Improving Vascular Services A Case for Centralisation of Vascular Services in Lancashire and Cumbria
|
|
|
- Malcolm Julian Roberts
- 5 years ago
- Views:
Transcription

1 Cardiac and Stroke Networks in Lancashire & Cumbria Improving Vascular Services A Case for Centralisation of Vascular Services in Lancashire and Cumbria Version Final Date Sept 2010-March 2011 Author Natalie Park Natalie.park@csnlc.nhs.uk
2 Contents Chapter 1 - Background 1.1 Review of Vascular Services in Lancashire and Cumbria 1.2 The Case for Change 1.3 Important Factors that Influence Patient Outcomes 1.4 Benefits of Centralisation 1.5 Impact 1.6 Risks Chapter 2 - Epidemiology 2.1 Impact of Risk Factors-Epidemiological Information 2.2 Age 2.3 Diabetes 2.4 Obesity and Diabetes 2.5 Smoking 2.6 Targets for Reducing CVD Chapter 3 - Vascular Procedures 3.1 What are Vascular Services? 3.2 Main Procedures to Consider Chapter 4 - Present Providers 4.1Present Provider Landscape 4.2 Current Patient Flows 4.3 Information on all Sites Currently Providing Vascular Services Chapter 5 - Length of Stay 5.1 Reducing Length of Hospital Stay by Centralisation 5.2 Length of Hospital Stay 5.3 Current Average Length of Stay in the Lancashire & Cumbria Network Chapter 6 - Numbers of Specialists Required 6.1 Numbers of Surgeons Required for the Population 6.2 Numbers of Interventional Radiologists 6.3 Vascular Specialists 6.4 Vascular Nurse Specialists Chapter 7 - Links with other Specialities 7.1 Critical Links - Specialties Supporting a Vascular Service 7.2 The Impact on Major Trauma and Stroke 7.3 Other Service Considerations 7.4 Amputations Amputee Rehabilitation in a Centralised Unit Chapter 8 - Workload Requirements 8.1 Activity and Length of Stay Assessment 8.2 Day Case & GP Referral 8.3 Procedure Volume Requirement 8.4 Current Activity Across the Network 8.5 Figures Based on Minimum Population 8.6 Required Theatre Capacity
3 Chapter 9 - Proposed Models 9.1 Recommendations of the Review 9.2 Proposals & Network Formation 9.3 Proposals made by the Vascular Clinical Advisory Group 9.4 Formation of Vascular Network 9.5 Proposed Model Options One and Two 9.6 Workforce Planning 9.7 Patient & Public Involvement Chapter 10 - Costs of Vascular Services 10.1 Tariff and Numbers of Vascular Procedures Commissioned 10.2 Procurement 10.3 Increased use of EVAR & Cost Implications 10.4 Reduced Aortic Aneurysm Repair Length of Stay Due to Increased Uptake of Endovascular Aneurysm Repairs 10.5 Financial Implications for Providers 10.6 Reduced Length of Stay Following CEA 10.7 Productive Bed Use 10.8 Ambulance Implications Chapter 11 - Implementation Plans 11.1 Implementation Timetable Chapter 12 - Recommendation Checklist for Vascular Reviews Recommendations from other North West Reviews Appendices Appendi 1 - Vascular procedure Levels 1-4 Appendi 2 - Quality Standards Appendi 3 - Maps and location of each site within the review Appendi 4 Present Patient Pathways Newly Revised Patient Pathways Appendi 5 - Average Theatre Times and Procedures Appendi 6 - Rehab Amputation Team Appendi 7 - SUS data Appendi 8 - Information Provided by each PCT on Vascular Procedures Commissioned 2009/
4 Chapter 1 Background 1.1 Review of Vascular Services in Lancashire and Cumbria The focus of this review is to improve quality and safety for patients. Evidence based standards have been agreed which seek to ensure the highest standards of quality and patient safety. Implementation of those standards will require a change from the way services are currently provided. This document eplores the compleities of vascular interventions and its clinical interdependencies and sets out options for providing services across the Network. 1.2 The Case for Change The initial impetus for a review of vascular services arises from the unsuccessful business case for an Abdominal Aortic Aneurysm (AAA) Screening Programme within Cumbria and Lancashire. There are around 6,000 deaths each year in England and Wales resulting from ruptured AAAs. 95% of ruptured AAAs are in men over 65 Vascular disease (including death from ruptured AAAs) accounts for 40 per cent of deaths in the UK. Vascular disease is as common as both cancer and heart disease. The Evidence The Multicentre Aneurysm Screening Study (MASS) provided strong evidence for both the clinical benefit and the cost-effectiveness of a screening programme for abdominal aortic aneurysms (AAAs) in men. MASS concluded: The results support the epectation of very few emergency operations, and principally elective operations, being performed following the introduction of a screening programme. For a typical district general hospital, a screening programme would be epected to lead to two additional elective AAA operations per month, and to save 11 AAA-related deaths per year. Implications for Delivery of AAA Services Within Lancashire and Cumbria, the AAA Screening Programme will only be implemented when a full review of present vascular surgical providers has been completed and delivery of surgical repair of screen-detected aneurysms are seen to be being performed with the lowest possible mortality rates and best patient outcomes. Significant reductions in peri-operative deaths have been proven to be achieved through the centralised delivery of AAA repair. (Holt PJ, Poloniecki JD, Hinchliffe RJ, Loftus IM, Thompson MM. Model for the reconfiguration of specialized vascular services. The British journal of surgery 2008; 95(12): ). Both The Vascular Society (VSGBI) and NCEPOD have recently published recommendations around emergency vascular provision. They stated that the best outcomes are achieved in specialist vascular units with dedicated vascular teams available 24 hours a day, seven days a week. (Abdominal Aortic Aneurysm: A Service in Need of Surgery, A report of the National Confidential Enquiry into Patient Outcome and Death, 2005: 11) 4

5 The present configuration of services in Cumbria and Lancashire does not promote the transfer of patients to high-volume centres so that these important advantages are available to them. The advent of screening for abdominal aortic aneurysms adds further importance to this work. Crude Mortality Rates Displayed by Country for AAA Repair: Table 1 shows that the UK has the worst mortality rates. (7% in the UK, 2% in Italy) (The Vascular Society of Great Britain & Ireland. (2007). The provision of emergency vascular services) Table 1 Remodelling vascular services by reducing the number of providers would reduce mortality and morbidity after major vascular surgery by concentrating medical and nursing epertise. 1.3 Important factors that influence patient outcomes Individual surgeons should maintain high volumes of surgery Surgeons that maintain high volumes of vascular surgery achieve mortality rates 2-4% lower than surgeons that perform low volumes of vascular surgery each year. (VSGBI 2009) There is also a clear link between the amount of surgery an individual surgeon does each year and their associated mortality outcomes. Studies have shown the principle reason high volume hospitals achieve better patient outcomes is because the surgeons tend to carry out high volumes of vascular procedures (Birkmeyer, J. D., Stukel, T. A., Siewers, A. E. Goodney, P. P., Wennberg, D. E. & Lucus, F. L. (2003). Surgeon volume and operative mortality in the United States. The New England Journal of Medicine, 349 (22): ) Modern surgical technologies Presently across Lancashire and Cumbria, there is a significant variance in the uptake of minimally invasive vascular surgery. This means that the hospital where the patient has their surgery is a bigger determining factor in deciding the type of surgery they will have rather than their clinical need. 5
6 Some vascular procedures can be done using a modern, minimally invasive surgical method called endovascular surgery. Evidence shows that this type of surgery reduces length of hospital stay, reduces the risk of acquiring a hospital infection and most significantly, reduces surgical mortality by around 3% compared to traditional surgical methods. Vascular surgery should be undertaken by a specialist vascular surgeon. Institutions should perform high volumes of vascular surgery. Hospitals performing high volumes of vascular surgery achieve significantly lower mortality than hospitals performing low volumes. (VSGBI 2009) A wealth of evidence supports the view that patients are less likely to suffer from postoperative strokes or die, when they have their carotid endarterectomy surgery at a hospital that performs a higher annual number of procedures. (Feasby, T. E., Quan, H. & Ghali, W. A. (2002). Hospital and surgeon determinants of carotid endarterectomy outcomes. Archives of Neurology, 59: ) (Holt, P. J. E., Poloniecki, J. D., Loftus, I. M. & Thompson, M. M. (2007). Meta-analysis and systematic review of the relationship between hospital volume and outcome following carotid endarterectomy. European Journal of Vascular and Endovascular Surgery, 33: ) In Lancashire and Cumbria the numbers of vascular procedures are classed as low volume - and mortality and length of stay compare badly to the rest of the UK. 1.4 The Benefits of Centralisation of Vascular Services Central units would perform all elective and emergency arterial surgery Rapid access to diagnostics and interventions forms part of a high quality service. The need for this has been an important driver for centralisation, as it requires around the clock working, which larger units are better placed to provide. The units would be staffed by vascular specialists and would operate 24 hours a day, seven days a week Performing all comple procedures at central units would ensure all patients have their surgery at a high volume hospital by an eperienced vascular specialist, using the latest technology and techniques Centralisation should ensure improved facilities for patient care (dedicated vascular wards), investigation (larger radiology units with 24/7 interventional radiology) and treatment (vascular operating theatres and staff, vascular anaesthetists, improved facilities for endovascular management, better critical care). When centralisation occurs, outpatient clinics and day surgery can continue in the hospitals that no longer have the primary service. The centralisation of vascular services to a small number of large centres is perhaps a radical option to consider but offers a number of potential benefits that are unlikely to be achieved through any other model, including: One or more specialist treatment centre for each vascular screening programme which could provide administrative efficiencies Centralisation of resources, with the potential to reduce overall costs and improve efficiency Dedicated vascular anaesthetic input High volumes of comple procedures per centre. Evidence for some procedures indicates that the more procedures that are carried out the better the outcomes 6
7 Training of junior staff would be facilitated with concentrated high volume work Individual surgeon volumes more likely to be maintained despite the predicted shift away from open surgical techniques towards endovascular technologies Potential cost savings in avoidance of duplication of comple equipment both within and eternal to theatre Provision of comprehensive and sustainable 24/7 vascular radiology services. Benefits for Academia and Research Central units would act as leading centres of research. This would mean greater opportunities for surgeons and specialists who want to pursue a joint career in academia and surgery. It would also help attract junior medical staff who will be the vascular specialists of the future. It is hoped that ongoing research can help define future management and treatment strategies for vascular diseases. 1.5 Impact Centralisation of vascular services to one or more intervention centres within Lancashire and Cumbria with outreach for outpatients and day cases would mean: Patients would potentially need to travel further for their operation, as would their visitors Patients would be treated at a centre carrying out higher volumes of comple work, which is linked to improved outcomes Patients would be treated by a surgeon or interventional radiologist carrying out large volumes of comple work Patients would be able to access the full range of procedures 24/7 Fewer clinical staff overall would be needed. 1.6 Risks There are a number of risks inherent to this approach, including: Potential difficulties include, concerns on the part of hospitals losing vascular surgery and insufficient capacity on a single site to manage the increase in workload and possibly a reluctance of surgeons to move sites. The review has identified a shortage of trained interventional radiologists and, whilst work is underway to develop interventional radiology as a recognized sub-specialty, it is likely to take some years before this position changes. This issue eists even if the recommendations of this review are not followed through Destabilisation of current providers through shifts in activity Management of patients who are too unstable to transfer for eample post partum haemorrhage may be delayed as the patient would either need to be transferred to the intervention centre or the surgeon would have to travel to the DGH Creation of a two-tier service, with patients living further away from large centres failing to access care Negative impact on relationships with other specialties for eample renal and stroke services Impact and cost implication of transferring patients Less contact/dialogue with primary care 7
8 Chapter 2 - Epidemiology 2.1 Impact of Risk Factors - Epidemiological Information 2.2 Age Population - the total population of Cumbria and Lancashire is just over two million and includes si Primary Care Trusts (PCTs) and five Acute Hospital Trusts, some of which link in with other sites to provide their Vascular cover. Cumberland Infirmary (CIC) in Carlisle takes vascular patients from Dumfries and Galloway, which has a population of 148,000. Royal Preston Hospital (RPH) works as part of an emergency 1 in 6 rota to offer emergency cover to Wigan, Bolton and Southport. The combined population of Wigan and Bolton PCTs is over 600,000. (Southport will be part of the Cheshire and Mersey Review) This makes the combined population detailed within this review to 2.7 million The prevalence of vascular disease increases with age. The compleity, outcome and costs of vascular intervention are age-dependant. Average life epectancy continues to rise and this factor alone suggests that demand for vascular services is likely to continue to increase with time. Demographic changes are predicted within the two counties, particularly Cumbria, which is projected to have a greater number of older people than the national average, which in itself predicts an aging population. 2.3 Diabetes Diabetes prevalence almost doubled between 1994 and Vascular disease is the major cause of morbidity in diabetes and the risks of disease progression are higher. It is likely that the great increase in the number of patients with diabetes over the net decade will have the biggest impact on vascular services. Many of these patients present as an emergency, and are at high risk of amputation. Prompt treatment of the infected diabetic foot can minimise the risk of subsequent amputation. The BHF Health Survey for England 2006 suggests that around 1% of men aged 16 to 34 years have diagnosed diabetes compared with 13.5% of those aged 75 and over. In Lancashire diabetes is described as significantly worse than the England average. For Cumbria the rates remain close to the England average. 2.4 Obesity and Diabetes Lack of eercise, poor diet and increasing age are all associated with an increasing incidence of Type 2 diabetes. The epidemic of obesity is likely to have the biggest impact on the prevalence of diabetes in the net decade, and may well cause a dramatic rise. These factors all contribute to the development of hyperlipidaemia and hypertension, both potent risk factors for vascular disease. Childhood obesity has also been linked to the development of diabetes and hypertension in later life. In % of adults were classified as obese; this rose to 24% by (HSE 2007) In Lancashire and Cumbria current levels of obesity in adults and Children are very similar to England s average. 8
9 2.5 Smoking Smoking is a major cause of vascular disease and over 80% of vascular patients are current or e-smokers. Although there was a rapid decline in the proportion of smokers during the 1980s, when 39% of adults smoked, this decline then levelled off in both men and women aged less than 65 years. Smokers are at greater risk of complications from vascular interventions because of cardiac and respiratory co-morbidity and the longer-term success of vascular intervention is reduced in patients who continue to smoke. (HSE 2007) In Lancashire and Cumbria current numbers of smokers is very similar to England s average. 2.6 Target for Reducing Mortality From Cardiovascular Disease Over the last ten years across England there have been decreases in early death rates for heart disease and stroke. In Lancashire early deaths from heart disease and stroke and deaths from smoking are described as significantly worse than the England average. For Cumbria the rates remain close to the England average. Chapter 3 Vascular Procedures 3.1 What are Vascular Services? Vascular surgery treats diseases of the arterial, venous and lymphatic systems. Surgery for venous disease is mostly high volume, low risk, and demand driven work. In contrast, diseases of the arteries are comple, time consuming and epensive to treat. Treatment options for arterial surgery are evolving as new technologies are introduced. Vascular services encompass all of the HRG 3.5 codes as well as a range of interventional radiology procedures that do not fall naturally within current codes. Vascular services can be broadly split into three distinct categories and four levels of compleity. A full eplanation of the vascular procedure level classifications can be found in Appendi 1. Vascular services include the treatment of aneurysm and other abnormal blood vessels, limb ischaemia, carotid artery disease, peripheral and visceral arterial disease, thoracic outlet surgery and venous disease. Surgery can also include vascular access work mainly used for renal patients requiring haemodialysis. Interventional radiology for vascular disease involves a range of minimally invasive imageguided techniques for stenting and repair of vessels. Interventional radiology is a developing specialism and the service offered across Lancashire and Cumbria varies greatly from hospital to hospital. Most sites offer some interventional radiology procedures, but the range of procedures offered and the degree to which interventional radiology is used at each site varies significantly. 9
. This is a major operation and carries some risk.")

10 3.2 Main Procedures to Consider Treatment of Abdominal Aortic Aneurysm Repairs Open Repair The traditional operation involves cutting open the abdomen to replace the aneurysm with an artificial piece of artery (a graft). This is a major operation and carries some risk. Endovascular Repair- EVAR This involves inserting a graft within the aneurysm through small groin incisions using X-rays to guide the graft into place. The advantage of this type of repair is that there is no abdominal surgery. This technique is therefore safer than the traditional operation and the patient spends less time in hospital. Femoropopliteal and Femorodistal Bypass The blocked artery is eposed both above and below the blockage. Normally a vertical incision is made in the groin to epose the common femoral artery. A second incision of similar length is made to epose the artery below the blockage. A tube used to perform the bypass, the bypass tube is joined to the artery at groin level and again to the artery below. 10

11 Carotid Endarterectomy- CEA The carotid artery is opened up and the thickened lining and atheroma which is making the artery narrow is removed. Amputations The vast majority of amputations are performed because the arteries of the legs have become blocked due to atherosclerosis. Most common in diabetics and smokers which causes atherosclerosis (about 30-40% of amputations are performed in patients with diabetes). Chapter 4 Present providers 4.1 Present Provider Landscape The Review process was facilitated by the Cardiac and Stroke Networks in Lancashire and Cumbria and began in September Progress to date includes: Appointment of Vascular Clinical Lead A Project Initiation Document was produced and agreed by the Vascular Clinical Advisory Group The Vascular Project Steering Group was established which were both formed to inform the review process. Both groups met on average every si weeks Full Terms of Reference for both advisory groups were developed An over-arching clinical network was agreed which will continue upon completion of the review with one network covering all centralised sites be that one/two or three sites in total As part of the Vascular Review, each site completed a detailed quality standards questionnaire (modelled on the Quality Standards devised by the West Midlands Vascular Review) detailing the present vascular service provided at each of these sites (Appendi 2) Epidemiological landscape was reviewed Full travel times and population analysis was undertaken of each site presently providing vascular services as well as other sites that presently do not (Appendi 3) Clinical pathways were reviewed by the clinical group and new pathways have been agreed (Appendi 4) Full analysis of average Theatre Times for Vascular Procedures (Appendi 5) Full data analysis of all vascular procedures at each site (Appendi 7) Full data of services commissioned by each PCT( Appendi 8) 11
12 A Vascular Coding Sub-Group was formed to address issues that the review uncovered regarding the coding of vascular procedures - it is envisaged that this group will continue to meet through out the review process A Service Specification was developed and fully ratified by the clinical group Stakeholder and GP engagement is underway Public and patient engagement is underway Local authority and relevant stakeholders have been consulted. Vascular Surgical Services are presently provided within the Lancashire and Cumbria on five sites and formal working networks are already in place, meaning that an out of hours service is available to the full population- detailed as below. There are a total of seven sites within the review they are: Royal Preston Hospital Lancashire Teaching Hospitals NHS Foundation Trust (LTHTR) Royal Lancaster Infirmary University Hospitals of Morecambe Bay NHS Trust (UHMBT) Cumberland Infirmary North Cumbria University Hospitals NHS Trust (NCUH) Royal Blackburn Infirmary East Lancashire Hospitals NHS Trust (ELHT) Royal Bolton Hospital Royal Bolton Hospitals NHS Foundation Trust (RBHT) Blackpool Victoria Hospital Blackpool Teaching Hospitals NHS Foundation Trust (BTHT) Royal Albert Edward Infirmary Wrightington, Wigan & Leigh NHS Foundation Trust (WWLT) Within the process it became apparent that network arrangements were already in place between the Blackpool and Lancaster sites, as well as the Preston site networking with Wigan, Bolton and Southport. The Wigan and Bolton sites became part of our review process and Southport part of the Cheshire and Mersey review. There is an agreement that patients from Dumfries and Galloway will be included within this review as described below. Present Provider Arrangements This information was formulated from the Quality Standards Questionnaire which was completed by the five sites presently providing Vascular Services Presently Royal Preston Hospital is part of the Northwest Emergency Vascular Network which also includes Wigan, Bolton and Southport Hospitals and means in emergencies the patient would be transferred to whichever appropriate site was on call. Arrangements at Cumberland Infirmary (CIC) - the present model to cover emergencies in CIC includes two surgeons from Dumfries and Galloway, for this model these surgeons travel to work at CIC and all patients are brought to this one site. This Solway Basin Network was established in 1999 and was formed to provide high quality vascular services for the population of North Cumbria and parts of South West Scotland, due to the geographical location of North Cumbria and Dumfries and Galloway there are essential clinical links, providing emergency and more recently elective services to a population of circa 400,000. It has now also been agreed that all elective aortic treatment will be undertaken at CIC. Discussions have taken place between NHS Dumfries & Galloway (D&G) and NCUH to agree joint arrangements, including the detail of patient pathways, shared care between D&G and NCUH clinicians, funding arrangements, etc. NCUH is undertaking internal redesign of clinical services to provide the theatre and bed capacity for D&G patients, as well as patients from west Cumbria. (From April 2011 this activity will be ~ 15 cases per annum, growing to ~30 p.a. following full implementation of the AAA screening programme). 12
13 Blackpool Victoria Hospital has a formal partnership to cover emergencies with Royal Lancaster Infirmary. Patients presenting acutely to Blackpool are referred and transferred when there is not a Blackpool Consultant available. Over the last three years the two trusts have eplored the possibilities of formalising this combined working arrangement, convened a Joint Vascular Steering Group and presented an options appraisal to the Chief Eecutive Officers of both trusts. An agreed clinical model has since been developed with a view to the vascular service working as one combined unit across both trust sites, covering the entire population base of 700,000. Details on all the sites presently providing Vascular Services Below is a sample map of one of the sites included in the review Royal Blackburn Hospital (colour coded for the three travel time zones). All the site maps are shown in Appendi 3. They show the travel times for 45, 60 and 90 minutes from each site these maps with the isochrones are important as they not only show travelling distances achievable to each site but also the population residing within these zones as detailed in Section 4.3. (The maps are formed using advance travel analysis provided by Navteq 2006 and in the appendi all maps show the location and travel times to all of the Acute Trusts included in the Review). 4.2 Current Patient Flows Detailed patient flows and cross site networking is shown in the flow charts on page 14 and 15. The numbers of beds/surgeons and major arterial procedures presently undertaken at each site is shown in the boes below for each site within the Review. 13
14 Current Patient flows - (North) NCUH/UHMBT/BTHT Data-average from last 3 yrs PCT Population 148,000 Dumfries & Galloway 2 Vasc/Gen Surgeons (Elective AAA contract ~15 per year from 04/2011) Emergency Whitehaven 2 Vasc/General Surgeons CARLISLE 2 Vasc/General Surgeons 2 IR Rehab 10 Ward Beds 6 ICU 2 HDU Level 3 Procedures Carotid 30 EVAR 8 AAA Repair ICU 2 HDU Population Cumbria PCT Barrow Kendal 3 ICU 3 HDU BLACKPOOL 2 FT Vasc Surgeons 2 IR Emergency LANCASTER 3 Vasc/Gen Surgeons 2 FT Vasc Surgeons 2 IR 20 Ward Beds 6 ICU 2 HDU Level 3 Procedures Carotid 55 EVAR 16 AAA Repair Ward Beds 8 ICU 4 HDU Population Blackpool PCT 156,889 Level 3 Procedures Carotid 53 EVAR 10 AAA Repair- 8 Population North Lancs PCT 338,854 14
15 Current Patient Flows - (South) LTHTR- (Wigan and Bolton)/ELHT Chorley Population Central Lancs PCT 469,219 4 HDU PRESTON 3 Vasc Surgeons 3 IR Rehab 10 Ward Beds 14 ICU 10 HDU Level 3 procedures Carotid 185 EVAR 32 AAA Repair-15 Emergency Emergency Emergency Southport 2 Surgeons 1 IR Wigan- 2 Surgeons / 2 IR Level 3 procedures Carotid- 27 EVAR- 6 AAA Repair- 12 Bolton- 2 Surgeons / 2 IR Level 3 procedures Carotid- 24 EVAR- 6 AAA Repair- 20 Population East Lancs PCT 388,769 Burnley 4 HDU Level 3 procedures Carotid- 99 EVAR- 13 AAA Repair- 27 BLACKBURN 3 FT Vasc Surgeons 1 Vasc/ General Surgeon 3 IR Population Blackburn with Darwen PCT 166, Ward Beds 14 ICU 12 HDU 15
16 4.3 Information on all Sites Currently Providing Vascular Services The full details of services, population coverage and travel times to each site are shown in the tables below. It is important to be mindful not only of numbers of present and projected vascular throughput but also local demographics such as; age, ethnicity and the geography. Whilst many parts of Lancashire benefit from easy access to the motorway network, travel across large rural areas of Lancashire and Cumbria can cause difficulties in relation to equitable access to services. ELHT in Blackburn Population ELHT serves population of Blackburn with Darwen PCT 166,998 and East Lancs PCT 388,769. Total 555,767 Population within the 45 minute radius - 2,664,134 Population within the 60 minute radius - 5,002,465 Population within the 90 minute radius - 8,523,792 Travel times from Royal Blackburn Hospital - within 45, 60 and 90 minutes all sites - Preston, Blackpool, Chorley, Burnley, Bolton, and Wigan can all be reached. Carlisle cannot. There is a high Asian and British Asian population in this area - (these being Blackburn (with 23% BME), Pendle (16.1%) - England average 5.7%) Numbers of Surgeons and Interventional Radiologists Surgeons- 3 FT Vasc /1 vasc /general - Total 4 Interventional Radiologist Total 3 Beds - Generic ICU beds 14/HDU beds 12/4 HDU beds - Burnley site/ward beds - 12 Cumberland Infirmary, Carlisle NCUH, work in partnership with 2 Consultants from Dumfries and Galloway to provide on call cover for both areas. Population NCUH serves population of Cumbria PCT 519,195 and covers Dumfries and Galloway PCT 148,000 (Solway Basin network). Total 667,195 Population within the 45 minute radius - 173,231 Population within the 60 minute radius - 224,553 Population within the 90 minute radius - 586,228 Cumbria is England's second largest county and has the third highest levels of population sparsity. Parts of West Cumbria and Barrow show a poorer than average performance across a range of health indices. The Barrow district has a life epectancy significantly lower than the national average and that of the North West. 16
17 Travel times from Carlisle - No other hospital is within the 45 or 60 minute radius. Lancaster can be reached within the 90 minute radius. Cumbria s geography can cause difficulties in relation to providing equitable access to services Numbers of Surgeons and Interventional Radiologists Surgeons - 4 vasc/general - Total 4 (2 Cumberland Infirmary, 2 West Cumberland Hospital) Interventional Radiologist - Total 2 Beds - Generic ICU beds 6/HDU beds 2/Ward beds -10 BTHT in Blackpool Presently work in partnership with UHMBT to provide on call cover. Population BTHT serves population of Blackpool PCT parts of North Lancashire PCT, and parts of Cumbria PCT (due to present arrangement with UHMBT) Population within the 45 minute radius - 919,229 Population within the 60 minute radius 2,052,006 Population within the 90 minute radius 5,872,354 Travel times from Blackpool - Within 45, 60 and 90 minutes Preston, Chorley, Blackburn, Wigan, Bolton and Lancaster can all be reached, Carlisle cannot. Numbers of Surgeons and Interventional Radiologists Surgeons- 2 FT vascular - Total 2 Interventional Radiologist - Total 2 Beds - Generic ICU beds 8/HDU beds 4/Ward beds - up to 17 UHMBT in Lancaster Population UHMBT serves population of North Lancashire PCT 338,854 as well as parts of Blackpool PCT and parts of Cumbria PCT Population within the 45 minute radius - 731,863 Population within the 60 minute radius - 1,868,371 Population within the 90 minute radius - 5,823,080 Travel times from Lancaster - Within 45 and 60 minutes Preston, Chorley, Blackburn, Blackpool, Kendal. Carlisle can be reached within 90 mins Presently work in partnership with BTH to provide on call cover. 17
18 Numbers of Surgeons and Interventional Radiologists Surgeons - 2 FT vasc, 3 Vasc /gen -Total 5. Interventional Radiologist - Total 2 Beds - Generic ICU beds 6/HDU beds 2/Ward beds - up to 20 LTHTR in Preston Presently LTHTR, work as part of North West Emergency Vascular Network to provide on call cover (other sites in Network are Wigan, Bolton, and Southport). LTHTR serves population of Central Lancashire PCT (population 469,219) as well as Ashton, Wigan and Leigh PCT, Bolton PCT and Sefton PCT as part of the NW network. High Asian and British Asian population in this area -Preston (15.5%) - England average 5.7%. Population Population within the 45 minute radius - 2, 245,016 Population within the 60 minute radius - 2,257,066 Population within the 90 minute radius- data not available Travel times from Preston - Within 45, 60 and 90 minutes all other sites in Lancashire and Cumbria (including Chorley, Blackburn, Blackpool, Lancaster, Burnley, Wigan, Bolton, and Southport) can be reached, Carlisle cannot. Numbers of Surgeons and Interventional Radiologists Surgeons- 3 FT vascular surgeons. Interventional Radiologist - Total 3 Beds - Generic ICU beds 10/HDU beds 14 (Chorley Site 4 HDU/Ward beds - 10) Cross Boundary Indications Wigan and Bolton are currently part of the North West Emergency Vascular Network and currently link in with Lancashire Teaching Hospitals they will be considered as part of this review as will Dumfries and Galloway who have a formal link with North Cumbria University Hospitals. Wigan Population Serves the population of Ashton Wigan and Leigh PCT- 318,567 Population within the 45 minute radius - 3,771,969 Population within the 60 minute radius - 5,886,065 Population within the 90 minute radius- data not available 18
19 Travel times from Wigan - Within 45 and 60 minutes all other sites in Lancashire and Cumbria (Including Chorley, Blackburn, Blackpool, Lancaster, Burnley, Wigan, Bolton, and Southport) can be reached, Carlisle cannot. Numbers of Surgeons and Interventional Radiologists Surgeons- 2 Interventional Radiologist -2 Bolton Population Serves the population of Bolton PCT - 290,715 Population within the 45 minute radius 4,183,093 Population within the 60 minute radius - 6,480,060 Population within the 90 minute radius - data not available Travel times from Bolton- Within 45 and 60 minutes all other sites in Lancashire and Cumbria (including Chorley, Blackburn, Blackpool, Lancaster, Burnley, Wigan, Bolton, and Southport) can be reached, Carlisle cannot. Numbers of Surgeons and Interventional Radiologists Surgeons- 2 Interventional Radiologist -2 Dumfries and Galloway Population Serves the population of Dumfries and Galloway PCT- 148,000 but cover a population circa 400,000. Dumfries and Galloway Hospital has an agreement with NCUH to cover emergency AAA Repairs. From April 2011 this will also include elective repairs - activity will be ~15 cases per annum, growing to ~30 per annum following full implementation of the AAA screening programme. Numbers of Surgeons and Interventional Radiologists Surgeons - 2 Interventional Radiologist
20 A full travel time and population analysis was also undertaken of other sites that presently do not provide full vascular services- these sites are: Chorley and South Ribble District Hospital based in Chorley Furness General Hospital based in Barrow in Furness West Cumberland Hospital based in Whitehaven Westmorland General Hospital based in Kendal Burnley District General Hospital based in Burnley See Appendi 3 for the maps of these sites and 45 / 60 and 90 min travelling distances of these five sites. Chapter 5 Length of Stay 5.1 Reducing Length of Hospital Stay by Centralisation The most recent VASCUNET data shows the UK lagging behind its European and international counterparts. The UK has the longest length of stay in Europe for elective AAA surgery. (VASCUNET Second Annual Vascular Surgery Database Report 2008) Also, length of stay in England has been shown to be significantly longer at hospitals performing lower volumes of elective AAA repairs compared with those performing high volumes. Length of stay has also been studied in relation to the type of procedure performed. VASCUNET data demonstrated that Endovascular Aortic Repair (EVAR) required significantly shorter post-operative stays in hospital compared with open repairs. (VASCUNET Second Annual Vascular Surgery Database Report 2008) The length of stay for patients following vascular surgery varies across Lancashire and Cumbria. It is likely that length of stay is higher than it could be due to the relatively low volume of EVAR undertaken. The length of stay in Lancashire and Cumbria could be reduced by performing vascular surgery at specialist centres that are more likely to adopt better surgical technologies, which are proven to reduce lengths of stay. 5.2 Length of Hospital Stay It has been found that, in addition to lower mortality rates, higher-volume hospitals also have a reduced length of hospital stay. Furthermore, patients are more likely to be discharged home, as opposed to nursing care, from higher-volume hospitals and less likely to be readmitted as an emergency. It may be possible to off set costs involved in the centralisation of Vascular Services by reducing length of stay hence cost savings. 20
21 5.3 Current Average Length of Stay in the Lancashire and Cumbria Network The graph shows the average length of stay for all sites within our review for the main Vascular Procedures. Source- SUS data (outliers taken out) (Average length of stay can be affected by available Primary care resources to discharge patients out to and a longer length of stay in no way reflects on the care provided at a specific site). 40 Average Length of Stay Trust Average C&L Varicose Veins Average C&L Bypass Average C&L Renal Average C&L Amputations Average 0 Varicose Veins Bypass Renal Am putations Varicose Veins Bypass Renal Am putations Varicose Veins Bypass Renal Am putations Varicose Veins Bypass Renal Am putations Varicose Veins Bypass Renal Am putations Varicose Veins Bypass Renal Am putations Varicose Veins Bypass Renal Am putations BLACKPOOL, EAST LANCASHIRE FYLDE AND WYRE HOSPITALS HOSPITALS LANCASHIRE TEACHING HOSPITALS MORECAMBE BAY HOSPITALS NORTH CUMBRIA ACUTE BOLTON WWL Procedures - Average Length of Stay for Lancashire and Cumbria AAA Repair 14 days (range days) EVAR 7 days (range 3 10 days) Carotid 5 days (range 3 7 days) Amputations 30 days (range days) Within our Network area Wigan and Blackpool has the lowest length of stay (consistently below the area average for Carotid, AAA and EVAR) 21
22 Chapter 6 Number of Specialists Required Population Coverage Required The Population of Lancashire and Cumbria including the populations of Dumfries and Galloway, Bolton and Wigan. Primary Care Trust Population Blackburn with Darwen 166,998 Blackpool 156,889 Central Lancashire 469,219 East Lancashire 388,769 North Lancashire 338,854 Cumbria 519,195 (Total 2,039,924) Wigan 318,567 Bolton 290,715 Dumfries and Galloway 148,000 Total population 2,797,206 Data from a survey by the VSGBI in 2009 suggested that one vascular surgeon is needed per 150,000 population, with an equivalent number of interventional radiologists. However The Vascular Clinical Advisory Group advocates 1 per 125,000 as this equates to a one in eight rota for a site covering 1 million population. 6.1 Numbers of Surgeons required for the Population Many patients with vascular disease present as an emergency, and in the past have often been managed by a general surgeon. This is no longer acceptable. Every patient with a vascular emergency should epect to be treated by a trained vascular specialist (VSGBI 2009). Across Lancashire and Cumbria we presently have 19 vascular surgeons, however only eight are full time vascular surgeons the rest are part Vascular and part General. These figures do not include surgeons from Wigan, Bolton or the two surgeons from Dumfries and Galloway that presently networks with NCUH to include these surgeons = 25 in total. 6.2 Numbers of Interventional Radiologists Interventional radiology is recognised as a discipline within radiology, although not all interventional radiologists work in the vascular field. Vascular surgical specialists work closely with their radiology colleagues. Currently there are 12 interventional radiologists working within the five sites in Lancashire and Cumbria and a further three including the Wigan and Bolton sites = 16 in total. 6.3 Vascular Specialists There is a growing consensus that the vascular specialist of the future will have operative and interventional skills, rather than being principally a surgeon. The Vascular Society has put forward proposals to address the training needs of surgeons who wish to become a vascular specialist, to ensure that this is accommodated within MMC (Modernising Medical Careers) arrangements. In March 2007, the Royal College of Radiologists and the Royal Colleges of Surgeons of England, Edinburgh and Glasgow produced a joint statement aimed at addressing the needs for provision of interventional radiology and vascular surgery and benefiting the development of both specialties. 22
23 The paper describes the concept of a vascular specialist as an umbrella term, encompassing a variety of clinicians with a shared set of core eperience related to vascular disease based on demonstrating competence in the relevant knowledge, skills and professional attitudes. With both vascular surgeons and interventional radiologists trained in interventional radiology techniques, fewer patients would require open surgery for vascular disease, thus freeing up theatre capacity and reducing patient length of stays. 6.4 Vascular Nurse Specialists The Vascular Nurse Specialists contribute to both inpatient and outpatient care. They have a key role to play in liaising between team members. The Vascular Nurse Specialist usually provides independent care and advice using agreed protocols. Nurse specialists may provide independent care to patients through lifestyle advice clinics, claudication clinics, leg ulcer clinics and diabetic foot clinics. They play an important role in vascular research and audit and are involved in the training and education of both community and hospital nursing staff. Each of the five sites within Lancashire and Cumbria presently employ one or more Vascular Nurse Specialist. Chapter 7 Links with Other Specialties 7.1 Critical Links Specialties Supporting a Vascular Service In order to provide Lancashire and Cumbria residents with a world-class service, patients undergoing specialist vascular surgery should also have access to interventional cardiology, interventional radiology, a specialist intensive care unit, specialist vascular anaesthetists, diabetic and neurology specialists, cardiac surgery and a step down intensive care facility. It is also desirable that patients have access to a renal unit that includes dialysis facilities. Currently in Lancashire and Cumbria, the services supporting vascular surgery vary from hospital to hospital. Arterial surgery is major surgery that requires the very best services available onsite to support it. It is important, to consider other services within the review as it is members of the vascular MDT who carry out this work. 7.2 The Impact on Major Trauma and Stroke Vascular Surgery cannot be seen in isolation, it has close links with major trauma and stroke services. Trauma There is presently a review of Trauma Services taking place in Lancashire and Cumbria. The location of major trauma centres in Cumbria and Lancashire should be a key factor in the decision-making process regarding vascular service delivery. In the future it is likely that patients with a major injury will be taken by ambulance to the nearest trauma centre for specialist treatment, in many of these instances, patients will need access to a specialist emergency vascular service. Stroke Acute stroke services are provided in stroke units which are based at all sites. Clear pathways will need to be established so that patients can have timely access to Carotid Endarterectomy (CEA) surgery which would only be available at the intervention centres. 23
24 The future provision of vascular services in Cumbria and Lancashire needs to ensure that patients who have a major injury or a stroke receive the quality of care they need. It is likely that in order to achieve this, the format of where and how vascular services are provided will need to consider the changes to major trauma and stroke services in Cumbria and Lancashire. 7.3 Other Service Considerations It is important to consider other services within the review as it is members of the vascular MDT who carry out this work, i.e. vascular surgeons and vascular interventional radiologists. Vascular cover is needed 24/7 for patients undergoing surgery for stroke/patients undergoing limb salvage surgery for diabetes/renal inpatient units/vascular access. Renal Access The best form of access for chronic haemodialysis is an autogenous arteriovenous fistula. This is usually performed by vascular surgeons. The majority of this work is planned, but there are also urgent cases where patients are failing dialysis access. Most of these can be treated within a few days, by either surgical or interventional radiology techniques. It has been estimated that one dedicated vascular access operating list is necessary for each 120 patients on dialysis (including peritoneal dialysis) assuming 3-4 patients can be operated upon per list. Most patients can be operated on under local anaesthesia and many of the operations can be performed as a day case procedure. In March 2010 the total number of patients across Cumbria and Lancashire on dialysis treatment was this does not include Wigan and Bolton patients. In addition there is a need for up to two interventional radiology sessions per week per 100 patients on dialysis for preoperative imaging, postoperative surveillance and for percutaneous angioplasty or thrombectomy of failing or thrombosed AV fistulae and grafts. The VSGBI 2009 epects 281 procedures per million population - this equates to 756 vascular access procedures per year for our population. Diabetes Diabetic patients have a high risk of peripheral arterial disease. Some patients can be managed in primary care; a minority require interventional treatment, either with interventional radiology or surgery. For some patients, disease may progress to critical limb ischaemia, which can lead to amputation. Early intervention and opinion of vascular surgeons can significantly reduce the number of amputations carried out. Patients with diabetes should have local access to a specialised foot clinic, with input from vascular surgeons. 7.4 Amputations - Amputee Rehabilitation in a Centralised Unit Leg amputation is currently defined as amputation above, below and through the knee. A recent aim of the Vascular Society s Quality Improvement Framework is to raise the profile of leg amputation, with the target of reducing peri-operative mortality below 5%. As with other vascular procedures evidence shows better outcomes and reduced length of stay from centres that perform a higher number of procedures. 24
25 A centralised unit for vascular services and thus amputation surgery would provide a significant opportunity for the post operative and early rehabilitation of amputees to be combined into a central location, concentrating skill levels and patient numbers; economies of scale. Currently no unit has enough amputees to warrant a ward or partly dedicated for amputee rehabilitation where intense rehabilitation is engaged by patients with an amputee rehabilitation team. The amputee rehabilitation team would be engaged with the patient as soon as amputation surgery has been proposed or as soon after emergency surgery as is practically possible, i.e. the same working day or the net working day. The amputee would come under shared care between the treating vascular surgeon and the rehabilitation physician. Appendi 6. Chapter 8 Workload Requirements 8.1 Activity and Length of Stay Assessment The Chart below shows the main Vascular and Arterial Procedures yearly averages across all sites including length of stay. This data has been taken from Hospital Episode Statistics (HES) and looks at the last three financial years (07/08, 08/09 and 09/10). Our etracted data is from Q HRG s (HRG version 3.5). Procedure Average Total Average Length Bed Days Yearly Activity of Stay in L&C Open AAA EVAR Carotid Renal artery Amputations Peripheral Bypass Total / Beds **Please note: The above table shows only the main vascular procedures and is by no means an ehaustive list - it is only intended as a guide and only shows the very minimum requirement that would be needed. The VSGBI (2009) note that based on current eperience and depending on local case-mi, a population of 500,000 will require beds on a dedicated vascular ward, ecluding rehabilitation, short stay, day case and ITU/HDU beds. Using this equation the population of Lancashire and Cumbria would require between vascular in patient beds. This equates to about 3-5 vascular wards. Our present capacity is only for 69 vascular ward beds. (The beds at Bolton and Wigan sites are general with none specifically designated for vascular so are not included within this 69). For ITU and HDU patients, the VSGBI 2009 recommends one vascular ITU and one HDU bed per 500,000 population. For our region that equates to 5-6 dedicated vascular HDU 25
26 and 5-6 dedicated vascular ITU beds across Lancashire and Cumbria. Presently across our region, there are not any HDU/ICU beds dedicated to vascular patients. It is important to be aware of any other specialties based at each site may also require critical care beds and this needs to be considered when deciding the placement of the Intervention Centres. 8.2 Day Case and GP Referral It is the view of the Vascular Clinical Advisory Group that all Day Cases continue in the DGH as is the present arrangement and only procedures that require an inpatient stay should be referred to the intervention centre. GP Referral GPs would continue to refer all vascular patients to their local hospital in the same way as they do now. Patients whose local hospital is also a central unit would continue to be referred to that hospital by their GP. The hospital would continue to act as their local hospital, meaning certain patients with venous, lymphatic and arterial disease would be referred directly to the central unit for treatment. Patients presenting at any other local hospital who need an elective arterial procedure would have most of their pre-surgery investigation at that local hospital before being transferred to a central unit for treatment. All patients would receive the same high quality standards of service regardless of whether they are transferred from a local hospital to the nearest central unit, or referred directly to the central unit by their GP. 8.3 Procedure Volume Requirements It is well established that a strong relationship eists between higher annual volume of procedures and lower mortality for elective and emergency endovascular aneurysm repair, mirroring similar robust relationships between volume and outcome in open AAA repair. In conjunction with the development of aneurysm screening programmes these highlight the need for regionalisation of AAA service provision to high-volume centres offering a full range of vascular services including advanced endovascular intervention. The same evidence supports centralisation for Carotid Endarterectomy and amputation. (VSGBI 2009) Minimum Recommended Number of Procedures per site Figures below from other Vascular Service Reviews Annual volume Source AAA CE Yorkshire &Humber Literature review West Midlands >20 >30 Vascular Society guidance London >100 >50 Literature review NW EVAR guidance Minimum of Not covered Holt et al EVAR equates to AAA total procedures in this document Leapfrog group >50 >100 Literature review 26
27 8.4 Current Activity across the Network Abdominal Aortic Aneurysm Repair The total numbers of all emergency and elective Abdominal Aortic Aneurysm repairs the past three years averages at 225 procedures per annum for the whole of Review area including Wigan and Bolton. (Please note the numbers of repairs is epected to increase when AAA screening is introduced) Of the total number of 225, 140 are open AAA repairs (101 open elective and 39 open non elective). Modelling of AAA services has highlighted the significant reduction in mortality that could be achieved in England through regionalisation of these procedures to highvolume centres. Minimum volume criteria of 50 elective AAA cases per annum should be set to ensure safe practice. (Holt PJ, Poloniecki JD, Gerrard D et al). Meta-analysis and systematic review of the relationship between volume and outcome in abdominal aortic aneurysm surgery. Br J Surg 2007; 94: ). EVAR The total numbers of all emergency and elective EVAR procedures for the past three years averages at 85 procedures per annum for the whole of Review area including Wigan and Bolton. A strong relationship has been shown in favour of hospitals that perform EVAR at high annual volumes. Despite the evidence showing EVAR has lower mortality rates and significantly shorter hospitals stays compared with traditional open surgery. Presently in our area only 85 of aneurysm repairs per year are currently by EVAR (79 elective, 6 non elective). This represents only 38% of the total numbers of repairs completed by Endovascular repair. An EVAR unit should epect to serve a population that will generate a minimum of EVAR procedures annually. It is generally accepted that between 50% and 80% of all AAA procedures should be EVAR. (Holt, P E., Poloniecki, J. D., Khalid, U., Hinchcliffe, R. J., Loftus, I. M. & Thompson, M. M. (2009). Effect of endovascular aneurysm repair on the volume outcome relationship in aneurysm repair. Circulation, published online Sept ) Carotid Endarterectomy- (CEA) The total number of all emergency and elective Carotid procedures for the past three years averages at 472 procedures per annum for the whole of Review area including Wigan and Bolton. Minimum Numbers of Procedures recommended per site is 35 per year. Statistical modelling of the volume-outcome effect for carotid endarterectomy for 10 years of a statewide database. Griswold, M.E., Chang, D.C., Perler, A.P. 59:12, The Vascular Clinical Advisory Group has agreed a minimum of 35 per site Presently there are 472 Carotid Procedures on average per year within the review area. (385 elective, 87 non elective). 27
28 8.5 Figures Based on Minimum Population The minimum population for an independent vascular unit is 800,000. Each emergency vascular service should employ a minimum of 1 WTE vascular surgical specialist per 150,000 population and should serve a minimum population of 800,000 as a whole. (VSGBI 2009) (Although the Vascular Clinical Advisory Group informing the review is recommending 1 per 125,000) There is no data recommending the maimum patient coverage. Including the populations of Wigan and Bolton takes the population to 2,797,206 which would require a minimum of 19 vascular surgeons and 19 interventional radiologists. However, to cover on call rotas, the review recommends 22 of each (as described in Chapter 9) To include the vascular surgeons and interventional radiologists currently available within all these sites would give us a present total of 25 surgeons and 16 interventional radiologists This again highlights a shortfall of interventional radiologists 8.6 Required Theatre Capacity - Appendi 4 Average Theatre Times for Main Vascular and Arterial Procedures (including anaesthetic time). Please note: The table shows only the main vascular procedures and is by no means an ehaustive list- it is only intended as a guide and only shows the very minimum requirement that would be needed. Chapter 9 Proposed Models 9.1 Recommendations of the Review Patient Pathways Reconfiguration of vascular services required a review of current referral pathways and patterns, to ensure the provision of comprehensive vascular care to the local population. A full pathway review has been completed as part of this review process. See Appendi 3 This shows the current pathway and then the new pathway agreed by the Clinical Advisory Group, all the pathways looked at primary prevention through to after care and end of life if appropriate. Pathways included for: Emergency AAA Elective AAA Carotid Stenosis Ischaemic legs Varicose Veins Leg ulcers Vascular Access Please note that the pathway for Vascular Access remains under review and will hopefully be complete by the end of this Vascular Reconfiguration process. 28



29 9.2 Proposals and Network Formation Proposed structure of the vascular clinical model The Vascular Clinical Advisory Group membership included a range of clinicians from across all the sites involved in the review. Its aim was to offer best clinical advice on the provision of safe, high quality evidence based services for vascular patients to the Lancashire and Cumbria Vascular Services Review. A number of factors were considered to determine the optimal number of central units to provide a high quality, safe and equitable service. Factors considered were: Minimal numbers of procedures needed at each site, and current and future volume projections of arterial procedures Number of surgeons Co-dependencies Geography of Lancashire and especially Cumbria The ability to maintain surgical rotas in line with all VSGBI 2009 recommendations. Proposed structure The central Unit would deal with all vascular inpatient activity and all other vascular procedures and Day Case would continue in the DGHs. 29
30 9.3 Proposals Made by the Vascular Clinical Advisory Group Numbers of procedures per site Below is the agreed Minimum number procedures per site (these are the Minimum Recommendations numbers set out by the VSGBI 2009 and agreed by the Vascular Clinical Advisory Group) to maintain highest quality standards and patient outcomes Minimum Numbers agreed for Lancashire and Cumbria Minimum of AAA Procedures - minimum 50 per site Minimum number of EVAR Procedures - minimum per site Minimum number of Carotid Procedures -minimum 35 per site VSGBI 2009, highlights that on average eight AAA procedures are generated per year per 100,000 population and an average of 8.2 Carotid procedures per year per 100,000 population. (Our data averages at 8.3 AAA procedures and 17 Carotid procedures per 100,000)* *Total Population Coverage - 2, (including the population of Bolton and Wigan PCTs). 9.4 Formation of Vascular Network The proposed model will operate as an effective cohesive system, comprising of centralised vascular units across Lancashire and Cumbria, so that the workload, access to beds and training etc can be shared. Each unit should work in partnership to provide a comprehensive vascular service for a defined local population. The central vascular units would be the source of ecellence for intervention ensuring that standards of clinical and non-clinical governance are robust and ensure vascular services would be delivered consistently across the network. 30
31 Proposed Model Options One and Two OPTION ONE is for two centres in total This option means ONE Intervention Centre in the North and ONE in the South of the Network area Figures for ONE proposed northern centre Minimum Number of Procedures It is envisaged that the intervention centre in the North of the network will cover a population of 700,000 using our current figures from the network area covering a population of 700,000 would generate on average 58 AAA repairs per year and 122 Carotid procedures per year. This is higher than the minimum procedure requirements and would make this a viable option. **Theatre Requirements (This needs further investigation- see appendi 5 shows average theatre times from ELHT and UHMBT). It is estimated that 2-3 vascular theatres would be required for this option. Emergency access needs to be considered. Numbers of Beds Needed According to VSGBI (2009) standards, to cover the population of 700,000 would require designated ward beds and 1-2 ICU and 1-2 HDU beds. (The number of required ICU/HDU beds may reduce once the NAASP is underway and the number of ruptured aneurysms reduces). The Carlisle site presently has (up to) 10 designated vascular beds and no designated Critical Care beds. A further ward beds and 2-4 critical care beds would be required. Numbers of Surgeons and Interventional Radiologists needed The VSGBI (2009) recommend one surgeon and one interventional radiologist per 150,000 population but also notes that Vascular on call rotas should be no more onerous than 1 in 6, therefore this site would need a minimum of si surgeons and si Interventional Radiologists. 31
32 Figures for ONE Intervention Centre in the South of the Network area Minimum Number of Procedures Having only one Intervention Centre in the South of the Network would cover a population of just over two million. Using our current figures from the network an intervention centre covering a population of two million would generate on average 166 AAA repairs per year and 349 Carotid procedures per year. **Theatre Requirements (This needs further investigation- see Appendi 5 shows average theatre times from ELHT and UHMBT). It is estimated 4-6 vascular theatres would be required at each site for this option. Emergency access needs to be considered. Numbers of Beds needed at each site According to VSGBI (2009) standards, to cover the population of 2 million would require designated ward beds and 4 ICU and 4HDU beds. (The number of required ICU/HDU beds may reduce once the NAAASP is underway and the number of ruptured aneurysms reduces). Numbers of Surgeons and Interventional Radiologists needed The VSGBI (2009) recognises that centres dealing with populations in ecess of 1 million people will have to deal with higher volumes of emergency cases and in such cases the emergency rota should be no more onerous than 1 in 8. The VSGBI 2009 recommends there should be one interventional radiologist and one vascular surgeon per 150,000 - however the Vascular Clinical Advisory Group has agreed one per 125,000, this is in line with concurrent reviews, so for a population of two million this equates to of each needed to cover this population number. The whole network area presently has 25 vascular surgeons in total and 12 interventional radiologists in total. A minimum of si of surgeons and si interventional radiologists would be required in the centre in the North of the network leaving a shortfall of 8-10 IRs (for the two site option). There is a National shortage of trained interventional radiologists and, whilst work is underway to develop interventional radiology as a recognized sub-specialty, it is likely to take some years before this position changes. An obvious solution is training vascular surgeons to become vascular specialists encompassing IR skills. 32
33 Views of Vascular Clinical Advisory Group for Lancashire and Cumbria. Assessment of the two site model was not seen as a viable option by Vascular Clinical Advisory Group, (Feb 2011) the advisory group dismissed the two site option and recommended the proposal of the 3 site option as set out below. The recommendation was that one site will be in the North of the region due to geography and travelling distances and two sites will be based in the South of the network area. It was felt two sites were needed in the South of the network as the population coverage would be over two million. OPTION TWO is for three centres in total This option is for ONE Intervention Centre in the North of the Network area and TWO Intervention Centres in the South of the Network area Figures for one proposed Northern Centre (All figures for a Northern centre remain unchanged from option one - see above - they remain unchanged due to the geography and travelling times) Figures for the TWO proposed sites in the South Minimum Number of Procedures The two intervention centres in the South of the network if equally split would cover a population of just over one million each. Using our current figures from the network area each intervention centre covering a population of one million would generate on average 83 AAA repairs per year and 174 Carotid procedures per year. This is higher than the minimum procedure requirements and would make this a viable option. Numbers of Beds needed at each site According to VSGBI (2009) standards, to cover the population of one million would require designated ward beds and two ICU and two HDU beds. (The number of required ICU/HDU beds may reduce once the NAASP is underway and the number of ruptured aneurysms reduces). **Theatre Requirements (This needs further investigation- see appendi 5 shows average theatre times from ELHT and UHMBT). It is estimated four vascular theatres would be required at each site for this option. Emergency access needs to be considered. Numbers of Surgeons and Interventional Radiologists needed The VSGBI (2009) recognises that centres dealing with populations in ecess of one million 33
34 people will have to deal with higher volumes of emergency cases and in such cases the emergency rota should be no more onerous than 1 in 8 therefore each Southern site would need a minimum of eight surgeons and eight interventional radiologists. This three centred approach requires a total of 22 surgeons and 22 radiologists. As highlighted in Figure 8.5, the whole network population as it stands would require 19 vascular surgeons and 19 interventional radiologists, however to cover three on call rotas of (1) 1 in 6 and (2) 1 in 8, requires a total of 22 surgeons and 22 interventional radiologists this would mean a shortfall of si interventional radiologists across the network area. Presently there are 25 surgeons and only 16 interventional radiologists; it may be that some of the vascular surgeons could develop their skills to become vascular specialists as described on page 18. This three site plan and network formation is a viable option and will provide an enhanced joined up approach to vascular services and improved diagnostics, in line with Vascular Society recommendations and will also build on the present good clinical network arrangements in place across the network area. **Theatre Requirements. It is hard to determine what the theatre requirements will be and this needs further investigation, the figures given in the tables in Appendi 5 were based on average theatre times for the main procedures which were received from ELHT and UHMBT See Appendi 5 Current times are not particularly good for vascular surgery, with finishes typically scheduled around 4:30 to 5:00pm. Etending this to 6:00pm the so-called three session day may be better. Staggering the start times of theatres also may be more efficient and avoid delays, as would greater use of weekends for elective work. While outside the influence of vascular surgeons alone, the establishment of league tables for late starts among surgeons in a unit have been found to improve their keeping to time. Vascular surgeons should support such local measures. Ref- Clinical Response to the downturn NHS Confederation 2010, pg Workforce Planning There are a number of key considerations in terms of future workforce and recruitment that will impact on vascular services and should be taken into consideration in recommending future models of service provision. These are: Vascular surgery is moving towards single specialty status. This will result in fewer junior doctor posts. Whilst services are primarily consultant-led and a reduction in junior doctor posts could be counterbalanced through the appointment of non-training grades, it is likely to impact on the ability of all eisting services to maintain current levels of medical cover. European Working Time Directive (EWTD) is enshrined in UK law. For Junior Doctors, a EWTD compliant rota requires a minimum of 6 junior doctors, even when on-call is not on site. This would require significant additional workforce capacity to deliver the service. This is an important consideration when looking at the sustainability of services with fewer consultants than this. There is a shortage of trained interventional radiologists and, whilst work is underway to develop interventional radiology as a recognised sub-specialty, it is likely to take some years before this position changes. Whilst there are no firm plans in place or agreed implementation dates, the intention is that in future vascular consultants will be vascular specialists, with skills in both surgery and vascular interventional radiology- This presents a potential solution - certainly in the interim and perhaps in the longer term and could have a significant impact on the 34
35 workforce within vascular centres, although these changes will take some years to materialize. 9.7 Patient and Public Engagement Patient and public consultation work is ongoing - a core script and press release have been formulated, public questionnaires have been completed and a public consultation document is presently being formulated. This work is being led by East Lancashire PCT Communication and Engagement team. This process is an etremely important part of the Vascular Review process and individual documents have been produced which can be seen upon request. Equality Impact Assessments have been completed and the review team have attended Overview and Scrutiny meetings. This work is ongoing. Chapter 10 Costs of Vascular Services The following recommendations were produced by the Vascular Society to highlight where resources could be released in NHS vascular services, while maintaining or enhancing quality Many unnecessary costs in vascular surgery derive from etended lengths of stay. Reducing these represents a clear area where cost efficiency and quality can be improved simultaneously. Remodelling vascular services by reducing the number of providers would reduce mortality and morbidity after major vascular surgery by concentrating medical and nursing epertise, increasing unit volumes and driving greater systematisation. The costs involved in the centralisation of services would be offset through improved outcomes by reducing the cost of post-operative morbidity and hence length of stay. A first phase of remodelling has already resulted in the number of vascular units in England being more than halved to just over 100. Vascular services are fully tariff based (with the eception of some interventional radiology procedures which the Clinical Advisory Group has recommended are addressed as part of this review). With the assumption that the recommendations will change the distribution of current services but not increase or decrease overall volumes, the net cost of the options to PCTs would be zero. It would seem reasonable to epect the centralised units to meet the proposed standards from within eisting tariff income, as this has been shown to be possible Tariff and Numbers of Vascular Procedures Commissioned As part of the review we engaged with all PCTs that commission vascular services within the review area. The information that each PCT provided can be found in Appendi 8. At first glance, the figures provided differ greatly from the vascular data that we gained from SUS*, however the data provided by the PCTs covers spells rather than actual procedures and includes ecess bed days. The list provided by the PCTs shows that the total costs for vascular procedures are 26,585,958. The data clearly needs further investigation and the review recommends that this is addressed when centralising - a coding sub-group, led by consultant Vascular Surgeon, Mark Tomlinson, from UHMBT has already been established within the review process, it is envisaged that this work will continue as part of the network, which is discussed on page 37. *SUS data is shown in Appendi 7. 35
36 Stakeholder Engagement We are set to engage with a wide range of stakeholders and have maintained a transparent approach throughout the review, sharing all key documents on a regular basis Procurement There is scope for increasing economies of scale in procurement through joint working between vascular surgery and other specialties, particularly as provision becomes more concentrated. Shared procurement with cardio-thoracic surgery in particular should be eplored by surgeons locally, particularly around hybrid theatres, high-end imaging and anaesthesia, as well as nursing and critical care. The over-regulation of basic devices results in very high costs for relatively simple devices such as endovascular stent grafts for aortic aneurysm repair. There is possibly some scope for vascular surgeons to agree to further limit the number of these devices available (although the range is already fairly small) or for manufacturers to agree to a set procedure price in order to continue supplying to the NHS. Ref- Clinical Response to the downturn NHS Confederation pg 16 Centralisation is associated with fewer complications and reduced length of stay which are both associated with reduced costs Increased Use of EVAR and Cost Implications The Payment by Result (PbR) spell price for endovascular aneurysm repair is similar as for open aneurysm repair. However endovascular aneurysm repair requires less critical care compared with open surgery but incurs costs for non-tariff devices (stents). The cost of the stent needed for endovascular aneurysm repair surgery is estimated at 6k per stent device*. Critical care costs are negotiated separately by each provider but are estimated at 1,500 per day*. *(The financial review of the implications of a Cardiovascular Review commissioned by London 2010) It is estimated that high volume units with a dedicated high dependency unit (circa 600 per day) will use one day in an intensive treatment unit and two days in the high dependency unit for open surgery, and lower volume units without the high dependency unit facility will use three days in an intensive treatment unit. In comparison, endovascular aneurysm repair requires one day in a high dependency unit before transfer to the ward. EVAR is associated with reduced length of stay and therefore lower costs overall Reduced Aortic Aneurysm Repair Length of Stay Due to Increased Uptake of Endovascular Aneurysm Repairs Endovascular aneurysm repair is associated with a lower length of stay compared with open repair techniques. Patients receiving abdominal aortic aneurysm repair surgery using endovascular surgery have a lower length of stay compared to those receiving open surgery. The average length of stay within Lancashire and Cumbria for both types of technique: EVAR = 7 days Open AAA = 14 days Difference = 7 days 36
37 10.5 Financial Implications for Providers There is a seven day length of stay difference for each procedure. The number of bed days saved across Lancashire and Cumbria in reduced length of stay could be significant - presently only 35% of AAA repairs are done by EVAR with a LOS at seven days as opposed to 14 days for open repairs. Increasing the numbers of EVAR procedures from 35% which it presently is in Lancashire and Cumbria to between 50% - 80% the figure proposed by the VSGBI will mean cost savings as length of stay could be halved. If the percentage of EVAR was to increase in line with VSGBI and local targets to 50-80% 896 to 1435 bed days could be saved. Increasing to 50% EVAR could save 896 bed days; Increasing to 80% of all AAA repairs could save 1,435 bed days Reduced Length of Stay Following Carotid Endarterectomy Surgery The average length of stay in Lancashire and Cumbria for carotid endarterectomy ranges from three to seven days with an average of five days. Average lengths of stay for carotid endarterectomy in Lancashire and Cumbria compare unfavourably to figures from Europe. Centralising services will enable providers to reduce this gap. Centralisation of vascular services has been shown to drive down length of stay for lower etremity by pass and amputations, which will also produce cost savings Productive Bed Use The use of same-day admission reduces length of stay and can provide savings in the numbers of beds needed to run a service. Protected beds - another model that has potential to be spread more widely is the establishment of protected beds to drive higher throughput for certain conditions. Protected beds for angioplasty have, where used, resulted in surgeons completing a greater number of cases per day. Beds outside of the acute unit for rehabilitation and low intensity care would also help the appropriate level of care to be delivered cost-effectively. Ref- Clinical Response to the downturn NHS Confederation 2010, pg Ambulance Costs Centralisation will require close liaison with the North West Ambulance Service (NWAS). However, until it is determined where the intervention centres will be placed it is not possible to know the impact and costs that will be involved in patient transportation. The outcomes of the subsequent Trauma Review will also need to be configured into any service agreements regarding the Ambulance requirements. 37
38 Consideration also needs to be given to The Joint Royal Colleges Ambulance Committee (JRCALC) guidelines which include the possible diagnosis of AAA and ischaemic legs as an area where consideration could be given for paramedics to directly refer the patient to specialist vascular services. This is an important potential development, which could further support the centralisation option. It is recommended that this is clarified in part two of the review. Chapter 11 Implementation Plans 11.1 Implementation Timetable A key issue now is how to move towards an implementation plan if the Clinical Advisory groups recommendations are accepted. The kinds of vascular services under discussion are unlikely to attract the attention of the independent sector as the need for ICU and specialist beds may present a barrier. If the approach adopted is one of co-operation, there are several alternatives: 1. A tendering approach is adopted with providers within a defined area being asked to put forward a business case based on the service specification 2. The providers are simply asked to go away and discuss amongst themselves where the centres will be and to put a business case based on the service specification back to commissioners. 3. Commissioners try and broker discussions between the sites to ensure that any decision takes into account issues of choice, accessibility and safety. In order to implement these recommended improvements to vascular services, it is recognised that some hospitals may not have capacity to accommodate all arterial surgery immediately. To overcome this issue, there should be a transition plan enabling designated central vascular units to initially perform abdominal aortic aneurysm repairs and carotid endarterectomise with lower etremity arterial bypass surgery being moved later to the central units over a planned, organised period of time. Chapter 12 - Recommendation Checklist for Vascular Reviews Comments below taken from the North West Specialised Commissioning Team Recommendation for North West Reviews Local barriers to change should be identified at the earliest opportunity and steps taken to address these. (The review has engaged with stakeholders from primary and secondary care patients, public and staff throughout the review process) Implementation planning should form an integral part of the review process. There should be named leads for this process and eplicit timelines. (This has been identified and will be implemented once the model has been agreed) Successful remodelling is more likely if early agreement between provider Trusts can be secured. (This work is ongoing) 38
39 Commissioners should look to remodel vascular services into a networked arrangement whereby all elective and emergency arterial surgery is located in a single unit. (Centralisation of services with an umbrella network is the aim of the review) The other components of vascular care should remain within DGHs to enable residents to benefit from fast access to specialised care but retain local availability of less specialised procedures and access to vascular opinion. (Within this model GP referral and outpatients would continue to be at the local DGHs. Central to this is the concept that the clinicians involved in the service operate as a single clinical team, working within MDT arrangements, with all members delivering care in both the central arterial intervention centre and in the DGHs. All should contribute to the delivery of a 24hr service through sustainable rotas. (This has been agreed and will be implemented once the model has been agreed) The detail of the service arrangement should be considered by the clinical advisory groups.(the Vascular Clinical Advisory Group has developed a model and service specification) The transfer of aortic surgery and carotid endarterectomy should take place at the earliest possible opportunity.- (This review recommends a staged approach to centralisation) 39
40 Appendi 1 Vascular Procedures are categorised into four levels: Level 1 Describes work that falls into vascular HRG codes but is non-specialised in nature and can be legitimately done in a hospital without a vascular inpatient unit, provided there are formal links with a vascular unit for advice. Level 2 Level 2 makes up the vast majority of vascular services. All other arterial and venous surgery, requiring input from a vascular surgeon or interventional radiologist and all miscellaneous procedures not included within Level 1, above. This includes lower and upper limb arterial surgery, venous surgery and amputations. Hospitals treating these patients musts have 24/7 consultant surgical cover and should have 24/7consultant interventional radiology cover, particularly if dealing with emergency admissions. There are potentially however, significant workforce issues in delivering 24/7 IR for this group of patients. This is a critical factor to consider when reviewing service configuration options. Level 3 AAA & CEA surgery and IR Whilst the surgical and IR skills needed for AAA and CEA are the same as those needed for other arterial work and cannot therefore be viewed in isolation, these procedures are low volume and there is clear evidence linking volume and outcome. Hospitals treating these procedures must have 24/7 consultant surgical and interventional radiology cover in order to deal with emergency admissions and complications of treatment. Level 4 Very comple, rare or requiring other highly specialist input, such as cardio thoracic surgeons. Including: Treatment of aortic arch and thoracoabdominal aneurysms Treatment of aortic dissections Thoracic aortic stent grafts Open or endovascular surgery for thoracic and thoracoabdominal aortic aneurysms Surgery for carotid body tumours Treatment of infected aortic grafts Treatment of mid-aortic syndrome Comple revision of arterial surgery Treatment of vascular malformations Deep vein reconstruction Treatment of difficult aneurysms by fenestrated and branched aortic stenting Laparoscopic aortic surgery 40
41 Appendi 2 Quality Standards QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Who is the nominated lead consultant vascular specialist? Mr Haytham Al-khaffaf MR. THEO OJIMBA Mr G. Thomson Consultant Vascular Surgeon Mr Vittorio Perricone Mr MARK TOMLINSON Is there a consultant vascular surgeon available at all times? Yes-There are four vascular surgeons who share 1 in 4 rota. August 2010 Rota attached At Lancashire Teaching Hospitals NHS Foundation Trust (LTH) there is a Consultant Vascular Surgeon available during normal working hours at all times. LTH participates in the NHS North West Emergency Vascular Network to ensure availability out of normal working hours. Yes- Also cover BLACKPOOL VICTORIA HOSPITAL on a 1 in 2 basis out of hours Yes. We do work in collaboration with Royal Lancaster in order to provide continuous care for the vascular patients. More specifically, outside working hours, the vascular surgeons on call at Royal Lancaster cover also for vascular emergency at Blackpool every Monday and Wednesday and on alternate weekends. 41
42 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH How many vascular surgeons are there in your team? FOUR There are a total of 6 vascular surgeons within the service, 4 at North Cumbria University Hospitals NHS Trust + 2 in Dumfries & Galloway Hospital. We provide a Solway basin service which includes the population of South West Scotland The Cumberland Infirmary, Carlisle is the main base for the vascular department which has vascular lab services and 24/7 hour cover by surgeons. They provide the full range of vascular services including: AAA, Carotid, Distal Reconstruction, varicose veins, vascular dialysis access. We provide Open Surgical Repair (OSR) for unruptured infra-renal abdominal aortic aneurysm repair at the Cumberland Infirmary Hospital and West Cumberland Hospital. This is provided by 2 surgeons on each site. The service now provides EVAR at Carlisle and plans to etend service for patients currently referred to Newcastle 2 substantive Whole Time Equivalents (WTE) Consultant Vascular Surgeons are employed at Lancashire Teaching Hospitals, with a further 1 WTE anticipated to start in January Consultant Vascular Surgeons currently participate in the Emergency Vascular Network Rota (will be 9 as of January 2011) FIVE There are 2 full time vascular consultants: Mr H Osman (HYO) and Mr Perricone (VP). The team is supported by four junior doctors (FY1 and FY2), one trust registrar with special interest in vascular surgery and one SPR 42
43 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH What other specialities does each surgeon cover? How much time does each surgeon dedicate to Vascular work? Three dedicated full time vascular surgeons Mr. Haytham Al-Khaffaf - full time vascular Mr Robert Arthur Salaman- full time vascular Mr. Simon Christopher Hardyfull time vascular Mr Kallingal Riyad, a fourth vascular surgeon, also takes part in the general surgical rota (wte vascular workload is estimated at 70%-80% vascular) Each vascular surgeon covers some General Surgery as well as the emergency rota. Some basic general surgical elective procedures such as hernia repairs and Lapascopic Cholecystectomies are also undertaken by the vascular As above there are 2 Vascular Surgeons of whom one contributes to the Surgeon of the Week Rota. This equates to 1:8 General Surgery cover so approimately 5 weeks of the year are devoted to Emergency General Surgery. As of January 2011 there will be 3 Full time Vascular Surgeons who will only participate in the Vascular On-Call Emergency Rota 1:16 and not the Surgeon of the Week Rota 50% Vascular Surgery and 1 in 5 Vascular Surgery on-call 50% General Surgery (1 in 10 on-call), with some Consultants providing specific General Surgery sub-specialty work including: Breast surgery, Endocrine surgery, Paediatric surgery The two vascular surgeons have no general surgical commitments and are purely involved in providing vascular service. 43
44 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH How many vascular sessions are offered per week within your Trust? We have 8 elective theatre sessions (Monday to Thursday) and 2 emergency sessions on Friday 43.5 sessions are provided at NCUHT/week which includes 10.5 theatre sessions per week (9.4 Inpatient sessions and 1.1 Day Case). On call includes 2 consultants from D&G. 6 Theatre sessions currently will be 9 from Jan Outpatients clinic sessions currently will be 6 from Jan UHMB Trust Hospital has five sites where vascular services are provided: RLI = Royal Lancaster Infirmary: main site with Vascular ward & centralised arterial surgery & Interventional Radiology FGH = Furness General Hospital Day surgery & Outpatients WGH = Westmorland General Hospital Day surgery & Outpatients QVH = Queen Victoria Hospital, Morecambe & Ulverston Hospital: Outpatients only Vascular: FGH = 1, RLI Day Surgery Unit = 1.75 (75%AM) G&V Day surgery WGH =2 RLI Main Centenary theatre = 3.5 (50%) RLI Endovascular suite = 2 vascular Interventional Radiology, Vascular & General CEPOD Emergency theatre daily PM alternate weeks = average 2.5 sessions per week with plans to provide an additional 2 emergency theatre sessions in the other week (i.e. increase to an average of 3.5 per week). Both vascular consultants are contracted to work 12PAs. These include 7 theatre sessions per week and 3 out patient clinics per week. Who is the nominated lead nurse? Sister Elaine Bell Lesley Robinson (CIC) & Ann Stanton (WCH) Vascular Nurse Practitioners Vicky Gordon Senior nurse on vascular ward Ingrid Saul, Vascular Clinical Nurse Specialist Liz McDougall, Modern Matron Jayne Robinson is the lead vascular specialist nurse 44
45 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Do you have nurse/nurses with specialist epertise in the following areas available? All of these can be covered Monday Friday regardless of holidays/sickness etc Further details are available on request Nurses on the vascular ward have completed level 3 study for Vascular Nursing, Leg Ulcer Management, Tissue Viability, Pain Management & NP2010 and ALERT Course Yes (Are there arrangements for cover during absences)? No Comment No Comment No Comment no Comment Wound/ulcer management All senior staff have eperience and skills in wound and leg ulcer management and diabetic foot management. We do have a tissue viability nurse, vascular nurse specialist and diabetic foot nurse specialist available to contact for advice Nurse led comple leg ulcer clinic, including patients with diabetic foot ulceration there is also an internal inpatient referral process. evidence file pages 1.2, 1.6, 2.11, 2.23, Gail Broadbent and Pat Vickers are the tissue viability lead nurses. They have special epertise on wound and ulcer management. Diabetic foot management Yes there is a specialist diabetic foot team Nurse led comple leg ulcer clinic, including patients with diabetic foot ulceration there is also an internal inpatient referral process. Diabetic nurse staff Deborah Whittle, Nurse Practitioner to Diabetes team evidence file 1.11,1.29 Judith Swift and Gaynor Richardson are senior podiatrist who are directly involved in diabetic foot management Claudication, and lifestyle advice Yes available for vascular nurses Nurse led vascular assessment clinic which involves diagnosing intermittent claudication (pre & post eercise ABPT s) patient information and lifestyle advice offered Yes evidence file 1.9,4.5. Denise Wilson SCP regular clinics Jayne Robinson and Emma Whiston run claudication and risk factor correction clinics 45
46 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Amputation and liaison with rehabilitation and limb-fitting services Access to this service which is supplied by another hospital - East Lancashire Hospitals NHS Trust presently have an amputee pathway which is followed and have strong links with our local limb fitting centre which is Preston and we have an outreach nurse that comes to our dept on a weekly basis to iron out any problems and counsel the patients and can refer on for other psychological care. Dedicated vascular Pre-Op clinic run by the specialist vascular nurses. 2 Specialist Rehabilitation Nurses in post who have a weekly MDT meeting with the Vascular Specialist Nurses to liaise over amputation, rehabilitation and limb-fitting. Yes regular MDT meeting fortnight and Cathie Greenwood attends from Preston limb fitting service. All ward staff have attended the Limb fitting unit. Evidence file pages 1.10,1.10, 3.5, 3.6 Kathryn Ashton is the lead amputation physiotherapist and liaison with rehabilitation and limb fitting services Vascular access for patients with renal disease No this is provided by the consultant vascular surgeons All the senior nurse are eperienced in caring for patients who are having new formations and revisions and have a close relationship with the satellite sites and main dialysis site at Preston 2 Renal Specialist Nurses who work in close liaison with the 2 Radiology Nurse Specialists link nurse on the dialysis unit and co ordinator nurse who links with Mr Abraham and Mr Calvey NO Aneurysms. yes all the senior nurse have eperience and knowledge of caring for patients with open aortic aneurysm / Endoscopic procedure EVAR and femoral and popiteal aneurysms and are aiming to produce a care pathway and have compiled a EVAR Patient info leaflet currently going through governance. Patients are seen Preoperatively & Post-operatively by the Vascular Clinical Nurse Specialists. This aspect of the service is consultant led and supported by the CNS Yes evidence file 1.9, 4.5. Denise Wilson SCP regular clinics /Developing this role with Advanced Nurse Practitioner Sheila Reay also. Evidence file pages 2.2, 2.3, /Developing this role. Evidence file pages 2.2, 2.3, Emma Whiston is the vascular specialist nurse who runs the aneurysm surveillance clinic coordinate the aneurysm/evar service 46
47 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH How many WTE vascular nurse specialists are there? 2 w.t.e. CIC and 2.8 wte at WCH 1.8 WTE at Band 7 I Vascular Surgical Care Practitioner (SCP) Denise Wilson /1 Vascular Advance Nurse Practitioner (ANP) Sheila Reay/ Ward staff on ward 37 Vascular Nurses./Evidence file 1.2,1.3,1.6, There are two full time vascular specialist nurses: Jayne Robinson and Emma Whiston. They are both involved in preoperative assessment of vascular patients and participate to the daily word round. In addition they both run risk factor/claudication clinics and aneurysm surveillance clinics independently. Is there a nominated lead consultant anaesthetist identified for liaison with the vascular service? Dr Steve Gilligan Yes Dr. Ewa Jankowska Dr Eamon McKiernon & Dr Martin Letheren Dr Muragesh Kinagi is the lead for vascular anaesthesia Dr Krishnaprasad Is there an anaesthetist with up to date eperience dealing with vascular emergencies available at all times? Consultant Anaesthetist available at all times who has undergone annual appraisal. There is a separate HDU/ICU anaesthetic rota Vascular emergencies are dealt with as part of the general anaesthetic emergency rota by consultant anaesthetists who complete annual appraisals and participate in audit plans including those for vascular surgery. Consultant Anaesthetist on-call Consultant Anaesthetist on-call All vascular acute admissions requiring emergency intervention are assessed by the anaesthetist consultant on call, who is available at all time. All the anaesthetic consultants are competent and up-to-date with the management of acute vascular emergencies Is there a separate HDU/ICU anaesthetic rota? yes at CIC There is a separate rota for theatre (including On Call) and HDU/ITU There are 8 consultant anaesthetists who have separate HDU/ICU on call rota On call Rotas supplied 47
48 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Is an interventional radiology service available at all times? There is no separate interventional rota but we have three vascular interventional radiologists who work fleibly and are prepared to come in even when they are not on call Yes Monday-Friday There are 3 Interventional Radiologists with an on-call rota coinciding with the Vascular Surgeons so when LTH is oncall for vascular, there will always be a Vascular Interventional Radiologist oncall. During working hours, Interventional Radiology is always available when LTH is not on-call; vascular emergencies are directed to one of the other Hospitals in the Vascular Emergency Network. All Consultant Surgeons are trained in basic angiography and angioplasty techniques & are supported by the on-call Consultant Radiologist or on occasions by the Vascular Interventional Radiologists The interventional radiology service is available from 9am to 5 pm Monday to Friday. There are two interventional radiologists working at Blackpool Victoria Hospital: Dr R Bury (RB) and Dr K Bowyer (KB). They do participate to the general radiology on call rota but currently there is no arrangement for an interventional radiology cover outside working hours. Are there times when they are not available? There are rare occasions when they are not available Vascular lab tests can be carried out on a 24/7 basis in the angiography suite as part of radiology. We have access to interventional theatre facilities e.g. modern image intensifier, carbon film table and appropriate software. We have access to modern interventional facilities in the Radiology department. no As above no 48
49 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Are all emergency and elective vascular interventional procedures undertaken by consultant vascular specialists or by staff under their supervision? All done by Consultant vascular specialists Yes. The vascular surgeons undertake sufficient interventional procedures per annum to maintain competence. All major vascular procedures (elective and emergency) are undertaken by a Consultant Surgeon or a Radiologist, or under their direct supervision. The elective and emergency endovascular interventions are undertaken by the two above mentioned interventional radiologists or by two consultant vascular surgeons only Do the surgeons sometimes work jointly? Yes Where there is clinical need to do so, Yes and always when appropriate. Yes, there are rare occasions when for particularly comple procedures the two vascular consultants work together; there is also close collaboration between vascular and cardiothoracic surgeons for the surgical management of patients with comple aortic thoraco-abdominal aneurysms and for combined carotidcoronary operations. Do the radiologists sometimes work jointly? Yes Where there is clinical need to do so, Yes always, when required. Many procedures are performed jointly with Surgeons and Radiologists. It is less likely that interventional radiologists are required to work jointly. 49
50 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Are all Endovascular aneurysm repairs, carotid surgery and stents undertaken only by vascular specialists with competences in these procedures? Yes All procedures are done by a Consultant Surgeon and/or Radiologist or directly supervising The evidence for carotid stenting is still debateable and at Blackpool we do not provide such service. All endovascular aneurysm repairs are undertaken by a team that include an interventional radiologist and a vascular consultant Are there vascular specialist and support staff with competences in interventional radiology available for all elective vascular radiology procedures? Yes Specialist radiographers and nurses available at all times Nurses working in the Interventional Radiology Unit have completed competencies as out lined in RCR/RCN Guidelines for Interventional Radiology Procedures Vascular Radiology Nurses 2 Vascular Radiographers All procedures requiring elective vascular radiology are discussed at the weekly MDT. Most interventions are undertaken in the appropriate environment (a fully equipped angio-suite) during scheduled sessions covered by one of the two interventional radiologists. Occasionally an operation which requires arterial reconstruction combined with angioplasty is undertaken in the vascular theatre with fully trained staff and with the participation of both interventional radiologist and vascular surgeon. 50
51 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Is there a member of staff with competences in vascular ultrasound available during normal working hours? vascular lab covers scan request from 8 am to 6pm Yes. 3 radiologists (2 CIC and 1 WCH) and 4 vascular sonographers (3 CIC and 1 WCH) Portable Duple is available for the vascular consultants 24/7 Portable Duple is available for the vascular consultants 24/7 Vascular Technologist during normal hours. -Vascular Sonographer A vascular laboratory staffed with 2 fully qualified vascular ultrasonographers is accessible during normal working hours. Such service is not available after 5 pm and during weekends and out of hours vascular ultrasounds are undertaken by the on call consultant radiologist. At weekends? Weekends and out of hours requests are covered by the Radiology department as above Interventional Radiologist with ultrasound competence always available when LTH is on-call for vascular emergencies (Vascular and Radiology rota coincides) Consultant Radiologist on-call As above Out of Hours? Weekends and out of hours requests are covered by the Radiology department as above Interventional Radiologist with ultrasound competence always available when LTH is on-call for vascular emergencies (Vascular and Radiology rota coincides) Consultant Radiologist on-call As above Do you have radiology nurses in the angiography suite? The service is provided by trained vascular radiographers Yes There are 9.4 WTE Nurses in the Radiology Unit (From 8a to Band 2) who cover the clinical areas as detailed in the rotas. Peter Sariwee and Caroline Kelly There are 3 qualified radiology nurses and 6 radiographers 51
52 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Is there a system for identifying patients needing vascular ultrasound and providing scanning, if required, on a daily basis? During working hours all vascular patients are referred directly to the vascular lab. They will be seen by the vascular specialist nurse who will carry out a provisional assessment and then inform the vascular registrar. A vascular ultrasound will be done there and then as required Yes. 2 radiologists (2 CIC rotate to WCH) and 2 vascular sonographers (1 CIC and 1 WCH) 3 headcount numbers Yes, patients identified by consultant Vascular specialists. All patients who may need this are always admitted under the care of a Consultant Vascular Surgeon? Vascular Consultant/middle grade urgent referral to Vascular Sonographers Even if the majority of vascular ultrasounds are requested by the vascular team, there are other departments who have direct access to this service (DVT clinic, cardiology and cardiothoracic surgery, stroke medicine, etc). The need for a scan is identified by the clinician and follows departmental guidelines. At weekends? This service is not available out of hours or at weekends. The surgical registrar on call will see the patients and inform the on call Vascular surgeon Yes for some emergencies and portable Duple is available for the vascular consultants 24/7 Out of hours and at weekends: When LTH is on call for Vascular Emergencies; all patients are assessed by a Consultant Vascular Surgeon, and scanned by Vascular Radiologist if necessary. The Vascular Consultant on call is notified by the Surgical Registrar who has either admitted or assessed the patient but vascular ultrasound service is adhoc dependent upon Consultant Radiologist on-call Outside working hours and over the weekend the need for an urgent vascular ultrasound is discussed with the consultant radiologist who does provide this service, when required. Out of Hours? This service is not available out of hours or at weekends. The surgical registrar on call will see the patients and inform the on call Vascular surgeon Yes for some emergencies and portable Duple is available for the vascular consultants 24/7 As Above but vascular ultrasound service is adhoc dependent upon Consultant Radiologist on-call Outside working hours and over the weekend the need for an urgent vascular ultrasound is discussed with the consultant radiologist who does provide this service, when required. 52
53 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Is there an in-patient ward available, fully staffed by nurses and HCAs with appropriate competences in care of patients with vascular disease? Yes. More information is available on request. Acute Life-threatening Events Recognition and Treatment (ALERT) All trained staff has attended ALERT training, we have a tissue viability link nurse who works closely with staff and ensures we are complying with nice guidelines and using the most appropriate treatment for that patient. Competencies are covered as part of several education and development programmes (see evidence log). Yes evidence file page 2.1 Tissue viability and wound care No Comment Competencies are covered as part of several education and development programmes (see evidence log). Yes evidence file page
54 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Pain management Two members of staff are pain management link nurses that attend updates and then cascade to staff we also have good links with Acute pain team who visit the ward daily Ward 12 is the Vascular Ward - There are Link Nurses on the ward who are fully trained in all these competencies they also have access to a Tissue Viability Nurse, Acute Pain Management Team, Diabetes Specialist Nurses and Critical Care Out -reach Team. Yes evidence file page 1.2 Care of patients with diabetes The majority of our patients are diabetic and we have again a diabetic link nurse who attends update sessions and cascades to staff she has also gained a qualification in diabetic management As Above and Competencies are covered as part of several education and development programmes (see evidence log). Yes evidence file page 1.3 High dependency care Some of our patients can be acutely ill and most of the staff is eperienced in this level of care and we use an early warning system which if triggered we call our critical care outreach team who will assess our patient and arrange transfer to a higher dependency unit. As Above Combined ITU/HDU Care of patients with disabilities, including patients with amputations. No Comment As Above 54
55 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Please show staffing details, competence framework showing epected competences No Comment Wte staff at CIC 1.0 Band 7, 5.16 Band 5, Band 5s, 14.9 HCAs 31 wte at WCH No Comment No Comment Documents enclosed: Learning and Development Strategies, Mandatory Risk Management training Do the ward staffs nurse any group of patients other than vascular patients and how frequently? Staffs are eperienced in the care of patients with all kinds of disabilities but mainly due to an amputation of a limb. Staff are eperienced in moving and handling, and we have a dedicated physiotherapy and Occupational therapist team who becomes involved with all these patients Yes all of the time as the vascular patients are managed on a general surgical ward The 27 bedded ward cares for both elective and emergency patients specialising in colorectal and vascular. Generally the proportion of patients receiving vascular care is approimately 10 in patients at any one time although the ward capacity allows for this to fle up and down as the service requires. Other surgical patients daily The ward staff nurse vascular and general surgical patients at the same time 55
56 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH What is the level of epertise of the junior medical staff covering vascular patients? Junior medical staff who support the vascular service are part of the generic general surgery rotation Vascular CT2/ST4/F2 & F1 available 24/7 FY1, FY2, ST3 or Senor Staff Grade General & Vascular Surgery Middle Grade surgeon on-call 24hours daily/ General & Vascular Surgery Middle Grade surgeon on-call 24hours daily/ 3 Specialist Registrars (1 Senior Vascular year 4+ & 2 General/vascular) & /1 Vascular Clinical Fellow (Specialty Doctor) are responsible for the vascular inpatients during normal working hours & provide daily ward rounds & review in conjunction with Consultant Vascular Surgeons/1 Vascular/General Specialty Trainee (ST1) & 1 Trust Vascular/General SHO provide additional ward & theatre support and also added supervision of the ward based FY1 doctors/2 Foundation Year 1 ward based house officers on the Vascular ward perform daily ward duties in conjunction with senior support The vascular team is supported by 2 FY1 and 2 FY2 doctors. There is also a trust vascular registrar and a rotating SPR. All the juniors participate to the general surgical on call rota. Are the junior staff on a separate rota from General Surgery? No No No- Junior Staff only participate in the General Surgical rota. A separate on call rota applies only for consultants. No 56
57 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH How many vascular inpatient beds are there available? 12 dedicated beds are available to vascular in patients services at East Lancashire Hospitals NHS Trust support Not defined, will depend upon demand but approimately bedded ward with approimately 10 vascular in patients at any one time, although the ward capacity allows for this to fle up and down as the service requires. Up to 17 beds 20 Is there an HDU area available on the Vascular Ward or is this a separate area? It is a separate area Separate HDU as part of Critical Care Unit An 8 beds High Dependency Unit is separated by the surgical wards and it is in close proimity to ICU. Such unit provides level 2 supportive care and it is managed by the intensive care staff. In addition there is a 10 beds Surgical Dependency Unit (SDU) in vicinity of the surgical wards. Such unit has a 1:2 nurse to patient ratio and provides more intense monitoring of surgical patients in the immediate postoperative period. Most vascular patients who do not require level 2/3 care are admitted in this area for 24 hours after their operation. How many HDU beds are available? The Trust has 20 beds based at the Royal Blackburn Hospital that can fle between level 2 and level 3 care. There are also 8 post operative care bed for level 2 care Vascular patients needing HDU care are sent to the general HDU. 14 level 3 10 level 2 24 beds in total Separate area as part of ITU Beds used fleibly as ITU or HDU as required 8 57
58 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Is a Physiotherapy service available daily for all in-patients with vascular disease? Monday to Friday a dedicated physio every morning has a referral meeting with the ward co ordinator and Occupational therapist ( who work cohesively as an effective team ) and plan their work for that day with the vascular patients. Yes Monday Friday with on call arrangements in place for weekends. Specialist amputee physiotherapist available. Physiotherapists are notified of patients by the CNS as part of the pre-op pathway if elective. Emergency patients are referred from the ward. Patients having amputation are automatically seen without the need for referral. Physiotherapy input for vascular in patients is on average 37.5 hours per week with the option to increase or decrease in put according to patients needs. There is sufficient resource available for patients to be seen every day. Is there access to Occupational Therapy for in-patients with vascular disease? As above Yes Monday- Friday only Occupational Therapists are notified of patients by the CNS as part of the pre-op pathway if elective. Emergency patients are referred from the ward. Patients having amputation are automatically seen without the need for referral. OT input for vascular in patients is on average 25 hours per week with the option to increase or decrease in put according to patient s needs. There is sufficient resource available for patients to be seen every day 58
59 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Is there access to the Social Work service for in-patients with vascular disease? Yes Yes Monday Friday only All in patient are assessed for eligibility for Continuing Health Care and then if appropriate a Section 2 Social Work referral form is completed for patients who may have social care needs - onsite social work team Patients are referred to Hospital Discharge Team (HDT), available 9am to 5pm Monday to Friday. HDT provides discharge planning support, assessment for future care and access to Social Services. How are Social Services contacted and what do Social Services then do? Inpatient referral system and it can be arranged for social worker to come to unit to discuss cases directly with the nurses, patient and relatives. A Contact 1 form is completed following an Occupational Therapy assessment. Social services will then assess the patient on the ward +/- a case conference to then decide an appropriate package of care. All Section 2 forms are collected by a Case Manager who sends it to the appropriate Social Work Department. Social Workers then attend to assess the patient s needs in accordance with the guidance stipulated in the Community Care Act Ward nursing staff liaise with Social Services. Social Worker allocated to patient then assessment takes place. We also use voluntary service.evidence file pages 3.3,4.2,4.3,4.4, Social Services can be accessed out of hours via an emergency Duty Team covering both Blackpool and Lancaster population. HDT provides a limited weekend service from 9am to 1pm both Saturday and Sunday Are the following facilities and services available at all times? If not please give details: Yes Yes Yes some some Emergency theatre There is an emergency theatre available 24 hours 365 days per year Available 24 hours yes A designated emergency theatre is available at all time. Emergency vascular theatre There is an emergency vascular theatre available 8-6 Monday to Friday No. Vascular patients share the general emergency theatre. In addition, urgent vascular patients can access an elective theatre every other day The emergency theatre is fully equipped to deal with emergency vascular cases. The nursing and support services are trained to support emergency vascular cases. NO but do have 2.5 weekday Vascular Emergency theatre sessions weekly Vascular emergencies are treated in this theatre as there is no sufficient demand to justify a purely vascular emergency theatre. 59
60 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Vascular angiography suite We have a dedicated vascular angiography suite no comment Vascular angiography suite is available only during normal working hours. Spiral CT We have Spiral CT NO There are 2 Spiral CT scanners which provide high quality imaging for all vascular patients within 24 hours from their admission when this is required. Critical care (at least Level 3) Critical Care is available unless the unit is full to capacity Critical care beds (See above There are 14 beds at level 3 and 10 beds at level 2. Level 3 is HDU within a Critical Care Unit and is in accordance with nationally defined standards. A 10 beds ICU provides level 3 critical care as defined below *Patients requiring advanced respiratory support together with support of at least two organ systems. This level includes all comple patients requiring support for multiple organ failure. Haematology (for urgent cross-match and blood products) Haematology, urgent crossmatch, Blood biochemistry Haematology and biochemistry are available all the time. Blood biochemistry and blood gas analysis facility to view imaging at other hospital within the catchment area are all available Facilities for the electronic transfer of images is available by PACS Haematology and biochemistry are available all the time. 60
61 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Facilities for electronic transfer of imaging from, or ability remotely to view imaging at, other acute hospitals within the catchment area of the vascular service. Facilities for the electronic transfer of images is available by PACS PACS link via VPN allows clinicians to view images in own and other hospitals Yes. Document : Transfer of Radiology Images to other Healthcare Providers Is Magnetic Resonance Angiography available during normal working hours? There are 3 scanners with access available out of hours Most diagnostic angiograms, both elective and emergency, are in fact MR angiograms. The practice of conventional diagnostic angiography is obsolete and it is not practiced in our unit. Do the in-patient wards for patients with vascular disease have: A,Hand-held Doppler ultrasound machine? B,Portable duple device? Every surgical ward has hand held Doppler ultrasound machine and portable duple devices are available even outside normal working hours. 61
62 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Does all vascular surgery take place in a theatre with: Theatre staff trained in vascular instruments, prosthetics and techniques Trained staff always available. Theatre staff trained in the use of cell salvage devices for blood conservation? Anaesthetists and Anaesthetic Practitioners are trained to undertake this and are available for vascular surgery. Stocks of grafts, instruments and sutures required for patients with vascular disease? Radiolucent operating tables and X-ray C- arms? 62
63 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Hand-held Doppler ultrasound machine and portable duple devices? Yes Access to blood and blood products? yes Are the Elective clinic and theatre sessions for patients needing permanent dialysis access sufficient to meet the needs of local patients with end stage renal failure? -East Lancashire hospitals trust has two satellite dialysis units with the Hub being at the Royal Preston hospital Yes, in addition, there is a specialist commissioning longterm plan to increase capacity They are treated as part of the general vascular emergency work load Both vascular consultants see patients requiring access in General Vascular clinics (on an urgent bases).fistulas are done in General Vascular Theatre Lists and etra WLI lists.. Elective outpatient & theatre sessions at Westmorland General where the satellite Dialysis unit is based. Dialysis Unit link to two vascular consultants Mr Abraham and Mr Calvey. Nurse co ordinator on site at Westmorland General Hospital. One of the two vascular consultants (HO) provides vascular access service for the local population. The regional dialysis centre is Preston. 63
64 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH What arrangements are there for the emergency management of these patients? 2 out of the 4 vascular surgeons have interest in vascular access and perform >100 vascular access procedures per year. The patients are seen in the general vascular clinic. One of the surgeons has a weekly session at the Royal Preston hospital combining a clinic and a theatre session. They are treated as part of the general vascular emergency work load Emergencies dealt with by Vascular Surgeons in Trust (working hours), on call vascular surgeon (out of hours) emergencies are referred initially to interventional Radiologist. No patients have eceeded any of the access targets in relation to this element of their care pathway and there is no waiting time for patients to be seen in clinic or listed for theatre. During normal working hours, such emergencies are notified to one of the Trust s Vascular Surgeons or Radiologists (depending on the nature of the emergency). Out of hours, notification will be to the Vascular Surgeon on-call. Admit to RLI if referred with acute symptoms but the majority of patients are referred directly to the central renal unit at Preston Hospital LTHT Patients who need urgent surgery are discussed with the renal physicians and if the clinical circumstances permit this, patients may be transferred to Preston prior to their intervention. Is information offered to all patients covering: SOME SOME SOME Vascular disease, including its causation and physical, psychological, social and financial impact All information is sourced from our local Intranet however if something is not there the staff will research it for the patient or find someone who can. Patient information leaflet on intermittent claudication outlines PVD, risk factors, lifestyles modifications etc Currently written information from the Vascular Foundation is supplied to patients & comprises Vascular disease booklet 64
65 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Treatment options available All treatment options are discussed with the patient either in clinic or on the ward. This is discussed with the patient who is provided with information verbally in respect of their holistic needs and is also covered in All About Claudication booklet Procedural leaflets as above Pharmacological treatments and their side effects Pre op either in clinic or on the ward as many are emergencies patients are given eido information leaflets on their procedure, what it entails, what to look out for and discharge details and who to contact should they have a problem. Briefly covered in All About Claudication. In addition to significant discussion with the clinical team including pharmacist. Referral to smoking cessation service. Evidence file page 2.13, 2.26 Promoting good health, including diet, eercise and smoking cessation Staff are able to promote a healthy lifestyle but we do have access to dieticians and we do have access to a smoking cessation service. Included in All About Claudication booklet Amputee benefits supplied by SMRC (Specialist Mobility Rehabilitation Centre) via Vascular SCP or ward. Evidence file page 4.3,4.5, 1.10 Access to benefits advice All information is sourced from our local Intranet however if something is not there the staff will research it for the patient or find someone who can. Advice provided by CNS with referral to Case Manager and Social services if further support needed Support group in process of being set up. Outpatient amputee group run in conjunction with Physiotherapy.Evidence file 1.10 Symptoms and action to take if become unwell All information is sourced from our local Intranet however if something is not there the staff will research it for the patient or find someone who can. See 33b & 33a evidence and in addition specific advice according to the patients needs is provided verbally by CNS and is supported in a letter to the GP and the patient NO epert patients programme 65
66 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Support groups available All information is sourced from our local Intranet however if something is not there the staff will research it for the patient or find someone who can. There is a Limb User Group and several other support groups that are referred to in the Specialist Mobility Rehabilitation Centre information leaflet. The Thinking About Stopping Smoking leaflet contains contact information for several support groups NO Epert Patients Programme (if available) All information is sourced from our local Intranet however if something is not there the staff will research it for the patient or find someone who can. No programmes currently provided for vascular patients. NO NO Vascular service staff and facilities available, including facilities for relatives All information is sourced from our local Intranet however if something is not there the staff will research it for the patient or find someone who can. On first contact with CNS this information is provided verbally as part of the initial assessment. A letter detailing this discussion is provided for the patient and the GP. CNS s working on developing more generic information about the vascular service. NO Who to contact with queries or for advice Staff are always willing find out the relevant information for that patient at that time or can put them in contact with someone who can help them. As Above NO 66
67 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH How to influence local services There is also a Lancashire carers contact monthly magazine which we display that has lots of info not just for patients but also for the carers Patient Advice Liaison Service leaflet Contact information detailed on advice leaflets In addition an Integrated Care Pathway is in development for use at LTH, regarding weight management and physical activity. Once implemented the Surgical Directorate will be formally measured for its performance in meeting a range of health promotion measures using the Health Promotion Audit Pro Forma NO NO Are the following support services available? East Lancashire Hospitals NHS Trust support a high multicultural demographic and as such has ecellent services integrated into the Trusts infrastructure in order to support interfaith and spiritual and translation support across a wide and diverse community Interfaith and spiritual support Pastoral Care and Spiritual Support provided by LTH Chaplaincy Service Evidence file page 3.11 Interpreters The PALS service will organise interpreters for different languages and sign language interpreters Interpreting service available for both in and out of working hours - Language line evidence file page 3.4, 67
68 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Bereavement support PALS will provide general support to the bereaved and will also organise Bereavement counselling from an outside agency Bereavement support team led by Bereavement and Donation team Evidence file 3.7, 3.8, 3.9, Advocacy services PALS will contact a local advocacy service for those patients requiring advocacy services but will also provide internal support to patients who just wish to be accompanied to an appointment. PALS available as above. Through contact with a Case Manager an advocate can be appointed for patients PALS Evidence file page 3.2,3.3, Benefits and employment advice PALS will contact the Citizens Advice Bureau or signpost to services from the internet Benefits advice leaflets available on wards, included specialist amputee rehabilitation sisters support with benefits for amputee patients and carers social services. Evidence file page 3.3, 4.4, Are Information leaflets about these services also available? No Comment Are clinical guidelines in use throughout the vascular service covering assessment and management of: We have guidelines available to junior doctors and nurses covering the management of patients with peripheral vascular disease and varicose veins Yes guidelines enclosed Yes guidelines enclosed 68
69 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Abdominal aortic aneurysm East Lancashire Hospitals NHS Trust guidelines are available to junior doctors and nurses delivering clinical management of patients with peripheral vascular disease and varicose veins We follow the Vascular Society of Great Britain and Ireland guidelines and NICE guidelines Yes guidelines enclosed Outpatient surveillance protocol Evidence file page 2.3,CT assessment llof a ll AAA & discussion in MDT regarding treatment protocol Pre-op assessment +/- Cardiac investigation as clinically indicated All patients have EVAR protocol CT scan. Every patient considered for intervention is pre-assessed and risk stratification takes place after CPEX. At this stage the patient is seen by the consultant anaesthetist. Every patient is discussed at MDT level. Theatre facilities comply with the Vascular Society document Framework for improving the results of elective AAA repair. Unfortunately the shortage of clinical clerks allocated to the surgical department has prevented the submission of AAA data to last year national audit. Carotid artery disease East Lancashire Hospitals NHS Trust support a joint Transient Ischemic Attack ( TIA) pathway agreed in partnership with the local stroke team. Where Carotid endarterectomy is indicated the team goal is to deliver services between 2 days or 2 weeks as is clinically prioritised against clinical need indicated. We follow the Vascular Society of Great Britain and Ireland guidelines and NICE guidelines Yes guidelines enclosed symptomatic patients with ABCD2 scoring < 4 should be referred urgently to the oncall Vascular surgeon for assessment & if appropriate surgery within 2weeks of the first event symptomatic patients with ABCD2 scoring 4 should be referred urgently to the on-call Vascular surgeon for IMMEDIATE surgery within 48hours of symptoms The pathway of care for stroke/tia patients has been agreed with the Stroke physicians and follows NICE guidelines. The inception of a daily TIA clinic and one weekly carotid list has unable us to reduce waiting time from inde event to surgery. Data are submitted to the national audit and an intra-departmental audit monitors the efficiency of this service every year. 69
70 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Diabetic foot The Trust has adopted and uses the University Hospital of North Staffordshire NHS Trusts protocols (See supporting information) Detailed within Central Lancashire Diabetes Guidelines page 64 MDT monthly meetings are attended by a Diabetic Consultant, a Vascular Surgeon and a Podiatrists for Diabetic Vascular Foot patients. Central Lancashire Diabetes Guidelines (included). Yes diabetic foot guidance, Evidence file page 2.29 Leg ulcers Scottish Intercollegiate Guidelines Network (SIGN) (See supporting information) Specified in LTH Clinical Guideline Management of Leg Ulcers in Adults Denise Wilson Evidence file page 2.11, 2.23, 2.25, Patients with leg ulcers may be assessed in hospital by vascular surgeons, vascular nurses or tissue viability nurses. All patients have a clinical evaluation of the arterial and venous circulation. Duple imaging is requested if indicated and, if indicated, a referral to the vascular surgeon is made. There is no written hospital guidelines specifically designed for leg ulcers. Claudication North East guidance is being drafted. The Trust currently uses SIGN guidelines LTH Clinical Guideline for Intermittent Clauditcation evidence files supplied Varicose veins See Trust s own Guidelines in supporting information Clinical Guidelines being developed however the current practices followed by the Vascular Team are detailed in Understanding VUUS Closure Procedure patient information leaflet Yes Evidence file page 2.9, 2.24, Yes evidence file page 2.18, 2.19 No 70
71 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Limb-threatening ischaemia Managed clinically through 24/7 consultant assessment cover Clinical Guidelines in development. Flow chart for the Management of vascular Emergencies details the emergency patient pathway. No referral to the on-call surgical middle-grade for urgent assessment, or direct with the on-call vascular surgeon if patient requires inter-hospital transfer for assessment or surgery No Lymphoedema North of England Cardiovascular Network guidelines (see supporting information) The Lymphoedema CNS is based at St Catherine s Hospice. Referrals are made by the Vascular CNSs using the Hospice referral form. The form and supporting information provide information about patients who need referral. When the Lymphoedema CNS see patients an individualised plan of care is recorded in the patients case notes and the patient is also given a copy. No No Do you have Guidelines on lifestyle advice for patients covering:- No - Evidence file page 4.5 referral form Vascular specialist nurses run a claudication and risk factor clinic. They initiate the referral when indicated. Dietician referral forms are available in out patient clinics and in the wards. In patients are seen within 24 hours from referral Support for smoking cessation Yes. Leaflets available at Pre assessment and on wards + Vascular Nurse reinforces advice as part of the Lifestyle modification clinic. Included in All About Claudication booklet and Thinking About Stopping Smoking - Evidence file page 4.5 referral form Smoke-free policy, Stop smoking start living 71
72 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Dietary advice There is a dietetic service provided within the Trust, available for advice and intervention Patients are advised in accordance with the information described in All About Claudication booklet - Evidence file page 4.5 referral form In addition to the walking programme for claudicating patients, all vascular patients receive informative leaflets on weight management and other healthy lifestyle. Most leaflets are from the British Hearth Foundation series Programmes of physical activity and weight management East Lancashire Hospitals NHS Trust support a referral system for smoking cessation and dietician. Physiotherapy services provide an eercise regime into which patients may be referred as clinically indicated and would also involve the Vascular nurse specialist in General Health Management. Internally via the vascular specialist nurse Patients are advised in accordance with the information described in All About Claudication booklet - Evidence Provided In addition to the walking programme for claudicating patients, all vascular patients receive informative leaflets on weight management and other healthy lifestyle. Most leaflets are from the British Hearth Foundation series Do you have clinical guidelines on monitoring and management of peripheral arterial disease risk factors covering East Lancashire Hospitals NHS Trust support set guidelines for the management of these therapies and services As below Referral form for Stop Smoking service (included). Referral to dietician service is verbal, although developing an intranet based referral process. Dietician will refer appropriate patients on to the community team for physical activity and weight management programmes where services currently eist. Yes 72
73 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Anti-platelet therapy East Lancashire Hospitals NHS Trust support set guidelines for the management of these therapies and services We follow national guidelines ( via Vascular Society) and the SIGN guidelines (see supporting information) No written guidelines Risk factor correction may be instigated in hospital but monitoring takes place predominantly in primary care. yes Lipid reduction therapy East Lancashire Hospitals NHS Trust support set guidelines for the management of these therapies and services We follow national guidelines ( via Vascular Society) and the SIGN guidelines (see supporting information) No written guidelines yes yes Control of hypertension East Lancashire Hospitals NHS Trust support set guidelines for the management of these therapies and services We follow national guidelines ( via Vascular Society) and the SIGN guidelines (see supporting information) No written guidelines yes yes Do you have clinical guidelines on the management of patients with diabetes covering: yes yes yes yes Yes Management of ischaemia and sepsis in patients with diabetes NO Detailed in both Central Lancashire Diabetes Guidelines and LTH Guidelines For Diagnosis and Treatment of Patients with Sepsis NO yes yes Peri-operative management of patients with Diabetes yes Yes Think Glucose National Programme and University Hospital of North Staffordshire NHS Trust guidelines.(see supporting information) Covered in LTH Peri-Operative Management of Diabetes yes yes 73
74 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Indications for involvement of the diabetic service in the care of the patient. Yes This is clinically decided upon. Detailed Central Lancashire Diabetes Guidelines. Diabetic Specialist Nurse Referral made on form included. no- referral as clinically indicated NO yes Do you have clinical guidelines on the management of patients with, or at risk of, impaired renal function including: Currently there are no set guidelines however staff work closely with renal physicians and refer patients as indicated. No No Indications for involvement of the renal service in the care of the patient? Currently there are no set guidelines however staff work closely with renal physicians and refer patients as indicated. The Trust has Acute renal failure guidelines see supporting documentation for a copy of this No written Guidelines are in place there is a close working relationship and liaison with the Vascular Team and the Renal Team covering the all of the MDT No No Prevention and management of complications Currently there are no set guidelines however staff work closely with renal physicians and refer patients as indicated. The Trust has Acute renal failure guidelines see supporting documentation for a copy of this Specific guidelines are in place for the prevention of Contrast Induced Nephrotoicity. No No 74
75 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Is there a protocol for by-pass graft surveillance in place? 2 of the surgeons have a surveillance protocol. Patients with fem-pop bypasses have a scan at 6 weeks and 6 months post op and annually thereafter. Vein grafts are scanned at 1 month 6 months and then yearly or if there are symptoms. Synthetic grafts are not routinely surveyed. No Evidence file page 2.30, 2.31, 2.32, 2.33, Our local policy is to invite for annual Doppler ultrasound every patient who undergoes the following: 1) below knee by-pass using vein as conduit 2) distal by-pass to crural vessels (vein and synthetic grafts) Such policy is endorsed by both vascular consultants Are clinical guidelines in use covering indications for involvement of cardiology services in the care of patients with vascular disease? NO Consultant referral as deemed appropriate The decision to refer to Cardiology is made by the pre assessment anaesthetists who refer to the European Heart Association Guidelines and the American Heart Association guidelines. Covered in Aortic Aneurysm Guidelines, otherwise is Consultant led referral based on identified clinical criteria NO Consultant referral as deemed appropriate With regard to the process of cardiac optimisation, no written guidelines have been agreed with the local cardiologists. Cardio-pulmonary reserves are assessed by a consultant anaesthetist in a specifically designated clinic (CPEX test). A cardiology referral is instigated at this stage when necessary. Are all patients offered: 75
76 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH A written individual care plan? Not in place at the moment but something that has been considered and been looked at introducing so that when a patient is admitted they could bring their plan which would list the procedures they have had, which consultants have been involved, what investigations they have had done, drugs, what dressings they are having if any.. ultimately what the patients preferred outcome would be etc Nursing pathways are used from the pre assessment stage of the patient s journey An individual care plan is devised and documented in the Shared Care Book by Vascular CNS. All Patients attending consultants Outpatients clinics and Vascular CNS clinics have a letter dictated and sent to their GP which includes the plan of care. Leg Ulcer Patients receive a standardised assessment by the CNS to inform their plan of care. All patients have a written individual care plan No A permanent record of consultations at which changes to their care plan are discussed? As above As part of the general case notes. Permanent records are made in the Shared Care Book described above and letters sent to patients GPS and patients if indicated A record of hospital episode with all relevant information is sent to GP electronically on the day of hospital discharge No A key worker/named contact? As above Each patient has a named consultant and a named nurse, plus a vascular specialist nurse who can be contacted at any point. Key Worker is named in Shared Care Book which includes contact details. This information is also included in the case notes and letters to the GP and patient. Contact name is available for relatives. No Comment 76
77 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH A copy of the patient s care plan should be sent to their general practitioner. Currently a discharge letter is sent electronically in most cases however this will change with the introduction of the revised pathway No Comment As above Discharge letter sent to GP after discharge Liverpool Care Pathway used Evidence file page 1.4, A record of hospital episode with all relevant information is sent to GP electronically on the day of hospital discharge Are clinical guidelines in use covering indications and arrangements for referral for psychological support? We have an assessment ( HAD ) hospital acquired depression which the doctors carry out if any concerns highlighted we also have a limb prosthetic outreach nurse that see the patients and we have a system in place were we can refer for psychological services at present for vascular patients Not at the Trust. We refer to the local Partnership Trust for this service. Information included in patient information which all staff are aware of and work in accordance with. Referral form to psychological Services (including hypnosis) specifies that the need for the referral must be discussed with the patient yes No Is there a formal Psychological assessment? East Lancashire Hospitals NHS Trust Vascular services have a pathway in place were referral for psychological services can be made for vascular patients As above Formal psychological assessments are conducted by the psychologist. No Guidelines Implementing The Mental Capacity Act 2005 and Apply The Supporting Code Of Practice Specifically for amputees there is support provided by the limb fitting centre from qualified counsellors. 77
78 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Are discharge planning guidelines in use covering: With regards to the amputation patient we have a pathway in place that cover rehab and discharge planning yes Detailed within LTH Discharge Policy. Specialty OT makes recommendations and liaises with Discharge Team/Social Worker and rehabilitation MDT as necessary. Rehabilitation available in hospital, community, settings and at home. IHDS are sent with to all GPs with a copy provided to the patient which is demonstrated on the Discharge Checklist Discharge to rehabilitation facilities? A limb prosthetic outreach nurse also reviews patients Patients that are not amputees are also thoroughly assessed by Physiotherapy and Occupational Therapy in aspects of safety in the home and home /property visits are carried anyone who are not quite ready would be referred to rehab and or social services involved This is covered under the nursing assessment and nursing plan. As above Discharge to rehabilitation facilities is mediated through a named consultant physician who identifies the individual rehabilitation needs. No Discharge home with support from local rehabilitation facilities? Patients that are not amputees are also thoroughly assessed by Physio and OT re their safety for home and home /property visits are carried anyone who are not quite ready would be referred to rehab and or social services involved There is a discharge policy. The nursing plans will also cover this. As above Home discharge with support from local rehabilitation facilities is co-ordinated by in hospital OT and discharge liaison officers. No 78
79 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Referral to limb-fitting service? A limb prosthetic outreach nurse also reviews patients This takes place via the dedicated Physiotherapist specialising in amputee care in association with disablement services. As above Our local limb fitting centre is based at Preston. Referral is mediated by physiotherapist with special interest in amputees Communication with the patient s GP? Discharge letters are sent electronically in most cases GP s receive a discharge letter As above electronic discharges Are there in-patient and community-based rehabilitation services with epertise in the care of patients with vascular disease, including amputees, available, including: Yes Pendle community Hospital has a specific rehab beds and have physio and OTs eperienced in dealing with amputees Some In patients are visited by Physiotherapy, OT and Rehabilitation Sister who also either continue to provide a community rehabilitation service or refer onto the community rehabilitation service. To support rehabilitation patients can be provided with foot wear by the Orthotist at SMRC Joan Donald is the lead inpatient occupational therapist who lease with colleagues in the community. There is a team of physiotherapists with particular epertise in management of vascular patients and amputees. The inhospital team links with Preston limb fitting centre. Specialist nurse from Preston visits Blackpool Victoria Hospital fortnightly to assess patients. Physiotherapy Yes Pendle community Hospital has a specific rehab beds and have physio and OTs eperienced in dealing with amputees Yes there is a physiotherapist who specialises in amputee care and who supports the community physiotherapists. The Specialist Physiotherapist sees the vascular patients as in patients and follows up all amputees as out patients at the Disablement Services Centre (known locally as SMRC). There is also community physiotherapy service. - two vascular physio who job share. As above 79
80 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Occupational therapy Yes Pendle community Hospital has a specific rehab beds and have physio and OTs eperienced in dealing with amputees NO Acute Specialist OT involved in acute care post op initially then as appropriate would be then managed by hospital rehabilitation OT or community. As above Yes Limb fitting and orthoses. we use our local fitting centre in Preston and an outreach nurse comes to the ward each week Yes disablement service plus input from our consultant in rehabilitation medicine and the prosthetist. Amputee Rehabilitation Sisters work with patients who have had amputation and patients who use wheelchairs at SMRC the sisters visit regional hospital to assess patients post operatively and liaise with OT, Physiotherapy, ward staff and refer all amputees to Dr Jepson Consultant in Rehabilitation. As above yes Is there a weekly multidisciplinary team meeting to review the care of patients with vascular disease involving: Yes We have a weekly MDT meeting attended by the vascular surgeons, vascular radiologists, vascular specialist nurses, vascular technologist and junior doctors The service holds regular MDT meetings on a weekly basis which involves all members of the vascular team. Our visiting consultants from Dumfries and Galloway Trust participate in the meeting via video conferencing. X-Ray weekly MDT meeting membership: Vascular Surgeons, Interventional Radiologists (and other Radiologists as indicated) and Vascular CNS. There is also a weekly meeting between the Vascular CNS, OT, Physiotherapy, Amputee Rehabilitation Sister and Orthotist. Interventional radiologists, vascular surgeons, ultrasonographers, vascular specialist nurses and radiographers from the angiosuite participate to a weekly MDT. Every patient considered for arterial reconstruction or endovascular intervention is discussed at this meeting and record of the clinical decision made is filed in the patient s note. Vascular specialists? As Above As Above As Above Vascular Radiology MDT & Vascular ward MDT Monday hrs As Above 80
81 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Imaging staff regularly involved with the care of patients with vascular disease? As Above As Above As Above Vascular Radiology MDT Tuesday hrs As Above Specialist nurses? As Above As Above As Above Vascular Radiology MDT & Vascular ward MDT As Above Is there a ward-based multi-disciplinary team meeting to discuss the care of patients with comple rehabilitation and discharge needs held at least weekly involving: This kind of meeting takes place on a daily basis with physio and OT and the ward staff if any further services needed they would be involved and bigger more comple MDT meeting would take place involving patient and family Yes. There is a weekly vascular ward round which can be followed up with individual case conferences including all of the healthcare professionals and social workers mentioned, when appropriate. Weekly meeting is held called Vascular MDT Ward Round and is attended by Physiotherapy, Occupational therapy, CNS and Ward Manager. Social Worker attends when requested by MDT Weekly Consultant led ward MDT (Mr Bukhari Monday 2pm) attended by Ward Manager or Sister, Physiotherapy, Occupational Therapy, junior & middle-grade surgical staff. Discuss all vascular inpatients & comple rehabilitation or discharge needs. Then enlist /refer to appropriate services as required e.g. social services, rehabilitation Consultant, Interim care facility etc A ward based MDT also takes place every week. Ward managers, vascular surgeons, vascular specialist nurses, physiotherapists, occupational therapists and discharge coordinators participate to such meeting. Patient rehabilitation needs and all other social aspect of patient care are discussed at this stage. Ward manager? As Above As Above As Above As Above Nurse with specialist epertise in care of patients with amputations? As Above As Above As Above As Above Physiotherapy? As Above As Above As Above Occupational therapy? As Above As Above As Above As Above As Above 81
82 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Social work? As Above As Above As Above NO As Above Are multi-disciplinary clinics for assessment of patients with diabetes and comple foot problems held involving: One of the surgeon has a joint clinic with the diabetic services Yes, this is through a case conference and can include all of those mentioned. There is also an orthopaedic foot and ankle clinic which runs parallel to a vascular clinic. This is an MDT clinic which includes the community podiatrist. The Disablement Services Centre also runs a diabetic service. Yes Monthly, all ecept orthopaedics Multi-disciplinary meetings are held monthly and are attended by Vascular Surgeons, Diabetes CNS, Orthotist and Podiatrist. All comple foot cases discussed and treatment plan formulated. Tuesday AM Vascular OPD with co-eistent Diabetic podiatry clinic at RLI NO Vascular surgeons A multidisciplinary meeting takes place on a daily basis with regular physiotherapy and Occupational therapy involvement. Other representatives are co-opted and invited as required. Or where clinical indications identify a more comple MDT meeting should take place involving patient and family. As Above discuss with Paul Smith re medical clinic NO Diabetes services As Above As Above Diabetic & Podiatry parallel clinics weekly Thursday am RLI, Tuesday pm RLI including WGH patients. FGH Cathie Hay combined day/podiatry clinic NO Orthopaedic services As Above As Above no NO NO 82
83 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Podiatry services As Above As Above 2 Orthopaedic Consultants with interest in foot and ankle NO Do you have any other multi disciplinary vascular clinics? As Above No Comment No Yes Tuesday pm RLI Diabetic Tuesday pm and Thursday am RLI and FGH Tuesday AM Vascular OPD with co-eistent Diabetic podiatry clinic at RLI No Are there guidelines agreed with the specialist palliative care services serving the local population covering: yes we have close links with the palliative care team and follow an end of life care pathway The vascular service is supported by the hospital palliative team lead by Dr Whitfield. In addition there is support from our local hospice which does provide access to patients with end stage vascular disease. Arrangements for accessing advice and support from the specialist palliative care team? As Above Any vascular patients with these needs would be seen by the Trust s Palliative Care Team Referral criteria for palliative care for both inpatients and outpatients and arrangements for accessing support and advice are described in LTH Hospital Palliative Care Team Inpatient Service and Outpatient Services. These documents also include arrangements for level of support to be provided by Specialist Palliative Care team from simple advice to comple cases requiring a collaborative shared care approach. Inpatient referral to Palliative care team who review & will advise or take over care Limb ischaemia, Unreconstructable vascular disease & patient refusing amputation Graft infection, sepsis & unfit for further vascular reconstruction As Above 83
84 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Indications for referral of patients to the specialist palliative care team? As Above Verbal referrals would be received from any member of the vascular care team by the palliative care team and dealt with appropriately In cases where Specialist Palliative Care input for symptom control becomes the main clinical priority patients can be referred to a Hospice. Referral criteria, process for accepting patients and documentation to be used are included in St Catherine s Hospice Specialist Palliative Care Services Referral Criteria and Form Inpatient referral to Palliative care team who review & will advise or take over care As Above Arrangements for shared care between the vascular service and palliative care services? As Above Palliative care would not take over care but would interface into vascular services. Once in the Hospice applicable to those cases, the palliative care team would continue with the care. Further information and guidance (including pain management and contact details for advice and support both in and out of working hours) on Caring for Patients at the End of Life is in Included in LTH The Liverpool Care Pathway for the Dying Patient: A User Guide Inpatient referral to Palliative care team who review & will advise or take over care As Above 84
85 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Is the Vascular Service aware of the local guidelines for end of life care? There is a Trust policy to support End of Life Care. Staff are aware of this policy and work within the policy parameters. Yes The Trust follows the Liverpool pathway for end of life care and there is a Trust palliative care team who are involved where appropriate The Vascular Team provide end of life care in accordance with the Liverpool Care Pathway. Information and guidance (including pain management and contact details for advice and support both in and out of working hours) on Caring for Patients at the End of Life is in Included in LTH The Liverpool Care Pathway for the Dying Patient: A User Guide Liverpool Care pathway used links with the Hospice at Lancaster Yes Enclosed documents: Care of the dying patient and their relatives/carers, Do not attempt resuscitation, Advanced Decisions / Living Wills Is there a meeting with local rehabilitation services (held at least annually) to review the links with the vascular service and address any problems identified? Yes, there is an annual Solway Basin Meeting which includes all members of the rehabilitation team. Weekly meetings are held attended by the Rehabilitation Sisters, MDT of the Rehabilitation Services and the Vascular CNS part of this meeting is devoted to discussions about the service and areas for improvement. NO NO Is vascular ultrasound available for all vascular out-patient services? 85
86 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Do all vascular outpatient clinics have: East Lancashire Hospitals NHS Trust supports one stop clinics for all vascular patients. ABPI, arterial and venous Duple scans for lower and upper limbs, carotid duple scans and abdominal aortic aneurysms can all be done in the same visit. Vascular out patients have 2 hand held Doppler ultrasound machines and ABPIs are regularly measured in clinic when necessary. There is no portable scanner in clinic since direct access to the vascular laboratory is available for urgent investigations Hand-held Doppler ultrasound machine? Portable duple scanner? NO NO Facilities to perform ankle brachial pressure tests? 86
87 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Do you have one-stop clinics and what investigations? We have a one stop clinic system for all vascular patients ABPI, arterial and venous Duple scans for lower and upper limbs, carotid duple scans and abdominal aortic aneurysms can all be done in the same visit NO - VARICOSE VEIN & DUPLEX SCANNING- CLAUDICATION & ABPIs Claudication/risk factor clinics are nurse lead and clinical assessment is complemented by an arterial Doppler ultrasound and resting and post-eercise ABPIs measurements carried out on the same day. All new referrals are scrutinised by one vascular consultant who select which patients should have a Doppler ultrasound on the same day of their out patient visit. As a consequence a large proportion of patients with venous and arterial ulcers do have a onestop clinic. 87
88 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Do you have a mechanism to supervise an eercise programme? Through the Physiotherapy department Yes, organised by the vascular specialist nurse. There are One-Stop TIA clinics carotid / duple & CTA. Some patients with varicose veins and patients requiring an A-V fistula are assessed on One-Stop basis using the Portable Ultrasound. Planning is currently underway to provide a more comprehensive One- Stop venous assessment and A-V fistula assessment. This development is included in the local Renal Strategy and the business case has already been approved. Once the third Vascular Surgeon is in post the service will be able to commence. Community based eercise programme which patients can be referred to (Nordic walking) Claudication clinic Do you have nurse led clinics? Yes These are set up 2 sessions per day, 5 days per week, Monday to Friday. The template for these clinics is 6 patients. Sue Kenny is the specialist nurse lead who runs the nurse led clinic at Level 3. There are community vascular clinics managed by community staff which undertake tests art level 1 and 2, referring patients at level 3 into East Lancashire Hospitals NHS Trust. yes - Vascular assessment clinic - Comple leg ulcer clinic- Pre-op clinic- Boto clinic for patients with Hyperhidrosis Claudication / risk factors clinic AAA surveillance clinic (aneurysm surveillance form) Follow-up clinic for radiofrequency ablation of varicose veins 88
89 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Do you have telephone follow-up clinics? East Lancashire Hospitals NHS Trust are currently in the process of etending this practice where clinically appropriate.. NO There are no clinic templates set up for telephone follow up but all patients and members of the Primary Care Team are provided with the contact numbers for the Vascular CNS and Consultant. Telephone advice and support both pre and post treatment is regularly provided by the CNSs. No, but we have a help-line directly to the vascular specialist nurses. All vascular patients are provided with this contact number at time of hospital discharge. NO Can you prescribe an eercise programme? Yes, in conjunction with the Trust s Physiotherapy department and eercise practitioner All patients with claudication are encouraged to have their own eercise programme, which involves completing a diary to monitor progress with regard to walking distance. The All About Intermittent Claudication leaflet is used for this purpose. Patients attending claudication clinic are advised on the following protocol walking programme for intermittent claudication Is there a local policy covering ultrasound screening of relatives of patients with abdominal aortic aneurysm? There is no written policy but generally we screen relatives of patients with abdominal aortic aneurysms, especially males at the age of 50. If the scan is negative then we scan them every 5 years. Yes. All patients are advised to get their male relatives more than 65 years of age to get ultrasound of their aortas via their GP There is no policy for LTH but it is practice for patients relatives to be advised to contact their GP by either the Vascular CNS or the Consultant if they are aware of the patient s relatives. GPs are able after discussion with the patient and obtaining their agreement, to refer for this purpose and USS screening scans are performed At AAA surveillance clinic family history of AAA is recorded and advice given by the specialist nurse. 89
90 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Who do you screen? as above as above N/A First degree Male relatives of AAA patients. Female relatives of female AAA patients as above At what age do you screen? 50 YEARS as above N/A 50 YEARS as above Does the vascular service have: 90
91 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Mechanisms for receiving feedback from patients and carers about the treatment and care they receive? we have patient satisfaction surveys and widely available comment cards placed in areas throughout the hospital i.e. on wards and in outpatient areas Patient eperience data is now captured with real time data using hand held technology to capture scores. The department also carry our regular paper surveys with patients and carers. The vascular ward (Ward 12) surveys all patients on discharge with a Patient Eperience Tracker (PET) which asks the patient 5 questions about their eperience of care and treatment. Results for the month of August show overall satisfaction at 89%. In addition LTH also undertakes an annual patient satisfaction survey supported by the Picker Institute. The PET is also used in the Out Patient Department but it is not possible to determine the feedback specifically from Vascular patients. The results from the PET, patient complaints (including lessons learned and action plans) and patient satisfaction surveys are discussed at the Ward 12 meetings, the Directorate Clinical Governance meetings attended by the Vascular Team. Varicose veins surgery questionnaire NO 91
92 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Mechanisms for involving patients and carers in decisions about the organisation of the Services As above Patient panels meet monthly in each of our localities and a joint panel is held bi-monthly. Members of these panels do attend the Trust board. The Directorate has a full Patient and Public Involvement action plan which details specific work being undertaken by the Vascular CNSs Varicose veins surgery questionnaire NO Do you provide guidance on driving advice, covering the type of licence and giving appropriate advice on DVLA notification? Verbal advise is given and informed to let insurance company know and follow DVLA guidelines which we can print out for the patients yes Verbal advice and information is provided to patient both pre and post operatively. All appropriate patients are referred to Wrightington (Local Centre). Addresses (including Wrightington) are detailed in Driving After Amputation patient information which also provides advice about adapted vehicles. No written protocols. The following group of patients are advised according to DVLA guidelines: 1) victims of stroke and TIA 2) amputees 3) AAA patients Are you collecting and submitting data to the National Vascular Database (all inde procedures) and British Society of Interventional Radiology Registries? Yes. All inde procedures are on the national vascular database (NVD). Our Trust name is on their website and we are required to submit figures to the database for each case. Information is collected and submitted for the following procedures Aneurysms Carotids Infra-inguinal bypass Amputations (National Vascular Database reports showing riskadjusted comparative outcomes for the service. BSIR Registries information). For the year only carotid data were submitted 92
93 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Does your service have an annual programme of audits covering: We have audits of radiological interventions. Yes. The service participates in a yearly audit in March on each surgeon in the Solway Basin network. Their performance is audited in detail to include the number of inde operations, data on mortality and morbidity and also to discuss the introduction of new techniques and the outcomes of these. Clinical Directors also have access to CHKS data which identifies consultant specific activity and data and the divisional governance lead will highlight any outlying practice which is then eamined further. Surgical Directorate has a full Audit Forward Plan which includes Vascular Audits and compliance against NICE and other best practice guidance. Surgical Directorate Audit Plan 2009 (2010 is to be confirmed). The vascular department participate to the audit meeting within the surgical division. There is no structured vascular audit looking at number of procedure per clinician. There is no audit looking at medical management of patients with PVD. The compliance to NICE guidelines for carotid surgery has been monitored and presented to our local meeting but also to the recent British Geriatrics Society meeting (form enclosed). Number of interventional procedures (surgical and interventional radiology) undertaken by each vascular specialist across the service s catchment area? As above yes As above As above 93
94 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Medical management of patients with peripheral vascular disease? As above yes As above As above As above Compliance with evidence-based guidelines? As above yes As above NO As above 94
95 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Are there clinical guidelines agreed with the ambulance service covering the clinical indications for taking emergency patients to the hospital/s providing in-patient vascular services and the patients who may be taken to Emergency Departments without on-site in-patient vascular services? East Lancashire Hospitals NHS Trust comprises of two hospital sites, Burnley General Hospital and Royal Blackburn Hospital. Burnley is a cold elective site whilst Royal Blackburn Hospital provides the areas only emergency hospital in the locality. All vascular emergency patients are treated at Royal Blackburn Hospital 24/7. yes NWAS have been formally informed of the Vascular Network on-call Rota. Guidelines are currently under review and therefore it has not been possible to provide a copy of these written guidelines Blackpool Victoria Hospital provides a 24 hours access to A&E for the local population. Patients with acute vascular conditions are therefore assessed in the A&E department at Blackpool. When Lancaster provides cover for vascular emergencies, the transfer of patient follows the enclosed guidelines Transfer of emergency vascular patients from Blackpool Victoria Hospital to royal Lancaster Infirmary. WRITTEN GUIDELINES 95
96 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Does the service produce an annual report summarising activity, compliance with quality standards and clinical outcomes? (The report should identify actions required to meet epected quality standards and progress since the previous year s annual report) Yes. This can be made available on request. The Surgical Directorate produces an Annual Clinical Governance Report which provides a summary for the Directorate of activity, compliance with national standards, quality standards and clinical outcomes. Information specific to the Vascular Service is detailed where appropriate in the report Annual report of activity and quality standard such as mortality, readmission rate and hospital length of stay are regularly published and discussed at directorate meeting and at eecutive board level. More specific vascular quality standard are discussed at MDT level NO- Does your service have sufficient administrative, clerical and data collection support available? We do, but I do not think it is sufficient. yes There are 2 WTE PAs at band 4 supporting the service. There is access to a band 2 typist providing an average of approimately 1 hour per week in support. These resources are adequate to meet the needs of the service. The is a full time band 3 HCA who supports the Vascular CNSs and undertakes some administrative duties. NO but Review of A & C roles in progress Definitely not. National audit data are still collected by the individual surgeons and clerical support is badly missed. 96
97 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Does your service run educational session on the assessment of vascular emergencies for Emergency Department staff, general surgeons, GPs and ambulance staff (at least annually)? We do but rather sporadically The Service holds annual educational clinical meetings involving presentations (topics and cases). All members of the vascular surgeon team are encouraged to attend 2 national or international meetings a year e.g. the vascular service of Great Britain and Ireland (VSGBI) and the European Society of Vascular Services (ESVS).Our comple cases are referred to a tertiary centre, the Freeman Hospital, Newcastle Upon Tyne which is the regional vascular unit. plus weekly in house medical staff training programme Training sessions have been provided as part of the In House Surgical Course which includes sessions on Blocked Arteries and Aneurysms The Vascular CNS are able to act as Mentors for Student Nurses and as such provide Spoke Placements The Vascular CNS s also act as assessors for Nurses completing the level 3 Leg Ulcer Course (specifically assessing competence for compression bandaging) Provide educational sessions on the assessment of Vascular Emergencies to FY1 & FY2s, which includes junior Emergency Department staff. Also in the regional Specialty Trainee General Surgery programme (Mr Wilson) Our department run every year educational sessions open to all hospital staff. The management of critical limb ischemia, carotid disease and AAA have been presented over the last 2 years. In addition the staffs in the ward have educational meetings every year with vascular specialist nurses. (folder with Vascular Training Session enclosed) We have separate meeting with GPs 97
98 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Any further information about your service you feel we should be aware of? East Lancashire Hospitals NHS Trust provide a service which includes one stop clinics, availability of scans for emergencies, and ecellent radiological service.the Trusts model where vascular emergency patients are referred directly to the vascular lab is unique and does speed up the management of patients. Our Solway basin network was established in It was formed to provide high quality vascular services for the population of North Cumbria and parts of South West Scotland. The amalgamation of 3 District general Hospitals into 1 hub provides a single service where travel to routine vascular hospitals can be achieved within 2 hours and 1 hour for access to outpatient facilities. The current provision has been discussed with NHS Cumbria s Public Health team and the Scottish Health Authority. It has been supported through visits of the GB&I Vascular Society as well as the Northern Vascular Centre (See supporting letter from Mr Mike Wyatt) Nursing staff on the Critical Care unit have completed competencies in providing care for vascular patients. An additional Consultant Vascular Surgeon is being recruited for LTH as a result of an 18 week sustainability Business Case and it is anticipated will be in post by January 2011 The Vascular ward (Ward 12) conducts monthly audits on the fundamental aspects of care and includes Nutrition, Tissue Viability, Medication, Pain, Observations and Falls. The audit results demonstrate ecellent compliance with quality care standards for patients. Ward 12 also has an ecellent record for infection prevention and control. There have been no MRSA bacteraemia on the ward in this year. Ecellent compliance is demonstrated through audit for hand hygiene. continued below.. UHMBT Vascular Unit and Blackpool, Fylde & Wyre Foundation Trust (BFWFT) have worked together providing vascular services for the populations of North Lancashire and South Cumbria for several years. UHMBT Vascular Unit and Blackpool, Fylde & Wyre Foundation Trust (BFWFT) have worked together providing vascular services for the populations of North Lancashire and South Cumbria for several years. This population is spread over a wide geographical area, (particularly that covered by UHMBT) which provides certain challenges to providing an elective and acute emergency vascular service. Blackpool Victoria Hospital also hosts the Lancashire Cardiac Unit, providing regional cardiothoracic services. UHMBT Vascular Unit has provided additional Consultant Vascular Surgical support and epertise to Blackpool Fylde & Wyre NHS Trust for a considerable number of years. This has comprised providing a centralised emergency vascular service at...continued below.. Any there other aspects of the care of vascular patients you feel have not been adequately covered in this questionnaire? Not at this time. It should be noted that due to the geographical location of North Cumbria services, there are essential clinical links with Dumfries and Galloway, which provide emergency and elective services to a population of circa 400,000. Our nearest tertiary centre is Newcastle Hospitals which is approimately 60 minutes travel time from Carlisle and 120 minutes from Whitehaven. No Thoracic & Thoraco-abdominal aneurysms Thoracic outlet surgery Hyperhidrosis and thoracoscopic sympathectomy services Hospital policy on infection control. Hospital policy on infection control. Infection is in fact one of the most disastrous complication in vascular surgery and almost inevitably lead to adverse outcomes. A quality assessment on vascular service must include local policies on infection prevention and control. 98
99 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH LTH has just embarked upon implementation of the Enhanced Recovery Programme (ERP) and while clinical areas who undertake surgery for cancer patients will be included in the first part of the roll out programme it is envisaged that ERP will be utilised as the model for delivering elective care and as such be available to vascular patients The Royal Lancaster Infirmary on a 1 in 2 basis out of hours for over 5years, to which patients presenting acutely to Blackpool are referred and transferred when there is no Blackpool Consultant Vascular Surgeon on-call at weekends and out of hours. In addition UHMBT have provided Consultant Vascular surgical epertise to the Cardiac Unit performing emergency and elective combined cases (e.g. Thoraco-abdominal aneurysm repair), and UHMBT have also offered a tertiary Vascular surgical service for comple aneurysm surgery, Thoracic Outlet surgery, thoracoscopic sympathectomy and hyperhidrosis. 99
100 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH More recently over the last three years the two trusts have eplored the possibilities of formalising this combined working arrangement, convened a Joint Vascular Steering Group and presented an options appraisal to the Chief Eecutive Officers of both trusts. An agreed clinical model has since been developed with a view to the Vascular service working as one combined unit across both trust sites, covering the entire population base of 700,000. The Joint Vascular Steering Group has spent the last si months working through the clinical caseload, financial and business aspects of the proposed model, including the necessary transfer of facilities, bed days, ITU & High Dependency requirements and Consultant staff time as appropriate. 100
101 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH The steering group has sought to maintain local vascular services close to home where possible, but accepted that some further centralisation of vascular services is required as suggested by the national AAA screening programme and in line with the Vascular Society AAA Quality Improvement Framework. The agreed clinical model is to Centralise ALL emergency vascular surgery at the Royal Lancaster Infirmary (RLI) completely (i.e. 24hours, 365days pa). Provide a daily Vascular surgery emergency theatre session, and access to emergency theatre 24hours a day Provide 24hours emergency vascular surgical presence on the acute RLI site, Consultants will provide a daily Consultant inpatient ward round, and supervised junior surgical training and teaching, as well as emergency and urgent vascular surgery. 101
102 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH This will comprise ALL seven Consultant Vascular surgeons performing on-call duties at RLI, and UHMBT surgeons will backfill some elective vascular activity at the Blackpool Victoria Hospital (BVH) Centralisation of ALL aortic surgery to the acute RLI site (both Endovascular & Open surgery) in defined scheduled sessions Transfer of patients requiring emergency carotid surgical intervention within 48hours of presentation (ABCD2 score 4 or more) to the acute RLI site, but maintain scheduled acute carotid surgery (ABCD2 score <4) at the Trust local to the patient within 14days of presentation Maintain elective peripheral vascular interventions (angioplasty and lower limb bypass procedures) at the Trust local to the patient, but transfer urgent or high risk cases to the acute RLI unit for intervention as appropriate 102
103 QUALITY STANDARD ELHT NCUH LTH UHMBT BFWH Perform Amputation surgery (ecept absolute emergencies), Diabetic foot debridements, and venous surgery at the Trust local to the patient Provide daily Vascular Consultant surgical presence on site at Blackpool Victoria Hospital (Mon-Friday 9.00am 5.00pm), with daily vascular surgical inpatient ward round, review of inpatient referrals, and support to the Cardiology & Cardiothoracic units. Scheduled Vascular surgical and interventional sessions will be provided for appropriate cases as defined above. We hope that the current regional Vascular service review will consider the close unit working links between UHMBT & BFWFT, and the agreed clinical service model and preparatory work that has already been completed. 103
104 Greater Manchester Review Wigan and Bolton Support for Patients and Carers S1-01 Does your Trust currently offer Information to all patients covering at least: S1-02 Are all patients offered: S1-03 S1-04 Are the following support services available in your Trust? Does your Trusts vascular service have: a. Vascular disease, including its causation and physical, psychological, social and financial impact b. Treatment options available c. Pharmacological treatments and their side effects d. Promoting good health, including diet, eercise and smoking cessation e. Access to benefits advice f. Symptoms and action to take if become unwell g. Support groups available h. Epert Patients Programme (if available) i. Vascular service staff and facilities available, including facilities for relatives j. Who to contact with queries or for advice k. How to influence local services (QSDN-199) l. Where to go for further information, including useful websites. a. A written individual care plan b. A permanent record of consultations at which changes to their care plan are discussed Bolton c. A key worker / named contact. a. Interfaith and spiritual support b. Interpreters c. Bereavement support d. Advocacy services e. Benefits and employment advice a. Mechanisms for receiving feedback from patients and carers about the treatment and care they receive. b. Mechanisms for involving patients and carers in decisions about the organisation of the services. Wigan 104
105 Staffing S2-01 S2-02 S2-03 S2-04 S2-05 S2-06 S2-07 Does the vascular service in your Trust have a nominated lead consultant vascular specialist and nominated lead nurse with responsibility for ensuring implementation of the Quality Standards for Services for Patients with Vascular Disease across the service s catchment area? Does your Trust have a nurse available with specialist epertise in the following areas? For In-patient services; is a consultant vascular surgeon available at all times? For In-patient services; do you have an anaesthetist with up to date eperience dealing with vascular emergencies available at all times? For In-patient services; do you have a nominated lead consultant anaesthetist identified for liaison with the vascular service? For In-patient service; do you have an interventional radiology service available at all times? Are all emergency and elective vascular interventional procedures undertaken by consultant vascular specialists or by staff under their supervision? And all vascular specialists undertaking sufficient a. Wound, ulcer and diabetic foot management b. Claudication, and lifestyle advice c. Amputation and liaison with rehabilitation and limb-fitting services d. Vascular access for patients with renal disease e. Aneurysms. 105
106 S2-08 S2-09 S2-10 S2-11 interventional procedures (operations or interventional radiology procedures) per annum to maintain competence. Are Endovascular aneurysm repairs and carotid stenting undertaken only by vascular specialists with competences in these procedures? Does your Trust have a vascular specialist and support staff with competences in interventional radiology available for all elective vascular radiology procedures? For In-patient services; do you have a member of staff with competences in vascular ultrasound available during normal working hours? At weekends is there a system for identifying patients needing vascular ultrasound as well as providing scanning, if required, on a daily basis? For In-patient services; Is there an inpatient ward available, staffed by nurses and HCAs with appropriate competences in care of patients with vascular disease? The competence framework should cover at least: a. Acute Life-threatening Events Recognition and Treatment (ALERT) b. Tissue viability and wound care c. Pain management d. Care of patients with diabetes e. High dependency care f. Care of patients with disabilities, including patients with amputations. 106
107 Support Services S3-01 S3-02 S3-03 S3-04 S3-05 For In-patient services; Are physiotherapy services available daily with time allocated for their work with in-patients with vascular disease? In-patient services; Is there access to the following services available for inpatients with vascular disease? Is there Vascular ultrasound available for all vascular out-patient services? Are there In-patient and communitybased rehabilitation services available with epertise in the care of patients with vascular disease, including amputees, including at least; Is there sufficient administrative, clerical and data collection support available? a. Occupational therapy b. Social work. a. Physiotherapy b. Occupational therapy c. Limb fitting and orthoses. 107
108 Facilities and Equipment S4-01 S4-02 S4-03 S4-04 S4-05 For In-patient services, are the following facilities and services available at all times: For In-patient services, is there magnetic resonance angiography available during normal working hours? For In-patient services, are there Inpatient wards for patients with vascular disease that have: Is there a theatre where all vascular surgery takes place with: Are there elective clinic and theatre sessions for patients needing permanent dialysis access sufficient to meet the needs of local patients with end stage renal failure? a. Emergency theatre b. Vascular angiography suite c. Spiral CT d. Critical care (at least level 3) e. Haematology (for urgent cross-match and blood products) f. Blood biochemistry and blood gas analysis g. Facilities for electronic transfer of imaging from, or ability remotely to view imaging at, other acute hospitals within the catchment area of the vascular service (DZ-607). a. Hand-held Doppler ultrasound machine b. Portable duple device. a. Theatre staff trained in vascular instruments, prosthetics and techniques and in the use of cell salvage devices for blood conservation b. Stocks of grafts, instruments and sutures required for patients with vascular disease c. Radiolucent operating tables and X-ray C- arms d. Hand-held Doppler ultrasound machine and portable duple devices e. Access to blood and blood products. 108
109 Guidelines and Protocols S4-06 S5-01 Do all vascular out-patient clinics have: Does your Trust have clinical guidelines agreed with the ambulance service covering the clinical indications for taking emergency patients to the hospital/s providing in-patient vascular services and the patients who may be taken to Emergency Departments without on-site in-patient vascular services? Are there clinical guidelines in use throughout the vascular service covering assessment and management of: S5-02 Do these guidelines cover: a. Hand-held Doppler ultrasound machine b. Portable duple scanner c. Facilities to perform ankle brachial pressure tests. a. Abdominal aortic aneurysm b. Carotid artery disease c. Diabetic foot d. Leg ulcers e. Claudication f. Varicose veins g. Limb-threatening ischaemia h. Lymphoedema. a. Investigations b. Lifestyle advice c. Treatment options available, including surgical and radiological interventions and conservative options d. Indications for choice of treatment e. Pre-operative assessment f. Post-operative monitoring g. Management of side-effects and complications of treatment h. Follow up arrangements i. Referral for rehabilitation j. Responsibilities for giving information to patients and carers (QSDN-101). 109
110 Guidelines and Protocols S5-03 S5-04 S5-05 S5-06 S5-07 S5-08 S5-09 S5-10 Does your Trust provide guidelines on lifestyle advice for all patients covering, at least: Does your Trust provide clinical guidelines on monitoring and management of peripheral arterial disease risk factors covering, at least: Does your Trust provide clinical guidelines on the management of patients with diabetes covering, at least: Does your Trust provide Clinical guidelines on the management of patients with, or at risk of, impaired renal function, including: Is there a protocol for by-pass graft surveillance in place? Are there clinical guidelines in use covering indications for involvement of cardiology services in the care of patients with vascular disease? Are there clinical guidelines in use covering indications and arrangements for referral for psychological support? Is there a local policy covering ultrasound screening of relatives of patients with abdominal aortic aneurysm? a. Support for smoking cessation b. Dietary advice c. Programmes of physical activity and weight management. a. Anti-platelet therapy b. Lipid reduction therapy c. Control of hypertension a. Management of ischaemia and sepsis in patients with diabetes b. Peri-operative management of patients with diabetes c. Indications for involvement of the diabetes service in the care of the patient. a. Indications for involvement of the renal service in the care of the patient b. Prevention and management of complications. 110
111 Guidelines and Protocols Service organisation and liaison with other services S5-11 S5-12 S5-13 S5-14 S6-01 S6-02 Are there discharge planning guidelines in use covering, at least: Are there guidelines, agreed with the specialist palliative care services serving the local population, in use covering, at least: Does your Trust have a protocol on driving advice in use, covering establishing the type of licence and giving appropriate advice on DVLA notification? Is the Trusts vascular service aware of local guidelines for end of life care? Does your Trust have a multidisciplinary team meeting to review the care of patients with vascular disease held at least weekly involving at least: For In-patient services, does your Trust have a ward-based multidisciplinary team meeting to discuss the care of patients with comple rehabilitation and discharge needs held at least weekly involving at least: a. Discharge to rehabilitation facilities (QSDN- 304) b. Discharge home with support from local rehabilitation facilities (QSDN-304) c. Referral to limb-fitting service d. Communication with the patient s GP. a. Arrangements for accessing advice and support from the specialist palliative care team. b. Indications for referral of patients to the specialist palliative care team. c. Arrangements for shared care between the vascular service and palliative care services. a. Vascular specialists b. Imaging staff regularly involved with the care of patients with vascular disease c. Specialist nurses (QSDN-202). a. Ward manager b. Nurse with specialist epertise in care of patients with amputations (QSDN-202) c. Physiotherapy (QSDN-301) d. Occupational therapy (QSDN-302) e. Social work (QSDN-302). 111
112 Service organisation and liaison with other services Governance S6-03 S6-04 S6-05 S6-06 S7-01 S7-02 Do the consultant and nurse representatives of the vascular service participate regularly in multidisciplinary meetings with services responsible for the care of: Are there Multi-disciplinary clinics for assessment of patients with diabetes and comple foot problems held involving: Is there a meeting with local rehabilitation services (QSDN-304) held at least annually to review the links with the vascular service and address any problems identified? Does the vascular surgery service at your Trust offer a session on the assessment of vascular emergencies for Emergency Department staff, general surgeons, GPs and ambulance staff at least annually? Is the vascular service at your Trust collecting and submitting data to the National Vascular Database (all inde procedures) and British Society of Interventional Radiology Registries? Does the vascular service at your Trust have an annual programme of audits covering at least: a. Patients with renal disease b. Patients with stroke or TIA c. Patients with thoracic aneurysms. a. Vascular surgeons b. Diabetes services c. Orthopaedic services d. Orthotic services e. Podiatry services. a. Number of interventional procedures (surgical and interventional radiology) undertaken by each vascular specialist across the service s catchment area. b. Medical management of patients with peripheral vascular disease. c. Compliance with evidence-based guidelines. 112
113 Governance S7-03 S7-04 Does the service in your Trust currently produce an annual report summarising activity, compliance with quality standards and clinical outcome? If so, does the report identify actions required to meet epected quality standards and progress since the previous year s annual report? Do all policies, procedures and guidelines comply with Trust document control procedures? 113

114 Appendi 3 Advanced Travel Analysis The service uses the Navteq Premium 2006 road network dataset, which includes turn restrictions. The service uses road traffic speeds provided by Journey Dynamics whereby each road link has an actual average traversal speed calculated based on analysis of 5 years of traffic information for all types of vehicles from cars to HGVs at 5 minute intervals, 365 days per year, as at There are multiple routes that can be used to get from point A to point B and these have been factored into the route calculations and make use of the patent pending algorithms from Cambridge Vehicle Information Technology (CAMVIT). The maps show the travel times for 45, 60 and 90 minutes from each site these maps with the isochrones are important as they show travelling distances achievable to/from each site. 114


115 115

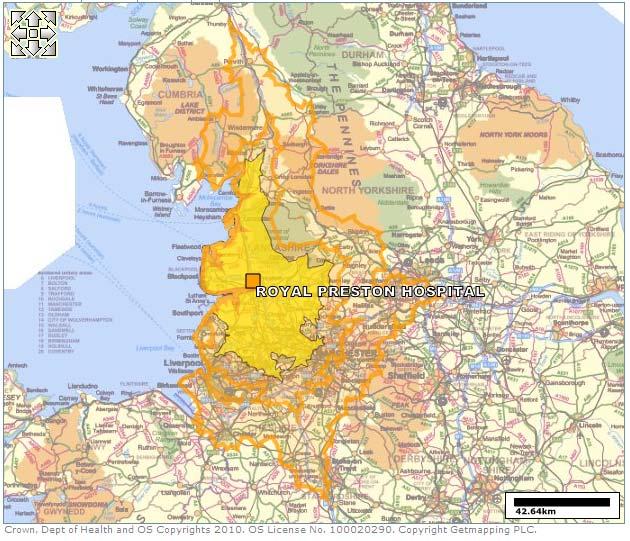
116 116


117 117

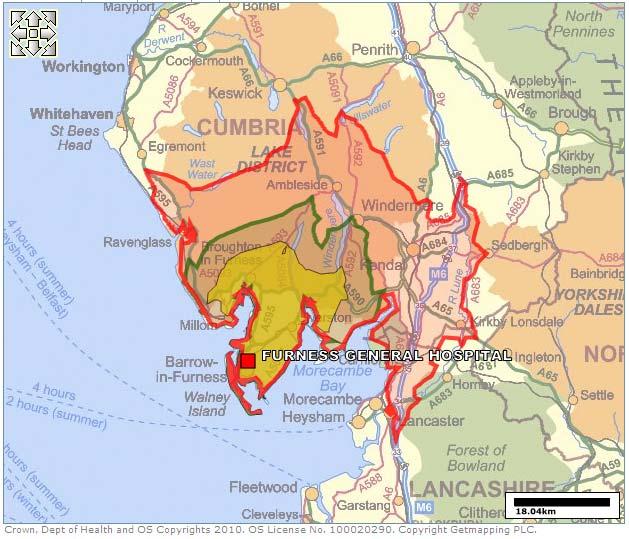
118 118


119 119
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD
 UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD Date of meeting: 25 July 2012 Title / Subject: Vascular Services at UHMBFT; the Impact of Centralising Inpatient and Emergency Vascular
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD Date of meeting: 25 July 2012 Title / Subject: Vascular Services at UHMBFT; the Impact of Centralising Inpatient and Emergency Vascular
SERVICE SPECIFICATION 2 Vascular Access
 SERVICE SPECIFICATION 2 Vascular Access Table of Contents Page 1 Key Messages 1 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies with other specialties
SERVICE SPECIFICATION 2 Vascular Access Table of Contents Page 1 Key Messages 1 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies with other specialties
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES
 GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES") PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification. 12 months
 E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
COMMON GROUND EAST REGION. DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing
 COMMON GROUND EAST REGION DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing SEPTEMBER 2018 1 COMMON GROUND It is fitting that in the 70th anniversary year of our National
COMMON GROUND EAST REGION DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing SEPTEMBER 2018 1 COMMON GROUND It is fitting that in the 70th anniversary year of our National
Delivering surgical services: options for maximising resources
 Delivering surgical services: options for maximising resources THE ROYAL COLLEGE OF SURGEONS OF ENGLAND March 2007 2 OPTIONS FOR MAXIMISING RESOURCES The Royal College of Surgeons of England Introduction
Delivering surgical services: options for maximising resources THE ROYAL COLLEGE OF SURGEONS OF ENGLAND March 2007 2 OPTIONS FOR MAXIMISING RESOURCES The Royal College of Surgeons of England Introduction
NHS GREATER GLASGOW AND CLYDE Vale of Leven Hospital REVIEW OF ANAESTHETIC SERVICES
 NHS GREATER GLASGOW AND CLYDE Vale of Leven Hospital REVIEW OF ANAESTHETIC SERVICES 1. Purpose of Paper 1.1 In September 2006 at the time of considering services within Clyde by the Greater Glasgow and
NHS GREATER GLASGOW AND CLYDE Vale of Leven Hospital REVIEW OF ANAESTHETIC SERVICES 1. Purpose of Paper 1.1 In September 2006 at the time of considering services within Clyde by the Greater Glasgow and
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
Excellence and Choice. Right Treatment, Right Place A Consultation on a Proposal to Reorganise the Delivery of Acute Services in Belfast
 Excellence and Choice Right Treatment, Right Place A Consultation on a Proposal to Reorganise the Delivery of Acute Services in Belfast VASCULAR SURGERY 5 July 31 October 2010 Contents Foreword Patricia
Excellence and Choice Right Treatment, Right Place A Consultation on a Proposal to Reorganise the Delivery of Acute Services in Belfast VASCULAR SURGERY 5 July 31 October 2010 Contents Foreword Patricia
Introducing a 7-day service: the benefits of increased consultant presence
 Introducing a 7-day service: the benefits of increased consultant presence This Future Hospital Programme case study comes from Wrightington, Wigan & Leigh NHS Foundation Trust (WWL). Here, Dr Stephen
Introducing a 7-day service: the benefits of increased consultant presence This Future Hospital Programme case study comes from Wrightington, Wigan & Leigh NHS Foundation Trust (WWL). Here, Dr Stephen
DRAFT 2. Specialised Paediatric Services in Scotland. 1 Specialised Services Definition
 Specialised Paediatric Services in Scotland 1 Specialised Services Definition Services provided for low numbers of patients. They require a critical mass of staff, facilities and equipment and are delivered
Specialised Paediatric Services in Scotland 1 Specialised Services Definition Services provided for low numbers of patients. They require a critical mass of staff, facilities and equipment and are delivered
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule
 Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
Separating emergency and elective surgical care: Recommendations for practice
 Separating emergency and elective surgical care: Recommendations for practice THE ROYAL COLLEGE OF SURGEONS OF ENGLAND September 2007 2 SEPARATING EMERGENCY AND ELECTIVE SURGICAL CARE The Royal College
Separating emergency and elective surgical care: Recommendations for practice THE ROYAL COLLEGE OF SURGEONS OF ENGLAND September 2007 2 SEPARATING EMERGENCY AND ELECTIVE SURGICAL CARE The Royal College
@ncepod #tracheostomy
 @ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
@ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
Daisy Hill Hospital Profile
 Daisy Hill Hospital Profile 2012 Daisy Hill Hospital Profile Mairead McAlinden, Southern Trust Chief Executive, and Chair Roberta Brownlee welcome Health Minister Edwin Poots on a recent visit to Daisy
Daisy Hill Hospital Profile 2012 Daisy Hill Hospital Profile Mairead McAlinden, Southern Trust Chief Executive, and Chair Roberta Brownlee welcome Health Minister Edwin Poots on a recent visit to Daisy
A healthier Lancashire and South Cumbria
 A healthier Lancashire and South Cumbria Improving health and care for local people Published May 2017 Bay Health & Care Partners Pennine Lancashire Fylde Coast West Lancashire Central Lancashire Healthier
A healthier Lancashire and South Cumbria Improving health and care for local people Published May 2017 Bay Health & Care Partners Pennine Lancashire Fylde Coast West Lancashire Central Lancashire Healthier
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Data, analysis and evidence
 1 New Congenital Heart Disease Review Data, analysis and evidence Joanna Glenwright 2 New Congenital Heart Disease Review Evidence for standards Joanna Glenwright Evidence to inform the service standards
1 New Congenital Heart Disease Review Data, analysis and evidence Joanna Glenwright 2 New Congenital Heart Disease Review Evidence for standards Joanna Glenwright Evidence to inform the service standards
OPERATIONAL POLICY DOCUMENT FOR THE DIALYSIS UNIT WARD 20 UNIVERSITY HOSPITAL AINTREE
 OPERATIONAL POLICY DOCUMENT FOR THE DIALYSIS UNIT WARD 20 UNIVERSITY HOSPITAL AINTREE CHRISTINE JONES RENAL SPECIALIST NURSE JANUARY 2005 UNIVERSITY HOSPITAL AINTREE OPERATIONAL POLICY DIALYSIS UNIT WARD
OPERATIONAL POLICY DOCUMENT FOR THE DIALYSIS UNIT WARD 20 UNIVERSITY HOSPITAL AINTREE CHRISTINE JONES RENAL SPECIALIST NURSE JANUARY 2005 UNIVERSITY HOSPITAL AINTREE OPERATIONAL POLICY DIALYSIS UNIT WARD
Portsmouth Hospitals NHS Trust Individual Placement (Job) Descriptions for Foundation Year 1
 Descriptions for Foundation Year 1") Portsmouth Hospitals NHS Trust Individual Placement (Job) Descriptions for Foundation Year 1 Placement The department Where the is for the in this F1 Acute Placement Acute Medicine Unit/Surgical Assessment
Portsmouth Hospitals NHS Trust Individual Placement (Job) Descriptions for Foundation Year 1 Placement The department Where the is for the in this F1 Acute Placement Acute Medicine Unit/Surgical Assessment
Integrated heart failure service working across the hospital and the community
 Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
NHS. Challenges and improvements in diagnostic services across seven days. Improving Quality
 NHS Improving Quality NHS Improving Quality working in partnership with NHS England Challenges and improvements in diagnostic services across seven days 2 Foreword Across the country, hospitals and primary
NHS Improving Quality NHS Improving Quality working in partnership with NHS England Challenges and improvements in diagnostic services across seven days 2 Foreword Across the country, hospitals and primary
OPTIONS APPRAISAL PAPER FOR DEVELOPING A SUSTAINABLE AND EFFECTIVE ORTHOPAEDIC SERVICE IN NHS WESTERN ISLES
 Highland NHS Board 9 August 2011 Item 4.3 OPTIONS APPRAISAL PAPER FOR DEVELOPING A SUSTAINABLE AND EFFECTIVE ORTHOPAEDIC SERVICE IN NHS WESTERN ISLES Report by Sheila Cascarino, Divisional Manager, Surgical
Highland NHS Board 9 August 2011 Item 4.3 OPTIONS APPRAISAL PAPER FOR DEVELOPING A SUSTAINABLE AND EFFECTIVE ORTHOPAEDIC SERVICE IN NHS WESTERN ISLES Report by Sheila Cascarino, Divisional Manager, Surgical
North Cumbria Clinical Strategy NHS Cumbria & North Cumbria University Hospitals NHS Trust
 North Cumbria Clinical Strategy NHS Cumbria & North Cumbria University Hospitals NHS Trust March 2011 North Cumbria Reconfiguration Plan: Clinical Strategy 1 Foreword This document describes a clinical
North Cumbria Clinical Strategy NHS Cumbria & North Cumbria University Hospitals NHS Trust March 2011 North Cumbria Reconfiguration Plan: Clinical Strategy 1 Foreword This document describes a clinical
Consultation Paper. Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network
 Consultation Paper Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network Issued: April 2016 TABLE OF CONTENTS TABLE OF CONTENTS 2 1. INTRODUCTION 3 2. PURPOSE
Consultation Paper Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network Issued: April 2016 TABLE OF CONTENTS TABLE OF CONTENTS 2 1. INTRODUCTION 3 2. PURPOSE
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Oldham Council Provision of NHS Health Checks Programme in Partnership with Local GP Practices
 Oldham Council Provision of NHS Health Checks Programme in Partnership with Local GP Practices 1. Population Needs 1. NATIONAL AND LOCAL CONTEXT 1.1 NATIONAL CONTEXT 1.1.1 Overview of commissioning responsibilities
Oldham Council Provision of NHS Health Checks Programme in Partnership with Local GP Practices 1. Population Needs 1. NATIONAL AND LOCAL CONTEXT 1.1 NATIONAL CONTEXT 1.1.1 Overview of commissioning responsibilities
FINAL HEALTH FOUNDATION REPORT
 THE VASCULAR SOCIETY OF GREAT BRITAIN AND IRELAND NATIONAL ABDOMINAL AORTIC ANEURYSM QUALITY IMPROVEMENT PROGRAMME FINAL HEALTH FOUNDATION REPORT APRIL 2012 Closing the Gap through Clinical Communities
THE VASCULAR SOCIETY OF GREAT BRITAIN AND IRELAND NATIONAL ABDOMINAL AORTIC ANEURYSM QUALITY IMPROVEMENT PROGRAMME FINAL HEALTH FOUNDATION REPORT APRIL 2012 Closing the Gap through Clinical Communities
Health and Care Framework
 Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation (Trust) Team MVCN LUTON AND DUNSTABLE Luton & Dunstable Colorectal MDT (11-2D-1) - 2011/12 Peer Review Visit Date 11th November 2011
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation (Trust) Team MVCN LUTON AND DUNSTABLE Luton & Dunstable Colorectal MDT (11-2D-1) - 2011/12 Peer Review Visit Date 11th November 2011
TRUST BOARD SEPTEMBER Surgical Services Reconfiguration
 def Agenda item: 8 (i) TRUST BOARD SEPTEMBER 2011 Surgical Services Reconfiguration PURPOSE: PREVIOUSLY CONSIDERED BY: To provide the Trust Board with an update on plans to reconfigure the Trust s surgical
def Agenda item: 8 (i) TRUST BOARD SEPTEMBER 2011 Surgical Services Reconfiguration PURPOSE: PREVIOUSLY CONSIDERED BY: To provide the Trust Board with an update on plans to reconfigure the Trust s surgical
North West COPD Report Nov 2011
 North West COPD Report Nov 2011 Working together to improve respiratory care in the North West 1 Contents Introduction foreword by NW Respiratory Leads... 3 4 reasons why COPD is important in the North
North West COPD Report Nov 2011 Working together to improve respiratory care in the North West 1 Contents Introduction foreword by NW Respiratory Leads... 3 4 reasons why COPD is important in the North
Advanced Roles and Workforce Planning. Sara Dalby SFA, ANP, SCP Associate Lecturer Winston Churchill Fellow
 Advanced Roles and Workforce Planning Sara Dalby SFA, ANP, SCP Associate Lecturer Winston Churchill Fellow Confusion of Advanced Roles Clinical Support Worker (CSW) Nurse Practitioner (NP) Physicians Associate
Advanced Roles and Workforce Planning Sara Dalby SFA, ANP, SCP Associate Lecturer Winston Churchill Fellow Confusion of Advanced Roles Clinical Support Worker (CSW) Nurse Practitioner (NP) Physicians Associate
Yvonne Blucher, Managing Director Southend University Hospital. Michael Catling, Cancer Programme Director MSB
 Meeting Title Mid and South Essex Acute Trusts Joint Working Board (meeting in public) Meeting Date 18 th October 2017 Agenda No 10 Report Title Oncology Service Report Lead Executive Director Report Author
Meeting Title Mid and South Essex Acute Trusts Joint Working Board (meeting in public) Meeting Date 18 th October 2017 Agenda No 10 Report Title Oncology Service Report Lead Executive Director Report Author
NHS SERVICE DELIVERY AND ORGANISATION R&D PROGRAMME PROGRAMME OF RESEARCH ON EVALUATING MODELS OF SERVICE DELIVERY
 NHS SERVICE DELIVERY AND ORGANISATION R&D PROGRAMME PROGRAMME OF RESEARCH ON EVALUATING MODELS OF SERVICE DELIVERY EVALUATION OF CONFIGURING HOSPITALS PILOTS Background There is currently a wide-ranging
NHS SERVICE DELIVERY AND ORGANISATION R&D PROGRAMME PROGRAMME OF RESEARCH ON EVALUATING MODELS OF SERVICE DELIVERY EVALUATION OF CONFIGURING HOSPITALS PILOTS Background There is currently a wide-ranging
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Neurosurgery. Themes. Referral
 06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Hip replacements: an update. REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 956 Session : 17 July 2003
 Hip replacements: an update REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 956 Session 2002-2003: 17 July 2003 The National Audit Office scrutinises public spending on behalf of Parliament. The Comptroller
Hip replacements: an update REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 956 Session 2002-2003: 17 July 2003 The National Audit Office scrutinises public spending on behalf of Parliament. The Comptroller
Specialised Services Service Specification. Adult Congenital Heart Disease
 Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
Golden Jubilee National Hospital. Leading Quality, Research. and. Innovation
 Golden Jubilee National Hospital Leading Quality, Research and Innovation W ELCOME to the Golden Jubilee National Hospital campus As Scotland s flagship health facility, the Golden Jubilee National Hospital
Golden Jubilee National Hospital Leading Quality, Research and Innovation W ELCOME to the Golden Jubilee National Hospital campus As Scotland s flagship health facility, the Golden Jubilee National Hospital
Supporting the acute medical take: advice for NHS trusts and local health boards
 Supporting the acute medical take: advice for NHS trusts and local health boards Purpose of the statement The acute medical take has proven to be a challenge across acute hospital trusts and health boards
Supporting the acute medical take: advice for NHS trusts and local health boards Purpose of the statement The acute medical take has proven to be a challenge across acute hospital trusts and health boards
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
Tele Stroke ( Telemedicine in Practice)
") Tele Stroke ( Telemedicine in Practice) Site Royal Surrey County Hospital East Surrey Hospital Frimley Park Hospital NHS Foundation Trust Ashford and St Peter's Hospital NHS Trust Epsom Hospital Surrey
Tele Stroke ( Telemedicine in Practice) Site Royal Surrey County Hospital East Surrey Hospital Frimley Park Hospital NHS Foundation Trust Ashford and St Peter's Hospital NHS Trust Epsom Hospital Surrey
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience
 Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience Jeffrey G. Carr, MD, FACC, FSCAI Founding and Immediate Past President- Outpatient Endovascular and Interventional
Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience Jeffrey G. Carr, MD, FACC, FSCAI Founding and Immediate Past President- Outpatient Endovascular and Interventional
European Working Time Directive
 European Working Time Directive Summary of positions of other postgrad training bodies, and issues specific to Faculty of Radiologists, RCSI Introduction: Efforts are being made to implement The European
European Working Time Directive Summary of positions of other postgrad training bodies, and issues specific to Faculty of Radiologists, RCSI Introduction: Efforts are being made to implement The European
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
Paediatric Cardiac and Adult Congenital Heart Disease Compliance Assessment. University Hospitals of Leicester NHS Trust. 7 th November 2016
 Paediatric Cardiac and Adult Congenital Heart Disease Compliance Assessment University Hospitals of Leicester NHS Trust 7 th November 2016 University Hospitals of Leicester NHS Trust welcomes the opportunity
Paediatric Cardiac and Adult Congenital Heart Disease Compliance Assessment University Hospitals of Leicester NHS Trust 7 th November 2016 University Hospitals of Leicester NHS Trust welcomes the opportunity
Pre Assessment Policy. Trust Policy Forum March 2004
 Policy No: OP19 Version 1.0 Name of Policy: Pre Assessment Policy Effective From: March 2004 Approved by: Trust Policy Forum March 2004 Next Review Date: March 2005 Reviewed by: This policy supercedes
Policy No: OP19 Version 1.0 Name of Policy: Pre Assessment Policy Effective From: March 2004 Approved by: Trust Policy Forum March 2004 Next Review Date: March 2005 Reviewed by: This policy supercedes
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Domain 5 Cardiothoracic Standards RCoA Accreditation 2017
 1 PRIORITY The Care Pathway 5.4.1.1 The process for preoperative assessment presenting for cardiac and thoracic patients (including thoracic aortic) is defined within the patient pathway. 1 A clinical
1 PRIORITY The Care Pathway 5.4.1.1 The process for preoperative assessment presenting for cardiac and thoracic patients (including thoracic aortic) is defined within the patient pathway. 1 A clinical
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Proposals to implement standards for congenital heart disease services for children and adults in England - Consultation Summary
 Proposals to implement standards for congenital heart disease services for children and adults in England - Consultation Summary Proposals to implement standards for congenital heart disease for children
Proposals to implement standards for congenital heart disease services for children and adults in England - Consultation Summary Proposals to implement standards for congenital heart disease for children
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Agenda for the next Government
 Agenda for the next Government General election 2017 The Richmond Group of Charities We are the Richmond Group of Charities and we help people of all ages who have serious long term physical and mental
Agenda for the next Government General election 2017 The Richmond Group of Charities We are the Richmond Group of Charities and we help people of all ages who have serious long term physical and mental
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Specialty Doctor in Emergency Medicine
 Specialty Doctor in Emergency Medicine DETAILS OF THE POST JOB DESCRIPTION Job Title Specialty Doctor in Emergency Medicine. Background Information of the Trust Wrightington, Wigan and Leigh NHS Foundation
Specialty Doctor in Emergency Medicine DETAILS OF THE POST JOB DESCRIPTION Job Title Specialty Doctor in Emergency Medicine. Background Information of the Trust Wrightington, Wigan and Leigh NHS Foundation
The Royal Wolverhampton Hospitals NHS Trust
 The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
Visit to Hull & East Yorkshire Hospitals NHS Trust
 Yorkshire and the Humber regional review 2014 15 Visit to Hull & East Yorkshire Hospitals NHS Trust This visit is part of a regional review and uses a risk-based approach. For more information on this
Yorkshire and the Humber regional review 2014 15 Visit to Hull & East Yorkshire Hospitals NHS Trust This visit is part of a regional review and uses a risk-based approach. For more information on this
Purpose of the Report: Update to the Trust Board on the clinically-led Trauma and Orthopaedic GIRFT review. Information Assurance X
 Item 9.4 To: Trust Board From: Mark Brassington Date: 18 th May 2018 Healthcare Standard Title: Trauma and Orthopaedic GIRFT Author: Richard James, General Manager Responsible Director/s: Mark Brassington
Item 9.4 To: Trust Board From: Mark Brassington Date: 18 th May 2018 Healthcare Standard Title: Trauma and Orthopaedic GIRFT Author: Richard James, General Manager Responsible Director/s: Mark Brassington
2017/18 and 2018/19 National Tariff Payment System Annex E: Guidance on currencies without national prices. NHS England and NHS Improvement
 2017/18 and 2018/19 National Tariff Payment System Annex E: Guidance on currencies without national prices NHS England and NHS Improvement December 2016 Contents 1. Introduction... 3 2. Critical care adult
2017/18 and 2018/19 National Tariff Payment System Annex E: Guidance on currencies without national prices NHS England and NHS Improvement December 2016 Contents 1. Introduction... 3 2. Critical care adult
AMP Health and Social Care Professional Implementation Group Update
 AMP Health and Social Care Professional Implementation Group Update November 2016 Welcome to another update from the National Acute Medicine Programme s Health and Social Care Professionals Implementation
AMP Health and Social Care Professional Implementation Group Update November 2016 Welcome to another update from the National Acute Medicine Programme s Health and Social Care Professionals Implementation
1. JOB PURPOSE. 2. ORGANISATIONAL POSITION Professor Nancy Fontaine. Job advertised. Deputy Chief Executive Chief Nurse
 Job Title: Vascular Nurse Practitioner/ Vascular Diabetic Foot Nurse Practitioner ( VNP) Band: 7 Reporting To: Head of Surgical Nursing and Vascular Consultants Department(s)/Location: Vascular Unit PAH
Job Title: Vascular Nurse Practitioner/ Vascular Diabetic Foot Nurse Practitioner ( VNP) Band: 7 Reporting To: Head of Surgical Nursing and Vascular Consultants Department(s)/Location: Vascular Unit PAH
Can we monitor the NHS plan?
 Can we monitor the NHS plan? Alison Macfarlane In The NHS plan, published in July 2000, the government set out a programme of investment and change 'to give the people of Britain a service fit for the
Can we monitor the NHS plan? Alison Macfarlane In The NHS plan, published in July 2000, the government set out a programme of investment and change 'to give the people of Britain a service fit for the
Aneurin Bevan University Health Board Stroke Services Redesign Programme
 Aneurin Bevan University Health Board Services Redesign Programme 1 Introduction This report aims to update the Health Board on progress with the Services Redesign Programme of work which commenced in
Aneurin Bevan University Health Board Services Redesign Programme 1 Introduction This report aims to update the Health Board on progress with the Services Redesign Programme of work which commenced in
Evidence on the quality of medical note keeping: Guidance for use at appraisal and revalidation
 Health Informatics Unit Evidence on the quality of medical note keeping: Guidance for use at appraisal and revalidation April 2011 Funded by: Acknowledgements This project was funded by the Academy of
Health Informatics Unit Evidence on the quality of medical note keeping: Guidance for use at appraisal and revalidation April 2011 Funded by: Acknowledgements This project was funded by the Academy of
Overview. Dr Stephen Gulliford & AKI Specialist Nurse Suzanne Wilson Page 1
 Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Recommendations of the NH Strategy
 Urgent care Newark Hospital should continue to provide sub-acute care1, based on the existing ambulance diversion protocol. Refine the ambulance protocol to include additional sub-acute presentations that
Urgent care Newark Hospital should continue to provide sub-acute care1, based on the existing ambulance diversion protocol. Refine the ambulance protocol to include additional sub-acute presentations that
Profile The following information reflects responses from 46 vascular surgeons who completed the 2003 Pathway Physician's Survey.
 VASCULAR SURGERY Vascular surgery is a subspecialty within general surgery that addresses the diagnosis and treatment of diseases of the vascular tree, including arteries, veins, and lymphatic vessels,
VASCULAR SURGERY Vascular surgery is a subspecialty within general surgery that addresses the diagnosis and treatment of diseases of the vascular tree, including arteries, veins, and lymphatic vessels,
Better Healthcare in Bucks Reconfiguring acute services
 service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
Business Case Authorisation Cover Sheet
 Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
The Health of the Humber 2015
 The Health of the Humber 2015 Report to the LEP Board, 13 th November 2015 Report from Lance Gardner, Board Member & Chief Executive, Care Plus Group 1. Summary 1.1. This paper explores the main challenges
The Health of the Humber 2015 Report to the LEP Board, 13 th November 2015 Report from Lance Gardner, Board Member & Chief Executive, Care Plus Group 1. Summary 1.1. This paper explores the main challenges
Catherine Hughson Kathryn Kearney Number of supervisors relinquishing role since last report:
 Name of Local Supervising Authority: Western Isles Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising Authority
Name of Local Supervising Authority: Western Isles Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising Authority
Investing in the interventional radiology workforce: the quality and efficiency case
 www.rcr.ac.uk 1 Investing in the interventional radiology workforce: the quality and efficiency case 2 www.rcr.ac.uk Contents Executive summary 3 Statistics at a glance 4 1. Introduction 5 2. The role
www.rcr.ac.uk 1 Investing in the interventional radiology workforce: the quality and efficiency case 2 www.rcr.ac.uk Contents Executive summary 3 Statistics at a glance 4 1. Introduction 5 2. The role
Diagnostics FAQs. Frequently Asked Questions on completing the Diagnostic Waiting Times & Activity monthly data collection
 Diagnostics FAQs Frequently Asked Questions on completing the Diagnostic Waiting Times & Activity monthly data collection First published: October 2006 Updated: 02 February 2015 Prepared by Analytical
Diagnostics FAQs Frequently Asked Questions on completing the Diagnostic Waiting Times & Activity monthly data collection First published: October 2006 Updated: 02 February 2015 Prepared by Analytical
MEET THE ACADEMIC TEAM
 MEET THE ACADEMIC TEAM Lancashire Teaching Hospitals Royal Preston Hospital and Chorley District Hospital 2016-17 Dr Paul Marsden Consultant Physician in Respiratory Medicine & Honorary Lecturer Respiratory
MEET THE ACADEMIC TEAM Lancashire Teaching Hospitals Royal Preston Hospital and Chorley District Hospital 2016-17 Dr Paul Marsden Consultant Physician in Respiratory Medicine & Honorary Lecturer Respiratory
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11 PAGE 2 WE PLAN. WE ACHIEVE We achieve 2009/10 was another great year
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11 PAGE 2 WE PLAN. WE ACHIEVE We achieve 2009/10 was another great year
NHS England Congenital Heart Disease Provider Impact Assessment
 NHS England Congenital Heart Disease Provider Impact Assessment NHS England Congenital Heart Disease Provider Impact Assessment First published: 9 February 2017 Prepared by: Specialised Commissioning,
NHS England Congenital Heart Disease Provider Impact Assessment NHS England Congenital Heart Disease Provider Impact Assessment First published: 9 February 2017 Prepared by: Specialised Commissioning,
Having an angiogram/angioplasty
 Having an angiogram/angioplasty Department of Radiology Information for Patients i Radiology Leaflet No. 1 Contents Page number Introduction 3 Referral 3 What is an angiogram/angioplasty? 4 Are there any
Having an angiogram/angioplasty Department of Radiology Information for Patients i Radiology Leaflet No. 1 Contents Page number Introduction 3 Referral 3 What is an angiogram/angioplasty? 4 Are there any
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Borders. Intensive Psychiatric Care Units
 NHS Borders Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Borders Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Improvement advice to the Competition and Markets Authority Proposed merger of Burton Hospitals NHS Foundation Trust and Derby Teaching Hospitals
 NHS Improvement advice to the Competition and Markets Authority Proposed merger of Burton Hospitals NHS Foundation Trust and Derby Teaching Hospitals NHS Foundation Trust: Annex 1 February 2018 We support
NHS Improvement advice to the Competition and Markets Authority Proposed merger of Burton Hospitals NHS Foundation Trust and Derby Teaching Hospitals NHS Foundation Trust: Annex 1 February 2018 We support
anaesthetic services Chapter 15 Services for neuroanaesthesia and neurocritical care 2014 GUIDELINES FOR THE PROVISION OF ACSA REFERENCES
 Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
The PCT Guide to Applying the 10 High Impact Changes. A guide from NatPaCT
 The PCT Guide to Applying the 10 High Impact Changes A guide from NatPaCT DH INFORMATION READER BOX Policy HR/Workforce Management Planning Clinical Estates Performance IM&T Finance Partnership Working
The PCT Guide to Applying the 10 High Impact Changes A guide from NatPaCT DH INFORMATION READER BOX Policy HR/Workforce Management Planning Clinical Estates Performance IM&T Finance Partnership Working
Dalton Review RCR Clinical Radiology Proposal Radiology in the UK the case for a new service model July 2014
 Dalton Review RCR Clinical Radiology Proposal Radiology in the UK the case for a new service model July 2014 Radiology services in the UK are in crisis. The ever-increasing role of imaging in modern clinical
Dalton Review RCR Clinical Radiology Proposal Radiology in the UK the case for a new service model July 2014 Radiology services in the UK are in crisis. The ever-increasing role of imaging in modern clinical
Organisational Audit Questions - Links to recommendations, standards and evidence
 Question Quoted recommendation/ standard / evidence Source Notes Section 1 - Hospital characteristics 1. a) How many adult in-patient or overnight beds (including 23- hours stay) are currently available
Question Quoted recommendation/ standard / evidence Source Notes Section 1 - Hospital characteristics 1. a) How many adult in-patient or overnight beds (including 23- hours stay) are currently available
1.3 At the present time there are 370 post-graduate medical trainees within NHS Lanarkshire across all services
 APPENDIX 4 MODERNISING MEDICAL CAREERS 1. Background 1.1 Modernising Medical Careers (MMC) is a UK-wide reform of all postgraduate medical training involving introduction of a two-year foundation programme
APPENDIX 4 MODERNISING MEDICAL CAREERS 1. Background 1.1 Modernising Medical Careers (MMC) is a UK-wide reform of all postgraduate medical training involving introduction of a two-year foundation programme
TRUST BOARD. Date of Meeting: 10/05/2011 Enclosure: 10
 TRUST BOARD Date of Meeting: 10/05/2011 Enclosure: 10 Agenda Item No: 10.1 Title of Report: Organ Donation Activity Report Aims: To provide overview of organ donation activity in North Cumbria University
TRUST BOARD Date of Meeting: 10/05/2011 Enclosure: 10 Agenda Item No: 10.1 Title of Report: Organ Donation Activity Report Aims: To provide overview of organ donation activity in North Cumbria University
Visiting Professional Programme: Paediatric ICU
 Visiting Professional Programme: Paediatric ICU 1 Introduction The Guy s and St Thomas NHS Foundation Trust Paediatric ICU Visiting Professional Programme (VPP) is designed to provide international visiting
Visiting Professional Programme: Paediatric ICU 1 Introduction The Guy s and St Thomas NHS Foundation Trust Paediatric ICU Visiting Professional Programme (VPP) is designed to provide international visiting
ROLE OF OUT-OF-HOURS NURSE CO-ORDINATORS IN A CHILDREN S HOSPITAL
 Art & science The synthesis of art and science is lived by the nurse in the nursing act JOSEPHINE G PATERSON ROLE OF OUT-OF-HOURS NURSE CO-ORDINATORS IN A CHILDREN S HOSPITAL Amy Hensman and colleagues
Art & science The synthesis of art and science is lived by the nurse in the nursing act JOSEPHINE G PATERSON ROLE OF OUT-OF-HOURS NURSE CO-ORDINATORS IN A CHILDREN S HOSPITAL Amy Hensman and colleagues