INTERACT 4 Patty Abele, FNP BC
|
|
|
- Lesley Manning
- 5 years ago
- Views:
Transcription

1 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the INTERACT program and the strategies it uses to improve care and prevent avoidable hospitalizations Identify the quality improvement, communication, advance care planning, and decision support tools used in the INTERACT 4 program MISSOURI QUALITY IMPROVEMENT (MOQI) INTIATIVE FOR NURSING HOMES Response to Centers for Medicare and Medicaid Services (CMS) funding opportunity: Initiative to Reduce Avoidable Hospitalizations University of Missouri Sinclair School of Nursing, Quality Improvement Program for Missouri (QIPMO), Primaris (Missouri Quality Improvement Organization), MHC (Missouri Health Connection, a federally designated Health Information Exchange service for MO) and others 14.8 million dollar grant Four year demonstration project 16 nursing homes in St. Louis Area Initiated early



2 WHY ST. LOUIS? Identified as a region with the highest rehospitalizations for key diagnoses of AMI, CHF, pneumonia, and high 30 day hospital readmissions. Identified NHs with good quality care/survey history with high hospitalization rates to high re hospitalization hospitals HOSPITALIZATIONS ARE EXPENSIVE AND DANGEROUS FOR FRAIL ELDERS 1 in 5 Medicare patients discharged from hospital in US are readmitted within 30 days at cost of over $15 billion each year 45% of re admissions could be avoided 30 67% of hospitalizations among NH residents could be prevented AGS 58: , 2010 r 2010, Copyright the Authors Journal compilation r 2010, The American Geriatrics Society N Engl J Med 2011; 365:


 Hospitalized Residents Risk: Disorientation Delirium Functional decline")
3 Potentially Avoidable Hospitalization (PAH) Rates by State for SOURCE: Chronic Condition Warehouse, MMRR 2014: Volume 4 (1) Highly Prevalent Conditions Associated with Potentially Avoidable Hospitalizations in 2009 NOTE: * Pneumonia was only considered as the primary diagnosis for a potentially avoidable hospitalizations for beneficiaries in institutions. SOURCE: Chronic Condition Warehouse, MMRR 2014: Volume 4 (1) Hospitalized Residents Risk: Disorientation Delirium Functional decline Immobility Pressure ulcers Falls Poly pharmacy Medication errors Incontinence and catheter use Hospital acquired infections 3

4 WHAT ARE THE MAJOR CAUSES OF UNNECESSARY HOSPITALIZATIONS FROM LONG TERM CARE FACILITIES? Not recognizing changes in condition soon enough Lack of adequate staffing Lack of lab, x ray or pharmacy services Lack of availability of on site physicians, NPs, PAs Poor communication with HCP, on call provider Lack of advance care planning or advance directives Resident and/or family preferences Concern about possible legal liability concern about possible survey citations Others? What can the hospital/er do for my patient that I can t do right here? Know your nursing home s capabilities: Lab work Xray, ultrasound, doppler, EKG SQ fluids, IV fluids, and antibiotics Tube feeding Oxygen, CPAP, breathing treatments, trach care Complex wound management PT/OT/ST WHY IT MATTERS Improve quality of care for residents with fewer complications and reduced cost Financial and regulatory incentives changing: Current situation, which favors hospital transfers, is going to change. Medicare changing payment to reward lower rates of avoidable hospitalizations. Surveyors will be examining how facilities assess and manage acute changes in status. Affordable Care Act mandates that each facility have a Quality Assurance and Performance Improvement (QAPI) program. Improving management of acute change in condition and reducing avoidable hospital transfers is one potential focus for QAPI work Reducing Hospitalizations Safely is a new goal for Advancing Excellence in America s Nursing Homes campaign 4

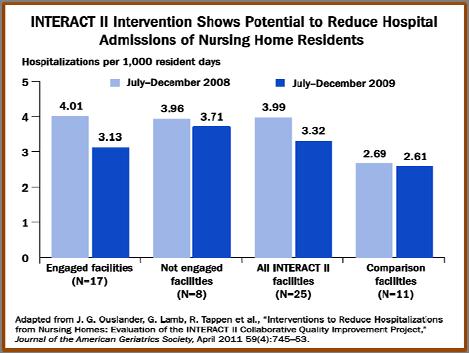
5 INTERACT stands for INTERVENTIONS TO REDUCE ACUTE CARE TRANSFERS is a quality improvement program designed to improve the care of nursing home residents with acute changes in condition. INTERACT PROGRAM The INTERACT Program was designed by Dr. Joseph Ouslander, MD and Mary Perloe, GNP at the Georgia Medical Care Foundation Project was supported by Centers for Medicare and Medicaid Services (CMS) The program was designed to help nursing homes improve their early illness detection skills so that residents could remain in the NH, and receive care for acute illnesses Revised based on input from staff from several nursing homes and national experts in a project supported by The Commonwealth Fund Interventions to Reduce Hospitalizations from Nursing Homes: Evaluation of the INTERACT II Collaborative Quality Improvement Project (J Am Geriatric Soc 59: , 2011) 25 NHs, 3 states, 6 month project providing tools, on site education, facility based champion, biweekly teleconferences facilitated by APRN Overall 17 % reduction in hospital admissions: 24%, compared with 6%, in NHs rated as engaged For an average size 100 bed NH, this would mean an average decrease of ~25 hospitalizations per year, or ~2 less per month Cost of implementation $7,700 per NH Would result in $125,000 savings to Medicare Part A per year Total projected savings based on 100 bed NH $117,000 per year per NH Challenges in implementing: no potent incentive to NH, competing priorities, high turnover, hospitalization rates self reported with questionable accuracy, short interval of study 5


6 6
7 INTERACT GOALS Reduce hospital transfers by: Preventing conditions from becoming severe enough to require hospitalization Early recognition of resident change in condition Accurate documentation and communication of assessment Managing some conditions in the NH when this is feasible and safe Awareness of Capabilities of the nursing home Improving advance care planning and the use of palliative care plans when appropriate as an alternative to hospitalization Early discussions with residents and families about hospitalizations Improving care transitions via improved communication with hospitals and medication reconciliation Analysis of acute care transfers to identify opportunities to reduce transfers that might be preventable Tracking hospitalizations, examining trends, root cause analysis to focus educational and care process improvement activities SUCCESS REQUIRES A WIDE SCALE CULTURAL CHANGE ACROSS THE WHOLE NURSING HOME Hundreds of nursing homes are using the INTERACT tools, but Dr. Ouslander believes relatively few have comprehensively adopted the entire program. Requires a major change in the way care is delivered Can not be effectively implemented or sustained without: Organizational commitment Administrators actively involved A team approach with a team champion; Engagement of staff and HCPs ( buy in ) Integration of program and tools into everyday care (tools visible and accessible) Many complex issues, social and relationship issues with family and HCP come into play as nursing home staff consider hospital transfers (Lola Butcher Bulletins/2012/July) INTERACT TOOLS Communication Tools Stop & Watch SBAR Med Reconciliation Worksheet Post Hospital Nursing Home Capabilities List NH to Hospital Transfer Form Acute Care Transfer Checklist Decision Support Tools Change in Condition File Cards Care Paths Advanced Care Planning Tools Advanced Care Planning Tracking Tool Advanced Care Planning Communication Guide Comfort Care Order Set Educational Handouts: Going to the Hospital, CPR, Tube Feeding Quality Improvement Tool for Review of Acute Care Transfers 7

, and these criteria are now included in the")
8 INTERACT Version 4.0 Tools New! Important changes include: 1. The SBAR Communication Form and Progress Note has been substantially revised to make it a more comprehensive and user friendly nursing evaluation that helps guide and document critical thinking in an efficient way. Changes have been made to several areas of terminology in response to user concerns and suggestions. 2. The criteria for notifying the clinician have been made more consistent between the Decision Support Tools (Change in Condition File Cards and Care Paths), and these criteria are now included in the revised SBAR. 3. The Stop and Watch early warning tool has been revised to facilitate its use in routine monitoring of high risk residents by adding a checkbox for "no change". 4. The Advance Care Planning Tracking Tool has been revised to include brief documentation of discussions, which are often not clearly communicated over time or during care transitions. STOP AND WATCH The Stop and Watch Early Warning Tool prompts staff, including CNAs, dietary, rehab and environmental services, to be alert for potential change in condition indicators. This tool provides a simple, clear way to communicate changes in condition to nursing staff. has been revised to facilitate its use in routine monitoring of high risk residents by adding a checkbox for no change. What does SBAR stand for? OLD VERSION: S = Situation INTERACT 4 VERSION: S = Situation B = Background B = Background A = Assessment A = Appearance R = Request R = Review and Notify 8
:")
 Check Vital Signs Review")



9 Action requested of SBAR Before calling Health Care Provider (HCP): Evaluate resident (see section B and A) Check Vital Signs Review Record: recent progress notes, labs, orders Review INTERACT Care Path or Acute Change in Condition card, if indicated (each nursing unit has this info) Have relevant info available when reporting SBAR INTERACT 4 SBAR 9




10 What does research say about use of SBAR? When INTERACT SBAR tool is consistently used: 1. HCP feel they are given better reports 2. Care of residents improves 3. Hospitalizations decline CHANGE IN CONDITION GUIDE Dehydration Fever Acute Mental Status Change/Confusion Behavioral Symptoms of Dementia New or Worsening Symptoms of CHF Symptoms of UTI Symptoms of LRI Shortness of Breath GI Symptoms CAREPATHS 10


11 11


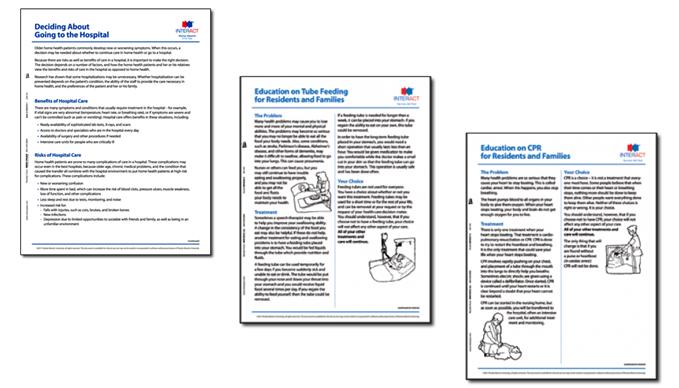
12 ADVANCE CARE PLANNING TOOLS ADVANCE CARE PLANNING EDUCATIONAL MATERIALS 12

13 A GOOD DEATH Is not the logical conclusion of healthy aging a good death? Myra Christopher 9 out of 10 adults polled in mid 1990 s would prefer to be cared for at home if they were terminally ill with 6 months or less to live 71% of Americans believe quality of life for the seriously ill is more important than extending life through every medical intervention possible DEATH DENYING SOCIETY We don t acknowledge the end of life like we do birth GOOD GERIATRIC CARE = GOOD PALLIATIVE CARE One way around end of life denial has been to discuss palliative care much earlier in a person s disease process or life. Nursing homes need to be in the business of providing high quality palliative and end of life care Huge opportunity for nursing homes to develop expertise in providing this care Robust advance care planning, care preferences clearly documented and followed, adept at caring for and managing symptoms like pain, partnering with palliative consultants and hospice 13






14 PUTTING IT ALL TOGETHER USING INTERACT THREE CHEERS FOR FINANCIAL INDEPENDENCE!! 3 GENERATIONS OF NURSES! 14
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Reducing Potentially Avoidable Hospitalizations of Nursing Home Residents
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for
4/13/2015. I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS.
 Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Why try to reduce hospitalizations? How many are avoidable?
 Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
OPTIMISTIC 8/13/2014. Outline OBJECTIVES
 OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
Tools Use Suggested Formats. All facility staff Provides a visual depiction of INTERACT in daily practice
 INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Agenda: Noon Overview of the regulatory sections affected by the Reform of RoP in Phase 2
 Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
INTERACT for Assisted Living
 INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services
 Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical
Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical
Transfer Trauma: A Trip to the ER Can Put an Older Adult at Risk
 Transfer Trauma: A Trip to the ER Can Put an Older Adult at Risk Mukaila Raji, MD, MSC Professor and Director, Internal Medicine-Geriatrics Program Director, UTMB Geriatric Fellowship Department of Internal
Transfer Trauma: A Trip to the ER Can Put an Older Adult at Risk Mukaila Raji, MD, MSC Professor and Director, Internal Medicine-Geriatrics Program Director, UTMB Geriatric Fellowship Department of Internal
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
February 27, Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models
 1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative
 Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative UPMC Senior Communities Skilled Nursing Facilities UPMC Senior Communities: Who are We? 5 Skilled Nursing Facilities 5 Personal
Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative UPMC Senior Communities Skilled Nursing Facilities UPMC Senior Communities: Who are We? 5 Skilled Nursing Facilities 5 Personal
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
An Innovative Approach to Identifying and Communicating Change of Condition
 An Innovative Approach to Identifying and Communicating Change of Condition Introduction to INTERACT II Presenters Cathy Lipton, Senior Medical Director, Evercare, cathy_lipton@uhc.com Pam O Rourke, VP
An Innovative Approach to Identifying and Communicating Change of Condition Introduction to INTERACT II Presenters Cathy Lipton, Senior Medical Director, Evercare, cathy_lipton@uhc.com Pam O Rourke, VP
Nursing Home Pearls or
 Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT
 04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
Rhonda Dickman, RN, MSN, CPHQ
 Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert-
 New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert- Rodney Farley, CHC Terry Raser, RN, RAC-CT, C-NE LW Consulting, Inc. LW Consulting, Inc. 5925 Stevenson Ave, Suite G 5925 Stevenson Ave,
New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert- Rodney Farley, CHC Terry Raser, RN, RAC-CT, C-NE LW Consulting, Inc. LW Consulting, Inc. 5925 Stevenson Ave, Suite G 5925 Stevenson Ave,
Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through Telemedicine
 PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics
 Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
The Case for Home Care Medicine: Access, Quality, Cost
 The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
Critical Thinking Steps
 CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations. Aetna s Compassionate Care SM Program
 Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents. Payment Model
 Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
CGS Administrators, LLC Clinical Hospice Documentation from CGS Missouri Hospice & Palliative Care Assoc. October 3, 2016
 Missouri Hospice & Palliative Care Conference Reviewer s decision is reliant upon documentation Results in a full denial for the submission Documentation must be legible Medical necessity is always based
Missouri Hospice & Palliative Care Conference Reviewer s decision is reliant upon documentation Results in a full denial for the submission Documentation must be legible Medical necessity is always based
improvement program to Electronic Health variety of reasons, experts suggest that up to
 Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home. Your thoughts
 Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
MDS 3.0: What Leadership Needs to Know
 MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
Using Quality Data to Market to Referral Sources BUSINESS OF HEALTHCARE
 Using Quality Data to Market to Referral Sources Cindy Mason Change as a Matter of Survival BUSINESS OF HEALTHCARE 2 National Transformation of Healthcare the Affordable Care Act provides CMS the flexibility
Using Quality Data to Market to Referral Sources Cindy Mason Change as a Matter of Survival BUSINESS OF HEALTHCARE 2 National Transformation of Healthcare the Affordable Care Act provides CMS the flexibility
Hospice and End of Life Care and Services Critical Element Pathway
 Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
The Medicare Hospice Benefit. What Does It Mean to You and Your Patients?
 The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
The Medicare Hospice Benefit What Does It Mean to You and Your Patients? The Medicare Hospice Benefit By the time Congress established the Medicare Hospice Benefit in 1982, hundreds of organizations in
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Long-Term Care Program
 Long-Term Care Program Long-Term Care Program p.1 Program Overview Nurses Improving Care for Healthysystem Elders (NICHE) is a nursing education and consultation program designed to improve geriatric
Long-Term Care Program Long-Term Care Program p.1 Program Overview Nurses Improving Care for Healthysystem Elders (NICHE) is a nursing education and consultation program designed to improve geriatric
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW
 CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-242-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-242-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017
 NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017 Disclaimer: The information contained in this presentation is representative of the current information provided
NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017 Disclaimer: The information contained in this presentation is representative of the current information provided
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
CMS s RAI Version 3.0 Manual October 2016
 Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
HealthStream Regulatory Script
 HealthStream Regulatory Script [EMTALA] Version: [May 2005] Lesson 1: Introduction Lesson 2: History and Enforcement Lesson 3: Medical Screening Lesson 4: Stabilizing Care Lesson 5: Appropriate Transfer
HealthStream Regulatory Script [EMTALA] Version: [May 2005] Lesson 1: Introduction Lesson 2: History and Enforcement Lesson 3: Medical Screening Lesson 4: Stabilizing Care Lesson 5: Appropriate Transfer
QUALITY MEASURES WHAT S ON THE HORIZON
 QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Is It Really a UTI? Do You Know It When You See It?
 Is It Really a UTI? Do You Know It When You See It? Today s Objectives 1. Define Symptomatic UTI versus Asymptomatic Bacteriuria 2. Review RAI MDS Coding Manual Definition of UTI 3. Analyze UTI as a Quality
Is It Really a UTI? Do You Know It When You See It? Today s Objectives 1. Define Symptomatic UTI versus Asymptomatic Bacteriuria 2. Review RAI MDS Coding Manual Definition of UTI 3. Analyze UTI as a Quality
Patient and Family Caregiver Interview Tool
 Patient and Family Caregiver Interview Tool Instructions: We recommend you select at least 5-10 patients who have been readmitted to your organization within the past 30 days to include in the group of
Patient and Family Caregiver Interview Tool Instructions: We recommend you select at least 5-10 patients who have been readmitted to your organization within the past 30 days to include in the group of
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Putting the Patient at the Center of Care
 CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
The New Survey Process What To Expect Paula G. Sanders, Esq.
 PHCA Webinar February 14, 2018 The New Survey Process What To Expect Paula G. Sanders, Esq. DEPARTMENT OF HEALTH ENFORCEMENT TRENDS How to Read State Tags DOH CMPs Per Year 2014-2017 2014 $79,250.00 2015
PHCA Webinar February 14, 2018 The New Survey Process What To Expect Paula G. Sanders, Esq. DEPARTMENT OF HEALTH ENFORCEMENT TRENDS How to Read State Tags DOH CMPs Per Year 2014-2017 2014 $79,250.00 2015
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Housekeeping. Harmony Healthcare International, Inc.
 Tackling Avoidable Readmission through Care Transition: PART I HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Diane Buckley, BSN, RN, RAC-CT Director
Tackling Avoidable Readmission through Care Transition: PART I HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Diane Buckley, BSN, RN, RAC-CT Director
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Nursing Home Walk of Fame Visiting What Really Works. Call in Number
 Nursing Home Walk of Fame Visiting What Really Works Call in Number 877.442.2859 Enter to Win Book Giveaways! Type in a successful practice (one or two sentences) from your nursing home in the chat box.
Nursing Home Walk of Fame Visiting What Really Works Call in Number 877.442.2859 Enter to Win Book Giveaways! Type in a successful practice (one or two sentences) from your nursing home in the chat box.
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Community Data Update Knoxville Community Readmissions Coalition January 25 th, 2018
 Community Data Update Knoxville Community Readmissions Coalition January 25 th, 2018 Corley Roberts, MHA, CPHQ, ACSM EP-C, EIM Quality Improvement Advisor, Qsource/atom Alliance croberts@qsource.org Readmissions
Community Data Update Knoxville Community Readmissions Coalition January 25 th, 2018 Corley Roberts, MHA, CPHQ, ACSM EP-C, EIM Quality Improvement Advisor, Qsource/atom Alliance croberts@qsource.org Readmissions
LTC Discharge and Transfer Requirements. Revised October 24, 2017
 LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
LTC Discharge and Transfer Requirements Revised October 24, 2017 OUTLINE Transitions of Care LTC Discharge and Transfer Documentation Requirements Intent of the Regulations TRANSITIONS OF CARE Understanding
The RoPs are here! Do you know what s changing?
 The RoPs are here! Do you know what s changing? Mary Madison, RN, RAC-CT, CDP Clinical Consultant, LTC/Senior Care Briggs Healthcare March 7, 2017 2 What we ll cover today CMS goals behind the updated
The RoPs are here! Do you know what s changing? Mary Madison, RN, RAC-CT, CDP Clinical Consultant, LTC/Senior Care Briggs Healthcare March 7, 2017 2 What we ll cover today CMS goals behind the updated
Effective Tools to Prevent and Manage Adverse Events
 Effective Tools to Prevent and Manage Adverse Events Based on Office of Inspector General Adverse Events Report Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com Objectives Upon completion
Effective Tools to Prevent and Manage Adverse Events Based on Office of Inspector General Adverse Events Report Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com Objectives Upon completion
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
WAR AGAINST PRESSURE ULCERS
 WAR AGAINST PRESSURE ULCERS KINGS HARBOR MULTICARE CENTER Liezel T. Vince Cruz, ANP-BC, WCC Louis A. Kaplan, PA-C, CWS, WCC Roy J. Goldberg, MD, FACP, AGSF, CMD Pressure Ulcers Pressure ulcers, also known
WAR AGAINST PRESSURE ULCERS KINGS HARBOR MULTICARE CENTER Liezel T. Vince Cruz, ANP-BC, WCC Louis A. Kaplan, PA-C, CWS, WCC Roy J. Goldberg, MD, FACP, AGSF, CMD Pressure Ulcers Pressure ulcers, also known
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
INTERACT INSIGHTS. Greater New York Hospital Association Continuing Care Leadership Coalition
 INTERACT INSIGHTS A GUIDE OF INSIGHTS AND LESSONS LEARNED FOLLOWING EXPERIENCES WITH THE INTERVENTIONS TO REDUCE PREVENTABLE ACUTE CARE TRANSFERS IN NEW YORK (INTERACT NY) PROGRAM. Greater New York Hospital
INTERACT INSIGHTS A GUIDE OF INSIGHTS AND LESSONS LEARNED FOLLOWING EXPERIENCES WITH THE INTERVENTIONS TO REDUCE PREVENTABLE ACUTE CARE TRANSFERS IN NEW YORK (INTERACT NY) PROGRAM. Greater New York Hospital
Reimbursement Policy. Subject: Inpatient Readmissions Committee Approval Obtained: Effective Date: 10/01/13
 Reimbursement Policy Subject: Inpatient Readmissions Committee Approval Obtained: Effective Date: 10/01/13 Section: Facilities 04/03/17 *****The most current version of the Reimbursement Policies can be
Reimbursement Policy Subject: Inpatient Readmissions Committee Approval Obtained: Effective Date: 10/01/13 Section: Facilities 04/03/17 *****The most current version of the Reimbursement Policies can be
POLST: What s New and How Can We Do Better? Pam Hiransomboon-Vogel, DNP, FNP-BC, ACHPN
 POLST: What s New and How Can We Do Better? Pam Hiransomboon-Vogel, DNP, FNP-BC, ACHPN The OHSU Center for Ethics in Health Care and POLST Program, have no relevant financial relationships to disclose
POLST: What s New and How Can We Do Better? Pam Hiransomboon-Vogel, DNP, FNP-BC, ACHPN The OHSU Center for Ethics in Health Care and POLST Program, have no relevant financial relationships to disclose
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Effective Tools to Prevent and Manage Adverse Events: Lesson 2
 Effective Tools to Prevent and Manage Adverse Events: Lesson 2 Based on the Office of Inspector General Adverse Events Report February 2014 Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com
Effective Tools to Prevent and Manage Adverse Events: Lesson 2 Based on the Office of Inspector General Adverse Events Report February 2014 Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Using Quality Data to Market to Referral Sources. Kim Hicks
 Using Quality Data to Market to Referral Sources Kim Hicks Change as a Matter of Survival BUSINESS OF HEALTHCARE 3 What s Happening here? It costs Medicare about $26 billion a year, with about $17 billion
Using Quality Data to Market to Referral Sources Kim Hicks Change as a Matter of Survival BUSINESS OF HEALTHCARE 3 What s Happening here? It costs Medicare about $26 billion a year, with about $17 billion
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Evidence-Based Medicine and Long- Term Care: Improving Outcomes in Pennsylvania Nursing Homes
 Evidence-Based Medicine and Long- Term Care: Improving Outcomes in Pennsylvania Nursing Homes Beryl Goldman Richard Lee Malcolm Morrison Sue Nonemaker Barry Fogel, Moderator Today s Presentations PA Department
Evidence-Based Medicine and Long- Term Care: Improving Outcomes in Pennsylvania Nursing Homes Beryl Goldman Richard Lee Malcolm Morrison Sue Nonemaker Barry Fogel, Moderator Today s Presentations PA Department
Objectives 2/23/2011. Crossing Paths Intersection of Risk Adjustment and Coding
 Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Palliative and Hospice Care In the United States Jean Root, DO
 Palliative and Hospice Care In the United States Jean Root, DO Hello. My name is Jean Root. I am an Osteopathic Physician who specializes in Geriatrics, or care of the elderly. I teach and practice Geriatric
Palliative and Hospice Care In the United States Jean Root, DO Hello. My name is Jean Root. I am an Osteopathic Physician who specializes in Geriatrics, or care of the elderly. I teach and practice Geriatric