Monday September 26 th, 2016
|
|
|
- Vincent Wilkins
- 5 years ago
- Views:
Transcription
1 Monday September 26 th, 2016
2 trauma NOUN Injury to human tissues and organs resulting from the transfer of energy from the environment


3 Optimizing Tar Heel Trauma Care: The Golden Hour Daryhl Johnson MD MPH FACS Elizabeth Schroeder BSN RN CEN TCRN Alberto Bonifacio MHA BSN RN
4 Trauma is the leading cause of death for individuals up to the age of fortyfour, costing the US an estimated $671 billion in healthcare costs and lost productivity. 1,2 1. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web based Injury Statistics Query and Reporting System (WISQARS) [online]. Accessed February 17, Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) 2015 [cited /26/15].


5 Sentinel Event Data Root Causes by Event Type

6

7
8 Aim: improve the consistency, efficiency and reliability of trauma resuscitations
9 KEY Physician Adult Trauma Positions ED Attending Airway MD Supervisory Staff Nurse Support Ancillary Staff Nursing Assistant Bedside Physician Respiratory Therapist Secondary RN (T2) Procedure Physician Pharmacy X-Ray1 X-Ray 2 Trauma Attending Trauma Captain Primary RN (T1) Hot Line HUC UNC PD Chaplain Air Care/ EMS AirCare/ EMS Charge RN
10



11 Role Specific Full Alert Trauma Drills



12 It was so cool to be included in the Trauma group and to truly see the patient s care from accident to discharge. I learned a lot about what each department s role is during our patient s recovery journey here at UNC. I believe we are a great team.



13




14 Teamwork, Communication and Leadership Each individual behaviour will improve teamwork and performance Perceived rudeness is the KILLER of Teamwork





15 Post-sim Debriefing



16


17 What Didn t Work? Adhesive role tags Red bouffant worn by trauma captain Electronic feedback system Role reversals Collaboration w/ pediatrics
18 Accomplishments New trauma resuscitation process Capabilities for immediate feedback Culture change with increased engagement and support from physician and administrative leadership Continuum of Care Conference Documentation, accountability, safety Defined leadership and staff roles with use of closed-loop communication Decreases in under-triage, patient complications, and risk adjusted mortality related to shock Consistent trauma paging notification Standardization of set-up for trauma bay Revitalization of ED Trauma Committee Decreased times to: manual BP, HR, O2 sats, X-ray, CT, and OR Implementation of monthly multidisciplinary in-situ trauma simulations Strengthened interdisciplinary relationships Expansion of the Trauma Survivor s Network Use of cognitive aids, advanced technology Launch of Integrated Emotional Support Program (IESP)
19 Comprehensive Improvement in Trauma Resuscitation Pre Go-Live Post Go-Live 96% 67% 77% 75% 80% 87% 67% 65% 60% 86% 55% 71% 45% 27% 34% 27% 9% 8% Trauma Bay Preparation Pre-arrival Huddle Sequential Primary Strong Teamwork Defined Leadership Closed-Loop Communication Met VS Time Requirements X-ray w/in 5 mins CT w/in 20 mins
20 Time (minutes) Decreased Time to Log-Roll INTERVENTION: Lecture and Sim with Surgery Residents Pre Go- Live 7/1 8/2 9/6 11/1 12/21 1/16 2/7 3/6
21 Time (minutes) 16 Decreased Time to Chest X-ray INTERVENTION: Implementation of Radiology Stretchers Pre Go- Live 7/23 8/2 9/6 10/1 11/1 12/8 1/16 2/7 3/6
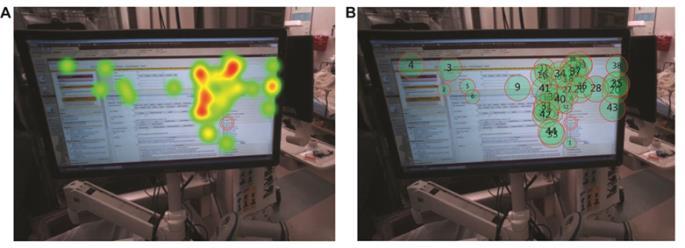
22 Sustainment FY 18 Improve the consistency, reliability and efficiency of trauma resuscitation through the implementatio n of a standardized process in the Emergency Department Consistent Resuscitation following UNC Consistent Education and Training Direct Observation and Performance Feedback Continuum of Care Conference Trauma Program Manager Trauma Medical Director ED Nurse Educator Residency Coordinators Trauma Adult Coordinator Eye Tracking Research Trauma Nurse Educator


23


24 Thank you Project Team Liz Dreesen MD FACS Daryhl Johnson MD MPH Alberto Bonifacio RN BSN MHA Elizabeth Schroeder RN BSN CEN Kelly Revels MSN CEN Nikki Waller MD Christian Lawson RN BSN Gene Hobbs CHES Katelyn Hausfeld RN BSN Tar Heel Trauma Team Disaster Preparedness Dalton Sawyer Emergency Services Jeff Phillips Michelle Pladsen Kayla Wilkerson Carolina Air Care Emergency Trauma Committee Respiratory Therapy Pharmacy Radiology Sheila Leviner Lauren Burton Radiology Team and to so many other incredible team members

25
26 SUPPLEMENT SLIDES
27 Optimizing Tar Heel Trauma Care METHODS

28 The UNC Institute for Healthcare Quality Improvement (IHQI) Seed Grant Program promotes the development of experience and expertise in quality improvement at UNC Hospitals, Faculty Physician practices and Physician Network practices.
29
30 Optimizing Tar Heel Trauma Care TAR HEEL TRAUMA





31 Level 1 Adult and Pediatric Trauma Center Manage the public health problem of injury (prevention) Reduce the degree of injury Optimize the outcome from injury Reduce mortality and morbidity Optimal care for the trauma patient across continuum of trauma care.




32 Dual Trauma Designation
33 Tar Heel Trauma Mission: Maintain UNC s Level I Adult and Pediatric Trauma Verification and ultimately work to ensure trauma patients receive optimal care. Vision: Move the needle of trauma-related morbidity and mortality in the Region in ten years.
34

35 Vision Timeline Year 1-2 Brand Baseline Fundamentals Survey Year 3-5 Geriatric Trauma Trauma Survivors Local / State Partners RAC Epidemiology Year 5-8 National Partners National Recognition Tipping Point Year 9-10 Post Data Publish Tar Heel Trauma 2035

36
37 Optimizing Tar Heel Trauma Care THE BURNING PLATFORM
 78 86 80 T1 (Primary Trauma Nurse) T2 (Secondary / Bedside Trauma Nurse) NA")
38 Comfort and Confidence in Trauma Roles How comfortable or confident are you when performing your role? (0 = very uncomfortable 100 = very comfortable) T1 (Primary Trauma Nurse) T2 (Secondary / Bedside Trauma Nurse) NA (Nursing Assistant Nurse)
 Agree (100) I feel we")

39 Quality N=38 83 Disagree (0) Agree (100) I feel we provide the highest quality nursing care for trauma patients.
40 Barriers 1. Trauma Process not followed (13) The trauma process is followed inconsistently and variably causing sense of disorganization, degradation of teamwork, inability to anticipate team's actions, disorderly communication of findings, orders shouted simultaneously, inability to adequately chart, and causes general frustration. 2. Ineffective leadership in trauma (10) Generally ineffective leadership and management in traumas. Specifically leader at times unclear or multiple leaders attempting to manage resulting in assessments and orders being given at the same time. Delegation also at times ineffective. 3. Observers Disruptive (6) Observers and others not directly involved in trauma care are often disruptive. 4. EPIC Problematic (5) Electronic charting in EPIC is problematic due to registration, user interface, inconsistency with trauma process and general usability. 1. Redesign T1 assignment (12) 2. Improve adherence to trauma process (7) Improve consistency and adherence to ATLS / TNCC trauma assessment process. 3. Provide more trauma education (6) Provide (and perhaps require) more trauma education and hands-on practice. 4. Improve EPIC documentation process (4) EPIC documentation process MUST be improved or consider return to paper documentation. 5. Reduce interference from observers (4) 6. Establish pre-trauma huddle (3) 5. Ineffective communication (5) Generally ineffective communication during traumas (e.g. unclear orders and plan of care)
41 Baseline




42 Morbidity Complications Blunt Multi-system TBI Elderly (complications) Elderly Blunt Multisystem
43
44
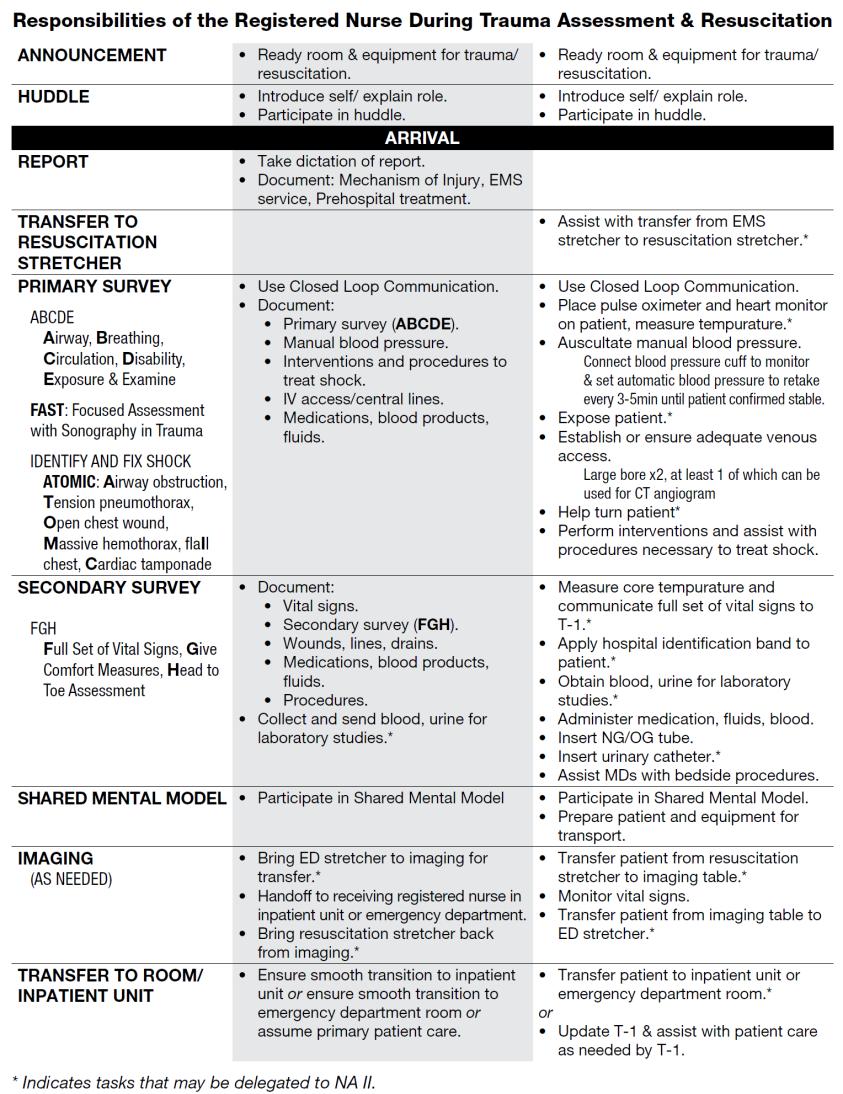
45 Phase: Sign-in / Preparation / Huddle Phase: Patient Arrival / Report Timeout Tar Heel Trauma Resuscitation Process Phase: Primary Survey Phase: Log Roll Phase: Secondary Survey and Other Adjuncts Phase: Disposition / Prepare for Transport Prep Identify and Fix Shock Secondary Survey Dispo. TRAUMA CAPTAIN CHIEF / FELLOW Lead Team Huddle Takes Repor t Directs Interventions Determines Disposition Lead Shared Mental Model AIRWAY PHYSICIAN EM3 Prep: airway equip, suction Patient Comfort A B Secures C-spine May Assist with Assessment of Head; Patient Comfort HUC and Family BEDSIDE PHYSICIAN PGY2 Prep resusc. equip Assists Transfer C D* Back Head to Toe* Prepare for Transport PROCEDURE PHYSICIAN INTERN Prep resusc. equip Assists Transfer Assist with procedures (chest tube, central line, etc.) Log Roll FAST Other Procedure s Prepare for Transport PRIMARY NURSE (T1) Pre-report Manage Prep. Asst. Team Huddle Takes Report Directs RN Care Documents Manages Transport / Handover SECONDARY NURSE (T2) NURSING ASSISTANT Prep: IV, IVF, Bair Hugger, Meds Prep: Monitor, O2, Bed, Foley Patient Comfort Assists Transfer VS (Manual BP) E Expose Pt Monitor PIVx2; IVF; Blood; Meds VS q5; Blankets; Bair Hugger Rectal temp. LSB Rectal Temp Meds; Labs; OGT Send Labs; Foley; UPT Prepare for Transport Prepare for Transport RESPIRATORY THERAPY Prep Vent Assists Transfer Asst. with Airway Breathing Secure s ETT Airway Management / ABG Prepare for Transport RADIOLOGY TECH Pre-set Plates Chest X-ray Pelvis X-ray Process and Deliver Films Minutes * Airway Physician may assist with assessment of head per Bedside Physician / Trauma Captain

 Cardiac Tamponade Early Log Roll (Blunt /")



46 Identify and Fix Shock A-B-C-D-E IDENTIFIES A-T-O-M-I-C Airway Obstruction Tension Pneumothorax Open Pneumothorax Massive Hemothorax I (Flail Chest) Cardiac Tamponade Early Log Roll (Blunt / Penetrating / Spinal) Fix Shock Assessment Findings Airway Patent Breathing Labored Trachea Midline No JVD Lung Sounds Clear, Equal Bilaterally Chest Wall Deformity Heart Sounds Muffled Central Pulses Strong Responder Transient Responder Non- Responder
47 Pre-Trauma Huddle Report: known MIVT on board Team: names, roles, responsibilities Equipment and Environment Alert: CT / ICU / OR as needed Most Important Thing Shared Mental Model: after 2 nd ax
48 Optimizing Tar Heel Trauma Care RESULTS

49
50 Percentage (%) Percentage (%) 1.4 Decrease in Trauma Patient Complications Pre Go-Live Post Go-Live GCS <8 w/out intubation Cardiac arrest w/ CPR Missing warming measures documentation Risk-adjusted mortality r/t shock Improvements in Trauma Documentation & Triage Documentation Deficiencies Undertriage Pre Go-Live Post Go-Live
51 Optimizing Tar Heel Trauma: Metrics Table Metric % Meeting Protocol Before n % Meeting Protocol After n Mean/ Avg Time Before Mean/ Median Median Avg Time Before After After Min Before Min After Max Before Max After Preparation "Yes" "Yes" Bay Stocked smaller n = after checksheet "Go-Live" Bay Cleaned Team Prep "Yes" "Yes" Plan Relayed Team Met cases excluded when "unobservable" or N/A (did not occur) Roles Defined Report Received Primary Obtained w/in 5 minutes of arrival Obtained w/in 5 minutes of arrival Airway Breathing Circulation Disability (GCS) Exposure Vital Signs Obtained w/in 5 minutes of arrival Obtained w/in 5 minutes of arrival Blood Pressure Heart Rate Temperature Pulse Ox Secondary Head & Face Neck Chest Abdomen Perineum Extremities Spine Studies X-ray w/in 5 FAST w/in 10 CT w/in 20 X-ray w/in 5 FAST w/in 10 CT w/in 20 X-Ray FAST CT "Entire 55Team" Communication "Usually and Always" "Yes" Debrief Closed- Loop Followed Leader
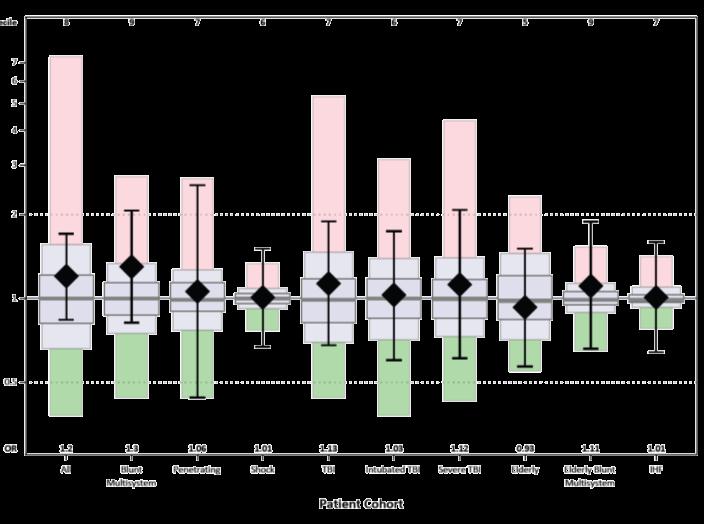
52 Trauma Registry Data : Pre and Post Go-Live Comparison Red Yellow All GCS < 8 and pt. not intubated % GCS < 8 and pt. not intubated Cardiac arrest w/ CPR % Cardiac arrest w/ CPR No documentation - temp w/in 20 mins % No documentation - temp w/in 20 mins No documentation - warming measures % No documentation - warming measures Pt. in shock (systolic </= 90) who didn't receive any blood % Pt. in shock (systolic </= 90) who didn't receive any blood Pt. in shock (systolic </= 90) who didn't receive blood w/in 1 hr % Pt. in shock (systolic </= 90) who didn't receive blood w/in 1 hr Pre Post Under triage cribari # cribari % Pre Jan Feb Mar Apr May Jun Average Post Jul Aug Sep Oct Nov Dec avg. time to OR (min) % doc deficiencies Pre Go-Live Period: 11/3/2015-7/3/2016 Post Go-Live Period: 7/4/2016 4/4/2017 Average 13 14
Title: ED Management of Trauma Patient Protocol
 Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Subject: Trauma Team Roles and Responsibilities for TRAUMA ACTIVATION patients
 UNM Trauma & EM Operational Policies Subject: Trauma Team Roles and Responsibilities for TRAUMA ACTIVATION patients Purpose: To define the roles and responsibilities of personnel responding to trauma activations,
UNM Trauma & EM Operational Policies Subject: Trauma Team Roles and Responsibilities for TRAUMA ACTIVATION patients Purpose: To define the roles and responsibilities of personnel responding to trauma activations,
ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221. I. Title Trauma team Activation Protocol/Roles & Responsibilities of the Trauma Team
 Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 221 Subject: Trauma Team Activation Protocol/Roles & Responsibilities of the Trauma Team Trauma Coordinator UTMB respects the diverse culture
Vanderbilt University Medical Center. Division of Trauma and Surgical Critical Care. Clinical Management Guideline: Standard Trauma Resuscitation
 Introduction Vanderbilt University Medical Center Division of Trauma and Surgical Critical Care Clinical Management Guideline: Standard Trauma Resuscitation Good communication and leadership are the keys
Introduction Vanderbilt University Medical Center Division of Trauma and Surgical Critical Care Clinical Management Guideline: Standard Trauma Resuscitation Good communication and leadership are the keys
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
of the respiratory checklist from July1, April 30, Measures were evaluated monthly. Primary measures:
 Surfactant Administration and Respiratory Care During the Golden Hour Adia Stokes MD, Bushra Saleem, MD, Melissa Oh, MD, Natalie Davis, MD and Sara Mola, MD University of Maryland Medical Center Primary
Surfactant Administration and Respiratory Care During the Golden Hour Adia Stokes MD, Bushra Saleem, MD, Melissa Oh, MD, Natalie Davis, MD and Sara Mola, MD University of Maryland Medical Center Primary
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Level 3 Trauma Hospital Criteria
 Level 3 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Level 3 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
1. Receives report from EMS and/or outlying facility. 5. Adheres to safety and universal precaution guidelines.
 Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
CAH Quality Improvement and Care Transitions Collaborative
 CAH Quality Improvement and Care Transitions Collaborative Lean Concepts and TeamSTEPPS Tools Working Together to Improve Quality Outcomes July 14, 2016 How to Participate in the Session If you have called
CAH Quality Improvement and Care Transitions Collaborative Lean Concepts and TeamSTEPPS Tools Working Together to Improve Quality Outcomes July 14, 2016 How to Participate in the Session If you have called
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
TRAUMA CENTER REQUIREMENTS
 California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
Improving Efficiency During Trauma Resuscitation in the ED
 Improving Efficiency During Trauma Resuscitation in the ED Michelle Maxson, RN, MSN Trauma Program Manager Hurley Medical Center Michael McCann, DO, FACOS, FACS Chief of Trauma and Surgical Critical Care
Improving Efficiency During Trauma Resuscitation in the ED Michelle Maxson, RN, MSN Trauma Program Manager Hurley Medical Center Michael McCann, DO, FACOS, FACS Chief of Trauma and Surgical Critical Care
Level 4 Trauma Hospital Criteria
 Level 4 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Level 4 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems NPSS Asheville, NC
 Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Busy Lots of variety Chance to do Procedures Mix of didactics and practical experience Amount of practical experience is up to you Trauma and General
 Busy Lots of variety Chance to do Procedures Mix of didactics and practical experience Amount of practical experience is up to you Trauma and General Surgery Trauma bay, ICU, OR, floor, clinic In your
Busy Lots of variety Chance to do Procedures Mix of didactics and practical experience Amount of practical experience is up to you Trauma and General Surgery Trauma bay, ICU, OR, floor, clinic In your
Trauma Rotation UMASS Memorial University Campus
 Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Interactive Trauma: Beyond the Moment of Impact
 , About the Speaker MSN, RN, CEN, CPEN, TCRN Bill is a dynamic and energetic speaker whose unique style not only provides insight to his audience but also to creates an engaging and fun atmosphere for
, About the Speaker MSN, RN, CEN, CPEN, TCRN Bill is a dynamic and energetic speaker whose unique style not only provides insight to his audience but also to creates an engaging and fun atmosphere for
The Digital ICU: Return On Innovation
 The Digital ICU: Return On Innovation Cheryl Hiddleson, MSN, RN, CCRN-E Director, Emory eicu Center May, 2017 The Digital ICU: Return on Innovation Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu
The Digital ICU: Return On Innovation Cheryl Hiddleson, MSN, RN, CCRN-E Director, Emory eicu Center May, 2017 The Digital ICU: Return on Innovation Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu
Modesto Junior College Course Outline of Record EMS 390
 Modesto Junior College Course Outline of Record EMS 390 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 390 Emergency Medical Technician 1 6 Units Limitations on Enrollment:
Modesto Junior College Course Outline of Record EMS 390 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 390 Emergency Medical Technician 1 6 Units Limitations on Enrollment:
Simulation Design Template. Date: May 7, 2008 File Name: Group 4
 Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
Improving Pain Center Processes utilizing a Lean Team Approach
 Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
North York General Hospital Policy Manual
 ORIGINATOR: Code Blue/Pink Committee APPROVED By: Operations Committee Medical Advisory Committee ORIGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012
ORIGINATOR: Code Blue/Pink Committee APPROVED By: Operations Committee Medical Advisory Committee ORIGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012
CAUTI Reduction A Clinton Memorial Presentation
 CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral)
") Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral) Eileen Sacco MSN, RN, CNRN, ONC
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral) Eileen Sacco MSN, RN, CNRN, ONC
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1
 Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Trauma Logistics: The things to know ED Charge RN
 The University East Bank Campus is verified by the American College of Surgeons as a Level II Trauma Center. We serve the metro and referring areas as a definitive care trauma center for our patients.
The University East Bank Campus is verified by the American College of Surgeons as a Level II Trauma Center. We serve the metro and referring areas as a definitive care trauma center for our patients.
Activation of the Rapid Response Team
 Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Objectives 10/09/2015. Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935
 Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Trauma Assessment: Primary Secondary Tertiary It s as easy as ABC Updated with 2014 TNCC 7 th Edition Data. Pete Benolken Kelly Simon Trauma Services
 Trauma Assessment: Primary Secondary Tertiary It s as easy as ABC Updated with 2014 TNCC 7 th Edition Data Pete Benolken Kelly Simon Trauma Services Education Goal: Learn about the Tertiary Assessment
Trauma Assessment: Primary Secondary Tertiary It s as easy as ABC Updated with 2014 TNCC 7 th Edition Data Pete Benolken Kelly Simon Trauma Services Education Goal: Learn about the Tertiary Assessment
Change Management at Orbost Regional Health
 Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
Developing a Trauma Center
 Developing a Trauma Center Amy Koestner, RN, BSN, MSN Trauma Program Manager Spectrum Health Medical Center Carol Spinweber, MS, RN Trauma Program Manager St. Joseph Mercy Oakland Objectives: Describe
Developing a Trauma Center Amy Koestner, RN, BSN, MSN Trauma Program Manager Spectrum Health Medical Center Carol Spinweber, MS, RN Trauma Program Manager St. Joseph Mercy Oakland Objectives: Describe
Application of Simulation to Improve Clinical Efficiency Systems Integration
 Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Objectives. Emergency Medicine Risk Factors
 The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
Course: Sub Internship Emergency Medicine Course Number: EMED 1902
 Course: Sub Internship Emergency Medicine Course Number: EMED 1902 Department: Course: Faculty Coordinator: Assoc Faculty Hospital: Periods Offered: Length: Max students: First Day Administrative Contact
Course: Sub Internship Emergency Medicine Course Number: EMED 1902 Department: Course: Faculty Coordinator: Assoc Faculty Hospital: Periods Offered: Length: Max students: First Day Administrative Contact
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals
 Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Supervision of Residents/Chain of Command
 Supervision of Residents/Chain of Command Creighton University Department of Surgery Residency Training Program Chain of command for Surgery residents at CUMC PGY1: The intern on call covers the two general
Supervision of Residents/Chain of Command Creighton University Department of Surgery Residency Training Program Chain of command for Surgery residents at CUMC PGY1: The intern on call covers the two general
HOW TO DO POST-HOC RESPONSE REVIEWS
 HOW TO DO POST-HOC RESPONSE REVIEWS Ken Hillman 6 th International Symposium on Rapid Response Systems and Medical Emergency Teams Pittsburgh, USA, 11 th -12 th May 2010 ACUTE HOSPITAL SYSTEM AUDIT OF
HOW TO DO POST-HOC RESPONSE REVIEWS Ken Hillman 6 th International Symposium on Rapid Response Systems and Medical Emergency Teams Pittsburgh, USA, 11 th -12 th May 2010 ACUTE HOSPITAL SYSTEM AUDIT OF
From Implementation to Optimization: Moving Beyond Operations
 From Implementation to Optimization: Moving Beyond Operations Session 260, March 8, 2018 Scott Aikey, Sr. Director, Core Clinical Applications Children s Hospital of Philadelphia 1 Conflict of Interest
From Implementation to Optimization: Moving Beyond Operations Session 260, March 8, 2018 Scott Aikey, Sr. Director, Core Clinical Applications Children s Hospital of Philadelphia 1 Conflict of Interest
Departments to Improve. February Chad Faiella RN, Terri Martin RN. 1 Process Excellence
 Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY
 MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY Joyce Kant, A/Prof Peter Morley, S. Murphy, R. English, L. Umstad Melbourne Private Hospital, University of Melbourne Background /
MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY Joyce Kant, A/Prof Peter Morley, S. Murphy, R. English, L. Umstad Melbourne Private Hospital, University of Melbourne Background /
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
Improving Transition Home through a Standardized Discharge Process. Christopher D. Baker, MD Associate Professor of Pediatrics May 10, 2016
 Improving Transition Home through a Standardized Discharge Process Christopher D. Baker, MD Associate Professor of Pediatrics May 10, 2016 Objectives Identify components of the Children s Hospital Colorado
Improving Transition Home through a Standardized Discharge Process Christopher D. Baker, MD Associate Professor of Pediatrics May 10, 2016 Objectives Identify components of the Children s Hospital Colorado
STEMI ALERT! Craig M. Hudak, MD, FACC,FACP 24 January 2015
 STEMI ALERT! Craig M. Hudak, MD, FACC,FACP 24 January 2015 STEMI Overview ST segment Elevated Myocardial Infarction Patient Outcome Goals: Save myocardium Reduce CHF Reduce arrhythmias Improve quality
STEMI ALERT! Craig M. Hudak, MD, FACC,FACP 24 January 2015 STEMI Overview ST segment Elevated Myocardial Infarction Patient Outcome Goals: Save myocardium Reduce CHF Reduce arrhythmias Improve quality
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Ontario Shores Journey to EMRAM Stage 7. October 21, 2015
 Ontario Shores Journey to EMRAM Stage 7 October 21, 2015 ICE BREAKER Agenda System overview & pervasiveness of use Review Clinical Practice Guideline implementation Discuss Patient Portal implementation
Ontario Shores Journey to EMRAM Stage 7 October 21, 2015 ICE BREAKER Agenda System overview & pervasiveness of use Review Clinical Practice Guideline implementation Discuss Patient Portal implementation
Difficult Airways: All Airways are NOT Created Equal July 23, 2018
 Difficult Airways: All Airways are NOT Created Equal July 23, 2018 ACS Quality and Safety Conference Lisa Failace, MSN, RN, CCRN-K Donna Swartz, MAS, RN, CPHQ, CPPS Hackensack University Medical Center
Difficult Airways: All Airways are NOT Created Equal July 23, 2018 ACS Quality and Safety Conference Lisa Failace, MSN, RN, CCRN-K Donna Swartz, MAS, RN, CPHQ, CPPS Hackensack University Medical Center
North York General Hospital Policy Manual
 ORIGINATOR: Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: May, 2002 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012 Page
ORIGINATOR: Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: May, 2002 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012 Page
ECPR Simulation at Seattle Children s Hospital
 ECPR Simulation at Seattle Children s Hospital Justin Sleasman CCP, MS, FPP Larissa Yalon BSN, RN, CCRN ECPR- Why? AHA Get with the Guidelines Resuscitation Registry: Hospital cardiac arrest in children
ECPR Simulation at Seattle Children s Hospital Justin Sleasman CCP, MS, FPP Larissa Yalon BSN, RN, CCRN ECPR- Why? AHA Get with the Guidelines Resuscitation Registry: Hospital cardiac arrest in children
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
Modesto Junior College Course Outline of Record EMS 350
 Modesto Junior College Course Outline of Record EMS 350 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 350 First Responder with Healthcare Provider CPR 3 Units Formerly
Modesto Junior College Course Outline of Record EMS 350 I. OVERVIEW The following information will appear in the 2011-2012 catalog EMS 350 First Responder with Healthcare Provider CPR 3 Units Formerly
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience. Presented by: Fadwa Jabboury, RN, MSN
 CMC Experience. Presented by: Fadwa Jabboury, RN, MSN") Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.
 Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.") Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
The curriculum is based on achievement of the clinical competencies outlined below:
 ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
FMS EMT. Monday Friday (R) & (L) DATE TOPIC INSTRUCTOR MODULE I Preparatory. Week 1
 & (L) DATE TOPIC INSTRUCTOR MODULE I Preparatory. Week 1") FMS 2017-2018 EMT August 21, 2017 December 16, 2017 Emergency Medical Technician Monday Friday (R) 1030 1120 & (L) 1150 1430 DATE TOPIC INSTRUCTOR MODULE I Preparatory Week 1 08/21/17 R = Related EMT-Basic
FMS 2017-2018 EMT August 21, 2017 December 16, 2017 Emergency Medical Technician Monday Friday (R) 1030 1120 & (L) 1150 1430 DATE TOPIC INSTRUCTOR MODULE I Preparatory Week 1 08/21/17 R = Related EMT-Basic
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Submission Form Deadline: November 9, 2015
 Submission Form Deadline: November 9, 2015 Organization: Sinai Hospital Contact Person: Pat Moloney-Harmon, MS, RN, CCNS, FAAN Title: Clinical Outcomes Specialist, Children s Services Address: 2401 W.
Submission Form Deadline: November 9, 2015 Organization: Sinai Hospital Contact Person: Pat Moloney-Harmon, MS, RN, CCNS, FAAN Title: Clinical Outcomes Specialist, Children s Services Address: 2401 W.
ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY)
") July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
North York General Hospital Policy Manual
 ORIGINTATOR: Chair Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29,
ORIGINTATOR: Chair Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29,
On Becoming a Health Literate Organization: A Journey with Urgency
 On Becoming a Health Literate Organization: A Journey with Urgency HARC VIII October 13, 2016 Laura Noonan, MD Director, Center for Advancing Pediatric Excellence Levine Children s Hospital at Carolinas
On Becoming a Health Literate Organization: A Journey with Urgency HARC VIII October 13, 2016 Laura Noonan, MD Director, Center for Advancing Pediatric Excellence Levine Children s Hospital at Carolinas
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool
 Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria)
") AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
Simulation Design Template
 Simulation Design Template Date: May 7/8, 2008 File Name: Discipline: RN, Charge nurse, medical radiology, pharmacy tech, social work, medicine (whatever is available at the institution) Student Level:
Simulation Design Template Date: May 7/8, 2008 File Name: Discipline: RN, Charge nurse, medical radiology, pharmacy tech, social work, medicine (whatever is available at the institution) Student Level:
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
Brief Summary. Educational Rationale. Learning Objectives: Nurse. Learning Objectives: Doctor
 Simulation Scenario Title Bacterial meningitis Version 10 Target Audience FY doctors & student nurses Run time 10-15 mins Authors Niamh Feely, Andrew Smith, Udesh Naidoo, Paul Wilder, Mark Loughrey Last
Simulation Scenario Title Bacterial meningitis Version 10 Target Audience FY doctors & student nurses Run time 10-15 mins Authors Niamh Feely, Andrew Smith, Udesh Naidoo, Paul Wilder, Mark Loughrey Last
POLICIES AND PROCEDURES
 POLICIES AND PROCEDURES POLICY: 553.25 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 5 I. AUTHORITY Division 2.5, California Health and Safety
POLICIES AND PROCEDURES POLICY: 553.25 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 5 I. AUTHORITY Division 2.5, California Health and Safety
Mitzi Cardenas Sr. VP/Strategy, Business Development and Technology Truman Medical Centers
 Mitzi Cardenas Sr. VP/Strategy, Business Development and Technology Truman Medical Centers HIMSS Stage 7: What it Means Heart of America HIMSS and the Missouri Health Information Management Association
Mitzi Cardenas Sr. VP/Strategy, Business Development and Technology Truman Medical Centers HIMSS Stage 7: What it Means Heart of America HIMSS and the Missouri Health Information Management Association
Corporate Services Employment Report: January Employment by Staff Group. Jan 2018 (Jan 2017 figure: 1,462) Overall 1,
 Overall 1,") Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Driving Obstetrical Excellence Through a Council Structure
 Driving Obstetrical Excellence Through a Council Structure Elizabeth Deckers, MD Director of Labor and Delivery, Hartford Hospital Deborah Feldman, M.D. Division director, Maternal Fetal Medicine, Hartford
Driving Obstetrical Excellence Through a Council Structure Elizabeth Deckers, MD Director of Labor and Delivery, Hartford Hospital Deborah Feldman, M.D. Division director, Maternal Fetal Medicine, Hartford
Process Redesign to Improve Chemotherapy Appointment Booking at the BC Cancer Agency
 Process Redesign to Improve Chemotherapy Appointment Booking at the BC Cancer Agency Vincent Chow BC Cancer Agency vchow@bccancer.bc.ca Ruben Aristizabal Pablo Santibáñ áñez Kevin Huang Martin Puterman
Process Redesign to Improve Chemotherapy Appointment Booking at the BC Cancer Agency Vincent Chow BC Cancer Agency vchow@bccancer.bc.ca Ruben Aristizabal Pablo Santibáñ áñez Kevin Huang Martin Puterman
Comparison: ITLS Provider and Trauma Nursing Core Course (TNCC)
") Overview International Trauma Life Support (ITLS) is a global organization dedicated to preventing death and disability from trauma through education and emergency care. ITLS educates emergency personnel
Overview International Trauma Life Support (ITLS) is a global organization dedicated to preventing death and disability from trauma through education and emergency care. ITLS educates emergency personnel
Clinical Operations in a Service Line Model
 Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year
 A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year Saturday March 25 th, 2017 Lindsay Altimare, MPA Director, LVPG Operations Lehigh Valley Health Network Michael Sheinberg,
A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year Saturday March 25 th, 2017 Lindsay Altimare, MPA Director, LVPG Operations Lehigh Valley Health Network Michael Sheinberg,
Collaboration with Rural EMS and Hospitals for Trauma Care
 Collaboration with Rural EMS and Hospitals for Trauma Care Darwin Ang, MD PhD FACS Trauma Medical Director, Ocala Health Associate Professor, USF College of Medicine Director of Quality and Research USF/HCA
Collaboration with Rural EMS and Hospitals for Trauma Care Darwin Ang, MD PhD FACS Trauma Medical Director, Ocala Health Associate Professor, USF College of Medicine Director of Quality and Research USF/HCA
GAMUT QI Collaborative Consensus Quality Metrics (v. 05/16/2016)
") 1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
Learning Objectives. Carolinas HealthCare System Who We Are
 1 Capturing Accurate Documentation Through Participation in Interdisciplinary Rounds: A Healthcare System Initiative Kay Blue, RN, BSN, CCDS, ACM, Director CDI Holley Pegram, RN, MSN, CCM, Manager CDI
1 Capturing Accurate Documentation Through Participation in Interdisciplinary Rounds: A Healthcare System Initiative Kay Blue, RN, BSN, CCDS, ACM, Director CDI Holley Pegram, RN, MSN, CCM, Manager CDI
Enhancing Psychosocial Care for Patients with Palliative Care Needs in the Acute Medical Wards
 Enhancing Psychosocial Care for Patients with Palliative Care Needs in the Acute Medical Wards Dr Stephanie Chu Associate Consultant Department of Medicine Queen Elizabeth Hospital Hospital Authority Convention
Enhancing Psychosocial Care for Patients with Palliative Care Needs in the Acute Medical Wards Dr Stephanie Chu Associate Consultant Department of Medicine Queen Elizabeth Hospital Hospital Authority Convention
Large-Scale Disaster Simulations: Advancing Pediatric Disaster Preparedness and Safety Through Whole-Hospital, Inter- Professional Learning
 Large-Scale Disaster Simulations: Advancing Pediatric Disaster Preparedness and Safety Through Whole-Hospital, Inter- Professional Learning Elene Khalil, MDCM, FRCPC, FAAP Ilana Bank, MDCM, FRCPC, FAAP
Large-Scale Disaster Simulations: Advancing Pediatric Disaster Preparedness and Safety Through Whole-Hospital, Inter- Professional Learning Elene Khalil, MDCM, FRCPC, FAAP Ilana Bank, MDCM, FRCPC, FAAP
2017 OMFRC Scenario #1 - "What goes up, must come down" SCENE/PRIMARY SURVEY 1 ß Did the team TAKE CHARGE of the situation?
 CYCLE: TEAM #: Score Sheet for Patient #1 - "INFERIOR INJURIES" SCENE/PRIMARY SURVEY 1 Did the team TAKE CHARGE of the situation? 2 Did the team wear protective GLOVES? 3 Did the team ASSESS for HAZARDS?
CYCLE: TEAM #: Score Sheet for Patient #1 - "INFERIOR INJURIES" SCENE/PRIMARY SURVEY 1 Did the team TAKE CHARGE of the situation? 2 Did the team wear protective GLOVES? 3 Did the team ASSESS for HAZARDS?
ASCO s Quality Training Program
 ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
Sudden Impact Mass Casualty Incidents Response and Planning. Charles M. Little, DO FACEP University of Colorado Denver
 Sudden Impact Mass Casualty Incidents Response and Planning Charles M. Little, DO FACEP University of Colorado Denver Can Multiple Untriaged/Untreated Battlefield Casualties Happen Here? Fort Hood, TX
Sudden Impact Mass Casualty Incidents Response and Planning Charles M. Little, DO FACEP University of Colorado Denver Can Multiple Untriaged/Untreated Battlefield Casualties Happen Here? Fort Hood, TX
It is a great pleasure and privilege for me to attend the 29 th annual meeting of The Japanese Association for The Surgery of Trauma, in Hokkaido.
 It is a great pleasure and privilege for me to attend the 29 th annual meeting of The Japanese Association for The Surgery of Trauma, in Hokkaido. This is truly the most beautiful place to be in, especially
It is a great pleasure and privilege for me to attend the 29 th annual meeting of The Japanese Association for The Surgery of Trauma, in Hokkaido. This is truly the most beautiful place to be in, especially
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring
 Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Initiating a Rapid Response Team
 Initiating a Rapid Response Team Trials and Tribulations! Washington County Hospital Facility Location Size Hagerstown, MD 320 bed Programs/Services History Emergency Services, Critical Care, Med/Surg,
Initiating a Rapid Response Team Trials and Tribulations! Washington County Hospital Facility Location Size Hagerstown, MD 320 bed Programs/Services History Emergency Services, Critical Care, Med/Surg,
ROTATION DESCRIPTION FORM PGY1
 ROTATION DESCRIPTION FORM PGY1 Rotation Title Medicine Intensive Care Unit (MICU) Level of Learner PY4 PGY1 PGY2 Preceptor(s) Stacy Campbell-Bright, Brian Murray Preceptor Contact Stacy.Campbell-Bright@unchealth.unc.edu;
ROTATION DESCRIPTION FORM PGY1 Rotation Title Medicine Intensive Care Unit (MICU) Level of Learner PY4 PGY1 PGY2 Preceptor(s) Stacy Campbell-Bright, Brian Murray Preceptor Contact Stacy.Campbell-Bright@unchealth.unc.edu;
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Celebrating our Successes 2014
 Celebrating our Successes 214 Nurse Involvement in Decision Making Groups 5 CODE SEPSIS: Time from Antibiotic Order to Administration 45 4 Time in Minutes from order to administration 35 3 25 2 15 1 5
Celebrating our Successes 214 Nurse Involvement in Decision Making Groups 5 CODE SEPSIS: Time from Antibiotic Order to Administration 45 4 Time in Minutes from order to administration 35 3 25 2 15 1 5
The Impact of a Daily Goals Tool in the ICU: More than a Checklist
 S Y S T E M The Impact of a Daily Goals Tool in the ICU: More than a Checklist May 24, 2016 Our Vision To be the Nation's leading public academic health care system. Leading. Teaching. Caring. Acknowledgements
S Y S T E M The Impact of a Daily Goals Tool in the ICU: More than a Checklist May 24, 2016 Our Vision To be the Nation's leading public academic health care system. Leading. Teaching. Caring. Acknowledgements
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
Iowa Methodist Medical Center Department of Surgery Education Resident Rotation Description
 Iowa Methodist Medical Center Department of Surgery Education Resident Rotation Description Rotation: Trauma Surgery Service, PGY-1 General Information: 1. Postgraduate year: PGY-1 2. Rotation Length:
Iowa Methodist Medical Center Department of Surgery Education Resident Rotation Description Rotation: Trauma Surgery Service, PGY-1 General Information: 1. Postgraduate year: PGY-1 2. Rotation Length: