Root Cause Analysis A Necessary Evil? Dr Joseph Lui HA Convention 8 th May 2012
|
|
|
- Arnold Shelton
- 5 years ago
- Views:
Transcription

1 Root Cause Analysis A Necessary Evil? Dr Joseph Lui HA Convention 8 th May 2012
2
3 Root Cause Analysis (RCA) The use of RCA as an organization learning tool first deployed by Veteran Affairs Hospitals in US in 1990s then it has been adopted by National Patient Safety Agency in UK & Canada Hong Kong jumped on the bandwagon since 2003 Up to 2010, VA had conducted over 10,000 RCAs & Joint Commission over 4,000 RCAs


4 RCA Seminar

5 RCA Workshop 2003
6 What is RCA? Defined as an analytic method that is able to articulate the most basic cause that can be reasonably identified and that management has control to fix Livingstone et al, 2001 RCA enables clinicians to investigate serious incidents to identify the underlying causes and to guide solutions to address safety system failures State Government of Victoria, Australia, 2006
7 Four Major Attributes of RCA Thoroughness Fairness Efficiency Independence State Government of Victoria, Australia
8 It displaces attention from individual s actions Focus on system and recurrent practices It challenges staff to confront the underlying principles of an incident with the objective to engage in double loop learning (Argyris, 1999)
9 Fundamental Issues Is the Healthcare industry the same as the other High Risk industries like the nuclear plant industry or aviation industry? Can the RCA process be used as a learning tool as well as governance tool?
10 Issues In a NPSA evaluation, wide variation of standards of RCA reports among different trusts Examinations of RCAs from 7 practice regions in England suggested exemplary practice in 2, less rigor in 3, and scant evidence of recognizable features of RCAs in 2 (Wallace LM, 2006) Not all RCA participants were aware of whether outcomes were implemented, or whether it impacted on patient safety Identifying contributory factors is only the first step towards developing solutions
11 Training Issues (1) In the NPSA evaluation, wide variation of standards of RCA reports among different trusts Unlikely that skilled practice can be achieved simply by attendance at a 2-3 day workshop It may not be good enough just to teach about the RCA techniques May need to teach critical thinking so that the practitioner has the cognitive tools to address the complexity and novelty of new incidents Wallace LM, 2006
12 Training Issues (2) Possible Solutions Develop RCA template Develop Master class Adopt an accreditation system for RCA practitioners Need to develop a system of training to ensure newcomers are trained
13 Involvement of Patients in RCA (1) 46% of NPSA RCA practitioners welcome service users as part of the RCA team (Braithwaite J et al, 2006) In a NPSA study, only 16% of patient surveyed were consulted on how the incidents could be prevented in future and only 20% were told what the hospital would do to prevent a similar occurrence (Wallace LM, 2006)
14 Involvement of Patients in RCA (2) Potential Benefits Demonstrate the organization s transparency regarding errors and its responsiveness to patients Improves fact finding Facilitates HCP own healing Promotes forgiveness Improves outcome of the RCA Helps the organization re-establish trust with the patient Grissinger M, 2011
15 Involvement of Patients in RCA (3) Potential Risks to Patient (& Family) Harm through reliving the trauma May exacerbate grieving and affect objectivity Emotional impact on the patient or family may outweigh the benefit of participation Potential Risks to Organization Legal risk Staff discomfort Grissinger M, 2011
16 RCA Recommendations Issues Quality of Recommendations sometimes too board and general Some recommendations are of low-level controls or mitigating measures for risks identified, e.g. training or policy changes Recommendations are made around symptoms for root causes rather than root causes themselves From recommendations to implementation Sensible, achievable, practical?
17 Classification of Recommendations (1) Recommendation Category Alerts/warning/labeling Checklists Expected practice no policy Communication & documentation processes Education - general Education - targeted Environmental (modifications/ storage) Weak Classification Medium Strong Taitz J et al, 2010
18 Classification of Recommendations (2) Recommendation Category Equipment Counseling/ directive/ memo Organizational/ management/ rostering Policies/ procedures/ guidelines (incl. review) Staffing numbers or skill mix (incl. review) Workflow or process redesign Weak Classification Medium Strong Taitz J et al, 2010
19 The NSW Experience Medium 7% Strong 5% Weak Medium Strong Weak 88% Taitz J, et al, 2010
20 Signing Off on Recommendations Dilemma faced by senior management How to reconcile change initiatives recommended with the realities of resources limitation and organization inertia? To have the team revise unpalatable recommendations or outright reject them?
21 Incident Management Vs Complaint Management Complaints are often handled by staff other than those involved in risk management Complaints are seldom investigated using the RCA approach Often there are 2 parallel processes going on Clearly there is a disconnect between complaint management and incident management
22 Outcome Issues No studies in peer-reviewed literature on the effectiveness of RCA in reducing risk or improving safety No evaluations of cost-effectiveness of RCA compared with other tools in mitigating hazards Wu AW, 2008

23 The HA Experience
24 HA System for Root Cause Analysis Hospitals set up the Panel (external members, lay person) Done for all Sentinel Events and other incidents / Near misses if feel necessary Not link to Accountability system
25 HA System for Root Cause Analysis All RCA for Sentinel Events reviewed by Corporate RCA panel Feedbacks back to the Hospital via the RCA hospital visits Follow up visits 6 months to ensure improvement measures are in place
26 The HA Experience Between Oct 2009 and Sept 2011, a total of 77 sentinel events were reported A total 216 recommendations were made In 2 RCA, there were no recommendations
27 Classification of Recommendations (1) Recommendation Category Weak Alerts/warning/labeling 15 Classification Checklists 8 Expected practice no policy 0 Communication & documentation processes Education - general 0 Medium Strong 23 Education - targeted 17 Environmental (modifications/ storage) 26
28 Classification of Recommendations (2) Recommendation Category Weak Classification Medium Strong Equipment 3 Counseling/ directive/ memo 78 Organizational/ management/ rostering Policies/ procedures/ guidelines (incl. review) Staffing numbers or skill mix (incl. review) Workflow or process redesign
29 The HA Experience Strong 15% Weak Medium Strong Medium 25% Weak 60%
30 HA Vs NSW HA NSW Strong 15% Weak Medium Strong Medium 7% Strong 5% Weak Medium Strong Medium 25% Weak 60% Weak 88%


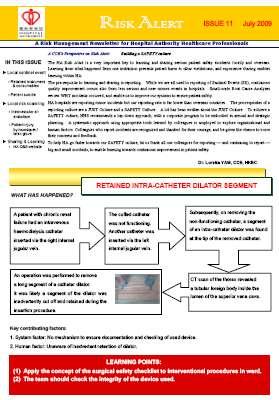
31 Some Examples of Recs Obstetric emergencies can occur anytime staff should be vigilant at all times To take appropriate measures to prevent, detect and manage complications of high risk pregnancy To alert staff on possibility of breakage of fragile consumables Emphasize use of appropriate pull force while pulling Hickman catheter through a tunnel


32 Some Example of Recs To develop and implement a Time-out practice to verify correct patient and correct site for bedside invasive procedure
33 How well are the recommendations being follow up? The Recommendation Explore feasibility of outreach team providing support to mentally ill patient during home leave on weekend and public holidays appears Jan 2010 X 2 Feb 2010 May 2010 June 2010 X 2 Feb 2011
34 How well are the recommendations being follow up? The Recommendation Design washroom to ensure that the partition are extended to the ceiling to minimize the risk of being used as supporting point for hanging appeared April 2011 X 2 June 2011




35 But We Do Have Success Stories.. Task force on Suicide Assessment tool ready Environmental screening



36 Sharing & Learning STAFF PUBLIC
37 Issues Identified by HA Quality Training Managers Depth of Recommendations Difference between clusters in their approach to processing recommendations Signing off process Implementation of recommendations at corporate level Corporate Incident Management Policy
38 Other Issues Patient and family participation in RCA Are we ready? Better communication of recommendations implementation
39 In Conclusion It is not a matter whether RCA is a necessary evil RCA is a useful tool and has contributed to the building of learning culture in HA However, in order that it won t lose its credibility and becomes just a ritual, we need to improve on the issues raised

40 Thank You
HALF YEAR REPORT ON SENTINEL EVENTS
 HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
How effective and sustainable are Root. HFESA Conference
 How effective and sustainable are Root Cause Analysis (RCA) investigations 27 th November 2017 HFESA Conference Peter Hibbert, Matthew Thomas, Anita Deakin, Bill Runciman, Jeffrey Braithwaite Acknowledgements:
How effective and sustainable are Root Cause Analysis (RCA) investigations 27 th November 2017 HFESA Conference Peter Hibbert, Matthew Thomas, Anita Deakin, Bill Runciman, Jeffrey Braithwaite Acknowledgements:
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA
 Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Root Cause Analysis (Part I) event/rca_assisttool.doc
 event/rca_assisttool.doc") (Part I) http://www.jcaho.org/accredited+organizations/sentinel+ event/rca_assisttool.doc Edited by Dr. E. Terry DIO Dr. S.K. Oliver OME Examines the reasons an error occurred Suggests changes to the system
(Part I) http://www.jcaho.org/accredited+organizations/sentinel+ event/rca_assisttool.doc Edited by Dr. E. Terry DIO Dr. S.K. Oliver OME Examines the reasons an error occurred Suggests changes to the system
United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI)
") United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI) March 11, 2015 Laura Lally, Caring Communities Victor Lane Rose, ECRI
United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI) March 11, 2015 Laura Lally, Caring Communities Victor Lane Rose, ECRI
NUCLEAR SAFETY PROGRAM
 Nuclear Safety Program Page 1 of 12 NUCLEAR SAFETY PROGRAM 1.0 Objective The objective of this performance assessment is to evaluate the effectiveness of the laboratory's nuclear safety program as implemented
Nuclear Safety Program Page 1 of 12 NUCLEAR SAFETY PROGRAM 1.0 Objective The objective of this performance assessment is to evaluate the effectiveness of the laboratory's nuclear safety program as implemented
BAY-ARENAC BEHAVIORAL HEALTH AUTHORITY POLICIES AND PROCEDURES MANUAL
 Page: 1 of 14 Policy It is the policy of Bay-Arenac Behavioral Health Authority (BABHA) that all adverse events, such as unusual events (including risk), critical incidents (including all deaths) and sentinel
Page: 1 of 14 Policy It is the policy of Bay-Arenac Behavioral Health Authority (BABHA) that all adverse events, such as unusual events (including risk), critical incidents (including all deaths) and sentinel
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
APEx Evidence Indicators: MIPS Improvement Activities
 APEx Evidence Indicators: Improvement Activities ASTRO s Accreditation Program for Excellence (APEx ) focuses on a culture of quality and safety, as well as patient-centered care. Evidence indicators required
APEx Evidence Indicators: Improvement Activities ASTRO s Accreditation Program for Excellence (APEx ) focuses on a culture of quality and safety, as well as patient-centered care. Evidence indicators required
Gantt Chart. Critical Path Method 9/23/2013. Some of the common tools that managers use to create operational plan
 Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Integrating Health Information Technology Safety into Nursing Informatics Competencies
 222 Forecasting Informatics Competencies for Nurses in the Future of Connected Health J. Murphy et al. (Eds.) 2017 IMIA and IOS Press. This article is published online with Open Access by IOS Press and
222 Forecasting Informatics Competencies for Nurses in the Future of Connected Health J. Murphy et al. (Eds.) 2017 IMIA and IOS Press. This article is published online with Open Access by IOS Press and
VA Radiotherapy Incident Reporting and Analysis System (RIRAS)
") VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
Patient Care Coordination Variance Reporting
 Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
E.H.R. s and Improving Patient Safety - What Has Been the Real Impact?
 E.H.R. s and Improving Patient Safety - What Has Been the Real Impact? Presented by: Mary Erickson, RN, HTS Accounting Manager HTS, a division of Mountain Pacific Quality Health Foundation 1 Understand
E.H.R. s and Improving Patient Safety - What Has Been the Real Impact? Presented by: Mary Erickson, RN, HTS Accounting Manager HTS, a division of Mountain Pacific Quality Health Foundation 1 Understand
Appendix G: The LFD Tool
 Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Changes in practice and organisation surrounding blood transfusion in NHS trusts in England
 See Commentary, p 236 1 National Blood Service, Birmingham, UK; 2 National Blood Service, Oxford, UK; 3 Clinical Evaluation and Effectiveness Unit, Royal College of Physicians, London, UK Correspondence
See Commentary, p 236 1 National Blood Service, Birmingham, UK; 2 National Blood Service, Oxford, UK; 3 Clinical Evaluation and Effectiveness Unit, Royal College of Physicians, London, UK Correspondence
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
ECRI Patient Safety Organization HFACS and Healthcare
 October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
Seven steps to patient safety A guide for NHS staff
 Seven steps to patient safety A guide for NHS staff Seven steps to patient safety Step 1 Build a safety culture Step 2 Lead and support your staff Step 3 Integrate your risk management activity Step 4
Seven steps to patient safety A guide for NHS staff Seven steps to patient safety Step 1 Build a safety culture Step 2 Lead and support your staff Step 3 Integrate your risk management activity Step 4
7084 MANAGEMENT OF INCIDENTS Facility Management Plan
 6 7084 MANAGEMENT OF INCIDENTS 7084.3 Facility Management Plan Each facility shall have a risk management plan that includes: 1. Explicit assignment of responsibilities for the facility s risk management
6 7084 MANAGEMENT OF INCIDENTS 7084.3 Facility Management Plan Each facility shall have a risk management plan that includes: 1. Explicit assignment of responsibilities for the facility s risk management
CLINICAL INCIDENT MANAGEMENT FRAMEWORK
 CLINICAL INCIDENT MANAGEMENT FRAMEWORK MY HEALTH RECORD SYSTEM PRASHAN MALALASEKERA NEVILLE BOARD 26 July 2016 My Health Record System My Health Record provides a repository of an individual s key health
CLINICAL INCIDENT MANAGEMENT FRAMEWORK MY HEALTH RECORD SYSTEM PRASHAN MALALASEKERA NEVILLE BOARD 26 July 2016 My Health Record System My Health Record provides a repository of an individual s key health
CROSSWALK FOR AADE S DIABETES EDUCATION ACCREDITATION PROGRAM
 Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
ANNUAL REPORT ON SENTINEL AND SERIOUS UNTOWARD EVENTS (1 October September 2011)
") 0 ANNUAL REPORT ON SENTINEL AND SERIOUS UNTOWARD EVENTS 1 October 2010 30 September 2011 HOSPITAL AUTHORITY HONG KONG 1 ACKNOWLEDGEMENT We would like to express our gratitude to all frontline staff, clinicians,
0 ANNUAL REPORT ON SENTINEL AND SERIOUS UNTOWARD EVENTS 1 October 2010 30 September 2011 HOSPITAL AUTHORITY HONG KONG 1 ACKNOWLEDGEMENT We would like to express our gratitude to all frontline staff, clinicians,
Objectives. Key Elements. ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management 5/20/2014
 ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
Patient Safety in Resource Poor Settings
 Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
MEDMARX ADVERSE DRUG EVENT REPORTING
 MEDMARX ADVERSE DRUG EVENT REPORTING Comparative Performance Reporting Helps to Reduce Adverse Drug Events Are you getting the most out of your adverse drug event (ADE) data? ADE reporting initiatives
MEDMARX ADVERSE DRUG EVENT REPORTING Comparative Performance Reporting Helps to Reduce Adverse Drug Events Are you getting the most out of your adverse drug event (ADE) data? ADE reporting initiatives
III International Conference on Patient Safety -- Patients for Patient Safety. Patient Safety Solutions
 III International Conference on Patient Safety -- Patients for Patient Safety Patient Safety Solutions Laura K. Botwinick Co-Director, Joint Commission International Center for Patient Safety Madrid 14
III International Conference on Patient Safety -- Patients for Patient Safety Patient Safety Solutions Laura K. Botwinick Co-Director, Joint Commission International Center for Patient Safety Madrid 14
QUALITY OPERATIONALIZED! Is your facility prepared?
 Performance Improvement Boot Camp For Assisted Living QUALITY OPERATIONALIZED! Is your facility prepared? Presented by: Barb Jezorski, RN, MSN & Brian R. Purtell WiCAL Executive Director 1 Objectives Describe
Performance Improvement Boot Camp For Assisted Living QUALITY OPERATIONALIZED! Is your facility prepared? Presented by: Barb Jezorski, RN, MSN & Brian R. Purtell WiCAL Executive Director 1 Objectives Describe
What Makes MFM Associates Unique? Privademics - A New Method of Delivering Expert Care
 We appreciate the confidence you have entrusted in us by choosing to become one of our patients. While we continue to keep pace with the latest advancements in health care, we never forget that each patient
We appreciate the confidence you have entrusted in us by choosing to become one of our patients. While we continue to keep pace with the latest advancements in health care, we never forget that each patient
Financial Disclosure. Learning Objectives: Preventing and Responding to Sentinel Events in Surgery 10/13/2015
 Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
High Reliability Organizations Healing Without Harm by 2014
 Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by 2014 1.1 Stand up if You have suffered harm as a patient at a hospital
Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by 2014 1.1 Stand up if You have suffered harm as a patient at a hospital
The Safety Risk Assessment: SRA Components: New in 2014 Falls 9/5/2014 HEALTHCARE REFORM AND DESIGN
 The Safety Risk Assessment: A new Guidelines requirement Ellen Taylor, AIA, MBA, EDAC Director of Research, The Center for Health Design HGRC Member 2014, 2018 * The views and opinions expressed in this
The Safety Risk Assessment: A new Guidelines requirement Ellen Taylor, AIA, MBA, EDAC Director of Research, The Center for Health Design HGRC Member 2014, 2018 * The views and opinions expressed in this
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
Preparing for ICD-10: Education and Clinical Documentation
 Preparing for ICD-10: Education and Clinical Documentation Agenda Background Road to Readiness Education Clinical Documentation Quick Start Today s presentation and recording will be sent to all attendees
Preparing for ICD-10: Education and Clinical Documentation Agenda Background Road to Readiness Education Clinical Documentation Quick Start Today s presentation and recording will be sent to all attendees
ASM. Common Operations Failure Modes in the Process Industries International Symposium. Dr. Peter Bullemer Human Centered Solutions
 Common Operations Failure Modes in the Process Industries 2009 International Symposium Beyond Regulatory Compliance, Making Safety Second Nature Dr. Peter Bullemer Human Centered Solutions Jason Laberge
Common Operations Failure Modes in the Process Industries 2009 International Symposium Beyond Regulatory Compliance, Making Safety Second Nature Dr. Peter Bullemer Human Centered Solutions Jason Laberge
The Hope Foundation SEED Fund for SWOG Early Exploration and Development 2016 Announcement
 The Hope Foundation SEED Fund for SWOG Early Exploration and Development 2016 Announcement OVERVIEW SWOG s mission is to improve the practice of cancer medicine in preventing, detecting, and treating cancer,
The Hope Foundation SEED Fund for SWOG Early Exploration and Development 2016 Announcement OVERVIEW SWOG s mission is to improve the practice of cancer medicine in preventing, detecting, and treating cancer,
System-wide learning from root cause analysis: a report from the New South Wales Root Cause Analysis Review Committee
 1 Clinical Excellence Commission, Martin Place, Sydney, New South Wales, Australia 2 Quality and Safety Branch, NSW Department of Health, North Sydney, New South Wales, Australia Correspondence to Dr Jonny
1 Clinical Excellence Commission, Martin Place, Sydney, New South Wales, Australia 2 Quality and Safety Branch, NSW Department of Health, North Sydney, New South Wales, Australia Correspondence to Dr Jonny
Re: Rewarding Provider Performance: Aligning Incentives in Medicare
 September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS
 I International Symposium Engineering Management And Competitiveness 2011 (EMC2011) June 24-25, 2011, Zrenjanin, Serbia EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS Branislav Tomić * Senior
I International Symposium Engineering Management And Competitiveness 2011 (EMC2011) June 24-25, 2011, Zrenjanin, Serbia EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS Branislav Tomić * Senior
Application of Simulation to Improve Clinical Efficiency Systems Integration
 Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Home administration of intravenous diuretics to heart failure patients:
 Quality and Productivity: Proposed Case Study Home administration of intravenous diuretics to heart failure patients: Increasing productivity and improving quality of care Provided by: British Heart Foundation
Quality and Productivity: Proposed Case Study Home administration of intravenous diuretics to heart failure patients: Increasing productivity and improving quality of care Provided by: British Heart Foundation
Defining incident-based peer review
 CHAPTER 1 Defining incident-based peer review Learning objectives After reading this chapter, the participant will be able to: Identify three external sources imposing higher nursing standards Discuss
CHAPTER 1 Defining incident-based peer review Learning objectives After reading this chapter, the participant will be able to: Identify three external sources imposing higher nursing standards Discuss
Overview of Root Cause Analysis
 Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
The Basic Principles of Developing Standards for Accreditation. Triona Fortune Deputy Chief Executive Officer 25 November 2014
 The Basic Principles of Developing Standards for Accreditation Triona Fortune Deputy Chief Executive Officer 25 November 2014 Overview- Standards Why? Where? Basic principles of how to write 2 3 What is
The Basic Principles of Developing Standards for Accreditation Triona Fortune Deputy Chief Executive Officer 25 November 2014 Overview- Standards Why? Where? Basic principles of how to write 2 3 What is
Standards of Practice for Hospice Programs (2010) (Veteran-related Standards)
 (Veteran-related Standards)") Standards of Practice for Hospice Programs (2010) (Veteran-related Standards) National Hospice and Palliative Care Organizations (NHPCO) Standards of Practice for Hospice Programs (2010) is a valuable
Standards of Practice for Hospice Programs (2010) (Veteran-related Standards) National Hospice and Palliative Care Organizations (NHPCO) Standards of Practice for Hospice Programs (2010) is a valuable
Self-Assessment Questionnaire: Establishing a Health Information Technology Safety Program
 Self-Assessment Questionnaire: Establishing a Health Information Technology Safety Program Initial assessment by: Date: In consultation with: Date of previous assessment: The success of a health information
Self-Assessment Questionnaire: Establishing a Health Information Technology Safety Program Initial assessment by: Date: In consultation with: Date of previous assessment: The success of a health information
ED0028 Adverse event, critical incident, serious issue, and near miss procedure
 ED0028 Adverse event, critical incident, serious issue, and near miss procedure 1. Full description Adverse event, critical incident, serious issue, 2. Preamble Doctors working in Australia have responsibilities
ED0028 Adverse event, critical incident, serious issue, and near miss procedure 1. Full description Adverse event, critical incident, serious issue, 2. Preamble Doctors working in Australia have responsibilities
Sentinel Event Data. Root Causes by Event Type Copyright, The Joint Commission
 Sentinel Event Data Root Causes by Event Type 2004 2014 Joint Commission Root Cause Information www.jointcommission.org/sentinel_event_policy_and_procedures/ Sentinel Events are reported to The Joint Commission
Sentinel Event Data Root Causes by Event Type 2004 2014 Joint Commission Root Cause Information www.jointcommission.org/sentinel_event_policy_and_procedures/ Sentinel Events are reported to The Joint Commission
CPPS RECERTIFICATION HANDBOOK
 CBPPS Certification Board for Professionals in Patient Safety 268 Summer Street, Sixth Floor Boston, MA 02210 info@cbpps.org CPPS RECERTIFICATION HANDBOOK Recertification Guidelines The Certified Professional
CBPPS Certification Board for Professionals in Patient Safety 268 Summer Street, Sixth Floor Boston, MA 02210 info@cbpps.org CPPS RECERTIFICATION HANDBOOK Recertification Guidelines The Certified Professional
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
SENTINEL AND SERIOUS UNTOWARD EVENTS
 ANNUAL REPORT ON SENTINEL AND SERIOUS UNTOWARD EVENTS 1 October 2012 30 September 2013 HOSPITAL AUTHORITY HONG KONG 1 ACKNOWLEDGEMENT This is the sixth Annual Report on Sentinel and Serious Untoward Events.
ANNUAL REPORT ON SENTINEL AND SERIOUS UNTOWARD EVENTS 1 October 2012 30 September 2013 HOSPITAL AUTHORITY HONG KONG 1 ACKNOWLEDGEMENT This is the sixth Annual Report on Sentinel and Serious Untoward Events.
Briefing: Quality governance for housing associations
 25 March 2014 Briefing: Quality governance for housing associations Quality and clinical governance in housing, care and support services Summary of key points: This paper is designed to support housing
25 March 2014 Briefing: Quality governance for housing associations Quality and clinical governance in housing, care and support services Summary of key points: This paper is designed to support housing
ANNUAL REPORT ON SENTINEL AND SERIOUS UNTOWARD EVENTS. October 2014 September 2015 HOSPITAL AUTHORITY HONG KONG
 ANNUAL REPORT ON SENTINEL AND SERIOUS UNTOWARD EVENTS October 2014 September 2015 HOSPITAL AUTHORITY HONG KONG January 2016 Annual Report on Sentinel and Serious Untoward Events October 2014 September
ANNUAL REPORT ON SENTINEL AND SERIOUS UNTOWARD EVENTS October 2014 September 2015 HOSPITAL AUTHORITY HONG KONG January 2016 Annual Report on Sentinel and Serious Untoward Events October 2014 September
Orientation to Risk Evaluation and Mitigation Strategies (REMS)
") Orientation to Risk Evaluation and Mitigation Strategies (REMS) Gary Slatko, MD Director, Off of Medication Error Prevention and Risk Management, OSE, CDER, FDA September 25, 2013 1 Background The REMS
Orientation to Risk Evaluation and Mitigation Strategies (REMS) Gary Slatko, MD Director, Off of Medication Error Prevention and Risk Management, OSE, CDER, FDA September 25, 2013 1 Background The REMS
Reporting and Disclosing Adverse Events
 Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
Supporting Healing. Restoring Hope.
 Session Code: M22 This presenter has nothing to disclose Supporting Healing. Restoring Hope. Linda K. Kenney President, MITSS (Medically Induced Trauma Support Services) IHI Forum, December 2013 Orlando,
Session Code: M22 This presenter has nothing to disclose Supporting Healing. Restoring Hope. Linda K. Kenney President, MITSS (Medically Induced Trauma Support Services) IHI Forum, December 2013 Orlando,
EP7f, CN III OB Hemorrhage.pdf OBSTETRIC HEMORRHAGE. Amelia Indig RN Clinical Nurse III Candidate December 17, 2009
 OBSTETRIC HEMORRHAGE Amelia Indig RN Clinical Nurse III Candidate December 17, 2009 1 OBJECTIVE OF THE PROJECT EP7f, CN III OB Hemorrhage.pdf Determine opportunities to improve patient safety and quality
OBSTETRIC HEMORRHAGE Amelia Indig RN Clinical Nurse III Candidate December 17, 2009 1 OBJECTIVE OF THE PROJECT EP7f, CN III OB Hemorrhage.pdf Determine opportunities to improve patient safety and quality
EXECUTIVE SUMMARY. The Military Health System. Military Health System Review Final Report August 29, 2014
 EXECUTIVE SUMMARY On May 28, 2014, the Secretary of Defense ordered a comprehensive review of the Military Health System (MHS). The review was directed to assess whether: 1) access to medical care in the
EXECUTIVE SUMMARY On May 28, 2014, the Secretary of Defense ordered a comprehensive review of the Military Health System (MHS). The review was directed to assess whether: 1) access to medical care in the
Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD
 Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
National Patient Safety Agency Root Cause Analysis (RCA) Investigation
 Investigation") National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager
 Ratchada Prakongsai Senior Manager") Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
 BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
A Million Little Pieces: Developing a Controlled Substance Diversion Program. Tanya Y. Barnhart, PharmD, BCPS
 A Million Little Pieces: Developing a Controlled Substance Diversion Program Tanya Y. Barnhart, PharmD, BCPS I have no conflicts of interest to disclose Objectives Explain the importance of building a
A Million Little Pieces: Developing a Controlled Substance Diversion Program Tanya Y. Barnhart, PharmD, BCPS I have no conflicts of interest to disclose Objectives Explain the importance of building a
Objective: To practice quality improvement tools by applying them to an improvement effort in an ambulatory care setting.
 Exercise 1 Objective: To practice quality improvement tools by applying them to an improvement effort in an ambulatory care setting. 1. Read the following case study. 2. Follow the instructions at the
Exercise 1 Objective: To practice quality improvement tools by applying them to an improvement effort in an ambulatory care setting. 1. Read the following case study. 2. Follow the instructions at the
Facility Assessment: How to Use the Toolkit
 Facility Assessment: How to Use the Toolkit State logo added here. If not, delete text box How to Use the Facility Assessment Toolkit The RoP Facility Assessment Toolkit is designed to provide practical,
Facility Assessment: How to Use the Toolkit State logo added here. If not, delete text box How to Use the Facility Assessment Toolkit The RoP Facility Assessment Toolkit is designed to provide practical,
AONE Nurse Executive Competencies Assessment Tool
 AONE Nurse Executive Competencies Assessment Tool The AONE Nurse Executive Competencies (originally published in the February 2005 issue of Nurse Leader) describe skills common to nurses in executive practice
AONE Nurse Executive Competencies Assessment Tool The AONE Nurse Executive Competencies (originally published in the February 2005 issue of Nurse Leader) describe skills common to nurses in executive practice
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
Lessons for Transfusion Laboratory Staff. from the 2007 SHOT Report SHOT SERIOUS HAZARDS OF TRANSFUSION
 Lessons for Transfusion Laboratory Staff from the 2007 SHOT Report SERIOUS HAZARDS OF TRANSFUSION SHOT The Serious Hazards of Transfusion Scheme (SHOT) is a UK-wide confidential enquiry that collects data
Lessons for Transfusion Laboratory Staff from the 2007 SHOT Report SERIOUS HAZARDS OF TRANSFUSION SHOT The Serious Hazards of Transfusion Scheme (SHOT) is a UK-wide confidential enquiry that collects data
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment. MEDCOM PS Center
 ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
Treatment Improvement Initiative: Improved Planning for Youths being Discharged from Inpatient Care CT BHP 2007
 Treatment Improvement Initiative: Improved Planning for Youths being Discharged from Inpatient Care CT BHP 2007 Introduction During 2007, CT BHP partnered with family members and providers to address the
Treatment Improvement Initiative: Improved Planning for Youths being Discharged from Inpatient Care CT BHP 2007 Introduction During 2007, CT BHP partnered with family members and providers to address the
Workplace Bullying/Critical Adverse Events
 Workplace Bullying/Critical Adverse Events October 25, 2014 Lynn Reede, CRNA, DNP, MBA AANA Senior Director, Professional Practice Explore Discuss the impact and how to mitigate vertical and lateral violence
Workplace Bullying/Critical Adverse Events October 25, 2014 Lynn Reede, CRNA, DNP, MBA AANA Senior Director, Professional Practice Explore Discuss the impact and how to mitigate vertical and lateral violence
Sunrise Regional Health Authority
 Sunrise Regional Health Authority Main points... 128 Background... 129 Audit objective, criteria, and conclusion... 130 Key findings and recommendations... 131 Set expectations that influence labour costs...
Sunrise Regional Health Authority Main points... 128 Background... 129 Audit objective, criteria, and conclusion... 130 Key findings and recommendations... 131 Set expectations that influence labour costs...
Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals
 Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals John M. Kessler, B.S. Pharm., Pharm. D. Steve C. Dedrick, MS Pharm. NCCMedS Project Directors
Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals John M. Kessler, B.S. Pharm., Pharm. D. Steve C. Dedrick, MS Pharm. NCCMedS Project Directors
Leroy Edozien. Consultants - Obstetrics & Gynaecology St Mary s Hospital, Manchester, UK
 Leroy Edozien Consultants - Obstetrics & Gynaecology St Mary s Hospital, Manchester, UK Introduction Clinicians fundamental principle: first do no harm 1 in every 10 patients suffers a medical accident
Leroy Edozien Consultants - Obstetrics & Gynaecology St Mary s Hospital, Manchester, UK Introduction Clinicians fundamental principle: first do no harm 1 in every 10 patients suffers a medical accident
snapshot SATISFACTION Trust Your Staff But Check Validation The Key to Hardwiring Change is the problem the tactic? - or is it the execution?
 SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
BUSINESS INCUBATION TRAINING PROGRAM
 + INNOVATION & ENTREPRENEURSHIP BUSINESS INCUBATION TRAINING PROGRAM Training Program Overview THE WORLD BANK www.infodev.org INTRODUCTION TO THE TRAINING PROGRAM infodev (www.infodev.org) is a research,
+ INNOVATION & ENTREPRENEURSHIP BUSINESS INCUBATION TRAINING PROGRAM Training Program Overview THE WORLD BANK www.infodev.org INTRODUCTION TO THE TRAINING PROGRAM infodev (www.infodev.org) is a research,
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
Standards for Laboratory Accreditation
 Standards for Laboratory Accreditation 2017 Edition cap.org 2017 College of American Pathologists. All rights reserved. [ T y p e t h e c o m p a n y a d d r e s s ] CAP Laboratory Accreditation Program
Standards for Laboratory Accreditation 2017 Edition cap.org 2017 College of American Pathologists. All rights reserved. [ T y p e t h e c o m p a n y a d d r e s s ] CAP Laboratory Accreditation Program
GAO DOD HEALTH CARE. Actions Needed to Help Ensure Full Compliance and Complete Documentation for Physician Credentialing and Privileging
 GAO United States Government Accountability Office Report to Congressional Requesters December 2011 DOD HEALTH CARE Actions Needed to Help Ensure Full Compliance and Complete Documentation for Physician
GAO United States Government Accountability Office Report to Congressional Requesters December 2011 DOD HEALTH CARE Actions Needed to Help Ensure Full Compliance and Complete Documentation for Physician
Communication Among Caregivers
 Communication Among Caregivers October 2015 John E. Sanchez - MS, CPHRM, Pendulum, LLC Amid the incredible advances, discoveries, and technological achievements in healthcare, one element has remained
Communication Among Caregivers October 2015 John E. Sanchez - MS, CPHRM, Pendulum, LLC Amid the incredible advances, discoveries, and technological achievements in healthcare, one element has remained
End-to-end infusion safety. Safely manage infusions from order to administration
 End-to-end infusion safety Safely manage infusions from order to administration New demands and concerns 56% 7% of medication errors are IV-related. 1 of high-risk IVs are compounded in error. 2 $3.5B
End-to-end infusion safety Safely manage infusions from order to administration New demands and concerns 56% 7% of medication errors are IV-related. 1 of high-risk IVs are compounded in error. 2 $3.5B
Checklist: What Can My Organization Do?
 Checklist: What Can My Organization Do? 2 Introduction About The Framework This is an evidence and consensus-based framework for successful clinical outcomes in long term and post-acute care. The framework
Checklist: What Can My Organization Do? 2 Introduction About The Framework This is an evidence and consensus-based framework for successful clinical outcomes in long term and post-acute care. The framework
Safe medication practice what can we learn from root cause analysis and related methods?
 Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Meeting of Bristol Clinical Commissioning Group Governing Body. Title: Bristol CCG Management of Serious Incidents Agenda Item: 17
 Meeting of Bristol Clinical Commissioning Group Governing Body To be held on Tuesday 22 December 2015 commencing at 13:30 at the Greenway Centre, Doncaster Road, Bristol, BS10 5PY Title: Bristol CCG Management
Meeting of Bristol Clinical Commissioning Group Governing Body To be held on Tuesday 22 December 2015 commencing at 13:30 at the Greenway Centre, Doncaster Road, Bristol, BS10 5PY Title: Bristol CCG Management
Accreditation Report
 ........................................................................................................................................................ Mackenzie Health Richmond Hill, ON On-site survey
........................................................................................................................................................ Mackenzie Health Richmond Hill, ON On-site survey
Pharmacovigilance Office of Product Review
 Pharmacovigilance Office of Product Review Dr Jane Cook Office Head Office of Product Review, Monitoring & Compliance Group, TGA 7/10/2011 Overview of talk Overview Post TGA 21 and OPR New Guidelines Key
Pharmacovigilance Office of Product Review Dr Jane Cook Office Head Office of Product Review, Monitoring & Compliance Group, TGA 7/10/2011 Overview of talk Overview Post TGA 21 and OPR New Guidelines Key
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
EDUCATIONAL COMMENTARY KEY COMPONENTS OF AN INDIVIDUALIZED QUALITY CONTROL PLAN
 Commentary provided by: E Susan Cease MT(ASCP) Laboratory Manager Three Rivers Medical Center Grants Pass, OR EDUCATIONAL COMMENTARY KEY COMPONENTS OF AN INDIVIDUALIZED QUALITY CONTROL PLAN Educational
Commentary provided by: E Susan Cease MT(ASCP) Laboratory Manager Three Rivers Medical Center Grants Pass, OR EDUCATIONAL COMMENTARY KEY COMPONENTS OF AN INDIVIDUALIZED QUALITY CONTROL PLAN Educational