Initiating a Rapid Response Team
|
|
|
- Jocelin Dawson
- 5 years ago
- Views:
Transcription
1 Initiating a Rapid Response Team Trials and Tribulations! Washington County Hospital Facility Location Size Hagerstown, MD 320 bed Programs/Services History Emergency Services, Critical Care, Med/Surg, PCU, Cardiac Cath Lab, Radiology, Outpatient Lab services, Family Birthing Center, Cardiac Rehab Program, CHF Program, Interventional Radiology Over 100 yrs old 1

2 Implementation Team Members Multidisciplinary Team Nursing Quality Management Respiratory Communications Physicians Pharmacy October 2005 Timeline Initial meetings Development of Action Plan Determination of Measures of Success Development of Team Characteristics Determination of Support Measures 2
3 Action Plan Preplanning Development of processes FMEA Determination of process failures prior to implementation PDSA Maintenance of rapid cycle change Action Plan ITEM ACTION DUE DATE Presentation Education 1.Introduction of Plan to Resource staff 2, Introduction of Plan to Critical Care staff 3.Introduction of Plan to PCU staff 4. Presentation of action plan to monthly peer to peer MD meeting 1.Develop scenarios for Resource staff 2. Develop scenarios for PCU staff 3.Train Resource staff 4.Train PCU staff 5. Training of Resp. staff 11/14/05 By Dec staff mtg 11/28 11/17 11/14/05 12/5/05 Week of 11/28 12/5-12/23 By 12/23 Data collection Meet and Greet with RNs and MDs Pre-Pilot Development of data collection tool Data collection at time of RRT calls Meeting of staff involved with RRT Gear Up Week! 11/28 ongoing Set up 12/20 Week of 1/2/06 Pilot Unit-PCU from 1/9/05 to 3/31/05 1/9/06 3


4 Key Elements Communication Staff Ancillary Departments Physicians Hospital Management Senior Management GET THE WORD OUT THERE!!!!! Education Key Elements Critical Care Staff Respiratory Therapists Hospitalists Pilot Unit Senior Management Physicians 4

5 Education Staff Pocket Cards Criteria for calling RRT -Acute change in heart rate < 40 or > 130 bpm. -Acute change in systolic BP < 90 or > 180mmHg. -Acute change in RR < 8 or > 28 per minutes. -Acute change in SaO2 < 90% despite oxygen. -Acute change in consciousness or cognition, or seizures. -Acute change in urine output < 50ml in 4 hours. -Staff is worried about the patient -> They just don t look right. Expectations of Those Utilizing RRT -Be prepared to give concise information, with chart in hand. Including latest lab results. -Assuring emergency equipment and supplies are available. -Remaining present to assist RRT. -Contact primary physician. -Follow-up assessments, documentation, report to receiving nurse if patient is transferred. - Never leave your wingman To call RRT: Dial > Give your unit and the phone extension to the patient s room. Education Role of the Respiratory Care Department on the RRT Assess respiratory status and consult with other team members Draw and analyze arterial blood sample as needed Select device and apply/adjust oxygen therapy as needed Administer one dose of albuterol vial medicated aerosol as indicated Maintain patent airway as indicated (including ET intubation) Provide assisted ventilation as needed Respiratory Therapist Attributes: Demonstrated competency in critical respiratory care Able to communicate effectively with other team members 5
6 Education SBAR Purpose What is it? Consistent form of communication that enables the caregiver to provide clear concise information about the patient. Expectation When to use it? During RRT When giving report to next caregiver When calling Physician Key Elements Data Collection Recognition of core measures Development of additional measures Development of Event Record Development of Surveys Data Assessment Evaluation of RRT calls Evaluation of codes 6




7 Data Collection Event Documentation Tool Implementation Pilot Unit-PCU Pilot Education-November-December 05 Pilot-January-February 06 Data collection-outcomes to be measured and reported to staff on continuous basis Revisions utilizing Rapid cycle change 7
8 In Process Delmarva collaborative March 2006 December 2006 Learning sessions Listserves Networking Implementation of frequent team meetings In Process Changes Implemented: Addressed issue of designated RT. Clarification of data collection. Addition of Med/Surg nurse to collaborative team. Increased education to MedSurg Staff. Feedback from critical care, respiratory and floor staff. Initiation of SBAR. 8
9 Feedback Surveys Given to RRT RN and Staff RN at time of event Respiratory Survey done randomly Recognition Saving Lives Report - # calls/unit Thank You for Helping Us to save lives this month by calling RRT Implementation of Essential Piece Recruitment Managers informing new candidates of program Survey results From Nurses: I felt that it was very helpful to have the RRT. I felt like the patient & family were satisfied also to see how quickly everyone responded. They were great! Thanks! Thanks! Thanks! I was very apprehensive about this patient, and they really took the pressure away. This is a helpful service. I had placed call to PMD prior to calling RRT. PMD on call did not call back until approx hour later, by then patient already settled in CC3 with appropriate care being delivered. 9
10 Respiratory Survey Respiratory Care RRT Survey Results Percentage of Respiratory Therapist who understand the RRT Concept 80%. Percentage of Respiratory Therapist who felt this was an important patient safety initiative 92%. Average response time to an RRT call, by the Respiratory Therapist 95% responded within 1-5 minutes, 5% responded between 6-10 minutes. Suggestions for Improvement Conduct inservices for staff, giving criteria for when to call the Rapid Response Team. Negative Experiences How are RT s to handle multiple STAT requests. How are RT s to handle multiple RRT calls, with insufficient staff to cover. Too many staff in the patient room during the RRT calls. Physician gave no direction, and left the patients room SUMMARY OF RRT CALLS NUMBER OF CALLS 159 AVERAGE RESPONSE TIME/MINUTES 3.44 AVERAGE LENGTH OF CALL/MINUTES 35.4 PRIMARY MD NOTIFIED 89% DISPOSITION OF PATIENT TRANSFER TO HIGHER LEVEL OF CARE 69% STAYED IN ROOM 31% 10


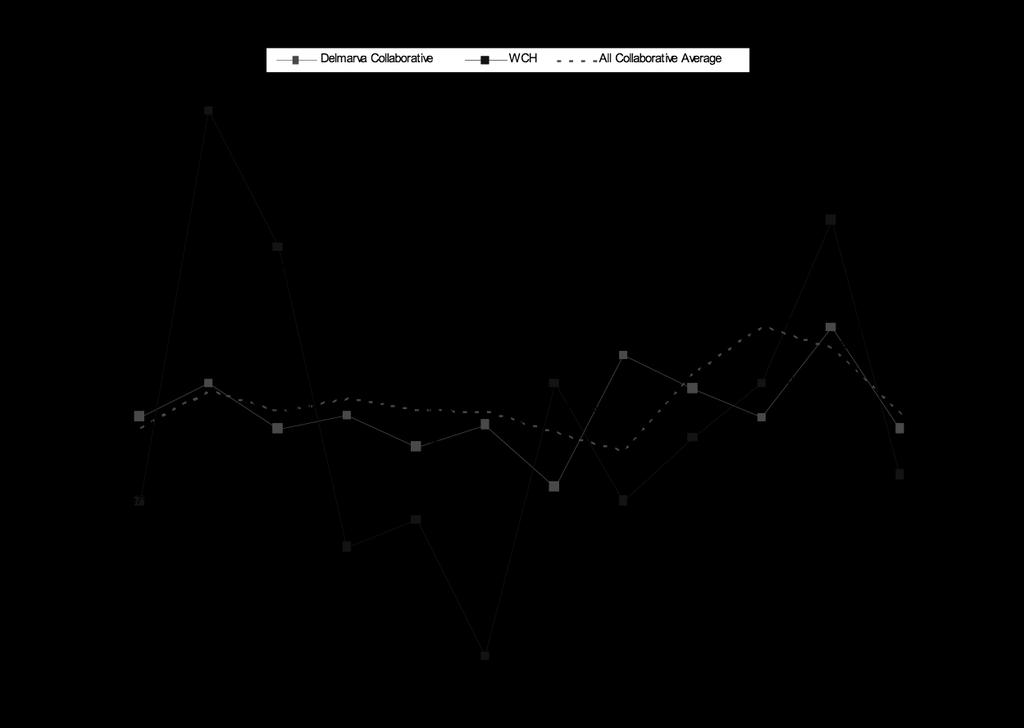
11 COMPARISON OF CODES OUTSIDE OF CRITICAL CARE PCU % decrease in codes MED/SURG % decrease in codes TOTAL % TOTAL DECREASE IN CODES OUTSIDE OF CRITICAL CARE Codes Outside of Critical Care 11
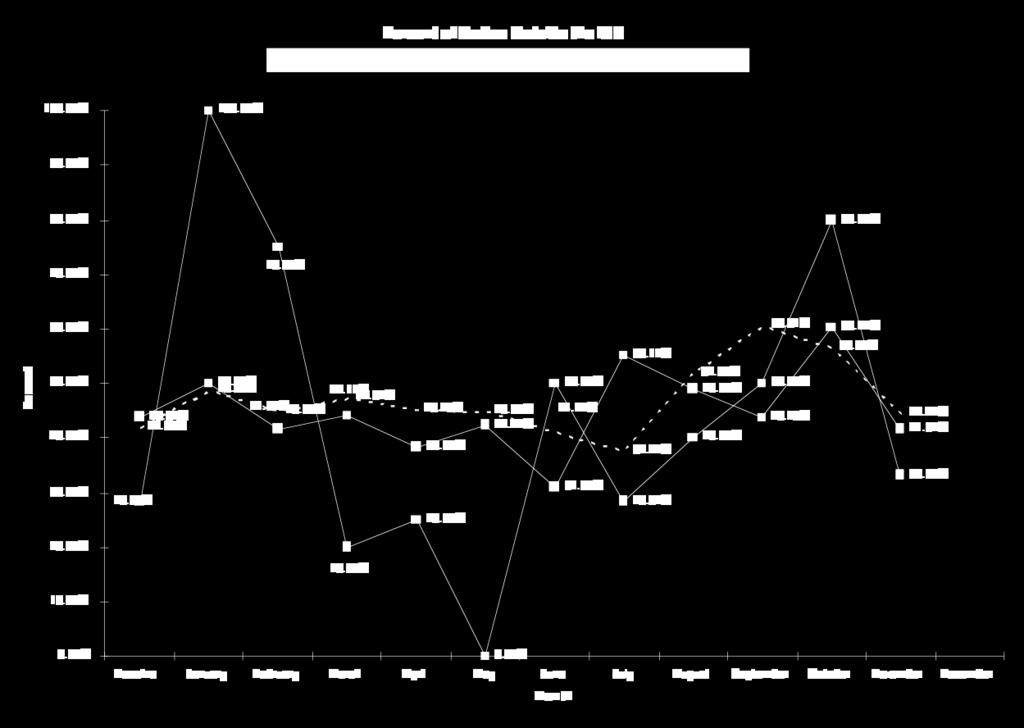
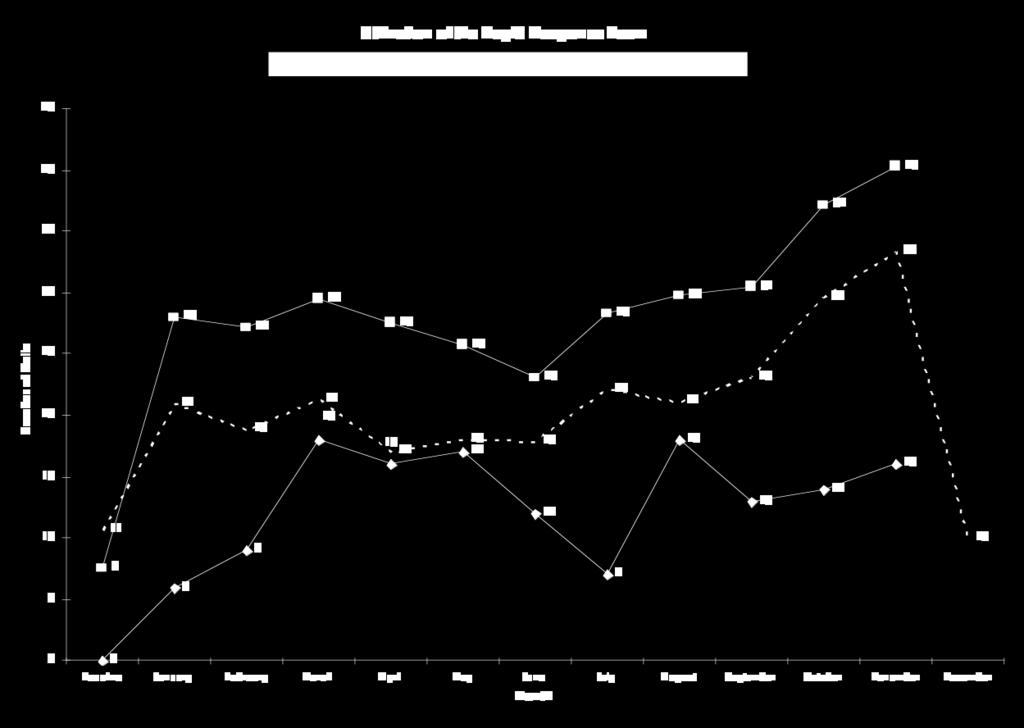
12 Collaborative Calls Outside Critical Care Collaborative Utilization of Team 12

13 Challenges Current staffing. Consistent application of SBAR tool for reporting. Consistent utilization of appropriate beds/units Continue communication 13

14 Next Steps THANK YOU 14
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Los Angeles Medical Center Policies and Procedures
 Section: OPERATIONS Title: GUIDELINES FOR RAPID RESPONSE TO CHANGES IN A PATIENT S CONDITION Approved by: POLICY & PROCEDURE COMMITTEE 10/09 MEDICAL EXECUTIVE COMMITTEE 10/09 REFERENCES: Institute for
Section: OPERATIONS Title: GUIDELINES FOR RAPID RESPONSE TO CHANGES IN A PATIENT S CONDITION Approved by: POLICY & PROCEDURE COMMITTEE 10/09 MEDICAL EXECUTIVE COMMITTEE 10/09 REFERENCES: Institute for
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
ADMINISTRATIVE CLINICAL Page 1 of 6. Origination Date: 6/2009, 10/2009
 ADMINISTRATIVE CLINICAL Page 1 of 6 INTRA-FACILITY TRANSPORT OF CRITICALLY ILL PATIENTS TO AND FROM SPECIAL CARE AREAS Origination Date: 6/2009, 10/2009 Revision/Reviewed Date: 9/2010 8/2011, 1/2013; 4/2014
ADMINISTRATIVE CLINICAL Page 1 of 6 INTRA-FACILITY TRANSPORT OF CRITICALLY ILL PATIENTS TO AND FROM SPECIAL CARE AREAS Origination Date: 6/2009, 10/2009 Revision/Reviewed Date: 9/2010 8/2011, 1/2013; 4/2014
Rapid Response Team Building
 Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Activation of the Rapid Response Team
 Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Document #: WR
 Rapid Response Team (RRT) Policy Northwest Network Effective Date: 2/8/2018 Version #: 2 Document #: WR.387.149 Patient Care Next Review: 2/8/2021 Page #: 1 of 7 SCOPE: All PeaceHealth St. Joseph Center
Rapid Response Team (RRT) Policy Northwest Network Effective Date: 2/8/2018 Version #: 2 Document #: WR.387.149 Patient Care Next Review: 2/8/2021 Page #: 1 of 7 SCOPE: All PeaceHealth St. Joseph Center
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Running head: FAILURE TO RESCUE 1
 Running head: FAILURE TO RESCUE 1 Failure to Rescue Susan Headley Ferris State University FAILURE TO RESCUE 2 Introduction Quality improvement in healthcare is a continuous process that evaluates care
Running head: FAILURE TO RESCUE 1 Failure to Rescue Susan Headley Ferris State University FAILURE TO RESCUE 2 Introduction Quality improvement in healthcare is a continuous process that evaluates care
North York General Hospital Policy Manual
 ORIGINATOR: Code Blue/Pink Committee APPROVED By: Operations Committee Medical Advisory Committee ORIGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012
ORIGINATOR: Code Blue/Pink Committee APPROVED By: Operations Committee Medical Advisory Committee ORIGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012
NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting
 NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting 1. Introduction To standardise the type and frequency of observations to be taken on adult
NHS LOTHIAN Standard Operating Procedure: EHSCP Physiological Observations of Patients in the Community Setting 1. Introduction To standardise the type and frequency of observations to be taken on adult
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
RAPID RESPONSE TEAM & E-ICU ROBOT. Kelly J. Green, R.N., J.D. Krieg DeVault LLP & Beth W. Munz,, R.N., M.S., J.D. Parkview Health
 RAPID RESPONSE TEAM & E-ICU ROBOT Kelly J. Green, R.N., J.D. Krieg DeVault LLP & Beth W. Munz,, R.N., M.S., J.D. Parkview Health Kelly J. Green, R.N., J.D. Krieg DeVault LLP 12800 N. Meridian Suite 300
RAPID RESPONSE TEAM & E-ICU ROBOT Kelly J. Green, R.N., J.D. Krieg DeVault LLP & Beth W. Munz,, R.N., M.S., J.D. Parkview Health Kelly J. Green, R.N., J.D. Krieg DeVault LLP 12800 N. Meridian Suite 300
North York General Hospital Policy Manual
 ORIGINATOR: Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: May, 2002 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012 Page
ORIGINATOR: Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: May, 2002 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29, 2012 Page
WebEx Quick Reference
 Kathy Duncan, RN, Director Christine McMullan, MPA, Faculty April 2011 These presenters have nothing to disclose WebEx Quick Reference Welcome to today s session! Please use Chat to All Participants for
Kathy Duncan, RN, Director Christine McMullan, MPA, Faculty April 2011 These presenters have nothing to disclose WebEx Quick Reference Welcome to today s session! Please use Chat to All Participants for
Minor/technical revision of existing policy X Major revision of existing policy Reaffirmation of existing policy
 Name of Policy: Policy Number: 3364-100-45-06 Department: Approving Officer: Responsible Agent: Scope: Heart and Vascular Center, Hospital Clinics, the George Isaac Outpatient Surgical Center, the First
Name of Policy: Policy Number: 3364-100-45-06 Department: Approving Officer: Responsible Agent: Scope: Heart and Vascular Center, Hospital Clinics, the George Isaac Outpatient Surgical Center, the First
North York General Hospital Policy Manual
 ORIGINTATOR: Chair Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29,
ORIGINTATOR: Chair Code Blue/Pink Committee APPROVED BY: Operations Committee Medical Advisory Committee ORGINAL DATE APPROVED: September, 1999 DATE REVIEWED: April, 2012 DATE OF IMPLEMENTATION: June 29,
Developing a Hospital Based Resuscitation Program. Nicole Kupchik MN, RN, CCNS, CCRN, PCCN-CSC, CMC & Chris Laux, MSN, RN, ACNS-BC, CCRN, PCCN
 Developing a Hospital Based Resuscitation Program Nicole Kupchik MN, RN, CCNS, CCRN, PCCN-CSC, CMC & Chris Laux, MSN, RN, ACNS-BC, CCRN, PCCN Objectives: Describe components of a high quality collaborative
Developing a Hospital Based Resuscitation Program Nicole Kupchik MN, RN, CCNS, CCRN, PCCN-CSC, CMC & Chris Laux, MSN, RN, ACNS-BC, CCRN, PCCN Objectives: Describe components of a high quality collaborative
Paediatrics. PEWS & Deteriorating Patients Linda Clerihew
 Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
Quality Improvement Project Control Report Out
 Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
AARC Clinical Practice Guideline
 AARC Clinical Practice Guideline Discharge Planning for the Respiratory Care Patient DPRP 1.0 PROCEDURE: Development and implementation of a comprehensive plan for the safe discharge of the respiratory
AARC Clinical Practice Guideline Discharge Planning for the Respiratory Care Patient DPRP 1.0 PROCEDURE: Development and implementation of a comprehensive plan for the safe discharge of the respiratory
IMPACT OF RN HYPERTENSION PROTOCOL
 1 IMPACT OF RN HYPERTENSION PROTOCOL Joyce Cheung, RN, Marie Kuzmack, RN Orange County Hypertension Team Kaiser Permanente, Orange County Joyce.m.cheung@kp.org and marie-aline.z.kuzmack@kp.org Cell phone:
1 IMPACT OF RN HYPERTENSION PROTOCOL Joyce Cheung, RN, Marie Kuzmack, RN Orange County Hypertension Team Kaiser Permanente, Orange County Joyce.m.cheung@kp.org and marie-aline.z.kuzmack@kp.org Cell phone:
Job Description. Job Title: (Respiratory Specialist)
") Job Title: (Respiratory Specialist) Reports to: Annette Moser Responsibility Level: Staff Direct Supervision: Respiratory Manager Job Location: UI Health Department: Respiratory Care Services Job Category:
Job Title: (Respiratory Specialist) Reports to: Annette Moser Responsibility Level: Staff Direct Supervision: Respiratory Manager Job Location: UI Health Department: Respiratory Care Services Job Category:
QUESTIONS. Print Student s/faculty Name: Date of Test Completion: Site of Experience: School/University: Semester:
 2017 - QUESTIONS Print Student s/faculty Name: Date of Test Completion: Site of Experience: School/University: Semester: Instructions: Read each question, write an answer on space provided, and return
2017 - QUESTIONS Print Student s/faculty Name: Date of Test Completion: Site of Experience: School/University: Semester: Instructions: Read each question, write an answer on space provided, and return
at OU Medicine Leadership Development Institute August 6, 2010
 Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
December 2008 RT Cerner Enhancements FAQ December 12, 2008
 December RT Cerner Enhancements FAQ December 12, Facility/Audience: Check information on each item Addition of Lag Time to Assignment Shift Change In order to see your Assignment during shift change, you
December RT Cerner Enhancements FAQ December 12, Facility/Audience: Check information on each item Addition of Lag Time to Assignment Shift Change In order to see your Assignment during shift change, you
SPECIAL MEMORANDUM. All Fresno/Kings/Madera/Tulare EMS Providers, Hospitals, First Responder Agencies, and Interested Parties
 Central California Emergency Medical Services Agency A Division of Fresno County Department of Public Health SPECIAL MEMORANDUM FILE #: F/K/M/T #05-2018 TO: FROM: All Fresno/Kings/Madera/Tulare EMS Providers,
Central California Emergency Medical Services Agency A Division of Fresno County Department of Public Health SPECIAL MEMORANDUM FILE #: F/K/M/T #05-2018 TO: FROM: All Fresno/Kings/Madera/Tulare EMS Providers,
Technology s Role in Support of Optimal Perinatal Staffing. Objectives 4/16/2013
 Technology s Role in Support of Optimal Perinatal Cathy Ivory, PhD, RNC-OB April, 2013 4/16/2013 2012 Association of Women s Health, Obstetric and Neonatal s 1 Objectives Discuss challenges related to
Technology s Role in Support of Optimal Perinatal Cathy Ivory, PhD, RNC-OB April, 2013 4/16/2013 2012 Association of Women s Health, Obstetric and Neonatal s 1 Objectives Discuss challenges related to
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
About the Critical Care Center
 Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Indications for Calling A Code Blue or Pediatric Medical Emergency
 Code Blue/Pediatric Medical Emergency Code Blue is a term used to alert the Code Team and hospital staff of the significant deterioration in an individual s status (e.g. unresponsiveness, absence of blood
Code Blue/Pediatric Medical Emergency Code Blue is a term used to alert the Code Team and hospital staff of the significant deterioration in an individual s status (e.g. unresponsiveness, absence of blood
Beth Israel Deaconess Medical Center Perioperative Services Manual. Guidelines for Perioperative Handoffs from OR to receiving units.
 Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease
 Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease Course lead Colette Laws-Chapman Faculty Course / Curriculum Recognising the Deteriorating Adult Target Delegates
Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease Course lead Colette Laws-Chapman Faculty Course / Curriculum Recognising the Deteriorating Adult Target Delegates
CRITICAL ACCESS HOSPITALS
 Does the CAH provide emergency services that meet acceptable standards of practice for inpatients and outpatients 24 hours a day? 19 CSR 30-20.092(1) Are all emergency services provided onsite as a direct
Does the CAH provide emergency services that meet acceptable standards of practice for inpatients and outpatients 24 hours a day? 19 CSR 30-20.092(1) Are all emergency services provided onsite as a direct
NCQC PSO Safe Tables. Failure To Rescue. Failure to Rescue
 NCQC PSO Safe Tables Failure To Rescue April 2015 Failure to Rescue Term coined in Australia in 1992 Associated with hospital not pa:ent characteris:cs In response RRTs championed by IHI (100,000 Lives
NCQC PSO Safe Tables Failure To Rescue April 2015 Failure to Rescue Term coined in Australia in 1992 Associated with hospital not pa:ent characteris:cs In response RRTs championed by IHI (100,000 Lives
Sedation/Analgesia by Non-Anesthesiologists. THE UNIVERSITY OF TOLEDO Approving Officer:
 Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Subject: Trauma Team Roles and Responsibilities for TRAUMA ACTIVATION patients
 UNM Trauma & EM Operational Policies Subject: Trauma Team Roles and Responsibilities for TRAUMA ACTIVATION patients Purpose: To define the roles and responsibilities of personnel responding to trauma activations,
UNM Trauma & EM Operational Policies Subject: Trauma Team Roles and Responsibilities for TRAUMA ACTIVATION patients Purpose: To define the roles and responsibilities of personnel responding to trauma activations,
CDRL A006 Training Manual User's Guide for STAT! TM EMEDS ICU Serious Medical Game. Release v November 26, 2014
 CDRL A006 Training Manual User's Guide for STAT! TM EMEDS ICU Serious Medical Game Copyright 2014 Vcom3D, Inc. Release v1.0.0 - November 26, 2014 Sponsored by Air Force Research Laboratory (AFRL) Prepared
CDRL A006 Training Manual User's Guide for STAT! TM EMEDS ICU Serious Medical Game Copyright 2014 Vcom3D, Inc. Release v1.0.0 - November 26, 2014 Sponsored by Air Force Research Laboratory (AFRL) Prepared
STATEMENT OF PURPOSE: Emergency Department staff care for observation patients in two main settings: the ED observation unit (EDOU) and ED tower obser
 and ED tower obser") DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
COA ADVANCED PRACTICE PROVIDER CALL
 COA ADVANCED PRACTICE PROVIDER CALL Tuesday, November 15 th, 12:30 pm ET 2015 Community Oncology Alliance 1 CAPP Co-Chairs: Sarah Alexander, NP-C, Lake Norman Oncology sarah@lakenormanoncology.com Diana
COA ADVANCED PRACTICE PROVIDER CALL Tuesday, November 15 th, 12:30 pm ET 2015 Community Oncology Alliance 1 CAPP Co-Chairs: Sarah Alexander, NP-C, Lake Norman Oncology sarah@lakenormanoncology.com Diana
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Protocol: Name of supervising ED provider: Name of RDTC Faculty: Disposition: Date: / / Time: : (military)
") RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
Medical Intensive Care Unit Rotation EUHM
 PGY 2 Residency Training Program Medical Intensive Care Unit Rotation EUHM Preceptor: Derek M. Polly, PharmD Office: EUHM, 2 nd Floor, Room 2182 Hours: ~ 7:30 4:00 Desk: 404 686 5674 Pager: 404 686 5500
PGY 2 Residency Training Program Medical Intensive Care Unit Rotation EUHM Preceptor: Derek M. Polly, PharmD Office: EUHM, 2 nd Floor, Room 2182 Hours: ~ 7:30 4:00 Desk: 404 686 5674 Pager: 404 686 5500
Complex Airway Services
 Complex Airway Services A REFERENCE GUIDE FOR FAMILIES LIVING OUTSIDE OF CALGARY ZONE CHILDREN WITH COMPLEX AIRWAY NEEDS NOVEMBER 2016 Alberta Children s Hospital Complex Airway Services Reference Guide
Complex Airway Services A REFERENCE GUIDE FOR FAMILIES LIVING OUTSIDE OF CALGARY ZONE CHILDREN WITH COMPLEX AIRWAY NEEDS NOVEMBER 2016 Alberta Children s Hospital Complex Airway Services Reference Guide
Working with Patients on Achieving the Triple Aim
 Working with Patients on Achieving the Triple Aim 1 Morristown Medical 5,940 employees 1,415 physicians 192 medical residents 687 licensed beds 2 39,886 admissions 3 4,254 births 11,986 inpatient surgeries
Working with Patients on Achieving the Triple Aim 1 Morristown Medical 5,940 employees 1,415 physicians 192 medical residents 687 licensed beds 2 39,886 admissions 3 4,254 births 11,986 inpatient surgeries
Quality Improvement 1.) Understand how to use a fishbone diagram and process map to analyze patient safety concerns 2.) Develop an AIM statement
 Understand how to use a fishbone diagram and process map to analyze patient safety concerns 2.) Develop an AIM statement") It s not about the quantity but the quality: A QI Workshop for Dummies John Raimo, MD Sara Cerrone, MD Semie Kang, DO Sean LaVine, MD 1 Quality Improvement 1.) Understand how to use a fishbone diagram
It s not about the quantity but the quality: A QI Workshop for Dummies John Raimo, MD Sara Cerrone, MD Semie Kang, DO Sean LaVine, MD 1 Quality Improvement 1.) Understand how to use a fishbone diagram
UPMC PRESBYTERIAN SHADYSIDE POLICY AND PROCEDURE MANUAL
 UPMC PRESBYTERIAN SHADYSIDE POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: CP-12 Care of Patients SUBJECT: Rapid Response System DATE: February 28, 2013 I. POLICY CORRESPONDING PROCEDURES: CP-12-PRO
UPMC PRESBYTERIAN SHADYSIDE POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: CP-12 Care of Patients SUBJECT: Rapid Response System DATE: February 28, 2013 I. POLICY CORRESPONDING PROCEDURES: CP-12-PRO
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
Title: ED Management of Trauma Patient Protocol
 Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Scope of Research Services
 Office of Clinical Research B-1177, CC 973-972-7909 Scope of Research Services This form should be used to request any hospital services related to the study that will not be provided by investigators.
Office of Clinical Research B-1177, CC 973-972-7909 Scope of Research Services This form should be used to request any hospital services related to the study that will not be provided by investigators.
MEDICAL DIRECTIVE Rapid Response System (RRS) Suspected Anaphylaxis Like
 Suspected Anaphylaxis Like") GENERAL PREAMBLE: The purpose of the Rapid Response System (RRS) is to assist in the early recognition of patients at risk of developing critical illnesses. It is well known that greater than 80% of in-hospital
GENERAL PREAMBLE: The purpose of the Rapid Response System (RRS) is to assist in the early recognition of patients at risk of developing critical illnesses. It is well known that greater than 80% of in-hospital
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
Respiratory Therapy Program Technical Standards
 Respiratory Therapy Program Technical Standards Technical Standards define the observational, communication, cognitive, affective, and physical capabilities deemed essential to complete this program and
Respiratory Therapy Program Technical Standards Technical Standards define the observational, communication, cognitive, affective, and physical capabilities deemed essential to complete this program and
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience. Presented by: Fadwa Jabboury, RN, MSN
 CMC Experience. Presented by: Fadwa Jabboury, RN, MSN") Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
The TeleHealth Model THE TELEHEALTH SOLUTION
 The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
Barriers to Early Rehabilitation in Critically Ill Patients. Shannon Goddard, MD Sunnybrook Health Sciences Centre
 Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
Shadow-a-Professional Program 2016 Application
 Thank you for your interest in The Shadow-A-Professional program that allows high school junior and senior students interested in the hospital industry to explore career options and/or gain experience
Thank you for your interest in The Shadow-A-Professional program that allows high school junior and senior students interested in the hospital industry to explore career options and/or gain experience
Documentation & Communication in Adult/Medical Settings. Devina Acharya, MA, CCC/SLP, CSUSM
 Documentation & Communication in Adult/Medical Settings Devina Acharya, MA, CCC/SLP, CSUSM When in Rome. do as your facility does 2 Who s the Boss? Doctor makes decisions and bears ultimate responsibility
Documentation & Communication in Adult/Medical Settings Devina Acharya, MA, CCC/SLP, CSUSM When in Rome. do as your facility does 2 Who s the Boss? Doctor makes decisions and bears ultimate responsibility
CAC: Understanding the Technology and Lessons Learned from Early Adopters and The Next Big Thing : Core Measures and Quality Reporting
 CAC: Understanding the Technology and Lessons Learned from Early Adopters and The Next Big Thing : Core Measures and Quality Reporting Matt Turner, Regional Manager, Dolbey mturner@dolbey.com What is Computer-Assisted
CAC: Understanding the Technology and Lessons Learned from Early Adopters and The Next Big Thing : Core Measures and Quality Reporting Matt Turner, Regional Manager, Dolbey mturner@dolbey.com What is Computer-Assisted
The ICU Outreach RN Team
 The ICU Outreach RN Team Results of a Three Year Evaluation Surrey Memorial Hospital Fraser Health Authority, B.C. Pam Dawson, Pamela McElheran, Wendy O Connor, Jennifer Caryk & Lori Lakusta Dynamics of
The ICU Outreach RN Team Results of a Three Year Evaluation Surrey Memorial Hospital Fraser Health Authority, B.C. Pam Dawson, Pamela McElheran, Wendy O Connor, Jennifer Caryk & Lori Lakusta Dynamics of
Level 3 Trauma Hospital Criteria
 Level 3 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Level 3 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
TITLE: Processing Provider Orders: Inpatient and Outpatient
 POLICY and PROCEDURE TITLE: Processing Provider Orders: Inpatient and Outpatient Number: 13211 Version: 13211.10 Type: Patient Care Author: Carol Vanetti; Provider Order Policy Committee Effective Date:
POLICY and PROCEDURE TITLE: Processing Provider Orders: Inpatient and Outpatient Number: 13211 Version: 13211.10 Type: Patient Care Author: Carol Vanetti; Provider Order Policy Committee Effective Date:
Gender. Age DEMOGRAPHICS POINTS OF DISTINCTION COMISSION FOR ACCREDITATION OF REHABILITATION FACILITIES STATE OF FLORIDA BRAIN AND SPINAL CORD PROGRAM
 POINTS OF DISTINCTION 89-bed Acute Adult Inpatient Rehabilitation Unit, All private rooms 4 th largest Rehabilitation provider in the state of Florida Admitted 2157 patients from April 2017 through March
POINTS OF DISTINCTION 89-bed Acute Adult Inpatient Rehabilitation Unit, All private rooms 4 th largest Rehabilitation provider in the state of Florida Admitted 2157 patients from April 2017 through March
JOB DESCRIPTION/PERFORMANCE EVALUATION NAME: JOB FUNCTION: CONTRACT AGENCY: DATE:
 JOB DESCRIPTION/PERFORMANCE EVALUATION NAME: JOB FUNCTION: CONTRACT AGENCY: DATE: This performance evaluation provides the contract worker and the organization with a clear understanding of the contract
JOB DESCRIPTION/PERFORMANCE EVALUATION NAME: JOB FUNCTION: CONTRACT AGENCY: DATE: This performance evaluation provides the contract worker and the organization with a clear understanding of the contract
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
1. Receives report from EMS and/or outlying facility. 5. Adheres to safety and universal precaution guidelines.
 Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Case study. Integrating Simulation into Nursing Curriculum. Fulda, Germany. Fulda University of Applied Sciences.
 Case study Integrating Simulation into Nursing Curriculum Fulda University of Applied Sciences Fulda, Germany By: Ellen Thomseth, Laerdal Medical This case study is one, in a series of three, describing
Case study Integrating Simulation into Nursing Curriculum Fulda University of Applied Sciences Fulda, Germany By: Ellen Thomseth, Laerdal Medical This case study is one, in a series of three, describing
Type of intervention Treatment. Economic study type Cost-effectiveness analysis.
 Human and financial costs of noninvasive mechanical ventilation in patients affected by COPD and acute respiratory failure Nava S, Evangelisti I, Rampulla C, Compagnoni M L, Fracchia C, Rubini F Record
Human and financial costs of noninvasive mechanical ventilation in patients affected by COPD and acute respiratory failure Nava S, Evangelisti I, Rampulla C, Compagnoni M L, Fracchia C, Rubini F Record
Family Practice Clinic
 Family Practice Clinic FNP Job Description (Hospital Privileges) General: The Family Nurse Practitioner (FNP) assesses, plans and provides comprehensive patient care independently or in autonomous collaboration
Family Practice Clinic FNP Job Description (Hospital Privileges) General: The Family Nurse Practitioner (FNP) assesses, plans and provides comprehensive patient care independently or in autonomous collaboration
HAWAII HEALTH SYSTEMS CORPORATION
 All Positions HE-13 6.822 Function and Location This position works in the respiratory therapy unit of a hospital and is responsible for supervising several respiratory therapy technicians in providing
All Positions HE-13 6.822 Function and Location This position works in the respiratory therapy unit of a hospital and is responsible for supervising several respiratory therapy technicians in providing
ASCO s Quality Training Program
 ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
Coding Guidelines for Certain Respiratory Care Services January 2018 (updates in red)
") Coding Guidelines for Certain Respiratory Care Services (updates in red) Overview From time to time the AARC receives inquiries about respiratory-related coding and coverage issues through its Help Line
Coding Guidelines for Certain Respiratory Care Services (updates in red) Overview From time to time the AARC receives inquiries about respiratory-related coding and coverage issues through its Help Line
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager A HEALTHIER WORLD THROUGH BOLD INNOVATION
 Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager Department of Respiratory Care UC Davis Medical Center, Sacramento CA UC Davis ROAD Center kmcraddock@ucdavis.edu University of California Davis ROAD
Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager Department of Respiratory Care UC Davis Medical Center, Sacramento CA UC Davis ROAD Center kmcraddock@ucdavis.edu University of California Davis ROAD
Creating Care Pathways Committees
 Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Guiding principles. The spectrum of home based hospital care 4/26/2018. Consistent with Triple Aim. Safe. Patient Centered
 Lake Superior QIN: 2018 Readmissions Action Learning Day April 30, 2018 Guiding principles Consistent with Triple Aim Safe Patient Centered Create new business opportunities and benefits for HealthPartners
Lake Superior QIN: 2018 Readmissions Action Learning Day April 30, 2018 Guiding principles Consistent with Triple Aim Safe Patient Centered Create new business opportunities and benefits for HealthPartners
IMPROVEMENT IN TIME TO ANTIBIOTICS FOR MGH PEDIATRIC ED PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014
 IMPROVEMENT IN TIME TO ANTIBIOTICS FOR MGH PEDIATRIC ED PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: This innovation reduces time to pediatric antibiotic administration by using
IMPROVEMENT IN TIME TO ANTIBIOTICS FOR MGH PEDIATRIC ED PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: This innovation reduces time to pediatric antibiotic administration by using
Health Information Technology and Interdisciplinary Teamwork in the VA
 Health Information Technology and Interdisciplinary Teamwork in the VA Joanne Spetz, Ph.D. University of California, San Francisco Ciaran Phibbs, Ph.D. VA Health Economics Resource Center October 2008
Health Information Technology and Interdisciplinary Teamwork in the VA Joanne Spetz, Ph.D. University of California, San Francisco Ciaran Phibbs, Ph.D. VA Health Economics Resource Center October 2008
KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 EFFECTIVE DATE: January January 2013 NPP600-E-6
 KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 Fall Prevention Barbara Bird, MSN, RN-BC, CCNS EFFECTIVE DATE: 8310-0005 Falls Council/ Prevention Committee
KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 Fall Prevention Barbara Bird, MSN, RN-BC, CCNS EFFECTIVE DATE: 8310-0005 Falls Council/ Prevention Committee
Medication Management: New Technology to Reduce Cost and Increase Efficiency. Dan Grady, MEd, RRT, FAARC. copyright 2011
 Medication Management: New Technology to Reduce Cost and Increase Efficiency By Dan Grady, MEd, RRT, FAARC 1 Disclosures Relationships with: CPC, Inc. TherOx, Inc. Outcome Solutions LLC AARC 2 Background
Medication Management: New Technology to Reduce Cost and Increase Efficiency By Dan Grady, MEd, RRT, FAARC 1 Disclosures Relationships with: CPC, Inc. TherOx, Inc. Outcome Solutions LLC AARC 2 Background
THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING. Australasian Rehabilitation Nurses Association June 26 th 2015
 THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING Australasian Rehabilitation Nurses Association June 26 th 2015 Conflict of Interest and affiliations No conflicts of interest regarding this topic. Current
THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING Australasian Rehabilitation Nurses Association June 26 th 2015 Conflict of Interest and affiliations No conflicts of interest regarding this topic. Current
Owning and Developing Your Practice Through Alignment
 Owning and Developing Your Practice Through Alignment David Mantz Director, Respiratory Care, Sleep Disorders Center and The Tammy Walker Cancer Center Salina Regional Health Center Salina Kansas Alignment
Owning and Developing Your Practice Through Alignment David Mantz Director, Respiratory Care, Sleep Disorders Center and The Tammy Walker Cancer Center Salina Regional Health Center Salina Kansas Alignment
SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE MATERNAL TRANSPORT TEAM
 SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE MATERNAL TRANSPORT TEAM EFFECTIVE DATE: REVISED DATE: STANDARD TYPE:, 4/95 1/18 DEPARTMENTAL INTERDEPARTMENTAL DEPARTMENTS PROVIDING NURSING
SARASOTA MEMORIAL HOSPITAL STANDARDS OF CARE STANDARDS OF PRACTICE MATERNAL TRANSPORT TEAM EFFECTIVE DATE: REVISED DATE: STANDARD TYPE:, 4/95 1/18 DEPARTMENTAL INTERDEPARTMENTAL DEPARTMENTS PROVIDING NURSING
Curricular area: Inpatient Internal Medicine Specific Rotations: Medicine Inpatient Service Responsible faculty:
 Curricular area: Inpatient Internal Medicine Specific Rotations: Medicine Inpatient Service Responsible faculty: Goals: develop and refine the necessary knowledge base, medical interviewing skills, and
Curricular area: Inpatient Internal Medicine Specific Rotations: Medicine Inpatient Service Responsible faculty: Goals: develop and refine the necessary knowledge base, medical interviewing skills, and
Transitions of Care. Scott Clark, President Leading Edge Health Care
 Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Mobile Communications
 Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Update on the Maryland Patient Safety Program
 Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Third Annual Maryland Patient
Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Third Annual Maryland Patient
San Joaquin County Emergency Medical Services Agency
 San Joaquin County Emergency Medical Services Agency http://www.sjgov.org/ems DATE: Mailing Address PO Box 220 French Camp, CA 95231 TO: FROM: SUBJ.: All Prehospital Personnel and Providers Emergency Department
San Joaquin County Emergency Medical Services Agency http://www.sjgov.org/ems DATE: Mailing Address PO Box 220 French Camp, CA 95231 TO: FROM: SUBJ.: All Prehospital Personnel and Providers Emergency Department