PREP the Course 2017 St. Petersburg, FL General Pediatrics Session II
|
|
|
- Dora Watkins
- 5 years ago
- Views:
Transcription


1 PREP the Course 2017 St. Petersburg, FL General Pediatrics Session II

2 The speaker has no conflicts of interest to disclose. No commercial support No discussion of off-label usage of drugs or devices/equipment CS = Content specification

3 Medical errors remain problematic in clinical practice Pediatric patients may be particularly susceptible to medical errors There are opportunities to redesign practice to make patient care safer

4 Review the cost (in terms of morbidity/mortality and finances) of medical errors in the U.S. Define adverse events, medical errors, near misses, and sentinel events Determine which tools of QI are best suited for process analysis and which are best suited to follow data over time Describe the components of a PDSA cycle and articulate the role of PDSA cycles in quality improvement

5 Everyone in healthcare really has two jobs when they come to work every day: to do their work and to improve it. Paul Batalden
 CS CS Preventable adverse event based on available medical knowledge, could have been prevented Non-preventable adverse")
6 Medical error act of commission (do something wrong) or omission (fail to do the right thing) that leads to an undesirable outcome or significant potential for such an outcome Adverse event any injury caused by medical care (rather than the patient s underlying disease) CS CS Preventable adverse event based on available medical knowledge, could have been prevented Non-preventable adverse event based on available medical knowledge, could not have been prevented

7 Adverse event CS Does not imply error, negligence, or poor quality care Simply indicates that an undesirable clinical outcome resulted from some aspect of diagnosis or therapy, not from underlying disease process
8 Near-miss event close call an error/event that did not produce harm Intercepted Non-intercepted (no harm by chance) Sentinel event - adverse event in which death or serious harm to a patient has occurred Usually refers to events that are not at all expected or acceptable Word sentinel reflects the egregiousness of the injury (e.g., wrong site surgery); high likelihood that investigation of such events will reveal serious problems in current policies/procedures CS CS

9 EVENT 1. Patient develops Stevens Johnson syndrome after taking Ibuprofen 2. PCN is ordered on a patient who is PCN allergic, but pharmacy catches the mistake 3. Wrong child gets circumcised 4. Child on ventilator develops PNA despite rigorous best staff hygiene/practices CLASSIFICATION A. Medical error B. Preventable adverse event C. Non preventable adverse event D. Near miss E. Sentinel event
:835 60")
10 Estimated 44,000-98,000 hospitalized patients die each year as a result of medical errors in the U.S. In 2015 there were 33,693 deaths in the U.S. due to guns (11,208 murders, 21,175 suicides, and the remainder were accidental) U.S. medical system is 3-9 times deadlier than a gun Estimated $17-29 billion/year 1 CS 1 Mello MM, Studdert EM, Thomas EJ, et al. Journal of Empirical Legal Studies, Dec (4):835 60
11 Review of 4 studies New methodology Lower limit of 210,000 PAEs that caused patient deaths
12
13 CS Some estimate 3x more risk of AEs in children Study of hospitalized children in Colorado and Utah AEs affected 1% of hospitalized children 70,000 children/year 60% are felt to be preventable Adverse drug events are the most common Birth related Diagnostic related Higher rates of AEs in adolescent patients Woods D, et al. Adverse events and preventable adverse events in children. Pediatrics ;115:
14 CS Weight-based dosing Over dosing Under dosing Long length of stay Complex medical regimens High severity of illness Adolescents
15 Most common adverse event (Why?) Multiple opportunities for errors Ordering Transcription Preparation Delivery Administration Medication errors include errors of commission and omission
16 Product naming and packaging Medical abbreviations (e.g., MgSO 4 and MSO 4, a.u. and o.u., etc.) Electronic prescribing v. handwritten Rxs Role of ancillary services (e.g., pharmacy) to prevent medication errors Medical device design CS
17 Error Diverted
18
19 People Procedures & Policies Equipment

20 CS System People Procedures Equipment Etc.
21 Every system is perfectly designed to achieve exactly the results it gets. Don Berwick, Former President and CEO Institute for Healthcare Improvement

22 Every system is perfectly designed to achieve exactly the results it gets. Don Berwick, Former President and CEO Institute for Healthcare Improvement
23 A bad system will beat a good person every time. - W. Edwards Deming
24 Knowledge, skill, training, experience Needs, bias, beliefs, mood, motivations Age (generation), gender, ethnicity Stress Fatigue Distraction CS
25 Failure mode effect analysis (FMEA) proactive QI process used to anticipate/determine system vulnerability, including points of potential failure and what their effect would be before an error actually happens Root cause analysis (RCA) is a reactive process, employed after an error occurs, to identify its underlying causes CS CS
26 CS Identifies the what, how, and why something happened Goal is to prevent recurrence of the event 4 steps Collect data Chart causal factors Identify root causes Make recommendations/implement changes
27 Recognition of potential for errors and detection of medical errors/aes is key first step Missed detection of errors = missed opportunities for improvement Near misses great opportunities to reflect on system and how errors can be eliminated prior to actual patient harm CS
28 Hubris Lack of detection/recognition Fear of blame Fear of litigation Time consuming Unclear mechanism for reporting CS

29 CS Non-punitive, non-blaming culture Focus on the system Anonymous reporting systems Non-discoverable Trigger methodology where specific events trigger a detailed case review/chart audit Ordering of certain drugs (e.g., antidiarrheals) Orders for antidotes Certain abnormal laboratory values Abrupt stop orders Voluntary systems for reporting adverse medical event Strongly endorsed by IOM e-ers underused by physicians (< 2%) 1 1 Milch CE, Salem DN, et al. Voluntary Electronic Reporting of Medical Errors and Adverse Events. J Gen Intern Med. 2006: 21:
30 Effective communication (e.g. SBAR) Computerized physician order entry (CPOE) and dose-range checking, allergy verification Maintain a culture of safety/quality improvement e.g., MMI conferences, QI training courses/conferences, morning report Role for institutional leadership Transparency (Practice-based learning and improvement) Practice EBM Utilize best-practice guidelines/protocols CS
 Avoid situations that increase errors (fatigue, distractions, stress, etc.")
31 CS Team approach to patient care (AND to QI) - physicians, nursing, pharmacy, etc. with all empowered to voice concerns/share ideas (System-based practice) Avoid situations that increase errors (fatigue, distractions, stress, etc.) Empower patients and families to help reduce errors National patient safety goals UAL Flt 173 to Portland, OR, 1978
32 Identify patients correctly Use at least 2 patient identifiers Eliminate transfusion errors Improve communication Timely communication of critical lab and diagnostic test results Use medicines safely Labeled medications drawn up for procedures Reduce harm from anticoagulation Rxs Update medication lists CS
33 CS Prevent health care associated infections Hand hygiene EBM practices to prevent multi-drug resistance infections EBM practices to prevent CLABSI EBM practices to prevent surgical site infections EBM practices to prevent CAUTI Prevent falls
34 CS Prevent decubitus ulcers Assess and reassess each patient s risk and take appropriate action to address identified risks Universal protocol to prevent wrong site, wrong procedure, wrong person surgery Conduct pre-procedure verification Mark surgical sites Procedural time out

35
36 CS Choose private area/set the stage Provide brief review of the course of care Warning shot to signal what is coming Be frank, kind, and PAUSE Empathy Comfort with silence Gauge patient/family readiness for information Invite future questions Advise regarding physician availability (dispel abandonment fears) Pichert JW, Hickson GB, et al. (2012) Communicating about Unexpected Outcomes, Adverse Events, and Errors. In: P. Carayon, ed. Handbook of Human Factors and Ergonomics in Health Care and Patient Safety. (pp Boca Raton, FL: CRC Press.
37 CS Precise apology When and where error occurred Causes, results of harm, action taken to reduce harm/prevent recurrence Who will manage ongoing care Describe error review process, reporting, how system issues are identified Provide contact for ongoing communication Offer counseling/support Address bills for additional care Pichert JW, Hickson GB, et al. (2012) Communicating about Unexpected Outcomes, Adverse Events, and Errors. In: P. Carayon, ed. Handbook of Human Factors and Ergonomics in Health Care and Patient Safety. (pp Boca Raton, FL: CRC Press.

38 For the patient and family For the physicians and other health care providers involved CS


39 VS
40 Supposing is good, but finding out is better. -Mark Twain in Eruption; -Mark Twain's Autobiography
41



42 CS Data measured over time Useful to track trends Run charts Control charts (AKA Shewhart charts)
43 When an intervention works Positive reinforcement When an intervention does not work Truthful assessment should lead to reallocation of resources/effort to find a better way When an intervention works differently than was expected Identification of unintended consequences CS
44 Cause-effect diagrams Flow charts Check sheets Scatter diagrams Histograms Pareto charts
45 AKA fishbone diagrams or Ishikawa diagrams Identifies factors leading to overall effect


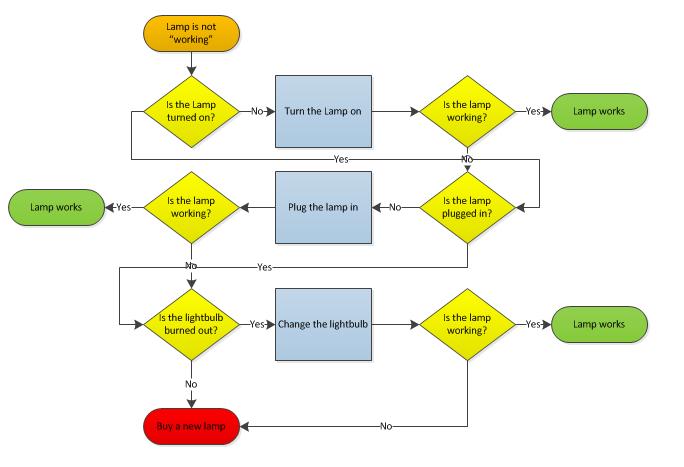
46 Schematic representation of an algorithm or step-wise process
47 Check sheets Scatter plots Histograms Pareto charts Pareto Chart of Reasons for Late Clinic Arrivals Weight (lbs) Scatter Diagram Weight v. Height Number of times reason cited Cumulative Percent Height (in)
 Plan to carry out the cycle (who, what, where,")
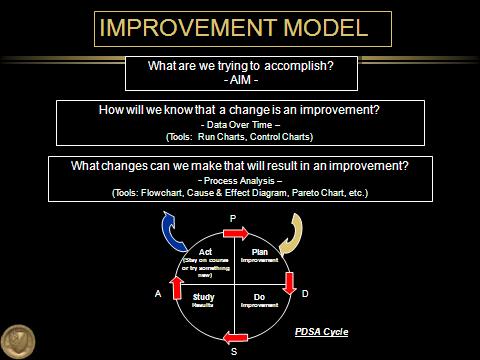
48 What is a PDSA Cycle? CS Act What changes are to be made? Next cycle? Study Complete the analysis of the data Compare data to predictions Summarize what was learned Plan Objective Questions and predictions (why) Plan to carry out the cycle (who, what, where, when) Do Carry out the plan Document problems and unexpected observations Begin analysis of the data Langley GL, et al. 2009
 What changes can we make that will result in an improvement? - Process Analysis (Tools: Flowchart, Cause & Effect Diagram, Pareto Chart, etc.")
49 IMPROVEMENT MODEL What are we trying to accomplish? -AIM - How will we know that a change is an improvement? - Data Over Time (Tools: Run Charts, Control Charts) What changes can we make that will result in an improvement? - Process Analysis (Tools: Flowchart, Cause & Effect Diagram, Pareto Chart, etc.) P Act (Stay on course or try something new) Plan Improvement A Study Results Do Improvement D PDSA Cycle S
50

51 Health care can be dangerous we need to make it safer for patients Medical errors and AEs have a lot of cost morbidity, mortality, and financial When errors occur disclosure is needed Quality Improvement necessary and part of our professional responsibilities IHI model for health care improvement PDSA cycle Importance of following data over time
52 Evaluate your practice in terms of its safety culture Consider educating your practice staff on the importance of recognizing medical errors Challenge all members of your health care team to become patient safety and quality care advocates Remind patients and family members of their roles in making patient care safer

53 One person can make a difference, and everyone should try. - John F. Kennedy waldon.garriss@wellstar.org
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB
 Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient Safety
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient Safety
Patient Safety Overview
 Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH, LSSBB Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH, LSSBB Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM
 Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Objectives. Key Elements. ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management 5/20/2014
 ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
PATIENT SAFETY KNOWLEDGEBASE. How to prepare for a Survey
 PATIENT SAFETY KNOWLEDGEBASE How to prepare for a Survey 1 DEFINITIONS Patient Safety v is a process that guards against any adverse condition occurring in a patient as a result of wrong diagnosis or treatment
PATIENT SAFETY KNOWLEDGEBASE How to prepare for a Survey 1 DEFINITIONS Patient Safety v is a process that guards against any adverse condition occurring in a patient as a result of wrong diagnosis or treatment
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference - November 9, 2013
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference - November 9, 2013 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference - November 9, 2013 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
Contact Hours (CME version ONLY) Suggested Target Audience. all clinical and allied patient care staff. all clinical and allied patient care staff
 Suggested Target Audience. all clinical and allied patient care staff. all clinical and allied patient care staff") 1 Addressing Behaviors That Undermine a Culture of Safety PA CE CME FL 8/31/2016 2 2 7 3 43 1.0 1.0 1.0 all staff Sentinel Event Alert, Issue 40: Behaviors that undermine a culture of safety 2 Adverse
1 Addressing Behaviors That Undermine a Culture of Safety PA CE CME FL 8/31/2016 2 2 7 3 43 1.0 1.0 1.0 all staff Sentinel Event Alert, Issue 40: Behaviors that undermine a culture of safety 2 Adverse
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
Innovative Techniques for Residents to Improve Safety
 Innovative Techniques for Residents to Improve Safety Eugene Terry, MD Modified from Tammy Lundsrum,MD www.mihealthandsafety.org/presentations/lundstrom.ppt What is a Safety Culture And how is it achieved?
Innovative Techniques for Residents to Improve Safety Eugene Terry, MD Modified from Tammy Lundsrum,MD www.mihealthandsafety.org/presentations/lundstrom.ppt What is a Safety Culture And how is it achieved?
Root Cause Analysis LITE (RCA Lite)
") Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Expanding Improvement Science Competencies: Successes & Challenges Terry L. Jones RN, PhD. utexas.edu/nursing
 Expanding Improvement Science Competencies: Successes & Challenges Terry L. Jones RN, PhD Objectives Review literature related to educational preparation for IS competencies. Describe an exemplar course
Expanding Improvement Science Competencies: Successes & Challenges Terry L. Jones RN, PhD Objectives Review literature related to educational preparation for IS competencies. Describe an exemplar course
PATIENT SAFETY OVERVIEW
 PATIENT SAFETY OVERVIEW MUHAMMAD ISLAM, MBBS, MS, MCH, LSSBB DIRECTOR OF PATIENT SAFETY SUNY DOWNSTATE MEDICAL CENTER 1 DEFINITIONS Patient Safety v is a process that guards against any adverse condition
PATIENT SAFETY OVERVIEW MUHAMMAD ISLAM, MBBS, MS, MCH, LSSBB DIRECTOR OF PATIENT SAFETY SUNY DOWNSTATE MEDICAL CENTER 1 DEFINITIONS Patient Safety v is a process that guards against any adverse condition
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Assessing Medical Technology- Are We Being Told the Truth. The Case of CPOE. David C Classen M.D., M.S. FCG and University of Utah
 Assessing Medical Technology- Are We Being Told the Truth. The Case of CPOE David C Classen M.D., M.S. FCG and University of Utah August 21, 2007 FCG 2006 Slide 1 November 2006 CPOE Adoption Growing Despite
Assessing Medical Technology- Are We Being Told the Truth. The Case of CPOE David C Classen M.D., M.S. FCG and University of Utah August 21, 2007 FCG 2006 Slide 1 November 2006 CPOE Adoption Growing Despite
Disclosure. Institute of Medicine (IOM) 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL
 1,2. Objectives 5/15/2014. Technician Education Day May 24, 2014 Ft. Lauderdale, FL") Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
Technician Education Day May 24, 2014 Ft. Lauderdale, FL The Pharmacy Technician s Role in Keeping Our Patients Safe Antonia Zapantis, MS, PharmD, BCPS Associate Professor, Nova Southeastern University
PHARMACY SERVICES/MEDICATION USE
 25.01. 10 Drug Reactions & Administration Errors & Incompatibilities. Drug administration errors, adverse drug reactions and incompatibilities must be immediately reported to the attending physician and
25.01. 10 Drug Reactions & Administration Errors & Incompatibilities. Drug administration errors, adverse drug reactions and incompatibilities must be immediately reported to the attending physician and
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
SHRI GURU RAM RAI INSTITUTE OF TECHNOLOGY AND SCIENCE MEDICATION ERRORS
 MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
PATIENT SAFETY OVERVIEW
 PATIENT SAFETY OVERVIEW MUHAMMAD ISLAM, MBBS, MS, MCH DIRECTOR OF PATIENT SAFETY SUNY DOWNSTATE MEDICAL CENTER 1 DEFINITIONS Patient Safety is a process that guards against any adverse condition occurring
PATIENT SAFETY OVERVIEW MUHAMMAD ISLAM, MBBS, MS, MCH DIRECTOR OF PATIENT SAFETY SUNY DOWNSTATE MEDICAL CENTER 1 DEFINITIONS Patient Safety is a process that guards against any adverse condition occurring
9/27/2017. Getting on the Path to Excellence. The path we are taking today! CMS Five Elements
 Getting on the Path to Excellence QAPI DESIGN AND IMPLEMENTATION Demi Haffenreffer, RN, MBA www.consultdemi.net The path we are taking today! The requirements at F944 (formerly F520) Key elements Survey
Getting on the Path to Excellence QAPI DESIGN AND IMPLEMENTATION Demi Haffenreffer, RN, MBA www.consultdemi.net The path we are taking today! The requirements at F944 (formerly F520) Key elements Survey
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE)
") COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
Guidelines for Disclosure Process. 1) Patient disclosure does not include:
 Patient disclosure does not include:") Disclosing Serious Unanticipated Adverse Events Educational Guidelines for Washington University Physicians Adopted: June 21, 2007 Amended: March 18, 2008 Timely, honest and sustained communication with
Disclosing Serious Unanticipated Adverse Events Educational Guidelines for Washington University Physicians Adopted: June 21, 2007 Amended: March 18, 2008 Timely, honest and sustained communication with
Fostering a Culture of Safety
 Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Joint Commission Update for Ambulatory Clinics
 Joint Commission Update for Ambulatory Clinics Mary Beth McLellan, RN, BSN Manager of Clinical Operations Rapid City Regional Hospital Family Medicine Residency Program Objectives: Participants will understand
Joint Commission Update for Ambulatory Clinics Mary Beth McLellan, RN, BSN Manager of Clinical Operations Rapid City Regional Hospital Family Medicine Residency Program Objectives: Participants will understand
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
NERC Improving Human Performance
 NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator
 Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator Presented at Webex Conferences: July 20, 21, & 22, 2010 Blood Sample Labeling Seminar 6255 West Sunset Blvd Los Angeles, CA Blood
Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator Presented at Webex Conferences: July 20, 21, & 22, 2010 Blood Sample Labeling Seminar 6255 West Sunset Blvd Los Angeles, CA Blood
Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals
 Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals John M. Kessler, B.S. Pharm., Pharm. D. Steve C. Dedrick, MS Pharm. NCCMedS Project Directors
Assessing and improving the use of near-miss reporting to prevent adverse events and errors in rural hospitals John M. Kessler, B.S. Pharm., Pharm. D. Steve C. Dedrick, MS Pharm. NCCMedS Project Directors
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
QAPI: Systematic Analysis and Systemic Action via Plan-Do-Study-Act Cycles. Objectives QAPI. Regulatory Phases
 QAPI: Systematic Analysis and Systemic Action via Plan-Do-Study-Act Cycles Emily Nelson and Diane Dohm MetaStar/Lake Superior Quality Innovation Network Objectives Obtain a high-level overview of QAPI
QAPI: Systematic Analysis and Systemic Action via Plan-Do-Study-Act Cycles Emily Nelson and Diane Dohm MetaStar/Lake Superior Quality Innovation Network Objectives Obtain a high-level overview of QAPI
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
ADMINISTRATIVE POLICY & PROCEDURE PATIENT SAFETY PLAN
 PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
Anatomy of a Fatal Medication Error
 Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
2018 LEAPFROG HOSPITAL SURVEY ORGANIZATIONAL BINDER
 2018 LEAPFROG HOSPITAL SURVEY ORGANIZATIONAL BINDER TABLE OF CONTENTS Section # Tab # Overview 1 Section 1: Basic Hospital Information 2 Section 2: Medication Safety CPOE 3 Section 3: Inpatient Surgery
2018 LEAPFROG HOSPITAL SURVEY ORGANIZATIONAL BINDER TABLE OF CONTENTS Section # Tab # Overview 1 Section 1: Basic Hospital Information 2 Section 2: Medication Safety CPOE 3 Section 3: Inpatient Surgery
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS
 PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS Active Error An error that occurs at the point of contact. Active errors are generally readily apparent (e.g., pushing an incorrect button, ignoring
PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS Active Error An error that occurs at the point of contact. Active errors are generally readily apparent (e.g., pushing an incorrect button, ignoring
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA
 Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Objective: To practice quality improvement tools by applying them to an improvement effort in an ambulatory care setting.
 Exercise 1 Objective: To practice quality improvement tools by applying them to an improvement effort in an ambulatory care setting. 1. Read the following case study. 2. Follow the instructions at the
Exercise 1 Objective: To practice quality improvement tools by applying them to an improvement effort in an ambulatory care setting. 1. Read the following case study. 2. Follow the instructions at the
Sentinel Events and S Patient Patient entinel Event Alerts Safety Act Safety Ac Revised: BW/September 2010
 Sentinel Events Sentinel Events and Sentinel Event Alerts Revised: BW/September 2010 Patient Patient Safety Safety Act Act What is a Sentinel Event? 0 A sentinel event is an unexpected occurrence involving
Sentinel Events Sentinel Events and Sentinel Event Alerts Revised: BW/September 2010 Patient Patient Safety Safety Act Act What is a Sentinel Event? 0 A sentinel event is an unexpected occurrence involving
Various Views on Adverse Events: a collection of definitions.
 Various Views on Adverse Events: a collection of definitions. April 20, 2008 Werner CEUSTERS a,1, Maria CAPOLUPO b, Georges DE MOOR c, Jos DEVLIES c a New York State Center of Excellence in Bioinformatics
Various Views on Adverse Events: a collection of definitions. April 20, 2008 Werner CEUSTERS a,1, Maria CAPOLUPO b, Georges DE MOOR c, Jos DEVLIES c a New York State Center of Excellence in Bioinformatics
Overview of the Leapfrog CPOE Evaluation Tool. An educational update to the HIMSS EIS Steering Committee August 13, 2009
 Overview of the Leapfrog CPOE Evaluation Tool An educational update to the HIMSS EIS Steering Committee August 13, 2009 1 Overview What is the CPOE Evaluation Tool? Development of the Tool Why is Tool
Overview of the Leapfrog CPOE Evaluation Tool An educational update to the HIMSS EIS Steering Committee August 13, 2009 1 Overview What is the CPOE Evaluation Tool? Development of the Tool Why is Tool
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
National Patient Safety Goals & Quality Measures CY 2017
 National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
The Leapfrog Hospital Survey Scoring Algorithms. Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey
 The Leapfrog Hospital Survey Scoring Algorithms Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey 2017 Leapfrog Hospital Survey Scoring Algorithms Table of Contents 2017 Leapfrog Hospital
The Leapfrog Hospital Survey Scoring Algorithms Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey 2017 Leapfrog Hospital Survey Scoring Algorithms Table of Contents 2017 Leapfrog Hospital
February New Zealand Health and Disability Services National Reportable Events Policy 2012
 February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
Care of the Caregiver STARTS and ENDS with full leadership support and involvement!
 Care of the Caregiver STARTS and ENDS with full leadership support and involvement! Care of the caregiver following an unintentional error or near miss should ideally incorporate: Unsafe Acts Algorithm
Care of the Caregiver STARTS and ENDS with full leadership support and involvement! Care of the caregiver following an unintentional error or near miss should ideally incorporate: Unsafe Acts Algorithm
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that
 Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Thanks to Anne C. Byrne, RN, Medical Monitor at Northwest Georgia Regional Hospital. This presentation was developed from one she designed for that hospital. 1 2 3 Note that an actual variance occurs when
Building a Safe Healthcare System
 Building a Safe Healthcare System Objectives 2 Discuss the process of improving healthcare systems. Introduce widely-used methodologies in QI/PS. What is Quality Improvement? 3 Process of continually evaluating
Building a Safe Healthcare System Objectives 2 Discuss the process of improving healthcare systems. Introduce widely-used methodologies in QI/PS. What is Quality Improvement? 3 Process of continually evaluating
3/24/2016. Value of Quality Management. Quality Management in Senior Housing: Back to the Basics. Objectives. Defining Quality
 Quality Management in Senior Housing: Back to the Basics Lisa Abicht-Swensen, M.H.A. Director of Home Health, Hospice and Assisted Living Services Objectives Understand the value of Quality Management
Quality Management in Senior Housing: Back to the Basics Lisa Abicht-Swensen, M.H.A. Director of Home Health, Hospice and Assisted Living Services Objectives Understand the value of Quality Management
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
HealthStream Ambulatory Regulatory Course Descriptions
 This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
Kupu Taurangi Hauora o Aotearoa
 Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
Health Management Information Systems: Computerized Provider Order Entry
 Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
National Patient Safety Goals from The Joint Commission
 National Patient Safety Goals from The Joint Commission Objectives After completion of this module, participants will be able to: List at least five National Patient Safety Goals that are required in a
National Patient Safety Goals from The Joint Commission Objectives After completion of this module, participants will be able to: List at least five National Patient Safety Goals that are required in a
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
TIME OUT! A Patient Safety Strategy. Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service
 TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
N ATIONAL Q UALITY F ORUM. Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT
 N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
Accreditation Program: Long Term Care
 ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference
 Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference INGA AIKMAN, MD, MPH PEDIATRIC CHIEF RESIDENT EAST CAROLINA UNIVERSITY Second Annual REACH Medical
Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference INGA AIKMAN, MD, MPH PEDIATRIC CHIEF RESIDENT EAST CAROLINA UNIVERSITY Second Annual REACH Medical
WPSC Teleconference Avoiding Never Events. Linda Furkay, PhD, RN Patient Safety Adverse Event Officer
 Linda Furkay, PhD, RN Patient Safety Adverse Event Officer Share Findings from adverse events surgical errors, pressure ulcers, & falls Successful patient safety strategies here in Washington & from other
Linda Furkay, PhD, RN Patient Safety Adverse Event Officer Share Findings from adverse events surgical errors, pressure ulcers, & falls Successful patient safety strategies here in Washington & from other
Go for the Gold. Incorporating Regulatory Issues into the Quality Management Process. June 9 11, 2008 Starr Pass Resort Tucson, Arizona
 Go for the Gold June 9 11, 2008 Starr Pass Resort Tucson, Arizona Incorporating Regulatory Issues into the Quality Management Process Recent regulatory changes have impacted the traditional hospital Quality
Go for the Gold June 9 11, 2008 Starr Pass Resort Tucson, Arizona Incorporating Regulatory Issues into the Quality Management Process Recent regulatory changes have impacted the traditional hospital Quality
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
Medication Reconciliation: Preventing Errors and Improving Patient Outcomes
 Murray State's Digital Commons Scholars Week 2016 - Spring Scholars Week Apr 18th, 12:00 PM - 2:00 PM Medication Reconciliation: Preventing Errors and Improving Patient Outcomes Amanda S. Boren Murray
Murray State's Digital Commons Scholars Week 2016 - Spring Scholars Week Apr 18th, 12:00 PM - 2:00 PM Medication Reconciliation: Preventing Errors and Improving Patient Outcomes Amanda S. Boren Murray
The Patient Safety Act Reporting and RCA Requirements
 The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
Safe medication practice what can we learn from root cause analysis and related methods?
 Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Quality Improvement/Systems-based Practice. Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery
 Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
Quality Management and Accreditation
 Quality Management and Accreditation Lina Mekawi, RPh, MS Epidemiology, CPHQ, Senior Quality Analyst, Quality, Accreditation and Risk Management Department, AUBMC November 2017 Disclosure Slide I, Lina
Quality Management and Accreditation Lina Mekawi, RPh, MS Epidemiology, CPHQ, Senior Quality Analyst, Quality, Accreditation and Risk Management Department, AUBMC November 2017 Disclosure Slide I, Lina
The Joint Commission Medication Management Update for 2010
 Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow
 The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
Leadership and Culture: Building Highly Reliable Systems of Care
 Learning Objectives Leadership and Culture: Building Highly Reliable Systems of Care Michael Batchelor, CEO Baptist Easley Hospital Easley, South Carolina Discuss recent developments in health systems
Learning Objectives Leadership and Culture: Building Highly Reliable Systems of Care Michael Batchelor, CEO Baptist Easley Hospital Easley, South Carolina Discuss recent developments in health systems
A23/B23: Patient Harm in US Hospitals: How Much? Objectives
 A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
Patient Safety Incident Report Form
 Page 1 This form is not meant to be a substitute to the health region s incident reporting. The purpose of this form is to assist with the identification and management of adverse events and near misses;
Page 1 This form is not meant to be a substitute to the health region s incident reporting. The purpose of this form is to assist with the identification and management of adverse events and near misses;
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Designing for Safety
 2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
Directing and Controlling
 NUR 462 Principles of Nursing Administration Directing and Controlling (Leibler: Chapter 7) Dr. Ibtihal Almakhzoomy March 2007 Dr. Ibtihal Almakhzoomy Directing and Controlling Define the management function
NUR 462 Principles of Nursing Administration Directing and Controlling (Leibler: Chapter 7) Dr. Ibtihal Almakhzoomy March 2007 Dr. Ibtihal Almakhzoomy Directing and Controlling Define the management function
Take ACTION: A Collaborative Approach to Creating a Culture of Safety
 Take ACTION: A Collaborative Approach to Creating a Culture of Safety Heidi Boehm, MSN, RN-BC, Unit Educator Steven P. Kellar, BSN, RN, Unit Educator Joann L. Moore, RPh, Medication Safety Coordinator
Take ACTION: A Collaborative Approach to Creating a Culture of Safety Heidi Boehm, MSN, RN-BC, Unit Educator Steven P. Kellar, BSN, RN, Unit Educator Joann L. Moore, RPh, Medication Safety Coordinator
(10+ years since IOM)
") Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Meeting Joint Commission Standards for Health Literacy. Communication and Health Care. Multiple Players in Communication
 Meeting Joint Commission Standards for Health Literacy Christina L. Cordero, PhD, MPH Project Manager Division of Standards and Survey Methods The Joint Commission Wisconsin Literacy SW/SC Regional Health
Meeting Joint Commission Standards for Health Literacy Christina L. Cordero, PhD, MPH Project Manager Division of Standards and Survey Methods The Joint Commission Wisconsin Literacy SW/SC Regional Health
A 21 st Century System of Patient Safety and Medical Injury Compensation
 A 21 st Century System of Patient Safety and Medical Injury Compensation Overview Our goal is to promote patient safety and reduce preventable errors and injuries. We want to replace our fault-based medical
A 21 st Century System of Patient Safety and Medical Injury Compensation Overview Our goal is to promote patient safety and reduce preventable errors and injuries. We want to replace our fault-based medical
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor
 Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Lesson 9: Medication Errors
 Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
What Every Patient Safety Officer Must Know:
 What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Focus on Diagnostic Errors: Understanding and Prevention
 Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
Focus on Diagnostic Errors: Understanding and Prevention Tejal Gandhi, MD MPH CPPS President, National Patient Safety Foundation Associate Professor, Harvard Medical School Thanks to Dr. Mark Graber for
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm
 Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
University of Washington School of Nursing - Continuing Nursing Education 1
 A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
Reporting and Disclosing Adverse Events
 Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
The Multidisciplinary aspects of JCI accreditation
 The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
The Multidisciplinary aspects of JCI accreditation Saleem Kiblawi MD, FCCP, Physician consultant, Joint Commission International Oakbrook, Illinois USA Lebanese American University April 15, 2016 Beirut,
Sign up to Safety Drivers and Measurement
 Sign up to Safety Drivers and Measurement Expert Partner Nicola Davey Topics for today Driver diagrams Linking improvement aims to strategic objectives Generating simple improvement measures Measures
Sign up to Safety Drivers and Measurement Expert Partner Nicola Davey Topics for today Driver diagrams Linking improvement aims to strategic objectives Generating simple improvement measures Measures
The Power of Quality. Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center
 The Power of Quality Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center What do you think of when you hear the word quality? LEAN RCA PDSA QAPI SIX SIGMA PIP TQM 5s Objectives Transplant
The Power of Quality Lindsay R. Smith, MSN,RN Quality Manager Vanderbilt Transplant Center What do you think of when you hear the word quality? LEAN RCA PDSA QAPI SIX SIGMA PIP TQM 5s Objectives Transplant