Stanford Coordinated Care
|
|
|
- Kathleen Lewis
- 5 years ago
- Views:
Transcription

1 The project described is supported by Grant Number 1C1CMS from the Department of Health and Human Services, Centers for Medicare & Medicaid Services. The contents of this presentation are solely the responsibility of the authors and do not necessarily represent the official views of the U.S. Department of Health and Human Services or any of its agencies. IOCP
2 Stanford Coordinated Care Support the Patients, Manage their Care Ann Lindsay MD, Co-Director August 10, 2015
3 Determinants of Health and Their Contribution to Premature Death 15% 30% 5% 10% Social Environmental Medical Behavioral Genetic 40% Schroeder, NEJM 357; 12
4 Hot Spotting in Employed Populations Boeing & Atlantic City Resorts (A. Milstein, Kothari, Fernandopulle) AICU in 2 self-funded industries Capitation fee plus FFS for specialized MD-led teams within 3 MD groups and free-standing (Atlantic City) 18%- 20% net reduction in per capita spending vs. propensity matched controls Humboldt (A. Glaseroff) Partnered with PERS and PBGH (Anthem as ASO); Disseminated rural county model within a distinguished IPA inserting RN care managers into 25 private practices 16% net savings estimated in first year
5 Better, Faster and Leaner: Boeing A-ICU Results After 1 Year Change in Combined Total Per Capita Health Care Spending, Functional Health Status, Patient Experience, and Absenteeism % change from baseline in unit price-standardized total annual per capita spending by patients and Boeing, compared to a propensitymatched control group, net of supplemental fees to medical groups % change in SF12 physical functioning score for IOCP patients compared to baseline % change in SF12 mental functioning score for IOCP patients compared to baseline % change in patient-rated care received as soon as needed compared to baseline** % change in average of patient-reported work days missed in last 6 months compared to baseline % Difference 20% * +14.8% +16.1% +17.6% 56.5% * p = 0.11 after first 12 months for 276 chronically ill enrollees vs. 276 matched controls. ** From the Ambulatory Care Experience Survey patients responding always or almost always to the question: When you needed care for illness or injury, how often did the IOCP provide care as soon as you needed it?
6 PBGH Intensive Outpatient Care Program in Brief 15,000: number of patients enrolled May 1, 2012 to June : participating delivery systems / 500 practices 72% patient engagement rate (range = 33% to 99%) 5: states represented (CA, AZ, ID, NV and WA) Organizational variation - Independent Practice Associations, medical foundations, integrated and non-integrated systems Payment variation - Pioneer and MSSP ACOs, Medicare Advantage and fee-for-service IOCP
7 Effective Targeting of Care Management Population Volume Healthy Area of Greatest Opportunity Clemons Hong MD, MPH Chronic Illnesses Medically Complex High Utilizers
8
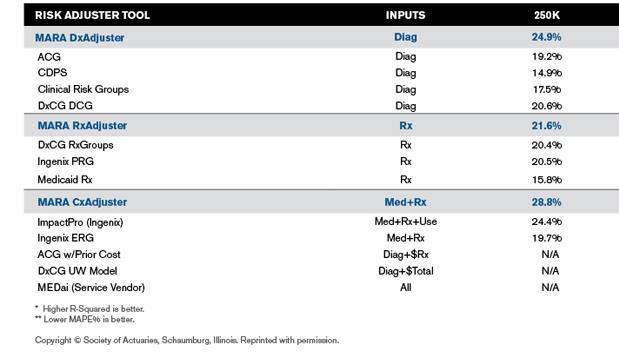
9 Predictive Modeling
10 Prospective Risk: from Claims Data High Concurrent/Low Predictive: Regression to the mean High Concurrent/ High Predictive: Main target - can demonstrate ROI $ Low Concurrent/Low Predictive: Care too expensive Low Concurrent/High Predictive: Avoiding avoidable care Predictive Risk

11 Predictive Risk: from Clinical Data
12 Predictive Risk: from Patient Surveys Hospital Admission Risk Multiplier Screen (HARMS-8): To identify further risks, ask the following questions: 1. In general, how would you rate your current health? Excellent Very Good Good Fair Poor For all, Why do you rate it that way? 2. How many prescription medications are you currently taking every day? None (SKIP to question 3) or more 2_a) During the past WEEK, how often did you forget to take or decide not to take one or more of these medications? Never Sometimes Usually Always 2_b) How sure are you that you understand the purpose of each medication you are taking? Very Sure Somewhat Sure Not very sure Unless Never/ Very Sure: What is most difficult for you in taking your medications? From CareOregon
13 HARMS-8 3. Think about your usual daily activities, such as bathing, toileting, dressing, grooming, feeding, housework, family or leisure activities. Which of the following best describes your situation in the last MONTH: I have no problems with performing my usual activities. I have some problems with performing my usual activities without assistance. I am unable to perform my usual activities without assistance. Unless no problems: Do you think you need help managing at home? If so, what kind? 4. In the last MONTH, how often did you have trouble with remembering or thinking clearly? Never Sometimes Usually Always Unless Never, What do you do when that happens?
14 HARMS-8 7. During the past 6 months, how many times did you go to the emergency room? None (SKIP to question 8) 1 or more times 7_a) Do you think it is likely you will need to go to the emergency room again in the next 6 months? Not likely Somewhat likely Very likely Unless Not likely, What do you think would help to keep you from needing to go to the emergency room? 8. During the past 6 months, how many times did you stay in the hospital overnight as a patient? None (END) 1 or more times 8_a) Do you think it is likely you will need to be hospitalized again in the next 6 months? Not likely Somewhat likely Very likely Unless Not Likely: What do you think causes your condition to get so bad you need to be in the hospital?
15 HARMS-8 5. If you needed immediate help for a health problem, how many friends or relatives do you feel close to such that you could call on them for help? None or more 5_a) Who are they? 5_b) How often do you communicate with them? If None or unclear, Is there someone who might be willing to help if they were asked? 6. Think about your current medical conditions. How confident are you that you can manage these medical conditions day-to-day? Very confident Somewhat confident Not very confident I don t have any health problems Unless Very confident: What is most challenging for you about your health? 15
16 Stanford Coordinated Care Ambulatory complex patients Employees and dependents of self-insured plan Capitated services with shared savings agreement Established 4/2012 Dr Arnie Milstein, Clinical Effectiveness Research Center Now 450 patients and growing


17 Primary Care Plus Services: No co-pays for SCC services 24/7 access to Primary Care Physician Coordination with specialists so everyone is on the same page Care transition planning at hospitalization with home visit if needed Contact with SCC staff once a week on average No charge to health plan for inoffice lab Management of coagulation medication with home lab testing Dietician Clinical Nurse Specialist Licensed Clinical Social Worker Primary Care Physician Patient Pharmacist Care Coordinator Physical Therapist






18 Care Support Services: FREE to those with Stanford health plans Counseling services as needed Health coaching and goal setting Assistance with ongoing health conditions like asthma, weight loss, high blood pressure, high cholesterol and stress Care transition planning at hospitalization with home visit if needed Coordination with primary care physicians and specialists so everyone is on the same page Clinical Nurse Specialist Patient Counseling Services
19 Human-Centered Design
20 From Our Lips to Whose Ears at Stanford? From Chronic diseases Ambulatory ICU Group visits Care management My (MD) care coordinator coordinate your care To Ongoing conditions Coordinated Care Seminars Care support Your (patient) care coordinator care with you at the center

21 Care Model Why wouldn t a person with a chronic condition do everything in their power to live long and feel well?

22 Patient Variation what the patient faces Domains From CareOregon, Intermed, and Humboldt IPA
 and Insignia")
23 Activation Level - What the Patient Brings 10-15% of the population* 20-25% of the population* 35-40% of the population* 25-30% of the population* * Medicaid and Medicare populations skew lower in activation From Judith Hibbard (OHSU) and Insignia Health
24 Depression Depression significantly increases the overall burden of illness in patients with chronic medical conditions depression is associated with a % increase in health services use and cost. Simon, Gregory E. Treating Depression in Patients With Chronic Disease. Western Journal of Medicine 2001:175:

25 Depression is Often Not the Only Health Problem Our Patients Face Chronic Pain 40-60% Cancer 10-20% Geriatric Syndromes 20-40% Depression Heart Disease 20-40% Diabetes 10-20% Neurologic Disorders 10-20% 2010 University of Washington AIMS Center

26 The Often Hidden Driver: Adverse Childhood Events ACE Score = 1 point each for positive responses to 10 questions inquiring about exposure to: Physical abuse Emotional abuse Sexual abuse Physical neglect Emotional neglect Divorce/separation Domestic violence in the home Parent that used drugs or alcohol Parent that was incarcerated Parent that was mentally ill From:
27 How does ACE play out later in life? Increased smoking: The higher the ACE score, the greater the likelihood of current smoking COPD: A person with an ACE score of 4 is 2.6 x more likely to have COPD than a person with an ACE score of 0 Depression: A person with an ACE score of 4 was 4.6 x more likely to be suffering from depression than a person with an ACE score of 0 Suicide: There was a 12.2 x increase in attempted suicide between ACE 4 vs. 0; at higher ACE scores, the prevalence of attempted suicide increases fold! Between 66-80% of all attempted suicides could be attributed to ACE.


28 SCC Approach: The Activation Model From: What bothers you the most? To: Where do you want to be in a year? First step Next step Getting there
29 Predicted Patient Costs ($) Predicted Average Per-Capita Costs 2 Years Later by Change in PAM Level 9000 $8,138 $8, $6,401 $6,465 $7,074 $7,290 $7, Level 4 both time periods Move Level 3 to Level 4 Level 3 both time periods Move Level 4 to Level 3 Move Level 1 or 2 to Level 3 or 4 Move Level 3 or 4 to Level 1 or 2 Level 1 or 2 both time periods Predicted costs are based upon regression models with log transformed costs that control for age, sex, chronic conditions, natural logarithm of income and percent of care that was received in-network. Costs were retransformed from log dollars using the Duan smear factor.
30 Patients with lower activation associated with higher costs; delivery systems should know their patients' 'scores'. Hibbard JH1, Greene J, Overton V. Health Aff (Millwood) Feb;32(2): doi: /hlthaff

31 How was this achieved? Humboldt Priority Care PAM Results
 show lower admission and ED utilization from IOCP")
32 Preliminary Patient Activation Measures (PAM) Results through June 2014 *Additionally, preliminary independent group findings (Wave 1 sites) show lower admission and ED utilization from IOCP participants.
33 # of Members per Level Stanford PAM Results Comparative Values by PAM Levels Level 1 Level 2 Level 3 Level 4 Initial Repeat
34 IOCP Metrics VR % improvement in physical health functioning 4.2% improvement in mental health functioning PHQ (depression score) 31% improvement PAM 37% increase 45% same 11% decrease 30% increase in graduation among patients whose PAM score increased The research presented here was conducted by PBGH IOCP
35 SCC Value: Patient Experience 99 th percentile in Press Ganey Likelihood to Recommend 19 out of last 20 months Employees and dependents appreciate the service 95% of MyHealth Medical Advice Requests responded to within 24 hours
36 SCC Value: Clinical metrics >90 th percentile HEDIS in 9 out of 10 process measures 83% colon cancer screening rate Improved screening can contribute to increased costs initially
37 Run Chart to Track Quality Improvement 100% 95% Systolic Blood Pressure Control SBP 90% 85% 80% 75% 70% >=150 [140,150) <140 65% 60% Will be updated monthly and posted on the Vis Wall 37
38 Senior leadership support Dedicated physician champion Identify appropriate patients Foundation for Success Take-up is greater in risk environments Most effective when there is provider-hospital integration Most successful when integrated into entire population health strategy Strong analytic capacity for program monitoring Adapt to local environment after meeting requirements IOCP
39 Financial Elements of Sustainability Financial and performance incentives create provider demand for new models - and provider demand leads to sustainability Continue evolution toward global or bundled payment and Total Cost of Care New care coordination code helps, but doesn t offset all cost Medical neighborhood reimbursement needed Continued alignment of public and private payers Creates consistency of care regardless of payer Provides reliable revenue stream Better communication, greater efficiencies IOCP



40 From Cup Runneth Over Provider Medical Assistant/Care Coordinator Nurse Behavioral Health Clinical Pharmacist Physical Therapist
41 To Share the Care Provider Medical Assistant/Care Coordinator Nurse LCSW/Behavio ral Health Physical Therapist Clinical Pharmacist

42 General Rules for Team Care Panel management: accountability Staff work to limits of their credential
43 Key Elements of Team Building Defined goals Overall mission Measurable operational objectives Systems Clinical Administrative Improvement methodology at frontline Division of labor Definition of workflows Assignment of roles Training Communication
44 From MA to Care Coordinator Artisanal vs. assembly line Coach, advocate, MA, scribe, outreach worker, pop health manager combined in single person: relationships are key Empanelment Training: onboarding and ongoing Case presentations at team meetings Staying with the patient few handoffs Scribing the visit: learning as the patient learns CREATE NEW JOB CATEGORY AND PAYSCALE to reflect greater skills and responsibility

45 EPIC Charting 45

46 HEDIS: SCC results 46
47 HEDIS: Care Gaps Tool 47 Care Coordinator : COLEMAN, DELILA Diabetes (Screening) Cardio (Screenin g) Preventative (Screening/Immunization) Med. Mgmt. SCC Patient Name Next Pneum Cervica ACE/AR Colorec B/Diureti Appt. Nephro ococca Chlamy l Breast tal c/digoxi PCP Date HbA1c LDL pathy LDL Flu l dia Cancer Cancer Cancer n PAM # Overdue VOLLRAT 01/09/20 Overdu 04/17/2 02/28/2 03/07/2 H, K 15 N/A N/A N/A N/A e N/A N/A N/A Overdue 2 VOLLRAT 09/01/2 12/08/2 09/30/2 09/26/20 03/26/20 H, K N/A N/A N/A N/A 014 N/A N/A N/A VOLLRAT 01/05/20 09/01/2 01/07/20 H, K 15 N/A N/A N/A N/A 014 N/A N/A N/A N/A N/A N/A 15 0 GLASERO 03/11/20 09/01/2 08/20/2 05/24/20 FF, A 15 N/A N/A N/A N/A 014 N/A N/A N/A N/A 015 N/A 15 0 GLASERO Overdu Overdu FF, A N/A N/A N/A N/A e N/A N/A e N/A N/A N/A Overdue 3 VOLLRAT 01/20/20 09/01/2 06/11/20 H, K 15 N/A N/A N/A N/A 014 N/A N/A N/A N/A N/A N/A 15 0 GLASERO 01/15/20 Overdu Adhere 10/14/2 02/20/20 FF, A 15 N/A N/A N/A N/A e nt N/A N/A N/A 015 N/A 15 1 LINDSAY, Overdu 08/09/2 03/20/2 02/21/20 A N/A N/A N/A N/A e N/A N/A N/A Overdue 15 2 LINDSAY, 01/08/20 11/14/2 11/15/2 01/04/2 09/01/2 11/15/20 02/27/20 A N/A 014 N/A N/A N/A N/A N/A LINDSAY, Overdu 03/19/2 05/19/20 A N/A N/A N/A N/A e N/A N/A 016 N/A N/A N/A 15 1 GLASERO 09/01/2 05/26/20 FF, A N/A N/A N/A N/A 014 N/A N/A N/A N/A N/A N/A 15 0 GLASERO 09/01/2 05/25/20 FF, A N/A N/A N/A N/A 014 N/A N/A N/A N/A N/A N/A 15 0 VOLLRAT 01/07/20 Overdu H, K 15 N/A N/A N/A N/A e N/A N/A N/A N/A N/A N/A Overdue 2 GLASERO 09/01/2 Overdu 06/03/20 05/25/20 FF, A N/A N/A N/A N/A 014 N/A N/A N/A N/A e GLASERO 01/07/20 04/01/20 FF, A 15 N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A 15 0

48 Analytics Risk Dashboard View by selected Patients, demographics, and/or clinician Summary of overall risk for patient population 48

49 Monthly Speed Dating 49 Each care coordinator conferences with relevant clinician on CC panel they share Each CC works with each clinician allows for crosscoverage Focus on red areas immediate risk for poor outcome CC panel ~100 No one falls through the cracks Care gaps also addressed
50 A quote from a patient: SCC Case Study Before enrolling in SCC 01/24/ /24/2012 After enrolling in SCC 06/25/ /25/12 Stanford Coordinated Care focused on the little things that were leading to my needing to be hospitalized. Conditions: Corns and Callosities Osteomyelitis Systemic Lupus Erythematosis Lupus anti-coagulant disorder Vitritis of right eye Chronic Kidney Disease (stage IV severe) on hemodialysis Immunosuppressed status Hx Peritonitis Pericarditis in SLE Gout Anemia 4 Urgent inpatient admission (syncope, sepsis, peritonitis, osteomyelitis) 1 PCP and 5 Specialists $627,076 billed charges $104,513/month Care Management Interventions PCP pared foot callouses (source of osteomyelitis) Conference call with providers to adjust immune suppression drugs to reduce sepsis risk Family conference with PCP about importance of not cancelling specialist visits or risk falling off transplant list Development of an Action Plan with patient Regular patient contact from the Care Coordinator No (0) inpatient stays or surgeries 1 PCP and 2 Specialists $7837 billed charges $1306/month A quote from the PCP: By getting the specialists together on a conference call we were able to reduce the patient s risk of sepsis.
Stanford Coordinated Care
 Stanford Coordinated Care Support the patients, manage their care Ann Lindsay MD Alan Glaseroff MD IHI Innovation Network Webinar April 12, 2013 Where s the Leverage on Trend? Registries Gaps in Care Planned
Stanford Coordinated Care Support the patients, manage their care Ann Lindsay MD Alan Glaseroff MD IHI Innovation Network Webinar April 12, 2013 Where s the Leverage on Trend? Registries Gaps in Care Planned
Advanced Medical Homes: Bending the Trend. Alan Glaseroff, MD Co-Director Stanford Coordinated Care
 Advanced Medical Homes: Bending the Trend Alan Glaseroff, MD Co-Director Stanford Coordinated Care aglasero@stanford.edu 1 Hot Spotting in Employed Populations 1. Humboldt County, CA : Priority Care Partnered
Advanced Medical Homes: Bending the Trend Alan Glaseroff, MD Co-Director Stanford Coordinated Care aglasero@stanford.edu 1 Hot Spotting in Employed Populations 1. Humboldt County, CA : Priority Care Partnered
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Intensive Outpatient Care Program (IOCP)
") Intensive Outpatient Care Program (IOCP) PACIFIC BUSINESS GROUP ON HEALTH TABLE OF CONTENTS Introduction 1 Development Criteria Process for Intensive Outpatient Care Program 4 Assess Readiness and the
Intensive Outpatient Care Program (IOCP) PACIFIC BUSINESS GROUP ON HEALTH TABLE OF CONTENTS Introduction 1 Development Criteria Process for Intensive Outpatient Care Program 4 Assess Readiness and the
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
HIMSS Davies Enterprise Application --- COVER PAGE ---
 HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Improving Outcomes for individuals with high needs and highcosts: there? Eleni Carr Alan Glaseroff Douglas McCarthy Rebecca Ramsay Cory Sevin
 L26 These presenters have nothing to disclose Improving Outcomes for individuals with high needs and highcosts: what help is there? Eleni Carr Alan Glaseroff Douglas McCarthy Rebecca Ramsay Cory Sevin
L26 These presenters have nothing to disclose Improving Outcomes for individuals with high needs and highcosts: what help is there? Eleni Carr Alan Glaseroff Douglas McCarthy Rebecca Ramsay Cory Sevin
The Playbook: Better Care for People with Complex Needs
 The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
California Pay for Performance: A Case Study with First Year Results. Tom Williams Integrated Healthcare Association (IHA) March 17, 2005
 March 17, 2005") California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
Virtual Care Solutions Moving Care from the Hospital to the Home
 Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
Medication Trauma Crisis: Primary Care Innovations. Session Code: D25, E25
 Medication Trauma Crisis: Primary Care Innovations Session Code: D25, E25 Speakers and Disclosures Speaker James Slater, PharmD Executive Pharmacy Director, CareOregon Kristen Benkstein, PharmD Pharmacy
Medication Trauma Crisis: Primary Care Innovations Session Code: D25, E25 Speakers and Disclosures Speaker James Slater, PharmD Executive Pharmacy Director, CareOregon Kristen Benkstein, PharmD Pharmacy
National Survey of Physician Organizations and the Management of Chronic Illness II (Independent Practice Associations)
") If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
Accelerating the Impact of Performance Measures: Role of Core Measures
 Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
2018 PROVIDER TOOLKIT
 1100 Circle 75 Parkway Suite 1100 Atlanta, GA 30339 2018 PROVIDER TOOLKIT Understanding the Centers for Medicare and Medicaid (CMS) Stars Rating System What is CMS Quality Star Ratings program? CMS evaluates
1100 Circle 75 Parkway Suite 1100 Atlanta, GA 30339 2018 PROVIDER TOOLKIT Understanding the Centers for Medicare and Medicaid (CMS) Stars Rating System What is CMS Quality Star Ratings program? CMS evaluates
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts
 PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts 575 Market St. Ste. 600 SAN FRANCISCO, CA 94105 PBGH.ORG OFFICE 415.281.8660 FACSIMILE 415.520.0927 1. Please comment
PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts 575 Market St. Ste. 600 SAN FRANCISCO, CA 94105 PBGH.ORG OFFICE 415.281.8660 FACSIMILE 415.520.0927 1. Please comment
Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives. Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018
 Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018 Why Standardization? MEDI-CAL CROSS PRODUCT San Francisco Health
Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018 Why Standardization? MEDI-CAL CROSS PRODUCT San Francisco Health
Disclosures. Platforms for Performance: Clinical Dashboards to Improve Quality and Safety. Learning Objectives
 Platforms for Performance: Clinical Dashboards to Improve Quality and Safety Disclosures The program chair and presenters for this continuing pharmacy education activity report no relevant financial relationships.
Platforms for Performance: Clinical Dashboards to Improve Quality and Safety Disclosures The program chair and presenters for this continuing pharmacy education activity report no relevant financial relationships.
Athena Forum Institute. Home Health Workforce Performance 21 st Century Training for Healthcare Professionals
 Athena Forum Institute Home Health Workforce Performance 21 st Century Training for Healthcare Professionals The Journey of Workforce Performance Begins on Athena Forum. Dear Care Director in Home Health,
Athena Forum Institute Home Health Workforce Performance 21 st Century Training for Healthcare Professionals The Journey of Workforce Performance Begins on Athena Forum. Dear Care Director in Home Health,
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
Better Health and Lower Costs for Patients With Complex Needs
 Better Health and Lower Costs for Patients With Complex Needs An IHI Triple Aim Collaborative Informational Call May 12, 2015 Faculty on Informational Call Today Cory Sevin IHI Director Catherine Craig
Better Health and Lower Costs for Patients With Complex Needs An IHI Triple Aim Collaborative Informational Call May 12, 2015 Faculty on Informational Call Today Cory Sevin IHI Director Catherine Craig
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost
 Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Mission Health Care Network. April 2017
 Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Passport Advantage Provider Manual Section 8.0 Quality Improvement
 Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
Disease Management at Anthem West Or: what have we learned in trying to design these programs?
 Disease Management at Anthem West Or: what have we learned in trying to design these programs? Lisa M. Latts, MD, MSPH Regional Medical Director May 12, 2003 Anthem Inc. Anthem Inc. Headquarters: Indianapolis
Disease Management at Anthem West Or: what have we learned in trying to design these programs? Lisa M. Latts, MD, MSPH Regional Medical Director May 12, 2003 Anthem Inc. Anthem Inc. Headquarters: Indianapolis
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Dear New Patient, Once again, we would like to thank you for choosing us as your primary health care provider. We look forward to working with you.
 307 West Central Street Wendy J. Parker, M.D. Natick, MA 01760 Deborah J. Riester, M.D. Telephone: 508-820-8383 Jo-Ann Suna,M.D. Fax: 508-820-0250 Hadia F. Tirmizi, M.D. Natalia Sedo, N.P. Christine Chang,
307 West Central Street Wendy J. Parker, M.D. Natick, MA 01760 Deborah J. Riester, M.D. Telephone: 508-820-8383 Jo-Ann Suna,M.D. Fax: 508-820-0250 Hadia F. Tirmizi, M.D. Natalia Sedo, N.P. Christine Chang,
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home
 Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
MAKING PROGRESS, SEEING RESULTS
 MAKING PROGRESS, SEEING RESULTS VALUE-BASED CARE REPORT HUMANA.COM/VALUEBASEDCARE Y0040_GCHK4DYEN 1117 Accepted 2 Americans are sick and getting sicker, with millions of us living with chronic conditions
MAKING PROGRESS, SEEING RESULTS VALUE-BASED CARE REPORT HUMANA.COM/VALUEBASEDCARE Y0040_GCHK4DYEN 1117 Accepted 2 Americans are sick and getting sicker, with millions of us living with chronic conditions
Employer Breakout Session Payment Change in Ohio: What it Means for Employers
 Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
Telecare Services 7/19/2017
 Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Franciscan Alliance ACO
 Franciscan Alliance ACO Jennifer Westfall Regional VP Franciscan Alliance Accountable Care Organization Regional Executive Director, St. Francis Health Network 2013 Franciscan Alliance, Inc. What is an
Franciscan Alliance ACO Jennifer Westfall Regional VP Franciscan Alliance Accountable Care Organization Regional Executive Director, St. Francis Health Network 2013 Franciscan Alliance, Inc. What is an
Bright Spots in primary care
 Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
The Why and How. Carol L. Henwood, DO, FACOFP dist.
 Patient-Centered Medical Home: The Why and How Carol L. Henwood, DO, FACOFP dist. AODME January 14, 2012 The Triple Aim Improved Health Enhanced Patient Experience of Care Reduced Cost [+1: Improved Productivity]
Patient-Centered Medical Home: The Why and How Carol L. Henwood, DO, FACOFP dist. AODME January 14, 2012 The Triple Aim Improved Health Enhanced Patient Experience of Care Reduced Cost [+1: Improved Productivity]
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Medicare Advantage Star Ratings
 Medicare Advantage Star Ratings December 2017 The Star Rating System measures how well Medicare Advantage (MA) and its prescription drug plans perform for consumers. As an integrated health system, Presbyterian
Medicare Advantage Star Ratings December 2017 The Star Rating System measures how well Medicare Advantage (MA) and its prescription drug plans perform for consumers. As an integrated health system, Presbyterian
Pharmacists Improve Care Through Team Collaboration
 Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Weaving Expanded Roles of the RN into Population Management
 Weaving Expanded Roles of the RN into Population Management Lois K. Andrews, DNP, RN-BC, CNS, ACNS-BC, CCRN Sentara Quality Care Network (SQCN), Norfolk, Va. Objectives: Explore the evolution of healthcare
Weaving Expanded Roles of the RN into Population Management Lois K. Andrews, DNP, RN-BC, CNS, ACNS-BC, CCRN Sentara Quality Care Network (SQCN), Norfolk, Va. Objectives: Explore the evolution of healthcare
How Does This Fit into the Provisions of the Affordable Care Act? The goals are aligned
 Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Shana Scott, JD, MPH, Health Systems Team Lead Tuesday, October 3, 2017
 Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Performance Measurement Work Group Meeting 10/18/2017
 Performance Measurement Work Group Meeting 10/18/2017 Welcome to New Members QBR RY 2020 DRAFT QBR Policy Components QBR Program RY 2020 Snapshot QBR Consists of 3 Domains: Person and Community Engagement
Performance Measurement Work Group Meeting 10/18/2017 Welcome to New Members QBR RY 2020 DRAFT QBR Policy Components QBR Program RY 2020 Snapshot QBR Consists of 3 Domains: Person and Community Engagement
How to Build a Medical Home
 How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
ONTARIO COUNTY HEALTH PROFILE. Finger Lakes Health Systems Agency, 2017
 ONTARIO COUNTY HEALTH PROFILE Finger Lakes Health Systems Agency, 2017 About the Report The purpose of this report is to provide a summary of health data specific to Ontario County. Where possible, benchmarks
ONTARIO COUNTY HEALTH PROFILE Finger Lakes Health Systems Agency, 2017 About the Report The purpose of this report is to provide a summary of health data specific to Ontario County. Where possible, benchmarks
ADULT PATIENT INFORMATION. Patient Name: Last Name First Name Address: City: State: Zip Code: Phone #: Cell Phone #: Social Security:
 716 S. Goldenrod Road n 3315 Orange Blossom Trail Fax (407) 658-2536 Fax (407) 343-1907 ADULT PATIENT INFORMATION Patient Name: Last Name First Name MI Address: City: State: Zip Code: Phone #: Cell Phone
716 S. Goldenrod Road n 3315 Orange Blossom Trail Fax (407) 658-2536 Fax (407) 343-1907 ADULT PATIENT INFORMATION Patient Name: Last Name First Name MI Address: City: State: Zip Code: Phone #: Cell Phone
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Quality Improvement Program
 How we measure up At HealthKeepers, Inc., we focus on helping our Anthem HealthKeepers Plus members get healthy and stay healthy. To help us serve you the best we can, each year we look closely at the
How we measure up At HealthKeepers, Inc., we focus on helping our Anthem HealthKeepers Plus members get healthy and stay healthy. To help us serve you the best we can, each year we look closely at the
Value Based Care: Trends for Boston Chicago Houston Los Angeles Miami San Francisco Washington, DC
 Value Based Care: Trends for 2018 Boston Chicago Houston Los Angeles Miami San Francisco Washington, DC Need head shot David Fairchild, MD Director BDC Advisors Dave Terry CEO & Co-Founder Archway Health
Value Based Care: Trends for 2018 Boston Chicago Houston Los Angeles Miami San Francisco Washington, DC Need head shot David Fairchild, MD Director BDC Advisors Dave Terry CEO & Co-Founder Archway Health
arizona health net a better decision sm Putting you at the center of everything we do.
 arizona health net a better decision sm Putting you at the center of everything we do. Nothing s more important than your health. When you re healthy, you want to stay healthy. When you re sick or have
arizona health net a better decision sm Putting you at the center of everything we do. Nothing s more important than your health. When you re healthy, you want to stay healthy. When you re sick or have
NextGen Population Health TEN TEN TEN TEN TE. Prevent Patients from Falling Through the Cracks in 10 Easy Steps
 NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Rural and Independent Primary Care.
 Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
LIVINGSTON COUNTY HEALTH PROFILE. Finger Lakes Health Systems Agency, 2017
 LIVINGSTON COUNTY HEALTH PROFILE Finger Lakes Health Systems Agency, 2017 About the Report The purpose of this report is to provide a summary of health data specific to Livingston County. Where possible,
LIVINGSTON COUNTY HEALTH PROFILE Finger Lakes Health Systems Agency, 2017 About the Report The purpose of this report is to provide a summary of health data specific to Livingston County. Where possible,
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Leading By Example. Begin with a vision. Disclosures. Learning Objectives 3/25/2017. Tripp Logan, PharmD
 Leading By Example Melissa Somma McGivney, PharmD, FAPhA, FCCP Associate Dean for Community Partnerships; Associate Professor University of Pittsburgh Tripp Logan, PharmD Senior Quality Consultant - MedHere
Leading By Example Melissa Somma McGivney, PharmD, FAPhA, FCCP Associate Dean for Community Partnerships; Associate Professor University of Pittsburgh Tripp Logan, PharmD Senior Quality Consultant - MedHere
STEUBEN COUNTY HEALTH PROFILE
 STEUBEN COUNTY HEALTH PROFILE 2017 ABOUT THE REPORT The purpose of this report is to provide a summary of health data specific to Steuben County. Where possible, benchmarks have been given to compare county
STEUBEN COUNTY HEALTH PROFILE 2017 ABOUT THE REPORT The purpose of this report is to provide a summary of health data specific to Steuben County. Where possible, benchmarks have been given to compare county
Community Paramedicine Seminar July, 20th 2015
 Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
The Virtual Connection: Electronic Visits. Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009
 The Virtual Connection: Electronic Visits Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009 The Holy Grail of Health Care 2009 Cost Reduction Quality Improvement Service Improvement
The Virtual Connection: Electronic Visits Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009 The Holy Grail of Health Care 2009 Cost Reduction Quality Improvement Service Improvement
Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance
 Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance Joan Valentine, MSA, RN Executive Vice President Visiting Physicians Association David
Session 10: Integrating Data and Analytics into Provider Workflows Improves ACO Quality and Financial Performance Joan Valentine, MSA, RN Executive Vice President Visiting Physicians Association David
SURVEY Being Patient. Accessibility, Primary Health and Emergency Rooms
 SURVEY 2017 Being Patient Accessibility, Primary Health and Emergency Rooms Being Patient: Accessibility, Primary Health and Emergency Rooms New Brunswick Health Council Who we are New Brunswickers have
SURVEY 2017 Being Patient Accessibility, Primary Health and Emergency Rooms Being Patient: Accessibility, Primary Health and Emergency Rooms New Brunswick Health Council Who we are New Brunswickers have
A legacy of primary care support underscores Priority Health s leadership in accountable care
 Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
What is Mental Health Integration?
 What is Mental Health Integration? Quality Experience Cost A standardized clinical and operational team process that incorporates mental health as a complementary component of wellness & healing * Mental
What is Mental Health Integration? Quality Experience Cost A standardized clinical and operational team process that incorporates mental health as a complementary component of wellness & healing * Mental
Moving the Dial on Quality
 Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Integrated Health System
 Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2