How Integrated Clinical Services and Technologies are Making Healthcare Work Better. Local Practice Divisional Support National Resources
|
|
|
- Rudolph McDaniel
- 5 years ago
- Views:
Transcription

1 How Integrated Clinical Services and Technologies are Making Healthcare Work Better Local Practice Divisional Support National Resources



2 YOUR PRESENTERS Kirk Jensen, MD, MBA, FACEP Chief Medical Officer, Best Practices, Inc. Executive Vice President, EmCare W. Mark Hamm, MBA Chief Executive Officer EmCare Hospital Medicine 2
3 OUTLINE Proposed format: 2:00-2:03 EDT Intro the call and housekeeping (Becker s) 2:03-2:05 Brief bios of the presenters 2:05-2:35 Dr. Jensen: Benefits of hospital-wide integration - Fostering a culture of integration & collaboration across departments - Medical leadership and alignment with hospital goals - Improved throughput reduces cost, improves patient satisfaction - Critical success factors for successfully integrating clinical operations 2:35-2:40 Mark describes example of EM and HM integration - Impact of ED boarding & implications for lost revenue - Process supporting early discharge from inpatient unit 2:40-2:50 Mark: Innovations & case studies - Integrated clinical technology to support clinical integration across service lines - Improved communications leads to improved flow, better care and better financial metrics - Experience of StoneCrest and other customers 2:50-3:00 Q&A. Kirk B. Jensen. MD, MBA, FACEP 3

4 Our Goals and Objectives Outline the benefits of hospitalwide integration Illustrate how Emergency Medicine and Hospitalist Medicine clinicians can work effectively together Discuss integration, innovation and selected case studies A healthcare system that works for your patients, your healthcare team, and for you Kirk B. Jensen. MD, MBA, FACEP 4

5 There are differing views of health care reform The impact and uncertainty of health care reform tops the list of more than one healthcare professional Kirk B. Jensen. MD, MBA, FACEP 5

6



7 The Future is Now-The Baby Boomers are Here Demographic growth is driven by the elderly: The 65 and older age cohort will experience a 28% growth in the next decade One baby-boomer turns 50 every 18 seconds and one baby-boomer turns 60 every 7 seconds (10,000 a day) This will continue for the next 18 years This cohort will comprise 15% of the total population by 2016 A higher proportion of patients in this cohort, in comparison to other age groups, are triaged with an emergent condition One-quarter of Medicare beneficiaries have five or more chronic conditions, sees an average of 13 physicians per year, and fills 50 prescriptions per year Kirk B. Jensen. MD, MBA, FACEP 7

8 Peter Drucker s Observations on Hospitals and Healthcare The hospital is altogether the most complex human organization ever devised. Kirk B. Jensen. MD, MBA, FACEP 8
9 TJC AND HOSPITAL-WIDE PATIENT FLOW TJC and the Hospital- Wide Patient Flow Committee: JCR Leadership Standard LD The Joint Commission says Boarding in the ED requires a hospital-wide solution. * *As reported in ACEP NEWS January 14, 2013 The leaders develop and implement plans to identify and mitigate impediments to efficient patient flow throughout the hospital. Effective for all accredited hospitals on January 1, 2005 Performance standards put into effect Jan 1, 2013 require hospital leaders namely the chief executive officer, medical staff and other senior hospital managers to set specific goals to: Improve patient flow Ensure availability of patient beds Maintain proper throughput in labs, ORs, inpatient units, telemetry, radiology and postanesthesia care units We want to make sure that organizations are looking at patient flow hospital-wide, even if the manifestation of a flow problem seems to be in the emergency room. ~ Lynne Bergero, The Joint Commission Kirk B. Jensen. MD, MBA, FACEP 9 9


10 HOSPITAL-WIDE PATIENT FLOW AND THE EMERGENCY DEPARTMENT Nearly half of the EDs in the U.S. report operating at or above capacity Approximately 500,000 ambulances are diverted each year away from the closest hospital 9 out of 10 hospitals report boarding patients in the ED while waiting for inpatient beds Kirk B. Jensen. MD, MBA, FACEP 10


11 AS A HOSPITAL S ED PERCENTILE RANKING INCREASES, SO DOES ITS HCAHPS OVERALL PERCENTILE RANKING* *Courtesy of a Studer Group analysis Kirk B. Jensen. MD, MBA, FACEP 11


12 THE TRIPLE AIM Improving care, improving health, reducing costs Improving the U.S. health care system requires simultaneous pursuit of three aims: improving the experience of care, improving the health of populations, and reducing per capita costs of health care. The integrator s role includes at least five components: partnership with individuals and families, redesign of primary care, population health management, financial management, and macro system integration. Preconditions for this include the enrollment of an identified population, a commitment to universality for its members, and the existence of an organization (an integrator ) that accepts responsibility for all three aims for that population. Health Affairs 27, no. 3 (208) /hlthaff Trendwatch Kirk B. Jensen. MD, MBA, FACEP 12

13 HOSPITAL-WIDE PATIENT FLOW Poor patient flow has a negative impact on overall hospital performance, slowing throughput and decreasing capacity. The negative impact of inefficient patient flow is often felt most in the emergency department, where movement, flexibility and efficiency are critical. Kirk B. Jensen. MD, MBA, FACEP Poor collaboration, strained communication, silo mentalities, and differing incentives contribute to fragmented relationships between emergency medicine and hospital medicine physicians. A primary culprit is physician communication and hand-offs at admission moving patients from the emergency department to the inpatient units. 13

14 MAJOR PATIENT FLOW DRIVERS Emergency Department Efficiency and Effectiveness The emergency department (E.D.) is the front door of the hospital. It addresses the urgent and acute care needs of patients. For many patients, the E.D. is only the first phase of their hospital experience. Approximately 50% of inpatient admissions come from the E.D In the E.D., efficiency and productivity are critical. Seconds count. Improving E.D. throughput has a distinct impact on success. Redesign efforts should focus on staffing, triage, registration and other patient-centered care factors. The Centers for Medicare & Medicaid Services (CMS) goals for 2013 and 2014 include measures to record improvement in E.D. efficiency and throughput times. Kirk B. Jensen. MD, MBA, FACEP 14
15 MAJOR PATIENT FLOW DRIVERS Hospital System Efficiency and Effectiveness Lab Transport The top three areas of concern for hospital leaders are HCAHPS, readmissions and poor patient flow.* Radiology E.D. efficiency is important, but not the sole determinant of good patient flow. Patient flow constraints exist throughout the entire hospital system. Housekeeping Kirk B. Jensen. MD, MBA, FACEP Inpatient Services *The 2012 Patient Flow Challenges Assessment (PFCA) report by AHA Solutions, an American Hospital Association company 15

16 POOR PATIENT FLOW ISSUES Hospitals with patient flow issues demonstrate: A culture allowing physicians and staff to work in silos instead of focusing on a broader picture of patientcentered care. Divergent perspectives and priorities of the emergency medicine and hospital medicine physicians causing inefficiencies, communication breakdowns and slow patient hand-offs. Kirk B. Jensen. MD, MBA, FACEP *The 2012 Patient Flow Challenges Assessment (PFCA) report by AHA Solutions, an American Hospital Association company Inpatients ready for discharge filling hospital beds into the late afternoon, blocking admissions from the emergency department. The average time to move the admitted patient from the emergency department to the inpatient unit was commonly 3½ hours or more (E.D. boarding time). 16

17 FOUNDATION OF PATIENT FLOW IMPROVEMENTS Improving patient flow often takes a complete refocus of the hospital organization on Process Critical bottlenecks Teamwork Hand-offs and Clinical leadership crucial elements that lead to culture change. Kirk B. Jensen. MD, MBA, FACEP Expert facilitation of changes to both processes and culture is a key element in bringing about improved overall efficiency and effectiveness. 17

18 CONTRIBUTIONS TO PATIENT FLOW BY SPECIALTY Significant flow and service efficiencies plus improved clinical outcomes can be achieved through the combined efforts of both services. Emergency Medicine Effective triage Professional, organized communication Lean thinking and patientcentered processes A continuous focus on improving flow and the patient experience Hospital Medicine Patient rounding throughout the day Foresight and planning Observing and understanding a patient s needs Arranging appropriate services and assistance Managing the patient experience and creating a positive care environment Kirk B. Jensen. MD, MBA, FACEP 18
19 HOSPITAL MEDICINE PHYSICIANS - HOSPITALISTS As Quarterbacks Hospital medicine physicians, or hospitalists, direct care for patients requiring hospital inpatient services. The hospitalist can serve as quarterback of the patient care team, teaming up with multiple players: Kirk B. Jensen. MD, MBA, FACEP E.D. physicians and personnel Primary care physicians Specialists Nursing staff Case managers Laboratory staff Radiology personnel Patients Family members Program coordinators Home care agencies Long term acute care hospitals Rehab facilities Nursing homes As many hospitals move to a model of 24- hour laboratory, radiology and other essential services, the advantages of 24-hour hospitalist services will likely become more dramatic. 19
20 HOSPITAL MEDICINE PHYSICIANS - HOSPITALISTS Impact and Advantages The impact of the hospital medicine group on HCAHPS scores is hefty because hospitalists provide the majority of clinical care for admitted patients. Kirk B. Jensen. MD, MBA, FACEP As a hospital-based practice, hospitalists are positioned to effectively manage and facilitate hospital admissions and discharges. Therefore, from a patient flow perspective, hospitalists have come to play major roles in improving flow efficiency, satisfaction and cost (McHugh et al, 2011). 20

21 VALUE-BASED SUCCESS Key Ingredients Uniting E.D. and hospitalist services around shared goals and operations Optimizing patient throughput via system-wide collaboration and integration Focusing on providing quality patient-centered care Kirk B. Jensen. MD, MBA, FACEP 21


22 INTEGRATION Leadership and Culture Change Behind virtually every successful, patient-centered E.D. is great leadership, a culture of service excellence and operational efficiency. Healthcare providers almost invariably support processes that improve patient care. When leadership can manage from a clinically and operationally integrated E.D. and hospitalist model, it can break down problematic silos, collaboratively addressing the availability of inpatient / ICU beds, spikes in arrival, diagnostic turnaround times and more. Kirk B. Jensen. MD, MBA, FACEP After all, helping others is the reason so many nurses and physicians go into healthcare. 22
23 CLINICAL INTEGRATION The Solution Today s focus on efficiency, cost effectiveness and quality has put coordination and collaboration at center stage. Foreword thinking healthcare organizations are realizing that integration of services and care requires a holistic approach. That s why many visionary healthcare organizations are pursuing a strategic path toward operational integration. Ultimately, the solution has been found in an integrated approach to emergency medicine and hospital medicine in order to improve communication, collaboration and performance Kirk B. Jensen. MD, MBA, FACEP 23

24 CLINICAL INTEGRATION Operational and Technical Components Integration includes behaviors, activities and tools to achieve, sustain and accelerate exceptional clinical, operational and financial outcomes. Even with existing integrated groups, turning a historically disjointed system into a well-oiled machine will be facilitated by applying the right tools. Shared operational tools can improve clarity, flow, hand-offs, communication and more. The benefits of integration and alignment include cost reduction, revenue enhancement, CMS-imposed penalty reduction, and increased satisfaction of all parties involved. Shared technology and structural improvements can improve communication and efficiency. Kirk B. Jensen. MD, MBA, FACEP 24


25 CLINICAL INTEGRATION Fast Track to Flow Improvement Integration of the emergency and hospital medicine practices on all levels - clinical, operational, technical, financial, etc. - quickly and profoundly impacts the hospital by: Improving patient flow, Optimizing care and efficiency, Improving the patient experience, and Generating related value. For the hospital, improvements in efficiency, faster bed turns in the E.D., the opportunity for incremental admissions and decreases in patients leaving the E.D. without treatment provides opportunities for new revenue, with synergies that lead to a better bottom line. Kirk B. Jensen. MD, MBA, FACEP 25
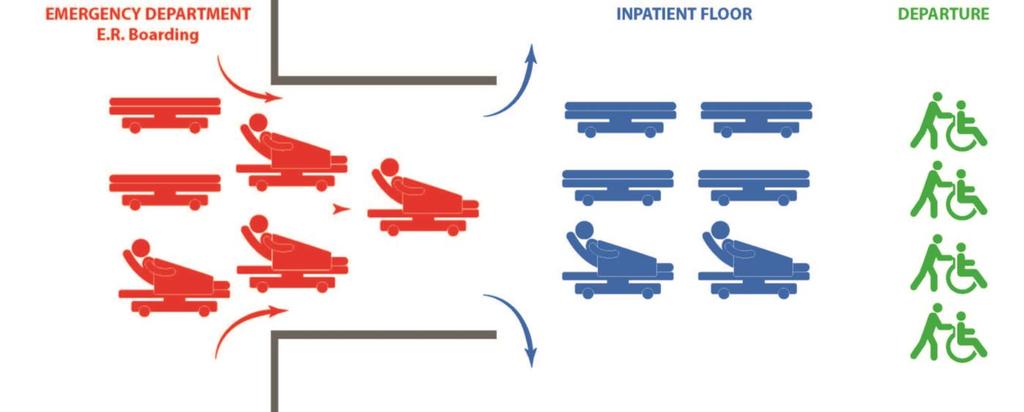
26 DOOR-TO-DISCHARGE: IDEALLY A SEAMLESS NETWORK OF PATIENT CARE, HANDOFFS, AND TRANSITIONS Kirk B. Jensen. MD, MBA, FACEP 26
27 Improving Patient Flow Key Strategies It s one thing to have processes in place that improve efficiency. But, flow is equally thwarted if there are no inpatient beds available when needed. Countless variables impacting bed availability are beyond the control of either the emergency physician or hospitalist. Still, it helps to be aware of initiatives and programs available to a hospital for addressing areas that can be managed. EmCare offers valuable support to the hospital for a number of strategies to improve both patient flow and the patient experience, such as: Accommodating discharge strategy planning within the first 24 hours. Supporting the hospital s 11 a.m. Discharge program or other focus on timely discharge. Starting Off Right Discharge planning typically begins the moment the patient is admitted. Hospitalists who collaborate with case managers can be instrumental in helping to successfully transition the patient to the next stage of appropriate care. Kirk B. Jensen. MD, MBA, FACEP 27

28 Improving Patient Flow Key Strategies Continued Participating in programs such as early rounding on inpatients or rounding with a multidisciplinary team. Assisting with initiatives such as day of discharge conferences or, preferably, next day discharge conferences to identify patients who may be ready to go home. Providing expertise in setting up a discharge lounge. Supporting the use of nurse practitioners and physician assistants in accordance with the hospital s bylaws and state laws. Investigating new concepts in hospital medicine such as ways to overcome inefficient routines, for example, rounding on discharges first and taking more time with sicker patients later as medically prudent. Providing educational programs customized and facilitated by clinical services experts. Designing and implementing an effective hospitalist orientation process (Quinn, 2011). Kirk B. Jensen. MD, MBA, FACEP 28
29 Integration Changes Everything EMCARE S DOOR-TO-DISCHARGE EmCare s Door-to-Discharge integrated hospitalist/ed service (D2D) expedites care by moving patients more efficiently from the ED to treatment to testing and a quicker discharge, leading to: Faster admission Less E.D. boarding time More E.D. capacity Less wait time in the E.D. Less ambulance diversion In addition to patient benefits, the D2D model delivered significant financial benefits to hospitals previously experiencing even minor challenges with LWBS, LPT and LPMSE rates. Hospitals utilizing EmCare s D2D with RAP&GO software experience a nearly 12% improvement in E.D. volume. EmCare processes are designed to drive greater: Kirk B. Jensen. MD, MBA, FACEP Efficiency and cost savings Potential new hospital revenue Positive perception of care Improved quality of care 29

30 Clinical Integration Powering through Software EmCare s proprietary Rapid Admission Process and Gap Orders (RAP&GO ) evidencebased software supports EmCare s D2D service. RAP&GO leverages technology to improve patient flow by organizing, automating and expediting the process of moving the patient from the ED to the floor; in short, hardwiring the LEAN process. RAP&GO helps organize and facilitate communication not only between physicians, but throughout all hospital departments. All entities associated with coordinating a hospital admission and moving patients more rapidly through the admission process benefit from RAP&GO including patients. Kirk B. Jensen. MD, MBA, FACEP 30
31 From the first day I used RAP&GO, I loved it! All the calls back and forth are eliminated. No more Let me call you back, where sometimes 30, 40 or 50 minutes would pass before you heard back. We can now stay ahead on beds as everyone who needs the message gets the message at the same time. ~ Quote from the House Supervisor of a hospital using RAP&GO Kirk B. Jensen. MD, MBA, FACEP 31
32 Integration Changes Everything The Industry Blueprint for Success Integration changes everything: Communication, collaboration, patient flow, patient perception of care and the bottom line. With this insight, EmCare has developed the industry blueprint for success. EmCare s Door-to-Discharge program with RAP&GO evidence-based software tackles the outdated silos and the rigidities of complex and cumbersome systems, and delivers improved quality, safety and service. Door-to-Discharge with RAP&GO : Addresses throughput and efficiency with lean and rapid process redesign Provides leadership to bring all departments together on a patient centered mission Integrates the emergency medicine and hospital medicine physician team Creates efficiencies in length of stay and implements an inpatient early rounding and discharge program Supports the process with software to improve communication, accuracy, confidence and efficiency Supports growth in E.D. volume / performance and the potential for new revenue generated by decreasing boarding time and opening up E.D. beds Kirk B. Jensen. MD, MBA, FACEP 32


33 CONCERNS OF HEALTHCARE LEADERS % expect ED operating margin to decrease 75% identified ED-to-Inpatient BIGGEST bottleneck 9 out of 10 expect ED volumes to increase 40 million newly insured patients from ACA using the ED Local Practice Divisional Support National Resources 33
34 TOP CHALLENGES Most healthcare leaders say that patient flow, wait time and patient boarding are their biggest ED challenges. Wait Time Patient Flow The ED only flows as well as the hospital flows. Patient Boarding Local Practice Divisional Support National Resources 34


35 THE COST IT ADDS UP In 2007, 1.9 million people representing 2% of all 1.9 E.D. million visits left the $1,086 E.D. before being seen. In 2007, 1.9 A 2006 study These walk-outs million people represent found significant that each lost revenue for representing hospitals. 2% hour of of all E.D. visits ambulance diversion was A 2006 study left found the E.D. that each hour of associated with ambulance diversion before being was associated $1,086 in with seen. $1,086 in foregone hospital revenues. foregone These walk-outs hospital A recent study represent showed that a revenues. 1-hour significant lost reduction in E.D. revenue boarding for time would result in over $9,000 hospitals. of additional revenue by reducing ambulance diversion and patients who left without being seen. $9,000 A recent study showed that a 1-hour reduction in E.D. boarding time would result in over $9,000 of additional revenue by reducing ambulance diversion and patients who left without being seen. Source: Ambulance Diversion: Economic and Policy Considerations, 14 July 2006 Robert M. Williams Annals of Emergency Medicine December 2006 Local Practice Divisional Support National Resources (Vol. 48, Issue 6, Pages ) Retrieved from April 29,
36 ILLUSTRATION OF POTENTIAL FINANCIAL BENEFIT TO XYZ HOSPITAL Assumptions: Projected Reduction in LPSME Based Upon Actual D2D Results: 24% (15 facilities with D2D program; year-over-year comparison) Projected Increase in ER Volume Based Upon Actual D2D Results: 10% (15 facilities with D2D program; year-over-year comparison) Projected Increase in Hospitalist Program Encounters Based Upon Actual D2D Results: 5% (15 facilities with D2D program; year-over-year comparison; the admissions increase is driven by increased ER volume - the total admission rate of ER patients under the D2D model is generally unchanged or slightly less than historical admission rate prior to D2D implementation) * Potential New Hospital Revenue is representative of a decrease in LWOT/LPMSE rates and/or improved bed availability which in turn contributes to an increase in E.D. volume. An increase in E.D. volume may result in improved revenue for the hospital through charges for the additional patients in the E.D. Historical data suggests that admission rates under the D2D program remain essentially flat compared to the time period immediately prior to implementation of the D2D program. Thus, thus the additional E.D. volume would result in additional admissions and potential increased revenue for the hospital. 36
37 ILLUSTRATION OF POTENTIAL FINANCIAL BENEFIT TO XYZ HOSPITAL Financial Illustration: Current ED Volume: 40,000 Projected Annual ED Volume Increase from improved flow: 10% Assumption 4,000 Hospital Revenue per ED case x $ 1,000 Total Potential Hospital Revenue from Increased ED Volume: $ 4,000,000 Potential New ED patients per day due to improved flow 11 Potential Additional Annual Admissions From ED Volume Increase Assuming 16.0% Admission Rate 640 Historical Medical Cases Composition Rate Revenue from Medical Cases at $7,500/case 70% 448 $ 3,360,000 Historical Surgical Cases Composition Rate Revenue from Surgical Cases at $15,000/case 20% 128 $ 1,920,000 Historical Cardiac Cases Composition Rate Revenue from Cardiac Cases at $12,000/case 10% 64 $ 768,000 Total Potential Hospital Revenue from Additional Admissions: $ 6,048,000 Potential New Admissions per day due to improved flow 2 Potential Additional Annual Hospital Revenue $ 10,048,000 * Potential New Hospital Revenue is representative of a decrease in LWOT/LPMSE rates and/or improved bed availability which in turn contributes to an increase in E.D. volume. An increase in E.D. volume may result in improved revenue for the hospital through charges for the additional patients in the E.D. Historical data suggests that admission rates under the D2D program remain essentially flat compared to the time period immediately prior to implementation of the D2D program. Thus, thus the additional E.D. volume would result in additional admissions and potential increased revenue for the hospital. 37
38 VALUE-BASED PURCHASING The Hospital Value-Based Purchasing (VBP) Program is a Centers for Medicare & Medicaid Services (CMS) initiative that rewards acute-care hospitals with incentive payments for the quality of care they provide to people. CMS bases hospital performance on an approved set of measures and dimensions, grouped into specific quality domains. 38
39 WEIGHTED VALUE OF EACH DOMAIN, FY Domain FY 2013 Weight FY 2014 Weight FY 2015 Weight Clinical Process of Care 70% 45% 20% Patient Experience of Care 30% 30% 30% Outcome N/A 25% 30% Efficiency N/A N/A 20% Source: Medicare Learning Network. (2013, March). MLN Products ICN March Retrieved from CMS.gov: MLN/MLNProducts/downloads/Hospital_VBPurchasing_Fact_Sheet_ICN pdf 39
 4. Median time ED arrival to ED departure - for admitted patients (FY 2014) 5.")
40 HOSPITAL REPORTING OF ED MEASURES TO CMS 1. Median time ED arrival to ED departure - for discharged patients (CY 2013) 2. Door-to-diagnostic (CY 2013) 3. Left without being seen (CY 2013) 4. Median time ED arrival to ED departure - for admitted patients (FY 2014) 5. Median time admit decision to ED departure - for admitted patients (FY 2014) 40

41 EMERGENCY MEDICINE PHYSICIANS AND HOSPITALISTS YIN AND YANG... ED Physician Acute condition Stabilize and transport Thinks of the big picture Diagnose, treat and discharge Move fast and make critical decisions quickly LOS measured in MINUTES HM Physician Evaluates all the details All conditions and comorbidities Treat, educate and prevent recurrence Has time to explore options with patients and caregivers Methodical decision making LOS measured in DAYS 41

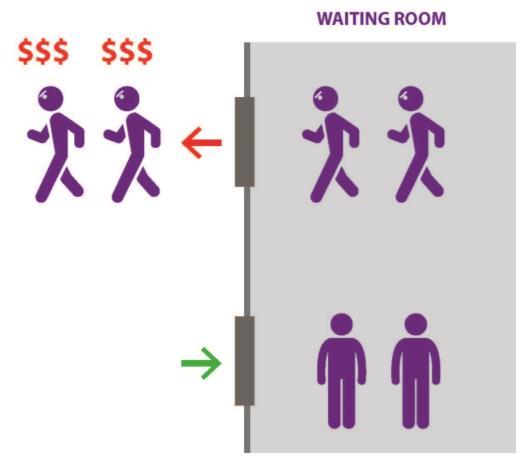



42 BOARDING AND BOTTLENECKS DISCHARGE SMOOTH PATIENT FLOW DISCHARGE 42

43 ALIGNMENT, CLINICAL INTEGRATION, AND TECHNOLOGY Lean Emergency Department Collaboration and Efficient Inpatient Discharge by 11am Efficient Inpatient Admission Services 43

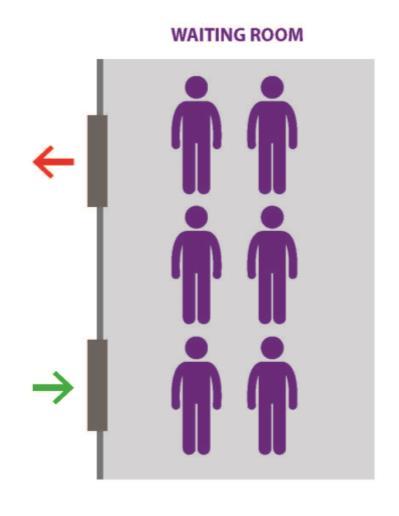
44 Priority Discharge Frees Up Inpatient Capacity 44

45 Technology Facilitates Communication and Process Efficiency Placeholder for Charge Capture screenshot illustrating priority discharge concept

46 Clinical Integration extends into the community
47 RAPID ADMISSION PROCESS RAP&GO (Rapid Admission Process and Gap Orders) software, an internet-based set of orders with predefined protocols, helps expedite patient admits from the emergency department. created by doctors to help hospitals achieve outstanding CMS time measures for patient admission from the ED Link to web demo 47
48









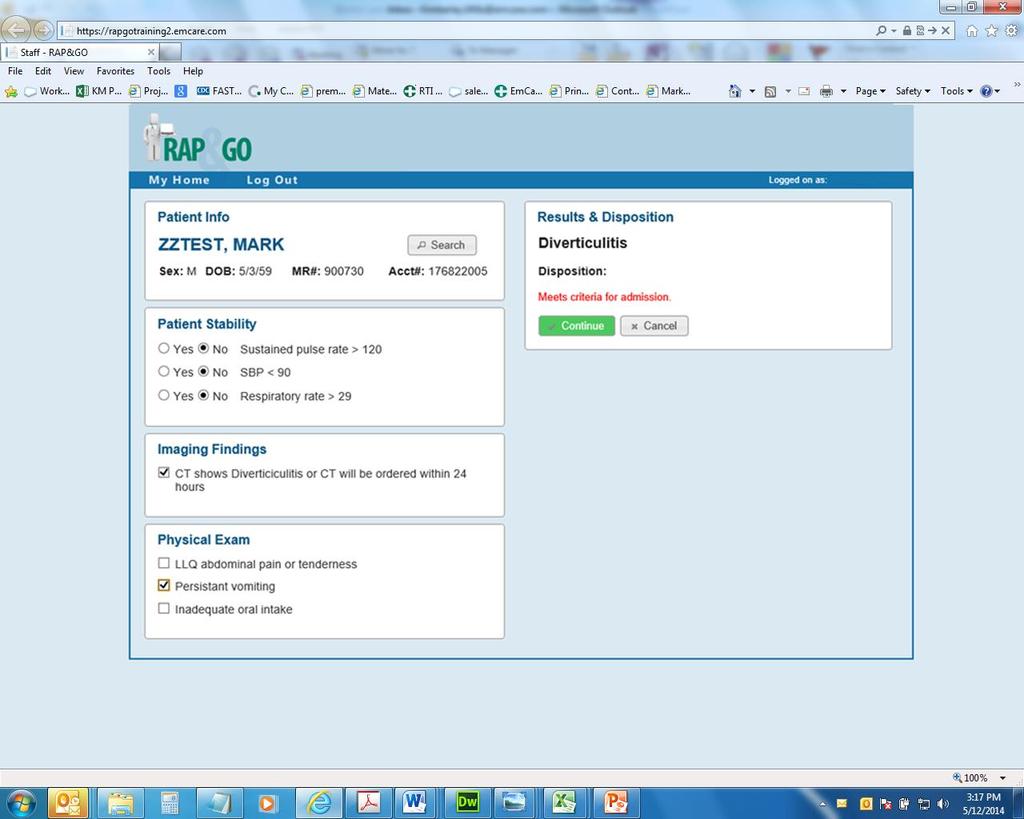
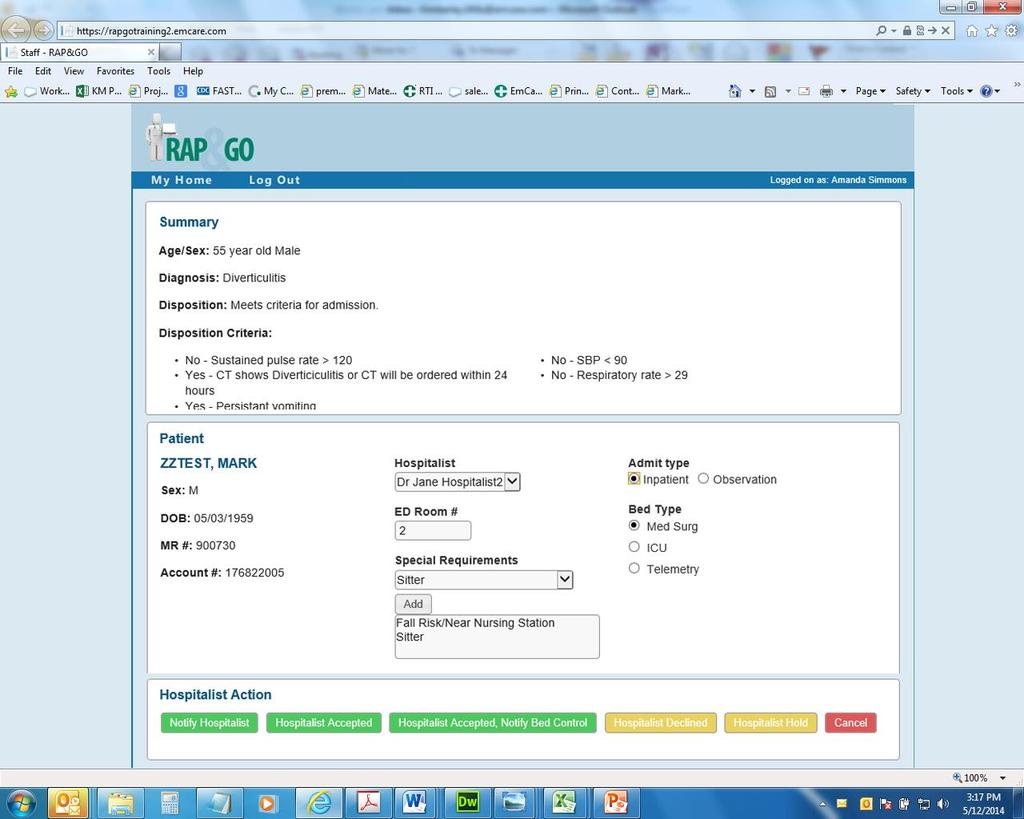
49 STEP ONE: COMPLETE ONLINE FORM BASED ON PATIENT DIAGNOSIS Complete checklist based on patient s condition. Results and Disposition created based on checklist. 49
 generated based on Rapid Admission Process (RAP)")
50 STEP TWO: GENERATE GAP ORDERS (GO) GENERATE GAP ORDERS Gap Orders (GO) generated based on Rapid Admission Process (RAP) 50
51




52 STEP THREE: HAND OVER PATIENT TO HOSPITALIST Gap Orders generated. Print and sign Gap Orders. ED Physician hands over patient to Hospitalist with defined orders and protocols. 52


53 PATIENT IMMEDIATELY MOVED FROM ED TO FLOOR Hospitalist Does Not See Patient In ED 53
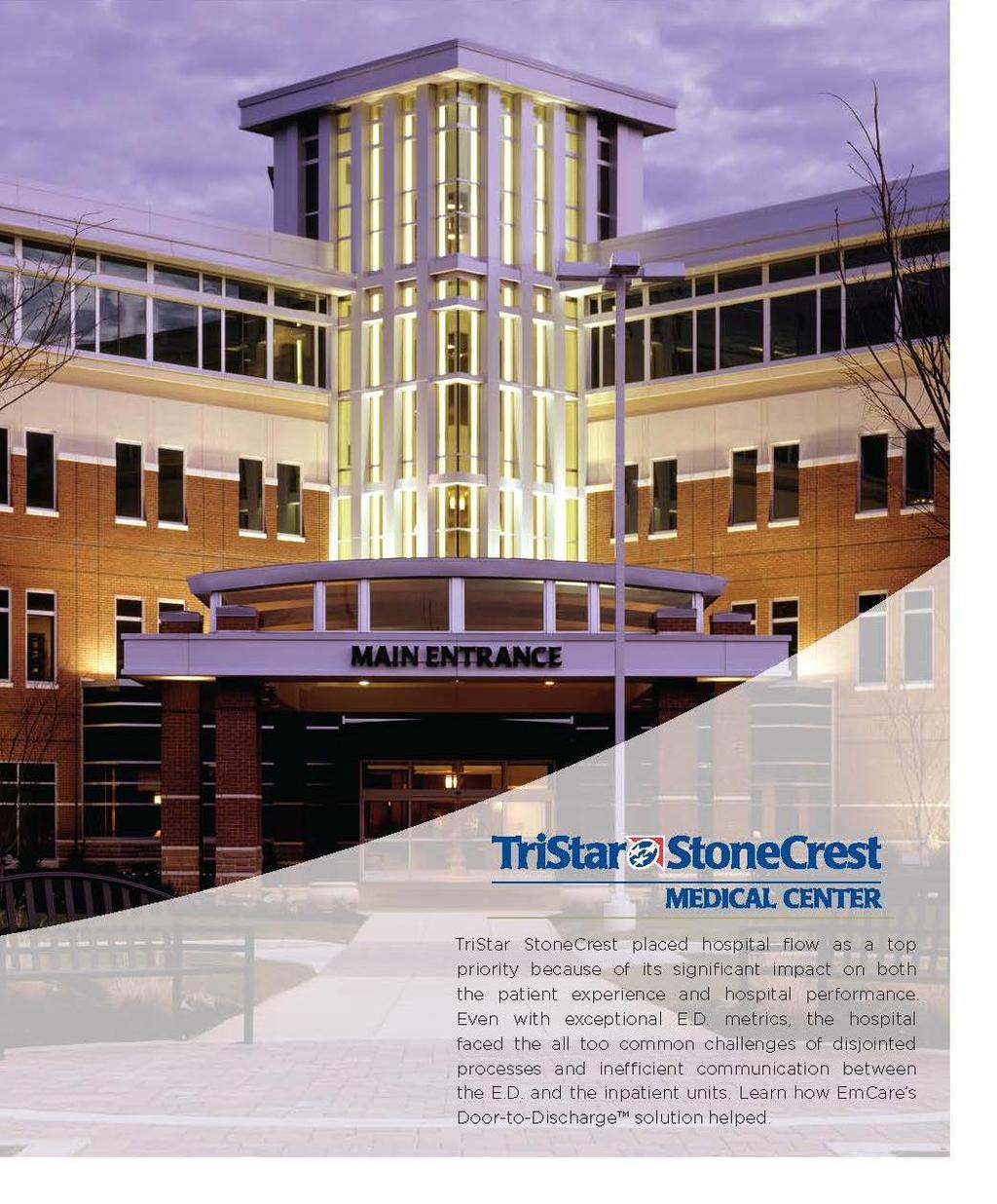

54 TRISTAR STONECREST MEDICAL CENTER
 hours Floor After Rapid Admission Process ED Floor <80")
55 BEFORE AND AFTER WITH RAP&GO Decreased ER boarding time by nearly 2 ⅟2 Before Rapid Admission Process ED >3 ⅟2 Hours (210 minutes) hours Floor After Rapid Admission Process ED Floor <80 Minutes 55
56 Q&A Emcare.com/integratedservices




57 How Integrated Clinical Services and Technology are Making Healthcare Work Better Thank You! Presenters: Kirk Jensen, MD, MBA, FACEP Chief Medical Officer Best Practices, Inc Executive Vice President, EmCare Mark Hamm CEO EmCare Hospital Medicine For more information, call
Perfecting Emergency Department Operations
 These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
DASH Direct Admissions as Easy as 1-2-3
 DASH Direct Admissions as Easy as 1-2-3 SEAMLESS COORDINATION. EASE OF USE. POWERFUL TWO-WAY COMMUNICATION. As pioneers in the delivery of care, EmCare offers simple and practical yet powerful technologies
DASH Direct Admissions as Easy as 1-2-3 SEAMLESS COORDINATION. EASE OF USE. POWERFUL TWO-WAY COMMUNICATION. As pioneers in the delivery of care, EmCare offers simple and practical yet powerful technologies
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
MAKING HEALTHCARE WORK BETTER. Hospital Medicine
 MAKING HEALTHCARE WORK BETTER Hospital Medicine EMCARE 3 CHANGING THE HORIZON OF HEALTHCARE EmCare Hospital Medicine A dependable partner Healthcare reform is changing the way healthcare leaders do business.
MAKING HEALTHCARE WORK BETTER Hospital Medicine EMCARE 3 CHANGING THE HORIZON OF HEALTHCARE EmCare Hospital Medicine A dependable partner Healthcare reform is changing the way healthcare leaders do business.
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation
 Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
The Point of Care Ecosystem Four Benefits of a Fully Connected Outpatient Experience
 Midmark White Paper The Point of Care Ecosystem Four Benefits of a Fully Connected Outpatient Experience Introduction This white paper from Midmark is the first in a series that defines the outpatient
Midmark White Paper The Point of Care Ecosystem Four Benefits of a Fully Connected Outpatient Experience Introduction This white paper from Midmark is the first in a series that defines the outpatient
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Emergency Department Patient Flow Strategies. University of Maryland Medical Center
 Emergency Department Patient Flow Strategies University of Maryland Medical Center Medical Admitting Officer Attending Hospitalist Hours: 9a 11p Mon Friday Goal to partner with ED team and provide oversight
Emergency Department Patient Flow Strategies University of Maryland Medical Center Medical Admitting Officer Attending Hospitalist Hours: 9a 11p Mon Friday Goal to partner with ED team and provide oversight
The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management
 The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management By Jim Hansen, Vice President, Health Policy, Lumeris November 19, 2013 EXECUTIVE SUMMARY When EMR data
The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management By Jim Hansen, Vice President, Health Policy, Lumeris November 19, 2013 EXECUTIVE SUMMARY When EMR data
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
The Patient Experience: Challenges and Opportunities in the Safety Net
 The Patient Experience: Challenges and Opportunities in the Safety Net Leon L. Haley Jr., MD, MHSA, FACEP Executive Associate Dean, Clinical Services Grady Chief Medical Officer, EMCF Associate Professor
The Patient Experience: Challenges and Opportunities in the Safety Net Leon L. Haley Jr., MD, MHSA, FACEP Executive Associate Dean, Clinical Services Grady Chief Medical Officer, EMCF Associate Professor
Chest Pain Accredited. Transplant Program-Heart, Kidney, Liver. Hear Transplant Program serving San Antonio area for 25 years
 PUTTING THE PATIENT FIRST IN PATIENT PLACEMENT 8 Hospital System, 1 Freestanding ED Provide healthcare to 26 surrounding counties within South Texas International Transfer Services Methodist Healthcare
PUTTING THE PATIENT FIRST IN PATIENT PLACEMENT 8 Hospital System, 1 Freestanding ED Provide healthcare to 26 surrounding counties within South Texas International Transfer Services Methodist Healthcare
The Accountable Care Organization Specific Objectives
 Accountable Care Organizations and You E. Christopher h Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences CEO, OSU Faculty Group Practice Chair, Department of Surgery Ohio State
Accountable Care Organizations and You E. Christopher h Ellison, MD, F.A.C.S Senior Associate Vice President for Health Sciences CEO, OSU Faculty Group Practice Chair, Department of Surgery Ohio State
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES
 EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
ENHANCE HEALTHCARE CONSULTING E. COUNTRY CLUB DRIVE, SUITE 2810 AVENTURA, FL
 In today s healthcare environment, anesthesia groups have many issues to deal with, including ACO s, pressure on reimbursement, quality tracking, the surgical home, and pressure on hospital subsidies.
In today s healthcare environment, anesthesia groups have many issues to deal with, including ACO s, pressure on reimbursement, quality tracking, the surgical home, and pressure on hospital subsidies.
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Emergency Department Throughput : The Cambridge Health Alliance Experience
 Emergency Department Throughput : The Cambridge Health Alliance Experience Assaad J. Sayah, MD, FACEP Sr. V.P. & Chief Medical Officer President, CHA Physician Organization IHI 2016 Cambridge Health Alliance
Emergency Department Throughput : The Cambridge Health Alliance Experience Assaad J. Sayah, MD, FACEP Sr. V.P. & Chief Medical Officer President, CHA Physician Organization IHI 2016 Cambridge Health Alliance
How an ACO Provides and Arranges for the Best Patient Care Using Clinical and Operational Analytics
 Success Story How an ACO Provides and Arranges for the Best Patient Care Using Clinical and Operational Analytics HEALTHCARE ORGANIZATION Accountable Care Organization (ACO) TOP RESULTS Clinical and operational
Success Story How an ACO Provides and Arranges for the Best Patient Care Using Clinical and Operational Analytics HEALTHCARE ORGANIZATION Accountable Care Organization (ACO) TOP RESULTS Clinical and operational
Driving Business Value for Healthcare Through Unified Communications
 Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
MERCY MEDICAL CENTER. Mercy Medical Center Improves Patient Care, Lowers Costs with the Hospital Operating System
 MERCY MEDICAL CENTER Mercy Medical Center Improves Patient Care, Lowers Costs with the Hospital Operating System Success Snapshot Reduced acute LOS from 4.6 to 3.74 and observation LOS from 1.51 to 1.31
MERCY MEDICAL CENTER Mercy Medical Center Improves Patient Care, Lowers Costs with the Hospital Operating System Success Snapshot Reduced acute LOS from 4.6 to 3.74 and observation LOS from 1.51 to 1.31
Yo u r Ke y t o Pay -f o r-
 Cha p t e r On e : HCAHPS Co u n t s: Wh y It s Yo u r Ke y t o Pay -f o r- Performance Success A Brief Introduction to HCAHPS If you re a newer leader, you may appreciate this quick overview. HCAHPS stands
Cha p t e r On e : HCAHPS Co u n t s: Wh y It s Yo u r Ke y t o Pay -f o r- Performance Success A Brief Introduction to HCAHPS If you re a newer leader, you may appreciate this quick overview. HCAHPS stands
Health Care Evolution
 Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012
 Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012 Presenters David Sayen, CMS Regional Administrator Betsy L. Thompson,
Updates from CMS: Value-Based Purchasing, ACOs, and Other Initiatives The Seventh National Pay for Performance Summit March 20, 2012 Presenters David Sayen, CMS Regional Administrator Betsy L. Thompson,
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
Measurement Strategy Overview
 Mobile Integrated Healthcare Program 911 Nurse Triage Measurement Strategy Overview Aim A clearly articulated goal statement that describes how much improvement by when and links all the specific outcome
Mobile Integrated Healthcare Program 911 Nurse Triage Measurement Strategy Overview Aim A clearly articulated goal statement that describes how much improvement by when and links all the specific outcome
Health Reform and IRFs
 American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
American Medical Rehabilitation Providers Association 8 th Annual AMRPA Educational Conference New Orleans, LA Health Reform and IRFs Planning Today for Success Tomorrow October 14, 2010 Agenda Introduce
The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care
 Includes Suggestions for Leveraging Improved BP Measurements to Achieve Quality Metrics Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care Introduction This
Includes Suggestions for Leveraging Improved BP Measurements to Achieve Quality Metrics Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care Introduction This
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty
 Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Examining a range of
Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Examining a range of
THE NEW IMPERATIVE: WHY HEALTHCARE ORGANIZATIONS ARE SEEKING TRANSFORMATIONAL CHANGE AND HOW THEY CAN ACHIEVE IT
 Today s challenges are not incremental, but transformational; across the country, many CEOs and executives in healthcare see the need not merely to improve traditional ways of doing business, but to map
Today s challenges are not incremental, but transformational; across the country, many CEOs and executives in healthcare see the need not merely to improve traditional ways of doing business, but to map
Critical Access Hospital Quality
 Critical Access Hospital Quality Current Performance and the Development of Relevant Measures Ira Moscovice, PhD Mayo Professor & Head Division of Health Policy & Management School of Public Health, University
Critical Access Hospital Quality Current Performance and the Development of Relevant Measures Ira Moscovice, PhD Mayo Professor & Head Division of Health Policy & Management School of Public Health, University
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
How Allina Saved $13 Million By Optimizing Length of Stay
 Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Medicare Physician Payment Reform:
 Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Session 92AB Improving Patient Experience and Outcomes Using Real-Time Care Rounding Technology
 Prepared for the Foundation of the American College of Healthcare Executives Session 92AB Improving Patient Experience and Outcomes Using Real-Time Care Rounding Technology Presented by: Sue Murphy Alison
Prepared for the Foundation of the American College of Healthcare Executives Session 92AB Improving Patient Experience and Outcomes Using Real-Time Care Rounding Technology Presented by: Sue Murphy Alison
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
The ins and outs of CDE 10 steps for addressing clinical documentation excellence
 The ins and outs of CDE 10 steps for addressing clinical documentation excellence What s at stake for CDE outpatient/inpatient integration? Historically, provider organizations have focused their clinical
The ins and outs of CDE 10 steps for addressing clinical documentation excellence What s at stake for CDE outpatient/inpatient integration? Historically, provider organizations have focused their clinical
Succeeding with Accountable Care Organizations
 Succeeding with Accountable Care Organizations The Point B Webinar Series October 25, 2011 Today s Discussion Key ACO trends and emerging models Critical success factors for building an ACO Developing
Succeeding with Accountable Care Organizations The Point B Webinar Series October 25, 2011 Today s Discussion Key ACO trends and emerging models Critical success factors for building an ACO Developing
Quality Improvement in the Advent of Population Health Management WHITE PAPER
 Quality Improvement in the Advent of Population Health Management WHITE PAPER For healthcare organizations whose reimbursement and revenue are tied to patient outcomes, achieving performance on quality
Quality Improvement in the Advent of Population Health Management WHITE PAPER For healthcare organizations whose reimbursement and revenue are tied to patient outcomes, achieving performance on quality
The influx of newly insured Californians through
 January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
January 2016 Managing Cost of Care: Lessons from Successful Organizations Issue Brief The influx of newly insured Californians through the public exchange and Medicaid expansion has renewed efforts by
Overview of Alaska s Hospitals and Nursing Homes. House HSS Committee March 1, 2012
 Overview of Alaska s Hospitals and Nursing Homes House HSS Committee March 1, 2012 Alaska Hospital and Nursing Homes Testifying Today Fairbanks Memorial Hospital Mike Powers Central Peninsula Hospital
Overview of Alaska s Hospitals and Nursing Homes House HSS Committee March 1, 2012 Alaska Hospital and Nursing Homes Testifying Today Fairbanks Memorial Hospital Mike Powers Central Peninsula Hospital
BUILDING THE PATIENT-CENTERED HOSPITAL HOME
 WHITE PAPER BUILDING THE PATIENT-CENTERED HOSPITAL HOME A New Model for Improving Hospital Care Authors Sonya Pease, MD Chief Medical Officer TeamHealth Anesthesia Kurt Ehlert, MD National Director, Orthopaedics
WHITE PAPER BUILDING THE PATIENT-CENTERED HOSPITAL HOME A New Model for Improving Hospital Care Authors Sonya Pease, MD Chief Medical Officer TeamHealth Anesthesia Kurt Ehlert, MD National Director, Orthopaedics
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC
 Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC Objectives Identify measures to facilitate Emergency Department throughput for non-emergent
Overutilization and Routine Non-emergent Use of the Emergency Departments. PUNEET FREIBOTT, DNP, RN,CCRN-K, NEA-BC Objectives Identify measures to facilitate Emergency Department throughput for non-emergent
Introduction. Staffing to demand increases bottom line revenue for the facility through increased volume and throughput and elimination of waste.
 Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
3/19/2013. Medicare Spending Per Beneficiary: The New Link Between Acute and Post Acute Providers
 The New Link Between Acute and Post Acute Providers Carol Quiring, RN President and CEO, Home Care and Hospice Saint Luke s Health System Shauna Thompson, RHIT Senior Director, Quality & Patient Safety
The New Link Between Acute and Post Acute Providers Carol Quiring, RN President and CEO, Home Care and Hospice Saint Luke s Health System Shauna Thompson, RHIT Senior Director, Quality & Patient Safety
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives"
 2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
Publication Year: 2013
 THE INITIAL ASSESSMENT PROCESS ST. JOSEPH'S HEALTHCARE HAMILTON Publication Year: 2013 Summary: The Initial Assessment Process (IAP) was developed collaboratively by the emergency physicians, nursing,
THE INITIAL ASSESSMENT PROCESS ST. JOSEPH'S HEALTHCARE HAMILTON Publication Year: 2013 Summary: The Initial Assessment Process (IAP) was developed collaboratively by the emergency physicians, nursing,
Assessing and Optimizing Operations and Patient Flow in VHA Facilities
 Assessing and Optimizing Operations and Patient Flow in VHA Facilities A six-month professional development program for VHA leaders and staff PROFESSIONAL DEVELOPMENT PROGRAM Assessing and Optimizing Operations
Assessing and Optimizing Operations and Patient Flow in VHA Facilities A six-month professional development program for VHA leaders and staff PROFESSIONAL DEVELOPMENT PROGRAM Assessing and Optimizing Operations
Toward the Electronic Patient Record:
 June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
Improving Patient Satisfaction with Minitab
 Improving Patient Satisfaction with Minitab Christopher Spranger, MBA, ASQ MBB Preview Changing healthcare environment Patient satisfaction process Defining our opportunity Establishing a baseline Finding
Improving Patient Satisfaction with Minitab Christopher Spranger, MBA, ASQ MBB Preview Changing healthcare environment Patient satisfaction process Defining our opportunity Establishing a baseline Finding
MACRA for Critical Access Hospitals. Tuesday, July 26, 2016 Webinar
 MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
Midmark White Paper Building Your Connected Point of Care Ecosystem. Point Of Care Ecosystem Series Part Four
 Midmark White Paper Introduction Before embarking on any construction project, it is always a good idea to have a set of blueprints or a detailed plan to guide progress and ensure alignment with objectives.
Midmark White Paper Introduction Before embarking on any construction project, it is always a good idea to have a set of blueprints or a detailed plan to guide progress and ensure alignment with objectives.
Low Acuity Emergency Department Visits. Joanna Cohen, MD June 2018
 Low Acuity Emergency Department Visits Joanna Cohen, MD June 2018 Goals and Objectives Identify and quantify low acuity ED visits Analyze challenges associated with low acuity ED visits Assess the impact
Low Acuity Emergency Department Visits Joanna Cohen, MD June 2018 Goals and Objectives Identify and quantify low acuity ED visits Analyze challenges associated with low acuity ED visits Assess the impact
 As healthcare moves toward value-based care and risk-sharing payment models, many hospitals are taking a new look at ambulatory surgery centers (ASCs) as a transformational outpatient strategy with potential
As healthcare moves toward value-based care and risk-sharing payment models, many hospitals are taking a new look at ambulatory surgery centers (ASCs) as a transformational outpatient strategy with potential
"Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital
 "Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital The University of Kansas Hospital Leading the Nation in Caring, Healing,
"Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital The University of Kansas Hospital Leading the Nation in Caring, Healing,
Future Proofing Healthcare: Who Knows?
 Future Proofing Healthcare: Who Knows? Marcel Loh Chief Executive, Swedish Suburban Hospitals & Affiliates Swedish Health Services 2 3 4 Things do not happen. Things are made to happen. John F. Kennedy
Future Proofing Healthcare: Who Knows? Marcel Loh Chief Executive, Swedish Suburban Hospitals & Affiliates Swedish Health Services 2 3 4 Things do not happen. Things are made to happen. John F. Kennedy
Emergency Department Strategic Design Considerations
 Emergency Department Strategic Design Considerations James Augustine, MD Director of Clinical Operations, EMP Associate Clinical Professor, Wright State University Department of Emergency Medicine. ED
Emergency Department Strategic Design Considerations James Augustine, MD Director of Clinical Operations, EMP Associate Clinical Professor, Wright State University Department of Emergency Medicine. ED
Executive Summary. Leadership Toolkit for Redefining the H: Engaging Trustees and Communities
 Executive Summary Leadership Toolkit for Redefining the H: Engaging Trustees and Communities Report produced by the AHA Committee on Research and Committee on Performance Improvement 2015 Executive Summary
Executive Summary Leadership Toolkit for Redefining the H: Engaging Trustees and Communities Report produced by the AHA Committee on Research and Committee on Performance Improvement 2015 Executive Summary
Services. Progress to date. Comments. Goal. Hours ED patients to our medicall. Maintainn. this year. excluding the. (consolidated) expense,
 expense,") Progress Report for 201/ /14 Quality ment Plan: Grey Bruce Health Services Priority Indicator ED Wait times: 90th percentile ED length of stay for Admitted patients. Hours ED patients Q4 2011/12 Q / /1
Progress Report for 201/ /14 Quality ment Plan: Grey Bruce Health Services Priority Indicator ED Wait times: 90th percentile ED length of stay for Admitted patients. Hours ED patients Q4 2011/12 Q / /1
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care
 Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Children s Hospital of Eastern Ontario
 Children s Hospital of Eastern Ontario April 1, 2011 Children s Hospital of Eastern Ontario 1 Part A: Overview of Our Hospital s Quality Improvement Plan 1. Overview of our quality improvement plan for
Children s Hospital of Eastern Ontario April 1, 2011 Children s Hospital of Eastern Ontario 1 Part A: Overview of Our Hospital s Quality Improvement Plan 1. Overview of our quality improvement plan for
APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS
 APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS Igor Georgievskiy Alcorn State University Department of Advanced Technologies phone: 601-877-6482, fax:
APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS Igor Georgievskiy Alcorn State University Department of Advanced Technologies phone: 601-877-6482, fax:
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL
 Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Advancing Accountability for Improving HCAHPS at Ingalls
 iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
Readmission Reduction and the ACO
 Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT
 April 13, 2018 The Misadventures of the Recently-Discharged Older Adult THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT Robert E. Burke MD, MS April 13, 2018 I have no conflicts of interest to
April 13, 2018 The Misadventures of the Recently-Discharged Older Adult THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT Robert E. Burke MD, MS April 13, 2018 I have no conflicts of interest to
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Alternative Managed Care Reimbursement Models
 Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
Emerging Strategies for Improving Hospital Medicine
 Emerging Strategies for Improving Hospital Medicine Improving efficiency, patient safety, metrics and satisfaction Improving communication among the patient s community of caregivers Your Presenters Francisco
Emerging Strategies for Improving Hospital Medicine Improving efficiency, patient safety, metrics and satisfaction Improving communication among the patient s community of caregivers Your Presenters Francisco
ED crowding: Causes, Consequences, Solutions
 ED crowding: Causes, Consequences, Solutions Jesse M. Pines, MD, MBA, MSCE Associate Professor of Emergency Medicine and Health Policy George Washington University Urgent Matters Webinar April 23, 2010
ED crowding: Causes, Consequences, Solutions Jesse M. Pines, MD, MBA, MSCE Associate Professor of Emergency Medicine and Health Policy George Washington University Urgent Matters Webinar April 23, 2010
THE ADVANCING ROLE OF ADVANCED PRACTICE CLINICIANS: COMPENSATION, DEVELOPMENT, & LEADERSHIP TRENDS
 THE ADVANCING ROLE OF ADVANCED PRACTICE CLINICIANS: COMPENSATION, DEVELOPMENT, & LEADERSHIP TRENDS INTRODUCTION The demand for Advanced Practice Clinicians (APCs) or Advanced Practice Providers (APPs)
THE ADVANCING ROLE OF ADVANCED PRACTICE CLINICIANS: COMPENSATION, DEVELOPMENT, & LEADERSHIP TRENDS INTRODUCTION The demand for Advanced Practice Clinicians (APCs) or Advanced Practice Providers (APPs)
Global Budget Revenue. October 8, 2015
 Global Budget Revenue October 8, 2015 Goals Understand GBR s connection to the goals of Maryland s Demonstration Understand impact on budgeting and planning for RFP and future phases Answer questions that
Global Budget Revenue October 8, 2015 Goals Understand GBR s connection to the goals of Maryland s Demonstration Understand impact on budgeting and planning for RFP and future phases Answer questions that
Future of Patient Safety and Healthcare Quality
 Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
2017 Edition. MIPS Guide. The rule is in and Medicare physician payments are changing. What does that mean for you?
 2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
Clinical Operations. Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012
 Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
University of Iowa Health Care
 University of Iowa Health Care Presentation to The Board of Regents, State of Iowa April 11-12, 2018 1 Agenda Today s Presentation Opening Remarks Operating and Financial Performance Preliminary FY19 Operating
University of Iowa Health Care Presentation to The Board of Regents, State of Iowa April 11-12, 2018 1 Agenda Today s Presentation Opening Remarks Operating and Financial Performance Preliminary FY19 Operating
Banner Health Friday, February 20, 2015
 Banner Health Friday, February 20, 2015 Leveraging the Power of Clinical and Business Intelligence: A Primer Presented by: Dr. Maxine Rand, DNP, RN-BC, CPHIMS, Director, Clinical Education, Practice and
Banner Health Friday, February 20, 2015 Leveraging the Power of Clinical and Business Intelligence: A Primer Presented by: Dr. Maxine Rand, DNP, RN-BC, CPHIMS, Director, Clinical Education, Practice and
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
AirStrip ONE Cardiology
 AirStrip ONE Cardiology A Synchronized View of the Vital Patient Data Needed to Improve Care Heart disease is the leading cause of death in the U.S. The associated costs exceed $100 billion annually. AirStrip
AirStrip ONE Cardiology A Synchronized View of the Vital Patient Data Needed to Improve Care Heart disease is the leading cause of death in the U.S. The associated costs exceed $100 billion annually. AirStrip
New York State s Ambitious DSRIP Program
 New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
H ospital Voice. Oregon Community Hospitals. Lean Methods and Mindsets. The CEO Perspective. Taking Aim at Health Care Reform
 H ospital Voice A magazine for and about Oregon Community Hospitals A magazine for and about Oregon Community Hospitals Taking Aim at Health Care Reform Triple Aim to change health care for good The CEO
H ospital Voice A magazine for and about Oregon Community Hospitals A magazine for and about Oregon Community Hospitals Taking Aim at Health Care Reform Triple Aim to change health care for good The CEO
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Case managers are consummate team players, working with. IssueBrief
 IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Medicare Beneficiary Quality Improvement Program (MBQIP) Stephen Njenga, Director of Performance Measurement Compliance March 2018
 Stephen Njenga, Director of Performance Measurement Compliance March 2018") Medicare Beneficiary Quality Improvement Program (MBQIP) Stephen Njenga, Director of Performance Measurement Compliance March 2018 Housekeeping Handouts Location of restrooms Instead of reimbursing for
Medicare Beneficiary Quality Improvement Program (MBQIP) Stephen Njenga, Director of Performance Measurement Compliance March 2018 Housekeeping Handouts Location of restrooms Instead of reimbursing for
Three Steps to Streamline Laboratory Operations:
 Three Steps to Streamline Laboratory Operations: A GUIDE FOR IMPROVING PERFORMANCE AND QUALITY By Richard Walker, MBA, MLS (ASCP), and Kelly Straub, M.S., Huron Healthcare The evolving healthcare environment
Three Steps to Streamline Laboratory Operations: A GUIDE FOR IMPROVING PERFORMANCE AND QUALITY By Richard Walker, MBA, MLS (ASCP), and Kelly Straub, M.S., Huron Healthcare The evolving healthcare environment