Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN
|
|
|
- Stuart Pearson
- 5 years ago
- Views:
Transcription
1 Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN
2 Fairview Health Services 6 hospitals, ranging from rural to academic 50+ primary care clinics Home care/hospice, home infusion, long term care, retail pharmacy, PBM 20,000 employees, 3,000 physicians 73,000 annual admissions; 175,000 ED visits; 1 million clinic visits $3 billion gross revenue > 8,000,000 annual inpatient doses dispensed 1.7 million annual retail pharmacy prescriptions
3 Disclaimer
4 What is medication safety?
5 What is medication safety? Absence of errors Absence of adverse events as measured by? Absence of preventable adverse events Absence of reportable events Adherence to guidelines/standards Adherence to NPSG Positive cultural surveys Good responses to self-assessment surveys (ISMP, Leapfrog)?
6 What is safety? Safety is a condition defined by the perception of the customer (patient). Safety is not synonymous with the absence of risk or adverse events. Instead it is marked by the knowledge and comfort that all efforts are being made to prevent everything we know how to prevent and that we are striving to make things even better. Aviation, automobile, nuclear power Error reduction, adherence to guidelines, etc are tactics, not strategies

7 Harm vs. Error
8 Fairview s ADE Measurement System 100% real-time review of triggers for harm from high hazard drugs: Naloxone use (narcotics) Flumazenil use (sedatives) Blood sugar <40 mg/dl (antidiabetic agents) INR >5 (warfarin)* PTT >200; anti-xa level > 1.6 (heparin) prothrombin complex concentrate and coagulation factor VIIa (rivaroxaban and dabigatran) * Threshold of 6 until 2Q 2012
9 Anticoagulation Review Criteria A legitimate screen. Example: a bedside PTT reading of 215 seconds but a subsequent laboratory analysis was 135 seconds. In these cases, the record is coded as artifact and no further action would be taken. If the screen is determined to be legitimate, was it associated with an anti-coagulant? Example: An INR of 7 relating to liver disease or malnutrition. In these cases, the record is coded as no adverse drug event.
10 Anticoagulation Review Criteria If the high INR or PTT or antidote was associated with the use of an anticoagulant and there was clinical intervention, an ADE has occurred. Simply modifying or holding the dose is NOT a clinical intervention The use of an antidote automatically mean that an adverse event occurred. Exception: planned reversals such as prior to surgery Warfarin-related bleeding resulting from outpatient services do NOT count as an ADE it is related to a prior hospital discharge.
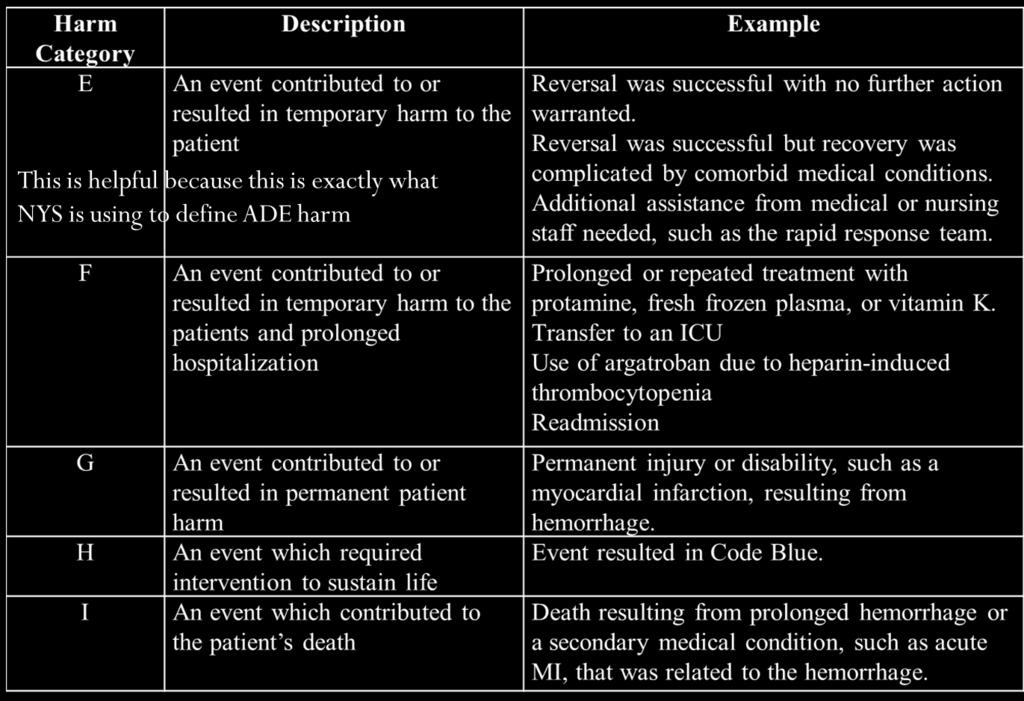
11 Anticoagulation Harm Ratings
12 ADE Gap Analysis Anticoagulants Courtesy of the Minnesota Hospital Association Hospital Engagement Network
13 1. Antithrombotic management practices 1a) Responsibility is assigned for coordinating anticoagulation monitoring functions. A process exists to ensure fields contained in standard protocols/order sets/ flowsheets are consistently populated (manually or automatically) with key information, including at a minimum: 1b) The patient s diagnosis 1c) Allergies 1d) Most recent pertinent laboratory results
14 1. Antithrombotic management practices Standard policies & practices exist for managing the initiation and maintenance of anticoagulation therapy which include: 1e) The specific medication used (e.g., low molecular weight heparin (LMWH), warfarin, unfractionated heparin (UFH), Vitamin K reversal, direct thrombin inhibitors) 1f) The condition being treated 1g) The potential for drug interactions
15 1. Antithrombotic management practices 1h) A protocol exists to determine the need to reverse supratherapeutic INR values based on key criteria, (e.g., the INR value, the presence or absence of bleeding, individual patient situation, e.g., imminent surgery). 1i) A process exists to ensure that anti-platelet agents are used for the appropriate indication (e.g., patients with mechanical valves, acute coronary syndrome or recent stent or bypass surgery.)
16 1. Antithrombotic management practices Vitamin K practice specifies (in patients with no evidence of warfarin associated bleeding): 1j) No routine use of Vitamin K for INR between k) The use of oral Vitamin K for INR >10. In patients with warfarin associated major bleeding: 1l) Reversal may be accomplished with the addition of Vitamin K 5-10 mg given slow IV infusion. 1m) Reversal may also be accomplished with prothrombin complex concentrate and the addition of Vitamin K 5-10 mg given slow IV infusion.
17 2. Prevention & mitigation practices (all) 2a) Antithrombotics are included in the defined list of high alert medications. 2b) Practitioners are alerted to significant drug interactions for patients on antithrombotic agents. 2c) Prescribers are reminded to evaluate the need for antithrombotic therapy when antithrombotics are being held for future surgical purposes. 2d) A pharmacy managed system exists for antithrombotic drug shortage situations which outlines how standard medication safety processes will be followed.
18 2. Prevention & mitigation practices (all) 2e) IV antithrombotic orders cannot be entered into the pharmacy and order entry systems without including patient weight. Smart infusion pumps are used for the IV administration of all antithrombotics (including platelet inhibitors), with functionality employed to: 2f) Intercept and prevent wrong dose errors. 2g) Intercept and prevent wrong infusion rate errors.
19 3. Therapeutic practices (all) A process exists, using a standardized tool, to address and document the following prior to initiating antithrombotic therapy: 3a) Nutritional status 3b) Recent trauma 3c) Surgery 3d) Bleeding problems experienced while receiving any previous antithrombotic therapy 3e) Clotting history 3f) Drug/drug interactions 3g) Pharmacists assist with identification of alternative antithrombotic agents when contraindications exist.
20 3. Therapeutic practices (all) 3h) The indication and therapeutic goal for antithrombotic therapy is documented in the medical record and communicated to pharmacy for monitoring and managing patient therapy. Processes exists for timely access to routine test results which include: 3i) INR, PTT and anti-xa level available within 2 hours. 3j) Health care providers can readily access inpatient and outpatient laboratory results to guide antithrombotic therapy. 3k) When an antithrombotic agent is administered in the ED or other outpatient settings (e.g., cardiac cath lab, radiology), the inpatient medication record and chart is updated to communicate this information to other practitioners.
21 3. Therapeutic practices (all) For critical test results reporting, the facility has defined acceptable lengths of time between: 3l) Ordering critical hematologic tests (e.g., INR, PPT) and reporting of the test results. 3m) The availability of the results and confirmation of receipt by a health care provider. 3n) The receipt of results by a health care provider and clinically appropriate antithrombotic dose changes
22 4, Warfarin management practices Standard processes exist for initiation of warfarin therapy and daily dosing, which include: 4a) Collection of baseline lab values prior to prescribing anticoagulant. (e.g. warfarin-naïve patient (30 days prior), warfarin maintenance patient (24 hr prior). 4b) The INR is the primary laboratory test used to monitor and adjust warfarin therapy. 4c) Nutritional assessment 4d) Drug/drug interactions 4e) Lab values 4f) History of thrombosis or bleeding event 4g) Recent trauma or surgery
23 4, Warfarin management practices 4h) Ability to adjust INR target range for clinical indication. 4i) Screening for interactions between enteral nutrition products and antithrombotic therapy. (e.g., drug/tube feed interactions.) 4j) Obtaining blood draws for INR at the same time each day. 4k) Administering warfarin at the same time each day after INR results are available (e.g., afternoon / evening) 4l) Warfarin is started on Day 1 or 2 of LMWH or UFH therapy initiation.
24 4, Warfarin management practices 4m) Pharmacists can automatically modify warfarin therapy doses or directly contact the prescriber when laboratory values are below or above approved target ranges. 4n) When warfarin therapy is initiated for a patient with active thrombosis, heparin or LMWH is continued until warfarin has been administered for a minimum of 5 (five) days and the INR reaches a therapeutic level for 2 (two) consecutive days. 4o) A process exists for detection of contraindication of warfarin in pregnancy.
25 5. Warfarin prevention & mitigation practices Warfarin management practices include: 5a) Notification of dietary services when a patient is receiving warfarin therapy. 5b) Automatic nutrition consults when patients are first placed on warfarin to avoid drug-food interactions 5c) Warfarin is dispensed in unit dose only (e.g., warfarin tablets are not split). 5d) Warfarin is not available as floor stock unless stored in an automated dispensing cabinet that is interfaced with pharmacy. 5e) All strengths of warfarin tablets dispensed within the facility are purchased from a single manufacturer.
26 5. Warfarin prevention & mitigation practices The facility s practice for handoff communication to the next provider of care includes: 5f) Inpatient warfarin dosing history 5g) Inpatient INR value history 5h) Date the next INR is due 5i) Daily warfarin dosing schedule to be followed until date of next INR 5j) A confirmed appointment scheduled for laboratory, physician, and/or antithrombotic clinic
27 5. Warfarin prevention & mitigation practices The facility s practice for patients who are being discharged on warfarin therapy and have a subtherapeutic INR includes a transition plan for: 5k) Consistent evaluation regarding the need for LMWH until a therapeutic INR is reached 5l) Maintaining patient on LMWH until a therapeutic INR is reached, (when appropriate)
28 6) Parenteral anticoagulant management practices Processes are in place for: 6a) Safely managing the care & removal of epidural catheters placed during regional anesthesia when LMWH has been administered. 6b) Monitoring and/or discontinuing antithrombotic therapy prior to invasive procedures. (e.g., INR within specific range or target.) 6c) Only continuous infusions are used for therapeutic IV heparin (no intermittent IV administration). 6d) When LMWH or UFH therapy is greater than 3 days, a process exists that ensures that a platelet count and serum creatinine are repeated every 3 days.
29 6) Parenteral anticoagulant management practices 6e) Standard guidelines are used for laboratory monitoring of LMWH in special populations (e.g. renal dosing, pregnancy, and morbid obesity) When laboratory reagents that are used to measure the PTT or other hematological tests are changed a process exists to: 6f) Inform prescribers, pharmacists and nurses about the change. 6g) Update affected dosing protocols and order sets.
30 7) Parenteral anticoagulant prevention & mitigation strategies Processes exist to eliminate errors in preparation, storage, and dispensing which includes: 7a) Utilizing unit dose LMWH (round to the nearest dose if using a pen) 7b) Limiting concentrations of Heparin stored in automated dispensing machines and as floor stock (e.g., Do not store 10,000 units/ml 1mL vials) Dispensing commercially prepared, pre-mixed IV solutions of UFH: 7c) In limited concentrations. 7d) In limited vial sizes. 7e) In prefilled heparin flush syringes.
31 7) Parenteral anticoagulant prevention & mitigation strategies Independent double-check for UFH are used (e.g., with smart pump technology and/or nurse doublecheck) with: 7f) Each new bag hung 7g) Each rate change
32 8) Parenteral anticoagulant therapeutic strategies Processes exist to initiate and monitor heparin via lab values including: 8a) A baseline hemoglobin, hematocrit, serum creatinine and platelet count are obtained prior to initiating antithrombotic therapy with UFH or LMWH. 8b) PTTs are obtained no sooner than 6-8 hours after UFH initiation. 8c) Laboratory tests have standard intervals for assessment. (e.g., hgb every 3 days, platelets every 3 days.) 8d) Prior to ordering any heparin product, prescribers are required to specifically ask patients if they have a known history of heparin induced thrombocytopenia (HIT) and/or an allergy to heparin; and positive responses are documented in the medical record.
33 8) Parenteral anticoagulant therapeutic strategies 8e) A VTE prophylaxis protocol exists and is used for acutely ill or critically ill medical patients that includes use of low dose UFH, LMWH or fondaparinux. 8f) The renal dosing program allows a pharmacist or prescriber to routinely adjust the doses of LMWH, Factor Xa inhibitors, and direct thrombin inhibitors. 8g) The documentation process for LMWH injections includes date and time of dose, and site of injection. For patients on UFH: 8h) If platelet count decreases to less than 100,000/mm 3 or less than 50% of the baseline that the patient is evaluated for HIT in real-time. 8i) If the patient is diagnosed with HIT, all sources of heparin are discontinued including heparin flush.
34 9) Implement appropriate critical thinking and knowledge strategies Interdisciplinary education on antithrombotic therapy is provided and includes: 9a) Initial training for new hires and existing staff, including protocols and guidelines. 9b) Post test incorporating a case-study approach to demonstrate proficiency. 9c) Plan for targeting gaps in knowledge. 9d) Ongoing antithrombotic education is provided to direct care staff when new relevant information is available.
35 10) Provide patient and family education 10a) When initiating therapy, patients/caregivers receive verbal & written information on purpose, action, side effects, & monitoring. Processes exist to educate patients & families, using teach-back method, to ensure safe therapy including: 10b) Indication 10c) Symptoms for monitoring 10d) Dietary issues 10e) Drug interactions 10f) Disease interactions 10g) Monitoring requirements 10h) Duration of therapy 10i) Potential adverse effects 10j) Pharmacists are available for consultations to assist with patient
36 Questions and Discussion
Drug Therapy Management
 4/17 Welcome to the Centers of Excellence Assessment Becoming an Anticoagulation Center of Excellence gives your service the chance to work as a multidisciplinary team to evaluate your current safety practices
4/17 Welcome to the Centers of Excellence Assessment Becoming an Anticoagulation Center of Excellence gives your service the chance to work as a multidisciplinary team to evaluate your current safety practices
Improving Safety Practices Anticoagulation Therapy
 Improving Safety Practices Anticoagulation Therapy Katie Cinnamon, PharmD, BCPS Clinical Pharmacist Genesis Medical Center - Davenport Objectives Review background information on medication errors and
Improving Safety Practices Anticoagulation Therapy Katie Cinnamon, PharmD, BCPS Clinical Pharmacist Genesis Medical Center - Davenport Objectives Review background information on medication errors and
Accreditation Program: Long Term Care
 ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
The Joint Commission Medication Management Update for 2010
 Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
Harrison Memorial Hospital Cynthiana, KY. Rachel Harney, PharmD Director of Pharmacy ADEs Related to Coumadin March 1, 2018
 Harrison Memorial Hospital Cynthiana, KY Rachel Harney, PharmD Director of Pharmacy ADEs Related to Coumadin March 1, 2018 About Us HMH is a regional healthcare facility licensed to operate 61 beds 20
Harrison Memorial Hospital Cynthiana, KY Rachel Harney, PharmD Director of Pharmacy ADEs Related to Coumadin March 1, 2018 About Us HMH is a regional healthcare facility licensed to operate 61 beds 20
Anticoagulation: Safe prescribing, dispensing and administration of oral and parenteral anticoagulants
 Trust Policy Anticoagulation: Safe prescribing, dispensing and administration of oral and parenteral anticoagulants Purpose Date Version March 2015 2 To manage the inherent risks to patients from the use
Trust Policy Anticoagulation: Safe prescribing, dispensing and administration of oral and parenteral anticoagulants Purpose Date Version March 2015 2 To manage the inherent risks to patients from the use
Protocol Applies To: UW Health Clinics: all adult outpatients with an active order for warfarin
 Protocol Number: 7 Protocol Title: Ambulatory Initiation and Management of Warfarin for Adults Protocol Applies To: UW Health Clinics: all adult outpatients with an active order for warfarin Target Patient
Protocol Number: 7 Protocol Title: Ambulatory Initiation and Management of Warfarin for Adults Protocol Applies To: UW Health Clinics: all adult outpatients with an active order for warfarin Target Patient
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Beyond Warfarin Clinic : Pharmacistmanaged. Anticoagulation Care Services
 Beyond Warfarin Clinic : Pharmacistmanaged Comprehensive Anticoagulation Care Services Nancy L. Shapiro, PharmD, FCCP, BCACP, CACP Clinical Associate Professor Clinical Pharmacist and Coordinator, Antithrombosis
Beyond Warfarin Clinic : Pharmacistmanaged Comprehensive Anticoagulation Care Services Nancy L. Shapiro, PharmD, FCCP, BCACP, CACP Clinical Associate Professor Clinical Pharmacist and Coordinator, Antithrombosis
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1
 Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
After reading this learning module, the nurse should be able to:
 After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
The Joint Commission Medication Management Update for 2010
 The Joint Commission Medication Management Update for 2010 U.S. Army Manager, Army Patient Safety Program U.S. Army Medical Command Fort Sam Houston, TX CPE Information and Professional Resources & Business
The Joint Commission Medication Management Update for 2010 U.S. Army Manager, Army Patient Safety Program U.S. Army Medical Command Fort Sam Houston, TX CPE Information and Professional Resources & Business
Indian River Medical Center Policy #: 10.1 Policies and Procedures
 Indian River Medical Center Policy #: 10.1 Policies and Procedures Title: ANTICOAGULATION CLINIC Effective Date: Chapter: Pharmacy Reviewed Date: Responsible Person: Director of Pharmacy Revised Date:
Indian River Medical Center Policy #: 10.1 Policies and Procedures Title: ANTICOAGULATION CLINIC Effective Date: Chapter: Pharmacy Reviewed Date: Responsible Person: Director of Pharmacy Revised Date:
Medication Safety & Electrolyte Administration. Objectives. High Alert Medications. *Med Safety Electrolyte Administration
 Medication Safety & Electrolyte Administration Jennifer Doughty, PharmD PGY2 Pharmacy Resident Emergency Medicine Stormont Vail Health, Topeka, KS Objectives Define and identify high alert medications
Medication Safety & Electrolyte Administration Jennifer Doughty, PharmD PGY2 Pharmacy Resident Emergency Medicine Stormont Vail Health, Topeka, KS Objectives Define and identify high alert medications
ISMP Medication Safety Self Assessment for Antithrombotic Therapy
 2017 ISMP Medication Safety Self Assessment for Antithrombotic Therapy cknowledgements Funding Source ISMP thanks oehringer-ingelheim Pharmaceuticals, Inc., SL ehring, and Pfizer, Inc. for their support
2017 ISMP Medication Safety Self Assessment for Antithrombotic Therapy cknowledgements Funding Source ISMP thanks oehringer-ingelheim Pharmaceuticals, Inc., SL ehring, and Pfizer, Inc. for their support
Objectives. Demographics: Type and Services 1/22/2014. ICAHN Aggregate Results. ISMP Medication Safety Self Assessment for Hospitals
 ICAHN Aggregate Results ISMP Medication Safety Self Assessment for Hospitals Matthew Fricker, RPH, MS, FASHP Rebecca Lamis, PharmD, FISMP January 23, 2014 1 Objectives Report the demographic characteristics
ICAHN Aggregate Results ISMP Medication Safety Self Assessment for Hospitals Matthew Fricker, RPH, MS, FASHP Rebecca Lamis, PharmD, FISMP January 23, 2014 1 Objectives Report the demographic characteristics
Safer use of anticoagulants: the NPSA patient safety alert Steve Chaplin MSc, MRPharmS
 Safer use of anticoagulants: the NPSA patient safety alert Steve Chaplin MSc, MRPharmS Steve Chaplin describes the NPSA s anticoagulant patient safety alert and the measures it recommends for making the
Safer use of anticoagulants: the NPSA patient safety alert Steve Chaplin MSc, MRPharmS Steve Chaplin describes the NPSA s anticoagulant patient safety alert and the measures it recommends for making the
REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY
 REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY Approved September 2014, Bangkok, Thailand, as revisions of the initial 2008 version. Overarching and Governance Statements 1. The overarching
REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY Approved September 2014, Bangkok, Thailand, as revisions of the initial 2008 version. Overarching and Governance Statements 1. The overarching
Prevention and Treatment of Venous Thromboembolism (VTE) Policy
 Policy") CONTROLLED DOCUMENT Prevention and Treatment of Venous Thromboembolism (VTE) Policy CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled
CONTROLLED DOCUMENT Prevention and Treatment of Venous Thromboembolism (VTE) Policy CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled
U: Medication Administration
 U: Medication Administration Alberta Licensed Practical Nurses Competency Profile 199 Competency: U-1 Pharmacology and Principles of Administration of Medications U-1-1 U-1-2 U-1-3 U-1-4 Demonstrate knowledge
U: Medication Administration Alberta Licensed Practical Nurses Competency Profile 199 Competency: U-1 Pharmacology and Principles of Administration of Medications U-1-1 U-1-2 U-1-3 U-1-4 Demonstrate knowledge
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016
 UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
MANAGING THE INR CLINIC : IJN EXPERIENCE
 MANAGING THE INR CLINIC : IJN EXPERIENCE Anticoagulation Workshop 21 st August 2015 KAMALESWARY ARUMUGAM PRINCIPAL PHARMACIST LEE LEE HO1 NURSE MENTOR, INR CLINIC HISTORY & OVERVIEW OF THE INR CLINIC HISTORY
MANAGING THE INR CLINIC : IJN EXPERIENCE Anticoagulation Workshop 21 st August 2015 KAMALESWARY ARUMUGAM PRINCIPAL PHARMACIST LEE LEE HO1 NURSE MENTOR, INR CLINIC HISTORY & OVERVIEW OF THE INR CLINIC HISTORY
Best Practices During an Interventional Acute Stroke Response. Michel MacPherson Kirby RT (R)(M)(VI) Aileen Luksic BSN RN
(M)(VI) Aileen Luksic BSN RN") Best Practices During an Interventional Acute Stroke Response Michel MacPherson Kirby RT (R)(M)(VI) Aileen Luksic BSN RN UCLA ACUTE ISCHEMIC STROKE SOP 90 min door to needle GOAL Timely intervention of
Best Practices During an Interventional Acute Stroke Response Michel MacPherson Kirby RT (R)(M)(VI) Aileen Luksic BSN RN UCLA ACUTE ISCHEMIC STROKE SOP 90 min door to needle GOAL Timely intervention of
Alert. Patient safety alert. Actions that can make anticoagulant therapy safer. 28 March Action for the NHS and the independent sector
 Patient safety alert 18 Alert 28 March 2007 Immediate action Action Update Information request Ref: NPSA/2007/18 Actions that can make anticoagulant therapy safer Anticoagulants are one of the classes
Patient safety alert 18 Alert 28 March 2007 Immediate action Action Update Information request Ref: NPSA/2007/18 Actions that can make anticoagulant therapy safer Anticoagulants are one of the classes
Sheffield Teaching Hospitals: Pulmonary Hypertension. Information for Medical Staff 31/03/2014. Local guidelines
 Sheffield Teaching Hospitals: Pulmonary Hypertension Information for Medical Staff 31/03/2014 Local guidelines Diagnostic pathway - page 2 Iloprost dosing chart and conversion table - page 3-4 Hickman
Sheffield Teaching Hospitals: Pulmonary Hypertension Information for Medical Staff 31/03/2014 Local guidelines Diagnostic pathway - page 2 Iloprost dosing chart and conversion table - page 3-4 Hickman
Measuring Medication Harm: Advantages of Using a Trigger Tool. Frank Federico Executive Director
 Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
The Newcastle upon Tyne Hospitals NHS Foundation Trust Venous. Thromboembolism (VTE) Assessment and Management
 Assessment and Management") The Newcastle upon Tyne Hospitals NHS Foundation Trust Venous Thromboembolism (VTE) Assessment and Management Version No: 2.0 Effective From: 16 April 2018 Expiry Date: 16 April 2021 Date Ratified: 23
The Newcastle upon Tyne Hospitals NHS Foundation Trust Venous Thromboembolism (VTE) Assessment and Management Version No: 2.0 Effective From: 16 April 2018 Expiry Date: 16 April 2021 Date Ratified: 23
Definitions: In this chapter, unless the context or subject matter otherwise requires:
 CHAPTER 61-02-01 Final Copy PHARMACY PERMITS Section 61-02-01-01 Permit Required 61-02-01-02 Application for Permit 61-02-01-03 Pharmaceutical Compounding Standards 61-02-01-04 Permit Not Transferable
CHAPTER 61-02-01 Final Copy PHARMACY PERMITS Section 61-02-01-01 Permit Required 61-02-01-02 Application for Permit 61-02-01-03 Pharmaceutical Compounding Standards 61-02-01-04 Permit Not Transferable
To prevent harm to patients from adverse medication events involving high-alert medications.
 TITLE MANAGEMENT OF HIGH-ALERT MEDICATIONS DOCUMENT # PS-46-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Management of High-alert Medications Policy APPROVAL LEVEL Alberta Health Services Executive
TITLE MANAGEMENT OF HIGH-ALERT MEDICATIONS DOCUMENT # PS-46-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Management of High-alert Medications Policy APPROVAL LEVEL Alberta Health Services Executive
PATIENT CARE MANUAL PROCEDURE
 PATIENT CARE MANUAL PROCEDURE NUMBER III-130 PAGE 1 OF 5 APPROVED BY: CATEGORY: Vice President and Senior Operating Officer, Rural Health Services & Professional Practice Lead Medication Administration
PATIENT CARE MANUAL PROCEDURE NUMBER III-130 PAGE 1 OF 5 APPROVED BY: CATEGORY: Vice President and Senior Operating Officer, Rural Health Services & Professional Practice Lead Medication Administration
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Single Technology Appraisal (STA)
") Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Organizational Initiative
 Organizational Initiative Prevention and Treatment of Venous Thromboembolism (VTE) Nursing s Role Donna Grochow MSN, RN May 2012 1 Agenda Organizational Initiative: Why Now? Review of current performance
Organizational Initiative Prevention and Treatment of Venous Thromboembolism (VTE) Nursing s Role Donna Grochow MSN, RN May 2012 1 Agenda Organizational Initiative: Why Now? Review of current performance
MEDCOM Medication Management Discussion
 MEDCOM Medication Management Discussion 2009 MEDCOM-TJC Conference Manager, Army Patient Safety Program Quality Management Office HQ, US Army Medical Command Fort Sam Houston, TX 19 Nov 2009 BRIEFING OUTLINE
MEDCOM Medication Management Discussion 2009 MEDCOM-TJC Conference Manager, Army Patient Safety Program Quality Management Office HQ, US Army Medical Command Fort Sam Houston, TX 19 Nov 2009 BRIEFING OUTLINE
Implementation of Clinical Services at Various Institutions
 Implementation of Clinical Services at Various Institutions Niki Carver, Pharm.D., UAMS Medical Center Shannon Hays, Pharm.D., White Co Medical Melanie Claborn, Pharm.D., Veterans Healthcare System of
Implementation of Clinical Services at Various Institutions Niki Carver, Pharm.D., UAMS Medical Center Shannon Hays, Pharm.D., White Co Medical Melanie Claborn, Pharm.D., Veterans Healthcare System of
Required Organizational Practices Resources for 2016
 Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Department Policy. Code: D: MM Entity: Fairview Pharmacy Services. Department: Fairview Home Infusion. Manual: Policy and Procedure Manual
 Department Policy Code: D: MM-5615 Entity: Fairview Pharmacy Services Department: Fairview Home Infusion Manual: Policy and Procedure Manual Category: Home Infusion Subject: Chemotherapy Purpose: Ensure
Department Policy Code: D: MM-5615 Entity: Fairview Pharmacy Services Department: Fairview Home Infusion Manual: Policy and Procedure Manual Category: Home Infusion Subject: Chemotherapy Purpose: Ensure
When Administering Warfarin
 What Special Instructions Must Be Followed When Administering Warfarin What special dietary instructions should I follow? What should I do if I forget a even if you feel well. Do not stop taking simvastatin
What Special Instructions Must Be Followed When Administering Warfarin What special dietary instructions should I follow? What should I do if I forget a even if you feel well. Do not stop taking simvastatin
PGY1 Oncology 2 Advanced Learning Experience
 PGY1 Oncology 2 Advanced Learning Experience Potential Preceptor: Kendra VanHandel, Rani Scranton Hours: 0700 to 1730 M-F Contact: kendra.vanhandel@asante.org, rani.scranton@asante.org General Description
PGY1 Oncology 2 Advanced Learning Experience Potential Preceptor: Kendra VanHandel, Rani Scranton Hours: 0700 to 1730 M-F Contact: kendra.vanhandel@asante.org, rani.scranton@asante.org General Description
Medication Control and Distribution. Minor/technical revision of existing policy. ± Major revision of existing policy Reaffirmation of existing policy
 Name of Policy: Policy Number: 3364-133-17 Department: Pharmacy Approvingofficer: Chief Executive Officer THE unrversity OF TOLEDO MEDICAL CERITER Responsible Agent: Scope: Director of Pharmacy University
Name of Policy: Policy Number: 3364-133-17 Department: Pharmacy Approvingofficer: Chief Executive Officer THE unrversity OF TOLEDO MEDICAL CERITER Responsible Agent: Scope: Director of Pharmacy University
MEDICATION USE EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014
 TITLE / DESCRIPTION: SAFETY PROCEDURES FOR MEDICATION USE DEPARTMENT: Pharmacy PERSONNEL: All Pharmacy Personnel EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014 Leadership and Culture A culture
TITLE / DESCRIPTION: SAFETY PROCEDURES FOR MEDICATION USE DEPARTMENT: Pharmacy PERSONNEL: All Pharmacy Personnel EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014 Leadership and Culture A culture
Patient Safety and Quality Measures for CRRT: The UAB Experience. Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012
 Patient Safety and Quality Measures for CRRT: The UAB Experience Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012 Quality Healthcare Quality is the extent to which health services for
Patient Safety and Quality Measures for CRRT: The UAB Experience Ashita Tolwani, M.D. University of Alabama at Birmingham CRRT 2012 Quality Healthcare Quality is the extent to which health services for
Oxfordshire Anticoagulation Service. Important information about anticoagulation with vitamin K antagonists Information for patients
 Oxfordshire Anticoagulation Service Important information about anticoagulation with vitamin K antagonists Information for patients Page 2 Your information Name:... Address:......... or patient stickie
Oxfordshire Anticoagulation Service Important information about anticoagulation with vitamin K antagonists Information for patients Page 2 Your information Name:... Address:......... or patient stickie
Policy for Venous Thromboembolism Prevention and Treatment
 Policy for Venous Thromboembolism Prevention and Treatment Start date: May 2013 Next Review: May 2015 Committee approval: Endorsed by: Distribution: Location Thrombosis and Thromboprophylaxis Steering
Policy for Venous Thromboembolism Prevention and Treatment Start date: May 2013 Next Review: May 2015 Committee approval: Endorsed by: Distribution: Location Thrombosis and Thromboprophylaxis Steering
Setting up the NOAC Service & Taking it to Primary Care
 Setting up the NOAC Service & Taking it to Primary Care Satinder Bhandal Consultant Anticoagulation Pharmacist November 2015 Buckinghamshire Health Care NHS Trust Quiz 1. What is the most serious side
Setting up the NOAC Service & Taking it to Primary Care Satinder Bhandal Consultant Anticoagulation Pharmacist November 2015 Buckinghamshire Health Care NHS Trust Quiz 1. What is the most serious side
WHAT are medication errors?
 Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
STANDING ORDERS FOR THE MANAGEMENT OF WARFARIN Dose adjustment and INR testing frequency Applicable to: Pharmacists. Issued by: Contact:
 STANDING ORDERS FOR THE MANAGEMENT OF WARFARIN Dose adjustment and INR testing frequency Applicable to: Pharmacists Standing Order used for the Community Pharmacy Anticoagulant Management (CPAM) Service
STANDING ORDERS FOR THE MANAGEMENT OF WARFARIN Dose adjustment and INR testing frequency Applicable to: Pharmacists Standing Order used for the Community Pharmacy Anticoagulant Management (CPAM) Service
Guidance for Medication Reconciliation and System Integration Process
 Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES Medication Administration Observation
 : Make random medication observations of several staff over different shifts and units, multiple routes of administration -- oral, enteral, intravenous (IV), intramuscular (IM), subcutaneous (SQ), topical,
: Make random medication observations of several staff over different shifts and units, multiple routes of administration -- oral, enteral, intravenous (IV), intramuscular (IM), subcutaneous (SQ), topical,
OUTPATIENT ENDOSCOPY (PULM) PROCEDURE PLAN - Phase: Diagnostic/Pre-Op Orders
 PROCEDURE PLAN - Phase: Diagnostic/Pre-Op Orders") - Phase: Diagnostic/Pre-Op Orders PHYSICIAN S Diagnosis Weight Allergies DETAILS Admit/Discharge/Transfer Request Endoscopy Services-GI Patient Care Obtain Consent Vital Signs Per Unit Standards Insert
- Phase: Diagnostic/Pre-Op Orders PHYSICIAN S Diagnosis Weight Allergies DETAILS Admit/Discharge/Transfer Request Endoscopy Services-GI Patient Care Obtain Consent Vital Signs Per Unit Standards Insert
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV TREPROSTINIL (REMODULIN ) Job Title of Reviewer: Director, Pharmacy POLICY
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV TREPROSTINIL (REMODULIN ) Job Title of Reviewer: Director, Pharmacy POLICY
4/9/2013. Best Practice Initiative: Inpatient Anticoagulation Stewardship. Dorcas Letting reports no relevant financial relationships
 Disclosure Best Practice Initiative: Inpatient Anticoagulation Stewardship Dorcas Letting reports no relevant financial relationships Dorcas Letting-Mangira, Pharm.D Pharmacotherapist, Internal Medicine
Disclosure Best Practice Initiative: Inpatient Anticoagulation Stewardship Dorcas Letting reports no relevant financial relationships Dorcas Letting-Mangira, Pharm.D Pharmacotherapist, Internal Medicine
Session 2 Improving Narcotics and Opiate Management
 Session 2 Improving Narcotics and Opiate Management Frank Federico, RPh, IHI Executive Director Steve Meisel, Pharm.D., IHI Faculty January 31,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH,
Session 2 Improving Narcotics and Opiate Management Frank Federico, RPh, IHI Executive Director Steve Meisel, Pharm.D., IHI Faculty January 31,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH,
SHRI GURU RAM RAI INSTITUTE OF TECHNOLOGY AND SCIENCE MEDICATION ERRORS
 MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
The CMS State Operations Manual Overview and Changes
 The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE)
") COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
NORTH CAROLINA. Downloaded January 2011
 NORTH CAROLINA Downloaded January 2011 10A NCAC 13D.2306 MEDICATION ADMINISTRATION (a) The facility shall ensure that medications are administered in accordance with standards of professional practice
NORTH CAROLINA Downloaded January 2011 10A NCAC 13D.2306 MEDICATION ADMINISTRATION (a) The facility shall ensure that medications are administered in accordance with standards of professional practice
Case Presentation. Cindy Felty MSN, RN, CNP, FCCWS Assistant Professor of Medicine Mayo Clinic March 27, 2008
 Case Presentation Cindy Felty MSN, RN, CNP, FCCWS Assistant Professor of Medicine Mayo Clinic March 27, 2008 Acute DVT Case 1- Day 1 68 year old male admitted overnight to hospital for painful acute DVT
Case Presentation Cindy Felty MSN, RN, CNP, FCCWS Assistant Professor of Medicine Mayo Clinic March 27, 2008 Acute DVT Case 1- Day 1 68 year old male admitted overnight to hospital for painful acute DVT
CRAIG HOSPITAL POLICY/PROCEDURE
 CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
CarePartners Nursing Care Plan Anticoagulant Therapy
 CarePartners Nursing Care Plan Anticoagulant Therapy ** If a CarePartners wound pathway, palliative care plan or oncology care plan is being used to guide the patient s care, this Nursing Care Plan may
CarePartners Nursing Care Plan Anticoagulant Therapy ** If a CarePartners wound pathway, palliative care plan or oncology care plan is being used to guide the patient s care, this Nursing Care Plan may
UNDERSTANDING THE CONTENT OUTLINE/CLASSIFICATION SYSTEM
 BOARD OF PHARMACY SPECIALTIES CRITICAL CARE PHARMACY SPECIALIST CERTIFICATION CONTENT OUTLINE/CLASSIFICATION SYSTEM FINALIZED SEPTEMBER 2017/FOR USE ON FALL 2018 EXAMINATION AND FORWARD UNDERSTANDING THE
BOARD OF PHARMACY SPECIALTIES CRITICAL CARE PHARMACY SPECIALIST CERTIFICATION CONTENT OUTLINE/CLASSIFICATION SYSTEM FINALIZED SEPTEMBER 2017/FOR USE ON FALL 2018 EXAMINATION AND FORWARD UNDERSTANDING THE
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Reducing Warfarin ADR s with a Nurse Led Anticoagulation Clinic: A New Model of Patient Care
 Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 6-16-2017 Reducing Warfarin ADR s with a Nurse Led Anticoagulation Clinic: A New Model of Patient Care Michael
Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 6-16-2017 Reducing Warfarin ADR s with a Nurse Led Anticoagulation Clinic: A New Model of Patient Care Michael
El Paso Integrated Physicians Group. Overview
 El Paso Integrated Physicians Group Protocol Name Protocol Number Infusion Services 01 Effective Date 6/1/2015 Supersedes Protocol Dated N/A Overview This clinical protocol defines requirements and activities
El Paso Integrated Physicians Group Protocol Name Protocol Number Infusion Services 01 Effective Date 6/1/2015 Supersedes Protocol Dated N/A Overview This clinical protocol defines requirements and activities
Hospital Guidance Webinar
 Hospital Guidance Webinar Using the CPOE Tool Results for Quality Improvement PRESENTED BY: DAVID BATES, MD, MS C AND DAVID CLASSEN, MD, MS C Overview Introduction What the current test looks like and
Hospital Guidance Webinar Using the CPOE Tool Results for Quality Improvement PRESENTED BY: DAVID BATES, MD, MS C AND DAVID CLASSEN, MD, MS C Overview Introduction What the current test looks like and
Venous Thromboembolism (VTE) Audit Day
 Audit Day") Venous Thromboembolism (VTE) Audit Day Questions If you have any questions or require clarification, please contact Artemis Diamantouros. Email: artemis.diamantouros@sunnybrook.ca Welcome to the Canadian
Venous Thromboembolism (VTE) Audit Day Questions If you have any questions or require clarification, please contact Artemis Diamantouros. Email: artemis.diamantouros@sunnybrook.ca Welcome to the Canadian
Licensed Pharmacy Technicians Scope of Practice
 Licensed s Scope of Practice Adapted from: Request for Regulation of s Approved by Council April 24, 2015 DEFINITIONS In this policy: Act means The Pharmacy and Pharmacy Disciplines Act means an unregulated
Licensed s Scope of Practice Adapted from: Request for Regulation of s Approved by Council April 24, 2015 DEFINITIONS In this policy: Act means The Pharmacy and Pharmacy Disciplines Act means an unregulated
N ATIONAL Q UALITY F ORUM. Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT
 N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
201 KAR 20:490. Licensed practical nurse intravenous therapy scope of practice.
 201 KAR 20:490. Licensed practical nurse intravenous therapy scope of practice. RELATES TO: KRS 314.011(10)(a), (c) STATUTORY AUTHORITY: KRS 314.011(10)(c), 314.131(1), 314.011(10)(c) NECESSITY, FUNCTION,
201 KAR 20:490. Licensed practical nurse intravenous therapy scope of practice. RELATES TO: KRS 314.011(10)(a), (c) STATUTORY AUTHORITY: KRS 314.011(10)(c), 314.131(1), 314.011(10)(c) NECESSITY, FUNCTION,
House Staff Orientation Department of Pharmacy
 House Staff Orientation Department of Pharmacy Paul Nowierski, Senior Director of Pharmacy Nicholas Zerilli, Clinical Pharmacist Advanced Practice, BCPS Lenox Hill Hospital Department of Pharmacy June
House Staff Orientation Department of Pharmacy Paul Nowierski, Senior Director of Pharmacy Nicholas Zerilli, Clinical Pharmacist Advanced Practice, BCPS Lenox Hill Hospital Department of Pharmacy June
NEW JERSEY. Downloaded January 2011
 NEW JERSEY Downloaded January 2011 SUBCHAPTER 29. MANDATORY PHARMACY 8:39 29.1 Mandatory pharmacy organization (a) A facility shall have a consultant pharmacist and either a provider pharmacist or, if
NEW JERSEY Downloaded January 2011 SUBCHAPTER 29. MANDATORY PHARMACY 8:39 29.1 Mandatory pharmacy organization (a) A facility shall have a consultant pharmacist and either a provider pharmacist or, if
5. returning the medication container to proper secured storage; and
 111-8-63-.20 Medications. (1) Self-Administration of Medications. Residents who have the cognitive and functional capacities to engage in the self-administration of medications safely and independently
111-8-63-.20 Medications. (1) Self-Administration of Medications. Residents who have the cognitive and functional capacities to engage in the self-administration of medications safely and independently
Low Molecular Weight Heparins
 ril 2014 Low Molecular Weight Heparins FINAL CONSOLIDATED COMPREHENSIVE RESEARCH PLAN September 2015 FINALCOMPREHENSIVE RESEARCH PLAN 2 A. Introduction The objective of the drug class review on LMWH is
ril 2014 Low Molecular Weight Heparins FINAL CONSOLIDATED COMPREHENSIVE RESEARCH PLAN September 2015 FINALCOMPREHENSIVE RESEARCH PLAN 2 A. Introduction The objective of the drug class review on LMWH is
Reimbursement for Anticoagulation Services
 Journal of Thrombosis and Thrombolysis 12(1), 73 79, 2001. # 2002 Kluwer Academic Publishers, Manufactured in The Netherlands. Reimbursement for Anticoagulation Services Paul W. Radensky McDermott, Will
Journal of Thrombosis and Thrombolysis 12(1), 73 79, 2001. # 2002 Kluwer Academic Publishers, Manufactured in The Netherlands. Reimbursement for Anticoagulation Services Paul W. Radensky McDermott, Will
Preventing hospital-acquired blood clots
 Preventing hospital-acquired blood clots Haematology Department Patient information leaflet This leaflet explains more about blood clots, which can form after illness and surgery. What are hospital-acquired
Preventing hospital-acquired blood clots Haematology Department Patient information leaflet This leaflet explains more about blood clots, which can form after illness and surgery. What are hospital-acquired
To establish a consistent process for the activity of an independent double-check prior to medication administration, where appropriate.
 TITLE INDEPENDENT DOUBLE-CHECK SCOPE Provincial, Clinical DOCUMENT # PS-60-01 APPROVAL LEVEL Senior Operating Officer, Pharmacy Services SPONSOR Provincial Medication Management Committee CATEGORY Patient
TITLE INDEPENDENT DOUBLE-CHECK SCOPE Provincial, Clinical DOCUMENT # PS-60-01 APPROVAL LEVEL Senior Operating Officer, Pharmacy Services SPONSOR Provincial Medication Management Committee CATEGORY Patient
National Medication Safety Network. Observatory Erskine David UKMI, Guy s and St Thomas NHS Foundation Trust
 National Medication Safety Network Observatory Erskine David UKMI, Guy s and St Thomas NHS Foundation Trust Slide 1 MSO Web Event 28 th January 2015 1 Slide 2 MSO Web Event 28 th January 2015 National
National Medication Safety Network Observatory Erskine David UKMI, Guy s and St Thomas NHS Foundation Trust Slide 1 MSO Web Event 28 th January 2015 1 Slide 2 MSO Web Event 28 th January 2015 National
Using Clinical Data Categories with the Pyxis MedStation
 Using Clinical Data Categories with the Pyxis MedStation system Using Clinical Data Categories Clinical Data Categories (CDCs) are a Pyxis MedStation system software tool that will allow facilities the
Using Clinical Data Categories with the Pyxis MedStation system Using Clinical Data Categories Clinical Data Categories (CDCs) are a Pyxis MedStation system software tool that will allow facilities the
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE MEDICATION ORDERS SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Provincial Medication Management Committee PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
TITLE MEDICATION ORDERS SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Provincial Medication Management Committee PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
JCAHO Med Management
 Hospital Pharmacy Volume 41, Number 9, pp 888 892 2006 Wolters Kluwer Health, Inc. JCAHO Med Management Meeting the Standards for Emergency Medications and Labeling Patricia C. Kienle, MPA, FASHP* This
Hospital Pharmacy Volume 41, Number 9, pp 888 892 2006 Wolters Kluwer Health, Inc. JCAHO Med Management Meeting the Standards for Emergency Medications and Labeling Patricia C. Kienle, MPA, FASHP* This
Schedule C1. Community Pharmacy Anti-Coagulation Management Services
 Schedule C1 Community Pharmacy Anti-Coagulation Management Services 1. Definition This service specification relates to the anticoagulation management of Service Users on warfarin by an accredited community
Schedule C1 Community Pharmacy Anti-Coagulation Management Services 1. Definition This service specification relates to the anticoagulation management of Service Users on warfarin by an accredited community
Document ref. no: Trust Policy and Procedure PP(16)238 MANAGEMENT OF ADULT PATIENTS TREATED WITH ORAL ANTICOAGULANTS. Approved
238 MANAGEMENT OF ADULT PATIENTS TREATED WITH ORAL ANTICOAGULANTS. Approved") Document ref. no: Trust Policy and Procedure PP(16)238 MANAGEMENT OF ADULT PATIENTS TREATED WITH ORAL ANTICOAGULANTS For use in: For use by: For use for: Document owner: Status: West Suffolk NHS Foundation
Document ref. no: Trust Policy and Procedure PP(16)238 MANAGEMENT OF ADULT PATIENTS TREATED WITH ORAL ANTICOAGULANTS For use in: For use by: For use for: Document owner: Status: West Suffolk NHS Foundation
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY. April 2009 September 2012
 MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY April 2009 September 2012 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire des médicaments du
MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY April 2009 September 2012 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire des médicaments du
Go for the Gold. Incorporating Regulatory Issues into the Quality Management Process. June 9 11, 2008 Starr Pass Resort Tucson, Arizona
 Go for the Gold June 9 11, 2008 Starr Pass Resort Tucson, Arizona Incorporating Regulatory Issues into the Quality Management Process Recent regulatory changes have impacted the traditional hospital Quality
Go for the Gold June 9 11, 2008 Starr Pass Resort Tucson, Arizona Incorporating Regulatory Issues into the Quality Management Process Recent regulatory changes have impacted the traditional hospital Quality
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009
 The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV EPOPROSTENOL (FLOLAN, VELETRI ) POLICY #: EFFECTIVE DATE: REVISED DATE: POLICY
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV EPOPROSTENOL (FLOLAN, VELETRI ) POLICY #: EFFECTIVE DATE: REVISED DATE: POLICY
War on Warfarin: Integrating DOACs into your Anticoagulation Service
 War on Warfarin: Integrating DOACs into your Anticoagulation Service David DeiCicchi, Pharm.D, CACP Brigham and Women s Hospital September 30 th, 2016 Disclosures I have no financial conflict of interest
War on Warfarin: Integrating DOACs into your Anticoagulation Service David DeiCicchi, Pharm.D, CACP Brigham and Women s Hospital September 30 th, 2016 Disclosures I have no financial conflict of interest
ANTICOAGULATION MANAGEMENT SERVICE PATIENT AND FAMILY EDUCATION
 Apixaban ANTICOAGULATION MANAGEMENT SERVICE PATIENT AND FAMILY EDUCATION 1 WHAT DOES APIXABAN (ELIQUIS ) DO? blood thinner Prevents or treats blood clots This is how a blood clot might look inside a blood
Apixaban ANTICOAGULATION MANAGEMENT SERVICE PATIENT AND FAMILY EDUCATION 1 WHAT DOES APIXABAN (ELIQUIS ) DO? blood thinner Prevents or treats blood clots This is how a blood clot might look inside a blood
Adverse Drug Events (ADE)
") Adverse Drug Events (ADE) Change Package PREVENTING ADVERSE DRUG EVENTS i 2016 U P D AT E ACKNOWLEDGEMENTS We would like to recognize the contributions of the American Hospital Association (AHA)/Health
Adverse Drug Events (ADE) Change Package PREVENTING ADVERSE DRUG EVENTS i 2016 U P D AT E ACKNOWLEDGEMENTS We would like to recognize the contributions of the American Hospital Association (AHA)/Health
PGY1 Oncology Rotation
 PGY1 Oncology Rotation Potential Preceptor(s): Kendra VanHandel PharmD, Rani Scranton PharmD Hours: 0700 to 1730 M-F Contact: kendra.vanhandel@asante.org, rani.scranton@asante.org General Description The
PGY1 Oncology Rotation Potential Preceptor(s): Kendra VanHandel PharmD, Rani Scranton PharmD Hours: 0700 to 1730 M-F Contact: kendra.vanhandel@asante.org, rani.scranton@asante.org General Description The
Community Health Network of San Francisco Committee on Interdisciplinary Practice
 Community Health Network of San Francisco Committee on Interdisciplinary Practice Title: Pain Consultation Service - Clinical Pharmacist I. Policy Statement A. It is the policy of the Community Health
Community Health Network of San Francisco Committee on Interdisciplinary Practice Title: Pain Consultation Service - Clinical Pharmacist I. Policy Statement A. It is the policy of the Community Health
COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016
 COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016 INTRODUCTION Incidents as part of COMPASS (Community Pharmacists Advancing Safety in Saskatchewan) Phase II reported by 87
COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016 INTRODUCTION Incidents as part of COMPASS (Community Pharmacists Advancing Safety in Saskatchewan) Phase II reported by 87
ACCOUNT NO. MED. REC. NO. NAME BIRTHDATE. Patient Identification ALL ORDERS MUST BE MARKED IN INK WITH A CHECKMARK ( ) TO BE ACTIVE.
 TO BE ACTIVE.") PO7071 *PO7071* Page 1 of 4 ALL MUST BE MARKED IN INK WITH A CHECKMARK ( ) TO BE ACTIVE. Weight: kg Height: cm Allergies: Treatment Start Date: Date(s) of Transfusion(s): Current Labs: WBC: Hgb/Hct: Platelets:
PO7071 *PO7071* Page 1 of 4 ALL MUST BE MARKED IN INK WITH A CHECKMARK ( ) TO BE ACTIVE. Weight: kg Height: cm Allergies: Treatment Start Date: Date(s) of Transfusion(s): Current Labs: WBC: Hgb/Hct: Platelets:
Developing a management plan to incorporate DOACs into what was a traditional warfarin clinic
 THSNA March 7, 2018, San Diego Nursing Pre Summit Workshop 1 4pm Thrombosis and Hemostasis Patient Education: Kernels and Pearls Developing a management plan to incorporate DOACs into what was a traditional
THSNA March 7, 2018, San Diego Nursing Pre Summit Workshop 1 4pm Thrombosis and Hemostasis Patient Education: Kernels and Pearls Developing a management plan to incorporate DOACs into what was a traditional
Interpretation of The Joint Commission Standards Related to Pain Management. Agenda. The Joint Commission Mission 9/6/2012
 Interpretation of The Joint Commission Standards Related to Pain Management ASPMN 22 nd National Conference Baltimore, MD September 13, 2012 Pat Adamski, RN, MS, MBA, FACHE Director, Standards Interpretation
Interpretation of The Joint Commission Standards Related to Pain Management ASPMN 22 nd National Conference Baltimore, MD September 13, 2012 Pat Adamski, RN, MS, MBA, FACHE Director, Standards Interpretation
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule
 HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
Improving the Patient Experience Through Pharmacy
 Rick Burnett Chief Operating Officer Kenneth Maxik Director, Patient Safety & Pharmacy Compliance Improving the Patient Experience Through Pharmacy August 19, 2015 Speakers Rick Burnett, PharmD, FACHE
Rick Burnett Chief Operating Officer Kenneth Maxik Director, Patient Safety & Pharmacy Compliance Improving the Patient Experience Through Pharmacy August 19, 2015 Speakers Rick Burnett, PharmD, FACHE
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING
 Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Sample. A guide to development of a hospital blood transfusion Policy at the hospital level. Effective from April Hospital Transfusion Committee
 Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A