@ncepod #tracheostomy
|
|
|
- Donna Holland
- 6 years ago
- Views:
Transcription
1 @ncepod #tracheostomy 1
2 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies has increased greatly in recent years Royal College of Anaesthetists, Difficult Airway Society, & the National Patient Safety Agency National Tracheostomy Safety Project/Global Tracheostomy Collaborative 2
3 Aim To explore factors surrounding the insertion and subsequent management of tracheostomies in both critical care and ward environments by: Exploring (percutaneous and surgical) tracheostomy-related complications following insertion in the operating theatre or the critical care unit Exploring remediable factors in the care of adult patients (aged 16 and over) undergoing the insertion of a surgical or percutaneous tracheostomy tube Assessing the number and variability of percutaneous tracheostomies performed annually in the critical care unit Making recommendations to improve future practice 3
4 Objectives Insertion of the tracheostomy Indications for the tracheostomy Cautions & contraindications Consent Delays Equipment & monitoring Staffing Anaesthesia Environment in which the tracheostomy tube was inserted & cared for 4
5 Objectives Routine care Essential equipment Cuff management Humidification Suctioning Inner cannula care Swallowing Oral care Communication needs Changing tracheostomy tubes 5
6 Objectives Emergencies, common complications and their management Decannulation and long term (30 day) follow up Facilities Staff capacity Staff competency Number of patients cared for Training Facilities available Policies & procedures 6
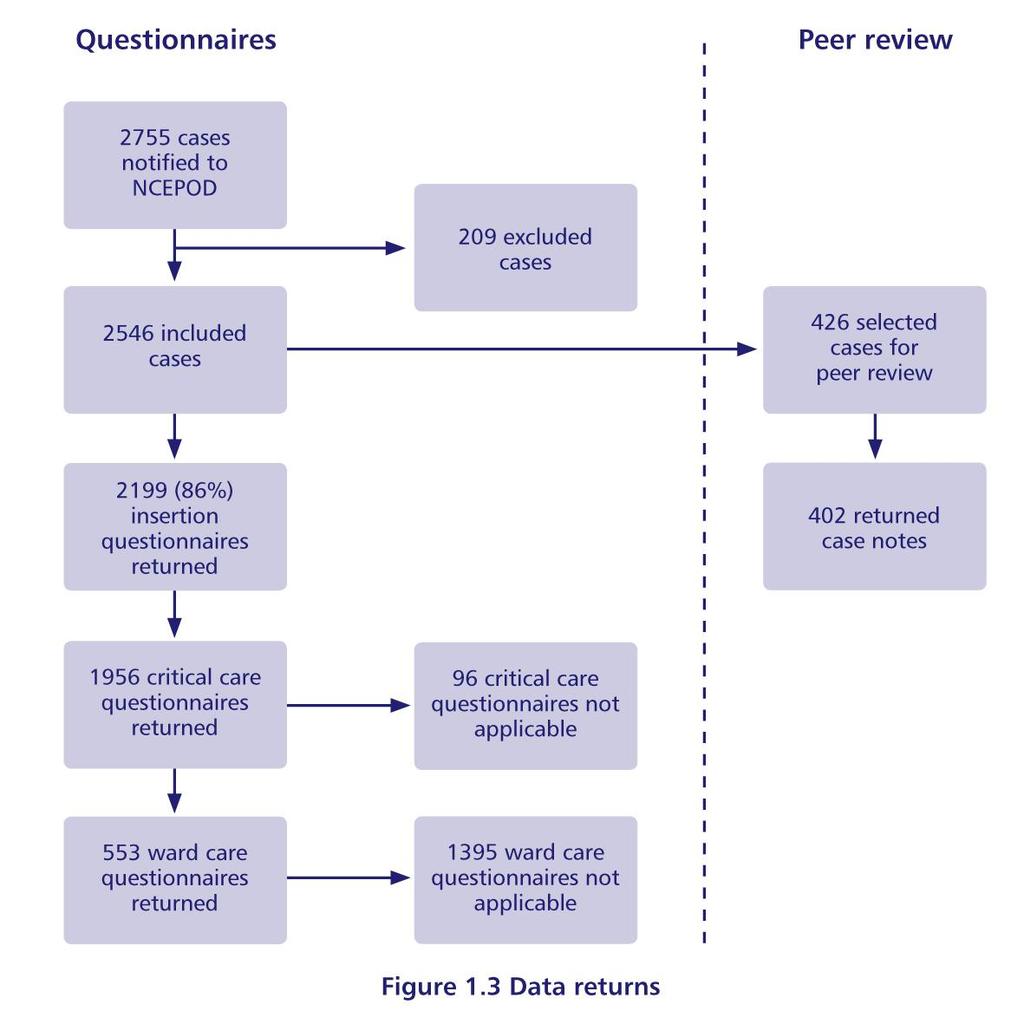
7 Method Hospital participation Study population th February 12 th May 2013 Case identification Prospective study At the point of tracheostomy insertion Study contact Critical care Theatre Ward 7
8 Method Questionnaires Insertion Critical care discharge Ward discharge Organisational Organisation of ward care 8
9 Method Case notes Inpatient annotations (main case notes) Nursing/speech and language therapy/ physiotherapy notes Intensive Care (Level 3)/High Dependency (Level 2) Unit notes Anaesthetic records Surgical/operation notes Observation charts Tracheostomy care records Ward discharge summaries Time period 9
10 10
11 Patient overview 11

12 Patient overview 12

13 Patient overview 13
14 Organisation of care 14
15 Organisation of care 15
16 Number of tracheostomies 187/219 (85.4%) sites provided data 101/186 (54.3%) estimate 82/186 (44.8% actual figure Range (average = 64) Critical care (average = 44) Theatre (average = 25) 16
17 Recommendation Tracheostomy insertion should be recorded and coded as an operative procedure. Data collection in all locations should be as robust as that for a theatre environment. 17
18 The insertion of tracheostomies 18

19 Urgency of admission 19
20 ASA prior to insertion 20
21 Patients location after admission 21
22 Patients location prior to insertion 22

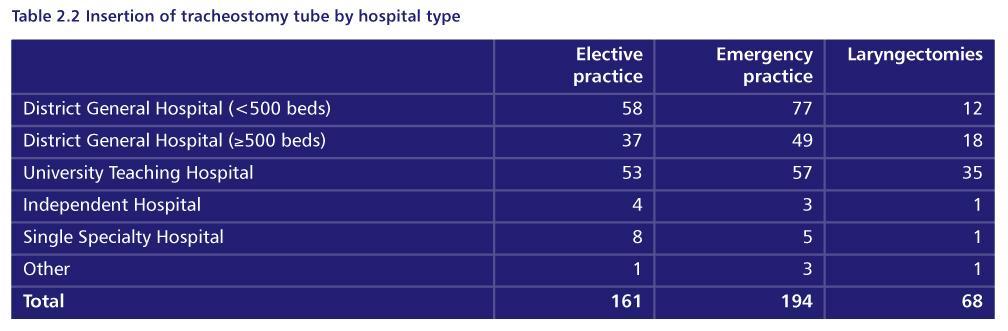
23 Type of insertion & urgency 23

24 Urgency of procedure 24

25 Day of insertion 25
26 Trials of extubation 26

27 Indication for tracheostomy 27
28 Documentation of airway difficulty 28

29 Difficult airway trolley 29
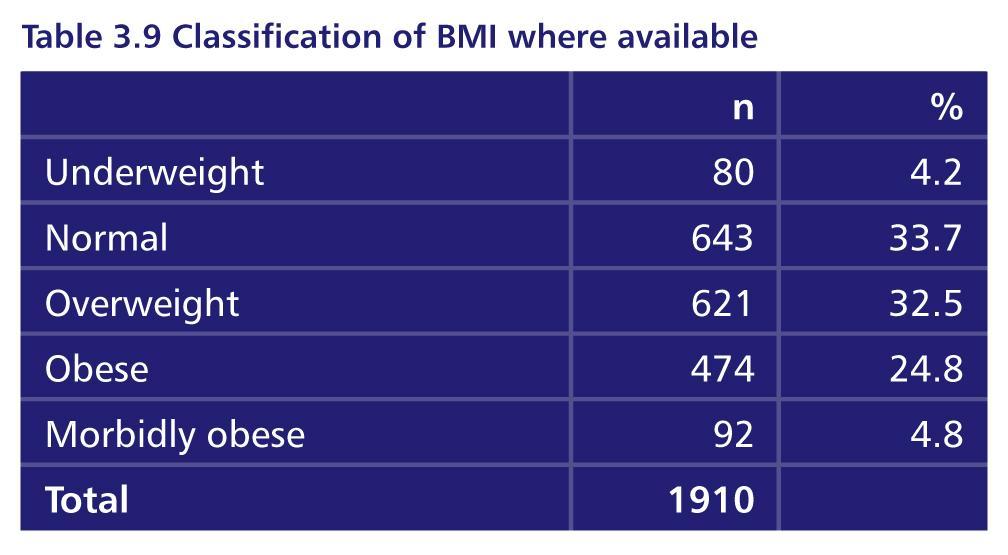
30 BMI 30
31 Case study An elderly and obese patient with sepsis and peritonitis was transferred to ICU following a Hartman s procedure. A consultant intensivist inserted a standard length percutaneous tracheostomy tube after 6 days because of failure to wean. The following day the patient de-saturated and suffered a PEA cardiac arrest whilst being positioned for physiotherapy. Thoracocentesis identified a tension pneumothorax. Advisors felt that the wrong sized tube had been used, and that there had been inadequate checking of tube position at insertion 31
32 Percutaneous tracheostomy insertion 32
33 Days between admission & insertion 33
34 Grade of clinician 34
35 Grade of clinician 35
36 Consent Consent form only completed in 728/1491 (48.8%) of patients undergoing a percutaneous tracheostomy insertion 36
37 Checklists Used in 239/1490 (16%) of percutaneous cases 37

38 Type of tube 38
39 Size of tube 39
40 How was the tube secured 40

41 Capnography at insertion 41
42 Case study An elderly obese patient with pneumonia underwent an attempted percutaneous tracheostomy. Bronchoscopy was performed and it was believed that the guidewire was identified within the tracheal lumen, however dilatation of the tract proved difficult and when the tube was inserted no CO2 was detected on capnography. The procedure was abandoned and the patient transferred to theatre for an open approach. This proved difficult due to the haematoma and oedema created by the attempted percutaneous tracheostomy, which had created a false passage. Advisors noted the importance careful pre-operative assessment and the value of capnography 42

43 Immediate complications 81/1482 (5.5%) 43
44 Surgical tracheostomy insertions 44

45 Indications for insertion 45
 Stridor noted in 86/596 (14.4%) Difficulty in intubation anticipated in 154/529 (29.")
46 Assessment of airway difficulty Recorded assessment of intubation difficulty in 318/488 (65.2%) Stridor noted in 86/596 (14.4%) Difficulty in intubation anticipated in 154/529 (29.1%) 46
47 Consent Form completed in 611/6387 (95.8%) patients 366/642 (57%) comatose or not awake 47

48 Location of operation 48
49 Seniority of anaesthetic staff Consultant anaesthetist in 534/607 (88.0%) Senior trainee in 53/607 (8.7%) Trainee present in 361/467 (77.3%) consultant cases Where the advisors could determine this information from the case notes, of 96 cases anaesthetised by trainee, supervision appropriate in all but 5 cases. 49
50 Seniority of surgical staff Consultant surgeon 397/630 (47.1%) Senior trainee in 260/630 (41.3%) Trainee present in 229/274 (83.6%) consultant cases Where the advisors could determine this information from the case notes, supervision appropriate in 91/99 50

51 Type of tube used 51

52 How was the tube secured? 52
53 Overall assessment 53

54 Area of care following insertion 54
55 Key findings Consent taken in 48.4% of percutaneous v 95.8% of surgical tracheostomies Checklists used in only 16% of percutaneous tracheostomies Adjustable length tubes used in 10.1% of cases overall and 18.8% of obese patients 20/217 (9.2%) hospitals did not have immediate access to a difficult airway trolley in the critical care unit 55
56 Recommendations Consent forms and checklists should be used prior to tracheostomy wherever it is performed Tube size and length should be appropriate Confirmation of tube placement must be obtained using capnography and documented Appropriate positioning of the tube should be confirmed and documented using airway endoscopy Critical care units need a rapidly available difficult airway trolley 56
57 Tube care in the patient with a tracheostomy 57

58 Day of week of tube change on critical care 58
59 First tube change in critical care 59
60 Timing of first tube change on ward 60

61 Early tube changes in critical care 61

62 Time of first tube change 62
63 Case study An elderly patient underwent emergency laparotomy for perforated duodenum and required post operative ventilation. A percutaneous tracheostomy was inserted by a surgeon and anaesthetist in theatre in a small DGH as the patient was obese and difficulties were anticipated. The patient suffered two episodes over the next 48 hours in which the tube was accidentally displaced. There was no documentation of how the tube was secured. Two weeks later the patient was successfully decannulated. Advisors commented upon the potential risks of early accidental decannulation in these circumstances. 63
64 Type of tube used at first tube change 64

65 BMI & type of tube used at first change 65
66 Case study A middle aged patient developed post operative multi-organ failure after planned bariatric surgery. A percutaneous tracheostomy was performed in the intensive care unit to assist with weaning. At insertion there was no documented capnography and an 8mm standard tube was inserted. The patient required an early tube change within 24 hours due to an immediate cuff leak. Advisors commented about the need for a very careful plan in such patients in whom insertion, tube positioning and ongoing care is likely to be particularly difficult. 66

67 Tube at discharge from critical care 67

68 Cuff pressure measurement on the ward 68

69 Equipment & continuous inflation 69

70 Equipment to measure pressure ward 70
71 Bedside information Documentation of routine information on tracheostomy tubes and ongoing care (including cuff pressure monitoring) was not always readily available as part of bedside observations in patients. For example, in 178/396 (45%) of cases there was insufficient data for Advisors to make a decision about cuff pressure when clinical notes were reviewed 71
72 Key findings 27% (112/419) of first tubes changes in critical Care occurred less than 7 days after insertion 50.4% (57/113) tube changes in the first 7 days were unplanned Only 15/89 patients with a BMI of >30 had a tube in which length could be adjusted at first tube change 95% (551/580) of critical care patients were discharged with a cuffed tracheostomy tube still in place In just 53.3% (211/396) of case notes was information available about cuff pressure 72
73 Recommendations When changing tracheostomy tubes the correct size and length of tube should be carefully selected according to patient need, and with particular care in patients with a high BMI Unplanned tube changes pose additional risks and should be reported as critical incidents At critical care discharge there must be careful consideration as to whether a cuffed tube is required. If a cuff is required competences and equipment must be available to measure cuff pressure Tracheostomy tube information as well as essential equipment should be readily available at the bedside * 73
74 The multidisciplinary team and care of tracheostomy patients 74
75 Number of wards caring for patients 75
76 Hospital policy for tracheostomy care 76
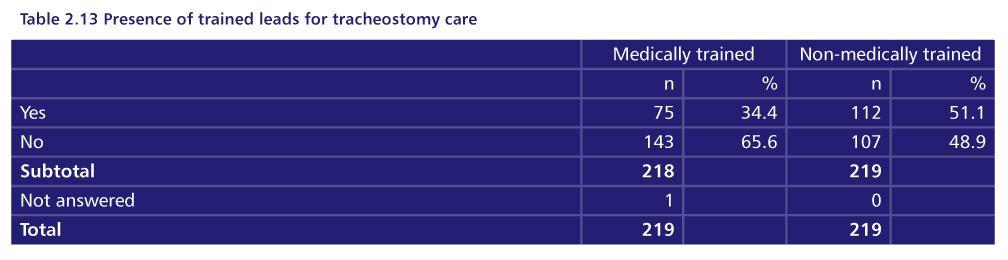
77 Tracheostomy leads 77

78 Clinical teams in the ward MDT 78

79 Discussion at the ward MDT 79

80 Patients not discussed at a ward MDT 80

81 Swallowing difficulty ward patients 81

82 Swallowing difficulty advisor opinion 82
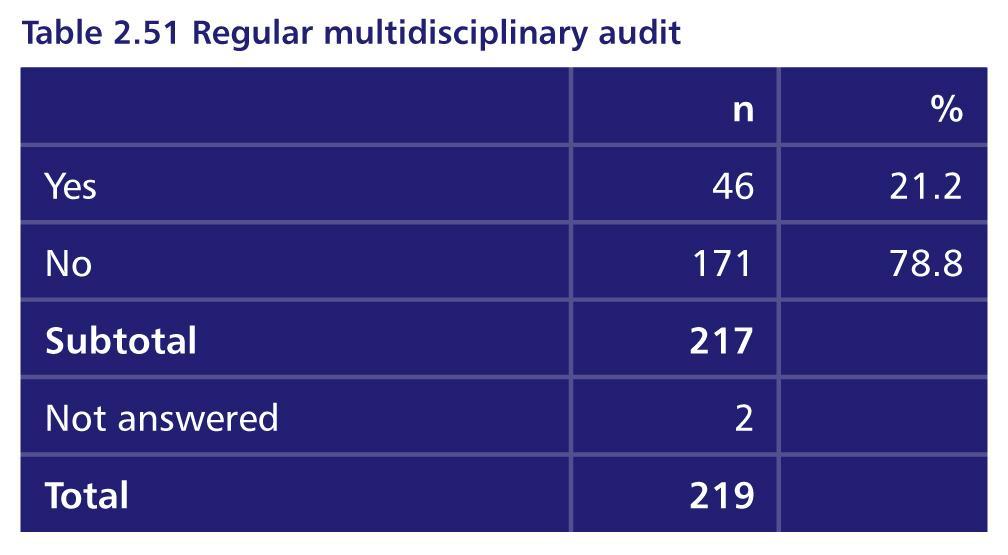
83 Multidisciplinary audit 83
84 Key findings 67.1% (318/474) of ward patients with a tracheostomy were discussed at an MDT meeting Composition of the MDT on the ward varied with relatively poor representation from Dietetics and Critical care outreach (42.7% and 58.8% of teams respectively) Swallowing difficulty occurred in 51% (220/425) of ward patients with a tracheostomy 57% (96/168) of patients with swallowing difficulty on the ward had an early referral to speech and language therapy (SLT) 26.9% (456/1693) of patients on critical care had input from SLT 84
85 Recommendations Multidisciplinary care pathways which provide continuity between critical care unit staff and ward clinicians, and which facilitate decannulation and discharge planning need to be established for all tracheostomy patients* Involvement of SLT in critical care units needs to be facilitated to provide high quality communication strategies particularly for more complex patients Swallowing difficulty in tracheostomy patients should be clearly recognised requiring referral to SLT Swallowing difficulty in tracheostomy patients should be the subject of ongoing study 85
86 Complications and adverse events 86

87 Complications in critical care 87

88 Number of complications per patient 88

89 Timing of complications in critical care 89

90 Major complications & consultant input 90
91 Case study A middle aged patient with a high BMI sustained a high cervical fracture with a high thoracic sensory level due to spinal cord trauma. There were other injuries, to chest & face, and the patient underwent a difficult surgical tracheostomy insertion. At day 10 and during day time hours the tube was either blocked or displaced which resulted in a cardiac arrest responding to a short period of CPR and tube re-insertion. Management was complicated by lack of venous access at this point. Advisors commented on the speed of onset of severe hypoxia and arrest in this patient which was ultimately very well managed by resident staff. Despite the potential for major harm as a result of this complication the patient was successfully decannulated about one month later. 91
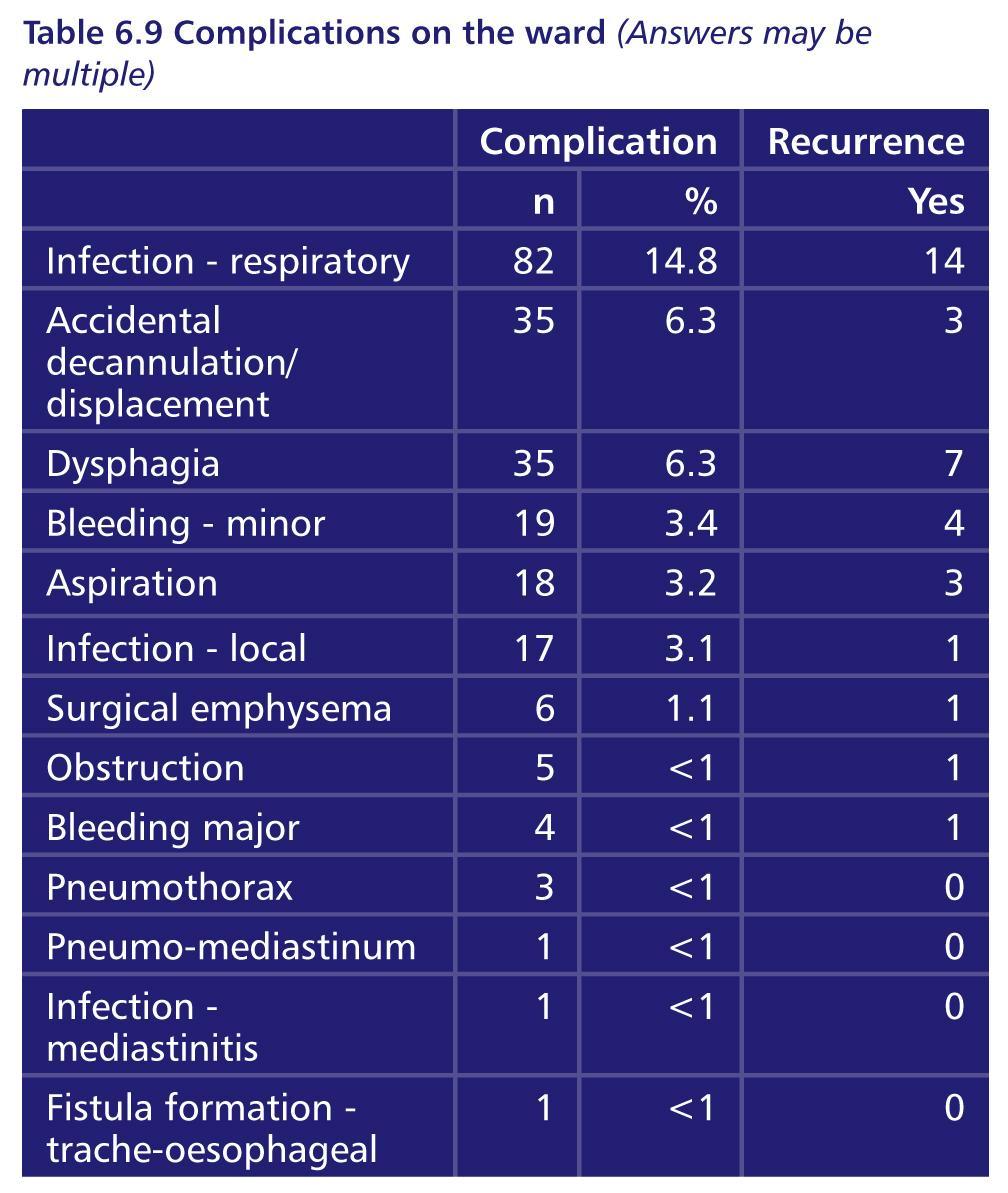
92 Ward complications 92

93 Long term effects Advisor opinion 93

94 Training in blocked & displaced tubes 94
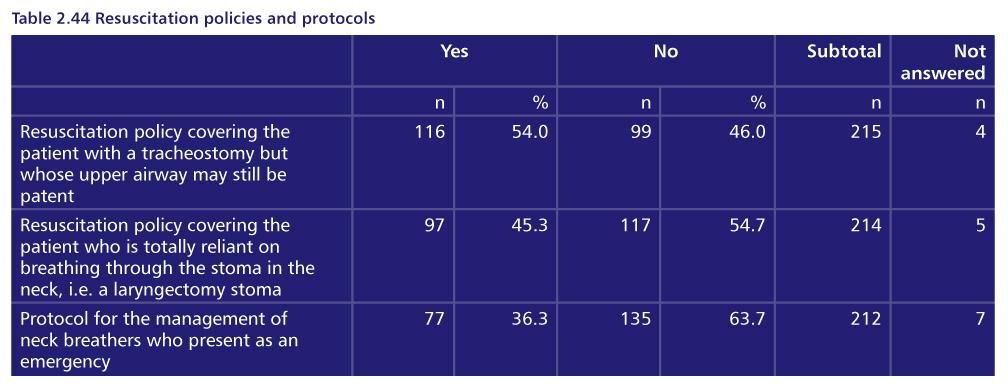
95 Resuscitation training 95

96 Bedside capnography organisational data 96
97 Key findings 23.6% of Critical care patients and 31.3% of ward patients in this study experienced defined complications related to their tracheostomy The most serious complications involved tube displacement, obstruction, pneumothorax and major haemorrhage Accidental tube displacement was more common in ward based patients (6.3% vs. 4.1%) 80.6% (174/216) of hospitals had a policy for management of blocked and displaced tubes 27.9% (48/172) of hospitals did NOT provide training programme for management of blocked and displaced tubes 71.5% of units used continuous capnography when patients were ventilator dependent 97
98 Recommendations Bedside staff caring for tracheostomy patients must be competent to recognise and manage common airway complications including tube obstruction or displacement * Emergency action plans need to reflect the escalation policy for a difficult airway event in order to summon appropriate senior staff Training programmes in management of blocked and displaced tubes and difficult tube changes need to be delivered in accordance with existing national guidelines Core competences for the care of tracheostomy patients including resuscitation should be set out by Trusts using existing national resources Capnography must be available and used at each bed space whilst a patient is ventilator dependent 98
99 Outcomes in tracheostomy patients 99
100 Outcome on critical care 100
101 Timing of decannulation on critical care 101
102 Early decannulation & trials of extubation 102
103 Airway assessment prior to decannulation 103
104 Case study A middle aged patient was admitted from clinic with squamous cell carcinoma of the mouth and had a surgical tracheostomy under general anaesthetic prior to major head & neck resection and flap reconstruction. The patient was discharged to a surgical ward from critical care and decannulated very rapidly after a ward round decision by the registrar, a total of just 3 days after tracheostomy formation. No checks to confirm adequate cough, swallow etc. were performed. Whilst the decannulation was successful, Advisors questioned why a simple bedside test of airway patency had not been performed first, and accompanied by basic documentation to explain the rationale for early decannulation. 104

105 Timing of critical care discharge 105
106 Days between insertion & discharge 106
107 Location of care after critical care discharge 107
108 Timing of critical care discharge 108

109 Discharge from critical care out of hours 109
110 Information transfer 90.9% (541/595) of patients had a discharge summary provided when they left critical care 85% (460/541) of summaries did not provide several key pieces of information such as weaning plans and who had responsibility for tracheostomy decisions 110
111 Timing of ward admission 111

112 Outcome on the ward 112
113 Ward discharge with a tracheostomy 113

114 Reasons for continued ward stay at day
115 Case study A young patient had a major stroke and needed airway support/ protection. After initial intubation a percutaneous tracheostomy was performed on critical care to facilitate ongoing needs. Whilst the patient received good SLT & physiotherapy input on the ward to which they were discharged, there were several problems with humidification during the ward stay. Ultimately the patient was prepared for discharge to a nursing home and there was evidence of good levels of training of receiving staff. Advisors commented upon the general lack of provision for such training in many parts of the country which often caused major delays in hospital discharge. 115
116 Key findings 18% (161/910) underwent decannulation less than 7 days from Tracheostomy insertion in critical care, with 85/141 patients not having undergone a trial of extubation prior to tracheostomy formation 31% (157/503) of critical care discharges of tracheostomy patients and 43% (165/384) of ward admissions occurred after and before patients were discharged from critical care after and before % (541/595) of patients had a discharge summary provided when they left critical care but 85% of summaries did not include key information about ongoing care of the tracheostomy 116
117 Recommendations If patients do not undergo a trial of extubation prior to tracheostomy formation the reason should be documented Unplanned and night time discharge of a patient with a tracheostomy is not recommended, particularly in patients with newly formed tracheostomy or those recently weaned from respiratory support * Wards accepting tracheostomy patients should be in a state of readiness in terms of equipment and competences Multidisciplinary agreement on minimum airway assessments prior to decannulation should be established Quality of discharge information should be improved and include key information about tracheostomy care 117

118 Overall assessment of care 118
119 Overall assessment of care critical care 40% 20% 21% 18% 1% 119
120 Overall assessment of care ward 120
121 Principal recommendations Tracheostomy insertion should be recorded and coded as an operative procedure in all locations, and data collection should be as robust as in a theatre environment. This will facilitate planning and allow national review and audit The diameter and length of the tracheostomy tube should be appropriate for the size and anatomy of the individual patient and should generally contain an inner tube Training for bedside staff should include routine care as well as resuscitation procedures for tracheostomy patients. This should be supported by hospital wide guidance for tracheostomy care. Tube data as well as essential equipment should be clearly available at the bedside 121
122 Principal recommendations Multidisciplinary care pathways which provide continuity of care between Critical Care and ward clinicians, and facilitate decannulation and discharge planning need to be established for all tracheostomy patients Bedside staff caring for tracheostomy patients must be competent to recognise and manage common airway complications Unplanned and night time discharge of a patient with a tracheostomy is not recommended, particularly in patients with newly formed tracheostomy or those recently weaned from respiratory support 122
123 Key references 123
124 Summary Tracheostomy insertion is regarded as a relatively low risk procedure which can now be carried out at the bedside in many high risk patients Information on how many procedures are carried out percutaneously has been poor and not captured by existing data collection systems to date Whilst improving patient comfort the importance of meticulous ongoing care of the tracheostomy patient is recognised and bedside staff must have the competence and confidence to deal with common emergencies 124
125 Summary NCEPOD presents a study which encompasses the full care pathway in patients with a new tracheostomy in hospital, alongside an extensive review of organisational aspects of care The study reinforces recommendations made by other healthcare groups, and presents new information which can be used as a basis for discussion and future planning to improve patient outcomes 125
126 Thank you 126
NCEPOD On the Right Trach?
 NCEPOD On the Right Trach? Hospital Number Tracheostomy insertion (1) Consent and WHO type (surgical) checklists should be adopted and used prior to tracheostomy insertion, wherever it is performed. Q8.
NCEPOD On the Right Trach? Hospital Number Tracheostomy insertion (1) Consent and WHO type (surgical) checklists should be adopted and used prior to tracheostomy insertion, wherever it is performed. Q8.
TEMPORARY CONSULTANT IN INTENSIVE CARE MEDICINE (TYPE B) National Clinical Programme Integrated Care Programme Patient Flow Job Description
 National Clinical Programme Integrated Care Programme Patient Flow Job Description") TEMPORARY CONSULTANT IN INTENSIVE CARE MEDICINE (TYPE B) National Clinical Programme Integrated Care Programme Patient Flow Job Description Mater Misericordiae University Hospital 39 hours National Rehabilitation
TEMPORARY CONSULTANT IN INTENSIVE CARE MEDICINE (TYPE B) National Clinical Programme Integrated Care Programme Patient Flow Job Description Mater Misericordiae University Hospital 39 hours National Rehabilitation
does staff intervene; used? If not, describe.
 Use this pathway for a resident who requires or receives respiratory care services (i.e., oxygen therapy, breathing exercises, sleep apnea, nebulizers/metered-dose inhalers, tracheostomy, or ventilator)
Use this pathway for a resident who requires or receives respiratory care services (i.e., oxygen therapy, breathing exercises, sleep apnea, nebulizers/metered-dose inhalers, tracheostomy, or ventilator)
Patient Name: David Thomas Diagnosis: Cancer, Tracheostomy
 Patient Name: David Thomas Diagnosis: Cancer, Tracheostomy Overview of Scenario Simulated Patient Overview Target Audience (Part A): 2 nd year Speech Pathology students, 2 nd year Social Work students
Patient Name: David Thomas Diagnosis: Cancer, Tracheostomy Overview of Scenario Simulated Patient Overview Target Audience (Part A): 2 nd year Speech Pathology students, 2 nd year Social Work students
1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure
 ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
SIMULATION COURSE PROGRAMME
 SIMULATION COURSE PROGRAMME 2016-2017 1 Contents PAGE Foundation Training.. 3 General Internal Medicine Regional Training. 4 ROBuST - RCOG Operative Birth Simulation Training. 5 Trauma Team Member Courses
SIMULATION COURSE PROGRAMME 2016-2017 1 Contents PAGE Foundation Training.. 3 General Internal Medicine Regional Training. 4 ROBuST - RCOG Operative Birth Simulation Training. 5 Trauma Team Member Courses
September 2007 Replaces: October 2001
 Inova Fairfax Hospital - Critical Care CRITICAL CARE STANDARD: 4.020 Passy-Muir Tracheostomy Speaking Valve September 2007 Replaces: October 2001 Sonia Astle, RN, MS, CCNS Chair Critical Care Standards
Inova Fairfax Hospital - Critical Care CRITICAL CARE STANDARD: 4.020 Passy-Muir Tracheostomy Speaking Valve September 2007 Replaces: October 2001 Sonia Astle, RN, MS, CCNS Chair Critical Care Standards
Case 1 Standard of Care. Disclosures. Defending Critical Care: Navigating Through the Malpractice Maze 5/9/2015. Defending Critical Care:
 Defending Critical Care: Navigating Through the Malpractice Maze Defending Critical Care: Navigating Through the Malpractice Maze Joseph Picchi, JD Richard Schoenberger, JD Critical Care Medicine Update
Defending Critical Care: Navigating Through the Malpractice Maze Defending Critical Care: Navigating Through the Malpractice Maze Joseph Picchi, JD Richard Schoenberger, JD Critical Care Medicine Update
Questions. Background to the ICNARC Case Mix Programme
 Number of admissions, unit length of stay and days of mechanical ventilation for admissions with blunt chest trauma to critical care in England, Wales and Northern Ireland Questions What were the number,
Number of admissions, unit length of stay and days of mechanical ventilation for admissions with blunt chest trauma to critical care in England, Wales and Northern Ireland Questions What were the number,
Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey
 Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey We want you to nominate the most important topics for future research in anaesthesia and perioperative care. We are therefore asking
Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey We want you to nominate the most important topics for future research in anaesthesia and perioperative care. We are therefore asking
Undergoing a Percutaneous Endoscopic Gastrostomy (PEG) Tube procedure
 Tube procedure") Page 1 of 7 Undergoing a Percutaneous Endoscopic Gastrostomy (PEG) Tube procedure Introduction This leaflet only contains information regarding a PEG tube and includes important information about the procedure.
Page 1 of 7 Undergoing a Percutaneous Endoscopic Gastrostomy (PEG) Tube procedure Introduction This leaflet only contains information regarding a PEG tube and includes important information about the procedure.
NHS Innovation Accelerator. Economic Impact Evaluation Case Study: PneuX TM 1. BACKGROUND
 NHS Innovation Accelerator Economic Impact Evaluation Case Study: PneuX TM 1. BACKGROUND The PneuX Pneumonia Prevention System is an endotracheal/tracheostomy tube system for airway management, designed
NHS Innovation Accelerator Economic Impact Evaluation Case Study: PneuX TM 1. BACKGROUND The PneuX Pneumonia Prevention System is an endotracheal/tracheostomy tube system for airway management, designed
Organisational Audit Questions - Links to recommendations, standards and evidence
 Question Quoted recommendation/ standard / evidence Source Notes Section 1 - Hospital characteristics 1. a) How many adult in-patient or overnight beds (including 23- hours stay) are currently available
Question Quoted recommendation/ standard / evidence Source Notes Section 1 - Hospital characteristics 1. a) How many adult in-patient or overnight beds (including 23- hours stay) are currently available
Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath
 Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath Up to 25,000 surgical deaths per year 5-10% of surgical cases are high risk 79% of deaths occur in the high risk group Overall
Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath Up to 25,000 surgical deaths per year 5-10% of surgical cases are high risk 79% of deaths occur in the high risk group Overall
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
SIMULATION COURSE PROGRAMME
 SIMULATION COURSE PROGRAMME 2014-2015 1 Contents PAGE Foundation Training.. 3 Human Factors in Urgent Care... 4 Joint Injection Day. 5 Emergency Airway Management for Acute Care Professionals 6 (EAMAP)
SIMULATION COURSE PROGRAMME 2014-2015 1 Contents PAGE Foundation Training.. 3 Human Factors in Urgent Care... 4 Joint Injection Day. 5 Emergency Airway Management for Acute Care Professionals 6 (EAMAP)
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
GAMUT QI Collaborative Consensus Quality Metrics (v. 05/16/2016)
") 1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
Rita Hunsucker, DNP, Nicole Cornell, MS, Gerald Hobbs, PhD, Jorge Con, MD & Alison Wilson, MD WVU Medicine, J.W. Ruby Memorial Hospital
 Rita Hunsucker, DNP, Nicole Cornell, MS, Gerald Hobbs, PhD, Jorge Con, MD & Alison Wilson, MD WVU Medicine, J.W. Ruby Memorial Hospital The authors have nothing to disclose. Post extubation dysphagia (PED)
Rita Hunsucker, DNP, Nicole Cornell, MS, Gerald Hobbs, PhD, Jorge Con, MD & Alison Wilson, MD WVU Medicine, J.W. Ruby Memorial Hospital The authors have nothing to disclose. Post extubation dysphagia (PED)
PICU tracheostomy protocol
 PICU tracheostomy protocol This protocol is based on the joint Royal Brompton & Harefield NHS Trust and Great Ormond Street Hospital for Children NHS Trust, Great Ormond Street Hospital Manual of Children
PICU tracheostomy protocol This protocol is based on the joint Royal Brompton & Harefield NHS Trust and Great Ormond Street Hospital for Children NHS Trust, Great Ormond Street Hospital Manual of Children
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
TRAINING IN OBSTETRIC ANAESTHESIA
 INTRODUCTION: TRAINING IN OBSTETRIC ANAESTHESIA The following brief curriculum outline and suggested assessment schedule was devised by an OAA working party. Originally written for the Royal College of
INTRODUCTION: TRAINING IN OBSTETRIC ANAESTHESIA The following brief curriculum outline and suggested assessment schedule was devised by an OAA working party. Originally written for the Royal College of
SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER. Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow
 SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow I. Clinical Mission of the North Carolina Jaycee Burn Center The clinical
SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow I. Clinical Mission of the North Carolina Jaycee Burn Center The clinical
Pre-operative categorization (triaging) of emergency surgical cases. A tool for improving patient care and emergency operating room efficiency
 of emergency surgical cases. A tool for improving patient care and emergency operating room efficiency") Pre-operative categorization (triaging) of emergency surgical cases A tool for improving patient care and emergency operating room efficiency Introduction No national or provincial guidelines exist for
Pre-operative categorization (triaging) of emergency surgical cases A tool for improving patient care and emergency operating room efficiency Introduction No national or provincial guidelines exist for
PLACEMENT. Disclaimer
 1 TITLE: GUIDELINE FOR PERCUTANEOUS ENDOSCOPIC GASTROSTOMY TUBE Disclaimer PLACEMENT The Canadian Society of Gastroenterology Nurses and Associates (CSGNA) presents this guideline to be used as a reference
1 TITLE: GUIDELINE FOR PERCUTANEOUS ENDOSCOPIC GASTROSTOMY TUBE Disclaimer PLACEMENT The Canadian Society of Gastroenterology Nurses and Associates (CSGNA) presents this guideline to be used as a reference
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs.
 6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
Effective: September, 2011 Revised: August 17, 2016 TRACHEOSTOMY TUBE REPLACEMENT
 TRACHEOSTOMY TUBE REPLACEMENT Purpose: Emergency tracheostomy tube replacement occurs when the tube becomes blocked, dislodged or has been unintentionally removed. Additional Authority: Nevada Revised
TRACHEOSTOMY TUBE REPLACEMENT Purpose: Emergency tracheostomy tube replacement occurs when the tube becomes blocked, dislodged or has been unintentionally removed. Additional Authority: Nevada Revised
THE ROYAL NATIONAL ORTHOPAEDIC HOSPITAL NHS TRUST QUALITY ACCOUNTS 2011/12
 THE ROYAL NATIONAL ORTHOPAEDIC HOSPITAL NHS TRUST Quality Narrative QUALITY ACCOUNTS 2011/12 (WORKING DRAFT OF CONTENT) 1. Statement from the Chief Executive, and summary of the quality of NHS services
THE ROYAL NATIONAL ORTHOPAEDIC HOSPITAL NHS TRUST Quality Narrative QUALITY ACCOUNTS 2011/12 (WORKING DRAFT OF CONTENT) 1. Statement from the Chief Executive, and summary of the quality of NHS services
St. James s Hospital, Dublin.
 Position Fellowship in Anaesthesia for Advanced Airway Management Assignment Department of Anaesthesia, St. James s Hospital. Commencement Date Monday, 09 th July, 2018. Purpose of the Post The St. James
Position Fellowship in Anaesthesia for Advanced Airway Management Assignment Department of Anaesthesia, St. James s Hospital. Commencement Date Monday, 09 th July, 2018. Purpose of the Post The St. James
PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification
 E07/S/c 2013/14 NHS STANDARD CONTRACT PAEDIATRIC LONG TERM VENTILATION PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner Lead Provider Lead Period
E07/S/c 2013/14 NHS STANDARD CONTRACT PAEDIATRIC LONG TERM VENTILATION PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner Lead Provider Lead Period
NCEPOD Recommendations that remain current
 NCEPOD Recommendations that remain current All recommendations from subsequent NCEPOD reports are considered current (Last updated 2014) 1989 The information systems, particularly clinical information
NCEPOD Recommendations that remain current All recommendations from subsequent NCEPOD reports are considered current (Last updated 2014) 1989 The information systems, particularly clinical information
Auckland District Health Board Summary 1 July 2011 to 30 June 2012 Serious and Sentinel Events
 DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
SAMPLE Bariatric Surgery Program Survey for Facilities and Surgeons
 I. Facility Section (to be completed by the facility s risk and/or quality department) Facility Name: Address: Date: Contact Person: Directions Please check the appropriate yes or no answer boxes where
I. Facility Section (to be completed by the facility s risk and/or quality department) Facility Name: Address: Date: Contact Person: Directions Please check the appropriate yes or no answer boxes where
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Australian and New Zealand College of Anaesthetists (ANZCA)
") PS08 2016 Australian and New Zealand College of Anaesthetists (ANZCA) Statement on the Assistant for the Anaesthetist 1. PURPOSE The purpose of this document is to recognise the importance of and to promote
PS08 2016 Australian and New Zealand College of Anaesthetists (ANZCA) Statement on the Assistant for the Anaesthetist 1. PURPOSE The purpose of this document is to recognise the importance of and to promote
Delayed discharges and unplanned admissions from the Day Care Unit at Mater Dei Hospital, Malta
 Delayed discharges and unplanned admissions from the Day Care Unit at Mater Dei Hospital, Malta Abstract Introduction: Day care units are playing an increasingly important role in healthcare provision,
Delayed discharges and unplanned admissions from the Day Care Unit at Mater Dei Hospital, Malta Abstract Introduction: Day care units are playing an increasingly important role in healthcare provision,
St. James s Hospital, Dublin.
 Position Senior House Officer in Anaesthesia Organisational Area Department of Anaesthesia, St. James s Hospital. Closing Date Sunday the 9 th July 2018 SACC Directorate. The Surgery, Anaesthesia and Critical
Position Senior House Officer in Anaesthesia Organisational Area Department of Anaesthesia, St. James s Hospital. Closing Date Sunday the 9 th July 2018 SACC Directorate. The Surgery, Anaesthesia and Critical
Specialised Services Service Specification. Adult Congenital Heart Disease
 Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
Simulation Scenario Management of obstructed tracheostomy
 INTRODUCTION: Scenario Goals and Objectives: Simulation Scenario Management of obstructed tracheostomy Simulation objectives By the end of this simulation participants will have: 1. Practiced the recognition
INTRODUCTION: Scenario Goals and Objectives: Simulation Scenario Management of obstructed tracheostomy Simulation objectives By the end of this simulation participants will have: 1. Practiced the recognition
ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE
 ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE Rotation Contacts and Scheduling Details Rotation Director: Kelly Yeh, MD Director of Pediatric Anesthesia Santa Clara Valley Medical Center kelly.yeh@hhs.sccgov.org.,
ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE Rotation Contacts and Scheduling Details Rotation Director: Kelly Yeh, MD Director of Pediatric Anesthesia Santa Clara Valley Medical Center kelly.yeh@hhs.sccgov.org.,
DRAFT POLICY GUIDELINES FOR THE BOOKING OF SURGICAL CASES ON THE EMERGENCY SLATE
 INTRODUCTION DRAFT POLICY GUIDELINES FOR THE BOOKING OF SURGICAL CASES ON THE EMERGENCY SLATE With the aim of improving emergency surgical case access to emergency theatre services the following areas
INTRODUCTION DRAFT POLICY GUIDELINES FOR THE BOOKING OF SURGICAL CASES ON THE EMERGENCY SLATE With the aim of improving emergency surgical case access to emergency theatre services the following areas
Consent Form and Patient information leaflet
 Consent Form and Patient information leaflet Introduction Around 2.9 million general anaesthetics are conducted annually in the UK. When patients are anaesthetised (put to sleep) for an operation the anaesthetist
Consent Form and Patient information leaflet Introduction Around 2.9 million general anaesthetics are conducted annually in the UK. When patients are anaesthetised (put to sleep) for an operation the anaesthetist
Prone Ventilation of the Critically Ill Patient
 Prone Ventilation of the Critically Ill Patient Statement of Best Practice Patients who require prone ventilation will be clinically assessed by the appropriate medical team, taking into account indications/contraindications,
Prone Ventilation of the Critically Ill Patient Statement of Best Practice Patients who require prone ventilation will be clinically assessed by the appropriate medical team, taking into account indications/contraindications,
anaesthetic services Chapter 15 Services for neuroanaesthesia and neurocritical care 2014 GUIDELINES FOR THE PROVISION OF ACSA REFERENCES
 Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
COBAFOLIO: DOCUMENTING THE EVIDENCE OF COMPETENCE
 COBAFOLIO: DOCUMENTING THE EVIDENCE OF COMPETENCE (2006) The CoBaTrICE Collaboration: 1 st September 2006. European Society of Intensive Care Medicine (ESICM) Avenue Joseph Wybran 40, B-1070,Brussels.
COBAFOLIO: DOCUMENTING THE EVIDENCE OF COMPETENCE (2006) The CoBaTrICE Collaboration: 1 st September 2006. European Society of Intensive Care Medicine (ESICM) Avenue Joseph Wybran 40, B-1070,Brussels.
About the Critical Care Center
 Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Your anaesthetic for a broken hip
 Your anaesthetic for a broken hip Information to help patients, relatives and carers prepare for an anaesthetic for a broken hip First Edition 2014 www.rcoa.ac.uk/patientinfo This leaflet explains what
Your anaesthetic for a broken hip Information to help patients, relatives and carers prepare for an anaesthetic for a broken hip First Edition 2014 www.rcoa.ac.uk/patientinfo This leaflet explains what
Your Hospital Stay After Iliac Crest Free Flap Surgery
 Your Hospital Stay After Iliac Crest Free Flap Surgery What to expect This handout explains what to expect during your hospital stay after your iliac crest free flap surgery. It includes where you will
Your Hospital Stay After Iliac Crest Free Flap Surgery What to expect This handout explains what to expect during your hospital stay after your iliac crest free flap surgery. It includes where you will
Your Hospital Stay After Fibular Free Flap Surgery
 Your Hospital Stay After Fibular Free Flap Surgery What to expect This handout explains what to expect during your hospital stay after your fibular free flap surgery. It includes where you will stay after
Your Hospital Stay After Fibular Free Flap Surgery What to expect This handout explains what to expect during your hospital stay after your fibular free flap surgery. It includes where you will stay after
Tracheostomy information for patients and relatives
 Tracheostomy information for patients and relatives What is a tracheostomy? A tracheostomy is when a small opening is made in the windpipe to help you breath more easily or to help you cough up phlegm.
Tracheostomy information for patients and relatives What is a tracheostomy? A tracheostomy is when a small opening is made in the windpipe to help you breath more easily or to help you cough up phlegm.
Supervision of Residents/Chain of Command
 Supervision of Residents/Chain of Command Creighton University Department of Surgery Residency Training Program Chain of command for Surgery residents at CUMC PGY1: The intern on call covers the two general
Supervision of Residents/Chain of Command Creighton University Department of Surgery Residency Training Program Chain of command for Surgery residents at CUMC PGY1: The intern on call covers the two general
Coroner's Corner - Inquest into the death of Gwendoline Mead
 Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Curriculum Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-SICU The Section Chief for the Emergency General Surgery section within the Division
Curriculum Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-SICU The Section Chief for the Emergency General Surgery section within the Division
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems NPSS Asheville, NC
 Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
MEET THE ACADEMIC TEAM
 MEET THE ACADEMIC TEAM Lancashire Teaching Hospitals Royal Preston Hospital and Chorley District Hospital 2016-17 Dr Paul Marsden Consultant Physician in Respiratory Medicine & Honorary Lecturer Respiratory
MEET THE ACADEMIC TEAM Lancashire Teaching Hospitals Royal Preston Hospital and Chorley District Hospital 2016-17 Dr Paul Marsden Consultant Physician in Respiratory Medicine & Honorary Lecturer Respiratory
Patient safety incidents associated with airway devices in critical care: a review of reports to the UK National Patient Safety Agency
 Anaesthesia, 2009, 64, pages 358 365 doi:10.1111/j.1365-2044.2008.05784.x Patient safety incidents associated with airway devices in critical care: a review of reports to the UK National Patient Safety
Anaesthesia, 2009, 64, pages 358 365 doi:10.1111/j.1365-2044.2008.05784.x Patient safety incidents associated with airway devices in critical care: a review of reports to the UK National Patient Safety
Recommended Minimum Facilities for Safe Anaesthetic Practice in Organ Imaging Units
 Page 1 of 7 Recommended Minimum Facilities for Safe Anaesthetic Practice in Organ Imaging Units Version Effective Date 1 Oct 1992 (reviewed Feb 02) 2 Nov 2011 3 Dec 2016 Document No. HKCA T3 v3 Prepared
Page 1 of 7 Recommended Minimum Facilities for Safe Anaesthetic Practice in Organ Imaging Units Version Effective Date 1 Oct 1992 (reviewed Feb 02) 2 Nov 2011 3 Dec 2016 Document No. HKCA T3 v3 Prepared
Policies and Procedures. I.D. Number: 1145
 Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
INTRODUCTION. LEARNING OBJECTIVES (CanMEDS)
") OVERVIEW The Thoracic Surgery selective is based at Health Sciences Centre. Students participate in the surgical management of patients with lung cancer and esophageal cancer, as well as other conditions
OVERVIEW The Thoracic Surgery selective is based at Health Sciences Centre. Students participate in the surgical management of patients with lung cancer and esophageal cancer, as well as other conditions
Teaching Methods. Responsibilities
 Avera McKennan Critical Care Medicine Rotation Goals and Objectives Pulmonary/Critical Care Medicine Fellowship Program University of Nebraska Medical Center Written: May 2011 I) Rotation Goals A) To manage
Avera McKennan Critical Care Medicine Rotation Goals and Objectives Pulmonary/Critical Care Medicine Fellowship Program University of Nebraska Medical Center Written: May 2011 I) Rotation Goals A) To manage
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Provincial Nursing Competencies List of e-learning Modules. Updated: September 25, 2015
 Provincial Nursing Competencies List of e-learning Modules Updated: September 25, 2015 Once you sign in on the home page, you will see the following search screen on the right hand side of the page: Search:
Provincial Nursing Competencies List of e-learning Modules Updated: September 25, 2015 Once you sign in on the home page, you will see the following search screen on the right hand side of the page: Search:
Activation of the Rapid Response Team
 Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Approved by: Activation of the Rapid Response Team Senior Operating Officer, Acute Services, GNCH; and Senior Operating Officer, Acute Services, MCH Edmonton Acute Care Patient Care Policy & Procedures
Policy on Resident Supervision. University of South Florida College of Medicine General Surgery Residency Rev. July 2013
 Policy on Resident Supervision University of South Florida College of Medicine General Surgery Residency Rev. July 2013 Policy Definitions: 1. Resident: A medical school graduate who is enrolled in the
Policy on Resident Supervision University of South Florida College of Medicine General Surgery Residency Rev. July 2013 Policy Definitions: 1. Resident: A medical school graduate who is enrolled in the
Guidelines on Postanaesthetic Recovery Care
 Page 1 of 10 Guidelines on Postanaesthetic Recovery Care Version Effective Date 1 OCT 1992 2 FEB 2002 3 APR 2012 4 JUN 2017 Document No. HKCA P3 v4 Prepared by College Guidelines Committee Endorsed by
Page 1 of 10 Guidelines on Postanaesthetic Recovery Care Version Effective Date 1 OCT 1992 2 FEB 2002 3 APR 2012 4 JUN 2017 Document No. HKCA P3 v4 Prepared by College Guidelines Committee Endorsed by
Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation
 Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation April 2018 Version 4.0 Document information Document purpose Document name Author Policy Specialised
Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation April 2018 Version 4.0 Document information Document purpose Document name Author Policy Specialised
Local anaesthesia for your eye operation
 Local anaesthesia for your eye operation Information for patients Fourth Edition 2014 www.rcoa.ac.uk/patientinfo This leaflet explains what to expect when you have an eye operation with a local anaesthetic.
Local anaesthesia for your eye operation Information for patients Fourth Edition 2014 www.rcoa.ac.uk/patientinfo This leaflet explains what to expect when you have an eye operation with a local anaesthetic.
Model of Care for Paediatric Critical Care
 Table of Contents 1 FOREWORD... 5 2 EXECUTIVE SUMMARY... 7 2.1 Introduction... 7 2.2 National Clinical Programme for Critical Care... 7 2.3 Governance of Paediatric Critical Care... 8 2.4 Capacity Planning...
Table of Contents 1 FOREWORD... 5 2 EXECUTIVE SUMMARY... 7 2.1 Introduction... 7 2.2 National Clinical Programme for Critical Care... 7 2.3 Governance of Paediatric Critical Care... 8 2.4 Capacity Planning...
EuroELSO GUIDELINES FOR TRAINING & CONTINUING EDUCATION OF ECMO PHYSICIANS
 EuroELSO GUIDELINES FOR TRAINING & CONTINUING EDUCATION OF ECMO PHYSICIANS PURPOSE The "EuroELSO Guidelines for Training & Continuing Education of ECMO Physicians" is a document developed by the Extracorporeal
EuroELSO GUIDELINES FOR TRAINING & CONTINUING EDUCATION OF ECMO PHYSICIANS PURPOSE The "EuroELSO Guidelines for Training & Continuing Education of ECMO Physicians" is a document developed by the Extracorporeal
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 13th March 2014 Compliance
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 13th March 2014 Compliance
Equivalence Guidance for GMP Domain 1
 Equivalence Guidance for GMP Domain 1 From 1 st August 2011 the new GMC approved curriculum in Intensive Care Medicine (ICM) came into effect. As a result of this new curriculum, all equivalence applications
Equivalence Guidance for GMP Domain 1 From 1 st August 2011 the new GMC approved curriculum in Intensive Care Medicine (ICM) came into effect. As a result of this new curriculum, all equivalence applications
Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust
 Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust Mark Simmonds (Acute and Critical Care Medicine Consultant,
Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust Mark Simmonds (Acute and Critical Care Medicine Consultant,
AHRC : Respiratory Critical Care
 University of Montana ScholarWorks at University of Montana Syllabi Course Syllabi 1-2015 AHRC 231.01: Respiratory Critical Care Nicholas J. Arthur University of Montana - Missoula, nicholas.arthur@umontana.edu
University of Montana ScholarWorks at University of Montana Syllabi Course Syllabi 1-2015 AHRC 231.01: Respiratory Critical Care Nicholas J. Arthur University of Montana - Missoula, nicholas.arthur@umontana.edu
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Z: Perioperative Nursing Specialty
 Z: Perioperative Nursing Specialty Alberta Licensed Practical Nurses Competency Profile 263 Major Competency Area: Z Perioperative Nursing Specialty Priority: One Competency: Z-1 HPA Authorizations and
Z: Perioperative Nursing Specialty Alberta Licensed Practical Nurses Competency Profile 263 Major Competency Area: Z Perioperative Nursing Specialty Priority: One Competency: Z-1 HPA Authorizations and
Policy Review Sheet. Review Date: 14/10/16 Policy Last Amended: 19/10/17. Next planned review in 12 months, or sooner as required.
 Category: Care Management Sub-category: Care Practice Page: 1 of 10 Policy Review Sheet Review Date: 14/10/16 Policy Last Amended: 19/10/17 Next planned review in 12 months, or sooner as required. Note:
Category: Care Management Sub-category: Care Practice Page: 1 of 10 Policy Review Sheet Review Date: 14/10/16 Policy Last Amended: 19/10/17 Next planned review in 12 months, or sooner as required. Note:
UNMH Critical Care Clinical Privileges. Name: Effective Dates: From To
 All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective November 17, 2016: INSTRUCTIONS: Applicant: Check off the requested box for each privilege requested.
All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective November 17, 2016: INSTRUCTIONS: Applicant: Check off the requested box for each privilege requested.
Your Hospital Stay After Radial Forearm Free Flap Surgery
 Your Hospital Stay After Radial Forearm Free Flap Surgery What to expect This handout explains what to expect during your hospital stay after your radial forearm free flap surgery. It includes where you
Your Hospital Stay After Radial Forearm Free Flap Surgery What to expect This handout explains what to expect during your hospital stay after your radial forearm free flap surgery. It includes where you
7 NON-ELECTIVE SURGERY IN THE NHS
 Recommendations Debate whether, in the light of changes to the pattern of junior doctors working, non-essential surgery can take place during extended hours. 7 NON-ELECTIVE SURGERY IN THE NHS Ensure that
Recommendations Debate whether, in the light of changes to the pattern of junior doctors working, non-essential surgery can take place during extended hours. 7 NON-ELECTIVE SURGERY IN THE NHS Ensure that
Policy for Admission to Adult Critical Care Services
 Policy Number: CCaNNI 008 Title: Policy for Admission to Adult Critical Care Services Operational Date: Review Date: December 2009 December 2012 Type of Document: EQIA Screening Date: Corporate x Clinical
Policy Number: CCaNNI 008 Title: Policy for Admission to Adult Critical Care Services Operational Date: Review Date: December 2009 December 2012 Type of Document: EQIA Screening Date: Corporate x Clinical
THE FUTURE OF YOUR HOSPITALS: Planned Care site
 THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
SCHEDULE 2 THE SERVICES. A. Service Specifications. E07/S/c Paediatric Long Term Ventilation
 Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E07/S/c Paediatric Long Term Ventilation 1. Population
Appendix 2 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Provider Lead Period Date of Review E07/S/c Paediatric Long Term Ventilation 1. Population
Choosing a Tracheostomy for a Child with a Neuromuscular Disorder
 Choosing a Tracheostomy for a Child with a Neuromuscular Disorder This handout explains what a tracheostomy is and can help you decide if this is right for your child. What is a tracheostomy? Surgery is
Choosing a Tracheostomy for a Child with a Neuromuscular Disorder This handout explains what a tracheostomy is and can help you decide if this is right for your child. What is a tracheostomy? Surgery is
CCT in Anaesthetics Assessment Guidance 2017
 CCT in Anaesthetics Assessment Guidance 2017 Royal College of Anaesthetists Introduction This document describes the various assessment methods used in the anaesthetic training programme. Trainees are
CCT in Anaesthetics Assessment Guidance 2017 Royal College of Anaesthetists Introduction This document describes the various assessment methods used in the anaesthetic training programme. Trainees are
Quality Indicator Local Use of Data
 Quality Indicator Local Use of Data The clinical audit lead for each contributing site was contacted and asked to answer the following questions (in their own words) about the use of STAG data. In general,
Quality Indicator Local Use of Data The clinical audit lead for each contributing site was contacted and asked to answer the following questions (in their own words) about the use of STAG data. In general,
September 2018 April Calendar of events. Educational events to support your professional development needs
 September 2018 April 2019 Calendar of events Educational events to support your professional development needs 2 Calendar of events EVENTS CALENDAR Further information about all of our events can be found
September 2018 April 2019 Calendar of events Educational events to support your professional development needs 2 Calendar of events EVENTS CALENDAR Further information about all of our events can be found
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
Recording and promoting good decision-making
 Recording and promoting good decision-making The Emergency Care and Treatment Plan Dr David Pitcher Vice President Resuscitation Council (UK) Author / co-author / contributor on this topic: National guidance:
Recording and promoting good decision-making The Emergency Care and Treatment Plan Dr David Pitcher Vice President Resuscitation Council (UK) Author / co-author / contributor on this topic: National guidance:
Regions Hospital Delineation of Privileges Critical Care
 Regions Hospital Delineation of Privileges Critical Care Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic
Regions Hospital Delineation of Privileges Critical Care Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic
Tracheostomy Care Test Questions
 Care Test Questions Free PDF ebook Download: Care Test Questions Download or Read Online ebook tracheostomy care test questions in PDF Format From The Best User Guide Database Ask questions about caring
Care Test Questions Free PDF ebook Download: Care Test Questions Download or Read Online ebook tracheostomy care test questions in PDF Format From The Best User Guide Database Ask questions about caring
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation (Trust) Team MVCN LUTON AND DUNSTABLE Luton & Dunstable Colorectal MDT (11-2D-1) - 2011/12 Peer Review Visit Date 11th November 2011
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation (Trust) Team MVCN LUTON AND DUNSTABLE Luton & Dunstable Colorectal MDT (11-2D-1) - 2011/12 Peer Review Visit Date 11th November 2011
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Portsmouth Hospitals NHS Trust Individual Placement (Job) Descriptions for Foundation Year 1
 Descriptions for Foundation Year 1") Portsmouth Hospitals NHS Trust Individual Placement (Job) Descriptions for Foundation Year 1 Placement The department Where the is for the in this F1 Acute Placement Acute Medicine Unit/Surgical Assessment
Portsmouth Hospitals NHS Trust Individual Placement (Job) Descriptions for Foundation Year 1 Placement The department Where the is for the in this F1 Acute Placement Acute Medicine Unit/Surgical Assessment
Inguinal hernia repair integrated care pathway (ICP)
") Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
The Royal College of Surgeons of England Provision of Trauma Care Policy Briefing This policy briefing outlines the view of the Royal College of Surgeons of England in relation to the planning and provision
Critical Care in Obstetrics Guideline
 This is an official Northern Trust policy and should not be edited in any way Critical Care in Obstetrics Guideline Reference Number: NHSCT/12/515 Target audience: This guideline is directed to all obstetricians,
This is an official Northern Trust policy and should not be edited in any way Critical Care in Obstetrics Guideline Reference Number: NHSCT/12/515 Target audience: This guideline is directed to all obstetricians,
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Anesthesia
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Anesthesia 1. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation.
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Anesthesia 1. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation.
ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY)
") July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
Policy for Vetting Surgical Referrals
 Policy for Vetting Surgical Referrals Date: September 2017 Version number: 2 Author: Mr Gordon McFarlane Review Date: September 2020 If you would like this document in an alternative language or format,
Policy for Vetting Surgical Referrals Date: September 2017 Version number: 2 Author: Mr Gordon McFarlane Review Date: September 2020 If you would like this document in an alternative language or format,