ERRORS IN RADIOLOGY: WHY DO WE MAKE THEM AND HOW CAN THEY BE REDUCED?
|
|
|
- Ashlynn Booker
- 5 years ago
- Views:
Transcription

1 ERRORS IN RADIOLOGY: WHY DO WE MAKE THEM AND HOW CAN THEY BE REDUCED? ANIA Z. KIELAR MD, FRCPC DIRECTOR OF ABDOMINAL AND PELVIC IMAGING, THE OTTAWA HOSPITAL Affiliated with Affilié à
2 DISCLOSURE The author has nothing to disclose Affiliated with Affilié à 2
3 OUTLINE At the conclusion of this session, participants should be able to: 1. Demonstrate an understanding of types of errors which can occur in an imaging department 2. Recognize situations in the radiology work environment which can predispose to increased risk of errors 3. Apply knowledge from this presentation to implement changes in the department to increase standardization and safety of patient imaging care Affiliated with Affilié à 3
4 OUTLINE Review of typical errors Active vs latent Sources of errors Situations in the radiology work environment which can predispose to increased risk of errors Examples of errors Systems available to identify errors, modify process and reduce risks Utility of standardization for safety of patient imaging care Affiliated with Affilié à 4
5 ERRORS Accuracy of radiology reports is critical in making appropriate patient care decisions Identify active and latent sources of error in a work place to devise plans to minimize their impact Institute of Medicine reported that 90% of medical errors result from systemic problems rather than individual factors Kohn LT, Corrigan JM, Donaldson MS, eds. To err is human: building a safer health system. Washington, DC: National Academy Press, 2000 Affiliated with Affilié à 5
6 ACTIVE AND LATENT ERRORS Processes may be referred to as having sharp and blunt ends Active = sharp end of sclapel: usually person-related Failure of execution of a task Slip/lapse Knowledge-based Inadequate planning Behavior related failure: Intentional or motivational problems Affiliated with Affilié à 6
7 LATENT ERROR Systems failure Blunt end parts of the process farther away from the action itself Regulators, accreditors, administrators, and designers function at the blunt end Equipment design flaws (e.g. interface not intuitive) Organizational flaws, such as staffing decisions that can increase the likelihood of error Affiliated with Affilié à 7
8 ERRORS Swiss Cheese model Acknowledges that humans make mistakes Focuses on identification of an underlying system failure Safeguards, defenses, and barriers must be implemented to prevent an error Affiliated with Affilié à 8
9 BACKGROUND OF ERRORS: Increasing focus in radiology literature on latent errors Patient experience from time of request to time physician acts on radiology finding, is the result of many individual steps It is everyone s responsibility to close up these latent holes Lee CS et al. AJR 2013;201(3) Reason,J Human Error: models and management. BMJ. 2000;320(7237) Affiliated with Affilié à



10 CORRECTING LATENT ERRORS Routines can then be analyzed, potential problems identified, and amendments made if necessary, in order to prevent future errors, incidents Airline industry uses this area to focus on most often Affiliated with Affilié à 10
11 OPTIMAL PATIENT CARE Need for continuous efforts to improve quality, safety and reduce errors in health care Balanced with efficiency and appropriateness Quality assurance goals: Patient safety Improving efficiency Lowering cost Improving patient outcomes Affiliated with Affilié à 11
12 DIVISION DIRECTOR Part of the job is quality assurance Identify errors, categorize active errors Work to identify underlying latent errors Make changes to reduce active & latent errors Affiliated with Affilié à 12
13 ACTIVE ERRORS Renfrew DL, et al. Error in radiology: classification and lessons in 182 cases presented at a problem case conference. Radiology 1992;183(1): Previously, emphasis on active/ human errors including: FN SOS FP Cognitive: complacency, faulty reasoning, lack of knowledge etc. Other Little emphasis on system related factors that could contribute to these errors


14 SAMPLE QUIP
15 TYPES OF ERRORS MADE BY YEAR IN DIVISION OF ABDOMINAL RADIOLOGY: FN AND SOSSOS QUIP SOS Ordering Issue Cognitive Error False positive False Negative
16 WHAT DID WE DO ABOUT THIS? QUIP (Quality initiative project) So that the individual learns of their error in a non punitive fashion Standardized template reports Case of the week (showing an anonymized error, and a pearl to reduce this in the future) So that everyone can learn from our errors Affiliated with Affilié à 16
17 CASE OF THE WEEK 72-year-old female Rectal cancer post surgery and chemotherapy &radiation. Fluctuation in CEA levels. Assess for disease status.

18 WHERE IS THE ERROR? THIS WAS REPORTED AS POSSIBLE RECURRENCE WITH SOFT TISSUE IN THE PRESACRAL SAPCE June 4, 2014

19 WHERE IS THE ERROR? THIS WAS REPORTED AS POSSIBLE RECURRENCE WITH SOFT TISSUE IN THE PRESACRAL SAPCE June 4, 2014
20 Where is the error? This was reported as possible recurrence with soft tissue in the presacral space June 4, 2014

21 FOLLOW UP MRI July 22, 2014

22 WHERE WAS THE ERROR? July 22, 2014

23 WHERE WAS THE ERROR? July 22, 2014

24 WHERE IS THE ERROR? July 22, 2014

25 DISCUSSION Specific Error: The structure being measured was actually the uterus Type of Error: Perceptual False Positive Organ Involved: Uterus Pearl to Avoid this Error: Sagittal reformats seem to help a lot In this case, sagittal images helpful to prevent false positive findings (normal uterus present there b/c rectum has been removed and the uterus is filling the potential space)

26

27

28 CORONAL REFORMATS HELP.
29 ERROR CLASSIFICATION 1. Perceptual: False-positive: An abnormality is described which is not real Renfrew DL, et al Radiology 1992;183: Pescariani L, Inches, Radio Med 2006;111:252


30 FALSE POSITIVE ERROR
31 ERROR CLASSIFICATION 1. Perceptual: False-negative : An abnormality is present but is not described Satisfaction-of-search: - One abnormality is described but a 2nd abnormality is not reported (form of false-negative study) QUIP SOS Ordering Issue Cognitive Error False Negative

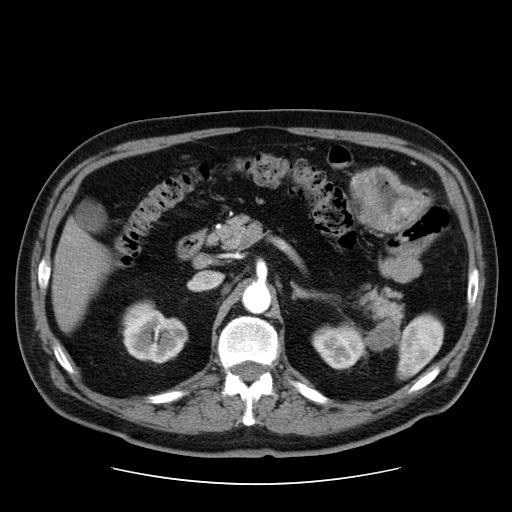
32 SATISFACTION-OF-SEARCH ERROR 64 year old man with prostate cancer CECT of abdomen demonstrated retroperitoneal lymph nodes (arrow) Base of lungs were included and in retrospect there were filling defects in the pulmonary arteries which were not described A CT using PE protocol was performed same day due to sudden increasing chest pain and shortness of breath. It demonstrated bilateral pulmonary emboli (arrows)
33 ANOTHER SOS History: Abdominal pain 33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55

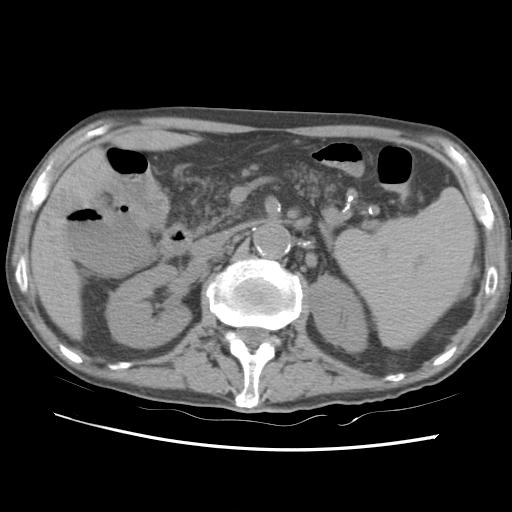
56 SOS ERROR Missed metastasis to tail of pancreas No history of melanoma provided. 56
57 ERROR CLASSIFICATION 2. Cognitive: An abnormality is identified but the wrong diagnosis is made (e.g. Epiploic appendagitis vs. diverticulitis) Lee CS, et al AJR.2013;201(3):611-7
58 CASE INTERPRETED AS SLUGE IN GB

59 Emphysematous cholecystitis
60 ERROR CLASSIFICATION (CONT ) 3. Communication: Report is misinterpretable due to spelling, grammar or transcription errors - Ania says Calcification. Computer says ossification, concretions etc Right/left - Ania says Vascetomy. Computer says mastectomy



61 LATENT FACTORS CONTRIBUTING TO ERRORS IN RADIOLOGY Environmental Temperature Lighting Ergonomics

62 LATENT FACTORS CONTRIBUTING TO ERRORS IN RADIOLOGY Interruptions Pages On the fly consults Lectures, meetings s and smart phones? Balint BJ et al. Do telephone call interruptions have an impact on radiology resident diagnostic accuracy? Acad Radiol Dec;21(12):
63 LATENT FACTORS CONTRIBUTING TO ERRORS IN RADIOLOGY Work volume Too high??? Studies have shown that most abnormal findings on plain radiographs are found during the first few seconds of searching the image, with the number of true-positive findings decreasing abruptly after a short time Early morning Last case Brady A et al. Discrepancy and Error in Radiology: Concepts, Causes and Consequences. Ulster Med J Jan; 81(1):
64 LATENT FACTORS CONTRIBUTING TO ERRORS IN RADIOLOGY Complicated cases Many images and sequences to review (hard if you get interrupted) Lack of provided history - Abdominal CT quality assurance review at TOH - 52/350 (15.1%) of cases were missing information that may have potentially impacted either the imaging protocol chosen or the final diagnosis 64
65 Wrong imaging requested History provided important!! Many imaging modalities available Many protocols to choose from 65



66 LATENT FACTORS CONTRIBUTING TO ERRORS IN RADIOLOGY Imaging Quality Motion artifact Lack of iv/oral contrast Previous not available on PACS 66
67 STEPS TO REDUCE ERRORS Identify if there is latent source Standardization Lifelong learning Affiliated with Affilié à 67


68 M&M ROUNDS Means of reviewing errors and adverse events in an environment that Facilitates learning Encourages accountability Promotes leadership Promotes academic development.
69 QUALITY ASSURANCE A comprehensive goal to ensure excellent standards by collecting and evaluating data in a systematic fashion Performance indicators: Metrics Safety, process/procedure, professional satisfaction, patient outcomes QA helps guide decisions about clinical practice and operational management Affiliated with Affilié à 69
70 YOU HAVE IDENTIFIED AN ERROR: NOW WHAT? One time thing or not? Communicate error in non-punitive fashion Peer education/ Peer review / QUIP Quality assurance PQI Affiliated with Affilié à 70
71 YOU HAVE IDENTIFIED A RECURRENT ERROR: NOW WHAT? PDSA Lean management Kaizen Root cause analysis Six Sigma Affiliated with Affilié à 71

72 PDSA CYCLE Trail and learning approach Hypothesis -> test on small scale before making large scale changes System flowchart Observations to determine problems Action implemented to improve the process Affiliated with Affilié à 72
73 CAN BE DONE FOR ALMOST ANY TOPIC! Can be simple Can be small scale Affiliated with Affilié à 73
74 PARACENTESIS PRACTICE ASSESSMENT Assessed use of pre-procedural pause, consent, time to complete paracentesis Medical student filled out standard form related to paracentesis observations Initial results (33 cases) analyzed 5 weeks into observations Each radiologists received of their own results and group means/ ranges Educational Powerpoint presented at divisional meeting Repeat observation for another 6 weeks (27 cases) Affiliated with Affilié à 74
 54% (n=14) 0.02* Outlined risk of infec3on 82% (n=27) 100% (n=26) 0.022* Outlined risk of bleeding 91% (n=30) 100% (n=26) 0.")
 77% (n=20) 0.0078* Gave pa3ent the opportunity to ask ques3ons 73% (n=24) 100% (n=26) 0.")
75 PRACTICE ASSESSMENT RESULTS: TIME 16 -> 13 MIN Areas of Interest Frequency Before Interven3on (n) Frequency A6er Interven3on (n) Significance (P- value) Outlined risk of damage to nearby structures 24% (n=8) 54% (n=14) 0.02* Outlined risk of infec3on 82% (n=27) 100% (n=26) 0.022* Outlined risk of bleeding 91% (n=30) 100% (n=26) 0.11 Inquired about padent allergies 36% (n=12) 54% (n=14) 0.18 Inquired about pa3ent use of blood thinners 67% (n=22) 88% (n=23) 0.051* Inquired about pa3ent bloodwork 42% (n=14) 77% (n=20) * Gave pa3ent the opportunity to ask ques3ons 73% (n=24) 100% (n=26) * Performed pre- procedural pause 22% (n=6) 85% (n=22) 3.91E- 07 * Affiliated with Affilié à 75
76 LEAN AND KAIZEN MODELS These tools include the human element to traditional PDSA cycles to reduce waste, improve efficiency and implement positive change Takes into account importance of human relations and workplace culture as a key component required for sustained change Culture Kaizen = "change for better" Affiliated with Affilié à 76


77 SIX SIGMA More complex analysis Set of techniques and tools for process improvement Goal: to improve quality of a process by identifying and removing the causes of defects and minimizing variability in processes Uses empirical & statistical methods A six sigma process is one in which % of all opportunities to produce some part are statistically expected to be free of defects (3.4 defective features per million opportunities) Affiliated with Affilié à 77
 Affiliated with Affilié à")
78 DMAIC (acronym for Define, Measure, Analyze, Improve and Control) Affiliated with Affilié à 78
79 ROOT CAUSE ANALYSIS Perform promptly after event Applies to errors, sentinel events or near misses Retrospective process 4-10 people with various roles Fishbone (cause and effect) diagram Affiliated with Affilié à 79
80 ROOT CAUSE ANALYSIS Affiliated with Affilié à 80
81 ROOT CAUSE ANALYSIS Determine both human factors and systems associated with the sentinel event Analyze the underlying systems and process though a series of why questions to determine where risk occurred in an attempt to redesign a system Identify risk points and their contributions towards an adverse event Determine improvement process that may lead to future reduction in likelihood for future similar events Affiliated with Affilié à 81
82 ROOT CAUSE ANALYSIS Who/What/When/Where/How? Should be a no blame discussion What factors were responsible rather than Who is responsible? Confidentially of the reporting within the RCA process Code of silence develops otherwise Affiliated with Affilié à 82
83 WHAT I HAVE LEARNED? A lot more to learn about these techniques. Don t make mountains out of molehills If something goes wrong. Once. Do we really need new policies and procedures for everything? Depends on how serious the error was However, people involved need to know about it and have an opportunity to learn Small steps until you can take bigger steps A work in progress Affiliated with Affilié à 83
84 WHAT WE HAVE IMPLEMENTED IN PAST FEW YEARS Common reporting rooms (abdomen, chest, MSK, neuro etc) Can discuss unusual cases and help each other Increased accountability Easier for technologists and clinicians to find help Standardized template reporting Radiology-specific M&M rounds Evidence-based reporting standards BIRADS, LIRADS, PIRADS, TIRADS etc Affiliated with Affilié à 84

85 STANDARDIZED REPORTS Reduces risks of satisfaction-of-search errors Complex cases (pancreatic tumor staging) Learners ensure they look at all structures Looks professional Faster for specialists to look up area they are interested in Faster for radiologists to perform comparisons? Affiliated with Affilié à 85
86 CONCLUSIONS There are many possible active and latent factors contributing to errors in radiology Identify them Communicate them in non-punitive fashion If repeated errors, use tools to study them and develop systems/ processes to help reduce the holes in your Swiss cheese Life long learning Affiliated with Affilié à 86
87 REFERENCES 1. Kelly A, Cronin P. Practical approaches to quality improvement for radiologists. Radiographics 2015;35(6): Adrian Brady, Risteárd Ó Laoide, Peter McCarthy, and Ronan McDermott Discrepancy and Error in Radiology: Concepts, Causes and Consequences. Ulster Med J Jan; 81(1): Cindy S. Lee1, Paul G. Nagy1, Sallie J. Weaver1 and David E. Newman-Toker1 Cognitive and System Factors Contributing to Diagnostic Errors in Radiology. AJR September 2013, Volume 201, Number 3 4. Vries, E. N. de, Prins, H. A., Crolla, R., & den Outer, A. J. (n.d.). Effect of a Comprehensive Surgical Safety System on Patient Outcomes NEJM. Retrieved January 19, 2016, from NEJMsa Nundy, S., Mukherjee, A., Sexton, B. J., Pronovost, P. J., Knight, A., Rowen, L. C., Makary, M. A. (n.d.). Impact of Preoperative Briefings on Operating Room Delays. Retrieved January 19, 2016, from file:///c:/users/etienne/ Downloads/soa80003_1068_1072.pdf Affiliated with Affilié à 87
Getting to Zero: A Quality Assessment of Multiple Interventions Aimed to Reduce Cancellation Rates in an Ultrasound-Guided Biopsy Program
 Getting to Zero: A Quality Assessment of Multiple Interventions Aimed to Reduce Cancellation Rates in an Ultrasound-Guided Biopsy Program Stephanie A. Kenny, BSc, MD Ania Z. Kielar, MD, FRCPC Conflicts
Getting to Zero: A Quality Assessment of Multiple Interventions Aimed to Reduce Cancellation Rates in an Ultrasound-Guided Biopsy Program Stephanie A. Kenny, BSc, MD Ania Z. Kielar, MD, FRCPC Conflicts
SURGICAL ONCOLOGY MCVH
 SURGICAL ONCOLOGY MCVH PGY-4 and PGY-5 Medical Knowledge: Demonstrates knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social-behavioral) sciences;
SURGICAL ONCOLOGY MCVH PGY-4 and PGY-5 Medical Knowledge: Demonstrates knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social-behavioral) sciences;
Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD
 Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Quality Improvement/Systems-based Practice. Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery
 Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
QUALITY IMPROVEMENT ON A GLOBAL LEVEL- HOW CAN THIS TASK BE ACCOMPLISHED?
 QUALITY IMPROVEMENT ON A GLOBAL LEVEL- HOW CAN THIS TASK BE ACCOMPLISHED? Marilyn J. Goske MD Chair, Alliance for Radiation Safety in Pediatric Imaging Corning Benton Endowed Chair for Radiology Education
QUALITY IMPROVEMENT ON A GLOBAL LEVEL- HOW CAN THIS TASK BE ACCOMPLISHED? Marilyn J. Goske MD Chair, Alliance for Radiation Safety in Pediatric Imaging Corning Benton Endowed Chair for Radiology Education
Root Cause Analysis LITE (RCA Lite)
") Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Failure Mode and Effects Analysis (FMEA) for the Surgical Patient
 for the Surgical Patient") How to Receive Your CE Credits Read your selected course Completed the quiz at the end of the course with a 70% or greater. Complete the evaluation for your selected course. Print your Certificate CE s
How to Receive Your CE Credits Read your selected course Completed the quiz at the end of the course with a 70% or greater. Complete the evaluation for your selected course. Print your Certificate CE s
Health Sciences Centre, Team C, Dr. M. Wells (Breast and Hernia) Medical Expert
 Medical Expert") Health Sciences Centre, Team C, Dr. M. Wells ( and ) Introduction The goal of this rotation is to afford senior residents the best possible opportunity to develop the foundational knowledge and skills
Health Sciences Centre, Team C, Dr. M. Wells ( and ) Introduction The goal of this rotation is to afford senior residents the best possible opportunity to develop the foundational knowledge and skills
Evidence-Based Quality Improvement: A recipe for improving medication safety and handover of care Smeulers, Marian
 UvA-DARE (Digital Academic Repository) Evidence-Based Quality Improvement: A recipe for improving medication safety and handover of care Smeulers, Marian Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Evidence-Based Quality Improvement: A recipe for improving medication safety and handover of care Smeulers, Marian Link to publication Citation for published version
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager
 Ratchada Prakongsai Senior Manager") Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference
 Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference INGA AIKMAN, MD, MPH PEDIATRIC CHIEF RESIDENT EAST CAROLINA UNIVERSITY Second Annual REACH Medical
Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference INGA AIKMAN, MD, MPH PEDIATRIC CHIEF RESIDENT EAST CAROLINA UNIVERSITY Second Annual REACH Medical
COOK COUNTY HEALTH & HOSPITALS SYSTEM
 COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
A Framework for Quality Improvement
 U019 - Integrating QI into the Derm Practice A Framework for Quality Improvement Margo Reeder, MD Assistant Professor Director of Quality Improvement UWSMPH July 30 2016 Quality is increasingly part of
U019 - Integrating QI into the Derm Practice A Framework for Quality Improvement Margo Reeder, MD Assistant Professor Director of Quality Improvement UWSMPH July 30 2016 Quality is increasingly part of
Year in Review ro ils RO ILS
 RO ILS RADIATION ONCOLOGY INCIDENT LEARNING SYSTEM Sponsored by ASTRO and AAPM Year in Review 2015 1 ro ils noun \ˈro i(-ə)ls\ Radiation Oncology Incident Learning System; a system to facilitate safer
RO ILS RADIATION ONCOLOGY INCIDENT LEARNING SYSTEM Sponsored by ASTRO and AAPM Year in Review 2015 1 ro ils noun \ˈro i(-ə)ls\ Radiation Oncology Incident Learning System; a system to facilitate safer
Quality Initiatives. Anatomy and Pathophysiology of Errors Occurring in Clinical Radiology Practice 1 QUALITY INITIATIVES
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. QUALITY INITIATIVES
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. QUALITY INITIATIVES
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Preventing Medical Errors : A Call to Action. Definitions of Quality. Quality of Care. Objectives. Background of the Quality Movement
 Quality Assessment, Quality Assurance and Quality Improvement in Dentistry November 18, 2003 With thanks to Drs. Georgina Zabos and James Crall Objectives Become familiar with the social, economic and
Quality Assessment, Quality Assurance and Quality Improvement in Dentistry November 18, 2003 With thanks to Drs. Georgina Zabos and James Crall Objectives Become familiar with the social, economic and
ECRI Patient Safety Organization HFACS and Healthcare
 October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
Introduction. Medication Errors. Objectives. Objectives. January What is a Medication Error? Define medication errors/variances
 Medication Errors Earlene Spence, Pharm.D., Miami VA Healthcare System Neena John, Pharm.D., Miami VA Healthcare System Eva Moreira, Pharm.D., Miami VA Healthcare System Chantal Chan, Pharm.D., Miami VA
Medication Errors Earlene Spence, Pharm.D., Miami VA Healthcare System Neena John, Pharm.D., Miami VA Healthcare System Eva Moreira, Pharm.D., Miami VA Healthcare System Chantal Chan, Pharm.D., Miami VA
Building a Safe Healthcare System
 Building a Safe Healthcare System Objectives 2 Discuss the process of improving healthcare systems. Introduce widely-used methodologies in QI/PS. What is Quality Improvement? 3 Process of continually evaluating
Building a Safe Healthcare System Objectives 2 Discuss the process of improving healthcare systems. Introduce widely-used methodologies in QI/PS. What is Quality Improvement? 3 Process of continually evaluating
Health Management Information Systems: Computerized Provider Order Entry
 Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
Medication Safety in LTC. Objectives. About ISMP Canada
 Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
* human beings or animals
 Description of Work: Positions in this banded class perform skilled technical work in the administration of radiologic procedures used for the diagnosis and treatment of patients*. These positions perform
Description of Work: Positions in this banded class perform skilled technical work in the administration of radiologic procedures used for the diagnosis and treatment of patients*. These positions perform
M E D I C AL D I AG N O S T I C T E C H N I C I AN Schematic Code ( )
") I. DESCRIPTION OF WORK M E D I C AL D I AG N O S T I C T E C H N I C I AN Schematic Code 14250 (31000080) Positions in this banded class perform skilled technical work in the administration of radiologic
I. DESCRIPTION OF WORK M E D I C AL D I AG N O S T I C T E C H N I C I AN Schematic Code 14250 (31000080) Positions in this banded class perform skilled technical work in the administration of radiologic
Proposed Standards Revisions Related to Pain Assessment and Management
 Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
Building and Sustaining a Culture of Safety
 Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
National Patient Safety Agency Root Cause Analysis (RCA) Investigation
 Investigation") National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
PREP the Course 2017 St. Petersburg, FL General Pediatrics Session II
 PREP the Course 2017 St. Petersburg, FL General Pediatrics Session II The speaker has no conflicts of interest to disclose. No commercial support No discussion of off-label usage of drugs or devices/equipment
PREP the Course 2017 St. Petersburg, FL General Pediatrics Session II The speaker has no conflicts of interest to disclose. No commercial support No discussion of off-label usage of drugs or devices/equipment
The Power of Quality. Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center
 The Power of Quality Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center What do you think of when you hear the word quality? LEAN RCA PDSA QAPI SIX SIGMA PIP TQM 5s Objectives Transplant
The Power of Quality Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center What do you think of when you hear the word quality? LEAN RCA PDSA QAPI SIX SIGMA PIP TQM 5s Objectives Transplant
Using CAST for Adverse Event Investigation in Hospitals
 Using CAST for Adverse Event Investigation in Hospitals Meaghan O Neil March 27, 2014 Motivation As many as 98,000 people, die in hospitals each year as a result of medical errors that could have been
Using CAST for Adverse Event Investigation in Hospitals Meaghan O Neil March 27, 2014 Motivation As many as 98,000 people, die in hospitals each year as a result of medical errors that could have been
A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care
 A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care Gordy Schiff, MD, Associate Director of Brigham and Women s Center for Patient Safety Research
A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care Gordy Schiff, MD, Associate Director of Brigham and Women s Center for Patient Safety Research
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Text-based Document. The Culture of Incident Reporting Among Filipino Nurses. de Guzman, Barbara Michelle. Downloaded 28-Apr :54:41
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Interactive Urological Outpatient Workshop
 Interactive Urological Outpatient Workshop One Stop Urology Clinic design Norfolk and Norwich University Hospitals 25 th September 2014 Is this your service? Multiple entry points into the service new
Interactive Urological Outpatient Workshop One Stop Urology Clinic design Norfolk and Norwich University Hospitals 25 th September 2014 Is this your service? Multiple entry points into the service new
Resident Core Curriculum Vascular and Interventional Radiology
 Resident Core Curriculum Vascular and Interventional Radiology General Goals: The specific goals include objectives required for every level of training with graduated levels of supervision and responsibility.
Resident Core Curriculum Vascular and Interventional Radiology General Goals: The specific goals include objectives required for every level of training with graduated levels of supervision and responsibility.
The Practice Standards for Medical Imaging and Radiation Therapy. Quality Management Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Quality Management Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of
The Practice Standards for Medical Imaging and Radiation Therapy Quality Management Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of
External retrospective Validation of BIG criteria. An example of PDSA for Neurotrauma patients.
 External retrospective Validation of BIG criteria. An example of PDSA for Neurotrauma patients. Ahmed M. Raslan, MD Assistant Professor in Neurological Surgery Neuroscience quality medical director Oregon
External retrospective Validation of BIG criteria. An example of PDSA for Neurotrauma patients. Ahmed M. Raslan, MD Assistant Professor in Neurological Surgery Neuroscience quality medical director Oregon
Anatomy of a Fatal Medication Error
 Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Setting: Emergency departments are high-risk contexts; they are over-crowded and
 QUALITY IMPROVEMENT STUDENT PROJECT PROPOSAL: IMPROVING HANDOFFS IN SAN FRANCISCO GENERAL HOSPTITAL S EMERGENCY DEPARTMENT TMIT Student Projects QuickStart Package 1. BACKGROUND Setting: Emergency departments
QUALITY IMPROVEMENT STUDENT PROJECT PROPOSAL: IMPROVING HANDOFFS IN SAN FRANCISCO GENERAL HOSPTITAL S EMERGENCY DEPARTMENT TMIT Student Projects QuickStart Package 1. BACKGROUND Setting: Emergency departments
Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship
 Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship Diane Levine, Wayne State University Allison Heacock, The Ohio State University Amy Shaheen, University of North Carolina
Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship Diane Levine, Wayne State University Allison Heacock, The Ohio State University Amy Shaheen, University of North Carolina
THE ROLE OF BIOMEDICAL ENGINEERING IN HEALTH TECHNOLOGY MANAGEMENT
 THE ROLE OF BIOMEDICAL ENGINEERING IN HEALTH TECHNOLOGY MANAGEMENT THE OPPORTUNITIES AND CHALLENGES IN A LOCAL HEALTH CARE SETTING 2017 CADTH SYMPOSIUM HAL HILFI, CORPORATE MANAGER THE OTTAWA HOSPITAL
THE ROLE OF BIOMEDICAL ENGINEERING IN HEALTH TECHNOLOGY MANAGEMENT THE OPPORTUNITIES AND CHALLENGES IN A LOCAL HEALTH CARE SETTING 2017 CADTH SYMPOSIUM HAL HILFI, CORPORATE MANAGER THE OTTAWA HOSPITAL
Image Gently: A Web-Based Practice Quality Improvement Program in CT Safety for Children
 Pediatric Imaging Technical Innovation Goske et al. CT Safety for Children Pediatric Imaging Technical Innovation FOCUS ON: Marilyn J. Goske 1 Rebecca R. Phillips 2 Keith Mandel 3 Daniel McLinden 4 Judy
Pediatric Imaging Technical Innovation Goske et al. CT Safety for Children Pediatric Imaging Technical Innovation FOCUS ON: Marilyn J. Goske 1 Rebecca R. Phillips 2 Keith Mandel 3 Daniel McLinden 4 Judy
Internal Medicine Curriculum Gastroenterology/Hepatology Rotation
 Internal Medicine Curriculum Gastroenterology/Hepatology Rotation Contact Person: Educational Purpose Gastrointestinal and hepatic disorders frequently cause patients to seek medical attention. Abdominal
Internal Medicine Curriculum Gastroenterology/Hepatology Rotation Contact Person: Educational Purpose Gastrointestinal and hepatic disorders frequently cause patients to seek medical attention. Abdominal
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
Radiology Review Course ABR Non interpretive Skills
 Radiology Review Course ABR Non interpretive Skills March 30, 2015 Annemarie Relyea Chew, JD, MS Associate Professor Radiology Adjunct Associate Professor BIME University of Washington School of Medicine
Radiology Review Course ABR Non interpretive Skills March 30, 2015 Annemarie Relyea Chew, JD, MS Associate Professor Radiology Adjunct Associate Professor BIME University of Washington School of Medicine
Patient Care. Medical Knowledge
 Interventional Radiology (First Year, First Block) This rotation involves performance and interpretation of diagnostic and therapeutic angiograms and venograms, dialysis access, line placement, drainage
Interventional Radiology (First Year, First Block) This rotation involves performance and interpretation of diagnostic and therapeutic angiograms and venograms, dialysis access, line placement, drainage
MRI Patient Screening and History
 Griffin Imaging, LLC 220 Rock Street Griffin, GA 30224 (770) 229-4660 Fax:: (770) 229-4632 Specializing In Open MRI, CT & Ultrasound MRI Patient Screening and History Patient Information Sheet PATIENT
Griffin Imaging, LLC 220 Rock Street Griffin, GA 30224 (770) 229-4660 Fax:: (770) 229-4632 Specializing In Open MRI, CT & Ultrasound MRI Patient Screening and History Patient Information Sheet PATIENT
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
By the final rotation in Nuclear Medicine as a first year Radiology Resident, the resident will demonstrate:
 Goals and Objectives Nuclear Medicine Rotation First Year Residents Patient Care Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health
Goals and Objectives Nuclear Medicine Rotation First Year Residents Patient Care Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health
UW MEDICINE PATIENT EDUCATION. Angiography: Radiofrequency Ablation to Treat Solid Tumor. What to expect. What is radiofrequency ablation?
 UW MEDICINE PATIENT EDUCATION Angiography: Radiofrequency Ablation to Treat Solid Tumor What to expect This handout explains radiofrequency ablation and what to expect when you have this treatment for
UW MEDICINE PATIENT EDUCATION Angiography: Radiofrequency Ablation to Treat Solid Tumor What to expect This handout explains radiofrequency ablation and what to expect when you have this treatment for
Laverne Estañol, M.S., CHRC, CIP, CCRP Assistant Director Human Research Protections
 Laverne Estañol, M.S., CHRC, CIP, CCRP Assistant Director Human Research Protections Quality Improvement Activities and Human Subjects Research September 7, 2016 TOPICS What is Quality Improvement (QI)?
Laverne Estañol, M.S., CHRC, CIP, CCRP Assistant Director Human Research Protections Quality Improvement Activities and Human Subjects Research September 7, 2016 TOPICS What is Quality Improvement (QI)?
How to Help Write a Good Consent Form: MOVING FROM! INFORMED CONSENT to INFORMED CHOICE
 How to Help Write a Good Consent Form: MOVING FROM! INFORMED CONSENT to INFORMED CHOICE Peggy Devine Founder & President Cancer Information & Support Network (CISN) C3 ASCO advocate training January 19,
How to Help Write a Good Consent Form: MOVING FROM! INFORMED CONSENT to INFORMED CHOICE Peggy Devine Founder & President Cancer Information & Support Network (CISN) C3 ASCO advocate training January 19,
CLINICAL IMAGING REFERRAL PROTOCOL FOR REGISTERED NURSE PRACTITIONERS IN THE EMERGENCY DEPARTMENT, URGENT CARE CENTRE AND AMBULATORY CARE
 CLINICAL IMAGING REFERRAL PROTOCOL FOR REGISTERED NURSE PRACTITIONERS IN THE EMERGENCY DEPARTMENT, URGENT CARE CENTRE AND AMBULATORY CARE CLINICAL GUIDELINE V4. Summary. Start The non-medical practitioner
CLINICAL IMAGING REFERRAL PROTOCOL FOR REGISTERED NURSE PRACTITIONERS IN THE EMERGENCY DEPARTMENT, URGENT CARE CENTRE AND AMBULATORY CARE CLINICAL GUIDELINE V4. Summary. Start The non-medical practitioner
IS YOUR QAPI COP READY?
 IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
Improving Access to Pediatric MR performed under General Anesthesia Benefits of a Rapid Improvement Event (RIE)
") /3/207 Improving Access to Pediatric MR performed under General Anesthesia Benefits of a Rapid Improvement Event (RIE) N I Sarwani, MD, FRCR, FSAR M A Bruno, MS, MD, FACR S Mrozowski, MHA, NRP, CPPS Corresponding
/3/207 Improving Access to Pediatric MR performed under General Anesthesia Benefits of a Rapid Improvement Event (RIE) N I Sarwani, MD, FRCR, FSAR M A Bruno, MS, MD, FACR S Mrozowski, MHA, NRP, CPPS Corresponding
1.3 Referrer: in the context of this protocol the term referrer refers to a health care worker who is authorised to refer individuals for X-rays.
 Clinical Guideline for Clinical Imaging Referral Protocol for Nurse Endoscopist (Lower GI) within the Royal Cornwall Hospitals Trust 1. Aim/Purpose of this Guideline 1.1 This protocol applies to Nurse
Clinical Guideline for Clinical Imaging Referral Protocol for Nurse Endoscopist (Lower GI) within the Royal Cornwall Hospitals Trust 1. Aim/Purpose of this Guideline 1.1 This protocol applies to Nurse
IMPACT OF TECHNOLOGY ON MEDICATION SAFETY
 Continuous Quality Improvement IMPACT OF Steven R. Abel, PharmD, FASHP TECHNOLOGY ON Nital Patel, PharmD. MBA MEDICATION SAFETY Sheri Helms, PharmD Candidate Brian Heckman, PharmD Candidate Ismaila D Badjie
Continuous Quality Improvement IMPACT OF Steven R. Abel, PharmD, FASHP TECHNOLOGY ON Nital Patel, PharmD. MBA MEDICATION SAFETY Sheri Helms, PharmD Candidate Brian Heckman, PharmD Candidate Ismaila D Badjie
Reporting and Disclosing Adverse Events
 Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
General Eligibility Requirements
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
Click to edit Master title. style. Click to edit Master title. style. style 8/3/ Are You on Track?
 Are You on Track? Diagnostic Test Results, Consults and Referrals Click to edit Master subtitle EXPLORE Conference August 9, 2018 8/3/2018 1 EXPLORE August 9, 2018 Today s speaker is Brenda Wehrle, BS,
Are You on Track? Diagnostic Test Results, Consults and Referrals Click to edit Master subtitle EXPLORE Conference August 9, 2018 8/3/2018 1 EXPLORE August 9, 2018 Today s speaker is Brenda Wehrle, BS,
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
OUTPATIENT DOCUMENTATION IMPROVEMENT
 OUTPATIENT DOCUMENTATION IMPROVEMENT Pam Brooks, MHA, COC, PCS, CPC Coding Manager Wentworth-Douglass Hospital Dover NH Disclaimer This presentation is for general education purposes only. The information
OUTPATIENT DOCUMENTATION IMPROVEMENT Pam Brooks, MHA, COC, PCS, CPC Coding Manager Wentworth-Douglass Hospital Dover NH Disclaimer This presentation is for general education purposes only. The information
Quality Assurance and Performance Improvement (QAPI)
") Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
Consensus Reports and Recommendations to Prevent Retained Surgical Items
 Consensus Reports and Recommendations to Prevent Retained Surgical Items Summary by the Institute for Population Health Improvement, UC Davis Health System Category Items included in surgical count When
Consensus Reports and Recommendations to Prevent Retained Surgical Items Summary by the Institute for Population Health Improvement, UC Davis Health System Category Items included in surgical count When
Stanford Surgical Oncology II: R1 Tuesday, February 02, 2016
 Stanford University General Surgery Residency Program Surgical Oncology II Surgery goals and objectives for residents: R-1 Rotation Director: Ralph Greco, MD Description The Surgical Oncology II rotation
Stanford University General Surgery Residency Program Surgical Oncology II Surgery goals and objectives for residents: R-1 Rotation Director: Ralph Greco, MD Description The Surgical Oncology II rotation
Goals and Objectives revised 9/09 OTO4 Facial Plastics and Reconstructive Surgery Rotation, Johns Hopkins University
 PGY-4 GBMC/JHH Facial Plastics and Reconstructive Surgery Rotation. Each OTO4 spends 3 months on the combined GBMC/JHH FPRS service (OTO4 FPRS resident). This rotation ensures that the resident has time
PGY-4 GBMC/JHH Facial Plastics and Reconstructive Surgery Rotation. Each OTO4 spends 3 months on the combined GBMC/JHH FPRS service (OTO4 FPRS resident). This rotation ensures that the resident has time
1/22/2014. Defining Quality in Healthcare. Objectives. Topics of discussion. Quality for the non-quality Manager Session 1
 Defining Quality in Healthcare Quality for the non-quality Manager Session 1 Presented by Paul E. Frigoli, Ph.D.(c), R.N., C.P.H.Q., C.S.S.B.B. Certified Lean Six Sigma Master Black Belt Objectives At
Defining Quality in Healthcare Quality for the non-quality Manager Session 1 Presented by Paul E. Frigoli, Ph.D.(c), R.N., C.P.H.Q., C.S.S.B.B. Certified Lean Six Sigma Master Black Belt Objectives At
ADMINISTRATIVE POLICY & PROCEDURE PATIENT SAFETY PLAN
 PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
Performance-Based Assessment of Radiology Practitioners: Promoting Improvement in Accordance with the 2007 Joint Commission Standards
 Performance-Based Assessment of Radiology Practitioners: Promoting Improvement in Accordance with the 2007 Joint Commission Standards Lane F. Donnelly, MD a,b New guidelines for medical credentialing and
Performance-Based Assessment of Radiology Practitioners: Promoting Improvement in Accordance with the 2007 Joint Commission Standards Lane F. Donnelly, MD a,b New guidelines for medical credentialing and
FieldStrength. Publication for the Philips MRI Community Issue 36 December Reducing examination waiting time and boosting patient throughput
 FieldStrength Publication for the Philips MRI Community Issue 36 December 2008 Reducing examination waiting time and boosting patient throughput This article is part of Field Strength issue 36, Dec. 2008
FieldStrength Publication for the Philips MRI Community Issue 36 December 2008 Reducing examination waiting time and boosting patient throughput This article is part of Field Strength issue 36, Dec. 2008
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Using the epoc Point of Care Blood Analysis System Reduces Costs, Improves Operational Efficiencies, and Enhances Patient Care
 Using the epoc Point of Care Blood Analysis System Reduces Costs, Improves Operational Efficiencies, and Enhances Patient Care Clarke Woods, BS, RRT, FABC, Director, Cardiopulmonary Services, Pinnacle
Using the epoc Point of Care Blood Analysis System Reduces Costs, Improves Operational Efficiencies, and Enhances Patient Care Clarke Woods, BS, RRT, FABC, Director, Cardiopulmonary Services, Pinnacle
Evaluation of an Eye Tracking Device to Increase Error Recovery by Nursing Students Using Human Patient Simulation
 University of Massachusetts Amherst ScholarWorks@UMass Amherst Masters Theses 1911 - February 2014 Dissertations and Theses 2010 Evaluation of an Eye Tracking Device to Increase Error Recovery by Nursing
University of Massachusetts Amherst ScholarWorks@UMass Amherst Masters Theses 1911 - February 2014 Dissertations and Theses 2010 Evaluation of an Eye Tracking Device to Increase Error Recovery by Nursing
CLINICAL GUIDELINE FOR CLINICAL IMAGING REFERRAL PROTOCOL FOR NURSE SPECIALISTS IN HEART FUNCTION WITHIN RCHT Summary. Start
 CLINICAL GUIDELINE FOR CLINICAL IMAGING REFERRAL PROTOCOL FOR NURSE SPECIALISTS IN HEART FUNCTION WITHIN RCHT Summary. Start The non-medical practitioner has received sufficient training to make clinical
CLINICAL GUIDELINE FOR CLINICAL IMAGING REFERRAL PROTOCOL FOR NURSE SPECIALISTS IN HEART FUNCTION WITHIN RCHT Summary. Start The non-medical practitioner has received sufficient training to make clinical
A Multi-Phased Approach to Using Clinical Data to Drive Evidence-Based EMR Redesign. Kulik, Carole Marie; Foad, Wendy; Brown, Gretchen
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Health Management Information Systems
 Health Management Information Systems Computerized Provider Order Entry (CPOE) Computerized Provider Order Entry (CPOE) Learning Objectives 1. Describe the purpose, attributes and functions of CPOE 2.
Health Management Information Systems Computerized Provider Order Entry (CPOE) Computerized Provider Order Entry (CPOE) Learning Objectives 1. Describe the purpose, attributes and functions of CPOE 2.
IMPORTANCE OF IMPROVING INTERPERSONAL COMMUNICATION SKILLS OF MEDICAL PERSONNEL IN MINIMIZING MEDICAL LIABILITY CLAIMS PIOTR DANILUK, MD
 Polskie Towarzystwo Medycyny Ubezpieczeniowej IMPORTANCE OF IMPROVING INTERPERSONAL COMMUNICATION SKILLS OF MEDICAL PERSONNEL IN MINIMIZING MEDICAL LIABILITY CLAIMS PIOTR DANILUK, MD Warsaw, 23.09.2016
Polskie Towarzystwo Medycyny Ubezpieczeniowej IMPORTANCE OF IMPROVING INTERPERSONAL COMMUNICATION SKILLS OF MEDICAL PERSONNEL IN MINIMIZING MEDICAL LIABILITY CLAIMS PIOTR DANILUK, MD Warsaw, 23.09.2016
Not the Same Old EOD: the New and Improved SEER EOD for 2018 and Beyond
 Not the Same Old EOD: the New and Improved SEER EOD for 2018 and Beyond Christina Schwarz, BA, CTR CCRA-Northern California Staging Symposium September 20, 2017 Objectives Evolution of EOD Crosswalk with
Not the Same Old EOD: the New and Improved SEER EOD for 2018 and Beyond Christina Schwarz, BA, CTR CCRA-Northern California Staging Symposium September 20, 2017 Objectives Evolution of EOD Crosswalk with
Department of Veterans Affairs VHA Directive Washington, DC March 5, 2016 PREVENTION OF RETAINED SURGICAL ITEMS
 Department of Veterans Affairs VHA Directive 1103 Veterans Health Administration Transmittal Sheet Washington, DC 20420 March 5, 2016 PREVENTION OF RETAINED SURGICAL ITEMS 1. REASON FOR ISSUE: This Veterans
Department of Veterans Affairs VHA Directive 1103 Veterans Health Administration Transmittal Sheet Washington, DC 20420 March 5, 2016 PREVENTION OF RETAINED SURGICAL ITEMS 1. REASON FOR ISSUE: This Veterans
10/23/2015. Don t drop the baton: Improving handover communication from the CMPA s perspective
 Don t drop the baton: Improving handover communication from the CMPA s perspective This is an abridged version of presentation with cases and videos removed Dr Janet Nuth, Physician Risk Manager CMPA Associate
Don t drop the baton: Improving handover communication from the CMPA s perspective This is an abridged version of presentation with cases and videos removed Dr Janet Nuth, Physician Risk Manager CMPA Associate
Operational Excellence at Lifespan. Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence
 Operational Excellence at Lifespan Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence Objectives Discuss Lifespan s approach to establishing a system-based quality structure Describe the organization
Operational Excellence at Lifespan Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence Objectives Discuss Lifespan s approach to establishing a system-based quality structure Describe the organization
Mandatory Licensure for Radiologic Personnel. Christopher Jason Tien
 Mandatory Licensure for Radiologic Personnel Christopher Jason Tien Licensure Permission to perform a given occupation 3 rd party examinations State hands out licenses Occupations licensed: teachers, architects,
Mandatory Licensure for Radiologic Personnel Christopher Jason Tien Licensure Permission to perform a given occupation 3 rd party examinations State hands out licenses Occupations licensed: teachers, architects,
NIOSH Coal Workers Health Surveillance Program
 NIOSH Coal Workers Health Surveillance Program Anita L. Wolfe Public Health Analyst Program Operations Coordinator, CWHSP Division of Respiratory Disease Studies, NIOSH Morgantown, WV Coal Workers Health
NIOSH Coal Workers Health Surveillance Program Anita L. Wolfe Public Health Analyst Program Operations Coordinator, CWHSP Division of Respiratory Disease Studies, NIOSH Morgantown, WV Coal Workers Health
From Risk Management to Action Addressing Diagnostic Error. Dr. Terrance Borman Dr. Joseph Britto
 From Risk Management to Action Addressing Diagnostic Error Dr. Terrance Borman Dr. Joseph Britto Overview of presentation Luther Midelfort and our risk management Making the case for diagnostic error as
From Risk Management to Action Addressing Diagnostic Error Dr. Terrance Borman Dr. Joseph Britto Overview of presentation Luther Midelfort and our risk management Making the case for diagnostic error as
The Practice Standards for Medical Imaging and Radiation Therapy. Radiologist Assistant Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Radiologist Assistant Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part
The Practice Standards for Medical Imaging and Radiation Therapy Radiologist Assistant Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part
Achieving Operational Excellence with an EHR a CIO s Perspective
 Achieving Operational Excellence with an EHR a CIO s Perspective Phyllis Schuck, SPHR CIO of Pinehurst Surgical HIT Session 6.02 Thursday, March 29, 2007 Pinehurst Surgical Organization Overview Founded
Achieving Operational Excellence with an EHR a CIO s Perspective Phyllis Schuck, SPHR CIO of Pinehurst Surgical HIT Session 6.02 Thursday, March 29, 2007 Pinehurst Surgical Organization Overview Founded
Fostering a Culture of Safety
 Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
The Practice Standards for Medical Imaging and Radiation Therapy. Computed Tomography Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Computed Tomography Practice Standards 2011 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of
The Practice Standards for Medical Imaging and Radiation Therapy Computed Tomography Practice Standards 2011 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of
Diagnostic Errors: A Persistent Risk
 Diagnostic Errors: A Persistent Risk Laura M. Cascella, MA The term medical error often conjures thoughts of wrong-site surgeries, procedures performed on the wrong patients, retained foreign objects,
Diagnostic Errors: A Persistent Risk Laura M. Cascella, MA The term medical error often conjures thoughts of wrong-site surgeries, procedures performed on the wrong patients, retained foreign objects,
Medical Errors. Christopher L. Nuland, Esq. September 10, 2016
 Medical Errors Christopher L. Nuland, Esq. September 10, 2016 WHY ARE WE HERE Medical errors statute 456.013 (7) 456.013 (7) (7) The boards, or the department when there is no board, shall require the
Medical Errors Christopher L. Nuland, Esq. September 10, 2016 WHY ARE WE HERE Medical errors statute 456.013 (7) 456.013 (7) (7) The boards, or the department when there is no board, shall require the
INTRODUCTION. LEARNING OBJECTIVES (CanMEDS)
") OVERVIEW The Thoracic Surgery selective is based at Health Sciences Centre. Students participate in the surgical management of patients with lung cancer and esophageal cancer, as well as other conditions
OVERVIEW The Thoracic Surgery selective is based at Health Sciences Centre. Students participate in the surgical management of patients with lung cancer and esophageal cancer, as well as other conditions
Auckland District Health Board Summary 1 July 2011 to 30 June 2012 Serious and Sentinel Events
 DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified