Emergency Department Strategic Design Considerations
|
|
|
- Georgia Riley
- 5 years ago
- Views:
Transcription
1 Emergency Department Strategic Design Considerations James Augustine, MD Director of Clinical Operations, EMP Associate Clinical Professor, Wright State University Department of Emergency Medicine.
2 ED Operations and Health Systems Relate ED project to the overall hospital mission How does form change in the ED lead to operations change for the entire system? Does the ED design fulfill hospital system marketing priorities? Will ED expansion expose other hospital issues? Is the specialty ED part of the hospital system future, or of our competitors? Will the ED project be consistent in fit/finish with other hospital areas?


3 How do other facilities and Send the Unfocused to the ED!!! providers get to Focus?


4 The Patient Count: Americans Vote With Their Feet


5 Not Only More ED Visits in the Senior Age Brackets More Population Enters those Age Groups Each Year 800 Graying of the ED All ED Visits Ages Age over 65 Age over 75
6 NHAMCS Helps Predict Future Patient Flows 2.3% more patients per year for about the last 17 years Injury is 34% of ED Patient Load Highest injury rates are over age 75 ECF Patients Most Frequent ED Use 2.5 m visits in % admission rate Conservative Cost: $5B
7 Trauma population ages The Patient Mix Important and Unrecognized Issues The Reduction in Burn, Trauma, Injury and Cardiac Arrest What should we have known? Prevention Works! When prevention works, people are alive to get ill
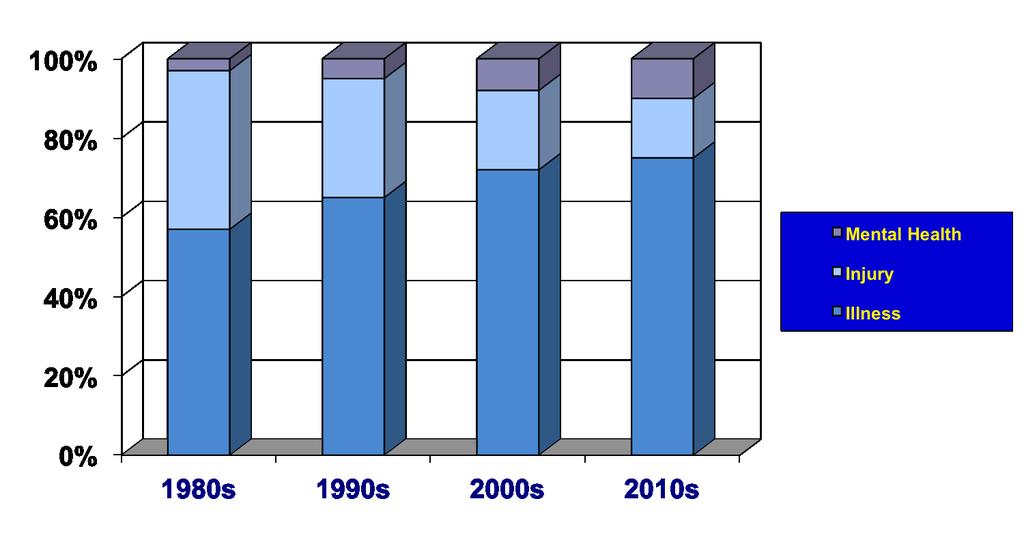
8 Predictable Change in ED Patient Mix
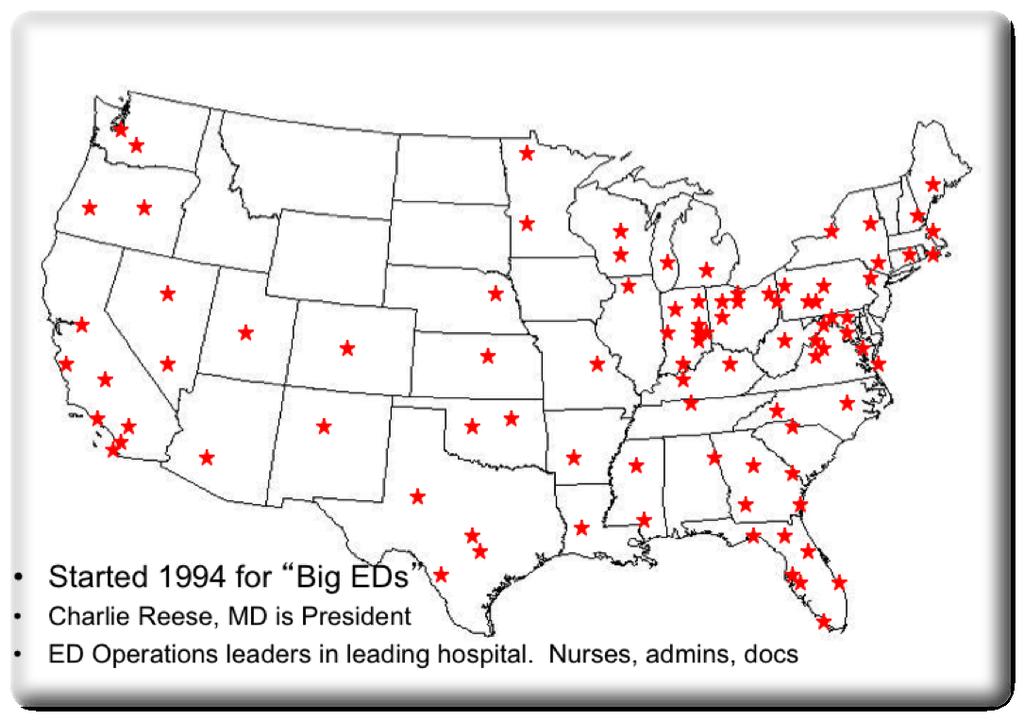
9 ED Benchmarking Alliance

10 EDs Operate in Stairsteps ED Operations reflect Volume Cohorts around 20K
 % Pediatric patients under age 2, and age 2 and 18 % admitted % of total hospital admissions through the ED % transferred to")
11 20 Numbers Needed to Manage an ED Patients Per Day High Acuity (Physician level code 4, 5, or critical care) % Pediatric patients under age 2, and age 2 and 18 % admitted % of total hospital admissions through the ED % transferred to another hospital % arrived by EMS % EMS patients admitted Median length of stay (MLOS) for all patients MLOS Treat and Release Patients Fast Track Patients (if you have one)


12 20 Numbers Needed to Manage an ED Median time Door to Bed and Door to Doctor % of patients Leave Before Treatment Complete Admitted patient decision to movement time EKGs per 100 patients seen Plain X-rays per 100 patients seen CT and MRI scans per 100 patients seen Patient Satisfaction Score Revenue per Patient Financial Contribution to Hospital ED Staff Satisfaction
13 EDBA Survey EDs serving 19 million patients Volume was down 3 to 5% versus 2009 Patient acuity higher, and more patients admitted. Acuity up due to lower volume, no viral (H1N1 or other) outbreaks in 2010 Continued increase in EKG utilization Plateau in use of CT
14 EDBA Survey 2010 EDs are improving throughput, walkaway rates have decreased About 17% arriving by ambulance and are admitted at an increasing rate Payor mix worsened Space utilization around 3.6 visits per square foot Bed Utilization around 1600 visits per patient care space
15 The EDBA Annual Data Survey Sites PPD Hi CPT Acuity Under Age 2 Peds % Admit % Transfer % EMS Arrival EMS Arrival Admit Median LOS TOTAL ALL EDs 2010 in 461 EDs 18.4 m 61.8% 5.0% 21.0% 17.9% 1.7% 16.4% 43.0% 165 Over 80K EDs 2010 results % 5.6% 21.0% 20.8% 1.1% 20.4% 43.7% to 80K EDs 2010 results % 5.2% 20.2% 20.7% 1.0% 19.6% 47.2% to 60K EDs 2010 results % 4.6% 18.5% 19.5% 1.4% 18.3% 44.5% to 40K EDs 2010 results % 4.5% 19.9% 17.6% 1.7% 15.3% 42.6% 152 Under 20K EDs 2010 results % 4.7% 21.6% 13.3% 2.8% 13.1% 38.3% 132 Pediatric EDs 2010 Results % 26.6% 99.9% 12.7% 0.6% 9.2% 34.9% 157 Adult, Specialty EDs 2010 Results % 0.5% 3.2% 27.0% 1.1% 21.5% 46.8% 235 Urgent Care, Freestanding EDs 2010 Results % 3.6% 23.0% 4.3% 3.3% 7.1% 36.0% 93

16 Length of Stay Statistics provided by: Emergency Department Benchmarking Alliance
17 Median Length Stay T&R, Admit Macro Very Large Large Medium Small Micro Pediatric EDs Adult EDs
18 Space Utilization Size of Facility Square Footage Per Bed Macro Very Large Large Medium Small Micro Pediatric EDs Adult EDs
19 The IOM Report Regional Accountable Emergency Systems (RAES) The Hope of RAES Unscheduled Care System Take care of right patient in the right place at the right time Eliminate unnecessary movement and cost (LEAN)
20 The Hospital or System Board How does ED project relate to hospital mission? Fulfill accountability to community and business? (Particularly relevant to hospitals that have community boards of directors) Will ED expansion expose hospital issues? How does form change in the ED lead to operations change for the entire system? Does ED design fulfill hospital system marketing priorities?
21 Mission Statement SAMPLE To facilitate the ED s mission statement and marketing program, a facility update is necessary. The design will fulfill the mission to provide unscheduled care; improve care to all patients with more patient amenities; improve staff satisfaction, productivity, and effectiveness; and maximizes access to care for critically ill or injured. The design will reflect our commitment to the community we serve, and the overall mission of the hospital and health system
22 Hospital Boards expect: Benchmarking The practice of being humble enough to admit that someone else is better at doing something AND Wise enough to learn how to match or surpass them at it And. Cost-Effectiveness
23 The ED Design should Anticipate Older, sicker, medical patients More need to greet promptly More Workup EKG, Complex Imaging, telemetry Access to old records More need to stay clean More family Greater demand for safety
24 The ED Design should Anticipate Learning from L&D Provide care in a dedicated patient space for each patient, meaning no hallway care No Diversion Focus on Flow Beautiful Volume planned well ahead
25 Typical Board Directions for ED Design Customer friendly Streamline process of evaluation, treating and discharging patient Implement new technology Enhance staff productivity and retention Accommodate changing ED patient population and role of the ED in the hospital Cost efficient
26 Growing Business Standard: Lean Models of ED Process Patient greeting gives critical first impression Consider an intake area Patients arriving ambulatory ushered by greeters May also be access point for non-critical EMS traffic Certain EDs will benefit from a physician greeting process at busy times of day
27 Appropriate ED design will decrease our average lengths of stay in the ED. Those who need to spend more time in the ED would have a more comfortable setting in which to stay Careful with LEAN efforts. Many ED patients need some time in the ED for Watchful Waiting. Time in ED alone is not the correct parameter
28 ED volume bands ED leaders should take design cues from EDs that are in the next volume band up from the current ED
29 For many community hospitals, an outpatient medical mall
30 Minimal patient and visitor movement in all critical patient groups
31 Design flexibility for future department and outpatient growth
32 Large lobby area directly on hallway to main hospital waiting area
33 Fast Track area in front of ED, including critical relationship with Xray Departmental Xray should be adjacent to intake area and Fast Track
34 Maximize ability of nurse and physician staff to view patients, but the patients not to view each other. Particularly, resuscitation and cardiac patients should be out of line of sight of other patients
35 Resuscitation area with access to CT, elevators to surgery and units. Cath lab in ED is NOT a proven concept
36 Mental health patient care area isolated in an auditory sense, but visual observation available by staff. Area should not be convenient for patients to escape to interior of hospital or out lobby doors
37 Nursing stations adjoined by supply corridor
38 IS support of Clinical Practice Computer integrated Early implementation patient registration, tracking, and discharge Real time QA for nurses and physicians NextGen = incorporation passive tracking functions for people and equipment
39 Communication system supports bedside clinical work. A separate telephone system supports patient and visitor communication needs
40 Tracking system widely accessible and supports single chart location near the bedside
41 Materials management supports all units, using user-friendly design and recycling
42 All patient care areas can access warm blankets and cold water
43 Signage performs wayfinding without using staff time
44 Food service to support patients, visitors, staff, EMS & police
45 Specific design components critical to success Efficient traffic patterns for ambulances approaching the hospital Consider overall campus traffic flow. The ED must have accommodating parking and patient offload areas Accommodating administrative and staff support area Construction process must allow the ED to continue to provide service to existing patients, and provide appropriate growth
46 Traditional ED Greeting T Help Me!! H E Patient Enters the ED Clerk Greeting Go Sit Nurse Triage Go Sit W A Room Assignment Chart in Rack Doctor L L Message = Time = Finances First 5-20 mins This is my caretaker, Right? 5-20 mins Why am I Waiting? Push or Pull System? Unknown time Unknown time
47 What Happens when Nobody Manages the ED? Waiting Room
48 Consumer Flows The License Bureau Medicaid Office INTAKE PROCESS EXIT Get Me Out Of Here!! Department Store Hotel
49 Funnel Options For The ED The Typical ED ED GREET WORKUP DISCHARGE Get Me Out Of Here!! The Constipated ED he Turnstile ED Pay Arrangements As You Leave The Open ED
50 HOME Or iphone Future Intake System Design Call in by patient or doctor to EDP Patient Care Area Physician, Nurse, Tech Care DISPOSITION We heard you were coming! Work Up Initiated
51 Workup Room For as short a time as possible Sniff Analyzer DC Out Payment Office Intake Doctor Intake Specialists EM S Walk-In
52 The Mass Media Attraction Making the ED Attractive to Staff: What Other Medical Specialty is so Attractive to TV Shows ER
53 Volume Increasing Traffic Access to the ED Becomes More Critical
54 Clinical Decision Unit(s) Improve Flow Improve ED Control over Boarding Good Patient Care!

55 CMS on Admission Times Current Definition Admit Decision to Departure Time Time Interval beginning when Admit Decision is made until the actual departure time of the patient from the ED Proposed as a CMS Hospital Inpatient Quality Measure for public reporting in 2013
56 Reducing Decision to Admit Time The Upstairs Challenge for the Downstairs Staff A CMS Mandate in next 2 Years Headboard Management In-flow Management Bed Command Center Care Initiation Unit Clinical Decision Units PACU s
57 Great Ideas That Work! The Good, the Bad and the Ugly of ED design
58 Concepts Above 30-35K, do Physician in Triage at appropriate times of day Open the Front End Families at bedside Add patient chairs as efficient patient care spaces

59 Focus on Intake Area Who is aware that patients are dying in the waiting room? TJC CMS, OIG State Regulators Prosecutors
60 Procedure Room IVs, Labs Roll Through Triage Sniff Analyzer To E D Security In

61 New Unscheduled Care Solutions Flexible Portable Cross platform decision support Opportunity to become front door of healthcare and personal health

62 ED in Real-Time Is the ED the right place for care? ED wait times Site Schedule an Appt.
63 Color code storage, and carts Build a subwaiting area Numbers matter. Build a good data system Look at L&D for system and designing cues
64 Design team should be multidisciplinary Go somewhere else, traveling together, to look at several EDs Get design elements together before you get off the plane Look up at the next volume band
65 Economic Considerations Consider nationalized medicine system Let Board/C-suite know you have maximized process, need facility Many ED leaders need to focus on renovation, rather then rebuild Some EDs not amenable to renovation (asbestos) Attempt to get CEO to understand the application of less expensive personnel (not management by FTE count)
66 Some Hospitals and EDs have Utilized Discharge Areas
67 Solutions to the Admitting Issues Admitting Process is recreated with every patient?? Apply Bed Ahead planning Design PUSH + PULL systems to get admissions processed correctly The Sunday Night Work Plan
68 Admission Flow Solutions Hospitalists Headboard Management Care Initiation Unit Clinical Decision Units PACU s
69 Disasters Design for The Prepared ED Staff Prep Area Negative Pressure Greeting Areas Communications Command Ctr
70 The ED Wraparound Welcome EMS Existing ED Community Disaster Supplies ED Wraparound Own the Parking Lot Control The Road Decon Space
71 Using the EDBA Data Hi CPT Acuity Peds % Admit % EMS Arrival EMS Arrival Admit Median LOS Over 80K EDs 2010 results 63% 19% 22% 21% 44% to 80K EDs 2010 results 65% 19% 21% 20% 47% to 60K EDs 2010 results 65% 18% 20% 14% 44% 183 Anderson 64% 13% 19% 17% 47% to 40K EDs
72 Using the EDBA Data Hi CPT Acuity Peds % Admit % EMS Arrival EMS Arrival Admit Median LOS LOS Treat & Release LOS Admit LBTC Door to Bed Door to Doc EKG per 100 Xray per 100 CT per 100 % Hosp Admits thru ED Over 80K EDs 2010 results 63% 19% 22% 21% 44% % % to 80K EDs 2010 results 65% 19% 21% 20% 47% % % to 60K EDs 2010 results 65% 18% 20% 14% 44% % % Anderson 64% 13% 19% 17% 47% % % ? 20 to 40K EDs 2010 results 63% 18% 18% 16% 43% % % Under 20K EDs 2010 results 59% 20% 15% 13% 39% % % NA Visits per Foot Beds Visits per Space Admit Time Pediatric EDs 2010 Results 45% 100% 13% 9% 35% % % 3.7 NA Adult, Specialty EDs 2010 Results 70% 3% 27% 21% 49% % %
73 In Our ED Today 130 Patients to be seen, although 3 want to leave 40 Will be in Fast Track 56 Will need Monitors 23 Will be Admitted 26% Of Patients in Main ED 6 Will have Dental Problem 991 Orders will be Entered in CPOE, or 7.6 per patient, and 21% of all orders Entered in the Hospital Today 25 Will Arrive by EMS
74 In Our ED Today 10 Will Arrive by EMS and be Admitted 25 Will be Injured 64 Xray procedures will be Performed 25 CT Procedures will be Performed 39 Will need EKGs 51 Will need IV start 98 Will need lab work
75 Go Home With Some Numbers Plan forward with hard data Know, understand and share your numbers Compare to cohorts Make sure all staff know numbers Tell your story effectively in developing a new system
Emergency Departments The State of the Union Background and Benchmarks
 . Emergency Departments The State of the Union Background and Benchmarks! Prepared by: James Augustine, MD! Director of Clinical Operations, EMP! Associate Clinical Professor, Wright State University Department
. Emergency Departments The State of the Union Background and Benchmarks! Prepared by: James Augustine, MD! Director of Clinical Operations, EMP! Associate Clinical Professor, Wright State University Department
Super Track. The Evolution of the Split Flow Emergency Department. John D Angelo, MD, FACEP Northwell Health
 Super Track The Evolution of the Split Flow Emergency Department John D Angelo, MD, FACEP Northwell Health Robert Masters, AIA, NCARB, LEED AP CannonDesign Agenda 1. Emergency Department Flow 2. Evolution
Super Track The Evolution of the Split Flow Emergency Department John D Angelo, MD, FACEP Northwell Health Robert Masters, AIA, NCARB, LEED AP CannonDesign Agenda 1. Emergency Department Flow 2. Evolution
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
Consultation Paper. Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network
 Consultation Paper Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network Issued: April 2016 TABLE OF CONTENTS TABLE OF CONTENTS 2 1. INTRODUCTION 3 2. PURPOSE
Consultation Paper Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network Issued: April 2016 TABLE OF CONTENTS TABLE OF CONTENTS 2 1. INTRODUCTION 3 2. PURPOSE
Emergency Department
 Emergency Department Elizabeth Lowry, Director, Internal Audit Darlene FitzPatrick, Director, Internal Audit Bon Secours Health System, Inc. ED: Performing a Value-Added Audit Understanding the structure
Emergency Department Elizabeth Lowry, Director, Internal Audit Darlene FitzPatrick, Director, Internal Audit Bon Secours Health System, Inc. ED: Performing a Value-Added Audit Understanding the structure
Chest Pain Accredited. Transplant Program-Heart, Kidney, Liver. Hear Transplant Program serving San Antonio area for 25 years
 PUTTING THE PATIENT FIRST IN PATIENT PLACEMENT 8 Hospital System, 1 Freestanding ED Provide healthcare to 26 surrounding counties within South Texas International Transfer Services Methodist Healthcare
PUTTING THE PATIENT FIRST IN PATIENT PLACEMENT 8 Hospital System, 1 Freestanding ED Provide healthcare to 26 surrounding counties within South Texas International Transfer Services Methodist Healthcare
Managing Queues: Door-2-Exam Room Process Mid-Term Proposal Assignment
 Concept/Objectives Managing Queues: Door--Exam Process Mid-Term Proposal ssignment Children s Healthcare of tlanta (CHO has plans to build a new facility that will be over 00,000 sq. ft., and they are
Concept/Objectives Managing Queues: Door--Exam Process Mid-Term Proposal ssignment Children s Healthcare of tlanta (CHO has plans to build a new facility that will be over 00,000 sq. ft., and they are
Looking at Patient Flow in Hours and Days
 This presenter has nothing to disclose Looking at Patient Flow in Hours and Days Getting Patients to the Right Level of Care at the Right Time October 23, 2014 Session Objectives Understand the differences
This presenter has nothing to disclose Looking at Patient Flow in Hours and Days Getting Patients to the Right Level of Care at the Right Time October 23, 2014 Session Objectives Understand the differences
APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS
 APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS Igor Georgievskiy Alcorn State University Department of Advanced Technologies phone: 601-877-6482, fax:
APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS Igor Georgievskiy Alcorn State University Department of Advanced Technologies phone: 601-877-6482, fax:
Frequently Asked Questions (FAQ) CALNOC 2013 Codebook
 CALNOC 2013 Codebook") Frequently Asked Questions (FAQ) CALNOC 2013 Codebook Maternal/Child and ED Service Lines QUESTION: Are the ED and Maternal/Child measures mandatory? What are the ramifications if we choose not to add
Frequently Asked Questions (FAQ) CALNOC 2013 Codebook Maternal/Child and ED Service Lines QUESTION: Are the ED and Maternal/Child measures mandatory? What are the ramifications if we choose not to add
Managing Psychiatric Patient Throughput in the Emergency Department
 Managing Psychiatric Patient Throughput in the Emergency Department Heartland Healthcare Executive Group (HHEG) October 22, 2015 Agenda Introductions U.S. Mental Health Access Crisis Risks to Patients,
Managing Psychiatric Patient Throughput in the Emergency Department Heartland Healthcare Executive Group (HHEG) October 22, 2015 Agenda Introductions U.S. Mental Health Access Crisis Risks to Patients,
Flex Care : An Integrated Care Delivery Approach for Low Acuity Patients Presenting to the ED
 Flex Care : An Integrated Care Delivery Approach for Low Acuity Patients Presenting to the ED Stuart M. Levine, MD, FACP President and Chief Medical Officer MedStar Harbor Hospital 1 Introduction CY17
Flex Care : An Integrated Care Delivery Approach for Low Acuity Patients Presenting to the ED Stuart M. Levine, MD, FACP President and Chief Medical Officer MedStar Harbor Hospital 1 Introduction CY17
ED Facility Design and Informatics. Disclosure Information. Stock Ownership Forerun. Objectives. A Must Have Book. Estimating Treatment Spaces
 ED Facility Design and Informatics Cambridge Health Alliance Harvard Medical School Cambridge, MA Disclosure Information Stock Ownership Forerun Objectives A Must Have Book! Review planning considerations
ED Facility Design and Informatics Cambridge Health Alliance Harvard Medical School Cambridge, MA Disclosure Information Stock Ownership Forerun Objectives A Must Have Book! Review planning considerations
Kennebec Valley Chamber of Commerce August 21, 2013
 Kennebec Valley Chamber of Commerce August 21, 2013 Keep high-quality health care services in the Kennebec Valley region; reducing the need to travel to Portland or Bangor Over the last year, we have added
Kennebec Valley Chamber of Commerce August 21, 2013 Keep high-quality health care services in the Kennebec Valley region; reducing the need to travel to Portland or Bangor Over the last year, we have added
SARASOTA MEMORIAL HOSPITAL POLICY
 PS1070 POLICY TITLE: SARASOTA MEMORIAL HOSPITAL (SMH) PATIENT FLOW AND OVER EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: PAGE #: 12/1/05 05/12/17 Clinical Non-Clinical 1 of 11 Job Title of Responsible
PS1070 POLICY TITLE: SARASOTA MEMORIAL HOSPITAL (SMH) PATIENT FLOW AND OVER EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: PAGE #: 12/1/05 05/12/17 Clinical Non-Clinical 1 of 11 Job Title of Responsible
We are growing to better serve you
 We are growing to better serve you Message from Robert L. Lord, Jr. Martin Health System President and CEO Founded in 1939, Martin Health System has a rich history of providing care to residents of the
We are growing to better serve you Message from Robert L. Lord, Jr. Martin Health System President and CEO Founded in 1939, Martin Health System has a rich history of providing care to residents of the
The Impact of Emergency Department Use on the Health Care System in Maryland. Deborah E. Trautman, PhD, RN
 The Impact of Emergency Department Use on the Health Care System in Maryland Deborah E. Trautman, PhD, RN The Future of Emergency Care in the United States Health System Institute of Medicine June 2006
The Impact of Emergency Department Use on the Health Care System in Maryland Deborah E. Trautman, PhD, RN The Future of Emergency Care in the United States Health System Institute of Medicine June 2006
Publication Year: 2013
 THE INITIAL ASSESSMENT PROCESS ST. JOSEPH'S HEALTHCARE HAMILTON Publication Year: 2013 Summary: The Initial Assessment Process (IAP) was developed collaboratively by the emergency physicians, nursing,
THE INITIAL ASSESSMENT PROCESS ST. JOSEPH'S HEALTHCARE HAMILTON Publication Year: 2013 Summary: The Initial Assessment Process (IAP) was developed collaboratively by the emergency physicians, nursing,
Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA
 These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
A Prescription for the Free-Standing ED. Kimberly Nealon, St. Vincent Health; Steve Mombach, TriHealth; John Marshall, BremnerDuke Healthcare
 A Prescription for the Free-Standing ED Kimberly Nealon, St. Vincent Health; Steve Mombach, TriHealth; John Marshall, BremnerDuke Healthcare Agenda I. Introductions: Kim, Steve, John II. III. IV. Market
A Prescription for the Free-Standing ED Kimberly Nealon, St. Vincent Health; Steve Mombach, TriHealth; John Marshall, BremnerDuke Healthcare Agenda I. Introductions: Kim, Steve, John II. III. IV. Market
How Integrated Clinical Services and Technologies are Making Healthcare Work Better. Local Practice Divisional Support National Resources
 How Integrated Clinical Services and Technologies are Making Healthcare Work Better Local Practice Divisional Support National Resources YOUR PRESENTERS Kirk Jensen, MD, MBA, FACEP Chief Medical Officer,
How Integrated Clinical Services and Technologies are Making Healthcare Work Better Local Practice Divisional Support National Resources YOUR PRESENTERS Kirk Jensen, MD, MBA, FACEP Chief Medical Officer,
Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care
 Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care Deborah Campbell Inova Fairfax Medical Campus Edwards Healthcare Leadership Series September
Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care Deborah Campbell Inova Fairfax Medical Campus Edwards Healthcare Leadership Series September
Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC
 Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC Objectives Identify measures to facilitate Emergency Department throughput for non-emergent
Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC Objectives Identify measures to facilitate Emergency Department throughput for non-emergent
LHH Acute Care Transfers Update
 LHH Acute Care Transfers Update July 12, 2016 LHH Joint Conference Committee Background LHH patients requiring acute hospital care frequently cannot be admitted to ZSFG, which may result in compromised
LHH Acute Care Transfers Update July 12, 2016 LHH Joint Conference Committee Background LHH patients requiring acute hospital care frequently cannot be admitted to ZSFG, which may result in compromised
Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare
 Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare Why build Principles of observational medicine ROI ED Hospital Clinical implications Define intended d use Open, closed or mixed use Impact
Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare Why build Principles of observational medicine ROI ED Hospital Clinical implications Define intended d use Open, closed or mixed use Impact
Planning for Improved Access and Orientation Anjali Joseph Jain EDRA 35
 Hospital planning strategies for improving patient access and orientation within the hospital Anjali Joseph, College of Architecture, Georgia Institute of Technology Most hospitals have been designed through
Hospital planning strategies for improving patient access and orientation within the hospital Anjali Joseph, College of Architecture, Georgia Institute of Technology Most hospitals have been designed through
FY2016 Budget Presentation
 FY2016 Budget Presentation CCHHS Finance Committee Meeting Dr. Jay Shannon, CEO Doug Elwell, Deputy CEO for Finance & Strategy August 21, 2015 FY15 Accomplishments Finances Hiring on track to fill 1,000
FY2016 Budget Presentation CCHHS Finance Committee Meeting Dr. Jay Shannon, CEO Doug Elwell, Deputy CEO for Finance & Strategy August 21, 2015 FY15 Accomplishments Finances Hiring on track to fill 1,000
Clinical Operations in a Service Line Model
 Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
Profit = Price - Cost. TAKT Time Map Capacity Tables. Morale. Total Productive Maintenance. Visual Control. Poka-yoke (mistake proofing) Kanban.
 Kanban.") GPS Mod 22 7 Flows of Medicine MUDA MUDA Cost Reduction By Eliminating Waste Just-in-Time Profit = Price - Cost GPS Depth Study NVA/VA- Functions/Mgrs R e d e p l o y m e n t Jidoka (human automation)
GPS Mod 22 7 Flows of Medicine MUDA MUDA Cost Reduction By Eliminating Waste Just-in-Time Profit = Price - Cost GPS Depth Study NVA/VA- Functions/Mgrs R e d e p l o y m e n t Jidoka (human automation)
Countywide Emergency Department Ambulance Patient Transfer of Care Report Performance Report
 Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/11/2016 Contra Costa
Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/11/2016 Contra Costa
Ascom MEDSTAR FRANKLIN SQUARE MEDICAL CENTER ASCOM COMMUNICATIONS STREAMLINE WORKFLOW THROUGH CLINICAL INTEGRATION. Introduction
 Customer: Medstar Franklin Square Medical Center Solution: Ascom Unite, IP-DECT handsets and clinical integrations MEDSTAR FRANKLIN SQUARE MEDICAL CENTER ASCOM COMMUNICATIONS STREAMLINE WORKFLOW THROUGH
Customer: Medstar Franklin Square Medical Center Solution: Ascom Unite, IP-DECT handsets and clinical integrations MEDSTAR FRANKLIN SQUARE MEDICAL CENTER ASCOM COMMUNICATIONS STREAMLINE WORKFLOW THROUGH
Riverside s Vigilance Care Delivery Systems include several concepts, which are applicable to staffing and resource acquisition functions.
 1 EP8: Describe and demonstrate how nurses used trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery System(s). Riverside Medical
1 EP8: Describe and demonstrate how nurses used trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery System(s). Riverside Medical
Managing Faculty Performance and Productivity. Sara M. Larch, FACMPE VP, Physician Services Inova Health System. Overview
 Association of Specialty Professors Division Chiefs Symposium March 3, 00 Managing Faculty Performance and Productivity Sara M. Larch, FACMPE VP, Physician Services Inova Health System Overview Measuring
Association of Specialty Professors Division Chiefs Symposium March 3, 00 Managing Faculty Performance and Productivity Sara M. Larch, FACMPE VP, Physician Services Inova Health System Overview Measuring
Welcome. A Guide for Patients and Visitors
 Welcome A Guide for Patients and Visitors 1 University s Heart & Vascular Institute is a world-class facility, thoughtfully and masterfully designed around the patient experience. The four-story heart
Welcome A Guide for Patients and Visitors 1 University s Heart & Vascular Institute is a world-class facility, thoughtfully and masterfully designed around the patient experience. The four-story heart
LWOT Reduction Plan Success Story: Advocate Trinity Hospital
 LWOT Reduction Plan Success Story: Advocate Trinity Hospital Draft Submitted Jan. 6, 2011 Jacquelyn Whitten, DNP, RN Kimberly McIntyre, EdD(c), MSN, RN Julian M. Magdaleno, MS February 19, 2012 The Leaving
LWOT Reduction Plan Success Story: Advocate Trinity Hospital Draft Submitted Jan. 6, 2011 Jacquelyn Whitten, DNP, RN Kimberly McIntyre, EdD(c), MSN, RN Julian M. Magdaleno, MS February 19, 2012 The Leaving
Emergency Department Throughput : The Cambridge Health Alliance Experience
 Emergency Department Throughput : The Cambridge Health Alliance Experience Assaad J. Sayah, MD, FACEP Sr. V.P. & Chief Medical Officer President, CHA Physician Organization IHI 2016 Cambridge Health Alliance
Emergency Department Throughput : The Cambridge Health Alliance Experience Assaad J. Sayah, MD, FACEP Sr. V.P. & Chief Medical Officer President, CHA Physician Organization IHI 2016 Cambridge Health Alliance
Developing an ED Facility Charge Calculator March 3, :00pm
 Developing an ED Facility Charge Calculator March 3, 2016 4:00pm Neal Kothe, The Ohio State University Wexner Medical Center Carol Gray, The Ohio State University Wexner Medical Center Conflict of Interest
Developing an ED Facility Charge Calculator March 3, 2016 4:00pm Neal Kothe, The Ohio State University Wexner Medical Center Carol Gray, The Ohio State University Wexner Medical Center Conflict of Interest
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
Proceedings of the 2005 Systems and Information Engineering Design Symposium Ellen J. Bass, ed.
 Proceedings of the 2005 Systems and Information Engineering Design Symposium Ellen J. Bass, ed. ANALYZING THE PATIENT LOAD ON THE HOSPITALS IN A METROPOLITAN AREA Barb Tawney Systems and Information Engineering
Proceedings of the 2005 Systems and Information Engineering Design Symposium Ellen J. Bass, ed. ANALYZING THE PATIENT LOAD ON THE HOSPITALS IN A METROPOLITAN AREA Barb Tawney Systems and Information Engineering
FUNCTIONAL PROGRAM for General Hospital
 FUNCTIONAL PROGRAM for General Hospital 1 General Considerations 1.1 Applicability As discussed with WY Dept of Health, it is anticipated that this facility will be surveyed and licensed as a General Hospital.
FUNCTIONAL PROGRAM for General Hospital 1 General Considerations 1.1 Applicability As discussed with WY Dept of Health, it is anticipated that this facility will be surveyed and licensed as a General Hospital.
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Low Acuity Emergency Department Visits. Joanna Cohen, MD June 2018
 Low Acuity Emergency Department Visits Joanna Cohen, MD June 2018 Goals and Objectives Identify and quantify low acuity ED visits Analyze challenges associated with low acuity ED visits Assess the impact
Low Acuity Emergency Department Visits Joanna Cohen, MD June 2018 Goals and Objectives Identify and quantify low acuity ED visits Analyze challenges associated with low acuity ED visits Assess the impact
The Transformation of Mount Sinai Beth Israel June 8 th Presentation before PHHPC
 The Transformation of Mount Sinai Beth Israel June 8 th Presentation before PHHPC 1 Mount Sinai Health System: Who We Are Integrated Health System of 7 hospitals with more than 200 community locations
The Transformation of Mount Sinai Beth Israel June 8 th Presentation before PHHPC 1 Mount Sinai Health System: Who We Are Integrated Health System of 7 hospitals with more than 200 community locations
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care
 Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
San Diego County 4 th Annual Overcrowding Summit. Roneet Lev, MD, FACEP
 San Diego County 4 th Annual Overcrowding Summit Roneet Lev, MD, FACEP Agenda Purpose of this conference Improve ED Care in San Diego County Inspire Ideas Learn from each others to improve care Collegiality
San Diego County 4 th Annual Overcrowding Summit Roneet Lev, MD, FACEP Agenda Purpose of this conference Improve ED Care in San Diego County Inspire Ideas Learn from each others to improve care Collegiality
Accomplishments Fiscal Year UPMC Passavant
 Accomplishments Fiscal Year 2015 UPMC Passavant UPMC Passavant Summary of Significant FY15 Accomplishments Continue employee engagement initiatives that are aligned with UPMC Passavant s Mission, Vision,
Accomplishments Fiscal Year 2015 UPMC Passavant UPMC Passavant Summary of Significant FY15 Accomplishments Continue employee engagement initiatives that are aligned with UPMC Passavant s Mission, Vision,
Measure: Current State Spaghetti Diagram
 Visual representation of process Measure: Current State Spaghetti Diagram Registration Triage Nursing Station Walk In Patient Total Time - 4:52 Entry to Triage 45min Triage to Bed-1:30 Bed to Disposition-2:35
Visual representation of process Measure: Current State Spaghetti Diagram Registration Triage Nursing Station Walk In Patient Total Time - 4:52 Entry to Triage 45min Triage to Bed-1:30 Bed to Disposition-2:35
Oregon Medical Group Team Medicine 3 April 2014
 Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Section 3. Functional Diagrams. Outpatient Clinic Satellite / Community-Based January 2009
 Functional Diagrams Section 3 Page General Considerations...3-1 Planning Module...3-2 Legend for Functional Diagrams...3-2 Clinics Single Module Relationship Diagram...3-3 Clinics Multiple Module Relationship
Functional Diagrams Section 3 Page General Considerations...3-1 Planning Module...3-2 Legend for Functional Diagrams...3-2 Clinics Single Module Relationship Diagram...3-3 Clinics Multiple Module Relationship
Wait Time Information in Priority Areas: Definitions
 Wait Time Information in Priority Areas: Definitions 1 Background In 2004, Canada's first ministers agreed to work towards reducing wait times for five priority areas: cancer treatment, cardiac care, diagnostic
Wait Time Information in Priority Areas: Definitions 1 Background In 2004, Canada's first ministers agreed to work towards reducing wait times for five priority areas: cancer treatment, cardiac care, diagnostic
Emerus, The Nation s Innovator of Micro-Hospitals
 Emerus, The Nation s Innovator of Micro-Hospitals VIC SCHMERBECK Executive Vice President of Strategy and Business Development 20+ yrs. Exp. Investment & Merchant Banking Healthcare & emerging markets
Emerus, The Nation s Innovator of Micro-Hospitals VIC SCHMERBECK Executive Vice President of Strategy and Business Development 20+ yrs. Exp. Investment & Merchant Banking Healthcare & emerging markets
Emergency Department Patient Flow Strategies. University of Maryland Medical Center
 Emergency Department Patient Flow Strategies University of Maryland Medical Center Medical Admitting Officer Attending Hospitalist Hours: 9a 11p Mon Friday Goal to partner with ED team and provide oversight
Emergency Department Patient Flow Strategies University of Maryland Medical Center Medical Admitting Officer Attending Hospitalist Hours: 9a 11p Mon Friday Goal to partner with ED team and provide oversight
MOHAWK VALLEY HEALTH SYSTEM INTEGRATED HEALTH CAMPUS UTICA, NY
 MOHAWK VALLEY HEALTH SYSTEM INTEGRATED HEALTH CAMPUS UTICA, NY 1 MAJOR PROJECT MILESTONES 2 MAJOR PROJECT MILESTONES MVHS announces it is exploring opportunities to fund and build a new, combined hospital
MOHAWK VALLEY HEALTH SYSTEM INTEGRATED HEALTH CAMPUS UTICA, NY 1 MAJOR PROJECT MILESTONES 2 MAJOR PROJECT MILESTONES MVHS announces it is exploring opportunities to fund and build a new, combined hospital
Thank you for joining us today!
 Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. 1 Emergency Room Overcrowding A multi-dimensional
Thank you for joining us today! Please dial 1.800.732.6179 now to connect to the audio for this webinar. To show/hide the control panel click the double arrows. 1 Emergency Room Overcrowding A multi-dimensional
Your Choice. 3-Tier Network Option Plan
 Your Choice 3-Tier Network Option Plan What is Your Choice? Click Here to Watch Video Your Top Questions What is Your Choice? Are my doctors in the plan? Are my medications covered by the plan? If I get
Your Choice 3-Tier Network Option Plan What is Your Choice? Click Here to Watch Video Your Top Questions What is Your Choice? Are my doctors in the plan? Are my medications covered by the plan? If I get
University of Michigan Health System Program and Operations Analysis. Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients
 University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
"Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital
 "Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital The University of Kansas Hospital Leading the Nation in Caring, Healing,
"Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital The University of Kansas Hospital Leading the Nation in Caring, Healing,
Countywide Emergency Department Ambulance Patient Transfer of Care Report Performance Report
 Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/28/2017 Patient Transfer
Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/28/2017 Patient Transfer
New Regional Hospital Questions & Answers
 New Regional Hospital Questions & Answers 1. There have been so many numbers tossed around, comparing beds and rooms in the current facility, to what is proposed in the new. Can you please explain the
New Regional Hospital Questions & Answers 1. There have been so many numbers tossed around, comparing beds and rooms in the current facility, to what is proposed in the new. Can you please explain the
COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL. Sepsis Treatment Order Sets Sepsis Treatment Order Sets
 Publication Year: 2013 COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL Summary: An organized accepted approach to sepsis recognition, early management in the ED including specific
Publication Year: 2013 COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL Summary: An organized accepted approach to sepsis recognition, early management in the ED including specific
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
ED Process Improvement Program HSAA (2012/13)
") Peterborough Regional Health Centre Update ED Process Improvement Program HSAA (2012/13) Central East Local Health Integration Network August 22, 2012 1 Overview of Presentation Focus on process improvement
Peterborough Regional Health Centre Update ED Process Improvement Program HSAA (2012/13) Central East Local Health Integration Network August 22, 2012 1 Overview of Presentation Focus on process improvement
Hospital Performance Report for Emergency Department Measures
 QUALIS HEALTH Hospital Outpatient Quality Reporting Hospital Performance Report for Emergency Department Measures Community: Washington State Includes Data Through: Q2 2015 - Q1 2016 Report Created: April
QUALIS HEALTH Hospital Outpatient Quality Reporting Hospital Performance Report for Emergency Department Measures Community: Washington State Includes Data Through: Q2 2015 - Q1 2016 Report Created: April
Matching Capacity and Demand:
 We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
Perfecting Emergency Department Operations
 These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
Predictive Analytics:
 Predictive Analytics: Real-world experiences of HIEs Transforming Themselves Mark J. Jacobs, MHA, CPHIMSS CIO, Delaware Health Information Network Becker's Hospital Review 3rd Annual Health IT + Revenue
Predictive Analytics: Real-world experiences of HIEs Transforming Themselves Mark J. Jacobs, MHA, CPHIMSS CIO, Delaware Health Information Network Becker's Hospital Review 3rd Annual Health IT + Revenue
Ambulatory Care Model
 Ambulatory Care Model Hong Kong May 2013 Andrew Stripp Deputy Chief Executive & Chief Operating Officer Outline What is the Alfred Centre? How does it fit into Alfred Health service model Key aspects of
Ambulatory Care Model Hong Kong May 2013 Andrew Stripp Deputy Chief Executive & Chief Operating Officer Outline What is the Alfred Centre? How does it fit into Alfred Health service model Key aspects of
BAY PARK HOSPITAL. CLIENT: ProMedica
 ProMedica Master Planning and Functional Programming 240,000 SF BAY PARK HOSPITAL The ProMedica System is a major integrated healthcare delivery system located in Northern Ohio and Southern Michigan. The
ProMedica Master Planning and Functional Programming 240,000 SF BAY PARK HOSPITAL The ProMedica System is a major integrated healthcare delivery system located in Northern Ohio and Southern Michigan. The
QUESTIONS. Print Student s/faculty Name: Date of Test Completion: Site of Experience: School/University: Semester:
 2017 - QUESTIONS Print Student s/faculty Name: Date of Test Completion: Site of Experience: School/University: Semester: Instructions: Read each question, write an answer on space provided, and return
2017 - QUESTIONS Print Student s/faculty Name: Date of Test Completion: Site of Experience: School/University: Semester: Instructions: Read each question, write an answer on space provided, and return
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
A GUIDE TO THE CRANBERRY CAMPUS EMERGENCY DEPARTMENT
 A GUIDE TO THE CRANBERRY CAMPUS EMERGENCY DEPARTMENT WELCOME TO UPMC PASSAVANT-CRANBERRY EMERGENCY DEPARTMENT The staff at UPMC Passavant-Cranberry would like to make your visit with us as easy and comfortable
A GUIDE TO THE CRANBERRY CAMPUS EMERGENCY DEPARTMENT WELCOME TO UPMC PASSAVANT-CRANBERRY EMERGENCY DEPARTMENT The staff at UPMC Passavant-Cranberry would like to make your visit with us as easy and comfortable
The Quality Colloquium on the Campus of Harvard University Annenberg Hall in Memorial Hall 45 Quincy Street, Cambridge, MA August 19-22, 2007
 The Quality Colloquium on the Campus of Harvard University Annenberg Hall in Memorial Hall 45 Quincy Street, Cambridge, MA August 19-22, 2007 Anshen+Allen Associated Architects for Palomar Pomerado Health
The Quality Colloquium on the Campus of Harvard University Annenberg Hall in Memorial Hall 45 Quincy Street, Cambridge, MA August 19-22, 2007 Anshen+Allen Associated Architects for Palomar Pomerado Health
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Proceedings of the 2016 Winter Simulation Conference T. M. K. Roeder, P. I. Frazier, R. Szechtman, E. Zhou, T. Huschka, and S. E. Chick, eds.
 Proceedings of the 2016 Winter Simulation Conference T. M. K. Roeder, P. I. Frazier, R. Szechtman, E. Zhou, T. Huschka, and S. E. Chick, eds. IDENTIFYING THE OPTIMAL CONFIGURATION OF AN EXPRESS CARE AREA
Proceedings of the 2016 Winter Simulation Conference T. M. K. Roeder, P. I. Frazier, R. Szechtman, E. Zhou, T. Huschka, and S. E. Chick, eds. IDENTIFYING THE OPTIMAL CONFIGURATION OF AN EXPRESS CARE AREA
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Linking Performance to Improvement: Using a System-wide Measurement Tool. Society for Health Systems February 2005
 Linking Performance to Improvement: Using a System-wide Measurement Tool Society for Health Systems February 2005 Presenters Kathryn Munsterman, FHIMSS Gulf Coast Division Office Senior Management Engineer
Linking Performance to Improvement: Using a System-wide Measurement Tool Society for Health Systems February 2005 Presenters Kathryn Munsterman, FHIMSS Gulf Coast Division Office Senior Management Engineer
Objective: Emergency Access Number Always use the code words, not the actual emergency!
 Emergency Codes Objective: At the end of this self-study module, participants will be able to demonstrate knowledge of all emergency codes and their responsibilities during each code. All codes are initiated
Emergency Codes Objective: At the end of this self-study module, participants will be able to demonstrate knowledge of all emergency codes and their responsibilities during each code. All codes are initiated
Clinical Operations in a Service Line Model
 These presenters have nothing to disclose. Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line
These presenters have nothing to disclose. Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line
Hospital Urgent Care Operations: A Pathway to Profitability
 Hospital Urgent Care Operations: A Pathway to Profitability Alan A. Ayers, MBA, MAcc Chief Executive Officer, Velocity Urgent Care Vice President of Strategic Initiatives, Practice Velocity, LLC Practice
Hospital Urgent Care Operations: A Pathway to Profitability Alan A. Ayers, MBA, MAcc Chief Executive Officer, Velocity Urgent Care Vice President of Strategic Initiatives, Practice Velocity, LLC Practice
Emergency Codes - Ouellette Campus
 The Emergency Codes # is: 555 CODE RED - FIRE 555 CODE PURPLE - HOSTAGE SITUATION OR PERSON WITH WEAPON CODE BLUE - CARDIAC ARREST CODE GREEN - EVACUATION CODE YELLOW - MISSING PATIENT CODE BLACK - CODE
The Emergency Codes # is: 555 CODE RED - FIRE 555 CODE PURPLE - HOSTAGE SITUATION OR PERSON WITH WEAPON CODE BLUE - CARDIAC ARREST CODE GREEN - EVACUATION CODE YELLOW - MISSING PATIENT CODE BLACK - CODE
How to Optimize ASC Efficiency Through Design
 ISSUE BRIEF How to Optimize ASC Efficiency Through Design O perational efficiency is an essential consideration in the development of any new health care facility, particularly ambulatory surgery centers.
ISSUE BRIEF How to Optimize ASC Efficiency Through Design O perational efficiency is an essential consideration in the development of any new health care facility, particularly ambulatory surgery centers.
Brent Treichler, M.D., FACEP Assistant Professor, UT Southwestern Department of Surgery, Division of Emergency Medicine Chief of Emergency Services,
 Brent Treichler, M.D., FACEP Assistant Professor, UT Southwestern Department of Surgery, Division of Emergency Medicine Chief of Emergency Services, Parkland Health and Hospital System September 13, 2010
Brent Treichler, M.D., FACEP Assistant Professor, UT Southwestern Department of Surgery, Division of Emergency Medicine Chief of Emergency Services, Parkland Health and Hospital System September 13, 2010
Building a healthier community Our new ER is coming!
 corona HEALTH NEWS from SPRING 2017 REGIONAL MEDICAL CENTER Building a healthier community Our new ER is coming! Transforming healthcare Improving the patient experience Diagnosing chronic reflux Minimally
corona HEALTH NEWS from SPRING 2017 REGIONAL MEDICAL CENTER Building a healthier community Our new ER is coming! Transforming healthcare Improving the patient experience Diagnosing chronic reflux Minimally
Vanderbilt University Medical Center. Division of Trauma and Surgical Critical Care. Clinical Management Guideline: Standard Trauma Resuscitation
 Introduction Vanderbilt University Medical Center Division of Trauma and Surgical Critical Care Clinical Management Guideline: Standard Trauma Resuscitation Good communication and leadership are the keys
Introduction Vanderbilt University Medical Center Division of Trauma and Surgical Critical Care Clinical Management Guideline: Standard Trauma Resuscitation Good communication and leadership are the keys
Improving Care Coordination to Manage an ACO Population. Greater Baltimore Medical Center
 Improving Care Coordination to Manage an ACO Population Greater Baltimore Medical Center Presenter: Julie Silver September 27, 2012 Background Greater Baltimore Medical Center (GBMC) 281 Licensed Beds
Improving Care Coordination to Manage an ACO Population Greater Baltimore Medical Center Presenter: Julie Silver September 27, 2012 Background Greater Baltimore Medical Center (GBMC) 281 Licensed Beds
TORRANCE MEMORIAL MEDICAL STAFF
 BYLAWS COMMITTEE: APPROVED WITH NO CHANGES 10/3/2017 Dates Approved: Medical Executive Committee 09/14/2010; 12/9/2014 PATIENT ATTRIBUTION PLAN: This Attribution Plan assures that all staff are able to
BYLAWS COMMITTEE: APPROVED WITH NO CHANGES 10/3/2017 Dates Approved: Medical Executive Committee 09/14/2010; 12/9/2014 PATIENT ATTRIBUTION PLAN: This Attribution Plan assures that all staff are able to
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE
 EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Hospital Outpatient Quality Reporting Program
 Hospital Outpatient Quality Reporting Program Support Contractor OQR 2016 Specifications Manual Update Questions & Answers Moderator: Pam Harris, BSN Speakers: Nina Rose, MA Samantha Berns, MSPH Bob Dickerson,
Hospital Outpatient Quality Reporting Program Support Contractor OQR 2016 Specifications Manual Update Questions & Answers Moderator: Pam Harris, BSN Speakers: Nina Rose, MA Samantha Berns, MSPH Bob Dickerson,
Executive Summary November 2008
 November 2008 Purpose of the Study This study analyzes short-term risks and provides recommendations on longer-term policy opportunities for the Marin County healthcare delivery system in general as well
November 2008 Purpose of the Study This study analyzes short-term risks and provides recommendations on longer-term policy opportunities for the Marin County healthcare delivery system in general as well
Urgent Care Centers and Free-Standing Emergency Rooms: A Necessary Alternative under the ACA
 Urgent Care Centers and Free-Standing Emergency Rooms: A Necessary Alternative under the ACA Kim Harvey Looney, Waller Lansden Dortch and Davis Mollie K. O Brien, Epstein Becker Green Jon Sundock, CareSpot
Urgent Care Centers and Free-Standing Emergency Rooms: A Necessary Alternative under the ACA Kim Harvey Looney, Waller Lansden Dortch and Davis Mollie K. O Brien, Epstein Becker Green Jon Sundock, CareSpot
Outpatient Quality Reporting Program
 The Question and Answer Show Moderator: Karen VanBourgondien, BSN, RN Speaker(s): Pam Harris, BSN, RN June 21, 2017 10:00 am Isn't Q2 submission due August 1, 2017? August 1, 2017 deadline is for Quarter
The Question and Answer Show Moderator: Karen VanBourgondien, BSN, RN Speaker(s): Pam Harris, BSN, RN June 21, 2017 10:00 am Isn't Q2 submission due August 1, 2017? August 1, 2017 deadline is for Quarter
Where Can You Volunteer
 Patient Areas Where Can You Volunteer Ambulatory Day Care To provide assistance with the care of the patient in Ambulatory Day Care, Pre and post operatively and to assist with maintaining a communication
Patient Areas Where Can You Volunteer Ambulatory Day Care To provide assistance with the care of the patient in Ambulatory Day Care, Pre and post operatively and to assist with maintaining a communication
Cloud Analytics As A Service
 Cloud Analytics As A Service Enabling Actionable Realtime Data Analytics July 13, 2016 Joanne White, CIO Mark Gerschutz, Director of IT Rick Crawford, Interface Architect Christine Wulff, RN, ED Analyst
Cloud Analytics As A Service Enabling Actionable Realtime Data Analytics July 13, 2016 Joanne White, CIO Mark Gerschutz, Director of IT Rick Crawford, Interface Architect Christine Wulff, RN, ED Analyst
One Hospital, Two Campuses. Delivering more services and better care to all of Rockford.
 One Hospital, Two Campuses Delivering more services and better care to all of Rockford. With nearly $1 billion in investment in the Rockford area, it can be hard to keep up on Mercyhealth s many service
One Hospital, Two Campuses Delivering more services and better care to all of Rockford. With nearly $1 billion in investment in the Rockford area, it can be hard to keep up on Mercyhealth s many service
Effective Date: 7/2004
 MEDICAL STAFF POLICY & PROCEDURE Page 1 of 6 Effective Date: 7/2004 Review/Revised: 9/1/2011 Policy No. MSP 003 Purpose: To assure that physicians at all levels are familiar with their roles during the
MEDICAL STAFF POLICY & PROCEDURE Page 1 of 6 Effective Date: 7/2004 Review/Revised: 9/1/2011 Policy No. MSP 003 Purpose: To assure that physicians at all levels are familiar with their roles during the
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Procedure. Applies To: UNM Hospitals Responsible Department: Quality Revised: 03/2014
 Procedure Patient Age Group: ( ) N/A ( ) All Ages ( ) Newborns (X) Pediatric (x ) Adult DESCRIPTION/OVERVIEW UNM Hospitals (UNMH) is recognized as a large academic health care system providing services
Procedure Patient Age Group: ( ) N/A ( ) All Ages ( ) Newborns (X) Pediatric (x ) Adult DESCRIPTION/OVERVIEW UNM Hospitals (UNMH) is recognized as a large academic health care system providing services
TeleCardiology Platform
 TeleCardiology Platform Michael GeRue MSN, COO Parkview Heart Institute October 21, 2017 Disclosures None TeleCardiology Telehealth fits into the IHI Triple Aim: Patient experience Less travel time, easier
TeleCardiology Platform Michael GeRue MSN, COO Parkview Heart Institute October 21, 2017 Disclosures None TeleCardiology Telehealth fits into the IHI Triple Aim: Patient experience Less travel time, easier
BCBSTX Admission Type Definitions Grouper Version 33
 Shared NPI between Acute Care and Specialty Provider numbers NPI is not shared between Acute Care and Specialty Provider numbers Residential Treatment Center, Eating Disorder Inpatient DRG 876, 880-887
Shared NPI between Acute Care and Specialty Provider numbers NPI is not shared between Acute Care and Specialty Provider numbers Residential Treatment Center, Eating Disorder Inpatient DRG 876, 880-887