Applying Human Factors to Healthcare Systems Safety
|
|
|
- Dale Sherman
- 5 years ago
- Views:
Transcription
1 April 29 th, 2014 To Better is Human TM Applying Human Factors to Healthcare Systems Safety A. Zach Hettinger, MD MS Medical Director National Center for Human Factors in Healthcare MedStar Institute for Innovation (MI2), MedStar Health Research Institute Assistant Professor of Emergency Medicine Georgetown University School of Medicine 1
2 Disclosures Root Cause Analysis Emergency Medicine Patient Safety Foundation Latham Foundation American Society for Healthcare Risk Mgt (ASHRM) Other Funding Agency for Healthcare Research & Quality Office of the National Coordinator National Institutes of Health 2
3 Agenda Case What is Human Factors? Concepts in Human Factors Effective & Sustainable Solutions Skill/Rule/Knowledge Based Errors Just Culture Conclusion 3

4 It starts with a CASE 4

5 Glucometer test result What was the glucose test result? HIGH or LOW? 5

6 6


7 How could you miss it? 7

8 Critical Low: 0.1% of results (119/80,000) 8
9 Who is the expert? Hospital Text of Out of Reportable Range message popup A Critical value; Repeat; Lab Draw for > 600. B RR Lo = result <40; RR Hi = result >600 C D E F Out of range: repeat test to confirm Critical value; repeat within 15 mins; notification required; lab draw for >600 Critical value; you must repeat immediately; STAT glucose Lab draw for RR HI Repeat test CRITICAL VALUE; REPEAT TEST: NOTIFY MD/RN 9
10 What is HUMAN FACTORS 10

11 What is Human Factors Engineering? Designing.. systems, process, and devices.with regards to what humans do well. 11

12 What is Human Factors Engineering? and what we do with variability.. 12



13 Human Factors Engineering We don t redesign humans; We redesign the system within which humans work 13

14 Human Factors Engineering (HFE) Designing for human use Human-Machine Interface (display, control) Optimizes the relationship between technology and the human user Designs the system to match abilities Data-driven, evidence based Normal in aviation, nuclear, military 14

15 15

16 16

17 17

18 18
19 19



20 20

21 Ambiguous Signage 21

22 Even Door Design has Real World Consequences 22
23 Human Factors CONCEPTS 23
24 Just Culture: The Three Behaviors Normal Error At-Risk Behavior Reckless Behavior Inadvertent action: slip, lapse, mistake A choice: risk not recognized or believed justified Conscious disregard of unreasonable risk Manage through changes in: Processes Procedures Recurrent training Design Environment Manage through: Removing incentives for At- Risk Behaviors Creating incentives for healthy behaviors Increasing situational awareness Re-examining environment Manage through: Remedial action Punitive action Support Coach Sanction Adapted from: David Marx, Just Culture. Outcome Engineering 2008: See also, Just Culture: Balancing Safety and Accountability, Sidney Dekker (2008) 24
25 Applying Human Factors to ROOT CAUSE ANALYSIS 25

26 Study Overview 26
27 27
28 Institutional Definition: Facility wide change that requires a large capital investment Example: Medical image delayed secondary to morbid obesity and lack of access to adequate inhouse imaging. Solution: New bariatric accesible imaging equipment 28
29 Information Technology Structure Definition: Changing features of EHR/Health IT system to change functionality Example: A patient aspirated despite being clinically identified as high risk for aspiration by staff members Solution: Ability to track aspiration precautions through EHR 29


30 30

31 31
32 32
33 Physical Environment Definition: Changes to the physical environment within which medical staff work Example Case: A patient with anaphylaxis is given 0.5 mg of 1:10,000 epinephrine, instead of 0.3mg of 1:1,000 because the later was not available. Solution: Patient care environments stocked with 1:1000 epinephrine 33

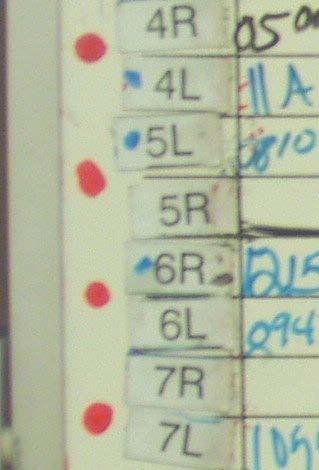
34 Defibrillator Case VF cardiac arrest nurse with patient charges unit clears patient presses on button Machine powers down 2-3 minute delay in shock 34


35 Projectors Don t Kill People
36 Process Definition: Changing the work process and flow of the healthcare workers in an attempt to reduce hazards Example: A post surgical patient aspirates and dies without a swallow evaluation, despite recognition as an aspiration risk by staff. Solution: A standard process/protocol developed to implement aspiration precautions. Aspiration precautions should be the standard of care for all patients with difficulty swallowing. Swallowing study can be done seven days a week 36
37 Forms & Paperwork Definition: New forms or changes to documentation templates and procedures. Example: A critically lab value repeated per protocol, but paper requisition never filed and test not performed. Solution: All lab specimens required to have a requisition/order for testing 37
38 38
39 Review Definition: An assessment of a particular system/process Example: A patient with sepsis (RRT evaluated the day before) was transported to radiology where she died while awaiting transport. Solution: Implement regular RRT case review with staff within 24 hours to provide a feedback loop to identify points in care where interventions could have prevented RRT 39
40 Training Definition: Education is the primary goal of the solution, either of individuals or groups. Example: Critical labs from a dialysis session and a hypotensive episode were not communicated to floor team, leading to a delayed response to a patient s critical lab values. Solution: Dialysis staff to provide written and a verbal report to home unit of any changes in patient status. 40
41 Knowledge-Based Improvisation in unfamiliar environments No routines or rules available to help handle Protocolized behavior Process, Procedure Rule-Based Skill-Based Automated Routines Require little conscious attention Figure adapted from: Embrey D. Understanding Human Behaviour and Error, Human Reliability Associates Based on Rasmussen s SRK Model of cognitive control, adapted to explain error by Reason (1990, 2008) 41
42 Slips and Lapses: Common Policies, Inservices, Discipline, Training, Vigilance Encouraging Mindfulness
43 Example: Skill-based level, humans see patterns Aoccdrnig to rscheearch at Cmabrigde Uinervtisy, it deosn't mttaer in waht oredr the ltteers in a wrod are, the olny iprmoetnt tihng is taht the frist and lsat ltteer be at the rghit pclae. The rset can be a toatl mses and you can sitll raed it wouthit a porbelm. Tihs is bcuseae the huamn mnid deos not raed ervey lteter by istlef, but the wrod as a wlohe. 43




44 Medication Labeling 44


45 45
46 Compliance Checks Definition: These solutions are focused on reviews of charts or processes for the purpose of monitoring or regulating a particular process. Case: An elderly woman fell out of bed and broke her hip. Solution: Incorporate hourly rounding into concurrent auditing. 46
47 Policy Definition: Changes that are limited to creating, changing or reinforcing a policy. Case: Due to a patient mix up, a hearing impaired patient received an unnecessary procedure. Solution: The nurse and the transporter must jointly ID the patient prior to the patient leaving the unit. 47

48 48
49 Counseling Definition: The creation of development plan, feedback or referral to practice committee for individuals. Contact Third Parties Definition: The involvement of third parties includes bringing in manufacturers representatives, motivational speakers and other consultants. 49
50 Risk Management Definition: These solutions focus only on the involvement of Risk Management Disciplinary Definition: These solutions focus disciplinary actions taken towards involved staff members. 50
51 Just Culture: The Three Behaviors Normal Error At-Risk Behavior Reckless Behavior Inadvertent action: slip, lapse, mistake A choice: risk not recognized or believed justified Conscious disregard of unreasonable risk Manage through changes in: Processes Procedures Recurrent training Design Environment Manage through: Removing incentives for At- Risk Behaviors Creating incentives for healthy behaviors Increasing situational awareness Re-examining environment Manage through: Remedial action Punitive action Support Coach Sanction Adapted from: David Marx, Just Culture. Outcome Engineering 2008: See also, Just Culture: Balancing Safety and Accountability, Sidney Dekker (2008) 51
52 Video
53 CONCLUSION 53
54 Staged Sustainability Approach Effectiveness Sustainability 54
55 Take Home Points Staged Approach Generalizability Limiting individual focused solutions Classify the contributing factors and create solution appropriate to the error Consider Implementation of Just Culture 55
56 Be Optimistic _g&feature=youtu.be 56
57 Thank you Terry Fairbanks, MD, MS Amy Bisantz, PhD Vicki Lewis, PhD Robert Wears, MD, PhD John Wreathall, MS Sudeep Hegde, MS Alex Rackoff, MD Kate Kellogg, MD 57
58 Questions? 58
59 TABLETOP EXCERCISE 59
60 Skill/Rule/Knowledge Based Errors Case 1: A new physician is admitting a patient from the emergency department, and places the patient with chest pain on a non-telemetry unit. While waiting to move to the correct floor, the patient has an arrhythmia that is not initially detected and the patient has a poor outcome. Case 2: While performing triage on a patient with stomach pain in the emergency department a nurse uses the standing abdominal pain orders to request lab and urine tests. An hour later the patient is seen by the physician who immediately orders an EKG which shows a STEMI (heart attack) and the patient is rushed to the cardiac catheterization lab. Case 3: A nurse receives an order for clindamycin 300mg PO, obtains the medication from the automated medication system and administers it to the patient after performing the safety checks. Thirty minutes after receiving the medication the patient has an anaphylactic reaction requiring a stay in the ICU. It was later determined that the patient was given Pen VK to which they have a known allergy, and that the medications were stocked in the system incorrectly. 60



61 Knowledge-Based Improvisation in unfamiliar environments No routines or rules available to help handle Protocolized behavior Process, Procedure Rule-Based Skill-Based Automated Routines Require little conscious attention Figure adapted from: Embrey D. Understanding Human Behaviour and Error, Human Reliability Associates Based on Rasmussen s SRK Model of cognitive control, adapted to explain error by Reason (1990, 2008) 61
62 Just Culture Case 1: In an effort to perform all of the patient care duties and documentation, a patient care tech uses barcodes taped to a desk instead of the patient s wrist bands to improve efficiency. Case 2: A medical staff member is known by other members to be disrespectful; when asked about some medical decisions that lead to hazardous situations and patient harm he states I don t care and I ve always done it this way. Case 3: After opening the chart to write an order for antibiotics for a patient with low blood pressure and sepsis (blood infection), a physician is approached by a nurse and asked for pain medications for a different patient. The physician writes the order for Dilaudid 1mg IV for the patient with sepsis that results in a further lowering of their blood pressure and requires additional IV fluids and monitoring. 62
63 Just Culture: The Three Behaviors Normal Error At-Risk Behavior Reckless Behavior Inadvertent action: slip, lapse, mistake A choice: risk not recognized or believed justified Conscious disregard of unreasonable risk Manage through changes in: Processes Procedures Recurrent training Design Environment Manage through: Removing incentives for At- Risk Behaviors Creating incentives for healthy behaviors Increasing situational awareness Re-examining environment Manage through: Remedial action Punitive action Support Coach Sanction Adapted from: David Marx, Just Culture. Outcome Engineering 2008: See also, Just Culture: Balancing Safety and Accountability, Sidney Dekker (2008) 63
64 Sustainable System Solutions Case 1: After an adverse event all staff members are given an in-service on the Patient Controlled Analgesia (PCA) pump (medical device) that has been involved in multiple medication overdoses. Case 2: After multiple observation sessions where medical staff is observed not washing their hands, the team decides to add alcohol-based hand sanitizers outside each patient room. Case 3: A physician is fired after performing a procedure on the wrong side of the patient. 64


65 Questions? 65
Systems Thinking & Human Factors Engineering in Healthcare
 Clinical Networks and Streams and Managers John Hunter Hospital Newcastle, NSW; August 10, 2015 Systems Thinking & Human Factors Engineering in Healthcare Rollin J. (Terry) Fairbanks, MD, MS Director,
Clinical Networks and Streams and Managers John Hunter Hospital Newcastle, NSW; August 10, 2015 Systems Thinking & Human Factors Engineering in Healthcare Rollin J. (Terry) Fairbanks, MD, MS Director,
Embracing a Culture of Safety and Learning
 Embracing a Culture of Safety and Learning Provincial Forum on Adverse Health Event Management St. John s Newfoundland May 26, 2008 Ward Flemons MD, FRCPC Vice-President, Health Outcomes Outline Adverse
Embracing a Culture of Safety and Learning Provincial Forum on Adverse Health Event Management St. John s Newfoundland May 26, 2008 Ward Flemons MD, FRCPC Vice-President, Health Outcomes Outline Adverse
Human Factor and Patient Safety. Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA)
") Human Factor and Patient Safety Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA) Human Factors and Patient Safety Unforeseen ice problem caused
Human Factor and Patient Safety Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA) Human Factors and Patient Safety Unforeseen ice problem caused
TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation
 TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation Donna Woods, EdM, PhD Assistant Professor and Co Director, Graduate Programs In Healthcare Quality
TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation Donna Woods, EdM, PhD Assistant Professor and Co Director, Graduate Programs In Healthcare Quality
What s the data telling you? Using evidence-based stories for health planning and decision-making
 MANITOBA CENTRE FOR HEALTH POLICY What s the data telling you? Using evidence-based stories for health planning and decision-making Bayline RRT Meeting Randy Fransoo May 25, 2007 Manitoba Centre for Health
MANITOBA CENTRE FOR HEALTH POLICY What s the data telling you? Using evidence-based stories for health planning and decision-making Bayline RRT Meeting Randy Fransoo May 25, 2007 Manitoba Centre for Health
JUST CULTURE FEBRUARY 20, 2013 KAREN ZANIN RN CNOR
 JUST CULTURE FEBRUARY 20, 2013 KAREN ZANIN RN CNOR Balance A Just Culture balances the need to learn from mistakes with the need to take corrective action against an individual if the individual s conduct
JUST CULTURE FEBRUARY 20, 2013 KAREN ZANIN RN CNOR Balance A Just Culture balances the need to learn from mistakes with the need to take corrective action against an individual if the individual s conduct
Medication Safety: Lessons Learned
 Medication Safety: Lessons Learned CINA 30 th Anniversary Conference October 20 th, 2005 Christine Koczmara,, RN, BScPsy Medication Safety: Lessons Learned ISMP Canada Research Highlights Making Health
Medication Safety: Lessons Learned CINA 30 th Anniversary Conference October 20 th, 2005 Christine Koczmara,, RN, BScPsy Medication Safety: Lessons Learned ISMP Canada Research Highlights Making Health
2017 Pharmacy Education Series
 2017 Pharmacy Education Series Featured Speaker: Christina Michalek, BS, RPh, FASHP Medication Safety Specialist Institute for Safe Medication Practices October 18, 2017 Improving Patient Safety: Preventing
2017 Pharmacy Education Series Featured Speaker: Christina Michalek, BS, RPh, FASHP Medication Safety Specialist Institute for Safe Medication Practices October 18, 2017 Improving Patient Safety: Preventing
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10
 Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
10/4/2012. Disclosure. Leading a Meaningful Event Investigation. Just Culture definition. Objectives. What we all have in common
 Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
How Should Policy Reflect a Culture of Safety?
 How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
Simulation Design Template. Date: May 7, 2008 File Name: Group 4
 Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
Patrol Procedures SURVIVAL TRIANGLE ATTITUDE. FBI/UCR Report of Officers Killed and Assaulted. Officers Killed and Assaulted
 Patrol Procedures SURVIVAL TRIANGLE ATTITUDE Statistics (2011) LOD are UP 6% As of August 0, 2011 at 112 Auto Related Deaths are DOWN 17% As of August 08, 2011 at 40 Gunfire Deaths are UP 21% As of August
Patrol Procedures SURVIVAL TRIANGLE ATTITUDE Statistics (2011) LOD are UP 6% As of August 0, 2011 at 112 Auto Related Deaths are DOWN 17% As of August 08, 2011 at 40 Gunfire Deaths are UP 21% As of August
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Disclosures. Medication Incident. Objectives 4/23/2015. No conflicts to disclose
 Disclosures No conflicts to disclose Kara Browne Senior Pharmacy Technician Saskatoon Cancer Centre Objectives Overview of common medication incidents and their causes Overview of available pharmacy technology
Disclosures No conflicts to disclose Kara Browne Senior Pharmacy Technician Saskatoon Cancer Centre Objectives Overview of common medication incidents and their causes Overview of available pharmacy technology
Drug Events. Adverse R EDUCING MEDICATION ERRORS. Survey Adapted from Information Developed by HealthInsight, 2000.
 Survey Adapted from Information Developed by HealthInsight, 2000. Adverse Drug Events R EDUCING MEDICATION ERRORS The Adverse Drug Events Survey will assist healthcare organizations evaluate the number
Survey Adapted from Information Developed by HealthInsight, 2000. Adverse Drug Events R EDUCING MEDICATION ERRORS The Adverse Drug Events Survey will assist healthcare organizations evaluate the number
Protocol: Name of supervising ED provider: Name of RDTC Faculty: Disposition: Date: / / Time: : (military)
") RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM
 CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Washington Patient Safety Coalition December 10, 2014
 Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
Simulation Design Template
 Simulation Design Template Date: May 7/8, 2008 File Name: Discipline: RN, Charge nurse, medical radiology, pharmacy tech, social work, medicine (whatever is available at the institution) Student Level:
Simulation Design Template Date: May 7/8, 2008 File Name: Discipline: RN, Charge nurse, medical radiology, pharmacy tech, social work, medicine (whatever is available at the institution) Student Level:
JUST CULTURE DECEMBER 12,2012
 JUST CULTURE DECEMBER 12,2012 P R E S E N T E D B Y : K A T H Y F O W L E R : Q I P R O J E C T M A N A G E R M A R G R E T T U C K E R : W O U N D C A R E N U R S E P A U L L E V Y : N U R S E E D U C
JUST CULTURE DECEMBER 12,2012 P R E S E N T E D B Y : K A T H Y F O W L E R : Q I P R O J E C T M A N A G E R M A R G R E T T U C K E R : W O U N D C A R E N U R S E P A U L L E V Y : N U R S E E D U C
Simulation Design Template. Location for Reflection:
 Simulation Design Template Date: Discipline: Expected Simulation Run Time: Location: Admission Date: Today s Date: Brief Description of Client Name: Gender: Age: Race: File Name: Student Level: Guided
Simulation Design Template Date: Discipline: Expected Simulation Run Time: Location: Admission Date: Today s Date: Brief Description of Client Name: Gender: Age: Race: File Name: Student Level: Guided
The Human Factor: Applying Safety Science in Health Care
 The Human Factor: Applying Safety Science in Health Care Sarah Henrickson Parker, PhD Director of Education and Academic Affairs, Research Scientist National Center for Human Factors Engineering in Healthcare
The Human Factor: Applying Safety Science in Health Care Sarah Henrickson Parker, PhD Director of Education and Academic Affairs, Research Scientist National Center for Human Factors Engineering in Healthcare
Example of a Health Care Failure Mode and Effects Analysis for IV Patient Controlled Analgesia (PCA) Failure Modes (what might happen)
 Failure Modes (what might happen)") Prescribing Assess patient Choose analgesic/mode of delivery Prescribe analgesic Institute for Safe Medication Practices Example of a Health Care and Effects Analysis for IV Patient Controlled Analgesia
Prescribing Assess patient Choose analgesic/mode of delivery Prescribe analgesic Institute for Safe Medication Practices Example of a Health Care and Effects Analysis for IV Patient Controlled Analgesia
About the Critical Care Center
 Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Professional Practice and Patient Safety Council
 Recommendation # 1 resubmitted by PPPSC on December 8, 2011 to Sue Eckert, Chief Nurse Executive Situation: We share the goal of the Hospital to decrease falls and pressure sores but there is redundancy.
Recommendation # 1 resubmitted by PPPSC on December 8, 2011 to Sue Eckert, Chief Nurse Executive Situation: We share the goal of the Hospital to decrease falls and pressure sores but there is redundancy.
Community Paramedic Program Mobile Integrated Healthcare
 Community Paramedic Program Mobile Integrated Healthcare Problem Statement Problem Statement ACCESS to healthcare Access to healthcare particularly and particularly PRIMARY, Primary and URGENT Specialized
Community Paramedic Program Mobile Integrated Healthcare Problem Statement Problem Statement ACCESS to healthcare Access to healthcare particularly and particularly PRIMARY, Primary and URGENT Specialized
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that
 Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 EFFECTIVE DATE: January January 2013 NPP600-E-6
 KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 Fall Prevention Barbara Bird, MSN, RN-BC, CCNS EFFECTIVE DATE: 8310-0005 Falls Council/ Prevention Committee
KENT HOSPITAL POLICY/PROCEDURE SUBJECT: AUTHORS: APPROVAL DATE: POLICY NUMBER: January 2012 Fall Prevention Barbara Bird, MSN, RN-BC, CCNS EFFECTIVE DATE: 8310-0005 Falls Council/ Prevention Committee
Reducing the risk of serious medication errors in community pharmacy practice
 Reducing the risk of serious medication errors in community pharmacy practice Eastern Medicaid Pharmacy Administrators Association (EMPAA) November 1, 2017 Newport, Rhode Island Michael R. Cohen, RPh,
Reducing the risk of serious medication errors in community pharmacy practice Eastern Medicaid Pharmacy Administrators Association (EMPAA) November 1, 2017 Newport, Rhode Island Michael R. Cohen, RPh,
Patient Safety (PS) 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.
 1) A collaborative process is used to develop policies and/or procedures that address the accuracy of patient identification.") Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Patient Safety (PS) Standard PS.1 [Patient identification] The organization has established procedures for accurately identifying patients. Intent of PS.1 Wrong-patient errors occur in virtually all aspects
Sample. A guide to development of a hospital blood transfusion Policy at the hospital level. Effective from April Hospital Transfusion Committee
 Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Update on the Maryland Patient Safety Program
 Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Fifth Annual Maryland Patient
Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Fifth Annual Maryland Patient
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS)
") PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
INPATIENT Annual Core Competency Performance Stations (Nursing) 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * )
 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * )") County of Los Angeles INPATIENT Annual Core Competency Performance Stations (Nursing) 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * ) * Staff who work in patient care areas 1 ANNUAL CORE
County of Los Angeles INPATIENT Annual Core Competency Performance Stations (Nursing) 2010 (Unlicensed Staff Direct & Non-Direct Care Providers * ) * Staff who work in patient care areas 1 ANNUAL CORE
Keep watch and intervene early
 IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
ENDOSCOPY ORIENTATION COMPETENCY CLINICAL PLAN PROCEDURE REGISTERED NURSE (RN)
") ENDOSCOPY ORIENTATION COMPETENCY CLINICAL PLAN PROCEDURE REGISTERED NURSE (RN) NAME: EMPLOYMENT/TRANSFER DATE: BLS RENEWAL DATE: ALLIANCE ORIENTATION DATE: HOSPITAL ORIENTATION DATE: NURSING ORIENTATION
ENDOSCOPY ORIENTATION COMPETENCY CLINICAL PLAN PROCEDURE REGISTERED NURSE (RN) NAME: EMPLOYMENT/TRANSFER DATE: BLS RENEWAL DATE: ALLIANCE ORIENTATION DATE: HOSPITAL ORIENTATION DATE: NURSING ORIENTATION
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Passage to Excellence Our Sepsis Journey
 Passage to Excellence Our Sepsis Journey St. Catherine of Siena Medical Center October/November 2017 St. Catherine of Siena Medical Center 311 bed community hospital Voluntary medical staff leadership
Passage to Excellence Our Sepsis Journey St. Catherine of Siena Medical Center October/November 2017 St. Catherine of Siena Medical Center 311 bed community hospital Voluntary medical staff leadership
Clinical Interdepartmental Policy and Procedure
 Clinical Interdepartmental Policy and Procedure Policy: Staff Response to Medical Errors/Adverse Events Policy Number: MR-006 Joseph S. Gordy, CEO Signature: Flagler Hospital Originator: President Coordinating
Clinical Interdepartmental Policy and Procedure Policy: Staff Response to Medical Errors/Adverse Events Policy Number: MR-006 Joseph S. Gordy, CEO Signature: Flagler Hospital Originator: President Coordinating
Critical Access Hospitals Site Visit Summary Tom Johns, PharmD, BCPS Director, Pharmacy Services UF Health Shands Hospital
 Critical Access Hospitals Site Visit Summary 2014 2015 Tom Johns, PharmD, BCPS Director, Pharmacy Services UF Health Shands Hospital 2014 2015 13 Critical Access Hospitals (CAH) Site Visits Compounded
Critical Access Hospitals Site Visit Summary 2014 2015 Tom Johns, PharmD, BCPS Director, Pharmacy Services UF Health Shands Hospital 2014 2015 13 Critical Access Hospitals (CAH) Site Visits Compounded
Protecting the Public through Disciplinary Action. Maryann Alexander, PhD, RN, FAAN Kathleen Russell, JD, RN
 Protecting the Public through Disciplinary Action Maryann Alexander, PhD, RN, FAAN Kathleen Russell, JD, RN The Board s Duty Is To Protect The Public Not Punish The Licensee Criminal Justice System Punishment
Protecting the Public through Disciplinary Action Maryann Alexander, PhD, RN, FAAN Kathleen Russell, JD, RN The Board s Duty Is To Protect The Public Not Punish The Licensee Criminal Justice System Punishment
N ATIONAL Q UALITY F ORUM. Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT
 N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
Patient-Centered Fall Prevention Toolkit Paper Fall TIPS Instruction Sheet for Nurses
 Overview Patient-Centered Fall Prevention Toolkit Paper Fall TIPS Instruction Sheet for Nurses Preventing falls is a three step process * : 1) identifying risk factors; 2) developing a tailored or personalized
Overview Patient-Centered Fall Prevention Toolkit Paper Fall TIPS Instruction Sheet for Nurses Preventing falls is a three step process * : 1) identifying risk factors; 2) developing a tailored or personalized
WHAT are medication errors?
 Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
TASCS 2017 Annual Conference 3/2/2017
 Texas Ambulatory Surgery Center Society 2017 Annual Conference Emergency Protocols for Ambulatory Surgery Centers Laura Schneider, RN, CGRN, CASC Objectives 1. Evaluate the level of emergency preparedness
Texas Ambulatory Surgery Center Society 2017 Annual Conference Emergency Protocols for Ambulatory Surgery Centers Laura Schneider, RN, CGRN, CASC Objectives 1. Evaluate the level of emergency preparedness
Surgical Preadmission Information. Joint Replacement Hip. Knee
 Surgical Preadmission Information Joint Replacement Hip Joint Replacement Knee Spine Surgery Planning for Surgery Preoperative Assessments and Tests An appointment for Preoperative Assessments and Tests
Surgical Preadmission Information Joint Replacement Hip Joint Replacement Knee Spine Surgery Planning for Surgery Preoperative Assessments and Tests An appointment for Preoperative Assessments and Tests
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Acute Care Workflow Solutions
 Acute Care Workflow Solutions 2016 North American General Acute Care Workflow Solutions Product Leadership Award The Philips IntelliVue Guardian solution provides general floor, medical-surgical units,
Acute Care Workflow Solutions 2016 North American General Acute Care Workflow Solutions Product Leadership Award The Philips IntelliVue Guardian solution provides general floor, medical-surgical units,
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
AirStrip ONE Cardiology
 AirStrip ONE Cardiology A Synchronized View of the Vital Patient Data Needed to Improve Care Heart disease is the leading cause of death in the U.S. The associated costs exceed $100 billion annually. AirStrip
AirStrip ONE Cardiology A Synchronized View of the Vital Patient Data Needed to Improve Care Heart disease is the leading cause of death in the U.S. The associated costs exceed $100 billion annually. AirStrip
3/9/2010. Objectives. Pharmacist Role in Medication Safety and Regulatory Compliance
 Pharmacist Role in Medication Safety and Regulatory Compliance Janet Greiwe Vice President, Systems Management Cleveland County Health System Objectives By the end of this presentation, you should be able
Pharmacist Role in Medication Safety and Regulatory Compliance Janet Greiwe Vice President, Systems Management Cleveland County Health System Objectives By the end of this presentation, you should be able
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Improving patient safety and infection. Patient Safety Forum Dr J Coleman 1 ELECTRONIC PRESCRIBING AND CLINICAL DECISION SUPPORT (CDS)
") Improving Patient Safety and Infection Control Through Electronic Prescribing Dr Jamie Coleman Senior Lecturer in Clinical Pharmacology / Honorary Consultant Physician The brief Clinical computing technologies
Improving Patient Safety and Infection Control Through Electronic Prescribing Dr Jamie Coleman Senior Lecturer in Clinical Pharmacology / Honorary Consultant Physician The brief Clinical computing technologies
Tools & Resources for QI Success
 Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
During pre-briefing, you will be assigned one of these roles according to the description below to participate in the simulation as a nurse.
 Student Instructions for Standardized Simulation NR 452 Eric Chilton PURPOSE The following information is to be used in guiding your preparation and participation in the scenario for this course. This
Student Instructions for Standardized Simulation NR 452 Eric Chilton PURPOSE The following information is to be used in guiding your preparation and participation in the scenario for this course. This
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Learning from Actual & Near Miss Events
 POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN
 Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Sepsis The Silent Killer in the NHS
 Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Minnesota Adverse Health Events Measurement Guide
 Minnesota Adverse Health Events Measurement Guide Prepared for the Minnesota Department of Health Revised December 2, 2015 is a nonprofit organization that leads collaboration and innovation in health
Minnesota Adverse Health Events Measurement Guide Prepared for the Minnesota Department of Health Revised December 2, 2015 is a nonprofit organization that leads collaboration and innovation in health
Auckland District Health Board Summary 1 July 2011 to 30 June 2012 Serious and Sentinel Events
 DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
Identification of Patient, Resident or Client Using Two Identifiers
 Approved by: Vice President & Chief Medical Officer; and Vice President & Chief Operating Officer Identification of Patient, Resident or Client Using Two Corporate Policy & Procedures Manual Date Approved
Approved by: Vice President & Chief Medical Officer; and Vice President & Chief Operating Officer Identification of Patient, Resident or Client Using Two Corporate Policy & Procedures Manual Date Approved
Text-based Document. Blood Transfusion Education in Medical-Surgical Acute Care Hospitals in the U.S. Downloaded 27-Jun :58:31
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Paediatric First Aid Level 3
 Paediatric First Aid Level 3 This qualification provides theoretical and practical training in emergency first aid techniques that are specific to infants aged under 1, and children aged from 1 year old
Paediatric First Aid Level 3 This qualification provides theoretical and practical training in emergency first aid techniques that are specific to infants aged under 1, and children aged from 1 year old
Two Hospitals-One Heart: World Class Heart Care through Multi-Disciplinary Collaboration
 Two Hospitals-One Heart: World Class Heart Care through Multi-Disciplinary Collaboration American Nurses Association Susie Schnitker RN, BSN, CEN 7 th Annual Nursing Quality Conference Director of Critical
Two Hospitals-One Heart: World Class Heart Care through Multi-Disciplinary Collaboration American Nurses Association Susie Schnitker RN, BSN, CEN 7 th Annual Nursing Quality Conference Director of Critical
Policy for Patient Identification. Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead:
 CONTROLLED DOCUMENT Policy for Patient Identification CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By:
CONTROLLED DOCUMENT Policy for Patient Identification CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By:
According to Lucian Leape, Professor of Health Policy at
 A Statewide Approach to a Just Culture for Patient Safety: The Missouri Story Rebecca Miller, MHA, CPHQ, FACHE; Scott Griffith, MS; and Amy Vogelsmeier, PhD, RN The Missouri Just Culture Collaborative
A Statewide Approach to a Just Culture for Patient Safety: The Missouri Story Rebecca Miller, MHA, CPHQ, FACHE; Scott Griffith, MS; and Amy Vogelsmeier, PhD, RN The Missouri Just Culture Collaborative
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
Student Orientation Post-Assessment
 Name Date Student Orientation Post-Assessment Print, answer questions and bring with you to Education Resources at Penrose Hospital. 1. List two (2) of the seven (7) Centura Core Values and describe their
Name Date Student Orientation Post-Assessment Print, answer questions and bring with you to Education Resources at Penrose Hospital. 1. List two (2) of the seven (7) Centura Core Values and describe their
RescueNet Dispatch, epcr, Care Exchange. HL7 v2. Ellkay LK EMR-Archive Smart on FHIR SAML Ellkay to Epic
 Use Case Title: Heart Attack Overview: Morgan is 40 years old and is experiencing chest pains. A 911 call is placed. Emergency Medical Services arrives and Morgan is evaluated. The decision comes down
Use Case Title: Heart Attack Overview: Morgan is 40 years old and is experiencing chest pains. A 911 call is placed. Emergency Medical Services arrives and Morgan is evaluated. The decision comes down
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Clinical and Financial Successes at Advocate Health Care Utilizing our
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring
 Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Leadership Forum: Promoting a Culture of Safety
 Leadership Forum: Promoting a Culture of Safety Dates: 5/10, 5/13 and 5/14 (Note: All sessions at the InterContinental Hotel) Times: 4-hour sessions (Note: Participants only attend 1 session) o Morning
Leadership Forum: Promoting a Culture of Safety Dates: 5/10, 5/13 and 5/14 (Note: All sessions at the InterContinental Hotel) Times: 4-hour sessions (Note: Participants only attend 1 session) o Morning
Health Management Information Systems: Computerized Provider Order Entry
 Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
STATEMENT OF PURPOSE: Emergency Department staff care for observation patients in two main settings: the ED observation unit (EDOU) and ED tower obser
 and ED tower obser") DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
Ambulatory Patient Safety
 We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Post Market Surveillance Requirements. SAMED Regulatory Conference 2 December 2015
 Post Market Surveillance Requirements SAMED Regulatory Conference 2 December 2015 Topics Surveillance & Vigilance Adverse Events Reportable Adverse Events Reporting Adverse Events Time frames Exemptions
Post Market Surveillance Requirements SAMED Regulatory Conference 2 December 2015 Topics Surveillance & Vigilance Adverse Events Reportable Adverse Events Reporting Adverse Events Time frames Exemptions
Cyclophosphamide INFUSION Infusion 4 Plus
 Cyclophosphamide Infusion Day DEPARTMENT OF RHEUMATOLOGY DAY CASE ADMISSION RECORD PATIENT DAY CASE BOOKING REQUEST To be completed by Consultant, Registrar requesting day case Admission Hospital No. Forename
Cyclophosphamide Infusion Day DEPARTMENT OF RHEUMATOLOGY DAY CASE ADMISSION RECORD PATIENT DAY CASE BOOKING REQUEST To be completed by Consultant, Registrar requesting day case Admission Hospital No. Forename
Mobile Communications
 Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Bedside Shift Reporting
 INCHES 1 2 3 4 5 6 Bedside Shift Reporting Pre-Bedside Checklist: 1. Notify PT/Family 30-60 minutes Before Report Starts 2. Check Pain Score/Adm. Meds if Needed Bedside Report Guide: 1. Introduce Oncoming
INCHES 1 2 3 4 5 6 Bedside Shift Reporting Pre-Bedside Checklist: 1. Notify PT/Family 30-60 minutes Before Report Starts 2. Check Pain Score/Adm. Meds if Needed Bedside Report Guide: 1. Introduce Oncoming
TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry
 TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry DEPARTMENT: PERSONNEL: Telemetry Telemetry Personnel EFFECTIVE DATE: 6/86 REVISED: 02/00, 4/10, 12/14 Admission Procedure: 1. The admitting
TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry DEPARTMENT: PERSONNEL: Telemetry Telemetry Personnel EFFECTIVE DATE: 6/86 REVISED: 02/00, 4/10, 12/14 Admission Procedure: 1. The admitting
The Path to Sustainable Improvements
 What Do You Do When Your Improvement Project FAILS? The Path to Sustainable Improvements Thursday, March 3, 2016 10:00 AM Reza Ziaee, MA, MSE, MBB, PhD, FHIMSS - Antelope Valley Hospital James Bologna
What Do You Do When Your Improvement Project FAILS? The Path to Sustainable Improvements Thursday, March 3, 2016 10:00 AM Reza Ziaee, MA, MSE, MBB, PhD, FHIMSS - Antelope Valley Hospital James Bologna
ED crowding: Causes, Consequences, Solutions
 ED crowding: Causes, Consequences, Solutions Jesse M. Pines, MD, MBA, MSCE Associate Professor of Emergency Medicine and Health Policy George Washington University Urgent Matters Webinar April 23, 2010
ED crowding: Causes, Consequences, Solutions Jesse M. Pines, MD, MBA, MSCE Associate Professor of Emergency Medicine and Health Policy George Washington University Urgent Matters Webinar April 23, 2010
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand