Addressing diabetes disparities on the South Side of Chicago: Combining community strengths with health system innovation
|
|
|
- Martin Russell
- 5 years ago
- Views:
Transcription
1 Addressing diabetes disparities on the South Side of Chicago: Combining community strengths with health system innovation Michael M. Davis Lecture Series Center for Health Administration Studies Monica E. Peek, MD, MPH Section of General Internal Medicine Chicago Center for Diabetes Translation Research Center for the Study of Race, Politics and Culture




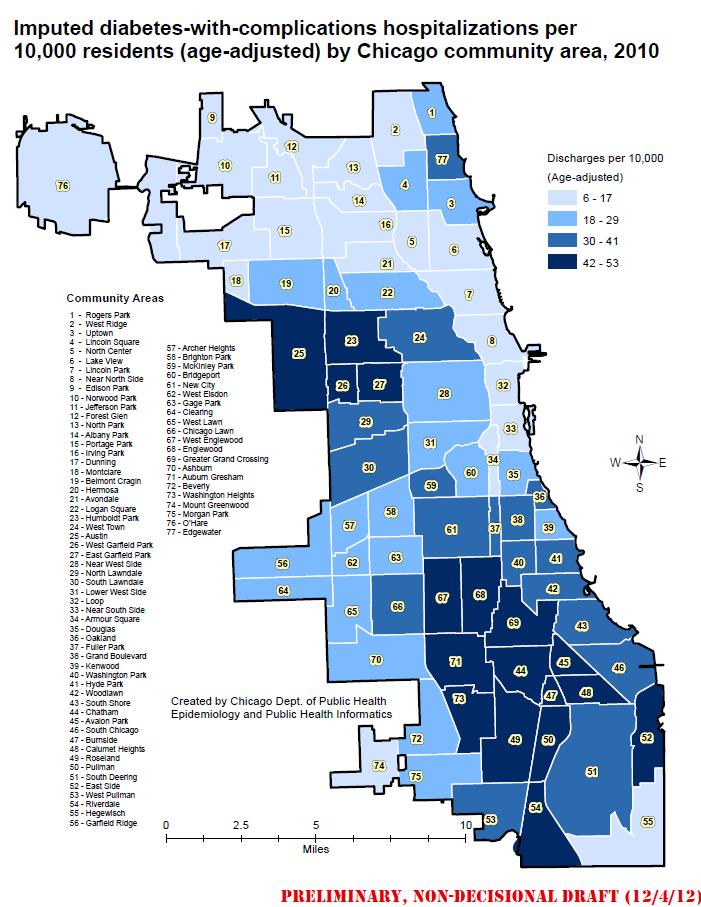
2 South Side of Chicago Challenges: Poverty Social challenges Food deserts Unsafe recreation Mistrust of healthcare Weakened hospital safety net Strengths Historical social, political and cultural traditions Community resources and institutions Healthcare institutions
3 Diabetes Health Disparities African-Americans have worse diabetes health indicators Higher incidence and prevalence of disease Worse control of diabetes, lipids, blood pressure 2-4 times the rate of complications (retinopathy, ESRD, amputations) South Side of Chicago 19% estimated prevalence 5x rate of LE amputation

4
5

6
7
 Health systems interventions (e.g. diabetes registries) Few multi-target interventions with community partnerships No existing literature on interventions that target the patient/provider relationship Peek ME, Cargill A, Huang E.")
8 Health Care Interventions to Reduce Diabetes Health Disparities Patient interventions (e.g. community health workers) Provider interventions (e.g. practice guidelines) Support staff interventions (e.g. RN case manager) Health systems interventions (e.g. diabetes registries) Few multi-target interventions with community partnerships No existing literature on interventions that target the patient/provider relationship Peek ME, Cargill A, Huang E. Diabetes health disparities: A systematic review of health care interventions. Med Care Res Rev. 2007;64(5):101S-156S.
9 Improving Diabetes Care and Outcomes on Chicago s South Side QI + Disparities Geographic areas Community + Healthcare systems Chronic care model
10 Short-term goals: Improve access to care Improve quality of care Improve clinical outcomes Project Goals Long-term goals: Strengthen partnerships among HCs, CBOs and University of Chicago Empower communities to address diabetes Be sustainable
11 6 Participating Health Centers ACCESS Booker Family Health Center ACCESS Grand Boulevard Health Center Chicago Family Health Center Friend Family Health Center University of Chicago Kovler Diabetes Center University of Chicago Primary Care Group
12 Conceptual Model Community Partnerships The Chronic Care Model Quality Improvement Community Health Systems Patient Practice Team Patient Activation Provider Training
13 Community Partnerships The Chronic Care Model Quality Improvement Community Health Systems Patient Practice Team Patient Activation Provider Training

14


15 Quality Improvement QI teams/collaborative One-on-one coaching Quarterly mtgs Organizational process evaluation/improvement PDSA cycles
 vs. <50% in controls -2.0 HbA1c at 6 mo (-3.")
16 Quality Improvement Nurse care management UC Primary Care Diabetes education, insulin initiation/titration, care management Evidence: 100% compliance w/ ADA standards (HbA1c, lipids, foot exam, kidney tests) vs. <50% in controls -2.0 HbA1c at 6 mo (-3.5 HbA1c w/in group Δ) 5x increased odds of retinopathy culturally-tailored case mgmt (RN + dietician)

17 Quality Improvement Diabetes group visits Shared medical appts (SMA) 2 FQHCs Diabetes education, medication titration/clinical care, support group Improved patient/provider satisfaction Some evidence re: reduced costs, hospitalizations and improved health outcomes (lower blood pressure)


18 Quality Improvement Nurse care management Diabetes group visits Care coordination Population Management TEAM-BASED CARE
19 ACIC Domain Mean score (0-10) (lowest score, highest score) Mar-09 Jun-10 Dec-10 Jun-11 Trend Organization of the Health Care System 6.6 (4.2, 8.5) 5.5 (3.2, 7.0) 7.1 (5.0, 9.3) 7.6 (5.8, 8.5) + Linkages to Community Resources 4.0 (2.7, 7.3) 3.8 (2.3, 5.3) 5.1 (2.7, 6.3) 5.8 (5.0, 8.3) + Diabetes Self-Management Support 6.1 (3.3, 8.8) 6.1 (4.0, 7.5) 6.8 (4.3, 10.0) 7.1 (5.8, 8.5) + Decision Support 5.1 (4.3, 6.3) 5.2 (3.3, 6.5) 6.2 (4.8, 10.0) 6.1 (4.5, 8.5) Delivery System Design 5.4 (4.5, 6.7) 4.9 (4.0, 6.7) 7.0 (6.0, 9.3) 7.2 (5.8, 8.8) + Clinical Information Systems 5.1 (2.4, 8.8) 5.0 (1.4, 6.6) 5.8 (4.6, 7.8) 7.2 (6.0, 8.0) + Integration 4.3 (3.3, 7.7) 4.3 (3.0, 6.2) 5.2 (4.0, 6.3) 6.1 (5.2, 7.7) + Average Score 5.2 (4.2, 7.3) 5.0 (3.6, 5.7) 6.1 (4.9, 7.2) 6.7 (6.1, 7.6) + ACIC v3.5 Copyright 2000, The MacColl Institute for Healthcare Innovation, Group Health Cooperative
20 Community Partnerships The Chronic Care Model Quality Improvement Community Health Systems Patient Practice Team Patient Activation Provider Training
21
 Updates on management of diabetes hypertension, hyperlipidemia,")
22 Provider Intervention Provider communication training Cultural competency Behavioral change Motivational Interviewing Patient/provider communication and Shared Decision-Making Continuing medical education (CME) Updates on management of diabetes hypertension, hyperlipidemia, etc.
23 Community Partnerships The Chronic Care Model Quality Improvement Community Health Systems Patient Practice Team Patient Activation Provider Training

24


25 Patient Activation Patient communication training Culturally tailored diabetes education Shared decision-making 2-3 hr classes x 10 weeks Community linkages Results: 86% attended > 70% classes Improved self-efficacy, self-mgmt Mean HbA1c: Transition to support groups: Mental health practitioners Group-led focus Peer health educators

26 Culturally Tailoring the Patient Empowerment Classes



27 Goddu, Raffel, Peek. JGIM. 2012;27:2:S99. The Role of Narrative
28 The narrative elements of the class built strong social support among participants that facilitated program retention and behavioral change Instead of me shunning and pushing away from [the education] it s an inspiration because you hear what others go through and we get a chance to share what we re going through I made so many friends here I mean we were all friends. We would tell about different experiences and how some of them had really stuck to what they were supposed to do and lost weight. And you know that gave me the incentive. I said, if they can do it, I can do it. I look forward to every three-month [follow-up meeting] because you be running back to your friends.
29 Patient Classes: Social Support I was getting tired of carrying that pressure but you know when I opened up, oh man, I felt like a brick was removed from off of my head because I was able to share what I was feeling. They listened She was so concerned about not one, not two. If it was 99 of us she was concerned, explaining and ready to answer any questions that any of us had.
30 Leveraging Technology to Enhance Patient Self-Care and Health Care Interactive text message reminders 4 week pilot at PCG (n=18) Improvements in: Diabetes self-efficacy Self-foot examinations Medication adherence

31 Daily messages Health Belief -Perceived susceptibility -Perceived severity -Perceived barriers -Perceived benefits SMS-DMCare - Text messages - Phone calls Reminders Diabetes Self- Management Frequent contact Feedback Self-Efficacy -Mastery experience -Social persuasion -Physiological Factors Social Support -Perceived support -Enacted support -Social integration
32 Texting: Social Support The texting program provided participants with someone who cared for and monitored them. But somebody is involved in being concerned about what s going on with you besides the visits with the doctor or maybe the nurse checking up on you. This is some kind of constant something. Some participants went further to describe the text messaging as a friend, sponsor, or social group. So the texting became a friend to me. And it was telling me, It s time to take your medicine, Did you take your medicine today, Did you check your feet. So therefore I had someone reminding me.
")

33 Leveraging Technology to Enhance Patient Self-Care and Health Care Interactive text message reminders 4 week pilot at PCG (n=18) Improvements in: Diabetes self-efficacy Self-foot examinations Medication adherence UCHP intervention Nurse care manager and healthcare team interface
34 Community Partnerships The Chronic Care Model Quality Improvement Community Health Systems Patient Practice Team Patient Activation Provider Training

35



36 Community Outreach and Education Regular Source of Care Urban Health Initiative Over 4,000 pts connected to primary care providers Public Education Television, Radio, Print Community health venues Center for Community Health & Vitality


37 Community Partnerships The Chronic Care Model Quality Improvement Community Health Systems Patient Practice Team Patient Activation Provider Training


38 Community Partnerships KLEO Community Family Life Center Chicago Food Depository Save-A-Lot Grocery Store Walgreens Chicago Park District Farmer s Markets



39 Patient Activation and Community Partnerships Patient empowerment classes Education Screening Resources Resources Reinforcement Sustainability Pantry partnership Free food Health information Cooking demonstrations Exercise lessons
![Integrating Patient Education and Community Partnerships The [food pantry] helps, because it is healthy.](/docs-images/86/93622274/images/40-1.jpg "I might be running short, and then they kind of fill in, so it all fits in together, it works perfectly KLEO is there")

40 Integrating Patient Education and Community Partnerships The [food pantry] helps, because it is healthy. I might be running short, and then they kind of fill in, so it all fits in together, it works perfectly KLEO is there as a community thing and I wouldn t have known anything about it if it wasn t for the class. It s a wonderful thing to know you re on the right track, that what you re doing is working. I m doing what I m supposed to do, and I m going to continue.

41 The KLEO partnership

42 The KLEO partnership
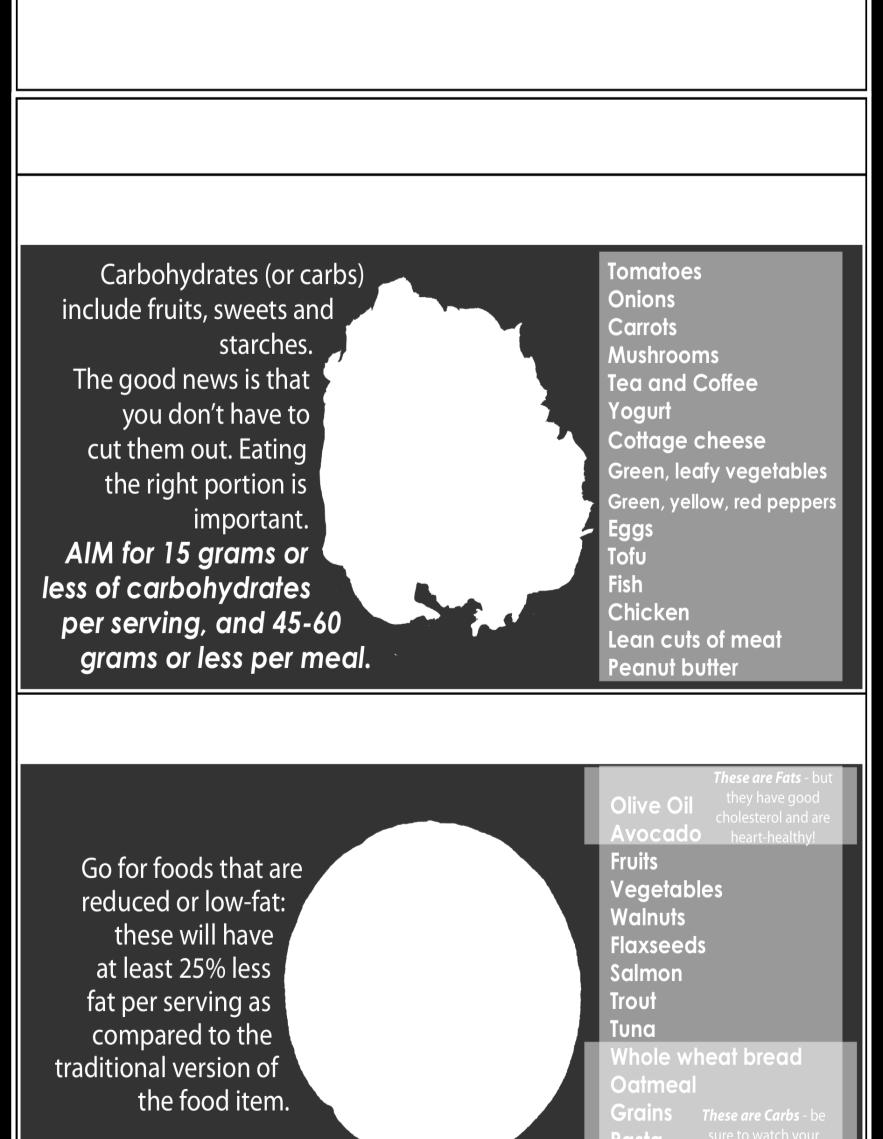
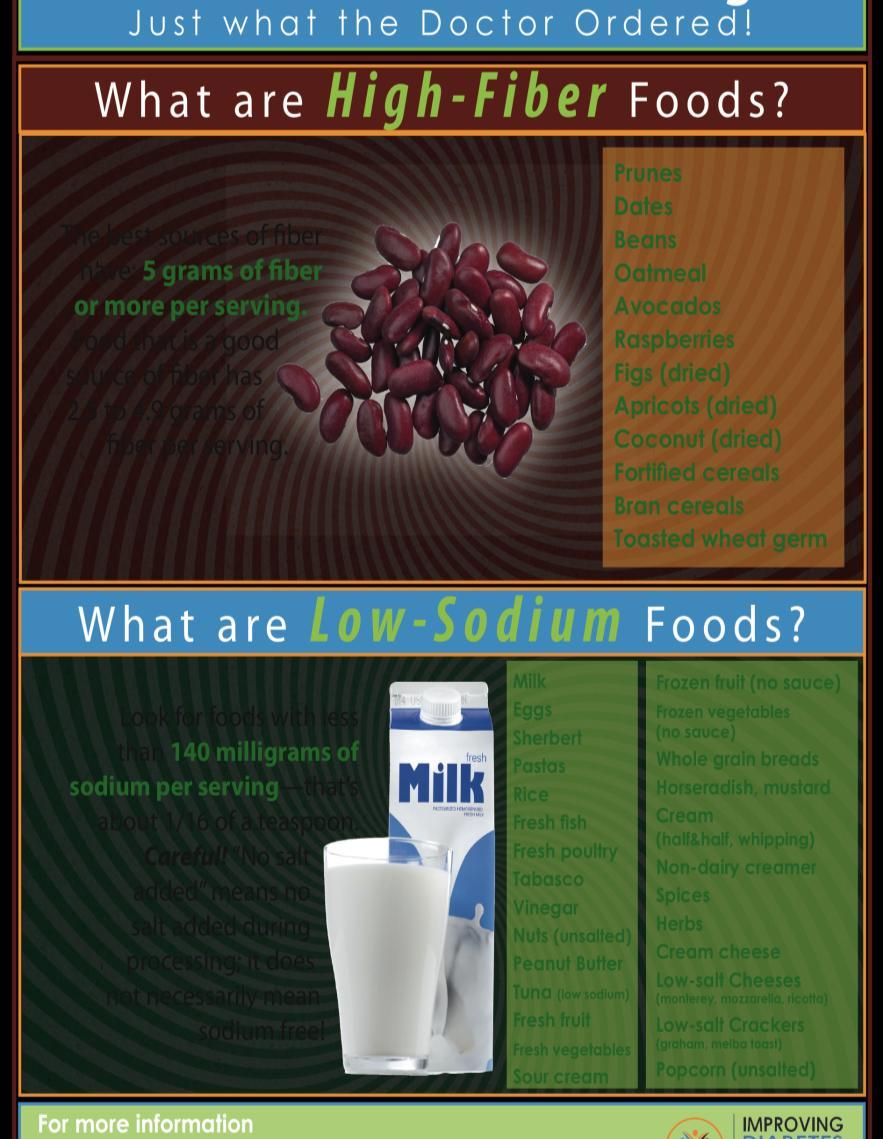
43 Prescriptions for Food and Exercise Guidelines for Chicago Park District (703) Walgreens Low Carb Low Fat Low Fiber Low Sodium Farmer s Market Get $5 off your healthy food purchase. See back for more informa tion. Food Depository

44

45

46

47 Save-A-Lot Grocery Store partnership

48
49 Health Policy Relevance: Quality of Care and Health Care Reform Medicare payments Quality, performance improvement and care coordination CMS Innovation Center Pilot and evaluate different payment structures Quality, patient-centered care and cost containment National QI strategy Improve health care delivery, health outcomes, population health Collection of race/ethnicity data Enhanced Preventive Care No cost-sharing for preventive services Medicaid coverage for tobacco cessation Employee rewards for joining wellness programs
50 Our Project Team Marshall Chin Monica Peek Tonya Roberson Anna Goddu Deb Maltby Kristine Bordenave Michael Quinn Doriane Miller Lisa Vinci Andrew Davis Elbert Huang Jonathan Birnberg Jonathan Dick Shantanu Nundy Seo Young Park Neha Setha Emily Lu Robert Sanchez Deborah Burnet Karen Kim Dawnavan Davis Sheila Harmon Quin Golden Eric Whitaker Shelley Scott Mickey Eder Peggy Hasenauer Louis Philipson Marla Soloman Hui Tang Robert Nocon Katie Raffel Ndang Azang-Njaah Gwen Burrows Braunda Anderson Melishia Bansa
51 Thank you! Merck Company Foundation NIDDK R18 DK NIDDK P30 DK NIDDK K23 DK NIDDK K24 DK University of Chicago CTSA Pilot and Collaborative Translational and Clinical Studies Award
The Roadmap to Reduce Disparities
 The Roadmap to Reduce Disparities Marshall H. Chin, MD, MPH Richard Parrillo Family Professor Director, RWJF Finding Answers University of Chicago Disclosures / Funding AHRQ T32 HS00084, K12 HS023007,
The Roadmap to Reduce Disparities Marshall H. Chin, MD, MPH Richard Parrillo Family Professor Director, RWJF Finding Answers University of Chicago Disclosures / Funding AHRQ T32 HS00084, K12 HS023007,
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships
 States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes. James X. Zhang, PhD, MS The University of Chicago
 Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes James X. Zhang, PhD, MS The University of Chicago April 23, 2013 Outline Background Medicare Dual eligibles Diabetes mellitus Quality
Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes James X. Zhang, PhD, MS The University of Chicago April 23, 2013 Outline Background Medicare Dual eligibles Diabetes mellitus Quality
PHCPI framework: Presentation Crosswalk to Service Delivery Elements
 PHCPI framework: Presentation Crosswalk to Service Delivery Elements C. Service Delivery America s Federally Qualified Health Centers (FQHC) Program David Stevens, MD, FAAFP George Washington University
PHCPI framework: Presentation Crosswalk to Service Delivery Elements C. Service Delivery America s Federally Qualified Health Centers (FQHC) Program David Stevens, MD, FAAFP George Washington University
Employee Benefits Planning Assn. Meredith Mathews, MD MPH
 Employee Benefits Planning Assn. Meredith Mathews, MD MPH 1 Meredith Mathews, MD, MPH Chief Medical Officer 18 years in practice of nephrology; CMO & SVP for Health Services, Premera Blue Cross; CMO &
Employee Benefits Planning Assn. Meredith Mathews, MD MPH 1 Meredith Mathews, MD, MPH Chief Medical Officer 18 years in practice of nephrology; CMO & SVP for Health Services, Premera Blue Cross; CMO &
Using the Patient Activation Measure (PAM) to Promote Patient Engagement
 to Promote Patient Engagement") Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
ehealth to Disseminate Lay Health Coaching
 ehealth to Disseminate Lay Health Coaching Patrick Yao Tang, MPH Program Manager, Peers for Progress yptang@email.unc.edu www.peersforprogress.org Society of Behavioral Medicine Annual Meeting April 1,
ehealth to Disseminate Lay Health Coaching Patrick Yao Tang, MPH Program Manager, Peers for Progress yptang@email.unc.edu www.peersforprogress.org Society of Behavioral Medicine Annual Meeting April 1,
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
11 th Scope of Work (SOW)
") Aug 19-20, 2015 11 th Scope of Work (SOW) 11 th SOW Desired outcomes: improve clinical outcomes of HbA1c, Lipids, Blood Pressure and Weight control decrease lower extremity amputations due to DM improve
Aug 19-20, 2015 11 th Scope of Work (SOW) 11 th SOW Desired outcomes: improve clinical outcomes of HbA1c, Lipids, Blood Pressure and Weight control decrease lower extremity amputations due to DM improve
Consumer Survey Results
 Consumer Survey Results Greater Area Health Council Survey Round Two Under the direction of The Aligning Forces for Quality (AF4Q) Evaluation Team Dennis Scanlon, Ph.D. May 2013 The survey and data analysis
Consumer Survey Results Greater Area Health Council Survey Round Two Under the direction of The Aligning Forces for Quality (AF4Q) Evaluation Team Dennis Scanlon, Ph.D. May 2013 The survey and data analysis
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc.
 Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
2019 Quality Improvement Program Description Overview
 2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
Health Care Sector Introduction. Thank you for taking the time to complete this Health Care Sector survey.
 Introduction Thank you for taking the time to complete this Health Care Sector survey. The purpose of this survey is to provide a snapshot of the policy, systems, and environmental (PSE) conditions that
Introduction Thank you for taking the time to complete this Health Care Sector survey. The purpose of this survey is to provide a snapshot of the policy, systems, and environmental (PSE) conditions that
Population Health: Physician Perspective. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015
 Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost
 Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Racial and Ethnic Health Disparities in Health and Health Care St. Louis Regional Data
 Racial and Ethnic Health Disparities in Health and Health Care St. Louis Regional Data By Debbie Chase, MPA Consultant, Center for Health Policy University of Missouri -- Columbia 1 Quantitative Data Overview
Racial and Ethnic Health Disparities in Health and Health Care St. Louis Regional Data By Debbie Chase, MPA Consultant, Center for Health Policy University of Missouri -- Columbia 1 Quantitative Data Overview
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
A M.A.P. for improving blood pressure: Application within the QIN-QIO community
 A M.A.P. for improving blood pressure: Application within the QIN-QIO community Donna Daniel, PhD Director, Improving Health Outcomes Strategies American Medical Association Michael Rakotz, MD Director,
A M.A.P. for improving blood pressure: Application within the QIN-QIO community Donna Daniel, PhD Director, Improving Health Outcomes Strategies American Medical Association Michael Rakotz, MD Director,
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Distinctive features of HPH in Taiwan: what made this network successful?
 Distinctive features of HPH in Taiwan: what made this network successful? Dr. Ying-Wei Wang, Director General, Health Promotion Administration, Taiwan HPH Taiwan Network Representative 1 Where is Taiwan?
Distinctive features of HPH in Taiwan: what made this network successful? Dr. Ying-Wei Wang, Director General, Health Promotion Administration, Taiwan HPH Taiwan Network Representative 1 Where is Taiwan?
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Objectives. Physician Leadership Engagement to Produce System Change
 Physician Leadership Engagement to Produce System Change David Swieskowski, MD, MBA Senior VP & Chief Accountable Care Officer Mercy Medical Center Des Moines, Iowa Objectives Discuss adoption of change
Physician Leadership Engagement to Produce System Change David Swieskowski, MD, MBA Senior VP & Chief Accountable Care Officer Mercy Medical Center Des Moines, Iowa Objectives Discuss adoption of change
A. DIABETES AND HEART/STROKE Data Detail
 A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
All 28 items with minimal wording changes to reflect prenatal tobacco screening and treatment instead of chronic illness
 Assessing Chronic Illness Care Source: Bonomi AE, Wagner EH, Glasgow RE, VonKorff M. Assessment of Chronic Illness Care (ACIC): A practical tool to measure quality improvement. Health Services Research
Assessing Chronic Illness Care Source: Bonomi AE, Wagner EH, Glasgow RE, VonKorff M. Assessment of Chronic Illness Care (ACIC): A practical tool to measure quality improvement. Health Services Research
Quality Management Report 2018 Q1
 Quality Management Report 2018 Q1 Care Wisconsin Participates in Many Quality Initiatives Across the State and Federal Levels These activities include: Centers for Medicare & Medicaid Services (CMS) Department
Quality Management Report 2018 Q1 Care Wisconsin Participates in Many Quality Initiatives Across the State and Federal Levels These activities include: Centers for Medicare & Medicaid Services (CMS) Department
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP)
 & Chronic Care Improvement Program (CCIP)") Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Healthy Hearts Northwest : A 2 x 2 Randomized Factorial Trial to Build Quality Improvement Capacity in Primary Care
 Healthy Hearts Northwest : A 2 x 2 Randomized Factorial Trial to Build Quality Improvement Capacity in Primary Care April 7, 2017 Michael Parchman, MD, MPH This project is supported by grant number R18HS023908
Healthy Hearts Northwest : A 2 x 2 Randomized Factorial Trial to Build Quality Improvement Capacity in Primary Care April 7, 2017 Michael Parchman, MD, MPH This project is supported by grant number R18HS023908
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Diabetes. Evidence Based/ Team Based Care in a Community Health Center ---
 Diabetes Evidence Based/ Team Based Care in a Community Health Center --- Sharon Mulvehill MD North Texas Area Community Health Center August 23, 2014 The Challenges Busy schedules, little time for system
Diabetes Evidence Based/ Team Based Care in a Community Health Center --- Sharon Mulvehill MD North Texas Area Community Health Center August 23, 2014 The Challenges Busy schedules, little time for system
2017 National Standards for Diabetes Self-Management Education and Support INTERPRETIVE GUIDANCE
 2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
Leveraging the Community Health Needs Assessment Process to Improve Population Health: Lessons Learned from Kaiser Permanente
 Leveraging the Community Health Needs Assessment Process to Improve Population Health: Lessons Learned from Kaiser Permanente Association for Community Health Improvement (ACHI) 2015 Conference What We
Leveraging the Community Health Needs Assessment Process to Improve Population Health: Lessons Learned from Kaiser Permanente Association for Community Health Improvement (ACHI) 2015 Conference What We
WEST VIRGINIA S MEDICAID CHANGES UNLIKELY TO REDUCE STATE COSTS OR IMPROVE BENEFICIARIES HEALTH By Judith Solomon
 820 First Street NE, Suite 510 Washington, DC 20002 Tel: 202-408-1080 Fax: 202-408-1056 center@cbpp.org www.cbpp.org May 31, 2006 WEST VIRGINIA S MEDICAID CHANGES UNLIKELY TO REDUCE STATE COSTS OR IMPROVE
820 First Street NE, Suite 510 Washington, DC 20002 Tel: 202-408-1080 Fax: 202-408-1056 center@cbpp.org www.cbpp.org May 31, 2006 WEST VIRGINIA S MEDICAID CHANGES UNLIKELY TO REDUCE STATE COSTS OR IMPROVE
Pursuing the Triple Aim: CareOregon
 Pursuing the Triple Aim: CareOregon The Triple Aim: An Introduction The Institute for Healthcare Improvement (IHI) launched the Triple Aim initiative in September 2007 to develop new models of care that
Pursuing the Triple Aim: CareOregon The Triple Aim: An Introduction The Institute for Healthcare Improvement (IHI) launched the Triple Aim initiative in September 2007 to develop new models of care that
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Patient Protection and Affordable Care Act Selected Prevention Provisions 11/19
 Patient Protection and Affordable Care Act Selected Prevention Provisions 11/19 Coverage of Preventive Health Services (Sec. 2708) Stipulates that a group health plan and a health insurance issuer offering
Patient Protection and Affordable Care Act Selected Prevention Provisions 11/19 Coverage of Preventive Health Services (Sec. 2708) Stipulates that a group health plan and a health insurance issuer offering
Alaska FQHC Quality Improvement Facilitator Coaching Project
 1 Alaska FQHC Quality Improvement Facilitator Coaching Project Tari O Connor, MSW Chief, Section of Chronic Disease Prevention and Health Promotion Alaska Division of Public Health 2 The QI Facilitator
1 Alaska FQHC Quality Improvement Facilitator Coaching Project Tari O Connor, MSW Chief, Section of Chronic Disease Prevention and Health Promotion Alaska Division of Public Health 2 The QI Facilitator
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS) 1,2,3
 1,2,3") Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Walking the Walk: The ACT Study Plans for Intervention Sustainability
 CENTER TO ELIMINATE CARDIOVASCULAR HEALTH Volume 2, Issue 1 Spring 2012 The Center s Beat Walking the Walk: The ACT Study Plans for Intervention Sustainability The Center s Project 2 is excited to have
CENTER TO ELIMINATE CARDIOVASCULAR HEALTH Volume 2, Issue 1 Spring 2012 The Center s Beat Walking the Walk: The ACT Study Plans for Intervention Sustainability The Center s Project 2 is excited to have
Southeast Michigan Beacon Community
 Southeast Michigan Beacon Community Background and Information on Text HEALTH November 8, 2011 1 Beacon Communities Funded by U.S. Department of Health and Human Services Administered by the Office of
Southeast Michigan Beacon Community Background and Information on Text HEALTH November 8, 2011 1 Beacon Communities Funded by U.S. Department of Health and Human Services Administered by the Office of
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Team Care Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc.
 2008 Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc. November 12-14, 2008, Scottsdale, AZ Great Falls Clinic, LLP Great Falls, Montana Team Care
2008 Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc. November 12-14, 2008, Scottsdale, AZ Great Falls Clinic, LLP Great Falls, Montana Team Care
Quality Management Report 2017 Q4
 Quality Management Report 2017 Q4 Care Wisconsin Participates in Many Quality Initiatives Across the State and Federal Levels. These activities include: CMS DHS DHS & CMS HEDIS Member Satisfaction (CAHPS
Quality Management Report 2017 Q4 Care Wisconsin Participates in Many Quality Initiatives Across the State and Federal Levels. These activities include: CMS DHS DHS & CMS HEDIS Member Satisfaction (CAHPS
CONNECTED SM. Blue Care Connection SIMPLY AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT
 SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Medicare Quality Improvement Initiatives
 Medicare Quality Improvement Initiatives Participation Opportunities in Minnesota February 2016 Achieve national quality goals in Minnesota. Join Stratis Health in working to achieve the Centers for Medicare
Medicare Quality Improvement Initiatives Participation Opportunities in Minnesota February 2016 Achieve national quality goals in Minnesota. Join Stratis Health in working to achieve the Centers for Medicare
Use of Health Information Technology to Reduce Health Risk
 Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
RN Behavioral Health Care Manager in Behavioral Health Settings
 RN Behavioral Health Care Manager in Behavioral Health Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Behavioral Health Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Shana Scott, JD, MPH, Health Systems Team Lead Tuesday, October 3, 2017
 Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Aetna Better Health of Illinois
 Aetna Better Health of Illinois Navigating Relationships in an Evolving Healthcare Environment: Community Health Centers and Managed Care Organizations Forum October 1, 2013 Sanjoy Musunuri Agenda Aetna
Aetna Better Health of Illinois Navigating Relationships in an Evolving Healthcare Environment: Community Health Centers and Managed Care Organizations Forum October 1, 2013 Sanjoy Musunuri Agenda Aetna
Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs. September 20, 2017
 Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs September 20, 2017 Introductions & Agenda Introduce Panelists Overview
Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs September 20, 2017 Introductions & Agenda Introduce Panelists Overview
Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012
 Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012 Presenters David Sayen, CMS Regional Administrator Betsy L. Thompson,
Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012 Presenters David Sayen, CMS Regional Administrator Betsy L. Thompson,
San Francisco is not exempt from the hypertension crisis, nor from the health disparities reflected in the African-American community.
 September 2017 San Francisco Health Network Heart Health Patient Communications and Community Events Project Brief and Request for Proposals I. Background Heart disease is the leading cause of death in
September 2017 San Francisco Health Network Heart Health Patient Communications and Community Events Project Brief and Request for Proposals I. Background Heart disease is the leading cause of death in
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers
 Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers Community Preventive Services Task Force Finding and Rationale Statement Ratified March 2015 Table of Contents
Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers Community Preventive Services Task Force Finding and Rationale Statement Ratified March 2015 Table of Contents
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Assessment of Chronic Illness Care Version 3
 Assessment of Chronic Illness Care Version 3 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the ICIC/IHI team. We would
Assessment of Chronic Illness Care Version 3 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the ICIC/IHI team. We would
An Integrative Health Home Pilot
 An Integrative Health Home Pilot Kellye Hudson, DNP, PMHNP-BC Director of Nursing Helen Ross McNabb Center December 2016 TN Healthcare Innovation Initiative Primary Care Transformation Launched in 2013
An Integrative Health Home Pilot Kellye Hudson, DNP, PMHNP-BC Director of Nursing Helen Ross McNabb Center December 2016 TN Healthcare Innovation Initiative Primary Care Transformation Launched in 2013
Webinar Instructions. Thank you for joining today, please wait while others sign in.
 Webinar Instructions Thank you for joining today, please wait while others sign in. Phone Dial-in: 1-866-740-1260 Access Code: 4796665# Due to the large number of participants, all lines will be muted
Webinar Instructions Thank you for joining today, please wait while others sign in. Phone Dial-in: 1-866-740-1260 Access Code: 4796665# Due to the large number of participants, all lines will be muted
Money and Members: Pay for Performance in a Medicaid Program
 Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
PATH Program. Getting Started Guide
 PATH Program Getting Started Guide We have a BIG opportunity. Together, we can empower and encourage people to take an active role in their health. Preventive health care services help people find and
PATH Program Getting Started Guide We have a BIG opportunity. Together, we can empower and encourage people to take an active role in their health. Preventive health care services help people find and
Using Quality Improvement to Reduce Racial and Ethnic Disparities in Medicaid Managed Care: Lessons from Oregon
 Using Quality Improvement to Reduce Racial and Ethnic Disparities in Medicaid Managed Care: Lessons from Oregon Matthew Carlson, Ph.D. Assistant Professor of Sociology Portland State University Charles
Using Quality Improvement to Reduce Racial and Ethnic Disparities in Medicaid Managed Care: Lessons from Oregon Matthew Carlson, Ph.D. Assistant Professor of Sociology Portland State University Charles
East Gippsland Primary Care Partnership. Assessment of Chronic Illness Care (ACIC) Resource Kit 2014
 Resource Kit 2014") East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs. September 20, 2017
 Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs September 20, 2017 Introductions & Agenda Introduce Panelists Overview
Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs September 20, 2017 Introductions & Agenda Introduce Panelists Overview
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
6 18 Evaluation and Impact Measurement
 6 18 Evaluation and Impact Measurement August 12, 2016 Center for Health Care Strategies Centers for Disease Control and Prevention Centers for Medicare and Medicaid Services Support provided by the Robert
6 18 Evaluation and Impact Measurement August 12, 2016 Center for Health Care Strategies Centers for Disease Control and Prevention Centers for Medicare and Medicaid Services Support provided by the Robert
Health Coaching: Filling a Gap In Primary Care
 Health Coaching: Filling a Gap In Primary Care Katie Ingle, DNP, FNP Cannon Falls, MN Introduction Katie Ingle, DNP-FNP Family nurse practitioner, working in family practice 2005 MSN graduate of AASU 2013
Health Coaching: Filling a Gap In Primary Care Katie Ingle, DNP, FNP Cannon Falls, MN Introduction Katie Ingle, DNP-FNP Family nurse practitioner, working in family practice 2005 MSN graduate of AASU 2013
HPV Vaccination Quality Improvement: Physician Perspective
 HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
Assessment of Chronic Illness Care Version 3.5
 Assessment of Chronic Illness Care Version 3.5 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the Learning Collaborative
Assessment of Chronic Illness Care Version 3.5 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the Learning Collaborative
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
California Pay for Performance: A Case Study with First Year Results. Tom Williams Integrated Healthcare Association (IHA) March 17, 2005
 March 17, 2005") California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016
 ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
Strategy for Quality Improvement in Health Care
 Strategy for Quality Improvement in Health Care Neal D. Kohatsu, MD, MPH, DHCS Medical Director Desiree Backman, DrPH, RD, UC Davis Institute for Population Heath Improvement & DHCS Chief Prevention Officer
Strategy for Quality Improvement in Health Care Neal D. Kohatsu, MD, MPH, DHCS Medical Director Desiree Backman, DrPH, RD, UC Davis Institute for Population Heath Improvement & DHCS Chief Prevention Officer
UPMC Health Plan. Value Based Insurance Design (VBID) Spark Your Health
 Spark Your Health") UPMC Health Plan Value Based Insurance Design (VBID) Spark Your Health Value Based Insurance Design (VBID) Spark Your Health Medicare Advantage Summit April 6, 2017 Helene Weinraub 1 The statements contained
UPMC Health Plan Value Based Insurance Design (VBID) Spark Your Health Value Based Insurance Design (VBID) Spark Your Health Medicare Advantage Summit April 6, 2017 Helene Weinraub 1 The statements contained
Keenan Pharmacy Care Management (KPCM)
") Keenan Pharmacy Care Management (KPCM) This program is an exclusive to KPS clients as an additional layer of pharmacy benefit management by engaging physicians and members directly to ensure that the best
Keenan Pharmacy Care Management (KPCM) This program is an exclusive to KPS clients as an additional layer of pharmacy benefit management by engaging physicians and members directly to ensure that the best
University of Cincinnati Patient Centered Medical Home Leadership Decisions
 University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Evaluation of State Public Health Actions: Overview and Progress to Date Rachel Davis, MPH
 Evaluation of State Public Health Actions: Overview and Progress to Date Rachel Davis, MPH Division for Heart Disease and Stroke Prevention Evaluation and Program Effectiveness Team Presentation Overview
Evaluation of State Public Health Actions: Overview and Progress to Date Rachel Davis, MPH Division for Heart Disease and Stroke Prevention Evaluation and Program Effectiveness Team Presentation Overview
Chairman Junge called the meeting to order. Present: Chairman Emilie N. Junge and Director Sidney A. Thomas, MSW (2) Director Ada Mary Gugenheim
 Director Ada Mary Gugenheim") Minutes of the meeting of the Managed Care Committee of the Board of Directors of the Cook County Health and Hospitals System held Monday, February 26, 2018 at the hour of 10:30 A.M. at 1900 W. Polk Street,
Minutes of the meeting of the Managed Care Committee of the Board of Directors of the Cook County Health and Hospitals System held Monday, February 26, 2018 at the hour of 10:30 A.M. at 1900 W. Polk Street,
INTEGRATING SELF-MANAGEMENT FOR CHRONIC ILLNESSES AND PREVENTIVE BEHAVIORS INTO HEALTH CARE
 INTEGRATING SELF-MANAGEMENT FOR CHRONIC ILLNESSES AND PREVENTIVE BEHAVIORS INTO HEALTH CARE Russell E. Glasgow, Ph.D. Kaiser Permanente Colorado Denver, Colorado Overview of Presentation! The Health Care
INTEGRATING SELF-MANAGEMENT FOR CHRONIC ILLNESSES AND PREVENTIVE BEHAVIORS INTO HEALTH CARE Russell E. Glasgow, Ph.D. Kaiser Permanente Colorado Denver, Colorado Overview of Presentation! The Health Care
Transforming Care for Vulnerable Populations:
 Transforming Care for Vulnerable Populations: Lessons from the Safety Net Medical Home Initiative Kathryn E. Phillips, MPH July 2015 Safety Net Medical Home Initiative Goals for this Session Describe the
Transforming Care for Vulnerable Populations: Lessons from the Safety Net Medical Home Initiative Kathryn E. Phillips, MPH July 2015 Safety Net Medical Home Initiative Goals for this Session Describe the
Better Health and Lower Costs for Patients With Complex Needs
 Better Health and Lower Costs for Patients With Complex Needs An IHI Triple Aim Collaborative Informational Call May 12, 2015 Faculty on Informational Call Today Cory Sevin IHI Director Catherine Craig
Better Health and Lower Costs for Patients With Complex Needs An IHI Triple Aim Collaborative Informational Call May 12, 2015 Faculty on Informational Call Today Cory Sevin IHI Director Catherine Craig
The John J. Conger Lecture Child Health Services in a Post Affordable Care Act World: What Do We Need to Know?
 The John J. Conger Lecture Child Health Services in a Post Affordable Care Act World: What Do We Need to Know? Dr. Lisa Simpson President and CEO March 8, 2013 Lisa Simpson I have documented that I have
The John J. Conger Lecture Child Health Services in a Post Affordable Care Act World: What Do We Need to Know? Dr. Lisa Simpson President and CEO March 8, 2013 Lisa Simpson I have documented that I have
EHR Innovations for Improving Hypertension Challenge Winners and Phase 2
 EHR Innovations for Improving Hypertension Challenge Winners and Phase 2 January 23, 2015 Agenda Million Hearts Blood Pressure Protocols Hilary Wall, MPH Green Spring Internal Medicine Holly Dahlman, MD,
EHR Innovations for Improving Hypertension Challenge Winners and Phase 2 January 23, 2015 Agenda Million Hearts Blood Pressure Protocols Hilary Wall, MPH Green Spring Internal Medicine Holly Dahlman, MD,
The SOMC Employee Wellness Program
 The SOMC Employee Wellness Program A Focus on Results Not Participation Pike County Health Coalition Julie Thornsberry, RN, BSN Manager Employee Health & Wellness What are today s objectives? Identify
The SOMC Employee Wellness Program A Focus on Results Not Participation Pike County Health Coalition Julie Thornsberry, RN, BSN Manager Employee Health & Wellness What are today s objectives? Identify
Challenges and Solutions in Adopting Electronic Patient Registries in Privately Owned Primary Care Practices Serving Minority Patients
 Challenges and Solutions in Adopting Electronic Patient Registries in Privately Owned Primary Care Practices Serving Minority Patients Thomas J. Van Hoof, MD, EdD Associate Professor University of Connecticut
Challenges and Solutions in Adopting Electronic Patient Registries in Privately Owned Primary Care Practices Serving Minority Patients Thomas J. Van Hoof, MD, EdD Associate Professor University of Connecticut