Using Community Health Workers and Volunteers to Reach Complex Needs Populations
|
|
|
- Marion Taylor
- 5 years ago
- Views:
Transcription
1 Advancing innovations in health care delivery for low-income Americans Workforce Innovations in Complex Care Series: Using Community Health Workers and Volunteers to Reach Complex Needs Populations April 18, 2017, 1:00-2:30 pm ET For Audio Dial: Passcode: Made possible with support from Kaiser Permanente Community Benefit and the Robert Wood Johnson Foundation

2 Questions? To submit a question, please click the question mark icon located in the toolbar at the top of your screen. Answers to questions that cannot be addressed due to time constraints will be shared after the webinar. 2





3 Agenda Welcome and Introductions Cultivating a Resource Network for Complex Beneficiaries in a Rural Setting Leveraging Community Partnerships to Connect East Baltimore Residents to Health and Social Services Q&A 3

4 Advancing innovations in health care delivery for low-income Americans Welcome & Introductions 4



5 Meet the Team Rachel Davis, Associate Director for Program Innovation, Center for Health Care Strategies Caitlin Thomas-Henkel, Senior Program Officer, Center for Health Care Strategies David Adler, Senior Program Officer, Robert Wood Johnson Foundation 5

6 About the Center for Health Care Strategies A non-profit policy center dedicated to improving the health of low-income Americans 6
7 Select Complex Populations Initiatives Complex Care Innovation Lab Multi-year learning collaborative, supported by Kaiser Permanente Community Benefit, focused on improving care for low-income individuals with complex medical and social needs Transforming Complex Care Two-year multi-site pilot demonstration, funded by the Robert Wood Johnson Foundation, aimed at refining and spreading effective care models that address the needs of high-need, high-cost patients 7

8 Robert Wood Johnson Foundation s Culture of Health 8
9 Advancing innovations in health care delivery for low-income Americans Cultivating a Resource Network for Complex Beneficiaries in a Rural Setting 9


10 Today s Speakers Jane Emmert, Director, ASSIST Lara Shadwick, Program Director, Mountain-Pacific Quality Health 10

 for Montana, Wyoming, Alaska, Hawaii and the U.S.")
, an agency of the U.S. Department of Health and Human Services.")
11 IMPROVING CARE COORDINATION FOR HIGH- NEED POPULATIONS Lara Shadwick, MBA Mountain-Pacific Quality Health April 18, 2017 This material was developed by Mountain-Pacific Quality Health, the Medicare Quality Innovation Network-Quality Improvement Organization (QIN-QIO) for Montana, Wyoming, Alaska, Hawaii and the U.S. Pacific Territories of Guam, American Samoa and the Commonwealth of the Northern Mariana Islands, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. Contents presented do not necessarily reflect CMS policy. 111SOW-MPQHF-MT-HS-17-02

12 Who We Are Mountain-Pacific Quality Health is the Quality Innovation Network-Quality Improvement Organization (QIN-QIO) for four states and three territories Montana Wyoming Alaska Hawaii Guam American Samoa The Commonwealth of the Northern Mariana Islands 12


13 Montana Communities Kalispell RN ASSIST Coaches Helena RN Keeping You Home Billings RN Two CHWs as veteran peers 13

14 New Project Apply nationally renowned Camden Coalition of Healthcare Providers and Transitional Care Models to rural settings Test, fund and deploy ReSource Teams, functioning as community outreach teams Test, fund and deploy cellular-enabled ipads to work with patients remotely via video chat Spread best practices through training and education Work with payers to develop sustainable community health teams Save $$$$$ 14
")
15 Funding Sources for Pilots CMS Special Innovation Project Robert Wood Johnson Foundation Montana Healthcare Foundation Same criteria but looking beyond Medicare to Medicaid, uninsured and commercial patients Funding allows teams to work with all applicable patients Multi-payer/Comprehensive Primary Care Plus (CPC+) Sustainability 15






16 Community Health Worker Delivery System Models: Community ReSource Teams Primary Care Coach Community Resources RN BH 16
17 Coming to the Table as a Community MHIP (Medicaid) Home Options FQHC (HHA and Hospice) RN Western MT Mental Health ASSIST Flathead (volunteer CHWs) Hospital Case Management Nursing Home SUMMIT (coaches) Pathways (IP Psych) 17



18 INNOVATION AT WORK 18

19 ipads and Video Conferencing with Patients Build relationship through video chat (HIPPA compliant) Cellular enabled for rural area ipads go with CHWs to patient home visits and connect RN Clinical concerns can be addressed, allows for nonverbals to be recognized Makes RNs more efficient with travel time and better able to focus on clinical elements of care 19
20 Multi-site Case Conferences Monthly calls De-identified cases are presented Experts on the calls Nurse Behavioral Health Pharmacist Peers Supportive of the emotional nature of the work 20
21 Veterans at Work 1 in 10 Montana residents are veterans Veterans connect better with those who served Hiring medically retired veterans to functions as CHWs Career adaptation 1+1=a bigger 1 Flexibility for follow-up medical care 21

22 MISSION STATEMENT Dedicated staff and volunteers connect people to the resources necessary to regain their health and independence. 22

23 At ASSIST we believe in the power of volunteers to impact the lives of their neighbors who are trying to regain their health and independence. 23
24 . 24

25 25

26 How We Began ASSIST is a 501(c)(3) not-for-profit corporation founded in 2014 by Curtis Lund, a retired business entrepreneur. As an avid volunteer himself, he knew the benefit of volunteering to the volunteer and well as to the community. 26
27 Funding Mr. Lund funded the program himself for nearly two years and then ASSIST came under the Non- Profit Foundation umbrella of the Kalispell Regional Medical Center in October
28 The Referral Process Our patients (whom we call Care Receivers) are referred to us by medical staff at Kalispell Regional Healthcare, North Valley Hospital and associated clinics who recognize a patient that needs help connecting to community resources. 28

29 The Three Departments of ASSIST The ASSIST Program Neighbors Helping Neighbors Transportation ASSIST Center Volunteers and staff who visit patients in their homes and connect them to resources. Rides to doctor appointments A 10-bed facility that provides non-medical care for patients that need to leave the hospital but aren t quite ready to go home. 29
30 Neighbors Helping Neighbors Year People Served Hours of Service , ,136 Our average Care Receiver is 66 years old and makes approximately $1350/month. 30

31 Snapshot of Volunteers Our current volunteers are former: Teachers Physical therapists Occupational therapists Loggers Computer programmers, Bookkeepers Nurses 31
32 Volunteer Training Application, interview, reference check and background check 3-hour orientation with the Volunteer Supervisor On-the-job training with skills modeled by staff on each visit into Care Receiver s homes Monthly training lunches with presentations by community resource organizations Resource manual (over 200 pages) with specific community resource information divided by categories: basic needs, disability, families, financial, food, health care, housing, senior adults, transportation and veterans 32

33 What We Do Volunteers and staff visit Care Receivers in their homes and LISTEN to their concerns. Together, we create a Plan of Action. 33
34 Top Three Concerns and Needs 1 Apply for Medicaid PLAN OF ACTION Care Receiver Gather 6 months of bank statements, taxes, medical expenses and Soc. Security statement ASSIST team Pick up Medicaid app and help fill it out with Care Receiver 2 Food Refer them to Meals on Wheels and Food Bank 3 Steep steps to trailer Contact the mobile home repair team ACTIONS TAKEN by ASSIST team 3/1/17 Helped fill out Medicaid app, but they still need to get bank statements 3/3/17 Called Meals on Wheels and Food Bank for Senior Commodities. Delivery will start on 3/5/17 for Mon, W and the last Friday of the month for commodities. 34

35 We generally are done with intensive involvement within days, but we are always available for them to call and ask us for help. Our Care Receivers know that we care about them. 35

36 We make a difference because we are face to face with our Care Receivers in their homes. 36

37 We are Connectors ASSIST Volunteers connect the Care Receivers to agencies that provide needed services. 37

38 Volunteers may help Care Receivers fill out financial assistance forms or help them apply for Medicaid, Medicare or Social Security Disability resources. 38

39 Or connect them to home care or homemaker services through organizations like the Agency on Aging. 39

40 Or connect them with public transportation or the ASSIST shuttle for rides to doctor appointments. Sometimes we ride along to teach them to use the transportation system. 40
 Ride of last resort (always encouraging use of public transport where available.")
41 ASSIST Transportation Three wheelchair accessible vehicles Providing over 350 rides per month, many of which are 50+ miles round trip(and still turning down ride requests because we re already booked.) Ride of last resort (always encouraging use of public transport where available.) 41
42 WE DO NOT PROVIDE: Personal Care Financial Assistance Medical Care Housekeeping But we may CONNECT our Care Receivers to those resources. 42
43 Resource Connections 2016 Statistics Medical Conditions Financial 113 COPD 57 Housing 133 Cardio Disease 66 Medicaid 144 Depression 30 Personal Care/Respite 110 Mental Health 28 Practical Help 124 Liver Failure 7 Transport 116 Obesity 17 Disability 57 Diabetes 62 End of Life 50 CVAStroke 23 Energy Assistance 50 Cancer 54 Food 88 Agency on Aging Homemaker Services 83 Legal Help 60 Medical/RX 50 Organizational 63 Wellness calls 65 43
44 Northwest Montana Care Transitions Coalition Diverse community representation Monthly Meetings for networking and educational presentations CMS Grant for an RN and Community Health Worker role (fulfilled by ASSIST) called the ReSource Program ipad technology What Works for the Flathead Valley 44

45 The ASSIST Center 10-bed, non-medical, short stay facility. 45

46 The greatest gift we provide is the gift of spending time and LISTENING. That means we can t be in a hurry. We get to slow down and listen. We build relationships that may allow us to speak honestly to them in a future situation. 46
47 Our Website When families face a medical crisis they frequently don t know where to start looking for the help they need. The ASSIST website provides information about community resources and makes information readily available for our volunteers and community members. 47

48 48
49 49

50 50
51 ASSIST is UNIQUE because we are: A volunteer-based organization We go into people s homes and listen to their concerns and needs Volunteers are trained to understand the resources available in our communities We connect our Care Receivers to those resources Our services are FREE. 51
52 Financial Value Hospital charge/day Readmission Reductions Better use of medical services (go to PCP or urgent care before ER) ReSource Program example (RN and CHW): A super-utilizer with chronic COPD who cost the hospital $100,000 in Medicare costs in 3 months stayed in the ASSIST Center, got connected to community resources and only had 1 ER visit in 4 months. To the people we help, our services are PRICELESS and that is our most important goal. 52

53 53


54 CONTACT INFORMATION: Jane Emmert, Director 54
55 Advancing innovations in health care delivery for low-income Americans Leveraging Community Partnerships to Connect East Baltimore Residents to Health and Social Services 55




56 Today s Speakers Linda Dunbar, Vice President, Population Health & Care Management, Johns Hopkins Healthcare Will Torriente, Community Health Worker Supervisor, Sisters Together and Reaching, Inc. Demetrius Frazier, Program Manager, Sisters Together and Reaching, Inc. Reverend Debra Hickman, Co-Founder and CEO, Sisters Together and Reaching, Inc. 56

57 Community Partnerships and Social Determinants Interventions April 18, 2017 Dr. Linda Dunbar, Johns Hopkins Medicine Rev. Debra Hickman, Demetrius Frazier, and Will Torriente, Sisters Together and Reaching

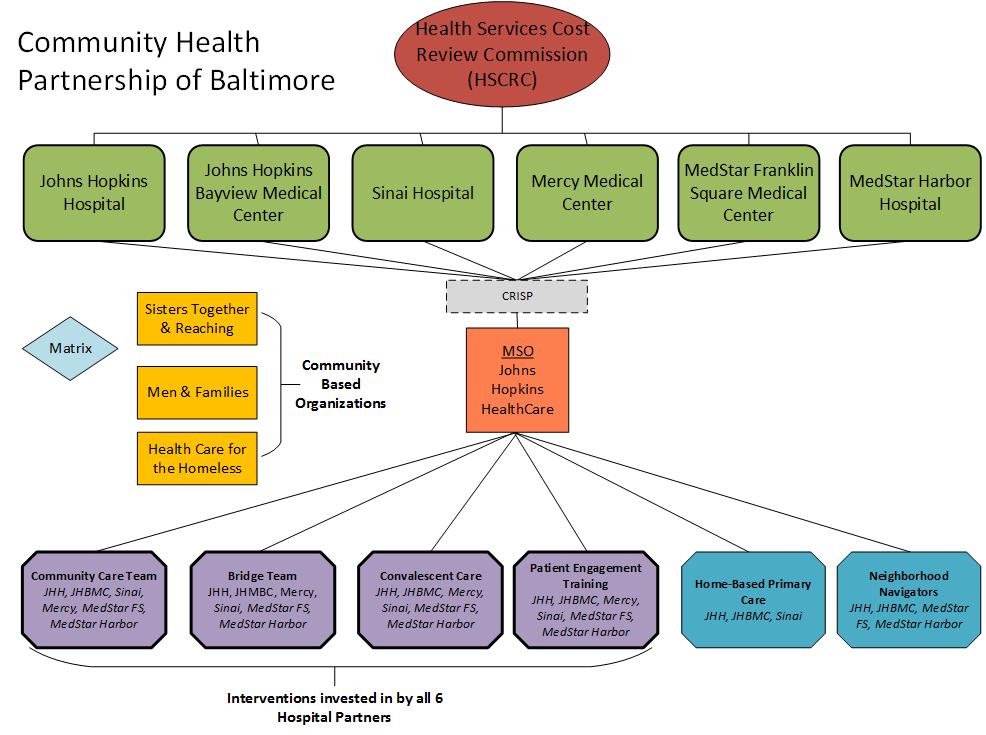
58 JCHiP: Johns Hopkins Community Health Partnership Launched in 2012 and built on existing programs Transforms across continuum: clinics, SNFs, hospitals, home, community and EDs Catalyzed by CMMI HCIA Award East Baltimore Community is the Core : 7 zip codes 58
59 Who Did J-CHiP Touch and what were the outcomes of J-CHiP? About 1,000 adult Medicaid and 2,000 adult Medicare patients with mental illness, substance use disorder and chronic illness receiving local community care were enrolled. Outcomes: Reduction in total quarterly cost of care (-$1,756 per beneficiary, Medicaid) Decrease in hospitalizations and ED visits (-17 and -16 per 1,000 Medicare beneficiaries per quarter, respectively) Decrease in hospitalizations and ED visits (-31 and -48 per 1,000 Medicaid beneficiaries per quarter, respectively) 82% of respondents report that they spoke with clinic staff about how to take care of themselves Most respondents report that they trust their community health worker (CHW) and would recommend their provider to family and friends 59
60 Community Heath Partnership of Baltimore, July
61 Maryland s Vision for Health Care Transformation Transform Maryland s health care system to be highly reliable, highly efficient, and patient-centered. HSCRC and DHMH envision a health care system in which multidisciplinary teams can work with high need/high-resource patients to manage chronic conditions in order to improve outcomes, lower costs, and enhance patient experience. Through aligned collaboration at the regional and state levels, the state and regional partnerships can work together to improve the health and well-being of the population. 61
62 62
63 Community Care Teams 63
 Community Health Workers (CHWs) from Sisters Together and Reaching Health Behavior Specialists (HBS) Regular rounding sessions and communication with")
64 CCT Overview CCTs expand upon existing services of primary care providers to meet the needs of the high-risk population and coordinate care 10 regional teams consisting of: Case Managers (CM) Community Health Workers (CHWs) from Sisters Together and Reaching Health Behavior Specialists (HBS) Regular rounding sessions and communication with providers 64
,")
 A multilevel community health worker program Aims")



65 Tumaini (Hope) for Health Collaborative effort within JCHiP involving Sisters Together and Reaching (STAR), and the Men and Families Center, Inc. (MFC) A multilevel community health worker program Aims to reduce barriers to accessing health care and facilitate uptake of social and health services Targets 19 zip codes in Baltimore City Composed of two intersecting interventions: Neighborhood Navigators, volunteers trained and overseen by the Men and Families Center Community Health Workers, trained and employed by Sisters Together and Reaching 65
66 Who Are The CHWs? Community Health Workers (CHWs) are frontline public health workers who are trusted members of and/or have an unusually close understanding of the community served. This trusting relationship enables CHWs to serve as a liaison/link/intermediary between health/social services and the community to facilitate access to services and improve the quality and cultural competence of service delivery. CHWs also build individual and community capacity by increasing health knowledge and self-sufficiency through a range of activities such as outreach, community education, informal counseling, social support and advocacy. American Public Health Association,


67 Tumaini CHW Qualities Shared life experiences Most essential element considered by employers Socio-economic, educational, racial/ethnic Single largest contributor to success Personal Attributes Essential to CHW work relational experiences Not just anyone can be a CHW Work Experience Roles, Tasks, Skills CHW Training Core competencies Specialty topics Least important Connected to Community Resourceful, Creative Mature, Prudent, Persistent Empathetic, Caring, and Compassionate Open-minded, Non-judgmental, Relativistic Respectful, Honest, Patient Friendly, Outgoing, Sociable Dependable, Responsible, Reliable 67
68 Tumaini CHW s Responsibilities Outreach/Community Mobilizing Preparation and dissemination of materials Case-finding and recruitment Community Strengths/Needs Assessment Home visiting Promoting health literacy Community advocacy System Navigation Translation and interpretation Preparation and dissemination of materials Promoting health literacy Patient navigation Addressing basic needs food, shelter, etc. Coaching on problem solving Coordination, referrals, and follow-ups Documentation 68
69 Tumaini CHW s Responsibilities Case Management/Care Coordination Family engagement Individual strengths/needs assessment Addressing basic needs food, shelter, etc. Promoting health literacy Goal setting, coaching and action planning Supportive counseling Coordination, referrals, and follow-ups Feedback to medical providers Treatment adherence promotion Documentation Home-based Support Family engagement Home visiting Environmental assessment Promoting health literacy Supportive counseling Coaching on problem solving Action plan implementation Treatment adherence promotion Documentation Health Promotion & Coaching Translation and interpretation Teaching health promotion and prevention Treatment adherence promotion Coaching on problem solving Modeling behavior change Promoting health literacy Harm Reduction Community/Cultural Liaison Community organizing Advocacy Translation and interpretation 69
70 Tumaini (Hope) for Health Neighborhood Navigators Adopts a Block-by-Block approach for community organizing for health Combines features of community health worker and peer advocate/mentor models Trained and overseen by the Men and Families Center 40 residents trained; 30 retained for final deployment Reside in specific neighborhoods within the Madison-East End Community Statistical area, located in the zip code Compensated through stipends based on living wage Document work through RedCap 70
71 Tumaini (Hope) for Health Neighborhood Navigators (continued) Serve four primary roles: General neighborhood education and outreach (neighborhoodwide) Informal monitoring and surveillance of unmet needs related to access to health care and social services (neighborhood-wide) Regular home visits to provide social support and promote engagement with care among a small caseload of high-risk patients Capacity-building and mobilization of neighborhood residents through regular participation in and presentation to neighborhood association meetings 71


72 Training for NNs Introduction to Johns Hopkins Health System, Tumaini, and NN and CHW roles Outreach and patient engagement Patient interviewing Means-tested benefit and health insurance eligibility Community resource identification, referral, and navigation Documentation of patients needs and referrals Social and economic determinants of health Introduction to Mental Health First Aid CPR 72
73 Questions? To submit a question, please click the question mark icon located in the toolbar at the top of your screen. Answers to questions that cannot be addressed due to time constraints will be shared after the webinar. 73
74 Look for Parts II and III of this Series Community Paramedicine: A New Approach to Serving Complex Populations May 11, 2017, 1:30-3:00 pm ET Integrating Community Pharmacists into Complex Care Management Programs June 22, 2017, 12:00-1:30 pm ET 74


75 Visit CHCS.org to Download practical resources to improve the quality and costeffectiveness of Medicaid services Learn about cutting-edge efforts to improve care for Medicaid s highestneed, highest-cost beneficiaries Subscribe to CHCS , blog and social media updates to learn about new programs and resources Follow us on 75
Kalispell Regional Healthcare Kalispell, Montana Managing the Needs of Medically and Socially Complex Patients or Superutilizers
 Kalispell Regional Healthcare Kalispell, Montana Managing the Needs of Medically and Socially Complex Patients or Superutilizers A small number of individuals drive much of the cost in the American health
Kalispell Regional Healthcare Kalispell, Montana Managing the Needs of Medically and Socially Complex Patients or Superutilizers A small number of individuals drive much of the cost in the American health
AccessHealth Spartanburg
 TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
TRANSFORMING COMPLEX CARE PROFILE AccessHealth Spartanburg Leveraging community partnerships to improve care for an uninsured population with complex health and social needs A ccesshealth Spartanburg (AHS)
COMMUNITY HEALTH WORKERS: IMPROVING HEALTH OUTCOMES
 COMMUNITY HEALTH WORKERS: IMPROVING HEALTH OUTCOMES The Southern Connecticut State University Department of Public Health Gateway Community College New Haven, CT June 21, 2013 Sergio Matos Executive Director
COMMUNITY HEALTH WORKERS: IMPROVING HEALTH OUTCOMES The Southern Connecticut State University Department of Public Health Gateway Community College New Haven, CT June 21, 2013 Sergio Matos Executive Director
PROGRESS MADE CONTRACT AND PROJECTS. Medicare Quality Innovation Network- Quality Improvement Organization (QIN-QIO) Overview.
 Overview.") Quality Payment Program Medicare Quality Innovation Network- Quality Improvement Organization (QIN-QIO) Overview Mountain-Pacific Quality Health October 26 2017 Medicare QIN-QIO PROGRESS MADE CONTRACT
Quality Payment Program Medicare Quality Innovation Network- Quality Improvement Organization (QIN-QIO) Overview Mountain-Pacific Quality Health October 26 2017 Medicare QIN-QIO PROGRESS MADE CONTRACT
Approaches to Extending Complex Care Models into the Community: Emerging Evidence
 Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community:
Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community:
Thursday, June 2, 2011, 2-3:30 PM ET
 CHCS Webinar: ROI Forecasting Calculator for Health Homes and Medical Homes Thursday, June 2, 2011, 2-3:30 PM ET For audio, dial: (866) 699-3239; Meeting/Event Number: 710 497 839. You may also listen
CHCS Webinar: ROI Forecasting Calculator for Health Homes and Medical Homes Thursday, June 2, 2011, 2-3:30 PM ET For audio, dial: (866) 699-3239; Meeting/Event Number: 710 497 839. You may also listen
New York University Prevention Research Center
 New York University Prevention Research Center May 9, 2013 New York City, New York Sergio Matos Executive Director Community Health Worker Network of NYC President Health Innovation Associates Leading
New York University Prevention Research Center May 9, 2013 New York City, New York Sergio Matos Executive Director Community Health Worker Network of NYC President Health Innovation Associates Leading
Mild-to-Moderate Mental Health Coverage in Medi-Cal: The Challenge and Promise of Coordination between Counties and Health Plans
 Advancing innovations in health care delivery for low-income Americans Mild-to-Moderate Mental Health Coverage in Medi-Cal: The Challenge and Promise of Coordination between Counties and Health Plans December
Advancing innovations in health care delivery for low-income Americans Mild-to-Moderate Mental Health Coverage in Medi-Cal: The Challenge and Promise of Coordination between Counties and Health Plans December
Lessons from the Front Lines: Insights into Trauma-Informed Care for Medicaid s Complex Populations
 Lessons from the Front Lines: Insights into Trauma-Informed Care for Medicaid s Complex Populations June 22, 2015 Call-in Number: 1-800-310-6649; Passcode: 799834 Supported by Kaiser Permanente Community
Lessons from the Front Lines: Insights into Trauma-Informed Care for Medicaid s Complex Populations June 22, 2015 Call-in Number: 1-800-310-6649; Passcode: 799834 Supported by Kaiser Permanente Community
Opportunities for Medicaid-Public Health Collaboration to Achieve Mutual Prevention Goals: Lessons from CDC s 6 18 Initiative
 Advancing innovations in health care delivery for low-income Americans Opportunities for Medicaid-Public Health Collaboration to Achieve Mutual Prevention Goals: Lessons from CDC s 6 18 Initiative June
Advancing innovations in health care delivery for low-income Americans Opportunities for Medicaid-Public Health Collaboration to Achieve Mutual Prevention Goals: Lessons from CDC s 6 18 Initiative June
Digital Health and the Underserved, Part 1: Emerging Opportunities
 Digital Health and the Underserved, Part 1: Emerging Opportunities Wednesday, September 3, 1:00 2:00 pm ET For Audio Dial: 888-352-6803 Passcode: 904104 Made possible through support from Kaiser Permanente
Digital Health and the Underserved, Part 1: Emerging Opportunities Wednesday, September 3, 1:00 2:00 pm ET For Audio Dial: 888-352-6803 Passcode: 904104 Made possible through support from Kaiser Permanente
CMMI-CHW Project: HCH Collaboration Julia Dobbins November 27, Health Care & Housing Are Human Rights
 + CMMI-CHW Project: HCH Collaboration Julia Dobbins November 27, 2012 Health Care & Housing Are Human Rights + Introduction The purpose of this webinar is to discuss the collaboration between the HCH and
+ CMMI-CHW Project: HCH Collaboration Julia Dobbins November 27, 2012 Health Care & Housing Are Human Rights + Introduction The purpose of this webinar is to discuss the collaboration between the HCH and
11 th Scope of Work (SOW)
") Aug 19-20, 2015 11 th Scope of Work (SOW) 11 th SOW Desired outcomes: improve clinical outcomes of HbA1c, Lipids, Blood Pressure and Weight control decrease lower extremity amputations due to DM improve
Aug 19-20, 2015 11 th Scope of Work (SOW) 11 th SOW Desired outcomes: improve clinical outcomes of HbA1c, Lipids, Blood Pressure and Weight control decrease lower extremity amputations due to DM improve
Adverse Drug Events in Wyoming
 Adverse Drug Events in Wyoming Where We Are and Where We Need to Go Stevi Sy, PharmD, RPh Adverse Drug Event Task Lead Mountain-Pacific Quality Health August 2017 Objectives Upon completion of this program
Adverse Drug Events in Wyoming Where We Are and Where We Need to Go Stevi Sy, PharmD, RPh Adverse Drug Event Task Lead Mountain-Pacific Quality Health August 2017 Objectives Upon completion of this program
Montana Community Health Worker Project Montana Healthcare Foundation Kristin Juliar, Director MT Office of Rural Health/AHEC July 13, 2017
 Montana Community Health Worker Project Montana Healthcare Foundation Kristin Juliar, Director MT Office of Rural Health/AHEC July 13, 2017 History Began exploring interest in CHWs in 2010 Periodic workforce
Montana Community Health Worker Project Montana Healthcare Foundation Kristin Juliar, Director MT Office of Rural Health/AHEC July 13, 2017 History Began exploring interest in CHWs in 2010 Periodic workforce
Family and Youth Peer Support September 19, 2011, 2:00 4:00 p.m., ET
 Care Management Entity Quality Collaborative Technical Assistance Webinar Series Family and Youth Peer Support September 19, 2011, 2:00 4:00 p.m., ET For audio and to participate, dial: (866) 699-3239
Care Management Entity Quality Collaborative Technical Assistance Webinar Series Family and Youth Peer Support September 19, 2011, 2:00 4:00 p.m., ET For audio and to participate, dial: (866) 699-3239
Beyond Cost and Utilization: Rethinking Evaluation Strategies for Complex Care Programs
 Beyond Cost and Utilization: Rethinking Evaluation Strategies for Complex Care Programs April 9, 2-3:30 pm (ET) Made possible with support from Kaiser Permanente Community Health Housekeeping This event
Beyond Cost and Utilization: Rethinking Evaluation Strategies for Complex Care Programs April 9, 2-3:30 pm (ET) Made possible with support from Kaiser Permanente Community Health Housekeeping This event
Designing a Medicaid ACO Program: Insights from Trailblazing States
 Designing a Medicaid ACO Program: Insights from Trailblazing States February 11, 2016, 3:30 5:00 pm ET For Audio Dial: 877-830-2582 Passcode: 805070 Made possible by The Commonwealth Fund www.chcs.org
Designing a Medicaid ACO Program: Insights from Trailblazing States February 11, 2016, 3:30 5:00 pm ET For Audio Dial: 877-830-2582 Passcode: 805070 Made possible by The Commonwealth Fund www.chcs.org
Addressing Social Determinants of Health: Connecting People with Complex Needs to Community Resources
 Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Addressing Social Determinants of Health: Connecting People
Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Addressing Social Determinants of Health: Connecting People
Community Health Workers: Supporting Diabetes Prevention in Michigan
 Community Health Workers: Supporting Diabetes Prevention in Michigan MICHIGAN DIABETES PREVENTION NETWORK Katie Mitchell, LMSW Project Director, MiCHWA March 31, 2016 Okemos, Michigan MiCHWA is supported
Community Health Workers: Supporting Diabetes Prevention in Michigan MICHIGAN DIABETES PREVENTION NETWORK Katie Mitchell, LMSW Project Director, MiCHWA March 31, 2016 Okemos, Michigan MiCHWA is supported
CDC s 6 18 Initiative: Informational Webinar for Prospective States and Territories
 Advancing innovations in health care delivery for low-income Americans CDC s 6 18 Initiative: Informational Webinar for Prospective States and Territories July 23, 2018 Tricia McGinnis, MPP, MPH, Senior
Advancing innovations in health care delivery for low-income Americans CDC s 6 18 Initiative: Informational Webinar for Prospective States and Territories July 23, 2018 Tricia McGinnis, MPP, MPH, Senior
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Quality and Improvement Activities Aaron Hubbard
 Quality and Improvement Activities Aaron Hubbard QPP Webinar Series May 16, 2017 HealthInsight Our business is redesigning health care systems for the better HealthInsight is a private, non-profit, community
Quality and Improvement Activities Aaron Hubbard QPP Webinar Series May 16, 2017 HealthInsight Our business is redesigning health care systems for the better HealthInsight is a private, non-profit, community
HSCRC Transformation Implementation Program The Community Health Partnership of Baltimore. Table of Contents
 HSCRC Transformation Implementation Program The Community Health Partnership of Baltimore Table of Contents Background Page 1 1. Target Population Pages 1-3 2. Proposed Program and Interventions Pages
HSCRC Transformation Implementation Program The Community Health Partnership of Baltimore Table of Contents Background Page 1 1. Target Population Pages 1-3 2. Proposed Program and Interventions Pages
Addressing Social Determinants of Health through Medicaid ACOs
 Advancing innovations in health care delivery for low-income Americans Addressing Social Determinants of Health through Medicaid ACOs February 14, 2018, 11:30 1:00 pm ET For Audio Dial: 855-303-0063 Passcode:
Advancing innovations in health care delivery for low-income Americans Addressing Social Determinants of Health through Medicaid ACOs February 14, 2018, 11:30 1:00 pm ET For Audio Dial: 855-303-0063 Passcode:
WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH
 WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH I. CURRENT LEGISLATION AND REGULATIONS Telehealth technology has the potential to improve access to a broader range of health care services in rural and
WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH I. CURRENT LEGISLATION AND REGULATIONS Telehealth technology has the potential to improve access to a broader range of health care services in rural and
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
MIPS Deep Dive: 9 steps to Reporting. Sharon Phelps QPP Webinar Series Webinar 4 June 20, 2017
 MIPS Deep Dive: 9 steps to Reporting Sharon Phelps QPP Webinar Series Webinar 4 June 20, 2017 HealthInsight Our business is redesigning health care systems for the better HealthInsight is a private, non-profit,
MIPS Deep Dive: 9 steps to Reporting Sharon Phelps QPP Webinar Series Webinar 4 June 20, 2017 HealthInsight Our business is redesigning health care systems for the better HealthInsight is a private, non-profit,
Demystifying Community Health Workers (CHWs)
") Demystifying Community Health Workers (CHWs) What do they do and how can they help your rural community? NW Rural Health Conference Spokane, WA 3/27/2018 Seth Doyle, Northwest Regional Primary Care Association
Demystifying Community Health Workers (CHWs) What do they do and how can they help your rural community? NW Rural Health Conference Spokane, WA 3/27/2018 Seth Doyle, Northwest Regional Primary Care Association
Overview of New Nursing Roles in Whole Person Care. Session 1
 Overview of New Nursing Roles in Whole Person Care Session 1 1 Introductions Anne Shields, MHA, RN Associate Director, UW AIMS Center 2 Learning Objectives RN Primary Care Managers Focus Patient Population:
Overview of New Nursing Roles in Whole Person Care Session 1 1 Introductions Anne Shields, MHA, RN Associate Director, UW AIMS Center 2 Learning Objectives RN Primary Care Managers Focus Patient Population:
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
COMMUNITY HEALTH WORKERS
 COMMUNITY HEALTH WORKERS Connecting Our Community to Better Health www.marc.org/communityhealthworkers OVERVIEW Who are Community Health Workers (CHWs)? Why do we need CHWs? What services do CHWs provide?
COMMUNITY HEALTH WORKERS Connecting Our Community to Better Health www.marc.org/communityhealthworkers OVERVIEW Who are Community Health Workers (CHWs)? Why do we need CHWs? What services do CHWs provide?
The Playbook: Better Care for People with Complex Needs
 The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
Leveraging Managed Care to Support Community Health Workers and Promote Population Health
 Leveraging Managed Care to Support Community Health Workers and Promote Population Health Association of State and Territorial Health Officials (ASTHO) September 9, 2015 9:30 AM 10:45 AM ET Thomas Pryor
Leveraging Managed Care to Support Community Health Workers and Promote Population Health Association of State and Territorial Health Officials (ASTHO) September 9, 2015 9:30 AM 10:45 AM ET Thomas Pryor
Connect the Dots in Community Services
 LEVERAGING THE POWER OF CARE MANAGEMENT Connect the Dots 2016 Population Health Colloquium Helen Dunkle MSN RN-BC Agenda in Community Services Caring for High-Need, High-Cost Patients: What Makes for a
LEVERAGING THE POWER OF CARE MANAGEMENT Connect the Dots 2016 Population Health Colloquium Helen Dunkle MSN RN-BC Agenda in Community Services Caring for High-Need, High-Cost Patients: What Makes for a
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States
: Reform Strategies for States") Advancing innovations in health care delivery for low-income Americans Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States March 6, 2018 Michelle Herman Soper and Alexandra
Advancing innovations in health care delivery for low-income Americans Strengthening Long Term Services and Supports (LTSS): Reform Strategies for States March 6, 2018 Michelle Herman Soper and Alexandra
Strategies for Training Care Coordinators and Care Managers in Integrated Programs
 Strategies for Training Care Coordinators and Care Managers in Integrated Programs January 14, 2015 Supported by the California HealthCare Foundation and The SCAN Foundation. Carolyn Ingram, Senior Vice
Strategies for Training Care Coordinators and Care Managers in Integrated Programs January 14, 2015 Supported by the California HealthCare Foundation and The SCAN Foundation. Carolyn Ingram, Senior Vice
State Approaches to Providing Health-Related Supportive Services through Medicaid
 State Approaches to Providing Health-Related Supportive Services through Medicaid June 2, 2016 1:00-2:30 pm ET Made possible through The Commonwealth Fund For Audio Dial: 1-888-819-8046 Passcode: 916263
State Approaches to Providing Health-Related Supportive Services through Medicaid June 2, 2016 1:00-2:30 pm ET Made possible through The Commonwealth Fund For Audio Dial: 1-888-819-8046 Passcode: 916263
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees
 TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
MIPS Tips. Question and Answer Series Jan. 24, Presented by HealthInsight and Mountain Pacific Quality Health
 MIPS Tips Question and Answer Series Jan. 24, 2018 Presented by HealthInsight and Mountain Pacific Quality Health HealthInsight Our business is redesigning health care systems for the better HealthInsight
MIPS Tips Question and Answer Series Jan. 24, 2018 Presented by HealthInsight and Mountain Pacific Quality Health HealthInsight Our business is redesigning health care systems for the better HealthInsight
1:00pm EST Webinar will begin shortly.
 Community Health Workers: Part of the Solution for Advancing Health Equity; Perspectives and Initiatives from the New England Regional Health Equity Council 1:00pm EST Webinar will begin shortly. Community
Community Health Workers: Part of the Solution for Advancing Health Equity; Perspectives and Initiatives from the New England Regional Health Equity Council 1:00pm EST Webinar will begin shortly. Community
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Medicare Shared Savings Program ACO Learning System
 Medicare Shared Savings Program ACO Learning System Leveraging Community Resources and Addressing Beneficiaries Social Needs Wednesday, September 14, 2016 2:30 4:00 PM ET Audio for this session can be
Medicare Shared Savings Program ACO Learning System Leveraging Community Resources and Addressing Beneficiaries Social Needs Wednesday, September 14, 2016 2:30 4:00 PM ET Audio for this session can be
Community Health Workers in Michigan: Addressing Social Determinants in the Community and the Clinic
 Community Health Workers in Michigan: Addressing Social Determinants in the Community and the Clinic MICHIGAN HEALTH POLICY FORUM Katie Mitchell, LMSW MiCHWA Project Director November 9, 2015 Lansing,
Community Health Workers in Michigan: Addressing Social Determinants in the Community and the Clinic MICHIGAN HEALTH POLICY FORUM Katie Mitchell, LMSW MiCHWA Project Director November 9, 2015 Lansing,
Financing of Community Health Workers: Issues and Options for State Health Departments
 Financing of Community Health Workers: Issues and Options for State Health Departments ASTHO Technical Assistance Presentation Terry Mason, PhD Carl Rush, MRP Geoff Wilkinson, MSW This webinar is supported
Financing of Community Health Workers: Issues and Options for State Health Departments ASTHO Technical Assistance Presentation Terry Mason, PhD Carl Rush, MRP Geoff Wilkinson, MSW This webinar is supported
Funding Opportunities with USDA
 Funding Opportunities with USDA Speakers: Shekinah Bailey and Steve Troendle Thursday, November 17, 2016 2 to 3 PM MST 12 to 1 PM AKST 11 to 12 PM HST HTS, a department of Mountain-Pacific Quality Health
Funding Opportunities with USDA Speakers: Shekinah Bailey and Steve Troendle Thursday, November 17, 2016 2 to 3 PM MST 12 to 1 PM AKST 11 to 12 PM HST HTS, a department of Mountain-Pacific Quality Health
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
State (and U. S. Territorial) Health Department Request for Technical Assistance (RTA): Applications due: (December 1, 2014) at 11:59 pm ET
 Health Department Request for Technical Assistance (RTA): Applications due: (December 1, 2014) at 11:59 pm ET") State (and U. S. Territorial) Health Department Request for Technical Assistance (RTA): Million Hearts Stakeholders Workshop Applications due: (December 1, 2014) at 11:59 pm ET I. Purpose: The purpose
State (and U. S. Territorial) Health Department Request for Technical Assistance (RTA): Million Hearts Stakeholders Workshop Applications due: (December 1, 2014) at 11:59 pm ET I. Purpose: The purpose
OMC Strategic Plan Final Draft. Dear Community, Working together to provide excellence in health care.
 Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
PCMH and the Care of Complex High Cost Patients
 PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
Minnesota Accountable Health Model: Community Advisory Task Force
 Minnesota Accountable Health Model: Community Advisory Task Force WEDNESDAY, MARCH 18, 2015 AMHERST H. WILDER FOUNDATION 451 LEXINGTON PARKWAY NORTH, ST. PAUL 9 AM- 12 PM Agenda Welcome and Overview of
Minnesota Accountable Health Model: Community Advisory Task Force WEDNESDAY, MARCH 18, 2015 AMHERST H. WILDER FOUNDATION 451 LEXINGTON PARKWAY NORTH, ST. PAUL 9 AM- 12 PM Agenda Welcome and Overview of
CoP/Training Call: Language Services In Health Care
 CoP/Training Call: Language Services In Health Care Guest Speakers: Marcos Pesquera, R.Ph, Adventist Healthcare Inc. Oscar Lanza, IMG, Kaiser Permanente Mercedes Blanco and Victoria Williams, MAXIMUS March
CoP/Training Call: Language Services In Health Care Guest Speakers: Marcos Pesquera, R.Ph, Adventist Healthcare Inc. Oscar Lanza, IMG, Kaiser Permanente Mercedes Blanco and Victoria Williams, MAXIMUS March
Integrating Behavioral and Physical Health
 Integrating Behavioral and Physical Health Kim Salamone, Ph.D. Vice President, Health Information Technology Wednesday, April 12, 2017 Agenda Introduce Health Services Advisory Group (HSAG) Centers for
Integrating Behavioral and Physical Health Kim Salamone, Ph.D. Vice President, Health Information Technology Wednesday, April 12, 2017 Agenda Introduce Health Services Advisory Group (HSAG) Centers for
Introduction to the BFCC-QIO Program
 Introduction to the BFCC-QIO Program Bryan Fischer Communications Lead 11-SOW-MD-2017-QIOBFCC-CP2 About Livanta LLC Established in 2004 Privately-held, government contracting firm headquartered in Annapolis
Introduction to the BFCC-QIO Program Bryan Fischer Communications Lead 11-SOW-MD-2017-QIOBFCC-CP2 About Livanta LLC Established in 2004 Privately-held, government contracting firm headquartered in Annapolis
Planning a Course to Population Health Management
 Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
Patient Navigator Program
 Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Value-Based Care Emergent Care Services. Presented by Cliff Frank Partnera Partners LLC
 Value-Based Care Emergent Care Services Presented by Cliff Frank Partnera Partners LLC Problem Un-doctored consumers are driving $575 billion inappropriate emergent care Fee-for-service ER visits add another
Value-Based Care Emergent Care Services Presented by Cliff Frank Partnera Partners LLC Problem Un-doctored consumers are driving $575 billion inappropriate emergent care Fee-for-service ER visits add another
Highline Health Connections: Care Navigation for Vulnerable Populations
 Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
Medicare Shared Savings Program ACO Learning System
 Medicare Shared Savings Program ACO Learning System Coordinating Care for Beneficiaries with Complex Care Needs Wednesday, June 24, 2015 2:30 4:00 PM ET Audio for this session can be streamed through your
Medicare Shared Savings Program ACO Learning System Coordinating Care for Beneficiaries with Complex Care Needs Wednesday, June 24, 2015 2:30 4:00 PM ET Audio for this session can be streamed through your
MIPS; Improving Your Score with ecqi. Patty Kosednar, PMP, CPEHR, CPHIMS HIT Project Manager
 MIPS; Improving Your Score with ecqi Patty Kosednar, PMP, CPEHR, CPHIMS HIT Project Manager HealthInsight Our business is redesigning health care systems for the better HealthInsight is a private, non-profit,
MIPS; Improving Your Score with ecqi Patty Kosednar, PMP, CPEHR, CPHIMS HIT Project Manager HealthInsight Our business is redesigning health care systems for the better HealthInsight is a private, non-profit,
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
KEPRO Beneficiary and Family Centered Care Quality Improvement Organization. Andrea Plaskett, MPH
 KEPRO Beneficiary and Family Centered Care Quality Improvement Organization Andrea Plaskett, MPH 1 KEPRO KEPRO is a federal contractor for the Centers for Medicare & Medicaid Services (CMS) KEPRO is the
KEPRO Beneficiary and Family Centered Care Quality Improvement Organization Andrea Plaskett, MPH 1 KEPRO KEPRO is a federal contractor for the Centers for Medicare & Medicaid Services (CMS) KEPRO is the
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
RPC and OMH Collaborative Care Webinar. February 1, pm
 RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Basic Training: Home Health Edition. OASIS and Outcomes. April 2, 2013
 Basic Training: Home Health Edition OASIS and Outcomes April 2, 2013 Presented by: Rhonda Will, RN, BS, COS-C, BCHH-C, Assistant Director of the Competency Institute, Fazzi Associates, Inc. 243 King Street,
Basic Training: Home Health Edition OASIS and Outcomes April 2, 2013 Presented by: Rhonda Will, RN, BS, COS-C, BCHH-C, Assistant Director of the Competency Institute, Fazzi Associates, Inc. 243 King Street,
Connecticut SIM: Enabling Accountable Care and Accountable Communities
 Connecticut SIM: Enabling Accountable Care and Accountable Communities SIM SYMPOSIUM FROM ACCOUNTABLE CARE TO ACCOUNTABLE COMMUNITIES: HOW CONNECTICUT S STATE INNOVATION MODEL INITIATIVE IS DRIVING REFORM
Connecticut SIM: Enabling Accountable Care and Accountable Communities SIM SYMPOSIUM FROM ACCOUNTABLE CARE TO ACCOUNTABLE COMMUNITIES: HOW CONNECTICUT S STATE INNOVATION MODEL INITIATIVE IS DRIVING REFORM
Health IT Enabled Clinical Quality
 Health IT Enabled Clinical Quality Improvement (ecqi) Mountain Pacific Quality Health Foundation Quality Innovation Network-Quality Improvement Organization (QIN-QIO) since 1973 QIN/QIO Regions include;
Health IT Enabled Clinical Quality Improvement (ecqi) Mountain Pacific Quality Health Foundation Quality Innovation Network-Quality Improvement Organization (QIN-QIO) since 1973 QIN/QIO Regions include;
Minnesota Community Health Worker Project
 Minnesota Community Health Worker Project Presentation Objectives Development of Partnership Development of CHW Curriculum Development of Policy Role of CHWs in MN Project Outcomes Minnesota CHW Project
Minnesota Community Health Worker Project Presentation Objectives Development of Partnership Development of CHW Curriculum Development of Policy Role of CHWs in MN Project Outcomes Minnesota CHW Project
Community Health Partnership. Improving the health of our community through collaboration
 Community Health Partnership Improving the health of our community through collaboration Working Together 101 co a li tion 1. an alliance or union between groups, factions or parties, especially for a
Community Health Partnership Improving the health of our community through collaboration Working Together 101 co a li tion 1. an alliance or union between groups, factions or parties, especially for a
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential
 A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential Stability and Reduced Costs Webinar Format Our Webinar Format:
A Hear from Your Peers Webinar Effective Coordination between Hospitals and CoC Homeless Assistance Providers Results in Improved Residential Stability and Reduced Costs Webinar Format Our Webinar Format:
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR
 CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound
 Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
National Disparities LAN Event Managing the Opioid Crisis: Perspectives from Rural Communities. Wednesday, March 14, :00 4:30 PM ET
 National Disparities LAN Event Managing the Opioid Crisis: Perspectives from Rural Communities Wednesday, March 14, 2018 3:00 4:30 PM ET Welcome and Reminders Please be prepared for sharing and open discussion
National Disparities LAN Event Managing the Opioid Crisis: Perspectives from Rural Communities Wednesday, March 14, 2018 3:00 4:30 PM ET Welcome and Reminders Please be prepared for sharing and open discussion
Serving CYSHCN in Medicaid Managed Care: Contract Language and the Contracting Process
 Serving CYSHCN in Medicaid Managed Care: Contract Language and the Contracting Process November 16, 2017 1:00-2:00 PM, ET For audio: 888-757-2790 Passcode: 105799 Press *6 to mute/unmute your line. Please
Serving CYSHCN in Medicaid Managed Care: Contract Language and the Contracting Process November 16, 2017 1:00-2:00 PM, ET For audio: 888-757-2790 Passcode: 105799 Press *6 to mute/unmute your line. Please
Connecting Value-Based Services to Whole Person Care
 Advancing innovations in health care delivery for low-income Americans Connecting Value-Based Services to Whole Person Care Caitlin Thomas-Henkel, Senior Program Officer The National Council December 6,
Advancing innovations in health care delivery for low-income Americans Connecting Value-Based Services to Whole Person Care Caitlin Thomas-Henkel, Senior Program Officer The National Council December 6,
Center for Health Care Strategies, Inc. From the Beneficiary Perspective: Core Elements to Guide Integrated Care for Dual Eligibles IN BRIEF
 CHCS Center for Health Care Strategies, Inc. From the Beneficiary Perspective: Core Elements to Guide Integrated Care for Dual Eligibles Technical Assistance Brief December 2010 By Alice Lind and Suzanne
CHCS Center for Health Care Strategies, Inc. From the Beneficiary Perspective: Core Elements to Guide Integrated Care for Dual Eligibles Technical Assistance Brief December 2010 By Alice Lind and Suzanne
National Council for Behavioral Health. Trauma-informed Primary Care: Fostering Resilience and Recovery Learning Community
 National Council for Behavioral Health Trauma-informed Primary Care: Fostering Resilience and Recovery Learning Community Request for Applications INTRODUCTION The National Council for Behavioral Health
National Council for Behavioral Health Trauma-informed Primary Care: Fostering Resilience and Recovery Learning Community Request for Applications INTRODUCTION The National Council for Behavioral Health
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships
 States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
Community Health Workers: Strengthening Community-Clinical Linkages
 Community Health Workers: Strengthening Community-Clinical Linkages Jamie R. Forrest, MS Epidemiology and Evaluation Administrator Bureau of Chronic Disease Prevention Marion Banzhaf Cessation Project
Community Health Workers: Strengthening Community-Clinical Linkages Jamie R. Forrest, MS Epidemiology and Evaluation Administrator Bureau of Chronic Disease Prevention Marion Banzhaf Cessation Project
The Census Scene in 2018: Strategies to Optimize Occupancy During Change Census Scorecard. Ohio Overall Certified Occupancy
 The Census Scene in 2018: Strategies to Optimize Occupancy During Change Linda L. Saunders, LNHA Founder, President 2016 Census Scorecard 1 84% 82% Ohio Overall Certified Occupancy Ohio Overall Licensed
The Census Scene in 2018: Strategies to Optimize Occupancy During Change Linda L. Saunders, LNHA Founder, President 2016 Census Scorecard 1 84% 82% Ohio Overall Certified Occupancy Ohio Overall Licensed
Population Health: The Role of the DNP. Linda Dunbar, PhD, RN Vice President, Population Health Johns Hopkins HealthCare
 Population Health: The Role of the DNP Linda Dunbar, PhD, RN Vice President, Population Health Johns Hopkins HealthCare TOPICS in Population Health Definitions Hopkins Conceptual Model Interventions Relationship
Population Health: The Role of the DNP Linda Dunbar, PhD, RN Vice President, Population Health Johns Hopkins HealthCare TOPICS in Population Health Definitions Hopkins Conceptual Model Interventions Relationship
RECOMMENDATIONS FROM WORKFORCE DEVELOPMENT WORKGROUP
 RECOMMENDATIONS FROM WORKFORCE DEVELOPMENT WORKGROUP Meeting Dates May 20, 2014 June 5, 2014 Committee Members Angela Anderson, Dean, Center for Health Studies, Prince George s Community College Charlene
RECOMMENDATIONS FROM WORKFORCE DEVELOPMENT WORKGROUP Meeting Dates May 20, 2014 June 5, 2014 Committee Members Angela Anderson, Dean, Center for Health Studies, Prince George s Community College Charlene
CAH/FQHC Collaboration
 1 2017 FLEX PROGRAM REVERSE SITE VISIT BETHESDA, MD CAH/FQHC Collaboration A Community s Success Story Coal Country Community Health Center Sakakawea Medical Center 2 Presentation Agenda & Objectives Rural
1 2017 FLEX PROGRAM REVERSE SITE VISIT BETHESDA, MD CAH/FQHC Collaboration A Community s Success Story Coal Country Community Health Center Sakakawea Medical Center 2 Presentation Agenda & Objectives Rural
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care
 Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright