To Reduce Resident s Pain Using Non-Medicine Treatments
|
|
|
- Brittney Johnston
- 5 years ago
- Views:
Transcription
1 Best Practices for Pain Management and Prevention of Re-admissions Angela Trahan, Mennonite Home Kris J. Modl, Dove Healthcare Jordan Emley, Grandview Heights Rehab and Healthcare August 14, 2018 To Reduce Resident s Pain Using Non-Medicine Treatments Angela Trahan, RN Director of Nursing Services Mennonite Village Albany, Oregon 2 1
/intermediate care facility (ICF) combined facility with a general census of approximately 75.")
2 About Us Mennonite Village is a not-for-profit, Continuing Care Retirement Community in Albany, Oregon. Mennonite Village began as a 24-room nursing home in Mennonite Home is a skilled nursing facility (SNF)/intermediate care facility (ICF) combined facility with a general census of approximately Problem We were not scoring as well as we would have liked to in our quality measures for pain. 4 2
3 PIP Team Members Tanya Boyd, RCM Lacy King, RCM Barb Jones, CMA Sage Forson, CNA Casey Tessen, LPN 5 Goals 1. Improve quality measures 2. Reduce resident opioid use 3. To reduce resident pain Additionally, using an interdisciplinary team (IDT) approach, it aimed to help improve residents that suffer from pain that is chronic in nature and difficult to control. 6 3
4 Intervention Conducted routine IDT meetings to formulate project, develop interventions, and continue to adjust as needed Identified barriers to pain reduction Modified current pain assessment tools Discussed case studies on residents suffering from chronic pain or pain difficult to control Developed non-pharmacologic pain program that included a variety of pain interventions that can be offered by CNAs and CMAs Monitoring of non-pharmacologic pain intervention effectiveness on the treatment record 7 Pilot We started with residents on our short term rehab unit. After evaluating, transitioned to the other units. 8 4
5 Measures/Indicators Pain scores are being monitored through MDS, Section J to evaluate pain scores as reported by resident. 20 rehab residents were tracked using the MDS to determine if non medicine interventions were successful in reducing pain. Tracking began in March 2017 and ended in June of the 20 residents had a decrease in pain reflected on the MDS. 9 Measures/Indicators Primary sources were therapy modalities and ice and heat packs. Sources for non pharm treatments heat/ice E-stim Diathermy Ultrasound 10 5
6 Results In February our quality measure (QM) for pain was 26.9 percent and the national was 15.8 percent In July our QM reduced to 20.4 percent and the national was 14.6 percent. 11 Lessons Learned Underutilizing non-pharmacologic pain interventions already available included therapy modalities Underutilizing available staff We now use CNAs and CMAs to assist with nonpharmacological pain interventions. 12 6
7 Next Steps Continuing monthly IDT meetings with case studies to further identify residents that could benefit. Transition to our long term care units. Continue to explore alternative pain interventions. 13 Resources Keilman, Linda (2015). Compendium of Evidence-Based Nonpharmacologic Interventions for Pain in Older Adults. Copyright 2015 by LJ Keilman, East Lansing: Michigan State University, College of Nursing Yurdanur Demir (2012). Non-Pharmacological Therapies in Pain Management, Pain Management - CurrentIssues and Opinions, Dr. Gabor Racz (Ed.), ISBN: , InTech, Available from:
8 Contact Information Tanya Boyd, RCM Lacy King, RCM Angela Trahan, DNS 15 Hospital Readmission Prevention Chippewa Valley Continuum of Care Coalition Kris J. Modl, ACBSW Director of Social Services/Admissions Dove Healthcare South and West Eau Claire, Wisconsin 16 8
9 About Us The Chippewa Valley Continuum of Care Coalition formed out of a strategic planning process in 2010 The coalition was initially comprised of two hospitals, five SNFs and a Family Care Organization 17 About Us Our focus was to improve the continuum of care process as patients transitioned from the acute care setting to SNF in a time sensitive manner 18 9
10 About Us The initial plan was to: Develop strategies to minimize the number of transitions and to ensure that all transitions were seamless Improve the well-being of our community by a collaborative process that promotes optimal patient care and services 19 About Us Today our coalition has grown to include three hospitals, hospice and home care agencies, medical clinics, Family Care, community based residential facilities (CBRFs) and multiple SNF s 20 10
11 About Us With a purpose: To build and sustain a community coalition with a focus on improving transitions of care To encourage person-centered and person-directed models of care To collaborate and encourage efforts of organizations with shared visions To advance policies that further that vision To reduce the number of re-hospitalization/ patient care transitions 21 Coalition Participation Participation in the Chippewa Valley Continuation of Care Coalition (CVCCC) is open to organizations and individuals interested in fostering the vision by actively engaging in the planning and work of the Coalition 22 11
12 Coalition Participation Charter members join in a commitment to: Share best practices and knowledge related to care transitions Mentor partners and providers Share data and support analyses related to care transitions Promote implementation of evidence-based interventions 23 Identified Gaps Some of our initial work identified gaps that impact transitioning patients between levels of care. Examples include: Patients being discharged to the SNF with higher acuity needs care needs that not all SNFs are prepared to meet Regulatory differences between acute care and SNF care i.e. use of restraints and medications to manage patient behaviors in acute setting but not allowed in SNF resulting in an incomplete picture of patients current state for the SNF 24 12
13 Identified Gaps Root cause analysis of patients that are experiencing number of transitions what pieces are missing? Patients with behavioral health issues are the most difficult to transition Inconsistent, incomplete information shared by the acute care facilities, impacting the ability of the receiving facility to make a timely decision 25 Identified Gaps Lack of education earlier education of patients and families on long term care planning 26 13
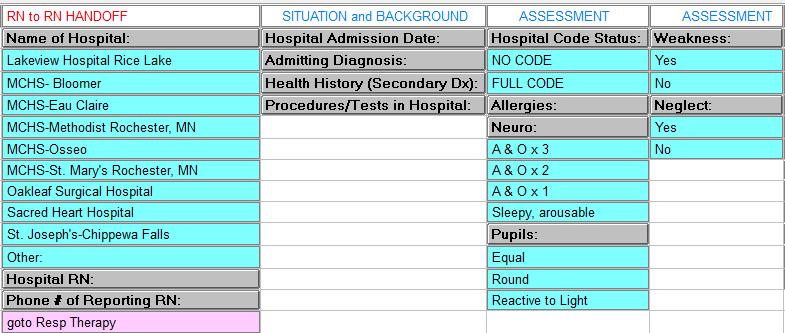
14 Improvement Processes Performance Improvement Opportunities included: Standardized acute care referral summary information Standardized acute care discharge information Standardized physician s plan of care (PPOC) information i.e. MD signed, free of communicable disease statement, etc. Timelier receipt of Discharge Summaries Accompaniment to appointments, tests, etc. 27 Improvement Processes Performance Improvement Opportunities include: Transfer / Communication tool from SNF Clinic Facility capabilities RN to RN handover 28 14
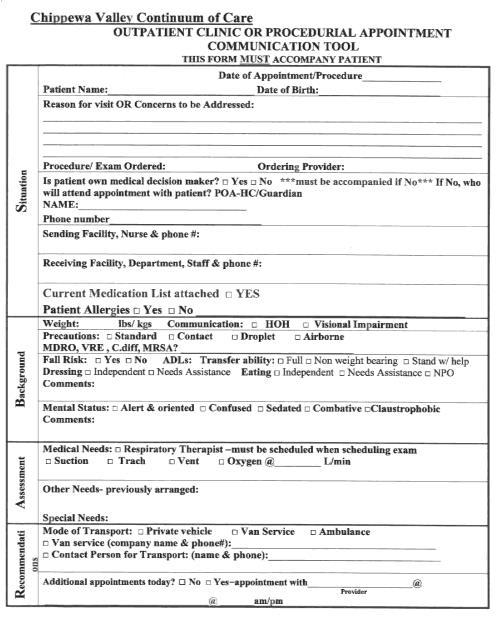
15 Communication Tool EHR Paper Communication Form Example 30 15


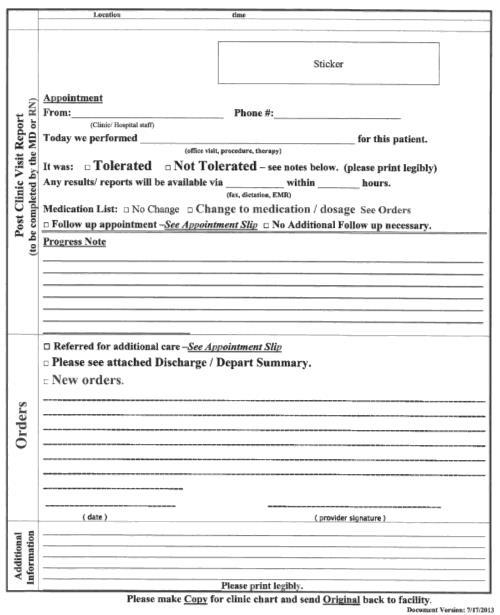
16 EHR Paper Communication Form Example 31 EHR Paper Communication Form Example 32 16

17 EHR Paper Communication Form Example 33 Coalition Subcommittees Subcommittee Development 1. Provider and Community Education 2. Transitions of Care 3. Transportation 34 17
18 Coalition Subcommittees 1. Provider and Community Education Identify knowledge gaps within our community related to the types of care transitions along with opportunities to improve communication and quality of care with those transitions Provide education to healthcare providers as well as the community at large regarding healthcare resources and support along the continuum of care 35 Coalition Subcommittees 2. Transitions of Care Monitors the transitions of care both from the hospital to the next level of care and vice versa Focus is on improving the continuum of care process as patients transitioned 36 18
19 Coalition Subcommittees 3. Transportation To compile transportation resources in one place so are accessible to all organizations in need Collaboration at the local and State level to ensure transportation services are available no matter the payer source or need 37 Next Steps Sponsoring a medical provider event to educate providers on current community data related to healthcare resource utilization, how to identify and treat our community based on patient centered goals of care from medical through end of life care, along with current resources in our community to support those patient goals of care. Sponsoring a community event to educate on need for Advance Directives and having goals of care discussions
20 Next Steps Implementing multi-directional flow of information i.e. to/from Hospital, SNF, Clinic, Home Care, etc. Educating receivers of this information as to what to do with it i.e. medication reconciliation, etc. 39 Next Steps Ongoing collaboration with MetaStar to reduce all cause admission and readmission rates 40 20
21 Contact Information Kris J. Modl Co-Chair CVCCC Transitions Subcommittee 41 Performance Improvement Project on Pain Management Jordan Emley, RN Director of Nursing Grandview Heights Rehab and Healthcare Marshalltown, Iowa 42 21

22 About Us Grandview Heights Rehab and Healthcare is a family owned and operated facility Started in Dually Certified beds Average Daily Census is 95 We pride ourselves on bringing people in from the community, providing skilled rehab, and returning them to their homes 43 Problem Our pain score for long stay residents reporting moderate to severe pain was well above both state and national averages 44 22
23 PIP Team Members Jordan Emley, RN/DON Carol Hazen, LPN/MDS Nurse Tammy Veldhouse, RN/QA Nurse Sue Tharp, Director of Rehab Kayla Perry, CNA Heather Melendrez, CNA Kelli Walsh, RN 45 Aim To reduce the percentage of long stay residents reporting moderate to severe pain
24 Intervention Pain assessment done two weeks prior to assessment period Different modalities to alleviate pain Education provided to residents regarding the comparative pain scale CNA education regarding pain assessment in residents with dementia 47 Measures/Indicators We primarily use our CASPER Report to collect and analyze our data regarding pain. When we began: Our state percentage was 6.7 percent Our national percentage was 5.6 percent Our facility percentage was 12.2 percent Latest numbers show: State: 7.6 percent National: 6.3 percent Facility: 3.7 percent 48 24
25 Results The results were quick and much better than what we had expected. Our goal was to decrease our percentage from 12.2 percent to 8.0 percent. After initiating our program, our number dropped to 5.3 percent and has continued to hover right around the 3.7 percent mark. 49 Lessons Learned One key lesson we learned was that people do not accurately report their level of pain. As nurses, we learn that pain is what the person tells us it is, but we all have experience with people who present in a manner contrary to the number they re reporting. Education was key and that s where the comparative pain scale came in to play. After we would provide the description that correlated with the number the resident gave us, they typically changed their rating. The second key was our focus was not on pharmacological interventions, but instead on therapy and education
26 Next Steps We now include the comparative pain scale in our everyday pain assessments with those residents who are able to use it. I feel this is what has continued to keep our numbers down. 51 Resources Comparative Pain Scale Pain Assessment in Advanced Dementia 52 26
27 Contact Information Jordan Emley Grandview Heights Rehab and Healthcare Phone: (641) Discussion Questions? 54 27

28 This material was prepared by the Lake Superior Quality Innovation Network, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The materials do not necessarily reflect CMS policy. 11SOW-MI/MN/WI-C
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015
 MODEL OF CARE TRAINING 2015") SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
Quality Improvement Program Evaluation
 Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA)
 Case Study Scenario 1: Following Quality Assurance (QA)") Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Community Health Needs Assessment Three Year Summary
 Community Health Needs Assessment Three Year Summary 2013 2016 Community Health Needs Assessment Three Year Summary 2014 2016 Key needs were identified by community stakeholders which included the following:
Community Health Needs Assessment Three Year Summary 2013 2016 Community Health Needs Assessment Three Year Summary 2014 2016 Key needs were identified by community stakeholders which included the following:
West Valley and Central Valley Care Coordination Coalitions
 West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees
 Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees") Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound
 Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling. Speaker: Thomas Martin November 2014
 Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
MDS Coding. Antipsychotic Quality Measure
 MDS Coding Antipsychotic Quality Measure The information in this presentation may be subject to copyright and may not be reproduced without permission of the presenter. Introduction Jessica Mirabal, RN
MDS Coding Antipsychotic Quality Measure The information in this presentation may be subject to copyright and may not be reproduced without permission of the presenter. Introduction Jessica Mirabal, RN
Objectives. Norlite Nursing Center and Rehab Marquette, MI. Applying QAPI Principles: Solutions for Unintended Weight Loss
 Applying QAPI Principles: Solutions for Unintended Weight Loss May 17, 2016 3:00 ET/2:00 CT Objectives 1. Identify at least two strategies to help reduce unintended weight loss for residents 2. Apply QAPI
Applying QAPI Principles: Solutions for Unintended Weight Loss May 17, 2016 3:00 ET/2:00 CT Objectives 1. Identify at least two strategies to help reduce unintended weight loss for residents 2. Apply QAPI
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Central Valley/West Valley Care Coordination Coalitions. Quarterly Community Meeting
 Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Proposed Standards Revisions Related to Pain Assessment and Management
 Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
OMC Strategic Plan Final Draft. Dear Community, Working together to provide excellence in health care.
 Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
2/13/2017. SNF Requirements for Participation. Facility Wide Resource Assessment
 Objectives SNF Requirements for Participation Facility Wide Resource Assessment Recognize the key concepts of the new facility wide resource assessment in the new regulations for skilled nursing facilities
Objectives SNF Requirements for Participation Facility Wide Resource Assessment Recognize the key concepts of the new facility wide resource assessment in the new regulations for skilled nursing facilities
4/22/2018. Redesign and Reimage Long Term Care for the Future. Health Care Landscape Change. Disclosure of Commercial Interests
 Redesign and Reimage Long Term Care for the Future Lisa Thomson Chief Strategy and Marketing Officer www.pathwayhealth.com Disclosure of Commercial Interests We consult for the following organization:
Redesign and Reimage Long Term Care for the Future Lisa Thomson Chief Strategy and Marketing Officer www.pathwayhealth.com Disclosure of Commercial Interests We consult for the following organization:
LOUISIANA MEDICAID PROGRAM ISSUED: 04/15/12 REPLACED: CHAPTER 24: HOSPICE SECTION 24.3: COVERED SERVICES PAGE(S) 5 COVERED SERVICES
 5 COVERED SERVICES") COVERED SERVICES Hospice care includes services necessary to meet the needs of the recipient as related to the terminal illness and related conditions. Core Services (Core services) must routinely be provided
COVERED SERVICES Hospice care includes services necessary to meet the needs of the recipient as related to the terminal illness and related conditions. Core Services (Core services) must routinely be provided
Palmetto GBA Hospice Coalition Questions August 7, 2001
 Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Palmetto GBA Hospice Coalition Questions August 7, 2001 1. How should billing be handled when the initial certification is provided outside of the 2 weeks before and 2 days after time frame? For example,
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Best Practices in Care Coordination & Transitions of Care Communications
 Best Practices in Care Coordination & Transitions of Care Communications Jessica Carpenter, MS, RD, LDN Director, Disability and Community Services University of Massachusetts Medical School Overview/Agenda
Best Practices in Care Coordination & Transitions of Care Communications Jessica Carpenter, MS, RD, LDN Director, Disability and Community Services University of Massachusetts Medical School Overview/Agenda
08-16 FORM CMS
 08-16 FORM CMS-2540-10 4110.1 4110 WORKSHEET S-8 - SNF-BASED HOSPICE IDENTIFICATION DATA In accordance with 42 CFR 418.310, hospice providers of service participating in the Medicare program are required
08-16 FORM CMS-2540-10 4110.1 4110 WORKSHEET S-8 - SNF-BASED HOSPICE IDENTIFICATION DATA In accordance with 42 CFR 418.310, hospice providers of service participating in the Medicare program are required
Implementing Managed Long Term Care in NYS and What You Need to Know. The Rochester Experience - Journey. Albany Guardian Society April 18, 2013
 Implementing Managed Long Term Care in NYS and What You Need to Know The Rochester Experience - Journey Albany Guardian Society April 18, 2013 About Lifespan of Greater Rochester A community-based aging
Implementing Managed Long Term Care in NYS and What You Need to Know The Rochester Experience - Journey Albany Guardian Society April 18, 2013 About Lifespan of Greater Rochester A community-based aging
Glendale Healthier Community Care Coordination Collaborative. Health Services Advisory Group (HSAG) March 06, 2018
 March 06, 2018") Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
PointRight: Your Partner in QAPI
 A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers
 Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Long-Term Care Program
 Long-Term Care Program Long-Term Care Program p.1 Program Overview Nurses Improving Care for Healthysystem Elders (NICHE) is a nursing education and consultation program designed to improve geriatric
Long-Term Care Program Long-Term Care Program p.1 Program Overview Nurses Improving Care for Healthysystem Elders (NICHE) is a nursing education and consultation program designed to improve geriatric
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Preparing for Quality-Based Reimbursement: Strategies for Success. Gina Zimmermann, MS Executive Director, Nursing Care Center Accreditation Program
 Copyright, The Joint Commission Preparing for Quality-Based Reimbursement: Strategies for Success Gina Zimmermann, MS Executive Director, Nursing Care Center Accreditation Program 1 Today s Objectives
Copyright, The Joint Commission Preparing for Quality-Based Reimbursement: Strategies for Success Gina Zimmermann, MS Executive Director, Nursing Care Center Accreditation Program 1 Today s Objectives
LeadingAge New York Technology Solutions
 LeadingAge New York Technology Solutions How to Measure for QAPI Success Susan Chenail, RN, CCM, RAC-CT Senior Quality Improvement Analyst Todays Objectives Define QAPI Provide background of QAPI initiative
LeadingAge New York Technology Solutions How to Measure for QAPI Success Susan Chenail, RN, CCM, RAC-CT Senior Quality Improvement Analyst Todays Objectives Define QAPI Provide background of QAPI initiative
We Honor Veterans Conference March 29, 2018
 VA PANEL What s it Like to Work at the VA? We Honor Veterans Conference March 29, 2018 VA OUTPATIENT PROGRAMS We Honor Veterans Conference March 29, 2018 Heather Rood, RN 1 Objectives Become familiar with
VA PANEL What s it Like to Work at the VA? We Honor Veterans Conference March 29, 2018 VA OUTPATIENT PROGRAMS We Honor Veterans Conference March 29, 2018 Heather Rood, RN 1 Objectives Become familiar with
NetworkCares (PPO SNP) 2017 Model of Care Training. H5215_360r2_ NHIC 01/2017 m-hm-ncprovpres-0117
 2017 Model of Care Training. H5215_360r2_ NHIC 01/2017 m-hm-ncprovpres-0117") NetworkCares (PPO SNP) 2017 Model of Care Training H5215_360r2_092714 NHIC 01/2017 m-hm-ncprovpres-0117 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training
NetworkCares (PPO SNP) 2017 Model of Care Training H5215_360r2_092714 NHIC 01/2017 m-hm-ncprovpres-0117 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training
Test Content Outline Effective Date: February 6, Gerontological Nursing Board Certification Examination
 Board Certification Examination There are 175 questions on this examination. Of these, 150 are scored questions and 25 are pretest questions that are not scored. Pretest questions are used to determine
Board Certification Examination There are 175 questions on this examination. Of these, 150 are scored questions and 25 are pretest questions that are not scored. Pretest questions are used to determine
Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications
 Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications Lisa Bridwell Program Specialist Telligen QIN-QIO March 2018 Objectives Review interpretive guidance F758 (Free from
Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications Lisa Bridwell Program Specialist Telligen QIN-QIO March 2018 Objectives Review interpretive guidance F758 (Free from
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Coordination of Care Initiative Mora Area Community
 Coordination of Care Initiative Mora Area Community Community Meeting October 9, 2018 FirstLight Health System Download meeting agenda and slide handout: Agenda Presentation handout 2 1 Welcome Introductions
Coordination of Care Initiative Mora Area Community Community Meeting October 9, 2018 FirstLight Health System Download meeting agenda and slide handout: Agenda Presentation handout 2 1 Welcome Introductions
Developing an Organizational QAPI Plan
 Developing an Organizational QAPI Plan Kathleen Lavich, R.N. Senior Clinical Quality Consultant MPRO LeadingAge Michigan - 2017 Annual Conference and Trade Show MPRO: Our Work QUALITY IMPROVEMENT REVIEW
Developing an Organizational QAPI Plan Kathleen Lavich, R.N. Senior Clinical Quality Consultant MPRO LeadingAge Michigan - 2017 Annual Conference and Trade Show MPRO: Our Work QUALITY IMPROVEMENT REVIEW
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Aligning Efforts for DSME Data Collection. May M. Leonard, R.N., BSN, MSBA Angela M. Vanker, MPH
 Aligning Efforts for DSME Data Collection May M. Leonard, R.N., BSN, MSBA Angela M. Vanker, MPH Sept. 9, 2015 Lake Superior Quality Innovation Network (QIN) Michigan (MPRO) Minnesota (Stratis Health) Wisconsin
Aligning Efforts for DSME Data Collection May M. Leonard, R.N., BSN, MSBA Angela M. Vanker, MPH Sept. 9, 2015 Lake Superior Quality Innovation Network (QIN) Michigan (MPRO) Minnesota (Stratis Health) Wisconsin
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT
 Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
CMS s RAI Version 3.0 Manual October 2016
 Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Special Needs Program Training. Quality Management Department
 10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
The CMS Five Star Nursing Home Rating System An incomplete and inaccurate consumer tool
 The CMS Five Star Nursing Home Rating System An incomplete and inaccurate consumer tool Myth: The Centers for Medicare and Medicaid Services (CMS) 5 Star Nursing Home Quality rating system provides a useful
The CMS Five Star Nursing Home Rating System An incomplete and inaccurate consumer tool Myth: The Centers for Medicare and Medicaid Services (CMS) 5 Star Nursing Home Quality rating system provides a useful
2018 Increase Rate of Patients Dialyzing at Home Using the 7-Step Process Quality Improvement Activity (QIA)
") 2018 Increase Rate of Patients Dialyzing at Home Using the 7-Step Process Quality Improvement Activity (QIA) Donna DeBello, RN Quality Improvement Director Health Services Advisory Group (HSAG): End Stage
2018 Increase Rate of Patients Dialyzing at Home Using the 7-Step Process Quality Improvement Activity (QIA) Donna DeBello, RN Quality Improvement Director Health Services Advisory Group (HSAG): End Stage
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care
 Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Care Transitions: What Does It Really Look Like?
 Care Transitions: What Does It Really Look Like? Selena Bolotin, LICSW Director WA Patient Safety & Care Transitions June 5, 2014 Qualis Health is one of the nation s leading healthcare consulting organizations,
Care Transitions: What Does It Really Look Like? Selena Bolotin, LICSW Director WA Patient Safety & Care Transitions June 5, 2014 Qualis Health is one of the nation s leading healthcare consulting organizations,
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor of Medicine, Brown University
 Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
7/1/2011 EVERYTHING YOU NEED TO KNOW TO SUCCEED WITH THIS NEW PROCESS ABOUT LEAH I FOCUS ON LEARNING, NOT TEACHING
 BIP-PITY BOB-PITY BOO!!!!!! MAKE THE MDS 3.0 WORK FOR YOU IT IS NOT MAGIC!!!!!! Leah Klusch, RN, BSN, FACHCA EVERYTHING YOU NEED TO KNOW TO SUCCEED WITH THIS NEW PROCESS ABOUT LEAH I FOCUS ON LEARNING,
BIP-PITY BOB-PITY BOO!!!!!! MAKE THE MDS 3.0 WORK FOR YOU IT IS NOT MAGIC!!!!!! Leah Klusch, RN, BSN, FACHCA EVERYTHING YOU NEED TO KNOW TO SUCCEED WITH THIS NEW PROCESS ABOUT LEAH I FOCUS ON LEARNING,
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512)
") NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
NURSING FACILITIES: FRIENDS OR FOES? Marie C. Berliner Joy & Young, LLP Austin, Texas (512) 330-0228 Program Overview Status of Hospice Nursing Facility Relationships Multiple contact points and transactions
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Rehospitalizations: How Do You Measure Up?
 Rehospitalizations: How Do You Measure Up? National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Today s Objectives Recognize the role skilled nursing facilities
Rehospitalizations: How Do You Measure Up? National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Today s Objectives Recognize the role skilled nursing facilities
Objectives. Assisted Living. O 2 : Opportunities & Outcomes in Assisted Living. Presented by: Chief Clinical Officer
 O 2 : Opportunities & Outcomes in Assisted Living Presented by: Leigh Ann Frick, PT, MBA Chief Clinical Officer Melissa Moffitt, MS, CCC-SLP Senior Vice President of Senior Living Objectives Identify the
O 2 : Opportunities & Outcomes in Assisted Living Presented by: Leigh Ann Frick, PT, MBA Chief Clinical Officer Melissa Moffitt, MS, CCC-SLP Senior Vice President of Senior Living Objectives Identify the
Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study
 Case Study") Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study Happy Acres Nursing Center is a 99-bed skilled nursing facility (SNF). The facility is divided into
Infection Control Performance Improvement Quality Assurance & Performance Improvement (QAPI) Case Study Happy Acres Nursing Center is a 99-bed skilled nursing facility (SNF). The facility is divided into
Organization. Hospital to SNF Communication. Care Coordination Goals. Chasing the Perfect Handoff The Missing Link to Interoperability 7/18/2016
 Organization Chasing the Perfect Handoff The Missing Link to Interoperability Annette Brown, BSN, RN Director, Clinical Informatics Eisenhower Medical Center abrown@emc.org Not for profit, academic, community
Organization Chasing the Perfect Handoff The Missing Link to Interoperability Annette Brown, BSN, RN Director, Clinical Informatics Eisenhower Medical Center abrown@emc.org Not for profit, academic, community
Model of Care Training
 Medicare Advantage Special Needs Plan Chronic Care Program Model of Care Training 2012-2013 Course Overview This course will describe: PHP s Model of Care Chronic Care Program Health Homes Interdisciplinary
Medicare Advantage Special Needs Plan Chronic Care Program Model of Care Training 2012-2013 Course Overview This course will describe: PHP s Model of Care Chronic Care Program Health Homes Interdisciplinary
Nursing Home Walk of Fame Visiting What Really Works. Call in Number
 Nursing Home Walk of Fame Visiting What Really Works Call in Number 877.442.2859 Enter to Win Book Giveaways! Type in a successful practice (one or two sentences) from your nursing home in the chat box.
Nursing Home Walk of Fame Visiting What Really Works Call in Number 877.442.2859 Enter to Win Book Giveaways! Type in a successful practice (one or two sentences) from your nursing home in the chat box.
Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage
 Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage March 23, 2011 marks the oneyear anniversary of the signing of the Patient Protection and
Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage March 23, 2011 marks the oneyear anniversary of the signing of the Patient Protection and
Webinar Objectives. Coordination of Care Initiative Home Health Gap Collaborative Informational Webinar
 Coordination of Care Initiative Home Health Gap Collaborative Informational Webinar February 14, 2018 Webinar Objectives Discuss the analysis findings for home health referrals, post hospital discharge,
Coordination of Care Initiative Home Health Gap Collaborative Informational Webinar February 14, 2018 Webinar Objectives Discuss the analysis findings for home health referrals, post hospital discharge,
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
2019 Quality Improvement Program Description Overview
 2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR
 CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
The Patient Centered Medical Home: 2011 Status and Needs Study
 The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
Get A Seat at the Table
 Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations. Aetna s Compassionate Care SM Program
 Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
GEORGIA CHAPTER CASE MANAGEMENT CONFERENCE
 WWW.ACMAWEB.ORG/GA 6th Annual GEORGIA CHAPTER CASE MANAGEMENT CONFERENCE The Classic Center Athens, GA 2-FOR-1 REGISTRATION OFFER! SESSION DESCRIPTIONS KEYNOTE ADDRESS The Healing Power of Laughter Diana
WWW.ACMAWEB.ORG/GA 6th Annual GEORGIA CHAPTER CASE MANAGEMENT CONFERENCE The Classic Center Athens, GA 2-FOR-1 REGISTRATION OFFER! SESSION DESCRIPTIONS KEYNOTE ADDRESS The Healing Power of Laughter Diana
Continuing Education Disclosures
 Supporting CHF Patients in the Home Setting through a Comprehensive Community Approach Diane Schuh, RN, BSN Aurora Sheboygan Memorial Medical Center September 26, 2017 Continuing Education Disclosures
Supporting CHF Patients in the Home Setting through a Comprehensive Community Approach Diane Schuh, RN, BSN Aurora Sheboygan Memorial Medical Center September 26, 2017 Continuing Education Disclosures
QAPI: Systematic Analysis and Systemic Action via Plan-Do-Study-Act Cycles. Objectives QAPI. Regulatory Phases
 QAPI: Systematic Analysis and Systemic Action via Plan-Do-Study-Act Cycles Emily Nelson and Diane Dohm MetaStar/Lake Superior Quality Innovation Network Objectives Obtain a high-level overview of QAPI
QAPI: Systematic Analysis and Systemic Action via Plan-Do-Study-Act Cycles Emily Nelson and Diane Dohm MetaStar/Lake Superior Quality Innovation Network Objectives Obtain a high-level overview of QAPI
Oregon Health Plan Care Coordination Program (OHPCC)
") Oregon Health Plan Care Coordination Program (OHPCC) John DiPalma, Executive Director KEPRO Oregon Dr. Jeffrey McWilliams, MD, Medical Director KEPRO Oregon Michael Wolf, Vice President of Government Relations
Oregon Health Plan Care Coordination Program (OHPCC) John DiPalma, Executive Director KEPRO Oregon Dr. Jeffrey McWilliams, MD, Medical Director KEPRO Oregon Michael Wolf, Vice President of Government Relations
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
MDS Accuracy and Compliance: Where There s Smoke
 MDS Accuracy and Compliance: Where There s Smoke November 2014 1 Objectives List the current trends in the Long Term Care industry that are driving scrutiny into the MDS assessment process Identify the
MDS Accuracy and Compliance: Where There s Smoke November 2014 1 Objectives List the current trends in the Long Term Care industry that are driving scrutiny into the MDS assessment process Identify the
Santa Clara Care Coordination Collaborative Meeting. Debra Nixon, PhD, MSHA, BSN Corporate Advisor Health Services Advisory Group (HSAG) June 8, 2018
 June 8, 2018") Santa Clara Care Coordination Collaborative Meeting Debra Nixon, PhD, MSHA, BSN Corporate Advisor Health Services Advisory Group (HSAG) June 8, 2018 You Are Here! Improving care coordination together with
Santa Clara Care Coordination Collaborative Meeting Debra Nixon, PhD, MSHA, BSN Corporate Advisor Health Services Advisory Group (HSAG) June 8, 2018 You Are Here! Improving care coordination together with
Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways
 Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways") Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways 1 What is On Lok? Original Vision: Help the low-income
Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways 1 What is On Lok? Original Vision: Help the low-income
STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT EXECUTIVE SUMMARY
 STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT Prepared by: THE BUCKLEY GROUP, L.L.C. OVERVIEW The Osawatomie State Hospital (OSH) in Osawatomie
STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT Prepared by: THE BUCKLEY GROUP, L.L.C. OVERVIEW The Osawatomie State Hospital (OSH) in Osawatomie
New Facts and Figures on Hospice Care in America
 New Facts and Figures on Hospice Care in America NHPCO has just released the 2010 edition of NHPCO Facts and Figures: Hospice Care in America. Through an easy-to-read narrative that is written for the
New Facts and Figures on Hospice Care in America NHPCO has just released the 2010 edition of NHPCO Facts and Figures: Hospice Care in America. Through an easy-to-read narrative that is written for the
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
SNF Requirements of Participation. Knowing Your Organization, Your Residents, Your Staff, and Your Resources
 SNF Requirements of Participation Knowing Your Organization, Your Residents, Your Staff, and Your Resources Develop Your Facility-Wide Resource Assessment for Phase 2 Objectives Recognize the key concepts
SNF Requirements of Participation Knowing Your Organization, Your Residents, Your Staff, and Your Resources Develop Your Facility-Wide Resource Assessment for Phase 2 Objectives Recognize the key concepts
Exploring the Possibilities with MIDAS+ SmartConnect
 June 1 3, 2009 Westin La Paloma Resort Tucson, Arizona Exploring the Possibilities with MIDAS+ SmartConnect Leverage your existing MIDAS+ Care Management tools and consider automating your transition planning
June 1 3, 2009 Westin La Paloma Resort Tucson, Arizona Exploring the Possibilities with MIDAS+ SmartConnect Leverage your existing MIDAS+ Care Management tools and consider automating your transition planning
Medicare: 2018 Model of Care Training
 Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
Trends in Nursing Facility Standard Health Survey Citations
 Trends in Nursing Facility Standard Health Survey Citations Prepared by Research Department American Health Care Association March 2015 Trends in Nursing Facilities Standard Health Survey Citations TABLE
Trends in Nursing Facility Standard Health Survey Citations Prepared by Research Department American Health Care Association March 2015 Trends in Nursing Facilities Standard Health Survey Citations TABLE