Medication Safety: Lessons Learned
|
|
|
- Samantha Heath
- 6 years ago
- Views:
Transcription


1 Medication Safety: Lessons Learned CINA 30 th Anniversary Conference October 20 th, 2005 Christine Koczmara,, RN, BScPsy
2 Medication Safety: Lessons Learned ISMP Canada Research Highlights Making Health Care Safer: Key Steps 2 Institute for Safe Medication Practices Canada
3 ISMP CANADA Independent nonprofit national organization Founded in 1999 with assistance from ISMP US and Board of Directors Established for: collection and analysis of medication error reports and development of recommendations for the enhancement of patient safety. 3 Institute for Safe Medication Practices Canada
4 Collection of Reports To date, we have collected 11,687 medication incidents in our database. Voluntary reporting Errors, near-misses and hazardous situations confidential non-punitive Front-line practitioners provide detailed, unrestricted information on incidents 4 Institute for Safe Medication Practices Canada
5 How Error Reports are received: 1. website: canada.org; 2. canada.org; 3. Phone: ISMPC [47672] or ISMP Canada guarantees confidentiality and security of information received. ISMP Canada respects the wishes of the reporter as to the level of detail to be included in publications. 5 Institute for Safe Medication Practices Canada

6 How Error Reports are received: 4. Version Supported by MOHLTC for facilities in Ontario 6 Institute for Safe Medication Practices Canada
7 ISMP Canada Programs cont d Analyze-Err Medication Safety Support Service Potassium Chloride Narcotics Medication Safety Self-Assessment Fellowship program- new Education/ Presentations 7 Institute for Safe Medication Practices Canada
 and ISMP Canada 12 per year 8 Institute for Safe Medication Practices")
8 Analysis and Recommendations Available on ISMP Canada s website Supported by Canadian Medication Incident and Reporting and Prevention System (CMIRPS) Collaborative between Health Canada, Canadian Institute for Health Information (CIHI) and ISMP Canada 12 per year 8 Institute for Safe Medication Practices Canada

9 Analysis and Recommendations Bi-Weekly Distribution supported by MOHLTC 9 Institute for Safe Medication Practices Canada
10 Other Initiatives: Journal publications on medication safety CMAJ, CACCN, CHSP Hospital News - monthly article Collaborations: organizations, associations, pharmaceutical, manufacturers, provincial and federal governments 10 Institute for Safe Medication Practices Canada
11 Relationships Between Med Errors, Potential ADEs and ADEs Medication Errors Pot ADEs Preventable ADEs Non- Preventable ADEs (ADRs) Institute for Safe Medication Practices Canada

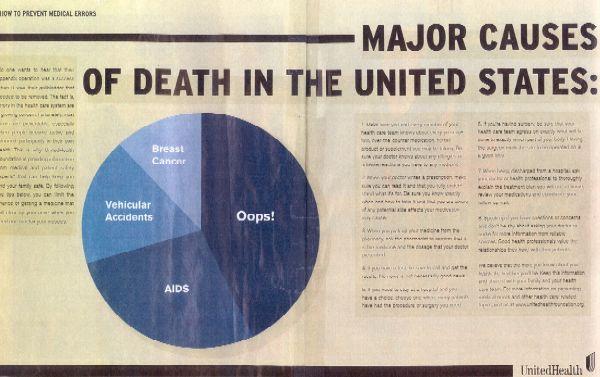
12 United States IOM (1999): To Err Is Human Hospital medical errors kill 44,000-98,000 people per year: More people die from medical errors each year than from suicides, highway accidents, breast cancer, or AIDS. These stunningly high rates of medical errors - resulting in deaths, permanent disability, and unnecessary suffering - are simply unacceptable in a system that promises to first do no harm. William Richardson 12 Institute for Safe Medication Practices Canada
13 Preventable medical mistakes cause more deaths per year than car accidents, breast cancer or AIDS 98,000 Deaths per Year 43,458 42,297 16,516 Preventable Medical Mistakes Car Accidents Breast Cancer AIDS Source: The Institute of Medicine: To Err is Human: Building a safer health system, Additional estimates from the Centres for Disease Control and Prevention, National Vital Statistics Reports, Vol. 47, No Institute for Safe Medication Practices Canada
14 Comparisons to Other Industries: What if we had 99.9% Accuracy? 2 unsafe landings at O Hare O Airport/ day 16,000 pieces of mail lost/ day 32,000 bank cheques deducted from the wrong account each HOUR! (Deming, 1987) 14 Institute for Safe Medication Practices Canada

15 15 Institute for Safe Medication Practices Canada
16 Incidence From Other Chart Review Studies Country Australia N Charts 14,000 Year 1995 Incidence of AE 16.6% Preventable? 51% USA (Utah( & Colorado) 15, % -- England % 50% New Zealand Denmark % 9.0% 71.8% 40.4% 16 Institute for Safe Medication Practices Canada




17 17 Institute for Safe Medication Practices Canada
18 Canadian Adverse Events Study Baker GR, Norton PG, Flintoft V, et al. CMAJ. 2004;170(1): Available online at Adverse Event an unintended injury or complication that results in disability at the time of discharge, death or prolonged hospital stay and that is caused by health care management rather than by the patient s s underlying disease process. (p.1679). 18 Institute for Safe Medication Practices Canada
19 Canadian Results 7.5% (or 187,500) patients in Canadian hospitals were seriously harmed by their care. As many as 9,250 to 23,750 people died in a Canadian hospital as a result of medical errors. 37% of adverse events were determined to be preventable. 19 Institute for Safe Medication Practices Canada
20 Related Adverse Events #1 Surgical = 34.2% #2 Medication and fluid-related = 23.6% 20 Institute for Safe Medication Practices Canada
21 Other Canadian Studies Forster AJ et al. Ottawa Hospital Patient Safety Study: incidence and timing of adverse events in patients admitted to a Canadian teaching hospital CMAJ 2004; 170(8): 1235 Forster AJ et al. Adverse events among medical patients after discharge from hospital. CMAJ 2004; 170(3): 345 Gurwitz JH et al. The incidence of adverse drug events in two large academic long-term care facilities. AMJ 2005; 118: Institute for Safe Medication Practices Canada
22 James Bagian, Anesthesiologist, space shuttle astronaut involved in the analysis of the Challenger explosion Just telling doctors and nurses to be more careful won t do much. We need to change the systems that allow errors to happen. Scientific America May 2000 New and analysis : Medicine 22 Institute for Safe Medication Practices Canada
23 Human Error Rates With Selected Activities Activity* General error of commission for example, misreading a label General error of omission in the absence of reminders General error of omission when items are embedded in a procedure for example, cash card is returned from cash machine before money is dispensed Simple arithmetic errors with self checking but without repeating the calculation on another sheet of paper Monitor or inspector fails to recognize an error Staff on different shifts fail to check hardware condition unless required by checklist or written directive General error rate given very high stress levels where dangerous activities are occurring rapidly * Unless otherwise indicated, assumes the activities are performed under no undue time pressures or stress. ** (# of errors / # of opportunities for the error) Rate of Human Error** 3/1000 1/100 3/1000 3/100 1/10 1/10 Adapted from Nolan TW. System changes to improve patient safety. BMJ 2000;320(7237): Nolan 23 Institute for Safe Medication Practices Canada 1/4
 Poorly Designed Order Forms Poorly Designed Drug Packaging Latent Failures 24 Institute for Safe Medication Practices")
24 Swiss Cheese Model Multiple Demands on Attention Barriers & Safeguards against Errors Poor Lighting Poorly Designed Storage facility Patient receives wrong drug Inadequate Training and Skills Mix (modified from James Reason, 1991) Poorly Designed Order Forms Poorly Designed Drug Packaging Latent Failures 24 Institute for Safe Medication Practices Canada
25 Making Health Care Safer Key steps: A. Recognize that improving safety is a priority B. Improve the reporting of errors and near misses C. Increase focus on system changes D. Gain greater knowledge about safer systems much already exists E. Leadership is needed on all levels G R Baker & P G Norton 25 Institute for Safe Medication Practices Canada
26 A. Recognize that Improving Safety National is a Priority CPSI: Safer Healthcare Now! Medication reconciliation Canadian Medication Incident Reporting and Prevention System (CMIRPS) Canadian Council on Health Services Accreditation (CCHSA) include patient safety goals Provincial (MOHLTC) ISMP Canada Medication Safety Support Service (KCl( KCl, Opioids, next anticoagulants) EMS / LTC / Community Pharmacy Patients (OHA) 26 Institute for Safe Medication Practices Canada
27 CCHSA Patient Safety Goals Culture Goal 1: Create a culture of safety within the organization Communication Goal 2: Improve the effectiveness and coordination among care/service providers and with the recipients of care/service across the continuum Medication Use Goal 3: Ensure the safe use of high risk medications Goal 4: Ensure the safe administration of parenteral medications 27 Institute for Safe Medication Practices Canada


28 B. Improve Reporting of Errors and Near Misses Reported Errors Errors NOT Reported 28 Institute for Safe Medication Practices Canada
29 Incident Reports As Safety Measures Method AE/1000 admissions Incident Reports 5 Retrospective Chart Review 30 Stimulated Voluntary Reports 30 Computer Flags 55 Daily chart review 85 Computer Flags and Daily review 130 Jha J Am Med Inf Assoc 1998;5:305 O'Neil Ann Int Med 1993;119: Institute for Safe Medication Practices Canada

30 Bulletin excerpt 30 Institute for Safe Medication Practices Canada

31 Canada: 3 reports 2 hospital 1 ambulance US: several reports 1 death Institute for Safe Medication Practices Canada

32 32 Institute for Safe Medication Practices Canada
33 33 Institute for Safe Medication Practices Canada

34 34 Institute for Safe Medication Practices Canada

35 35 Institute for Safe Medication Practices Canada
36 C. Increase the Focus on System Changes
37 Typical Medication Error Response I I should have read the label. This has not happened before. This is unlikely to happen again. Physician who reported a medication error 37 Institute for Safe Medication Practices Canada
38 Culture Change Need to dispel the belief that healthcare workers are or can be perfect 38 Institute for Safe Medication Practices Canada
39 High Alert Medications High-alert medications are drugs that bear a heightened risk of causing significant harm when they are used in error. From the ISMP Medication Safety Alert!, October 16, 2003, Survey on high-alert medications - Differences between nursing and pharmacy perspectives revealed 39 Institute for Safe Medication Practices Canada
40 Examples of High-Alert (Risk) Medications hypertonic IV solutions IV potassium (phosphate & chloride) all narcotic medications chemotherapeutic agents heparin & oral warfarin neuromuscular blocking agents insulin & oral hypoglycemics inotropic medication (e.g. digoxin) Institute for Safe Medication Practices Canada
41 Reality of Health Care Environments Cognitive overload Workloads Multitasking Interruptions Miscommunication Difficult technology 41 Institute for Safe Medication Practices Canada

42 42 Institute for Safe Medication Practices Canada

43 43 Institute for Safe Medication Practices Canada

44 44 Institute for Safe Medication Practices Canada
45 Confirmation Bias It leads one to see information that confirms our expectation rather than to see information that contradict our expectation. 45 Institute for Safe Medication Practices Canada
46 46 Institute for Safe Medication Practices Canada
47 The pweor of the hmuan mnid Aoccdrnig to a rscheearch at Cmabrigde Uinervtisy, it deosn't mttaer in what oredr the ltteers in a wrod are. The olny iprmoetnt tihng is taht the frist and lsat ltteer be at the rghit pclae. The rset can be a total mses and you can sitll raed it wouthit porbelm. Tihs is bcuseae the huamn mnid deos not raed ervey lteter by istlef, but the wrod as a wlohe. Amzanig huh? 47 Institute for Safe Medication Practices Canada
48 48 Institute for Safe Medication Practices Canada
49 49 Institute for Safe Medication Practices Canada
50 50 Institute for Safe Medication Practices Canada
51 51 Institute for Safe Medication Practices Canada

52 52 Institute for Safe Medication Practices Canada

53 53 Institute for Safe Medication Practices Canada

54 54 Institute for Safe Medication Practices Canada

55 55 Institute for Safe Medication Practices Canada

56 56 Institute for Safe Medication Practices Canada


57 57 Institute for Safe Medication Practices Canada

58 58 Institute for Safe Medication Practices Canada

59 59 Institute for Safe Medication Practices Canada
60 Medication Errors- a new way of thinking Who did it? Punishment Errors are rare Add more layers Calculating error rates What allowed it? Thank you! Errors are everywhere Simplify/standardize No thresholds 60 Institute for Safe Medication Practices Canada
61 D. Gain Greater Knowledge About Safer Systems 61 Institute for Safe Medication Practices Canada
62 Human Factors Engineering Research and practical applications designed to improve the interface of humans with systems Develops practical design principles that account for the psychological and physical characteristics of people 62 Institute for Safe Medication Practices Canada
63 Principles Reduce or eliminate the possibility of errors Make errors visible Minimize the consequences of errors 63 Institute for Safe Medication Practices Canada
64 Rank Order of Error Reduction Strategies 1. Forcing functions and constraints 2. Automation and computerization 3. Simplify, standardize and differentiate 4. Reminders, check lists and double check systems 5. Rules and policies 6. Education 7. Information 8. Punishment (no value) Institute for Safe Medication Practices Canada




65 Applying Error Reduction Strategies 1. Forcing functions and constraints 65 Institute for Safe Medication Practices Canada

66 Constraint: Hydromorphone 10 mg was removed 66 Institute for Safe Medication Practices Canada




67 Applying Error Reduction Strategies 2. Automation and Computerization: CPOE Bar Code technology Automated bedside verification Smart pumps 67 Institute for Safe Medication Practices Canada
68 Applying Error Reduction Strategies 3. Simplify, standardize and differentiate Bedrock Human Factors Principles o reduce steps and interfaces o Call 911 Standardize processes and procedures o Airline industry 68 Institute for Safe Medication Practices Canada

69 69 Institute for Safe Medication Practices Canada

70 70 Institute for Safe Medication Practices Canada

71 Standardization 71 Institute for Safe Medication Practices Canada
72 Standardize Order Communication Use leading zero (0.1 mg not.1 mg) No trailing zeros (1 mg not 1.0 mg) Avoid nonstandard abbreviations ( U ( for unit, q.d., drug name abbreviations such as MS ) Institute for Safe Medication Practices Canada
73 Differentiate vincristine vinblastine vincristine vinblastine 73 Institute for Safe Medication Practices Canada
74 Applying Error Reduction Strategies 4. Independent double checks & other redundancies 74 Institute for Safe Medication Practices Canada
75 Where Medication Errors Occur PRESCRIBING 39% of errors TRANSCRIPTION 12% of errors DISPENSING 11% of errors ADMINISTERING 38% of errors 75 Institute for Safe Medication Practices Canada
76 Independent Double Checks: Working Definition An Independent Double Check is a process in which a second practitioner conducts an individual verification. 76 Institute for Safe Medication Practices Canada

77 Independent Double Checks Common in other industries Acknowledges complex and high risk systems and that practitioners are human, and therefore fallible 77 Institute for Safe Medication Practices Canada
78 Independent Double Checks Research show that people find 95% of mistakes when double checking the work of others Grasha et al. Process and Delayed Verification Errors in Community Pharmacy. Tech Report Number (2001) Cognitive Systems Performance Lab 78 Institute for Safe Medication Practices Canada
79 It Reduces the Probability of Error 1 x 1 = , Institute for Safe Medication Practices Canada
80 Expectation of the 5 Rights Right drug Right patient Right dose Right route Right time These are desired outcomes but do not provide standardized process on how to achieve them 80 Institute for Safe Medication Practices Canada
81 Patient Safety MEASURING PATIENT SAFETY Interventions to PREVENT errors Medical Product Design (IV tubing, pumps, monitors, drug packaging & labels, medical records) Work Environment Design (Architecture, Work Station Design) Task or Process Design Interventions to MAKE ERRORS errors VISIBLE and REDUCE HARM Close Call Reporting Checks (auto or manual) 81 Institute for Safe Medication Practices Canada
82 Patient Safety MEASURING PATIENT SAFETY Interventions to PREVENT errors Interventions to MAKE ERRORS errors VISIBLE and REDUCE HARM Analyze & understand errors to develop Interventions Reporting Checks Prevent immediate harm 82 Institute for Safe Medication Practices Canada
83 Why do we need independent double checks? Front line staff work with: High Stress Environment High Risk Drugs Poorly designed Order Forms Poorly designed Packages & Labels! Poorly designed Pumps Human Factors 83 Institute for Safe Medication Practices Canada
84 The Physical & Cognitive 4 2 Sdjflsdjf sdfsadfsa Asdfsdfsdfsdf GHTYS AFKDJF SLDJFSDKJFKSF sfsdfsafaf ASLDJFL sdfsdf ALSJDF sdfsdf KJFSsf LJFasdfsDKlsdfk ASJlsjdflkjsdlkfjsd dfsdfsdfs sdfsdfsfd Saldfjsldkjflskdjf sldjflksjdf sldjf Sldjflsd skjsf lsjdf sf Sldkjflsdkjf dlsjf Lsdjflsdjf lsjflsjf fsfsjf d Sldjfldjf lsajdflkdsjflks djsdjsldfj Sldjfsdf jsldfj lksjfls df 1 3 World 2 QRSTUVWXYZ QRSTUVWXYZ ## MG/ML ## MG/##ML 1 ABCBCDEFGHIJ GRAPHICS TEXT TEXT TEXT TEXT TEXT TEXT TEXT GRAPHICS WARNING TEXT TEXT TEXT ABCDEFGHIJ TEXT TEXT TEXT TEXT ### MG FOR ORAL USE ONLY ### MG 3 4 ORDER FORM DRUG PACKAGE & LABELS 84 Institute for Safe Medication Practices Canada
85 Infusion Pumps 4 2 Drug Concentration PCA ORDER FORM Asdfsdfsdfsdf GrtytyTYS tydjf mvbnvytslhfgjfsdkjfksf ASdfhJFL sdfsdf sfsdfsafaf ALdhfyJDF sdfsdf cvbfssf LJFasdfsDKlsdfk ASdsjdflkjsdlkfjsd dfsdfsdfs sdfsdfsfd rtytrydfjsldkjflskdjf sldjflksjdf sldjf tryldjflsd skjsf lsjdf sf 1 Drug Name 3 Dose KEYHOLE EFFECT Rate rtyrtrtyldkjflsdkjf dlsjf Lsdjflsdjf lsjflsjf fsfsjf d rtyrtydjfldjf lsajdflkdsjflks djsdjsldfj tytyjfsdf jsldfj lksjfls df 5 Lockout 6 4 Hr Limit ORDER FORM INFUSION PUMP 85 Institute for Safe Medication Practices Canada


86 Looking Through the Keyhole Underlying Programming Sequence INFUSION PUMP 86 Institute for Safe Medication Practices Canada
87 Looking Through the Keyhole Poor Usability = Prone to Errors INFUSION PUMP 87 Institute for Safe Medication Practices Canada
88 ISMP Canada Medication Safety Support Service (MSSS) Supported MOHLTC This is an example of an existing PCA order form. This order form was NOT evaluated. Only the Independent Double Check CHECKLIST was evaluated in the usability test. 5. Rules and Policies bring to point of care Independent Double Check CHECKLIST Patient Name? Syringe Drug? Syringe Conc? Programmed Conc? Micro- or Milligram? Dose? Lockout? Four hour limit? signature Focus of usability test 88 Institute for Safe Medication Practices Canada
89 Independent Double Check CHECKLIST Patient Name? Syringe Drug? Syringe Conc? - Programmed Conc? Micro or Milligram? Dose? Lockout? Independent Double Check Tool Four hour limit? signature 89 Institute for Safe Medication Practices Canada
90 Applying Error Reduction Strategies Culture and Communication 6. Education and Information Educating staff: System-based causes of medication errors Hierarchy of effectiveness of error prevention strategies Bring patients and family into the medication-use process 90 Institute for Safe Medication Practices Canada
91 E. Leadership Needed Culture of Safety = FOUNDATION Making safety a priority (quality, outcomes) Eliminate use of error rates as a measurement tool Use of meaningful error tracking methods Proactive approach Failure Mode and Effects Analysis (FMEA) Learning from each other (internal, external, outside healthcare) High reliability organizations 91 Institute for Safe Medication Practices Canada
92 What Nurses Can Do? Cultivate a culture of safety Report errors/ near misses/ hazardous conditions Learn and talk about errors in your system Ensure orders are complete Authority gradient challenge Avoid use of dangerous abbreviations (telephone or verbal orders, MAR, PCP) Embrace patient/ family into process Cohen MR. Medication Errors. Causes, Prevention, and Risk Management; Institute for Safe Medication Practices Canada
93 What Nurses Can Do? Avoid work-a-rounds rounds Read- back orders (e.g., five zero ) Independent double checking Learn and apply system-based strategies Be vigilant Trust your intuition: if it doesn t t feel right, it probably isn t 93 Institute for Safe Medication Practices Canada
94 Technically the biggest safety system in healthcare is the minds and hearts of the workers who keep intercepting the flaws in the system and prevent patients from being hurt. They are the safety net, not the cause of injury. Don Berwick, IHI Institute for Safe Medication Practices Canada
Embracing a Culture of Safety and Learning
 Embracing a Culture of Safety and Learning Provincial Forum on Adverse Health Event Management St. John s Newfoundland May 26, 2008 Ward Flemons MD, FRCPC Vice-President, Health Outcomes Outline Adverse
Embracing a Culture of Safety and Learning Provincial Forum on Adverse Health Event Management St. John s Newfoundland May 26, 2008 Ward Flemons MD, FRCPC Vice-President, Health Outcomes Outline Adverse
Medication Safety in LTC. Objectives. About ISMP Canada
 Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Medication Safety in the Operating Room: Using the Operating Room Medication Safety Checklist
 Medication Safety in the Operating Room: Using the Operating Room Medication Safety Checklist CPSI Safe Surgery Saves Lives Workshop Montréal, QC 29Mar2011 Julie Greenall, RPh, BScPhm, MHSc, FISMPC Institute
Medication Safety in the Operating Room: Using the Operating Room Medication Safety Checklist CPSI Safe Surgery Saves Lives Workshop Montréal, QC 29Mar2011 Julie Greenall, RPh, BScPhm, MHSc, FISMPC Institute
Safe Medication Practices
 Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Human Factor and Patient Safety. Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA)
") Human Factor and Patient Safety Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA) Human Factors and Patient Safety Unforeseen ice problem caused
Human Factor and Patient Safety Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA) Human Factors and Patient Safety Unforeseen ice problem caused
Why is Critical Incident Reporting and Shared Learning Important for Patient Safety?
 Why is Critical Incident Reporting and Shared Learning Important for Patient Safety? Reporting on Critical Incidents Related to Medication / IV Fluid Ontario Hospital Association Video and Webcast Toronto,
Why is Critical Incident Reporting and Shared Learning Important for Patient Safety? Reporting on Critical Incidents Related to Medication / IV Fluid Ontario Hospital Association Video and Webcast Toronto,
Applying Human Factors to Healthcare Systems Safety
 April 29 th, 2014 To Better is Human TM Applying Human Factors to Healthcare Systems Safety A. Zach Hettinger, MD MS Medical Director National Center for Human Factors in Healthcare MedStar Institute for
April 29 th, 2014 To Better is Human TM Applying Human Factors to Healthcare Systems Safety A. Zach Hettinger, MD MS Medical Director National Center for Human Factors in Healthcare MedStar Institute for
TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation
 TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation Donna Woods, EdM, PhD Assistant Professor and Co Director, Graduate Programs In Healthcare Quality
TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation Donna Woods, EdM, PhD Assistant Professor and Co Director, Graduate Programs In Healthcare Quality
2017 Pharmacy Education Series
 2017 Pharmacy Education Series Featured Speaker: Christina Michalek, BS, RPh, FASHP Medication Safety Specialist Institute for Safe Medication Practices October 18, 2017 Improving Patient Safety: Preventing
2017 Pharmacy Education Series Featured Speaker: Christina Michalek, BS, RPh, FASHP Medication Safety Specialist Institute for Safe Medication Practices October 18, 2017 Improving Patient Safety: Preventing
Systems Thinking & Human Factors Engineering in Healthcare
 Clinical Networks and Streams and Managers John Hunter Hospital Newcastle, NSW; August 10, 2015 Systems Thinking & Human Factors Engineering in Healthcare Rollin J. (Terry) Fairbanks, MD, MS Director,
Clinical Networks and Streams and Managers John Hunter Hospital Newcastle, NSW; August 10, 2015 Systems Thinking & Human Factors Engineering in Healthcare Rollin J. (Terry) Fairbanks, MD, MS Director,
What s the data telling you? Using evidence-based stories for health planning and decision-making
 MANITOBA CENTRE FOR HEALTH POLICY What s the data telling you? Using evidence-based stories for health planning and decision-making Bayline RRT Meeting Randy Fransoo May 25, 2007 Manitoba Centre for Health
MANITOBA CENTRE FOR HEALTH POLICY What s the data telling you? Using evidence-based stories for health planning and decision-making Bayline RRT Meeting Randy Fransoo May 25, 2007 Manitoba Centre for Health
To prevent harm to patients from adverse medication events involving high-alert medications.
 TITLE MANAGEMENT OF HIGH-ALERT MEDICATIONS DOCUMENT # PS-46-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Management of High-alert Medications Policy APPROVAL LEVEL Alberta Health Services Executive
TITLE MANAGEMENT OF HIGH-ALERT MEDICATIONS DOCUMENT # PS-46-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Management of High-alert Medications Policy APPROVAL LEVEL Alberta Health Services Executive
MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY. April 2009 September 2012
 MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY April 2009 September 2012 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire des médicaments du
MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY April 2009 September 2012 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire des médicaments du
Objectives. Key Elements. ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management 5/20/2014
 ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
Medication Safety & Electrolyte Administration. Objectives. High Alert Medications. *Med Safety Electrolyte Administration
 Medication Safety & Electrolyte Administration Jennifer Doughty, PharmD PGY2 Pharmacy Resident Emergency Medicine Stormont Vail Health, Topeka, KS Objectives Define and identify high alert medications
Medication Safety & Electrolyte Administration Jennifer Doughty, PharmD PGY2 Pharmacy Resident Emergency Medicine Stormont Vail Health, Topeka, KS Objectives Define and identify high alert medications
SHRI GURU RAM RAI INSTITUTE OF TECHNOLOGY AND SCIENCE MEDICATION ERRORS
 MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Report on the. Results of the Medication Safety Self- Assessment for Long Term Care. Ontario s Long-Term Care Homes
 Report on the Results of the Medication Safety Self- Assessment for Long Term Care by Ontario s Long-Term Care Homes Report Submitted to: Ministry of Health And Long-Term Care Prepared by: ISMP Canada
Report on the Results of the Medication Safety Self- Assessment for Long Term Care by Ontario s Long-Term Care Homes Report Submitted to: Ministry of Health And Long-Term Care Prepared by: ISMP Canada
To describe the process for the management of an infusion pump involved in an adverse event or close call.
 TITLE INFUSION PUMPS FOR MEDICATION & PARENTERAL FLUID ADMINISTRATION SCOPE Provincial, Clinical DOCUMENT # PS-70-01 APPROVAL LEVEL Executive Leadership Team SPONSOR Provincial Medication Management Committee
TITLE INFUSION PUMPS FOR MEDICATION & PARENTERAL FLUID ADMINISTRATION SCOPE Provincial, Clinical DOCUMENT # PS-70-01 APPROVAL LEVEL Executive Leadership Team SPONSOR Provincial Medication Management Committee
Presentation to the Federal, Provincial and Territorial (FPT) Deputy Ministers of Health Meeting
 Deputy Ministers of Health Meeting") Presentation to the Federal, Provincial and Territorial (FPT) Deputy Ministers of Health Meeting Gatineau, Quebec June 10, 2011 (Amended for Project Web Page) Canadian Pharmaceutical Bar Coding Project
Presentation to the Federal, Provincial and Territorial (FPT) Deputy Ministers of Health Meeting Gatineau, Quebec June 10, 2011 (Amended for Project Web Page) Canadian Pharmaceutical Bar Coding Project
Reducing the risk of serious medication errors in community pharmacy practice
 Reducing the risk of serious medication errors in community pharmacy practice Eastern Medicaid Pharmacy Administrators Association (EMPAA) November 1, 2017 Newport, Rhode Island Michael R. Cohen, RPh,
Reducing the risk of serious medication errors in community pharmacy practice Eastern Medicaid Pharmacy Administrators Association (EMPAA) November 1, 2017 Newport, Rhode Island Michael R. Cohen, RPh,
A MEDICATION SAFETY ACTION PLAN. Produced September 2014
 We are not, as a country, doing enough to ensure the safe use of medications. Medicine, in all its forms, is the most common treatment in health care and it works miracles every day when it s used appropriately.
We are not, as a country, doing enough to ensure the safe use of medications. Medicine, in all its forms, is the most common treatment in health care and it works miracles every day when it s used appropriately.
(10+ years since IOM)
") Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
INQUEST INTO THE DEATH OF: MARIE TANNER
 INQUEST INTO THE DEATH OF: MARIE TANNER Details Name of Deceased: Marie Tanner Date of Death: January 21, 2002 Place of Death: Peterborough Regional Health Centre Cause of Death: Cardiac Arrest Caused
INQUEST INTO THE DEATH OF: MARIE TANNER Details Name of Deceased: Marie Tanner Date of Death: January 21, 2002 Place of Death: Peterborough Regional Health Centre Cause of Death: Cardiac Arrest Caused
Policy Statement Medication Order Legibility Medication orders will be written in a manner that provides a clearly legible prescription.
 POLICY POLICY PURPOSE: The purpose of this policy is to provide a foundation for safe communication of medication and nutritional orders in-scope, thereby reducing the potential for preventable medication
POLICY POLICY PURPOSE: The purpose of this policy is to provide a foundation for safe communication of medication and nutritional orders in-scope, thereby reducing the potential for preventable medication
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Improving Staff Education
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Improving Staff Education
Medication Safety Way Beyond the 5 Rights
 Safety Way Beyond the 5 Rights JoAnne Phillips, MSN, RN, CCRN, CCNS, CPPS The University of Pennsylvania Health System Philadelphia, PA Current State. Of Chaos Prescriptions 12 per /person / year 4 BILLION
Safety Way Beyond the 5 Rights JoAnne Phillips, MSN, RN, CCRN, CCNS, CPPS The University of Pennsylvania Health System Philadelphia, PA Current State. Of Chaos Prescriptions 12 per /person / year 4 BILLION
Required Organizational Practices Resources for 2016
 Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Never Events in Healthcare
 Never Events in Healthcare Raising awareness to protect patients from serious harm or death September 11, 2015 The 4 th International Medication Safety Summit Conference Beijing, China Lindsay Yoo, BScPhm,
Never Events in Healthcare Raising awareness to protect patients from serious harm or death September 11, 2015 The 4 th International Medication Safety Summit Conference Beijing, China Lindsay Yoo, BScPhm,
Example of a Health Care Failure Mode and Effects Analysis for IV Patient Controlled Analgesia (PCA) Failure Modes (what might happen)
 Failure Modes (what might happen)") Prescribing Assess patient Choose analgesic/mode of delivery Prescribe analgesic Institute for Safe Medication Practices Example of a Health Care and Effects Analysis for IV Patient Controlled Analgesia
Prescribing Assess patient Choose analgesic/mode of delivery Prescribe analgesic Institute for Safe Medication Practices Example of a Health Care and Effects Analysis for IV Patient Controlled Analgesia
Nurse Orientation. Medication Management
 Nurse Orientation Medication Management Objectives Discuss basic principles/rights of medication administration, according to your site policy Describe principles of patient/family education related to
Nurse Orientation Medication Management Objectives Discuss basic principles/rights of medication administration, according to your site policy Describe principles of patient/family education related to
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow
 The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
Disclosure. Institute of Medicine (IOM) 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL
 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL") Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
Re-Engineering Medication Processes to Capitalize on Technology. Jane Englebright, PhD, RN Vice President, Quality HCA
 Re-Engineering Medication Processes to Capitalize on Technology Jane Englebright, PhD, RN Vice President, Quality HCA Who is HCA? % % % % U.K. % % % Switzerland % %% % % % % % %% % % % % % % % %% % % %
Re-Engineering Medication Processes to Capitalize on Technology Jane Englebright, PhD, RN Vice President, Quality HCA Who is HCA? % % % % U.K. % % % Switzerland % %% % % % % % %% % % % % % % % %% % % %
Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003
 Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003 Susan M. Proulx, Pharm.D. President, Med-E.R.R.S. Subsidiary of ISMP (www.med-errs.com) Mission of ISMP Translate errors into education
Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003 Susan M. Proulx, Pharm.D. President, Med-E.R.R.S. Subsidiary of ISMP (www.med-errs.com) Mission of ISMP Translate errors into education
Medication Safety Technology The Good, the Bad and the Unintended Consequences
 Medication Safety Technology The Good, the Bad and the Unintended Consequences Michelle Mandrack RN, MSN Director of Consulting Services Matthew Fricker, RPh, MS Program Director 1 Objectives Consider
Medication Safety Technology The Good, the Bad and the Unintended Consequences Michelle Mandrack RN, MSN Director of Consulting Services Matthew Fricker, RPh, MS Program Director 1 Objectives Consider
Medication errors and patient safety: tools for system improvement
 Medication errors and patient safety: tools for system improvement PHM 301 Julie Greenall ISMP Canada 2013 Institute for Safe Medication Practices Canada (ISMP Canada) 2013 Institute for Safe Medication
Medication errors and patient safety: tools for system improvement PHM 301 Julie Greenall ISMP Canada 2013 Institute for Safe Medication Practices Canada (ISMP Canada) 2013 Institute for Safe Medication
Ontario Hospital Critical Incidents Related to Medications or IV Fluids Analysis Report. October 2011 to December 2012
 Ontario Hospital Critical Incidents Related to Medications or IV Fluids Analysis Report October 2011 to December 2012 Submitted to the Ontario Ministry of Health and Long-Term Care and Health Quality Ontario
Ontario Hospital Critical Incidents Related to Medications or IV Fluids Analysis Report October 2011 to December 2012 Submitted to the Ontario Ministry of Health and Long-Term Care and Health Quality Ontario
Innovative Techniques for Residents to Improve Safety
 Innovative Techniques for Residents to Improve Safety Eugene Terry, MD Modified from Tammy Lundsrum,MD www.mihealthandsafety.org/presentations/lundstrom.ppt What is a Safety Culture And how is it achieved?
Innovative Techniques for Residents to Improve Safety Eugene Terry, MD Modified from Tammy Lundsrum,MD www.mihealthandsafety.org/presentations/lundstrom.ppt What is a Safety Culture And how is it achieved?
Breakfast With the Chiefs December 15, 2005 Philip Hassen, CEO, CPSI
 Reflections: Ten Months and Where to From Here Breakfast With the Chiefs December 15, 2005 Philip Hassen, CEO, CPSI 1 Presentation Overview Nature of the Problem Safer Healthcare Now Campaign Systems vs.
Reflections: Ten Months and Where to From Here Breakfast With the Chiefs December 15, 2005 Philip Hassen, CEO, CPSI 1 Presentation Overview Nature of the Problem Safer Healthcare Now Campaign Systems vs.
PURPOSE To establish a standardized process for the activity of an independent double check for medication administration.
 PURPOSE To establish a standardized process for the activity of an independent double check for medication administration. POLICY STATEMENTS Health Care Providers will complete the independent double check
PURPOSE To establish a standardized process for the activity of an independent double check for medication administration. POLICY STATEMENTS Health Care Providers will complete the independent double check
Alaris Products. Protecting patients at the point of care
 Alaris Products Protecting patients at the point of care Overview The medication process is the largest source of medical errors 1 with medication errors costing an estimated $3.5 billion yearly in hospitals.
Alaris Products Protecting patients at the point of care Overview The medication process is the largest source of medical errors 1 with medication errors costing an estimated $3.5 billion yearly in hospitals.
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA
 Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Quality Improvement Overview. Paul vanostenberg, DDS. MS Vice President Accreditation and Standards Joint Commission International
 Quality Improvement Overview Paul vanostenberg, DDS. MS Vice President Accreditation and Standards Joint Commission International The History of Improving We are perfect! Get rid of the bad apples! System
Quality Improvement Overview Paul vanostenberg, DDS. MS Vice President Accreditation and Standards Joint Commission International The History of Improving We are perfect! Get rid of the bad apples! System
Anatomy of a Fatal Medication Error
 Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Objectives. Demographics: Type and Services 1/22/2014. ICAHN Aggregate Results. ISMP Medication Safety Self Assessment for Hospitals
 ICAHN Aggregate Results ISMP Medication Safety Self Assessment for Hospitals Matthew Fricker, RPH, MS, FASHP Rebecca Lamis, PharmD, FISMP January 23, 2014 1 Objectives Report the demographic characteristics
ICAHN Aggregate Results ISMP Medication Safety Self Assessment for Hospitals Matthew Fricker, RPH, MS, FASHP Rebecca Lamis, PharmD, FISMP January 23, 2014 1 Objectives Report the demographic characteristics
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Advancing Medication Safety in the Delivery of High Alert Medications in Paediatrics. Table of Contents
 Table of Contents Acknowledgements CAPHC ISMP Canada National Advisory Committee CAPHC Member Organizations Participating in the Project Executive Summary iv iv v vi vii viii 1. Introduction 1 2. First
Table of Contents Acknowledgements CAPHC ISMP Canada National Advisory Committee CAPHC Member Organizations Participating in the Project Executive Summary iv iv v vi vii viii 1. Introduction 1 2. First
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Required Organizational Practices. September 2011
 s September 2011 CONTENTS OVERVIEW...1 ABOUT THE ROP HANDBOOK...2 SAFETY CULTURE Adverse events disclosure...3 Adverse events reporting...4 Client safety as a strategic priority...5 Client safety quarterly
s September 2011 CONTENTS OVERVIEW...1 ABOUT THE ROP HANDBOOK...2 SAFETY CULTURE Adverse events disclosure...3 Adverse events reporting...4 Client safety as a strategic priority...5 Client safety quarterly
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN
 Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Disclosures. Medication Incident. Objectives 4/23/2015. No conflicts to disclose
 Disclosures No conflicts to disclose Kara Browne Senior Pharmacy Technician Saskatoon Cancer Centre Objectives Overview of common medication incidents and their causes Overview of available pharmacy technology
Disclosures No conflicts to disclose Kara Browne Senior Pharmacy Technician Saskatoon Cancer Centre Objectives Overview of common medication incidents and their causes Overview of available pharmacy technology
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Culture of Safety: What s in Your Toolbox?
 Culture of Safety: What s in Your Toolbox? Kathy Ghomeshi, PharmD, BCPS Medication Safety Specialist Victoria Serrano Adams, PharmD, FASHP, FCSHP Director of Pharmaceutical Services UCSF Medical Center
Culture of Safety: What s in Your Toolbox? Kathy Ghomeshi, PharmD, BCPS Medication Safety Specialist Victoria Serrano Adams, PharmD, FASHP, FCSHP Director of Pharmaceutical Services UCSF Medical Center
Overview. Diane Cousins, R.Ph U.S. Pharmacopeia. 1 Pharmacy Labeling with Color
 As more medications are approved and become available to Americans, the opportunity for potentially dangerous or even deadly errors due to drug mix-ups from look alike or sound alike names becomes increasingly
As more medications are approved and become available to Americans, the opportunity for potentially dangerous or even deadly errors due to drug mix-ups from look alike or sound alike names becomes increasingly
Constant Pursuit of Medication Safety. Geraldine Koh Chief Pharmacist
 Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use
 Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use Our vision is to create a culture where patients and those who care for them are
Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use Our vision is to create a culture where patients and those who care for them are
Using MEDMARX for Reporting and Benchmarking. Anne Skinner, RHIA Katherine Jones, PhD, PT
 Using MEDMARX for Reporting and Benchmarking Anne Skinner, RHIA Katherine Jones, PhD, PT Purpose of the Grant: Assist small rural hospitals to Voluntarily report and analyze medication errors Identify
Using MEDMARX for Reporting and Benchmarking Anne Skinner, RHIA Katherine Jones, PhD, PT Purpose of the Grant: Assist small rural hospitals to Voluntarily report and analyze medication errors Identify
Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses
 Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses March 2018 College of Licensed Practical Nurses of Nova Scotia http://clpnns.ca Starlite Gallery, 302-7071 Bayers Road,
Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses March 2018 College of Licensed Practical Nurses of Nova Scotia http://clpnns.ca Starlite Gallery, 302-7071 Bayers Road,
Human Factors. Frank Federico, RPh. This presenter has nothing to disclose.
 Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration
 One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration Presented by: Marla Husch Northwestern Memorial Hospital Northwestern Memorial Hospital Chicago, Illinois
One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration Presented by: Marla Husch Northwestern Memorial Hospital Northwestern Memorial Hospital Chicago, Illinois
During Robert s hospitalization
 Nursing Student Medication Errors: A Retrospective Review Lorill Harding, MA, RN; and Teresa Petrick, MN, RN ABSTRACT This article presents the findings of a retrospective review of medication errors made
Nursing Student Medication Errors: A Retrospective Review Lorill Harding, MA, RN; and Teresa Petrick, MN, RN ABSTRACT This article presents the findings of a retrospective review of medication errors made
Medication Error Reporting Systems: Problems and Solutions
 1112-NM 1-2 November NEW 9/11/01 11:23 am Page 61 Medication Error Reporting Systems: Problems and Solutions David U, President and CEO, Institute for Safe Medication Practices, Ontario, Canada Reform
1112-NM 1-2 November NEW 9/11/01 11:23 am Page 61 Medication Error Reporting Systems: Problems and Solutions David U, President and CEO, Institute for Safe Medication Practices, Ontario, Canada Reform
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009
 The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
Considerations for Sterile Compounding of Parenteral Products for Pediatric Use: Part 2 PharMEDium Lunch and Learn Series LUNCH AND LEARN
 LUNCH AND LEARN Considerations for Sterile Compounding of Parenteral Products for Pediatric Use: Part 2 November 10, 2017 Featured Speaker: Kirsten H. Ohler, PharmD, BCPS, BCPPS Neonatal / Pediatric Clinical
LUNCH AND LEARN Considerations for Sterile Compounding of Parenteral Products for Pediatric Use: Part 2 November 10, 2017 Featured Speaker: Kirsten H. Ohler, PharmD, BCPS, BCPPS Neonatal / Pediatric Clinical
student interests. The 1. Develop of error schema. develop
 Sample Medication Safety APPE Student Rotation Rotation Description The medication safety rotation willl help students become familiar with the key principles utilized in hospitals and health systems to
Sample Medication Safety APPE Student Rotation Rotation Description The medication safety rotation willl help students become familiar with the key principles utilized in hospitals and health systems to
Human Factors and Ergonomics in Health Care and Patient Safety
 Human Factors and Ergonomics in Health Care and Patient Safety Pascale Carayon, Ph.D. Procter & Gamble Bascom Professor in Total Quality Department of Industrial and Systems Engineering Director of the
Human Factors and Ergonomics in Health Care and Patient Safety Pascale Carayon, Ph.D. Procter & Gamble Bascom Professor in Total Quality Department of Industrial and Systems Engineering Director of the
To establish a consistent process for the activity of an independent double-check prior to medication administration, where appropriate.
 TITLE INDEPENDENT DOUBLE-CHECK SCOPE Provincial, Clinical DOCUMENT # PS-60-01 APPROVAL LEVEL Senior Operating Officer, Pharmacy Services SPONSOR Provincial Medication Management Committee CATEGORY Patient
TITLE INDEPENDENT DOUBLE-CHECK SCOPE Provincial, Clinical DOCUMENT # PS-60-01 APPROVAL LEVEL Senior Operating Officer, Pharmacy Services SPONSOR Provincial Medication Management Committee CATEGORY Patient
Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals
 Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals John M. Kessler, B.S. Pharm., Pharm. D. Steve C. Dedrick, MS Pharm. NCCMedS Project Directors
Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals John M. Kessler, B.S. Pharm., Pharm. D. Steve C. Dedrick, MS Pharm. NCCMedS Project Directors
PATIENT CARE MANUAL PROCEDURE
 PATIENT CARE MANUAL PROCEDURE NUMBER III-130 PAGE 1 OF 5 APPROVED BY: CATEGORY: Vice President and Senior Operating Officer, Rural Health Services & Professional Practice Lead Medication Administration
PATIENT CARE MANUAL PROCEDURE NUMBER III-130 PAGE 1 OF 5 APPROVED BY: CATEGORY: Vice President and Senior Operating Officer, Rural Health Services & Professional Practice Lead Medication Administration
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE MEDICATION ORDERS SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Provincial Medication Management Committee PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
TITLE MEDICATION ORDERS SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Provincial Medication Management Committee PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
3/9/2010. Objectives. Pharmacist Role in Medication Safety and Regulatory Compliance
 Pharmacist Role in Medication Safety and Regulatory Compliance Janet Greiwe Vice President, Systems Management Cleveland County Health System Objectives By the end of this presentation, you should be able
Pharmacist Role in Medication Safety and Regulatory Compliance Janet Greiwe Vice President, Systems Management Cleveland County Health System Objectives By the end of this presentation, you should be able
Recommendations from National Patient Safety Agency alerts that remain relevant to the Never Events list 2018
 Recommendations from National Patient Safety Agency alerts that remain relevant to the Never Events list 2018 January 2018 We support providers to give patients safe, high quality, compassionate care within
Recommendations from National Patient Safety Agency alerts that remain relevant to the Never Events list 2018 January 2018 We support providers to give patients safe, high quality, compassionate care within
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE)
") COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
MEDICATION ASSISTANCE GUIDELINES: TEACHING PLAN
 MEDICATION ASSISTANCE GUIDELINES: TEACHING PLAN Lesson Overview Time: One Hour This lesson covers basic guidelines for assisting residents with their medications. Learning Goals At the end of this session,
MEDICATION ASSISTANCE GUIDELINES: TEACHING PLAN Lesson Overview Time: One Hour This lesson covers basic guidelines for assisting residents with their medications. Learning Goals At the end of this session,
How BPOC Reduces Bedside Medication Errors White Paper
 How BPOC Reduces Bedside Medication Errors White Paper July 2008 Brad Blackwell, M.S., R.Ph. Eloise Keeler, R.N., B.S.N. Abstract Medication errors are a significant source of harm to patients in U.S hospitals,
How BPOC Reduces Bedside Medication Errors White Paper July 2008 Brad Blackwell, M.S., R.Ph. Eloise Keeler, R.N., B.S.N. Abstract Medication errors are a significant source of harm to patients in U.S hospitals,
National Patient Safety Goals from The Joint Commission
 National Patient Safety Goals from The Joint Commission Objectives After completion of this module, participants will be able to: List at least five National Patient Safety Goals that are required in a
National Patient Safety Goals from The Joint Commission Objectives After completion of this module, participants will be able to: List at least five National Patient Safety Goals that are required in a
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU. Change Package.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Session Objectives. Medication Errors in Adults and Children. Dennis Quaid American Society of Health- System Pharmacists (ASHP) Meeting December 2009
 Meeting December 2009") Medication Errors in Adults and Children Carly C. Feldott, PharmD Medication Safety Program Director, VUMC Amy L. Potts, PharmD, BCPS Assistant Director, Monroe Carell, Jr. Children s Hospital at Vanderbilt
Medication Errors in Adults and Children Carly C. Feldott, PharmD Medication Safety Program Director, VUMC Amy L. Potts, PharmD, BCPS Assistant Director, Monroe Carell, Jr. Children s Hospital at Vanderbilt
A Collaborative Failure Mode and Effects Analysis Project with an Ontario Hospital:
 M< A Collaborative Failure Mode and Effects Analysis Project with an Ontario Hospital: Reducing the Risk of Inadvertent Injection of Concentrated Epinephrine Intended for Topical Use March 2011 Revised
M< A Collaborative Failure Mode and Effects Analysis Project with an Ontario Hospital: Reducing the Risk of Inadvertent Injection of Concentrated Epinephrine Intended for Topical Use March 2011 Revised
Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016
 Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016 DISCLOSURE STATEMENT I have nothing to disclose regarding
Medication Errors in Chemotherapy PORSCHA L. JOHNSON, PHARM.D. CLINICAL PHARMACIST II MEDSTAR WASHINGTON HOSPITAL CENTER SATURDAY, SEPTEMBER 17, 2016 DISCLOSURE STATEMENT I have nothing to disclose regarding
Anne Huben-Kearney, RN, BSN, MPA, CPHQ, CPHRM Assistant Vice President, Healthcare Risk Management AWAC Services, a member company of Allied World
 Slide 1 Human Factors: The Science of Reliability MSHRM February 2015 Anne Huben-Kearney, RN, BSN, MPA, CPHQ, CPHRM Assistant Vice President, Healthcare Risk Management AWAC Services, a member company
Slide 1 Human Factors: The Science of Reliability MSHRM February 2015 Anne Huben-Kearney, RN, BSN, MPA, CPHQ, CPHRM Assistant Vice President, Healthcare Risk Management AWAC Services, a member company
WHAT are medication errors?
 Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Improving Safety Practices Anticoagulation Therapy
 Improving Safety Practices Anticoagulation Therapy Katie Cinnamon, PharmD, BCPS Clinical Pharmacist Genesis Medical Center - Davenport Objectives Review background information on medication errors and
Improving Safety Practices Anticoagulation Therapy Katie Cinnamon, PharmD, BCPS Clinical Pharmacist Genesis Medical Center - Davenport Objectives Review background information on medication errors and
Running head: MEDICATION ERRORS 1. Medications Errors and Their Impact on Nurses. Kristi R. Rittenhouse. Kent State University College of Nursing
 Running head: MEDICATION ERRORS 1 Medications Errors and Their Impact on Nurses Kristi R. Rittenhouse Kent State University College of Nursing MEDICATION ERRORS 2 Abstract One in five medication dosages
Running head: MEDICATION ERRORS 1 Medications Errors and Their Impact on Nurses Kristi R. Rittenhouse Kent State University College of Nursing MEDICATION ERRORS 2 Abstract One in five medication dosages
Shifting from Blame-&-Shame to a Just-and-Safe Culture
 Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Overview. Improving Safety with Health Information Technology. Prioritizing Safety. Question 22/10/2013
 Improving Safety with Health Information Technology ISQua 2013, Edinburgh David Bates, MD, MSc Chief Quality Officer, Chief, Division of General Internal Medicine, Brigham and Women s Hospital Medical
Improving Safety with Health Information Technology ISQua 2013, Edinburgh David Bates, MD, MSc Chief Quality Officer, Chief, Division of General Internal Medicine, Brigham and Women s Hospital Medical
POLICY. Clinician is any health care professional accepting responsibility for care of patients and their medications.
 POLICY Number: 7311-60-020 Title: HIGH ALERT MEDICATIONS IDENTIFICATION, DOUBLE CHECK AND LABELING Authorization [ ] President and CEO [X ] Vice President, Finance and Corporate Services Source: Chair,
POLICY Number: 7311-60-020 Title: HIGH ALERT MEDICATIONS IDENTIFICATION, DOUBLE CHECK AND LABELING Authorization [ ] President and CEO [X ] Vice President, Finance and Corporate Services Source: Chair,
The Joint Commission Medication Management Update for 2010
 Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS
 PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS Active Error An error that occurs at the point of contact. Active errors are generally readily apparent (e.g., pushing an incorrect button, ignoring
PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS Active Error An error that occurs at the point of contact. Active errors are generally readily apparent (e.g., pushing an incorrect button, ignoring
Objectives MEDICATION SAFETY & TECHNOLOGY. Disclosure. How has technology improved the way we dispense and compound medications AdminRx AcuDose Rx
 MEDICATION SAFETY & TECHNOLOGY Objectives Identify technology that can improve medication safety and decrease medication errors Identify ways that technology can cause medication errors if used inappropriately
MEDICATION SAFETY & TECHNOLOGY Objectives Identify technology that can improve medication safety and decrease medication errors Identify ways that technology can cause medication errors if used inappropriately
Long Term Care Initiatives in Ontario. Kris Wichman Project Leader LTC June 2005
 Long Term Care Initiatives in Ontario Kris Wichman Project Leader LTC June 2005 Support Ministry of Health and Long Term Care of Ontario provided funding for ISMP Canada projects Fall 2004, scope expanded
Long Term Care Initiatives in Ontario Kris Wichman Project Leader LTC June 2005 Support Ministry of Health and Long Term Care of Ontario provided funding for ISMP Canada projects Fall 2004, scope expanded
N ATIONAL Q UALITY F ORUM. Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT
 N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
Medication Reconciliation Bundle of Care. Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013
 Medication Reconciliation Bundle of Care Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013 Overview Problem of medication errors at transitions of care Who is at risk Recognition as a patient
Medication Reconciliation Bundle of Care Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013 Overview Problem of medication errors at transitions of care Who is at risk Recognition as a patient
Preventing Adverse Drug Events and Harm
 Preventing Adverse Drug Events and Harm Frank Federico, RPh, IHI Executive Director Steve Meisel, PharmD, IHI Faculty March 27th,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH, Institute
Preventing Adverse Drug Events and Harm Frank Federico, RPh, IHI Executive Director Steve Meisel, PharmD, IHI Faculty March 27th,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH, Institute
Most of you flew to this meeting
 Most of you flew to this meeting on an airplane and, like me, ignored the flight attendant asking you to pay attention and listen to a few safety warnings that were being offered. In spite of having listened,
Most of you flew to this meeting on an airplane and, like me, ignored the flight attendant asking you to pay attention and listen to a few safety warnings that were being offered. In spite of having listened,
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
University of Mississippi Medical Center University of Mississippi Health Care. Pharmacy and Therapeutics Committee Medication Use Evaluation
 University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
Case Study from Parallon
 Case Study from Parallon Improving Compliance with the Smart Pump drug library across a large hospital system Part 2 Monday, July 10, 2017 AAMI Foundation Vision: To drive the safe adoption and safe use
Case Study from Parallon Improving Compliance with the Smart Pump drug library across a large hospital system Part 2 Monday, July 10, 2017 AAMI Foundation Vision: To drive the safe adoption and safe use