Approaches to Extending Complex Care Models into the Community: Emerging Evidence
|
|
|
- Stanley Andrews
- 5 years ago
- Views:
Transcription

1 Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community: Emerging Evidence August 16, 2018, 12:30-2:00 pm ET Made possible with support from the Robert Wood Johnson Foundation



2 Questions? To submit a question online, please click the Q&A icon located at the bottom of the screen. Answers to questions that cannot be addressed due to time constraints will be shared after the webinar. 3




3 Agenda Welcome and Introductions Strategies for Supporting Outreach Workers for Complex Populations Q&A Building the Business Case for Community-Based Complex Care Interventions Q&A 4

4 About the Center for Health Care Strategies A nonprofit policy center dedicated to improving the health of low-income Americans 5

5 Project Overview Multi-site demonstration aimed at refining and spreading effective care models that address the complex health and social needs of highneed, high-cost patients Made possible with support from the Robert Wood Johnson Foundation 6






6 Meet Today s Presenters Caitlin Thomas-Henkel, Senior Program Officer, Center for Health Care Strategies Sandi Groenewold, MD, Expanded Care Team Physician Lead, ThedaCare Health System Kim Lewis, Program and Community Outreach Coordinator, VCU Health Laurie Moore, Project Coordinator, ThedaCare Health System Derek DeLia, PhD, Director of Health Economics and Health Systems Research, MedStar Health Research Institute 7
7 Advancing innovations in health care delivery for low-income Americans Strategies for Supporting Outreach Workers for Complex Populations 8



8 VCUHS Complex Care Clinic TakeCCARE (Complex Care Assisting and Reviewing Education) Beyond the Clinic Walls

9 VCC Complex Care Clinic Model designed to enhance management of patients with five or more chronic conditions. Focused on the population with the highest cost and utilization. Goal: Achieve the Triple Aim: Better Care: Decrease readmission rate, inpatient and ED utilization Better Health: Improve clinical outcomes: HgbA1c Hypertension Cholesterol, BMI Lower Cost: Reduce total cost of care 10
10 VCUHS Complex Care Program Principles Coordination across the care continuum Access to medication management Access to behavioral health services Coordination of post-hospital and longitudinal care Leverages information technology PCMH certification for primary care practices Uses data to measures and improves performance Develops interventions to address social determinants of health 11
11 Complex Care Clinic Supported by an Interdisciplinary team Physicians Nurse Practitioner Social Worker Clinical Psychology Fellow Pharmacist Clinical Nurse RN Case Manager Medical Outreach Worker Community Health Workers 12

12 Community Health Workers 2-FTE CHW s VCU Graduates- B.S. Health Sciences Certified- State of Virginia Examples of Required Competencies Identifies problems and resources to help patients solve problems with the goal of teaching the patient/family/others how to navigate the health care system independently. Works with enrollees to empower them to become an active participant in their health care. Utilizes reports including hospital activity and patient engagement to contact and/or visit patients directly to discuss program access, prevention services, and utilization of services. 13
13 CHW Engagement Process Each day, the team receives reports outlining patients who have arrived at and are discharged from the hospital for in-patient, observational stays and emergency department services. These reports are used by the team to identify patients that may be appropriate for the CHW TakeCCARE Program. CHWs engage at the bedside during the hospital encounter to introduce themselves and to schedule a home visit within two business days post discharge to reinforce medical care plans, address social needs and to identify barriers to care. After the initial home visit, they call the patient daily for one week (reporting back to the team during the morning huddle). With team approval, they perform weekly visits for six weeks up to 12 weeks or until the patient is able to self-manage. Patient is transitioned back to the complex care outreach worker. 14


14 Beyond Clinic Walls Engage Patients at Bedside 83 Engage patients in the clinic Engage Patients by Telephone 316 Engage Patients at Community Partner Sites 13 Engage Patients at the Home 360 Escort Patients to Community Resources and/or Specialty Appointments When needed 73 15
15 Social Needs Screening Tool 16
16 Reflection Logs- What: Brief voice recordings used to monitor the outreach workers weekly patient interactions, experiences, and needs. When: At the end of each week. Five to eight minute recordings done by each CHW. Why: To capture the weeks experiences and learnings and to help manage employee burnout and stress. How: Uses the voice recorder app on the CHW s cellphone saved to shared folder on office computers. What worked well this week? What didn t work well this week? Did you have any challenges with your technology? Do you need any additional supplies or equipment? 17
17 Reflection Logs: The Evolution What would you consider a particular success this week? Was there a particular situation this week that required more of your time than you expected? If so, what was it and what was the outcome? Did anything happen this week that made you feel especially stressed or frustrated with your work? Did anything happen this week that left you feeling especially proud or enthusiastic about your work? 18

18 In Her Own Words. Briana Did anything happen this week that left you feeling especially proud or enthusiastic about your work? I was most proud of the fact that the patient listened to me! When I saw that he didn t look good and didn t seem like he was feeling well, I called our nurse. She said to tell him to go to the ED and he listened to me. I found out later that while he wasn t admitted, his blood sugar had been elevated I m glad he listened, they don t always. 19
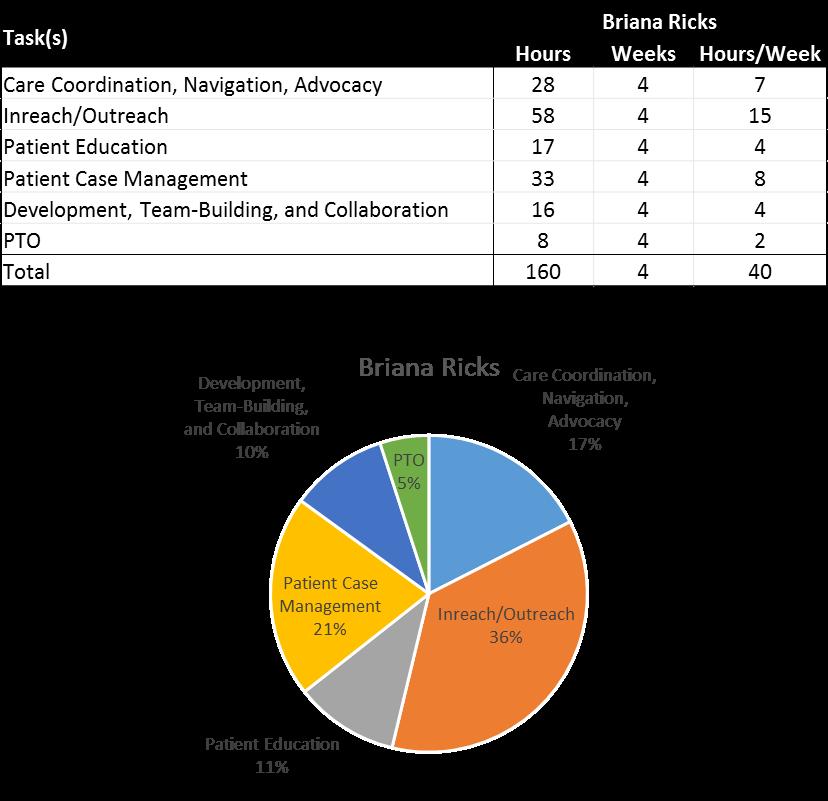
19 CHW Productivity 20
20 CHW Support Teambuilding with other outreach workers Educational opportunities at the individual and organizational level Staff recognition One-on-one discussions Reflection follow-up and coaching Special projects 21
21 Preliminary Evaluation Findings for VCU Health System Derek DeLia, PhD Director of Health Economics and Health Systems Research
22 VCUHS Preliminary quantitative evaluation Available data from VCU records Enrollment period: Aug Jul 2017 Comparison group: Historical, Aug Jul 2016 Observation: 6 months pre/post enrollment, baseline & 3-month social determinant measures Brief highlights from qualitative evaluation In-person interviews conducted in June 2017 Recorded, transcribed, & analyzed independently by two evaluators 23
23 VCUHS Patient Characteristics % Gender 51 Female 49 Male % Age % Insurance 26 Medicaid 24 Medicare 20 Dual Eligible 19 Uninsured patients from August 2016-July
24 Changes in Hospital Use at VCUHS Intervention N=39 Comparison N= ED visits per person 2.50 Admissions per person Intervention Comparison Intervention Comparison 6 months before 6 months after 6 months before 6 months after 25
25 Patient Activation and Social Service Needs: Intervention Patients at VCUHS At enrollment At exit (3 months) PAM score N=25 patients at both time points. PAM: Patient activation measure. At enrollment At exit (3 months) Food insecurity 25% 0% Utility needs 0% 0% Housing Stability 10% 5% Child Care 5% 0% Financial Issues 0% 5% Transportation 25% 0% Literacy 20% 10% Safety 5% 0% N=20 patients at both time points. 26
26 Qualitative findings for VCUHS MOWs extend clinic services into patients homes, provide early warnings to clinicians about breakdowns in patient care plans, and address idiosyncratic problems. MOWs translate medical information and have more open conversations than patients could have with clinicians. Barriers faced by TakeCCARE enrollees involve health literacy, medical transportation, and access to healthy food. Patients best suited for TakeCCARE are those who have low health literacy but high motivation and adequate family support. Relative to other CHW-type interventions, MOWs require a higher level of health system skills and draw significantly upon their college education. MOWs have substantial autonomy in how they manage their patient responsibilities. The time and criteria needed for patients to complete the TakeCCARE program are patient-specific and continue to evolve. 27
27 Questions? To submit a question online, please click the Q&A icon located at the bottom of the screen. Answers to questions that cannot be addressed due to time constraints will be shared after the webinar. 28
28 Advancing innovations in health care delivery for low-income Americans Building the Business Case for Community-Based Complex Care Interventions 29



29 Our Organization 7 hospitals 34 clinics 85+ onsite clinics 7,000 team members 240,000 patients annually 30








30 31 Our Organization

31 Our Background in Complex Care Community Paramedic 32

32 Gap Analysis Helped identify what type of program to create based on needs not currently being met by existing programs. Avoided duplicating services already in place 33

33 Our Community Paramedic Program Our Vision: To identify and fill the gaps in the current care delivery systems through creation of a Community Paramedic (CP) program utilizing nonemergent, team-based, patient-centered, mobile resources. The CP is part of the patient care team The CP presents in uniform and an identified vehicle not an ambulance Does not compete on any level with existing internal or community services 34
34 Best Use In partnership with patients Services performed at a visit: Assessment for social determinants of health Life and home risk evaluation Chronic disease management education and support Medication review Referral to ThedaCare and community services With the purpose of: Readmission prevention ED utilization reduction HbA1c improvement Better medication management Bridging to/from Home Services Connecting to community resources Increased patient independence 35



35 Our Electronic Connection Referral department Encounter posted as patient outreach Complete visit note Use of staff message and in-basket 36
36 Social Determinants of Health (Sample questions) 17. New barriers identified No barriers Financial Caregiver Transportation Cognitive disability Language Vision Emotional Cultural Disease state Family Pain Other 18. Life hazards No employment No home No community No transportation Inhalants (employment) Noise (employment) Fire concerns (home) Air pollution (home) Clutter (home) Noise (community) Clean water (community) Air pollution (community) Seatbelt use (transportation) Vision (transportation) Vehicle (transportation) 37



37 Keys to Success Taking a trauma-informed approach to care, using motivational interviewing to learn what is important to patients and identify their health care and personal life goals. 38
38 Engaging Leadership through Data Quantitative data supported by qualitative data Comparison group data Baseline comparison data (pre/pre-post intervention) Program data Financial data 39
39 Engaging Leadership through Data Quantitative data supported by qualitative data Wins and great stories Testimonials from patients, families, physicians Program plan and approach 40

40 Qualitative Data Recent case study success with cost reduction Patient X History: Prior to working with CP program, HbA1C ranged from best 9.9, to worst Last controlled HbA1c was May Paramedic actions at home visit: Full med-review Education Goal setting 100% from the patient using the Spirit of Motivational Interviewing Current state: First reading post-enrollment: 6.7 Second reading post enrollment: 6.2 Discontinued Trulicity ($8400/year) Discontinued Lantus ($3600/year) 41

41 Testimonials There s no way I would have been able to do this on my own. There s no way! - Patient Having eyes on a patient in their home environment assists in finally breaking down barriers that have prevented us from reaching ideal goals for patients. - Physician I can leave him alone now and go to my own appointments. - Patient s wife This is the most confident I have felt with my care team in years. -Patient This has created tighter connections between the clinic and home life and helps reiterate what we do. - Complex Care RN I am able to go back to church! - Patient 42
 Primary care redesign Physician engagement")
42 Building the Business Case Aligned our work with other current system initiatives Transitions of care management Value-based payment models (ACOs) Primary care redesign Physician engagement 43
43 Alignment with Systems of Care: Outpatient Care Management Community Paramedic 44
44 Aligning with the ACO Have numbers to show them Actual case studies with cost savings Identifying patient population Served Medicare/Medicaid/dually eligible Partner with ACO in identifying potential populations that we could/should serve Proforma 45
45 Aligning with the ACO Need Their Data Too! Utilizations outside your EMR and ability to capture on your own Payer specific interpretations of avoidable/preventable May validate what your own data and impressions are telling you Number of High Utilizer Patients (>=6 ED Visits/Year) Number of ED Visits Number of Non-ThedaCare ED Visits Number of Potentially Avoidable ED Visits Diabetes Dx CHF Dx CAD Dx COPD Dx Substance Abuse Dx Mental Health Dx Payer Payer Payer Payer Totals
46 Aligning with the ACO The Proforma Understand the opportunities 1 IP and 1 OP ALL IP ALL OP EXPECTED EXAMPLE # 1 EXAMPLE # 2 EXAMPLE #3 EXAMPLE #4 Account Type / Payor #1 Total Gross Charges Total Cases TOTAL Encounter Charge Shared Savings Facotr % Maximum Savings % of Population Populatio Adjusted n in ACO Savings Savings per Avoided Episode Savings Per Attributed Life Case (with a TCP Payor Provider) Mix Adovided Encounters Financial Return of Avoided Encounter Adovided Encounters Financial Return of Avoided Encounter Adovided Encounters Financial Return of Avoided Encounter Adovided Encounters Financial Return of Avoided Encounter Inpatient 1 1,000,000 1,000 12,000,000 80% 6,000,000 50% 3,000,000 3,000 6,000 71% 1 $ 4, $ 73,714 - $ - 7 $ 42, , ,000,000 25% 300, % 300,000 3,000 3,000 7% 0 $ $ 3,686 - $ - 1 $ 2, , ,000,000 50% 1,000, % 1,000,000 3,333 3,333 21% 0 $ $ 12,286 - $ - 2 $ 7,143 Outpatient 1 $ 5, $ 89,686 - $ - 10 $ 52, ,000,000 2,000 8,000,000 80% 1,000,000 50% 500, % 0 $ $ $ 69, $ 57, , ,000 25% 100, % 100, % 0 $ 24 - $ - 48 $ 6, $ 5, ,000 1,500 5,000,000 50% 200, % 200, % 0 $ 48 - $ $ 13, $ 11,429 1 $ $ $ 89, $ 74,286 Total Savings of Avoided Cases 5,524 89,686 89, ,429 Cost / FTE 90,000 90,000 90,000 Net Impact (314) (238) 36,429 47

47 Aligning with the ACO Understand their world Have ACO leader present at key meetings Have ACO share results with payers Prepare to take referrals from ACO push 48


48 49 Thank You!

49 Preliminary Evaluation Findings for ThedaCare Health System Derek DeLia, PhD Director of Health Economics and Health Systems Research
50 ThedaCare Preliminary quantitative evaluation Available data from ThedaCare records Enrollment period: Jan - Aug 2017 Comparison groups: Neenah IM patients, matched controls for diabetics Observation: Six months pre/post enrollment for utilization, 3-4 months for A1c measures Brief highlights from qualitative evaluation In-person interviews conducted in July 2017 Recorded, transcribed, & analyzed independently by two evaluators 51
51 ThedaCare Patient Characteristics % Gender 57 Female 43 Male % Age % Insurance 26 Medicaid 62 Medicare * Each includes Dual Eligibles due to small cell sizes 52
52 Changes in A1c Levels for Diabetics at ThedaCare Matched pair Intervention Comparison 18 intervention patients matched with 18 comparison patients based on initial A1c level (all>9), age, & sex. 53
53 Changes in Hospital Use for Patients at ThedaCare with a History of High ED Use High ED utilization defined as 3+ ED visits in 6 months Intervention N=19 Comparison N=20 8 ED visits per person 0.8 Admissions per person Intervention Comparison 0 Intervention Comparison 180 days before 180 days after 180 days before 180 days after 54
54 Qualitative Findings for ThedaCare CPs are deployed when ThedaCare clinicians sense a gap in patient care or compliance that requires detailed investigation that cannot be done in the clinic setting. CPs often address medication issues such as compliance, reconciliation, and dosage optimization. The paramedic uniform appears widely respected by patients and contributes to CP effectiveness in motivating patients to engage in healthy and medically compliant behaviors. CPs utilize some paramedic skills but must have a different temperament and learn different skills relative to traditional paramedics. The workflow for CP communication with the complex care team at ThedaCare depends heavily on their fully functioning EHR. 55
55 Questions? To submit a question online, please click the Q&A icon located at the bottom of the screen. Answers to questions that cannot be addressed due to time constraints will be shared after the webinar. 56
56 Part Two in the Series Addressing Social Determinants of Health: Connecting People with Complex Needs to Community Resources»September 10, 2018, 2:00 3:30 PM ET»Registration link will be sent to today s attendees Related resources»thedacare: Leveraging Community Paramedics to Bridge Persistent Gaps in Care»Virginia Commonwealth University Health System: Beyond the Walls and Into Communities 57




57 Visit CHCS.org to Download practical resources to improve the quality and costeffectiveness of Medicaid services Learn about cutting-edge efforts to improve care for Medicaid s highestneed, highest-cost beneficiaries Subscribe to CHCS , blog and social media updates to learn about new programs and resources Follow us on 58
Addressing Social Determinants of Health: Connecting People with Complex Needs to Community Resources
 Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Addressing Social Determinants of Health: Connecting People
Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Addressing Social Determinants of Health: Connecting People
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
September, James Misak, M.D. Linda Stokes, MSPH The MetroHealth System
 Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Designing a Medicaid ACO Program: Insights from Trailblazing States
 Designing a Medicaid ACO Program: Insights from Trailblazing States February 11, 2016, 3:30 5:00 pm ET For Audio Dial: 877-830-2582 Passcode: 805070 Made possible by The Commonwealth Fund www.chcs.org
Designing a Medicaid ACO Program: Insights from Trailblazing States February 11, 2016, 3:30 5:00 pm ET For Audio Dial: 877-830-2582 Passcode: 805070 Made possible by The Commonwealth Fund www.chcs.org
AccessHealth Spartanburg
 TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
Thursday, June 2, 2011, 2-3:30 PM ET
 CHCS Webinar: ROI Forecasting Calculator for Health Homes and Medical Homes Thursday, June 2, 2011, 2-3:30 PM ET For audio, dial: (866) 699-3239; Meeting/Event Number: 710 497 839. You may also listen
CHCS Webinar: ROI Forecasting Calculator for Health Homes and Medical Homes Thursday, June 2, 2011, 2-3:30 PM ET For audio, dial: (866) 699-3239; Meeting/Event Number: 710 497 839. You may also listen
PCMH to ACO: Carilion Clinic s Journey
 PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
CDC s 6 18 Initiative: Informational Webinar for Prospective States and Territories
 Advancing innovations in health care delivery for low-income Americans CDC s 6 18 Initiative: Informational Webinar for Prospective States and Territories July 23, 2018 Tricia McGinnis, MPP, MPH, Senior
Advancing innovations in health care delivery for low-income Americans CDC s 6 18 Initiative: Informational Webinar for Prospective States and Territories July 23, 2018 Tricia McGinnis, MPP, MPH, Senior
Opportunities for Medicaid-Public Health Collaboration to Achieve Mutual Prevention Goals: Lessons from CDC s 6 18 Initiative
 Advancing innovations in health care delivery for low-income Americans Opportunities for Medicaid-Public Health Collaboration to Achieve Mutual Prevention Goals: Lessons from CDC s 6 18 Initiative June
Advancing innovations in health care delivery for low-income Americans Opportunities for Medicaid-Public Health Collaboration to Achieve Mutual Prevention Goals: Lessons from CDC s 6 18 Initiative June
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States
: Reform Strategies for States") Advancing innovations in health care delivery for low-income Americans Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States March 6, 2018 Michelle Herman Soper and Alexandra
Advancing innovations in health care delivery for low-income Americans Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States March 6, 2018 Michelle Herman Soper and Alexandra
Using Community Health Workers and Volunteers to Reach Complex Needs Populations
 Advancing innovations in health care delivery for low-income Americans Workforce Innovations in Complex Care Series: Using Community Health Workers and Volunteers to Reach Complex Needs Populations April
Advancing innovations in health care delivery for low-income Americans Workforce Innovations in Complex Care Series: Using Community Health Workers and Volunteers to Reach Complex Needs Populations April
The Playbook: Better Care for People with Complex Needs
 The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
6 18 Evaluation and Impact Measurement
 6 18 Evaluation and Impact Measurement August 12, 2016 Center for Health Care Strategies Centers for Disease Control and Prevention Centers for Medicare and Medicaid Services Support provided by the Robert
6 18 Evaluation and Impact Measurement August 12, 2016 Center for Health Care Strategies Centers for Disease Control and Prevention Centers for Medicare and Medicaid Services Support provided by the Robert
Mild-to-Moderate Mental Health Coverage in Medi-Cal: The Challenge and Promise of Coordination between Counties and Health Plans
 Advancing innovations in health care delivery for low-income Americans Mild-to-Moderate Mental Health Coverage in Medi-Cal: The Challenge and Promise of Coordination between Counties and Health Plans December
Advancing innovations in health care delivery for low-income Americans Mild-to-Moderate Mental Health Coverage in Medi-Cal: The Challenge and Promise of Coordination between Counties and Health Plans December
Lessons from the Front Lines: Insights into Trauma-Informed Care for Medicaid s Complex Populations
 Lessons from the Front Lines: Insights into Trauma-Informed Care for Medicaid s Complex Populations June 22, 2015 Call-in Number: 1-800-310-6649; Passcode: 799834 Supported by Kaiser Permanente Community
Lessons from the Front Lines: Insights into Trauma-Informed Care for Medicaid s Complex Populations June 22, 2015 Call-in Number: 1-800-310-6649; Passcode: 799834 Supported by Kaiser Permanente Community
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
CONNECTED SM. Blue Care Connection SIMPLY AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT
 SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
Slide 1. Slide 2 Rural Princeton. Slide 3 Agenda Rural ACO RURAL ACOS CAN WORK AND LEAD THE WAY
 Slide 1 RURAL ACOS CAN WORK AND LEAD THE WAY Nebraska Rural Health Association September 20, 2017 Slide 2 Rural Princeton Slide 3 Agenda Rural ACO Illinois Rural Community Care Organization (IRCCO)/Statewide
Slide 1 RURAL ACOS CAN WORK AND LEAD THE WAY Nebraska Rural Health Association September 20, 2017 Slide 2 Rural Princeton Slide 3 Agenda Rural ACO Illinois Rural Community Care Organization (IRCCO)/Statewide
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
11/7/2016. Objectives. Patient-Centered Medical Home
 Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System
 Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System Roxanne Elliott, MS Policy Director FirstHealth of the Carolinas Goals For Today Review scope of project Integrate
Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System Roxanne Elliott, MS Policy Director FirstHealth of the Carolinas Goals For Today Review scope of project Integrate
Medicare Shared Savings Program ACO Learning System
 Medicare Shared Savings Program ACO Learning System Coordinating Care for Beneficiaries with Complex Care Needs Wednesday, June 24, 2015 2:30 4:00 PM ET Audio for this session can be streamed through your
Medicare Shared Savings Program ACO Learning System Coordinating Care for Beneficiaries with Complex Care Needs Wednesday, June 24, 2015 2:30 4:00 PM ET Audio for this session can be streamed through your
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
State Approaches to Providing Health-Related Supportive Services through Medicaid
 State Approaches to Providing Health-Related Supportive Services through Medicaid June 2, 2016 1:00-2:30 pm ET Made possible through The Commonwealth Fund For Audio Dial: 1-888-819-8046 Passcode: 916263
State Approaches to Providing Health-Related Supportive Services through Medicaid June 2, 2016 1:00-2:30 pm ET Made possible through The Commonwealth Fund For Audio Dial: 1-888-819-8046 Passcode: 916263
SWAN Alerts and Best Practices for Improved Care Coordination
 SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Essentia Health. A View on Information Technology. ND HIMS Conference April 12, Tim Sayler, COO Essentia Health - West
 Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement
 Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement #OMPerformance The 2017 OPEN MINDS Performance Management Institute
Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement #OMPerformance The 2017 OPEN MINDS Performance Management Institute
Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts
 Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts May 9, 2018 www.hcttf.org 1 Speakers Jeff Micklos Executive Director HCTTF Kelly McCracken National
Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts May 9, 2018 www.hcttf.org 1 Speakers Jeff Micklos Executive Director HCTTF Kelly McCracken National
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Building a Culture of Engagement for Medicare- Medicaid Enrollees: Health Plan Approaches
 TECHNICAL ASSISTANCE BRIEF August 2015 Building a Culture of Engagement for Medicare- Medicaid Enrollees: Health Plan Approaches By Sarah Barth and Brianna Ensslin, Center for Health Care Strategies I
TECHNICAL ASSISTANCE BRIEF August 2015 Building a Culture of Engagement for Medicare- Medicaid Enrollees: Health Plan Approaches By Sarah Barth and Brianna Ensslin, Center for Health Care Strategies I
Community Paramedicine: A New Approach to Serving Complex Populations
 Advancing innovations in health care delivery for low-income Americans Workforce Innovations in Complex Care Series: Community Paramedicine: A New Approach to Serving Complex Populations May 11, 2017,
Advancing innovations in health care delivery for low-income Americans Workforce Innovations in Complex Care Series: Community Paramedicine: A New Approach to Serving Complex Populations May 11, 2017,
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects. Submitted by:
 Tier One Milestone (STC-61) Application for Enhancement Projects. Submitted by:") 2012-2013 Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects Submitted by: Florida Health Sciences Center, Inc. d/b/a Tampa General Hospital July 31, 2012 1 1. Applicant:
2012-2013 Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects Submitted by: Florida Health Sciences Center, Inc. d/b/a Tampa General Hospital July 31, 2012 1 1. Applicant:
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study
 Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Primary Care Renewal. Building Successful Practices In The Era Of Accountability Creating Contagious Change
 Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Reforming Health Care with Savings to Pay for Better Health
 Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Medical Home Renovations: A Patient-centered Medical Home Case Study
 Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
FirstHealth Moore Regional Hospital. Implementation Plan
 FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
Effects of Patient Navigation on Chronic Disease Self Management
 Effects of Patient Navigation on Chronic Disease Self Management M. Christina R. Esperat, RN, PhD, FAAN, Professor and Associate Dean for Clinical Services, Texas Tech University Health Sciences Center
Effects of Patient Navigation on Chronic Disease Self Management M. Christina R. Esperat, RN, PhD, FAAN, Professor and Associate Dean for Clinical Services, Texas Tech University Health Sciences Center
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015
 Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Beyond Cost and Utilization: Rethinking Evaluation Strategies for Complex Care Programs
 Beyond Cost and Utilization: Rethinking Evaluation Strategies for Complex Care Programs April 9, 2-3:30 pm (ET) Made possible with support from Kaiser Permanente Community Health Housekeeping This event
Beyond Cost and Utilization: Rethinking Evaluation Strategies for Complex Care Programs April 9, 2-3:30 pm (ET) Made possible with support from Kaiser Permanente Community Health Housekeeping This event
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
HealthPartners and the Triple Aim. IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners
 HealthPartners and the Triple Aim IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners HealthPartners Not for profit, consumer governed Integrated care and financing
HealthPartners and the Triple Aim IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners HealthPartners Not for profit, consumer governed Integrated care and financing
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE (MOC) PROVIDER TRAINING
 MODEL OF CARE (MOC) PROVIDER TRAINING") SPECIAL NEEDS PLAN (SNP) MODEL OF CARE (MOC) PROVIDER TRAINING AlohaCare Advantage Plus (HMO SNP) Revised May 2018 HISTORY AlohaCare was formed by a network of Hawaii community health centers in 1994.
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE (MOC) PROVIDER TRAINING AlohaCare Advantage Plus (HMO SNP) Revised May 2018 HISTORY AlohaCare was formed by a network of Hawaii community health centers in 1994.
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Adopting a Care Coordination Strategy
 Adopting a Care Coordination Strategy Authors: Henna Zaidi, Manager, and Catherine Castillo, Senior Consultant Current state of health care The traditional approach to health care delivery is quickly becoming
Adopting a Care Coordination Strategy Authors: Henna Zaidi, Manager, and Catherine Castillo, Senior Consultant Current state of health care The traditional approach to health care delivery is quickly becoming
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Watch Program Overview.
 Watch Program Overview www.healthyharford.org Agenda Our mission Who is the WATCH team What does the WATCH team do Overview of program design Program goals/benefits Patient experience How to refer to WATCH
Watch Program Overview www.healthyharford.org Agenda Our mission Who is the WATCH team What does the WATCH team do Overview of program design Program goals/benefits Patient experience How to refer to WATCH
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Community Paramedicine: Lessons Learned from South Carolina
 Community Paramedicine: Lessons Learned from South Carolina Dr. Chris Oxendine, CP Medical Director Abbeville Area Medical Center Will Blackwell Abbeville County EMS Sarah M. Craig, MHA South Carolina
Community Paramedicine: Lessons Learned from South Carolina Dr. Chris Oxendine, CP Medical Director Abbeville Area Medical Center Will Blackwell Abbeville County EMS Sarah M. Craig, MHA South Carolina
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Health Coaching in Team-Based Care. Recipes for Success
 Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
Preliminary Evaluation Findings NJHI-Expecting Success in Cardiac Care
 Preliminary Evaluation Findings NJHI-Expecting Success in Cardiac Care Presentation to the NJHI-ES Learning Network May 12, 2009 Joel Cantor, ScD Professor and Director Acknowledgements Funded by the Robert
Preliminary Evaluation Findings NJHI-Expecting Success in Cardiac Care Presentation to the NJHI-ES Learning Network May 12, 2009 Joel Cantor, ScD Professor and Director Acknowledgements Funded by the Robert
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Kentucky Stroke Transitions Assistance Resource
 Kentucky Stroke Transitions Assistance Resource Patrick Kitzman, Ph.D., MSPT, Division of Physical Therapy, University of Kentucky Violet Sylvia, Ph.D., Director ARH System of Rehabilitation Services Kentucky
Kentucky Stroke Transitions Assistance Resource Patrick Kitzman, Ph.D., MSPT, Division of Physical Therapy, University of Kentucky Violet Sylvia, Ph.D., Director ARH System of Rehabilitation Services Kentucky
Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations. April 26, 2018
 Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations April 26, 2018 Agenda Welcome and Overview of Interview Results Claudia Ellison, Director of Programs,
Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations April 26, 2018 Agenda Welcome and Overview of Interview Results Claudia Ellison, Director of Programs,
Technology Fundamentals for Realizing ACO Success
 Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
Programs and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance Program
 s and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance HealthPartners Disease and Case Management programs are targeted to those who have been identified with a
s and Procedures for Chronic and High Cost Conditions Related to the Early Retiree Reinsurance HealthPartners Disease and Case Management programs are targeted to those who have been identified with a
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Ministry of Health Patients as Partners Provincial Dialogue Report
 Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
The Camden Coalition Of Healthcare Providers: An Organization Overview August I. Introduction: The Camden Coalition of Healthcare Providers
 The Camden Coalition Of Healthcare Providers: An Organization Overview August 2017 I. Introduction: The Camden Coalition of Healthcare Providers The Camden Coalition of Healthcare Providers (Camden Coalition)
The Camden Coalition Of Healthcare Providers: An Organization Overview August 2017 I. Introduction: The Camden Coalition of Healthcare Providers The Camden Coalition of Healthcare Providers (Camden Coalition)
Using Patient and Family Centered Care Fundamentals in Establishing an Office of Patient Experience
 Using Patient and Family Centered Care Fundamentals in Establishing an Office of Patient Experience Presenters: Keith Gran, CPA, MBA, Chief Patient Experience Officer Molly Dwyer-White, MPH, Administrative
Using Patient and Family Centered Care Fundamentals in Establishing an Office of Patient Experience Presenters: Keith Gran, CPA, MBA, Chief Patient Experience Officer Molly Dwyer-White, MPH, Administrative
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Building the Universal Roadmap to Population Health Management
 Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE
 SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE") MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach