality Manager, Blood Transfusion Lab Claire Thompson Transfusion Nurse Practitioner, Hospital Transfusion Team LTH Transfusion
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Guidance Notes on the Investigation of Marine Incidents
 Guidance Notes on the Investigation of Marine Incidents Incidents & Human Element Incidents (accidents and near misses) and their causes must be identified and documented Including the role of humans in
Guidance Notes on the Investigation of Marine Incidents Incidents & Human Element Incidents (accidents and near misses) and their causes must be identified and documented Including the role of humans in
Clinical Governance & Risk Management Awareness. Incl. investigation of accidents, complaints and claims. Unit 2
 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
Page 1 of 5 Version No: 6 Authorised by: General Counsel
 Feedback Action Analysis Prioritisation Classificattion Notification Identification INCIDENT MANAGEMENT Patient informed / Family informed if required Event occurs If staff injury form must be printed,
Feedback Action Analysis Prioritisation Classificattion Notification Identification INCIDENT MANAGEMENT Patient informed / Family informed if required Event occurs If staff injury form must be printed,
Safe medication practice what can we learn from root cause analysis and related methods?
 Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Better Blood Transfusion & anti-d Immunoglobulin
 Better Blood Transfusion & anti-d Immunoglobulin - an analysis of adverse events reports from the Serious Hazards of Transfusion scheme Tony Davies - Transfusion Liaison Practitioner SHOT / NHSBT The Royal
Better Blood Transfusion & anti-d Immunoglobulin - an analysis of adverse events reports from the Serious Hazards of Transfusion scheme Tony Davies - Transfusion Liaison Practitioner SHOT / NHSBT The Royal
Changes in practice and organisation surrounding blood transfusion in NHS trusts in England
 See Commentary, p 236 1 National Blood Service, Birmingham, UK; 2 National Blood Service, Oxford, UK; 3 Clinical Evaluation and Effectiveness Unit, Royal College of Physicians, London, UK Correspondence
See Commentary, p 236 1 National Blood Service, Birmingham, UK; 2 National Blood Service, Oxford, UK; 3 Clinical Evaluation and Effectiveness Unit, Royal College of Physicians, London, UK Correspondence
Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant
 Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant Today s presentation is an overview of the Investigating Workplace
Introduction to Investigating Workplace Incidents January 25 th, 2017 Presented by: Jack Slessor SAFE Work Manitoba Prevention Consultant Today s presentation is an overview of the Investigating Workplace
The Newcastle upon Tyne Hospitals NHS Foundation Trust
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Incidents, Accidents and the Trust Disciplinary Process - Guidelines for Managers, Clinical Directors and Employees Version.: 4.1 Effective From:
The Newcastle upon Tyne Hospitals NHS Foundation Trust Incidents, Accidents and the Trust Disciplinary Process - Guidelines for Managers, Clinical Directors and Employees Version.: 4.1 Effective From:
The Patient Safety Act Reporting and RCA Requirements
 The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
Chapter 13. Documenting Clinical Activities
 Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
SOP:14:QA:110:01:NIBT PAGE 1 of 8
 SOP:14:QA:110:01:NIBT PAGE 1 of 8 Northern Ireland Blood Transfusion Service STANDARD OPERATING PROCEDURE (Operational Copy) Document Details Document Number: SOP:14:QA:110:01:NIBT Supersedes Number: Not
SOP:14:QA:110:01:NIBT PAGE 1 of 8 Northern Ireland Blood Transfusion Service STANDARD OPERATING PROCEDURE (Operational Copy) Document Details Document Number: SOP:14:QA:110:01:NIBT Supersedes Number: Not
Unit 2 Clinical Governance & Risk Management Awareness
 Unit 2 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Unit 2 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Policy for the Investigation, Analysis and Learning from Incidents, Complaints and Claims
 Policy for the Investigation, Analysis and Learning from Incidents, Complaints and Claims Please be aware that this printed version of the Policy may NOT be the latest version. Staff are reminded that
Policy for the Investigation, Analysis and Learning from Incidents, Complaints and Claims Please be aware that this printed version of the Policy may NOT be the latest version. Staff are reminded that
Management of Reported Medication Errors Policy
 Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
The Newcastle Upon Tyne Hospitals NHS Foundation Trust. Procedure for Incident Investigation. Effective Date: December 2007 Review Date: December 2010
 The Newcastle Upon Tyne Hospitals NHS Foundation Trust Procedure for Incident Investigation Effective Date: December 2007 Review Date: December 2010 1. Introduction 1.1 Many people feel that errors are
The Newcastle Upon Tyne Hospitals NHS Foundation Trust Procedure for Incident Investigation Effective Date: December 2007 Review Date: December 2010 1. Introduction 1.1 Many people feel that errors are
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS
 I International Symposium Engineering Management And Competitiveness 2011 (EMC2011) June 24-25, 2011, Zrenjanin, Serbia EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS Branislav Tomić * Senior
I International Symposium Engineering Management And Competitiveness 2011 (EMC2011) June 24-25, 2011, Zrenjanin, Serbia EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS Branislav Tomić * Senior
Patient Safety Hazard Risk Assessment FY 2018
 Completed by: Patient Safety Committee Date Completed: Ocber 31, 2017 Methodology: Information utilized complete this Patient Safety Hazard Assessment included availa patterns/trends, high risk, prom prone
Completed by: Patient Safety Committee Date Completed: Ocber 31, 2017 Methodology: Information utilized complete this Patient Safety Hazard Assessment included availa patterns/trends, high risk, prom prone
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
Reducing MRSA. HCAIs are a disgrace. Does your CE know about HCAIs as quickly as 4 hour wait or waiting list breaches?
 Reducing MRSA HCAIs are a disgrace Does your CE know about HCAIs as quickly as 4 hour wait or waiting list breaches? How can a Trust succeed in financial turnaround if patients are languishing on the wards
Reducing MRSA HCAIs are a disgrace Does your CE know about HCAIs as quickly as 4 hour wait or waiting list breaches? How can a Trust succeed in financial turnaround if patients are languishing on the wards
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Competency Assessment for Non Medical Prescribing of Blood and Blood Components
 Competency Assessment for Non Medical Prescribing of Blood and Blood Components Name of Candidate (please print). Ward/Department:... Band/Job Title:.. Professional Registration Number Date initial in-house
Competency Assessment for Non Medical Prescribing of Blood and Blood Components Name of Candidate (please print). Ward/Department:... Band/Job Title:.. Professional Registration Number Date initial in-house
Safe Blood Transfusion
 Safe Blood Transfusion Cardiff & Vale uhb & Welsh Blood Service Education Sub-group Objectives Complex pathway Overview ~ pre-transfusion blood sampling ~ collection from blood bank fridge ~ administration
Safe Blood Transfusion Cardiff & Vale uhb & Welsh Blood Service Education Sub-group Objectives Complex pathway Overview ~ pre-transfusion blood sampling ~ collection from blood bank fridge ~ administration
JOB DESCRIPTION. Specialist Practitioner of Transfusion for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:-
 JOB DESCRIPTION Job Title:- Specialist Practitioner of for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:- Associate Director of Patient Safety Professionally Accountability
JOB DESCRIPTION Job Title:- Specialist Practitioner of for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:- Associate Director of Patient Safety Professionally Accountability
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
Policies, Procedures, Guidelines and Protocols
 Policies, Procedures, Guidelines and Protocols Document Details Title Complaints and Compliments Policy Trust Ref No 1353-29025 Local Ref (optional) N/A Main points the document This policy and procedure
Policies, Procedures, Guidelines and Protocols Document Details Title Complaints and Compliments Policy Trust Ref No 1353-29025 Local Ref (optional) N/A Main points the document This policy and procedure
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
List of Policies and Standard Operational Procedures (SOPs) for cell collection, processing and transplantation programmes
 for cell collection, processing and transplantation programmes") Format of SOPs (SOPs) for cell collection, processing and transplantation programmes There must be an SOP covering the procedure of preparing, implementing and revising all procedures and an SOP for document
Format of SOPs (SOPs) for cell collection, processing and transplantation programmes There must be an SOP covering the procedure of preparing, implementing and revising all procedures and an SOP for document
Fitting Automation into a Small Transfusion Service
 Fitting Automation into a Small Transfusion Service Jo Bruner, MLS (ASCP) CM Blood Bank, Hematology & Coagulation Section Head Fulton County Health Center Laboratory Objectives - List the advantages and
Fitting Automation into a Small Transfusion Service Jo Bruner, MLS (ASCP) CM Blood Bank, Hematology & Coagulation Section Head Fulton County Health Center Laboratory Objectives - List the advantages and
STANDARD OPERATING PROCEDURE FOR PATIENT HISTORY CHECK
 STANDARD OPERATING PROCEDURE FOR PATIENT HISTORY CHECK 1.0 Principle 1.1 To review current patient results with previous records for possible discrepancies to check for special instructions or comments
STANDARD OPERATING PROCEDURE FOR PATIENT HISTORY CHECK 1.0 Principle 1.1 To review current patient results with previous records for possible discrepancies to check for special instructions or comments
DON T GIVE UNIT TWO WITHOUT REVIEW!
 DON T GIVE UNIT TWO WITHOUT REVIEW! Single Unit Blood Transfusion QIP Dr Aqeem Azam CT1 Dr Sarah Clegg FY1 Nobles Hospital, Isle of Man SMART Aim To increase the percentage of RBC transfusions given as
DON T GIVE UNIT TWO WITHOUT REVIEW! Single Unit Blood Transfusion QIP Dr Aqeem Azam CT1 Dr Sarah Clegg FY1 Nobles Hospital, Isle of Man SMART Aim To increase the percentage of RBC transfusions given as
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA
 Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Manchester Patient Safety Framework (MaPSaF) Ambulance
 Ambulance") Manchester Patient Safety Framework (MaPSaF) Ambulance How to use MaPSaF MaPSaF is best used as a team based self-reflection and educational exercise: it should be used by all appropriate members of your
Manchester Patient Safety Framework (MaPSaF) Ambulance How to use MaPSaF MaPSaF is best used as a team based self-reflection and educational exercise: it should be used by all appropriate members of your
DEVELOPING AND IMPLEMENTING A CORRECTIVE ACTION PLAN
 DEVELOPING AND IMPLEMENTING A CORRECTIVE ACTION PLAN Linda Ohler, MSN, RN, CCTC, FAAN Quality and Regulatory Manager George Washington University Transplant Institute And Editor, Progress in Transplantation
DEVELOPING AND IMPLEMENTING A CORRECTIVE ACTION PLAN Linda Ohler, MSN, RN, CCTC, FAAN Quality and Regulatory Manager George Washington University Transplant Institute And Editor, Progress in Transplantation
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME
 Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Blood Transfusion Policy. Version Number: 6.1 Controlled Document Sponsor: Controlled Document Lead: On: December 2014.
 Blood Transfusion Policy CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Policy Clinical The policy describes the framework and principles required to deliver best transfusion
Blood Transfusion Policy CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Policy Clinical The policy describes the framework and principles required to deliver best transfusion
Appendix 5. Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to the Safeguarding Adults Procedures
 Appendix 5 Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to the Safeguarding Adults Procedures Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to
Appendix 5 Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to the Safeguarding Adults Procedures Safeguarding Adults and Pressure Ulcer Protocol: Deciding whether to refer to
Patient Safety Case Study. Clara K. Terral. Angelo State University
 Running Head: PATIENT SAFTEY CASE STUDY Patient Safety Case Study Clara K. Terral Angelo State University PATIENT SAFTEY CASE STUDY 2 The case study that stood out most to me was Case 18, which is Not
Running Head: PATIENT SAFTEY CASE STUDY Patient Safety Case Study Clara K. Terral Angelo State University PATIENT SAFTEY CASE STUDY 2 The case study that stood out most to me was Case 18, which is Not
Check-Plan-Do-Check-Act-Cycle
 Adequacy of hemodialysis 1 Adequacy of Hemodialysis Introduction Providing adequate hemodialysis treatment is dependent on numerous factors ranging from type of dialyzer used to appropriate length of treatment
Adequacy of hemodialysis 1 Adequacy of Hemodialysis Introduction Providing adequate hemodialysis treatment is dependent on numerous factors ranging from type of dialyzer used to appropriate length of treatment
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Root Cause Analysis Investigation Report. The Royal National Orthopaedic Hospital
 Root Cause Analysis Investigation Report The Royal National Orthopaedic Hospital Root Cause Analysis on a case of Clostridium Difficile on Margaret Harte March 2012 CONTENTS Incident description and consequences
Root Cause Analysis Investigation Report The Royal National Orthopaedic Hospital Root Cause Analysis on a case of Clostridium Difficile on Margaret Harte March 2012 CONTENTS Incident description and consequences
REPORT OF BLOOD SAFETY REVIEW
 REPORT OF BLOOD SAFETY REVIEW 11 th February 2010 Table of Contents Acknowledgements 2 The Review Team 3 1 Context for Review 4-5 2 Background 6 3 HSS Circular MD 6/03: Better Blood Transfusion 7-8 4 National
REPORT OF BLOOD SAFETY REVIEW 11 th February 2010 Table of Contents Acknowledgements 2 The Review Team 3 1 Context for Review 4-5 2 Background 6 3 HSS Circular MD 6/03: Better Blood Transfusion 7-8 4 National
SOUTH EAST COAST AMBULANCE SERVICE NHS TRUST. General Risk Assessment Form
 Assessment No. General Risk Assessment Form Completed by and role: Karen Dawes PTS Manager Initial assessment date: 14.09.12 Location of the risk: Vehicle General Assessment of GJ52 GZA Task / Hazard being
Assessment No. General Risk Assessment Form Completed by and role: Karen Dawes PTS Manager Initial assessment date: 14.09.12 Location of the risk: Vehicle General Assessment of GJ52 GZA Task / Hazard being
Putting the Person in Person- Centered Care Plans. Patty Austin, RN, CPHQ Penny Imes, RN, BSN
 Putting the Person in Person- Centered Care Plans Patty Austin, RN, CPHQ Penny Imes, RN, BSN Objectives Discuss person centered care plans as they relate to regulations and new rule Demonstrate the use
Putting the Person in Person- Centered Care Plans Patty Austin, RN, CPHQ Penny Imes, RN, BSN Objectives Discuss person centered care plans as they relate to regulations and new rule Demonstrate the use
Blood / Blood Products Transfusion A Liquid Transplant
 Blood / Blood Products Transfusion A Liquid Transplant Caroline Holt Specialist Practitioner of Transfusion caroline.holt@tgh.nhs.uk Tel : 922 5484 Mob: 07759260044 The Transfusion Team Gillian Lewis Blood
Blood / Blood Products Transfusion A Liquid Transplant Caroline Holt Specialist Practitioner of Transfusion caroline.holt@tgh.nhs.uk Tel : 922 5484 Mob: 07759260044 The Transfusion Team Gillian Lewis Blood
February New Zealand Health and Disability Services National Reportable Events Policy 2012
 February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
Meeting of Bristol Clinical Commissioning Group Governing Body. Title: Bristol CCG Management of Serious Incidents Agenda Item: 17
 Meeting of Bristol Clinical Commissioning Group Governing Body To be held on Tuesday 22 December 2015 commencing at 13:30 at the Greenway Centre, Doncaster Road, Bristol, BS10 5PY Title: Bristol CCG Management
Meeting of Bristol Clinical Commissioning Group Governing Body To be held on Tuesday 22 December 2015 commencing at 13:30 at the Greenway Centre, Doncaster Road, Bristol, BS10 5PY Title: Bristol CCG Management
CLINICAL PROTOCOL FOR THE IDENTIFICATION OF SERVICE USERS
 CLINICAL PROTOCOL FOR THE IDENTIFICATION OF SERVICE USERS RATIONALE All Professionals/healthcare workers are personally accountable for their practice and, in the exercise of their professional accountability,
CLINICAL PROTOCOL FOR THE IDENTIFICATION OF SERVICE USERS RATIONALE All Professionals/healthcare workers are personally accountable for their practice and, in the exercise of their professional accountability,
POLICY FOR INCIDENT AND SERIOUS INCIDENT REPORTING
 POLICY FOR INCIDENT AND SERIOUS INCIDENT REPORTING Policy Acceptance Applies to: All staff, patients, & carers Date Issued: 7 th March 2016 Status Ratified Version 4 Date for Review March 2018 Responsible
POLICY FOR INCIDENT AND SERIOUS INCIDENT REPORTING Policy Acceptance Applies to: All staff, patients, & carers Date Issued: 7 th March 2016 Status Ratified Version 4 Date for Review March 2018 Responsible
Manis Aged Care Limited
 Manis Aged Care Limited Introduction This report records the results of a Surveillance Audit of a provider of aged residential care services against the Health and Disability Services Standards (NZS8134.1:2008;
Manis Aged Care Limited Introduction This report records the results of a Surveillance Audit of a provider of aged residential care services against the Health and Disability Services Standards (NZS8134.1:2008;
INCIDENT POLICY Page 1 of 15 July 2017
 Page 1 of 15 Policy Applies To All Mercy Hospital Staff Credentialed Medical Specialists and Allied Health Personnel are required to indicate understanding of the incident policy via the credentialing
Page 1 of 15 Policy Applies To All Mercy Hospital Staff Credentialed Medical Specialists and Allied Health Personnel are required to indicate understanding of the incident policy via the credentialing
Policy for the Reporting and Management of Incidents Including Serious Incidents. Version Number: 006
 CONTROLLED DOCUMENT Policy for the Reporting and Management of Incidents Including Serious Incidents CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the principles
CONTROLLED DOCUMENT Policy for the Reporting and Management of Incidents Including Serious Incidents CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the principles
HAEMOVIGILANCE POLICY
 REASON FOR ISSUE: New document describing Haemovigilance System 1. INTRODUCTION NZBS has adopted the Council of Europe definition that states that haemovigilance is: The organised surveillance procedures
REASON FOR ISSUE: New document describing Haemovigilance System 1. INTRODUCTION NZBS has adopted the Council of Europe definition that states that haemovigilance is: The organised surveillance procedures
Seniorcare Geraldine Incorporated
 Seniorcare Geraldine Incorporated Introduction This report records the results of a Surveillance Audit of a provider of aged residential care services against the Health and Disability Services Standards
Seniorcare Geraldine Incorporated Introduction This report records the results of a Surveillance Audit of a provider of aged residential care services against the Health and Disability Services Standards
ECRI Patient Safety Organization HFACS and Healthcare
 October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
Understanding safety culture to improve the safety of individual patients
 Understanding safety culture to improve the safety of individual patients Prof Darren Ashcroft Director, Centre for Innovation in Practice School of Pharmacy and Pharmaceutical Sciences University of Manchester,
Understanding safety culture to improve the safety of individual patients Prof Darren Ashcroft Director, Centre for Innovation in Practice School of Pharmacy and Pharmaceutical Sciences University of Manchester,
Clinical Interdepartmental Policy and Procedure
 Clinical Interdepartmental Policy and Procedure Policy: Staff Response to Medical Errors/Adverse Events Policy Number: MR-006 Joseph S. Gordy, CEO Signature: Flagler Hospital Originator: President Coordinating
Clinical Interdepartmental Policy and Procedure Policy: Staff Response to Medical Errors/Adverse Events Policy Number: MR-006 Joseph S. Gordy, CEO Signature: Flagler Hospital Originator: President Coordinating
Irradiated blood products - Pathway for requesting To provide healthcare professionals with clear guidance on the use of irradiated blood products.
 Document Title: Document Purpose: Document Statement: Document Application: Responsible for Implementation: Irradiated blood products - Pathway for requesting To provide healthcare professionals with clear
Document Title: Document Purpose: Document Statement: Document Application: Responsible for Implementation: Irradiated blood products - Pathway for requesting To provide healthcare professionals with clear
The document has been issued to:- Name Position Department Date
 VALIDATION PROTOCOL PARTICIPANTS: Validation of Traceability / Return Label VALIDATION REF # Prepared by: The document has been
VALIDATION PROTOCOL PARTICIPANTS: Validation of Traceability / Return Label VALIDATION REF # Prepared by: The document has been
Trust Policy for Blood Transfusion
 Trust Policy for Blood Transfusion Approval and Authorisation Reviewed by Job Title Date Simon Middleton Chair of Hospital Transfusion Committee 03.09.2010 Rebecca Sampson Consultant Haematologist 01.09.2010
Trust Policy for Blood Transfusion Approval and Authorisation Reviewed by Job Title Date Simon Middleton Chair of Hospital Transfusion Committee 03.09.2010 Rebecca Sampson Consultant Haematologist 01.09.2010
Guidance for completing the Internal Agency Investigation Report. This form requires completion within 28 days of the alert being raised.
 Guidance for completing the Internal Agency Investigation Report The purpose of this is to support managers completing the Mandatory Internal Agency Investigation Report. This report should be completed
Guidance for completing the Internal Agency Investigation Report The purpose of this is to support managers completing the Mandatory Internal Agency Investigation Report. This report should be completed
Incident Reporting and Learning
 Section 3 Incident Reporting and Learning Contents Guidelines to defining and managing all radiation incidents Definition of a Patient Radiation Incident Definition of a Near Miss Patient Radiation Incident
Section 3 Incident Reporting and Learning Contents Guidelines to defining and managing all radiation incidents Definition of a Patient Radiation Incident Definition of a Near Miss Patient Radiation Incident
How to Report Medication Safety Incidents from a GP Practice on the National Reporting and Learning System (NRLS)
") pecialist Pharmacy ervice Medicines Use and afety How to Report Medication afety Incidents from a GP Practice on the National Reporting and Learning ystem (NRL) This document provides a quick explanation
pecialist Pharmacy ervice Medicines Use and afety How to Report Medication afety Incidents from a GP Practice on the National Reporting and Learning ystem (NRL) This document provides a quick explanation
Administration of blood components. Denise Watson Patient Blood Management Practitioner 11th January, 2016
 Administration of blood components Denise Watson Patient Blood Management Practitioner 11th January, 2016 Introduction British Committee for Standards in Haematology guidelines Administration process Case
Administration of blood components Denise Watson Patient Blood Management Practitioner 11th January, 2016 Introduction British Committee for Standards in Haematology guidelines Administration process Case
A summary of: Five years of cerebral palsy claims
 A summary of: Five years of cerebral palsy claims A thematic review of NHS Resolution data September 2017 Advise / Resolve / Learn Our report Five years of cerebral palsy claims, provides an in-depth examination
A summary of: Five years of cerebral palsy claims A thematic review of NHS Resolution data September 2017 Advise / Resolve / Learn Our report Five years of cerebral palsy claims, provides an in-depth examination
Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator
 Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator Presented at Webex Conferences: July 20, 21, & 22, 2010 Blood Sample Labeling Seminar 6255 West Sunset Blvd Los Angeles, CA Blood
Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator Presented at Webex Conferences: July 20, 21, & 22, 2010 Blood Sample Labeling Seminar 6255 West Sunset Blvd Los Angeles, CA Blood
PGY1 Medication Safety Core Rotation
 PGY1 Medication Safety Core Rotation Preceptor: Mike Wyant, RPh Hours: 0800 to 1730 M-F Contact: (541)789-4657, michael.wyant@asante.org General Description This rotation is a four week rotation in duration.
PGY1 Medication Safety Core Rotation Preceptor: Mike Wyant, RPh Hours: 0800 to 1730 M-F Contact: (541)789-4657, michael.wyant@asante.org General Description This rotation is a four week rotation in duration.
Risk Management Policy: overarching framework
 Title: Management Policy: overarching framework Issue No: 3 No. of Pages (including front page) 31 Prepared by: CEO Regional Directors Date: November 2014 Implementation by: Local Managers Person in Charge
Title: Management Policy: overarching framework Issue No: 3 No. of Pages (including front page) 31 Prepared by: CEO Regional Directors Date: November 2014 Implementation by: Local Managers Person in Charge
Emergency Blood Supply and Disaster Management Policy
 Emergency Blood Supply and Disaster Management Policy National Blood Service, Ghana EMERGENCY BLOOD SUPPLY AND DISASTER MANAGEMENT POLICY First Edition 2013 Emergency Blood Supply and Disaster Management
Emergency Blood Supply and Disaster Management Policy National Blood Service, Ghana EMERGENCY BLOOD SUPPLY AND DISASTER MANAGEMENT POLICY First Edition 2013 Emergency Blood Supply and Disaster Management
Laboratory Errors n=455 and MHRA 5 Serious Adverse Events n=765
 Laboratory Errors n=455 and MHRA 5 Serious Adverse Events n=765 Authors: Peter Baker, Joanne Bark, Hema Mistry and Chris Robbie Introduction This year the SHOT laboratory chapter has been written in conjunction
Laboratory Errors n=455 and MHRA 5 Serious Adverse Events n=765 Authors: Peter Baker, Joanne Bark, Hema Mistry and Chris Robbie Introduction This year the SHOT laboratory chapter has been written in conjunction
Incident and Serious Incident Management Policy
 Authors Sarah Hemsley Clinical Safety Manager Abi Eaves Patient Safety Manager Quality and Professional Development Leeds Community Healthcare NHS Trust Corporate Lead Angie Clegg Executive (Nurse) Director
Authors Sarah Hemsley Clinical Safety Manager Abi Eaves Patient Safety Manager Quality and Professional Development Leeds Community Healthcare NHS Trust Corporate Lead Angie Clegg Executive (Nurse) Director
Level 5 Diploma in Occupational Health and Safety Practice ( )
") Level 5 Diploma in Occupational Health and Safety Practice (3654-06) January 2017 Version 1.6 Qualification Handbook Qualification at a glance Subject area Health and Safety City & Guilds number 3654 Age
Level 5 Diploma in Occupational Health and Safety Practice (3654-06) January 2017 Version 1.6 Qualification Handbook Qualification at a glance Subject area Health and Safety City & Guilds number 3654 Age
Title: Massive Transfusion Event Protocol Policy: Clinical Manual/General Clinical
 Title: Massive Transfusion Event Protocol Policy: Manual/General I. POLICY: Massive Transfusion Event (MTE) Protocol: The MTE Protocol is initiated at the request of the anesthesiologist, surgeon or physician
Title: Massive Transfusion Event Protocol Policy: Manual/General I. POLICY: Massive Transfusion Event (MTE) Protocol: The MTE Protocol is initiated at the request of the anesthesiologist, surgeon or physician
Operations Director, Specialist Community & Regional Services Clinical Director, Mental Health Director of Nursing
 TO Hospital Advisory Committee FROM Operations Director, Specialist Community & Regional Services Clinical Director, Mental Health Director of Nursing DATE 26 August 2014 SUBJECT Mental Health Review MEMORANDUM
TO Hospital Advisory Committee FROM Operations Director, Specialist Community & Regional Services Clinical Director, Mental Health Director of Nursing DATE 26 August 2014 SUBJECT Mental Health Review MEMORANDUM
Learning from Actual & Near Miss Events
 POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
Root Cause Analysis Investigation Report. Clostridium Difficile Ian Monro Ward. The Royal National Orthopaedic Hospital
 Root Cause Analysis Investigation Report Clostridium Difficile Ian Monro Ward The Royal National Orthopaedic Hospital CONTENTS Incident description and consequences Pre-investigation risk assessment Background
Root Cause Analysis Investigation Report Clostridium Difficile Ian Monro Ward The Royal National Orthopaedic Hospital CONTENTS Incident description and consequences Pre-investigation risk assessment Background
Potential challenges when assessing organisational processes for assurance of clinical competence in labs with limited clinical staff resource
 Contents 1. Introduction... 1 2. Examples of Clinical Activity... 2 3. Automatic selection and reporting... 3 Appendix 1... 8 Appendix 2... 9 1. Introduction ISO 15189 is necessarily written such that
Contents 1. Introduction... 1 2. Examples of Clinical Activity... 2 3. Automatic selection and reporting... 3 Appendix 1... 8 Appendix 2... 9 1. Introduction ISO 15189 is necessarily written such that
Patient Care Coordination Variance Reporting
 Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Overview of Root Cause Analysis
 Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Problem Solving Tools
 Problem Solving Tools Report 162 Self Assessment of Radiation Safety Programs (2009) Report 173 - Investigation of Radiological Incidents (2012?) Mary L. Birch NC HPS Meeting October 4, 2012 Problem Solving
Problem Solving Tools Report 162 Self Assessment of Radiation Safety Programs (2009) Report 173 - Investigation of Radiological Incidents (2012?) Mary L. Birch NC HPS Meeting October 4, 2012 Problem Solving
Establishing and Implementing a Process to Investigate and Resolve Privacy Breaches and Complaints
 Establishing and Implementing a Process to Investigate and Resolve Privacy Breaches and Complaints Barbara Seitz, RHIA Privacy Officer/Director of HIM South Peninsula Hospital Homer, AK Becky Buegel, RHIA
Establishing and Implementing a Process to Investigate and Resolve Privacy Breaches and Complaints Barbara Seitz, RHIA Privacy Officer/Director of HIM South Peninsula Hospital Homer, AK Becky Buegel, RHIA
Seven steps to patient safety A guide for NHS staff
 Seven steps to patient safety A guide for NHS staff Seven steps to patient safety Step 1 Build a safety culture Step 2 Lead and support your staff Step 3 Integrate your risk management activity Step 4
Seven steps to patient safety A guide for NHS staff Seven steps to patient safety Step 1 Build a safety culture Step 2 Lead and support your staff Step 3 Integrate your risk management activity Step 4
MHA Patient Safety Organization
 MHA Patient Safety Organization Membership Benefits 2014 Copyright ECRI Institute PSO MHA PSO does more than analyze reported events and near misses. They provide members with tools and resources to help
MHA Patient Safety Organization Membership Benefits 2014 Copyright ECRI Institute PSO MHA PSO does more than analyze reported events and near misses. They provide members with tools and resources to help
Employer Link Service
 Employer Link Service Joint Regulator Workshop for Managers of Regulated Services Michele Harrison - Regulation Adviser, NMC 7 th March 2018 What we aim to cover Part 1 Who are the Employer Link Service?
Employer Link Service Joint Regulator Workshop for Managers of Regulated Services Michele Harrison - Regulation Adviser, NMC 7 th March 2018 What we aim to cover Part 1 Who are the Employer Link Service?
RCA in Healthcare 3/23/2017. Why Root Cause Analysis is Performed. Root Cause Analysis in Healthcare Part - 1. Contd. Contd.
 Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
The Power of Quality. Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center
 The Power of Quality Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center What do you think of when you hear the word quality? LEAN RCA PDSA QAPI SIX SIGMA PIP TQM 5s Objectives Transplant
The Power of Quality Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center What do you think of when you hear the word quality? LEAN RCA PDSA QAPI SIX SIGMA PIP TQM 5s Objectives Transplant
How effective and sustainable are Root. HFESA Conference
 How effective and sustainable are Root Cause Analysis (RCA) investigations 27 th November 2017 HFESA Conference Peter Hibbert, Matthew Thomas, Anita Deakin, Bill Runciman, Jeffrey Braithwaite Acknowledgements:
How effective and sustainable are Root Cause Analysis (RCA) investigations 27 th November 2017 HFESA Conference Peter Hibbert, Matthew Thomas, Anita Deakin, Bill Runciman, Jeffrey Braithwaite Acknowledgements:
Procedure for the Management of Incidents and Serious Incidents
 Procedure for the Management of Incidents and Serious Incidents This Procedure outlines the key actions staff should undertake in the management of incident and Serious Incidents occurring in NHS Lambeth
Procedure for the Management of Incidents and Serious Incidents This Procedure outlines the key actions staff should undertake in the management of incident and Serious Incidents occurring in NHS Lambeth