TOOLS AND TECHNIQUES FOR PRACTICE TRANSFORMATION
|
|
|
- Morris Lucas
- 5 years ago
- Views:
Transcription
1 TOOLS AND TECHNIQUES FOR PRACTICE TRANSFORMATION
2 TOPICS Assessing your current environment Cultivating a culture of excellence Closing care gaps Improving patient self management Reducing ED Utilization
3 ASSESSING YOUR CURRENT ENVIRONMENT
4 ORGANIZATIONAL CAPACITY FOR IMPROVEMENT Organizational leadership is interested in specific or general improvement (improved patient outcomes, patient satisfaction, etc.) Organization is willing and able to identify an improvement champion who will be the practice facilitator s point person. Leadership is willing to provide protected time for key staff to engage in improvement work. Team members are willing to meet regularly as a quality improvement team, and members follow through with this plan.
5 ORGANIZATIONAL CAPACITY FOR IMPROVEMENT Team members are willing to gather and report data on practice performance on key metrics Practice has sufficient organizational and financial stability to avoid becoming too distracted or overwhelmed by competing demands or financial concerns. Practice is not engaged in other large-scale improvement projects and does not have other demanding competing priorities.
6 CHANGE PROCESS CAPABILITY QUESTIONNAIRE (CPCQ) 32 questions targeting: 1. How your practice approaches quality improvement 2. How your clinic has used various strategies to improve quality of care in the past
7 PROCESS CAPABILITY QUESTIONNAIRE (CPCQ) Dimensions of Focus: Importance of quality care and outcomes Cares is patient focused Deliberate design of systems catered to the patient Availability of resources Use of data, measurement to gauge performance quality, achieve goals Rapid cycle system tests of change, pre-testing, piloting
8 CULTIVATING A CULTURE OF EXCELLENCE


9 CULTURE Culture is the way we think, act and interact


10 HOW BEHAVIORS INFLUENCE OUTCOMES Adapted from R. Cook and D. Woods, Operating at the Sharp End: The Complexity of Human Error (1994)
11 TOOL FOR CHANGING PRACTICE CULTURE RELATIONSHIP-CENTERED MEETINGS Invest Time in Relationship Building; It Will Pay Large Dividends in Efficiency and Performance. Foster High-Quality Conversation Explore Differences with Openness and Curiosity -stimulus for creativity, not conflict. In Pursuing Change, Learn from Successes. When Meetings Get Stuck, Interrupt the Pattern Trust the Process; Don t Try to Control the Outcome. Reproduced with permission from: Anthony L. Suchman and Penelope R. Williamson. Principles and Practices of Relationship-Centered Meetings
12 CLOSING CARE GAPS

13 GOALS FOR CLOSING CARE GAPS FOR SAFETY NET PATIENTS Reduce costly preventable readmissions Improve chronic disease management Boost patient engagement Develop robust and effective population health management programs.



14 FOUNDATIONAL STEPS AIMED AT CLOSING GAPS Shared knowledge and shared decision making Improve health literacy Provide impactful education Focused on patient s individual background, beliefs, and experiences. Team-based, collaborative care Collaborative effort involving caretakers and family members Consult other members of the patient s care team, Cultural sensitivity and respect When care impacts cultural norms, religious beliefs, or lifestyle choices, clinicians must approach these issues with respect, sensitivity, and understanding. Building trusting relationships




15 FOUNDATIONAL STEPS AIMED AT CLOSING GAPS Risk Stratification Based on multiple co-morbidities, unstable chronic conditions Recent re-admissions, ED visits Care Management Education Group visits Wellness & prevention classes IT Systems Patient Portals Text reminders s Care Gaps Reports ADT Feeds
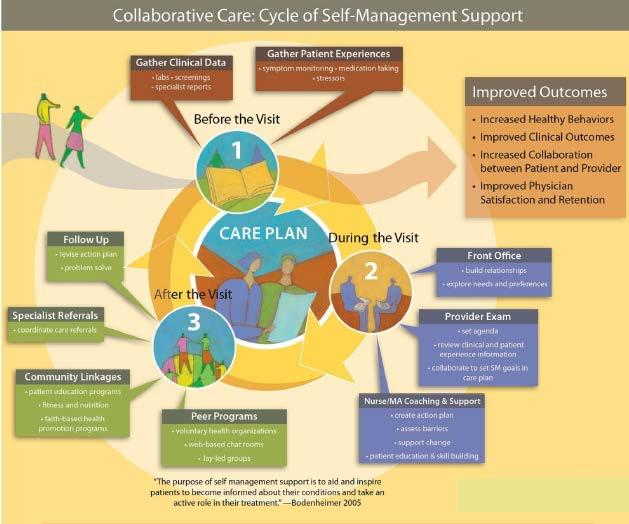
16 IMPROVING PATIENT SELF MANAGEMENT
17 HOW CAN SELF-MANAGEMENT SUPPORT BE PUT INTO ACTION? Defining and sharing the roles and responsibilities of the practice care team. Successful teams are made up of clinical and administrative staff whose roles are planned in advance. Provides effective self-management support, a team of clinicians and administrative staff need to coordinate closely with each other to provide care before, during, and after the patient visit. Maximizes the functionality of the team, streamlines workflow and combats duplication of tasks
18 SELF-MANAGEMENT SUPPORT Some roles and responsibilities include: Conducting a team huddle prior to clinic starting Gathering clinical data before a visit Setting agendas for the visit Helping patients set health goals Developing action plans for achieving goals Tracking health outcomes Referring patients to community programs
19 19
20 REDUCING ED UTILIZATION
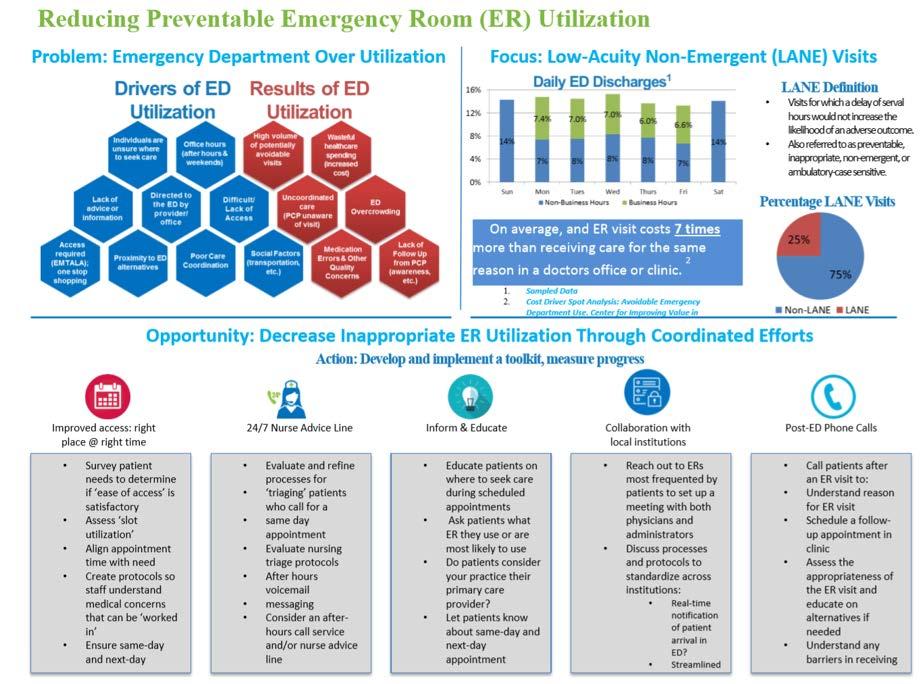
21 REDUCTION IN ED VISITS Why is this important? The overuse of U.S. emergency departments (EDs) is responsible for $38 billion in wasteful spending each year ED overuse is on the rise across all patient populations, irrespective of age or insurance coverage Drivers of ED overuse include lack of access to timely primary care services, referral to the ED by primary care physicians themselves, and financial and legal obligations by hospitals to treat all patients who arrive in the ED Strategies to curb ED overuse include redesigning primary care to improve access and scheduling; providing alternative sites for non-urgent primary care; improving case management of patients with chronic disease, and using financial incentives and disincentives for visit to the ED

; EMERGENT ED CARE NEEDED- PREVENTABLE/AVOIDABLE - Emergency department care was required based on the complaint or procedures performed/resources used, but the")
; and PAGE 22 NON-EMERGENT- The patient's initial complaint, presenting symptoms, vital signs, medical history, and age indicated that immediate medical care was not required within 12 hours; LANE")
22 Low Acuity Non Emergent ED Visit Definition NYU Classification Categories EMERGENT-PRIMARY CARE TREATABLE- Based on information in the record, treatment was required within 12 hours, but care could have been provided effectively and safely in a primary care setting. The complaint did not require continuous observation, and no procedures were performed or resources used that are not available in a primary care setting (e.g., CAT scan or certain lab tests); EMERGENT ED CARE NEEDED- PREVENTABLE/AVOIDABLE - Emergency department care was required based on the complaint or procedures performed/resources used, but the emergent nature of the condition was potentially preventable/avoidable if timely and effective ambulatory care had been received during the episode of illness (e.g., the flare-ups of asthma, diabetes, congestive heart failure, etc.); and PAGE 22 NON-EMERGENT- The patient's initial complaint, presenting symptoms, vital signs, medical history, and age indicated that immediate medical care was not required within 12 hours; LANE VISIT EMERGENT ED CARE NEEDED- NOT PREVENTIABLE/AVOIDABLE: Emergency department care was required and ambulatory care treatment could not have prevented the condition (e.g., trauma, appendicitis, myocardial infarction, etc.)
23
24 POTENTIAL TACTICS After-hours access: Practices that implement after hours call systems that allow patients to access care providers have been seen to reduce the frequency of patients going to the ED unnecessarily Specialist Collaboration with Primary Care Physician: Specialists should consider contacting a patient s primary care provider prior to recommending a patient go to the ED to determine if a PCP clinic visit is appropriate. Patient alerts: Partnerships with local Emergency Departments can create protocols to alert your practice when your patients are seen in the ED, letting your practice set follow up appointments to see the patient in clinic the next day. Tracking ED visits: Working with local hospitals to receive monthly reports about ED visits of patients affiliated with your practice can help identify key opportunities to prevent future non-urgent ED visits. Collaboration on care with the local ED: Developing a relationship with the local ED can help to develop shared approaches to care for patients that could help to reduce unnecessary emergency department visits and hospitalizations. For example, providers can work with local EDs to develop approaches for the prescription of controlled substances such as narcotics, and for management of common conditions (ex. cellulitis, deep vein thrombosis, heart failure, etc.). Community Partnerships: collaborations with local resources, such as urgent care clinics, can provide after-hours and weekend coverage for patients while ensuring coordinated care. See the case example above. Patient education:voice messaging systems should clearly indicate how to reach an on-call physician or answering service for non-emergent requests. Similarly, education of patients regarding after hours needs should be provided during standard care visits, particularly focusing on high utilizers.
25 Self Management Support: 1. Resources and Links 2. ED Utilization Tool KIT 1. Health Literacy Measurement Tools: 1. Brief Health Literacy Screen (BHLS) 2. Test Of Functional Health Literacy for Adults (TOFHLA) 3.Subjective Numeracy Scale (SNS) 3.Rapid Estimate of Adult Literacy in Medicine (REALM) 4.Newest Vital Sign (NVS) 5.General Health Numeracy Test (GHNT)
26 RESOURCES & TOOLKITS American Academy of Family Physicians' A New Approach to Group Visits: Helping High-Need Patients Make Behavioral Change California HealthCare Foundation s Helping Patients Help Themselves: How to Implement Self-Mangement Support California HealthCare Foundation's Coaching Patients for Successful Self-Management American Academy of Family Physicians Improve Care With Patient Self-Management Support American Medical Association's Self-Management Strategies for Vulnerable Populations

27 QUESTIONS
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Webinar Series on Innovation and Re-Design of Systems of Behavioral Health Care March 23, :00 PM With Roger Resar, MD of IHI IBHI
 www.ibhi.net Webinar Series on Innovation and Re-Design of Systems of Behavioral Health Care March 23, 2011 3:00 PM With Roger Resar, MD of IHI IBHI Alden (Joe) Doolittle, Moderator Joe@IBHI.net Peter
www.ibhi.net Webinar Series on Innovation and Re-Design of Systems of Behavioral Health Care March 23, 2011 3:00 PM With Roger Resar, MD of IHI IBHI Alden (Joe) Doolittle, Moderator Joe@IBHI.net Peter
Issue Brief. Non-urgent Emergency Department Use in Shelby County, Tennessee, May August 2012
 Issue Brief May 2011 Non-urgent Emergency Department Use in Shelby County, Tennessee, 2009 Cyril F. Chang, Ph.D. Professor of Economics and Director of Methodist Le Bonheur Center for Healthcare Economics
Issue Brief May 2011 Non-urgent Emergency Department Use in Shelby County, Tennessee, 2009 Cyril F. Chang, Ph.D. Professor of Economics and Director of Methodist Le Bonheur Center for Healthcare Economics
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
All ACO materials are available at What are my network and plan design options?
 ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Michigan Primary Care Transformation Project. HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care
 Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Putting Health Literacy into Practice. IHC Care Coordination Conference June 3, 2015
 Putting Health Literacy into Practice IHC Care Coordination Conference June 3, 2015 Objectives Review the essentials of health literacy. Detail how health literacy can improve existing patient engagement
Putting Health Literacy into Practice IHC Care Coordination Conference June 3, 2015 Objectives Review the essentials of health literacy. Detail how health literacy can improve existing patient engagement
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Chapter VII. Health Data Warehouse
 Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
POPULATION HEALTH LEARNING NETWORK 1
 In partnership with the California Health Care Foundation (CHCF) and the Blue Shield of California Foundation (BSCF), the Center for Care Innovations (CCI) is launching a Population Heath Learning Network
In partnership with the California Health Care Foundation (CHCF) and the Blue Shield of California Foundation (BSCF), the Center for Care Innovations (CCI) is launching a Population Heath Learning Network
Advocate Health Care. PURPOSE: Describe briefly the overall purpose of this position, i.e., Why does it exist?
 http://corp2371.ahc-ad.advocatehealth.com/jobdescriptions/printpreview.aspx?jdid=40442 4/24/2012 Advocate Health Care Title: Practice Operations Coach PURPOSE: Describe briefly the overall purpose of this
http://corp2371.ahc-ad.advocatehealth.com/jobdescriptions/printpreview.aspx?jdid=40442 4/24/2012 Advocate Health Care Title: Practice Operations Coach PURPOSE: Describe briefly the overall purpose of this
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices
 Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
University of California, Davis Family Practice Center: Update 2014
 University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
UnitedHealth Center for Health Reform & Modernization September 2014
 Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Fast-Track PCMH Recognition
 Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Oregon s Health System Transformation: The Coordinated Care Model. March 2014 Jeanene Smith MD, MPH Chief Medical Officer- Oregon Health Authority
 Oregon s Health System Transformation: The Coordinated Care Model March 2014 Jeanene Smith MD, MPH Chief Medical Officer- Oregon Health Authority The Challenges Oregon Faced Rising healthcare costs outpacing
Oregon s Health System Transformation: The Coordinated Care Model March 2014 Jeanene Smith MD, MPH Chief Medical Officer- Oregon Health Authority The Challenges Oregon Faced Rising healthcare costs outpacing
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Deriving Value from a Health Information Exchange. HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017
 Deriving Value from a Health Information Exchange HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017 About Healthix About Healthix Hundreds of healthcare organizations at more than
Deriving Value from a Health Information Exchange HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017 About Healthix About Healthix Hundreds of healthcare organizations at more than
TELEHEALTH FOR HEALTH SYSTEMS: GUIDE TO BEST PRACTICES
 TELEHEALTH FOR HEALTH SYSTEMS: GUIDE TO BEST PRACTICES Overview Telemedicine delivers care that s convenient and cost effective letting physicians and patients avoid unnecessary travel and wait time. Health
TELEHEALTH FOR HEALTH SYSTEMS: GUIDE TO BEST PRACTICES Overview Telemedicine delivers care that s convenient and cost effective letting physicians and patients avoid unnecessary travel and wait time. Health
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Coordinated Care: Key to Successful Outcomes
 Coordinated Care: Key to Successful Outcomes Best practices in care coordination improve health, lower costs and increase patient satisfaction 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.continuumhealth.net
Coordinated Care: Key to Successful Outcomes Best practices in care coordination improve health, lower costs and increase patient satisfaction 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.continuumhealth.net
URAC Patient Centered Medical Home
 URAC Patient Centered Medical Home Presented by: Cynthia Cook, RN, BSN Sr. Director Business Development Data Only 27% of U.S. adults can easily contact their primary care physicians by telephone, obtain
URAC Patient Centered Medical Home Presented by: Cynthia Cook, RN, BSN Sr. Director Business Development Data Only 27% of U.S. adults can easily contact their primary care physicians by telephone, obtain
TABLE H: Finalized Improvement Activities Inventory
 TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014
 USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
Central Ohio Primary Care (COPC) Spotlight on Innovation
 Spotlight on Innovation") Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Patient-Clinician Communication:
 Discussion Paper Patient-Clinician Communication: Basic Principles and Expectations Lyn Paget, Paul Han, Susan Nedza, Patricia Kurtz, Eric Racine, Sue Russell, John Santa, Mary Jean Schumann, Joy Simha,
Discussion Paper Patient-Clinician Communication: Basic Principles and Expectations Lyn Paget, Paul Han, Susan Nedza, Patricia Kurtz, Eric Racine, Sue Russell, John Santa, Mary Jean Schumann, Joy Simha,
Specialty practices and primary care practices join forces in providing patient centered medical care
 Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Community Mental Health and Care integration. Zandrea Ware and Ricardo Fraga
 Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Verdien av egengenerert helsedata. Oslo, Tor Jakob Ramsøy
 Verdien av egengenerert helsedata Oslo, 1.9.2015 Tor Jakob Ramsøy torjakob@arundo.com 0 Patient Generated Data is not new, but has taken on a much bigger role in this new era of data abundance and ubiquitous
Verdien av egengenerert helsedata Oslo, 1.9.2015 Tor Jakob Ramsøy torjakob@arundo.com 0 Patient Generated Data is not new, but has taken on a much bigger role in this new era of data abundance and ubiquitous
Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait
 Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait A White Paper March 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800-680-7570 Impact-Advisors.com
Transforming Clinical Care: Why Optimization of Clinical Systems Can t Wait A White Paper March 2016 Impact Advisors LLC 400 E. Diehl Road Suite 190 Naperville IL 60563 1-800-680-7570 Impact-Advisors.com
Community Health Excellence (CHE) Grant Program Application Guide
 Grant Program Application Guide") Community Health Excellence (CHE) Grant Program 2018 2019 Application Guide CHE Mission and Goals The PacificSource Community Health Excellence (CHE) initiative was created to align with and support the
Community Health Excellence (CHE) Grant Program 2018 2019 Application Guide CHE Mission and Goals The PacificSource Community Health Excellence (CHE) initiative was created to align with and support the
2014 Patient Centered Medical Home (PCMH) Recognition
 Recognition") Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Consumer ehealth Affinity Group
 Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Transforming Delivery Systems for Population Health
 Transforming Delivery Systems for Population Health George Isham, M.D., M.S. Senior Advisor, HealthPartners Senior Fellow, HealthPartners Institute for Education and Research October 9, 2015 Presenter
Transforming Delivery Systems for Population Health George Isham, M.D., M.S. Senior Advisor, HealthPartners Senior Fellow, HealthPartners Institute for Education and Research October 9, 2015 Presenter
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement?
 Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Improving Emergency Department Transitions of Care Can It Help with ED Overcrowding? Stephen V. Cantrill, MD, FACEP Denver Health Medical Center
 Improving Emergency Department Transitions of Care Can It Help with ED Overcrowding? Stephen V. Cantrill, MD, FACEP Denver Health Medical Center Improving Emergency Department Transitions of Care: Can
Improving Emergency Department Transitions of Care Can It Help with ED Overcrowding? Stephen V. Cantrill, MD, FACEP Denver Health Medical Center Improving Emergency Department Transitions of Care: Can
Shifting from Volume to Value-based Healthcare. November 2014 Briefing
 Shifting from Volume to Value-based Healthcare November 2014 Briefing The Healthcare Collaborative of Greater Columbus is a non-profit, public-private partnership. We serve as a catalyst, convener, and
Shifting from Volume to Value-based Healthcare November 2014 Briefing The Healthcare Collaborative of Greater Columbus is a non-profit, public-private partnership. We serve as a catalyst, convener, and
Community Integrated Paramedicine:
 Community Integrated Paramedicine: An Emerging Model to Improve Outcomes in Rural AZ Will Humble, MPH Director, Health Policy and Evaluation The University of Arizona Center for Population Science and
Community Integrated Paramedicine: An Emerging Model to Improve Outcomes in Rural AZ Will Humble, MPH Director, Health Policy and Evaluation The University of Arizona Center for Population Science and
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Transforming Clinical Practices Initiative
 Transforming Clinical Practices Initiative Overview CMS through its Center for Medicare & Medicaid Innovation is launching its Transforming Clinical Practices Initiative (TCPI), which over a four-year
Transforming Clinical Practices Initiative Overview CMS through its Center for Medicare & Medicaid Innovation is launching its Transforming Clinical Practices Initiative (TCPI), which over a four-year
PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER
 PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER Presented by: Kevin Bozza, MPA, FACHE, CPHQ, RHIT Sr. Director, Network Development
PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER Presented by: Kevin Bozza, MPA, FACHE, CPHQ, RHIT Sr. Director, Network Development
Cutting Avoidable Readmissions Starts in the Emergency Department
 WHITE PAPER Cutting Avoidable Readmissions Starts in the Emergency Department SMARTER EMERGENCY CARE: EVERYWHERE, EVERY TIME. Our experience and innovative approach offers smarter solutions for emergency
WHITE PAPER Cutting Avoidable Readmissions Starts in the Emergency Department SMARTER EMERGENCY CARE: EVERYWHERE, EVERY TIME. Our experience and innovative approach offers smarter solutions for emergency
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS
 UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
Integrated Leadership for Hospitals and Health Systems: Principles for Success
 Integrated Leadership for Hospitals and Health Systems: Principles for Success In the current healthcare environment, there are many forces, both internal and external, that require some physicians and
Integrated Leadership for Hospitals and Health Systems: Principles for Success In the current healthcare environment, there are many forces, both internal and external, that require some physicians and
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework
 The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
Report on a QI Project Eligible for Part IV MOC
 Report on a QI Project Eligible for Part IV MOC Instructions Determine eligibility. Before starting to complete this report, go to the UMHS MOC website [ocpd.med.umich.edu], click on Part IV Credit Designation,
Report on a QI Project Eligible for Part IV MOC Instructions Determine eligibility. Before starting to complete this report, go to the UMHS MOC website [ocpd.med.umich.edu], click on Part IV Credit Designation,
Informatics, PCMHs and ACOs: A Brave New World
 Informatics, PCMHs and ACOs: A Brave New World R. Clark Campbell, MSN, RN-BC, CPHIMS, FHIMSS Kathleen Kimmel, RN, BSN, MHA, CPHIMS, FHIMSS Engagement Executive with Health Catalyst Objectives - Define
Informatics, PCMHs and ACOs: A Brave New World R. Clark Campbell, MSN, RN-BC, CPHIMS, FHIMSS Kathleen Kimmel, RN, BSN, MHA, CPHIMS, FHIMSS Engagement Executive with Health Catalyst Objectives - Define
Care Compact Guide Patient-Centered Specialty Care (PCSC) A Component of Medical Neighborhood Initiatives
 A Component of Medical Neighborhood Initiatives") Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Checklist for Ocean County Community Health Improvement Plan Implementation of Strategies- Activities for Ocean County Health Centers: CHEMED & OHI
 Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Building Coordinated, Patient Centered Care Management Teams
 Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Fostering Effective Integration of Behavioral Health and Primary Care in Massachusetts Guidelines. Program Overview and Goal.
 Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs
 The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs Medical Group Management Association (MGMA ) publications are intended to provide current and accurate information and
The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs Medical Group Management Association (MGMA ) publications are intended to provide current and accurate information and
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Community Paramedicine Seminar July, 20th 2015
 Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions
 Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions Instructions: Please find below guiding questions for behavioral health organizations or divisions
Completing the Specialty Practice Assessment Tool: Guide for Behavioral Health Organizations and Divisions Instructions: Please find below guiding questions for behavioral health organizations or divisions
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of
 2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
2016 Experian Information Solutions, Inc. All rights reserved. Experian and the marks used herein are service marks or registered trademarks of Experian Information Solutions, Inc. Other product and company
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
Clinical Program Cost Leadership Improvement
 Clinical Program Cost Leadership Improvement December 2017 Presbyterian recently developed a rapid-cycle process for integrating sustainable cost and quality improvements within clinical programs. Population
Clinical Program Cost Leadership Improvement December 2017 Presbyterian recently developed a rapid-cycle process for integrating sustainable cost and quality improvements within clinical programs. Population
Four Game-Changing Strategies for Transforming the Patient Experience
 Four Game-Changing Strategies for Transforming the Patient Experience Reaching and engaging your population is one of the most challenging components of patient-centered care. Despite the challenges, there
Four Game-Changing Strategies for Transforming the Patient Experience Reaching and engaging your population is one of the most challenging components of patient-centered care. Despite the challenges, there
Identifying and Treating Your High Risk Patient Population. Beth Hickerson Quality Improvement Advisor August 15, 2017
 Identifying and Treating Your High Risk Patient Population Beth Hickerson Quality Improvement Advisor August 15, 2017 HIGH RISK PATIENTS What and Why? What is a high-risk patient? High level of resource
Identifying and Treating Your High Risk Patient Population Beth Hickerson Quality Improvement Advisor August 15, 2017 HIGH RISK PATIENTS What and Why? What is a high-risk patient? High level of resource
WPS Integrated Care Management Improving health, one member at a time
 WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
The Physician s Perspective
 The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
Rethinking the model of primary care. Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine
 Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
APEx Evidence Indicators: MIPS Improvement Activities
 APEx Evidence Indicators: Improvement Activities ASTRO s Accreditation Program for Excellence (APEx ) focuses on a culture of quality and safety, as well as patient-centered care. Evidence indicators required
APEx Evidence Indicators: Improvement Activities ASTRO s Accreditation Program for Excellence (APEx ) focuses on a culture of quality and safety, as well as patient-centered care. Evidence indicators required
Provider Manual. Utilization Management Care Management
 Provider Manual Utilization Management Care Management Utilization Management This section of the Manual was created to help guide you and your staff in working with Kaiser Permanente s Resource Stewardship
Provider Manual Utilization Management Care Management Utilization Management This section of the Manual was created to help guide you and your staff in working with Kaiser Permanente s Resource Stewardship
Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP)
 & Patient-Centered Specialty Practice (PCSP)") Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP) Foundation for a Better Health Care System Presenter Jeanette Ikan, M.D., MHAI Objectives: Definition and benefits of PCMH,
Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP) Foundation for a Better Health Care System Presenter Jeanette Ikan, M.D., MHAI Objectives: Definition and benefits of PCMH,
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition
 What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
Behavioral and Mental Health: High-Weighted. Behavioral and Mental Health: Medium-Weighted. Implementation of co-location PCP and MH services
 Behavioral and Mental Health: High-Weighted Implementation of co-location PCP and MH services *Implementation of integrated PCBH model Integration facilitation, and promotion of the colocation of mental
Behavioral and Mental Health: High-Weighted Implementation of co-location PCP and MH services *Implementation of integrated PCBH model Integration facilitation, and promotion of the colocation of mental
General Eligibility Requirements
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)