Systems Thinking & Human Factors Engineering in Healthcare
|
|
|
- Nathan Cross
- 5 years ago
- Views:
Transcription
1 Clinical Networks and Streams and Managers John Hunter Hospital Newcastle, NSW; August 10, 2015 Systems Thinking & Human Factors Engineering in Healthcare Rollin J. (Terry) Fairbanks, MD, MS Director, National Center for Human Factors Engineering in Healthcare Director, Simulation & Training Environment Laboratory (SiTEL) MedStar Health, Washington DC, USA Associate Professor of Emergency Medicine, Georgetown University Attending Emergency Physician, MedStar Washington Hospital Center
2 Goal Think Differently. To view safety and risk through the lens of safety science Twitter Discussion: #HFsafety
3 Chart Credit: Modified from L. Leape
 Wachter RM.")
4 The Problem USA s Institute of Medicine (IOM) Report: 2000 Govt: 50% less error in 5 years Funding, Regs, High Focus 15 Years later. ESSENTAILLY NO CHANGE WHY? Focus still on individual performance Solutions inconsistent with safety science Leape LL, Berwick DM. Five years after To Err Is Human: what have we learned? JAMA. May ;293(19) Wachter RM. The end of the beginning: Patient Safety Five Years After 'To Err Is Human'. Health Aff. 2004(11) Wachter RM. Patient Safety At Ten: Unmistakable Progress, Troubling Gaps. Health Aff (29:1) Landrigan, Parry, et al. Temporal Trends in Rates of Patient Harm Resulting from Medical Care. NEJM 363(22): 2010 Shekelle, Pronovost, et al. Advancing the science of patient safety. Ann Int Med 154(10): 2011 Longo, Hewett, Ge, Schubert. The long road to patient safety: a status report on patient safety systems. JAMA, 294(22): 2005.
5 Why No Change? Preoccupation with Human Error Instead of reducing HARM.Leads to ineffective solutions
6 Systems Approach Is the goal: Eliminate Human Error? NO Human Error cannot be eliminated Futile goal; misdirects resources/focus Causes culture of blame and secrecy name, blame, shame, and train mentality It is about reducing HARM



7 Human Factors Engineering We don t redesign humans; We redesign the system within which humans work
8 Cognitive Science (how we think) Industrial and Organizational Psychology (how we collaborate) Work Analysis (how we work now) System Safety Engineering (how we manage risk)


9 809M airline passengers/yr....30,000 flights per day Pilots & ATC: 2 errors per hour


10

11 Example: Defibrillator Case
12 Defibrillator Case VF cardiac arrest nurse with patient charges unit clears patient presses on button Machine powers down 2-3 minute delay in shock


13 Huh? Medical Professionals: Just don t make errors



14 Knowledge-Based Improvisation in unfamiliar environments No routines or rules available Protocolized behavior Process, Procedure Rule-Based Skill-Based Automated Routines Require little conscious attention Figure adapted from: Embrey D. Understanding Human Behaviour and Error, Human Reliability Associates Based on Rasmussen s SRK Model of cognitive control, adapted to explain error by Reason (1990, 2008)


15 Slips and Lapses: Common Policies, Inservices, Signage Discipline, Training, Vigilance, Mindful Moments, etc
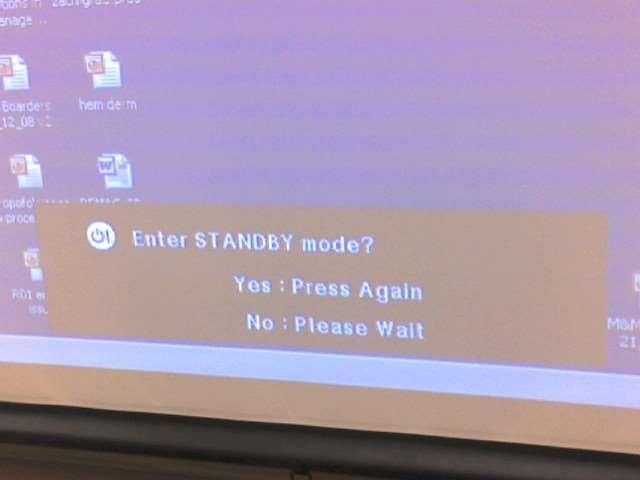
16 Defibrillator Case #2 32 year old healthy man Presents to ED with sustained SVT & chest pain Primary interventions unsuccessful Synchronized refractory Try 100j VF Arrest 45m resuscitation attempt patient dies Investigation reveals that MD failed to put device in SYNC mode for second shock
17 Defibrillator Usability Study Two defibrillator models SimMan TM patient simulator 50% of participants inadvertently delivered an unsynchronized countershock for SVT 71% of participants never aware Fairbanks RJ, Caplan SH, et al. Usability Study of Two Common Defibrillators Reveals Hazards. Annals of Emergency Medicine Oct 2007; 50(4):
18 Response #1 Physician should have taken time to ask ED staff for an operator s manual for the defibrillator and read it after he arrived in the ED to perform a cardioversion Fairbanks RJ and Wears RL. Hazards With Medical Devices: the Role of Design. Annals of Emergency Medicine Nov 2008; 52(5):
19 Response #2 the preventative or corrective action is provided in the device labeling Fairbanks RJ and Wears RL. Hazards With Medical Devices: the Role of Design. Annals of Emergency Medicine Nov 2008; 52(5):
20


21
22 Defibrillator Case= COMMON ERROR Trend found in EMS Reporting system Simulation study (Denmark) 72 physicians 5 of 192 defib attempts Turned it off Measurable delay in shock Devices turn off even if charged and ready Hoyer, Christensen, et al. Annals of Emergency Medicine 2008; 52(5): Fairbanks and Wears. Annals of Emergency Medicine 2008; 52(5):
23 Safety Attitudes The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. --Lucian Leape, Testimony to congress
24 Why is a culture of safety so important? 1 serious or major injury 10 minor injuries 30 property damage injuries 600 incidents with no visible damage or injury Bird, ,753,498 accidents from 297 companies, 21 different industries Slide acknowledgment: Robert Panzer, MD
25 US Airways Non-Reprisal Policy US Airways will not initiate disciplinary proceedings against any employee who discloses an incident or occurrence involving flight safety This policy excludes events known or suspected to involve criminal activity, substance abuse, controlled substances, alcohol, or intentional falsification. Bad Apples Safety
26 Airline Safety Approaches It is vastly more important to identify the hazards and threats to safety, than to identify and punish an individual for a mistake. We exchange the ability to reprimand an individual for the ability to gain greater knowledge. --Jeff Skiles, Miracle on Hudson first officer, On airline safety philosophy


27 Too soft, you say?


28 Just Culture: The Three Behaviors Normal Error At-Risk Behavior Reckless Behavior Inadvertent action: slip, lapse, mistake A choice: risk not recognized or believed justified Conscious disregard of unreasonable risk Manage through changes in: Manage through: Manage through: Processes Procedures Recurrent training Design Environment Removing incentives for At- Risk Behaviors Creating incentives for healthy behaviors Increasing situational awareness Re-examining environment Griffith University Remedial action Punitive action Support Coach Sanction Adapted from: David Marx, Just Culture. Outcome Engineering 2008: Alternative Perspective: Just Culture: Balancing Safety and Accountability, Sidney Dekker (2008)

29



30 SAFE SYSTEM & PROCESS DESIGN SELECTION, TRAINING, ETC HAZARD REPORTING OPEN SAFETY CULTURE Identify & mitigate Existing hazards Before adverse events occur PATIENT COMPLAINTS

31 Indiana: 5 nurses
32 We See What We Expect To See Aoccdrnig to rscheearch at Cmabrigde Uinervtisy, it deosn't mttaer in waht oredr the ltteers in a wrod are, the olny iprmoetnt tihng is taht the frist and lsat ltteer be at the rghit pclae. The rset can be a toatl mses and you can sitll raed it wouthit a porbelm. Tihs is bcuseae the huamn mnid deos not raed ervey lteter by istlef, but the wrod as a wlohe.
33 Healthcare: Complex adaptive system Unordered: Cannot predict cause & Effect & Cannot be modeled or forecasted Ordered & Constrained & Can be reduced to a set of rules Adaptive in that their individual and collective behavior changes as a result of experience Figure: Sardone G, Wong G, 2010; See also: Snowden D, cognitive-edge.com ; Hollnagel, Woods, Leveson 2006; Plsek, Greenhalgh Sardone G, Wong G, Making sense of safety: a complexity based approach to safety interventions. Proceedings of the Association of Canadian Ergonomists 41st Annual Conference, Kelowna, BC, October 2010; 2. Snowden D, cognitive-edge.com 3. Hollnagel, Woods, Leveson 2006
34 Complex Adaptive Systems: work as done vs- work as imagined How managers believe work is being done (rules) GAP Resilience Every-day work: How work IS being done Adapted from: Ivan Pupulidy

35 How the gap reduces margin 12n meds Allow 11a-1p RN compliance Measured Introduce barcoding Patterson ES, et al (2006). Compliance with intended use of bar code medication administration in acute and long-term care. Human Factors, 48(1),
36 Complex Adaptive Systems Imposed solutions may not cover all circumstances They arise from the circumstances (emergence) Relationship between causes & effects can appear evident in retrospect hindsight does not lead to foresight the external conditions and the system itself constantly change. 1. Sardone G, Wong G, Making sense of safety: a complexity based approach to safety interventions. Proceedings of the Association of Canadian Ergonomists 41st Annual Conference, Kelowna, BC, Oct Snowden D, cognitive-edge.com
37 Resilience Engineering Safety I: Why did they give the wrong vial? Safety II: Why did they give the right vial all the other times?


38 People: Sources of Error. or sources of resilience If you weed out all the error prone health professionals, there won t be anyone left

39 sensitive dependence on initial conditions, unruly technology, tipping points, diversity failure emerges opportunistically, nonrandomly, from the very webs of relationships that breed success and that are supposed to protect organizations from disaster.
40 Skills-Based Error = Slips and Lapses = Automaticity Errors HUGE OPPORTUNITY

41 Usability Services Activities

42 GemStar Replacement Project 42
43 CADD Solis No major safety issues found Users able to perform tasks without safety critical errors Clinician user satisfaction not as high as the Sapphire 43
44 Hospira Sapphire 3 major safety hazards found Users observed committing safety-critical errors High user satisfaction 44
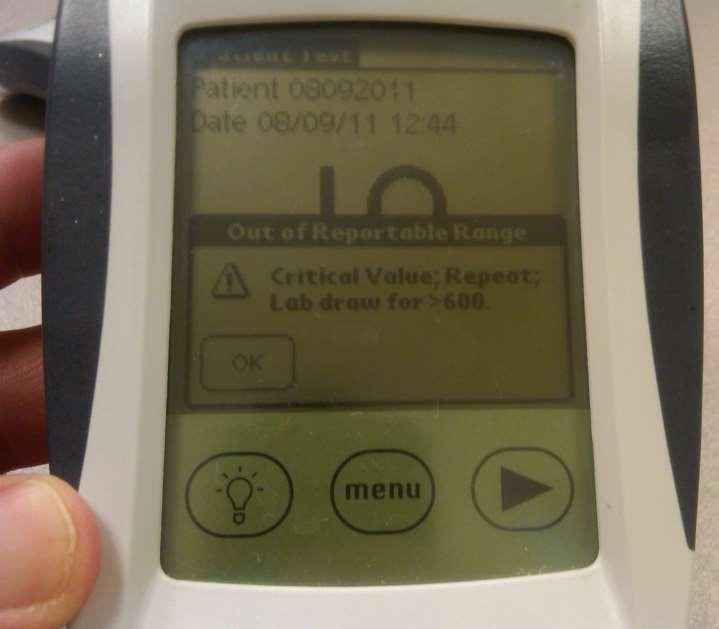
45 Glucometer Case Patient with hx of poorly-controlled BG levels Admitted to diabetic unit at hospital Pt appears normal or hyperglycemic Accucheck indicates critically low BG Misinterpreted by tech and RN as critical high Pt given repeated doses of insulin Altered, rapid response called Receives D50, Glucagon, & D10 drip Stays in ICU for 3 days: MAJOR EVENT
46 Nurse SUSPENDED
47 One week later Repeated Incident Same scenario, different unity Multiple RNs, NP involved All misinterpreted critical LO as critical HI Did disciplinary response make us safer?
48 The Second Story Patient has multiple signs of normal-high BG Initial ED values = hyperglycemia I know my sugars, and I m not low Ate all meals, snacks There was an ongoing failure to revise Due to fixation effect and expectations Glucometer design plays into this failure to revise Actions taken initially have no effect Fresh personnel discover true problem
49 Critical Low 0.1% (119/80,000) Within Reportable Range Critical High Critical Low
50


51 How could you miss it?
52 video
53 Procurement: Who determines wording? l Hospital Text of Out Text of of Reportable Out of Reportable Range message Range popup message popup A Critical value; Critical Repeat; value; Lab Repeat; Draw for Lab > Draw 600. for > 600. B RR Lo = result RR Lo <40; = result RR Hi <40; = result RR Hi >600 = result >600 C D E F Out of range: Out repeat of range: test repeat to confirm test to confirm Critical value; Critical repeat value; within repeat 15 mins; within notification 15 mins; notification required; lab required; draw for >600 for >600 Critical value; Critical you value; must repeat you must immediately; repeat immediately; STAT glucose STAT Lab glucose draw for RR HI for RR HI Repeat test Repeat test
54 We See What We Expect To See Aoccdrnig to rscheearch at Cmabrigde Uinervtisy, it deosn't mttaer in waht oredr the ltteers in a wrod are, the olny iprmoetnt tihng is taht the frist and lsat ltteer be at the rghit pclae. The rset can be a toatl mses and you can sitll raed it wouthit a porbelm. Tihs is bcuseae the huamn mnid deos not raed ervey lteter by istlef, but the wrod as a wlohe.
 https://www.youtube.com/watch?")
55 Video showing impact on the safety culture (Annie s story) 55

56 Fallibility is part of the human condition; We cannot change the human condition; But we can change the conditions under which people work --James Reason, PhD

57 Insanity Continuing to do the same thing and expecting different results. --Einstein
58 Develop Sustainable Solutions Develop Effective Solutions Consider Solutions in Context Focus on HAZARDS
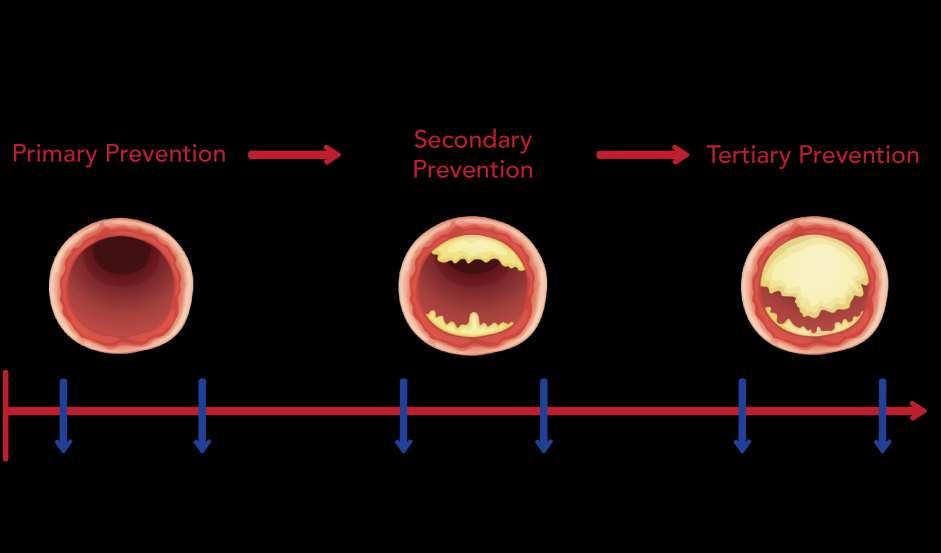
59 3 things leaders can do 1. Shift resources to 1 o and 2 o prevention 2. Implement Just Culture and start the change Senior Leaders to frontline workers 3. Formally implement an event review process based on safety science It will change the culture NPSF s new RCA squared (npsf.org) AHRQ s new CANDOR (Fall 2015 release)
 Fairbanks, MD, MS Director, National Center for Human Factors Engineering in Healthcare Director, Simulation Training & Education Lab (SiTEL) MedStar Institute for Innovation, MedStar Health")
60 Rollin J. (Terry) Fairbanks, MD, MS Director, National Center for Human Factors Engineering in Healthcare Director, Simulation Training & Education Lab (SiTEL) MedStar Institute for Innovation, MedStar Health / Washington DC USA Associate Professor of Emergency Medicine, Georgetown University Attending Emergency Physician, MedStar Washington Hospital Center Fairbanks.au@MedicalHFE.org (until 8/20/15) Terry.Fairbanks@MedicalHFE.org
Applying Human Factors to Healthcare Systems Safety
 April 29 th, 2014 To Better is Human TM Applying Human Factors to Healthcare Systems Safety A. Zach Hettinger, MD MS Medical Director National Center for Human Factors in Healthcare MedStar Institute for
April 29 th, 2014 To Better is Human TM Applying Human Factors to Healthcare Systems Safety A. Zach Hettinger, MD MS Medical Director National Center for Human Factors in Healthcare MedStar Institute for
Embracing a Culture of Safety and Learning
 Embracing a Culture of Safety and Learning Provincial Forum on Adverse Health Event Management St. John s Newfoundland May 26, 2008 Ward Flemons MD, FRCPC Vice-President, Health Outcomes Outline Adverse
Embracing a Culture of Safety and Learning Provincial Forum on Adverse Health Event Management St. John s Newfoundland May 26, 2008 Ward Flemons MD, FRCPC Vice-President, Health Outcomes Outline Adverse
Human Factor and Patient Safety. Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA)
") Human Factor and Patient Safety Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA) Human Factors and Patient Safety Unforeseen ice problem caused
Human Factor and Patient Safety Christopher Ente Imperial College Healthcare London Director Patient Safety and Quality for Africa (PASQUA) Human Factors and Patient Safety Unforeseen ice problem caused
TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation
 TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation Donna Woods, EdM, PhD Assistant Professor and Co Director, Graduate Programs In Healthcare Quality
TRANSFORMING HEALTHCARE: Educating the Healthcare Workforce For Quality and Safety Practice and Innovation Donna Woods, EdM, PhD Assistant Professor and Co Director, Graduate Programs In Healthcare Quality
The Human Factor: Applying Safety Science in Health Care
 The Human Factor: Applying Safety Science in Health Care Sarah Henrickson Parker, PhD Director of Education and Academic Affairs, Research Scientist National Center for Human Factors Engineering in Healthcare
The Human Factor: Applying Safety Science in Health Care Sarah Henrickson Parker, PhD Director of Education and Academic Affairs, Research Scientist National Center for Human Factors Engineering in Healthcare
Medication Safety: Lessons Learned
 Medication Safety: Lessons Learned CINA 30 th Anniversary Conference October 20 th, 2005 Christine Koczmara,, RN, BScPsy Medication Safety: Lessons Learned ISMP Canada Research Highlights Making Health
Medication Safety: Lessons Learned CINA 30 th Anniversary Conference October 20 th, 2005 Christine Koczmara,, RN, BScPsy Medication Safety: Lessons Learned ISMP Canada Research Highlights Making Health
What s the data telling you? Using evidence-based stories for health planning and decision-making
 MANITOBA CENTRE FOR HEALTH POLICY What s the data telling you? Using evidence-based stories for health planning and decision-making Bayline RRT Meeting Randy Fransoo May 25, 2007 Manitoba Centre for Health
MANITOBA CENTRE FOR HEALTH POLICY What s the data telling you? Using evidence-based stories for health planning and decision-making Bayline RRT Meeting Randy Fransoo May 25, 2007 Manitoba Centre for Health
2017 Pharmacy Education Series
 2017 Pharmacy Education Series Featured Speaker: Christina Michalek, BS, RPh, FASHP Medication Safety Specialist Institute for Safe Medication Practices October 18, 2017 Improving Patient Safety: Preventing
2017 Pharmacy Education Series Featured Speaker: Christina Michalek, BS, RPh, FASHP Medication Safety Specialist Institute for Safe Medication Practices October 18, 2017 Improving Patient Safety: Preventing
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10
 Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Response to Safety Events Just Culture HR Policy 5.24 Page 1 of 10 Policy : 5.24 Subject: Supersedes: Effective: October 8, 2008 Revised: July 1, 2002, December 1, 2012 Reviewed: December 1, 2012 Response
Just and Accountable Culture (JAC): An Introduction
: An Introduction") Just and Accountable Culture (JAC): An Introduction Maureen S Padilla, DNP, RN, NEA-BC Sr. VP and Chief Nurse Executive Co-Chair, Just & Accountable Steering Committee Yvonne Chu, MD, MBA Chief, Ophthalmology
Just and Accountable Culture (JAC): An Introduction Maureen S Padilla, DNP, RN, NEA-BC Sr. VP and Chief Nurse Executive Co-Chair, Just & Accountable Steering Committee Yvonne Chu, MD, MBA Chief, Ophthalmology
(10+ years since IOM)
") Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
How Should Policy Reflect a Culture of Safety?
 How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
According to Lucian Leape, Professor of Health Policy at
 A Statewide Approach to a Just Culture for Patient Safety: The Missouri Story Rebecca Miller, MHA, CPHQ, FACHE; Scott Griffith, MS; and Amy Vogelsmeier, PhD, RN The Missouri Just Culture Collaborative
A Statewide Approach to a Just Culture for Patient Safety: The Missouri Story Rebecca Miller, MHA, CPHQ, FACHE; Scott Griffith, MS; and Amy Vogelsmeier, PhD, RN The Missouri Just Culture Collaborative
Shifting from Blame-&-Shame to a Just-and-Safe Culture
 Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Washington Patient Safety Coalition December 10, 2014
 Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
Innovating the RCA: Root Cause Analysis & Just Culture Washington Patient Safety Coalition December 10, 2014 Andrea Halliday, MD Interim Patient Safety Officer, PeaceHealth David Allison, CPHRM Interim
10/4/2012. Disclosure. Leading a Meaningful Event Investigation. Just Culture definition. Objectives. What we all have in common
 Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
When words and actions matter most: The Case for CANDOR
 January 20, 2017 When words and actions matter most: The Case for CANDOR Timothy B McDonald, MD Director, Center for Open and Honest Communication in Healthcare MedStar Health, Institute for Quality and
January 20, 2017 When words and actions matter most: The Case for CANDOR Timothy B McDonald, MD Director, Center for Open and Honest Communication in Healthcare MedStar Health, Institute for Quality and
What Every Patient Safety Officer Must Know:
 What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
Culture of Safety: What s in Your Toolbox?
 Culture of Safety: What s in Your Toolbox? Kathy Ghomeshi, PharmD, BCPS Medication Safety Specialist Victoria Serrano Adams, PharmD, FASHP, FCSHP Director of Pharmaceutical Services UCSF Medical Center
Culture of Safety: What s in Your Toolbox? Kathy Ghomeshi, PharmD, BCPS Medication Safety Specialist Victoria Serrano Adams, PharmD, FASHP, FCSHP Director of Pharmaceutical Services UCSF Medical Center
Text-based Document. The Culture of Incident Reporting Among Filipino Nurses. de Guzman, Barbara Michelle. Downloaded 28-Apr :54:41
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Protecting the Public through Disciplinary Action. Maryann Alexander, PhD, RN, FAAN Kathleen Russell, JD, RN
 Protecting the Public through Disciplinary Action Maryann Alexander, PhD, RN, FAAN Kathleen Russell, JD, RN The Board s Duty Is To Protect The Public Not Punish The Licensee Criminal Justice System Punishment
Protecting the Public through Disciplinary Action Maryann Alexander, PhD, RN, FAAN Kathleen Russell, JD, RN The Board s Duty Is To Protect The Public Not Punish The Licensee Criminal Justice System Punishment
A culture of safety is a culture of compassion
 A culture of safety is a culture of compassion Compassion in Action Webinar Series March 21, 2017 1 Moderator Andrea Greenberg Communications and Partnerships Associate The Schwartz Center for Compassionate
A culture of safety is a culture of compassion Compassion in Action Webinar Series March 21, 2017 1 Moderator Andrea Greenberg Communications and Partnerships Associate The Schwartz Center for Compassionate
Patrol Procedures SURVIVAL TRIANGLE ATTITUDE. FBI/UCR Report of Officers Killed and Assaulted. Officers Killed and Assaulted
 Patrol Procedures SURVIVAL TRIANGLE ATTITUDE Statistics (2011) LOD are UP 6% As of August 0, 2011 at 112 Auto Related Deaths are DOWN 17% As of August 08, 2011 at 40 Gunfire Deaths are UP 21% As of August
Patrol Procedures SURVIVAL TRIANGLE ATTITUDE Statistics (2011) LOD are UP 6% As of August 0, 2011 at 112 Auto Related Deaths are DOWN 17% As of August 08, 2011 at 40 Gunfire Deaths are UP 21% As of August
The Newcastle upon Tyne Hospitals NHS Foundation Trust
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Incidents, Accidents and the Trust Disciplinary Process - Guidelines for Managers, Clinical Directors and Employees Version.: 4.1 Effective From:
The Newcastle upon Tyne Hospitals NHS Foundation Trust Incidents, Accidents and the Trust Disciplinary Process - Guidelines for Managers, Clinical Directors and Employees Version.: 4.1 Effective From:
Anatomy of a Fatal Medication Error
 Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
JUST CULTURE FEBRUARY 20, 2013 KAREN ZANIN RN CNOR
 JUST CULTURE FEBRUARY 20, 2013 KAREN ZANIN RN CNOR Balance A Just Culture balances the need to learn from mistakes with the need to take corrective action against an individual if the individual s conduct
JUST CULTURE FEBRUARY 20, 2013 KAREN ZANIN RN CNOR Balance A Just Culture balances the need to learn from mistakes with the need to take corrective action against an individual if the individual s conduct
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Presentation to the Maryland Patient Safety Center 14 th Annual Patient Safety Conference, Baltimore, Maryland Rosemary Gibson, Author, Wall of
 Presentation to the Maryland Patient Safety Center 14 th Annual Patient Safety Conference, Baltimore, Maryland Rosemary Gibson, Author, Wall of Silence Senior Advisor, The Hastings Center April 13, 2018
Presentation to the Maryland Patient Safety Center 14 th Annual Patient Safety Conference, Baltimore, Maryland Rosemary Gibson, Author, Wall of Silence Senior Advisor, The Hastings Center April 13, 2018
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Incident Reporting Systems and Future Strategies for Patient Safety Improvement
 WHITE PAPER: Incident Reporting Systems and Future Strategies for Patient Safety Improvement Author: Datix Date: 2016/17 Driving down harm How can healthcare providers most successfully pursue the goal
WHITE PAPER: Incident Reporting Systems and Future Strategies for Patient Safety Improvement Author: Datix Date: 2016/17 Driving down harm How can healthcare providers most successfully pursue the goal
Ambulatory Patient Safety
 We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
Disclosures. Medication Incident. Objectives 4/23/2015. No conflicts to disclose
 Disclosures No conflicts to disclose Kara Browne Senior Pharmacy Technician Saskatoon Cancer Centre Objectives Overview of common medication incidents and their causes Overview of available pharmacy technology
Disclosures No conflicts to disclose Kara Browne Senior Pharmacy Technician Saskatoon Cancer Centre Objectives Overview of common medication incidents and their causes Overview of available pharmacy technology
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM
 CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
Kate Beaumont. Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign.
 Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003
 Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003 Susan M. Proulx, Pharm.D. President, Med-E.R.R.S. Subsidiary of ISMP (www.med-errs.com) Mission of ISMP Translate errors into education
Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003 Susan M. Proulx, Pharm.D. President, Med-E.R.R.S. Subsidiary of ISMP (www.med-errs.com) Mission of ISMP Translate errors into education
Focus on Diagnostic Errors: Understanding and Prevention
 Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
Human Factors and Ergonomics in Health Care and Patient Safety
 Human Factors and Ergonomics in Health Care and Patient Safety Pascale Carayon, Ph.D. Procter & Gamble Bascom Professor in Total Quality Department of Industrial and Systems Engineering Director of the
Human Factors and Ergonomics in Health Care and Patient Safety Pascale Carayon, Ph.D. Procter & Gamble Bascom Professor in Total Quality Department of Industrial and Systems Engineering Director of the
Understanding the Causes of Events. Objectives
 Introduction to Root Cause Analysis (RCA) Understanding the Causes of Events HSAG Pressure Ulcer Collaborative August 19, 2009 Andrea B. Silvey, PhD, MSN HSAG Chief Quality Improvement Officer 1 Objectives
Introduction to Root Cause Analysis (RCA) Understanding the Causes of Events HSAG Pressure Ulcer Collaborative August 19, 2009 Andrea B. Silvey, PhD, MSN HSAG Chief Quality Improvement Officer 1 Objectives
How BPOC Reduces Bedside Medication Errors White Paper
 How BPOC Reduces Bedside Medication Errors White Paper July 2008 Brad Blackwell, M.S., R.Ph. Eloise Keeler, R.N., B.S.N. Abstract Medication errors are a significant source of harm to patients in U.S hospitals,
How BPOC Reduces Bedside Medication Errors White Paper July 2008 Brad Blackwell, M.S., R.Ph. Eloise Keeler, R.N., B.S.N. Abstract Medication errors are a significant source of harm to patients in U.S hospitals,
JUST CULTURE DECEMBER 12,2012
 JUST CULTURE DECEMBER 12,2012 P R E S E N T E D B Y : K A T H Y F O W L E R : Q I P R O J E C T M A N A G E R M A R G R E T T U C K E R : W O U N D C A R E N U R S E P A U L L E V Y : N U R S E E D U C
JUST CULTURE DECEMBER 12,2012 P R E S E N T E D B Y : K A T H Y F O W L E R : Q I P R O J E C T M A N A G E R M A R G R E T T U C K E R : W O U N D C A R E N U R S E P A U L L E V Y : N U R S E E D U C
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Medication Safety in LTC. Objectives. About ISMP Canada
 Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Care of the Caregiver STARTS and ENDS with full leadership support and involvement!
 Care of the Caregiver STARTS and ENDS with full leadership support and involvement! Care of the caregiver following an unintentional error or near miss should ideally incorporate: Unsafe Acts Algorithm
Care of the Caregiver STARTS and ENDS with full leadership support and involvement! Care of the caregiver following an unintentional error or near miss should ideally incorporate: Unsafe Acts Algorithm
HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots
 HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots Sharon Burnett, R.N., BSN, MBA Vice President of Clinical and Regulatory Affairs Missouri Hospital Association Objectives Discuss how the results of the
HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots Sharon Burnett, R.N., BSN, MBA Vice President of Clinical and Regulatory Affairs Missouri Hospital Association Objectives Discuss how the results of the
Anne Huben-Kearney, RN, BSN, MPA, CPHQ, CPHRM Assistant Vice President, Healthcare Risk Management AWAC Services, a member company of Allied World
 Slide 1 Human Factors: The Science of Reliability MSHRM February 2015 Anne Huben-Kearney, RN, BSN, MPA, CPHQ, CPHRM Assistant Vice President, Healthcare Risk Management AWAC Services, a member company
Slide 1 Human Factors: The Science of Reliability MSHRM February 2015 Anne Huben-Kearney, RN, BSN, MPA, CPHQ, CPHRM Assistant Vice President, Healthcare Risk Management AWAC Services, a member company
Overcoming Barriers to Error Reporting: Individual, Organizational and Regulatory Issues
 Overcoming Barriers to Error Reporting: Individual, Organizational and Regulatory Issues Jason M. Etchegaray, PhD Krisanne Graves, RN, BSN, CPHQ Debora Simmons, RN, MSN, CCRN, CCNS Institute for Healthcare
Overcoming Barriers to Error Reporting: Individual, Organizational and Regulatory Issues Jason M. Etchegaray, PhD Krisanne Graves, RN, BSN, CPHQ Debora Simmons, RN, MSN, CCRN, CCNS Institute for Healthcare
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
The American Association of Nurse Attorneys
 TAANA Position Paper on Samuel s Law Executive Summary The American Association of Nurse Attorneys supports efforts to prevent fatal medication errors. However, the approach of S. 371 is counterproductive
TAANA Position Paper on Samuel s Law Executive Summary The American Association of Nurse Attorneys supports efforts to prevent fatal medication errors. However, the approach of S. 371 is counterproductive
A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care
 A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care Gordy Schiff, MD, Associate Director of Brigham and Women s Center for Patient Safety Research
A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care Gordy Schiff, MD, Associate Director of Brigham and Women s Center for Patient Safety Research
Eileen C. Kugler, RN, MSN, MPH, FNP Manager, Practice
 Nursing Regulation Update Eileen C. Kugler, RN, MSN, MPH, FNP Manager, Practice Nurse Executives Legal Conference November 8, 2010 Mission The mission of the North Carolina Board of Nursing is to protect
Nursing Regulation Update Eileen C. Kugler, RN, MSN, MPH, FNP Manager, Practice Nurse Executives Legal Conference November 8, 2010 Mission The mission of the North Carolina Board of Nursing is to protect
High Reliability Organizing (HRO) in the Ambulatory Setting
 in the Ambulatory Setting") High Reliability Organizing (HRO) in the Ambulatory Setting High Reliability Training Sisters of Charity Leavenworth Health System 25 May 2016 2014 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
High Reliability Organizing (HRO) in the Ambulatory Setting High Reliability Training Sisters of Charity Leavenworth Health System 25 May 2016 2014 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Human Factors. Frank Federico, RPh. This presenter has nothing to disclose.
 Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
Reducing the risk of serious medication errors in community pharmacy practice
 Reducing the risk of serious medication errors in community pharmacy practice Eastern Medicaid Pharmacy Administrators Association (EMPAA) November 1, 2017 Newport, Rhode Island Michael R. Cohen, RPh,
Reducing the risk of serious medication errors in community pharmacy practice Eastern Medicaid Pharmacy Administrators Association (EMPAA) November 1, 2017 Newport, Rhode Island Michael R. Cohen, RPh,
Keep watch and intervene early
 IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
Disclosure. Institute of Medicine (IOM) 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL
 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL") Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
Re-Engineering Medication Processes to Capitalize on Technology. Jane Englebright, PhD, RN Vice President, Quality HCA
 Re-Engineering Medication Processes to Capitalize on Technology Jane Englebright, PhD, RN Vice President, Quality HCA Who is HCA? % % % % U.K. % % % Switzerland % %% % % % % % %% % % % % % % % %% % % %
Re-Engineering Medication Processes to Capitalize on Technology Jane Englebright, PhD, RN Vice President, Quality HCA Who is HCA? % % % % U.K. % % % Switzerland % %% % % % % % %% % % % % % % % %% % % %
Disclosure of Adverse Events and Medical Errors. Albert W. Wu, MD, MPH
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
A23/B23: Patient Harm in US Hospitals: How Much? Objectives
 A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care
 Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care IHI Workshop 12/6/16 Gordon Schiff, MD, Associate Dir Brigham & Women s Ctr for Patient Safety Research
Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care IHI Workshop 12/6/16 Gordon Schiff, MD, Associate Dir Brigham & Women s Ctr for Patient Safety Research
Culture. Safety. Process. Culture of Safety and Improvement
 Culture Safety Process Culture of Safety and Improvement Objectives Define key elements in a Culture of Safety Describe your role in the culture and process of safety Identify three personal actions to
Culture Safety Process Culture of Safety and Improvement Objectives Define key elements in a Culture of Safety Describe your role in the culture and process of safety Identify three personal actions to
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Zukunftsperspektiven der Qualitatssicherung in Deutschland
 Zukunftsperspektiven der Qualitatssicherung in Deutschland Future of Quality Improvement in Germany Prof. Richard Grol Fragmentation in quality assessment and improvement Integration of initiatives and
Zukunftsperspektiven der Qualitatssicherung in Deutschland Future of Quality Improvement in Germany Prof. Richard Grol Fragmentation in quality assessment and improvement Integration of initiatives and
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers
 Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Adverse Events in Hospitals: How Many and Why Not Reported. Fran Griffin Senior Manager Clinical Programs, BD
 Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
TIME OUT! A Patient Safety Strategy. Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service
 TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
Engaging Leaders: From Turf Wars to Appreciative Inquiry
 Engaging Leaders: From Turf Wars to Appreciative Inquiry Principles of Leadership for a Quality and Safety Culture Harvard Safety Certificate Program 2010 Gwen Sherwood, PhD, RN, FAAN Gwen Sherwood, PhD,
Engaging Leaders: From Turf Wars to Appreciative Inquiry Principles of Leadership for a Quality and Safety Culture Harvard Safety Certificate Program 2010 Gwen Sherwood, PhD, RN, FAAN Gwen Sherwood, PhD,
Practical Approaches to Establishing a Culture of Safety*
 Practical Approaches to Establishing a Culture of Safety* Leading the Transformation to High-Reliability Care IHI National Forum 8 December 2014 Gregg S. Meyer, MD, MSc Chief Clinical Officer, Partners
Practical Approaches to Establishing a Culture of Safety* Leading the Transformation to High-Reliability Care IHI National Forum 8 December 2014 Gregg S. Meyer, MD, MSc Chief Clinical Officer, Partners
Refer to Appendix A for definitions of the terminology used throughout this policy.
 Category: BOARD POLICY ADMINISTRATIVE PARAMETERS Title: Stop the Line : Authority to Intervene to Ensure Patient Safety Approved by: PHSA Board of Directors Reference Number: AS 130 Last Approved: June
Category: BOARD POLICY ADMINISTRATIVE PARAMETERS Title: Stop the Line : Authority to Intervene to Ensure Patient Safety Approved by: PHSA Board of Directors Reference Number: AS 130 Last Approved: June
Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD
 Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Wired to Save Lives: A Virtual Hospital Experience
 Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
LEADERSHIP CHALLENGES IN PATIENT SAFETY
 LEADERSHIP CHALLENGES IN PATIENT SAFETY Kenneth W. Kizer, MD, MPH. California Hospital Patient Safety Organization Annual Meeting Sacramento, CA April 8, 2013 Presentation Charge Discuss some of the challenges
LEADERSHIP CHALLENGES IN PATIENT SAFETY Kenneth W. Kizer, MD, MPH. California Hospital Patient Safety Organization Annual Meeting Sacramento, CA April 8, 2013 Presentation Charge Discuss some of the challenges
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring
 Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Quality From the View Point of the Patient
 Rethinking Critical Care: Building a Foundation with Reliability Terry P. Clemmer, MD LDS Hospital Salt Lake City, Utah terry.clemmer@imail.org Quality From the View Point of the Patient Don t Kill Me
Rethinking Critical Care: Building a Foundation with Reliability Terry P. Clemmer, MD LDS Hospital Salt Lake City, Utah terry.clemmer@imail.org Quality From the View Point of the Patient Don t Kill Me
Patient Safety Initiatives of the VA National Center for Patient Safety
 Patient Safety Initiatives of the VA National Center for Patient Safety At the Quality Colloquium at Harvard University John Gosbee, MD, MS August 27, 2003 National Center for Patient Safety Department
Patient Safety Initiatives of the VA National Center for Patient Safety At the Quality Colloquium at Harvard University John Gosbee, MD, MS August 27, 2003 National Center for Patient Safety Department
6/17/2014. Resilient health care: forging new directions. Australian Institute of Health Innovation s mission
 Question 1: what s your definition of resilience, please? Resilient health care: forging new directions Australian Institute of Health Innovation Professor Jeffrey Braithwaite, PhD Professor of Health
Question 1: what s your definition of resilience, please? Resilient health care: forging new directions Australian Institute of Health Innovation Professor Jeffrey Braithwaite, PhD Professor of Health
Think proactively = prevent codes Elective intubation better than PEA arrest
 Kyla Terhune, MD Treat all the same Think proactively = prevent codes Elective intubation better than PEA arrest Floor patient going to ICU? Treat if you are waiting! Rapid Response if Needed Does this
Kyla Terhune, MD Treat all the same Think proactively = prevent codes Elective intubation better than PEA arrest Floor patient going to ICU? Treat if you are waiting! Rapid Response if Needed Does this
To err is human. When things go wrong: apology and communication. Apology and communication position statement
 When things go wrong: apology and communication Kristi Eldredge R.N., J.D., CPHRM Senior Risk and Safety Consultant Fresident To err is human position statement To err is human. Mistakes are part of the
When things go wrong: apology and communication Kristi Eldredge R.N., J.D., CPHRM Senior Risk and Safety Consultant Fresident To err is human position statement To err is human. Mistakes are part of the
Learning from Actual & Near Miss Events
 POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
POST-EVENT DEBRIEFING TOOL & INTERVIEW GUIDE Learning from Actual & Near Miss Events Using Debriefing Methodology Jeffrey Klenklen, MS, RN, NE-BC, CPHQ, CPHRM Senior Director of Patient Safety & Clinical
Using Transparency to Drive Patient Safety
 Session Code These presenter s have nothing to disclose Using Transparency to Drive Patient Safety Doug Salvador, MD MPH Chief Quality Officer, Baystate Health Chief Medical Officer, Baystate Medical Center
Session Code These presenter s have nothing to disclose Using Transparency to Drive Patient Safety Doug Salvador, MD MPH Chief Quality Officer, Baystate Health Chief Medical Officer, Baystate Medical Center
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
RIVER EDGE BOARD OF EDUCATION FILE CODE: 5141 River Edge, NJ 07661
 RIVER EDGE BOARD OF EDUCATION FILE CODE: 5141 River Edge, NJ 07661 Policy HEALTH The board of education believes that good health is vital to successful learning. In order to help district pupils achieve
RIVER EDGE BOARD OF EDUCATION FILE CODE: 5141 River Edge, NJ 07661 Policy HEALTH The board of education believes that good health is vital to successful learning. In order to help district pupils achieve
A Just Culture: Accountability for Patient Safety. Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012
 A Just Culture: Accountability for Patient Safety Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012 A Just Culture: Accountability for Patient Safety Today s Presenters:
A Just Culture: Accountability for Patient Safety Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012 A Just Culture: Accountability for Patient Safety Today s Presenters:
Clearing the Err Reporting Serious Adverse Events and Never Events in Today s Health Care System
 Legal Issues Clearing the Err Reporting Serious Adverse Events and Never Events in Today s Health Care System Lawrence H. Plawecki, RN, JD, LLM; and David W. Amrhein, MD Abstract Absent an infinitesimal
Legal Issues Clearing the Err Reporting Serious Adverse Events and Never Events in Today s Health Care System Lawrence H. Plawecki, RN, JD, LLM; and David W. Amrhein, MD Abstract Absent an infinitesimal
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
The Board s position applies to all nurse license holders and applicants for licensure.
 Disciplinary Sanctions for Lying and Falsification The Texas Board of Nursing (Board), in keeping with its mission to protect the public health, safety, and welfare, believes it is important to take a
Disciplinary Sanctions for Lying and Falsification The Texas Board of Nursing (Board), in keeping with its mission to protect the public health, safety, and welfare, believes it is important to take a
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
CROSSING THE QUALITY CHASM: HEALTH CARE FOR THE 21 ST CENTURY
 CROSSING THE QUALITY CHASM: HEALTH CARE FOR THE 21 ST CENTURY May 10, 2002 Donald M. Berwick, M.D. President & CEO Institute for Healthcare Improvement The Foundation IOM Roundtable President s Advisory
CROSSING THE QUALITY CHASM: HEALTH CARE FOR THE 21 ST CENTURY May 10, 2002 Donald M. Berwick, M.D. President & CEO Institute for Healthcare Improvement The Foundation IOM Roundtable President s Advisory
The Patient Safety Act Reporting and RCA Requirements
 The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Root Cause Analysis (Part I) event/rca_assisttool.doc
 event/rca_assisttool.doc") (Part I) http://www.jcaho.org/accredited+organizations/sentinel+ event/rca_assisttool.doc Edited by Dr. E. Terry DIO Dr. S.K. Oliver OME Examines the reasons an error occurred Suggests changes to the system
(Part I) http://www.jcaho.org/accredited+organizations/sentinel+ event/rca_assisttool.doc Edited by Dr. E. Terry DIO Dr. S.K. Oliver OME Examines the reasons an error occurred Suggests changes to the system
9/15/2017. Nursing Management Congress 2017 Interruptions in Clinical Practice. Interruptions in Clinical Practice. Review of the Literature
 Nursing Management Congress 2017 Interruptions in Clinical Practice Elizabeth A. Duthie, RN, Ph.D., CPPS Director of Patient Safety at Montefiore Health System Interruptions in Clinical Practice The speaker
Nursing Management Congress 2017 Interruptions in Clinical Practice Elizabeth A. Duthie, RN, Ph.D., CPPS Director of Patient Safety at Montefiore Health System Interruptions in Clinical Practice The speaker
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm
 Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive