90% of seniors surveyed want to age in their own homes yet adequate home-based and community-based services are limited in most communities.
|
|
|
- Barbara McCoy
- 5 years ago
- Views:
Transcription


1 Dr. Allan Chip Teel

2 90% of seniors surveyed want to age in their own homes yet adequate home-based and community-based services are limited in most communities.

3 53% admitted to a nursing home died in 6 months; the median survival for males was only 3 months! (Journal of American Geriatrics Society )

4 Among elders needing care: 60% live in their own homes, 31% live with family or close friends, 5% live in nursing homes, and 4% live in assisted living (AARP)

5 Loneliness among elders increased functional decline by 59% and rate of death by 45%. ( Archives of Internal Medicine June 18, 2012)

6 60% of all nursing home residents NEVER have a visitor.

7 LIVING LONGER. WHO PAYS? Senior Actuarial Table (Fidelity Investments)


8 Monthly Costs FCA Package Includes $350- FCA Tech Support $800- Rent Mortgage $750- Personal Care $200-Food $250- Utilities $160-Nursing
9 The Elder Cost Cascade 30MM annual US ER visits are people over 65 Average Cost of these ED visits is $2168 Half of >65 year-olds in ED admitted to Hospital Average Length of Stay in Hospital for >65 is 5.4 days at $2100/day 40% of >85yo and 30% of all hospitalized Medicare patients go to SNF Average Stay in SNF is 29 days at $423/day NH admissions at $83400/yr: 1/3 from hospital, 1/3 from SNFs/ ALFs, and 1/3 from home Congressional Medical Advisory Group estimates 60% of ED visits and 25% admissions unnecessary if more home-based services available. FCA Program total healthcare systems savings estimated at 40%.
 4.")
10 Medication Reminders 76% 37% 59% 22% 10% 23% 66% Americans age 60+ use two or more prescription medications Americans age 60+ use five or more prescription medications On five or more medications per day take them improperly. Americans take less medication than prescribed Of hospital admissions are due to failure to take prescribed medications (avg. length of stay) 4.2 days Of NF admissions due to noncompliance The likelihood of increased drug discontinuation after a pill-shape change. (34% after a pill-color change)
11





12 Full Circle America Dr. Chip Teel At Home Support with Social Connections People Empowered members. Doing for others. Circle of Caring. Reconfigured resources. Attitude Goals and aspirations. Dignity of Risk. Family, pets, interests. Purposeful living. Technology Tools. Easy to use. Affordable. Access. Making connections. Reducing loneliness.


13 The Dignity of Risk We must give everyone the opportunity to live a full and rich life. With living comes risk. With success or failure comes growth. Take away risk and take away the chance to live a full life.

14 The Health Benefits of Volunteering Provides a sense of purpose Lowers mortality rates by 1/3 to 1/2 2/3 less likely to report bad health Lowers depression Less heart disease Less functional decline Benefits last more than a decade More effective than medical care

15 Full Circle America Building the Stay at Home Network around You We help you age at home with a High Tech, High Touch approach to elder care. Using available community resources, including family, friends and technology, we build a network of support around our members. Remote Monitoring Virtual Check Ins 24/7 Family Access Social Networking Peer-2-Peer Calling Community Outings Companion Visits Video Calling Medical Support Home Health Personnel Virtual House Calls Hospital At-Home PCPs/PCMH/Hospital/SNF Support Services Shopping/Errands/Transportation Home Modification/Repairs Meals/Housekeeping Adaptive Devices Call Button Quick Call to FCA 24/7 On Call Full Circle America MEMBER Physical and Mental Health Exercise Entertainment Education Companionship Chronic Disease Management BP/ Weight/ O2 Sat / Peak Flow Diet/ Exercise Full Circle America 2014

16






17 FULL CIRCLE AMERICA: CHRONIC CARE KIT Talking Scale Medication Reminder Blood Pressure Cuff Pulse Oximeter Peak Flow Meter Pedometer/ FM Radio
18
19

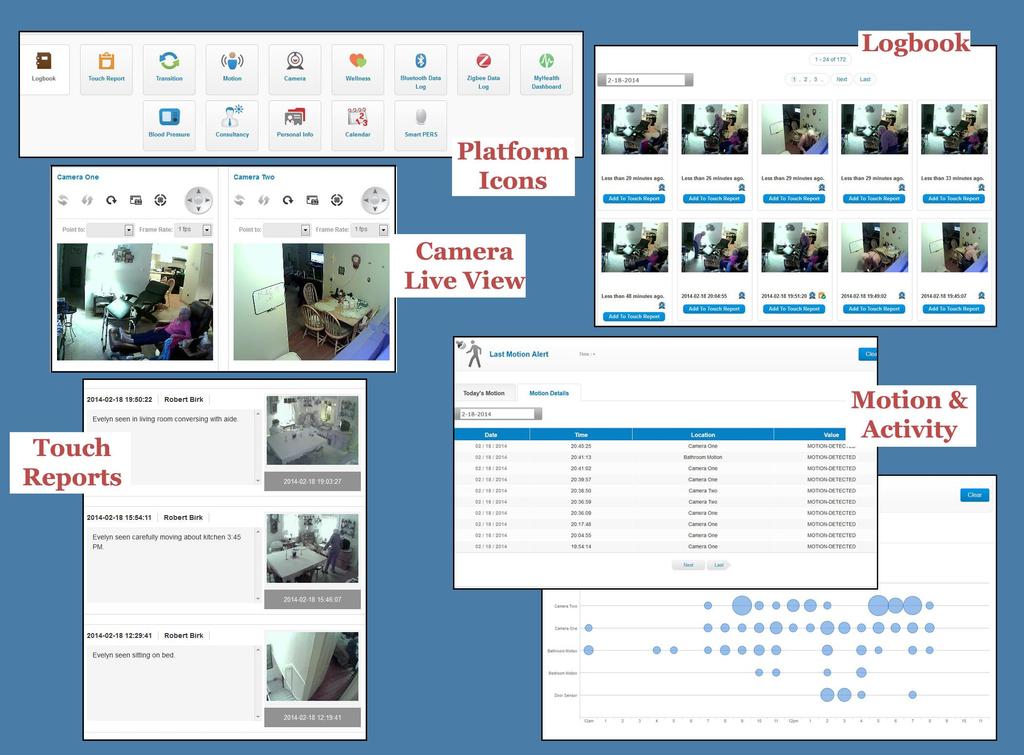
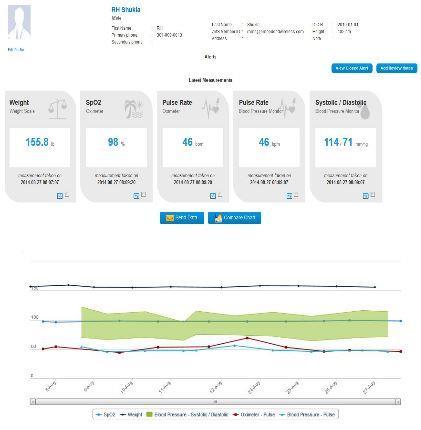
20 Chronic Care/ Telemedicine Visits Video House Calls from your Health Care Team Encrypted data, secure connections, and HIPPA compliance of all patient data Daily vital sign collection supported by phone calls and video Simple medical devices for you and your physician to manage your chronic care Medication reminders by phone or programmed pillbox Caregiver app for quick communication between FCA and your family & care team Web-based 'Circle of Caring' logbook with alerts and data displays

21

22

23 Flannel Inn Helen Ed Elizabeth Anne Ginny and Neil
24 Readmissions Highest w/ Fragile Support Systems Issues With Housing No Transportation for Follow-up Care Did not Pick up Prescriptions Limited Support Lack of Person-Centered Care Plan Lack of Patient Involvement in Self Management No Family Involvement in Transition Low Health IQ Lack of Social Services for Chronic Medical and Mental Health Poor Care Transitions/ Poor Communications Poor Medication Reconciliation 20% MEDICARE PATIENTS READMITTED <30 DAYS COSTING $28B/ YEAR
25 Translating FCA Model into $avings High Utilizers Consume Most of Services: 6 ED visits/pp/yr = $ Hospitalizations = $ SNF days = $19035 Current Spend $66063 FCA projects >40% Reduction 2 less ED visits = $ less hospitalization & 1 shorter one =$ less SNF days = $10575 Projected Savings: $30451 pp/yr
26 Full Circle America PO Box 484 Damariscotta, Maine
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
Transitions of Care. Scott Clark, President Leading Edge Health Care
 Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
How 2018 Will Be The Year You Embrace Continuous Connectivity. NERSI NAZARI, PHD Chief Executive Officer
 How 2018 Will Be The Year You Embrace Continuous Connectivity NERSI NAZARI, PHD Chief Executive Officer WE ARE CONTINUOUSLY CONNECTED Socially Friends and community Financially Balances and bills Parenting
How 2018 Will Be The Year You Embrace Continuous Connectivity NERSI NAZARI, PHD Chief Executive Officer WE ARE CONTINUOUSLY CONNECTED Socially Friends and community Financially Balances and bills Parenting
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM
 ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM Objectives Understand the needs/goals that the Community Paramedic program was designed to address Understand how Abbeville County implemented
ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM Objectives Understand the needs/goals that the Community Paramedic program was designed to address Understand how Abbeville County implemented
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM
 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
PROVIDER & PATIENT. Communication Guide CULTURAL COMPETENCY COALITION. QB C3 Provider and Patient Communication Guide Document Date: 05/27/2016
 QB 2021 - C3 Provider and Patient Communication Guide Document Date: 05/27/2016 PROVIDER & PATIENT Communication Guide CULTURAL COMPETENCY COALITION All health care organizations that receive federal funds
QB 2021 - C3 Provider and Patient Communication Guide Document Date: 05/27/2016 PROVIDER & PATIENT Communication Guide CULTURAL COMPETENCY COALITION All health care organizations that receive federal funds
August 25, Dear Acting Administrator Slavitt:
 August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
O n e o n O n e C a r e
 One on One Care Our Care, Your Peace of Mind.O O n e o n O n e C a r e Our Care, Your Peace of Mind. The One on One Care Home Franchise Investing In Your Future! In US history, there have never been such
One on One Care Our Care, Your Peace of Mind.O O n e o n O n e C a r e Our Care, Your Peace of Mind. The One on One Care Home Franchise Investing In Your Future! In US history, there have never been such
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Driving Business Value for Healthcare Through Unified Communications
 Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care
 Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care Geriatric Day Hospitals Institute Sunnybrook Health Science Centre November 25, 2013 Liana Sikharulidze,
Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care Geriatric Day Hospitals Institute Sunnybrook Health Science Centre November 25, 2013 Liana Sikharulidze,
Breaking Down Barriers to Care Pamela Crider, MSN, CNP Christine Karpen, MSW, LSW. MetroHealth Medical Center
 Breaking Down Barriers to Care Pamela Crider, MSN, CNP Christine Karpen, MSW, LSW MetroHealth Medical Center Goals: Improved Outcomes Better patient experience Improved Communication Ease of access Lower
Breaking Down Barriers to Care Pamela Crider, MSN, CNP Christine Karpen, MSW, LSW MetroHealth Medical Center Goals: Improved Outcomes Better patient experience Improved Communication Ease of access Lower
Reducing Hospital Re-Admissions with Telemedicine & Medication Reconciliation The prescription for improved patient outcomes
 Reducing Hospital Re-Admissions with Telemedicine & Medication Reconciliation The prescription for improved patient outcomes Download the presentation at RxConcile.com or asaging.org Who we are Chad Worz
Reducing Hospital Re-Admissions with Telemedicine & Medication Reconciliation The prescription for improved patient outcomes Download the presentation at RxConcile.com or asaging.org Who we are Chad Worz
Test bank PowerPoint slides for each chapter Instructor guides for each chapter (with answers for discussion questions and case studies)
") This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
Use Case Study: Remote Patient Monitoring for Chronic Disease
 Use Case Study: Remote Patient Monitoring for Chronic Disease Hackensack Alliance Accountable Care Organization New Jersey March 2014 The Hackensack Alliance Accountable Care Organization (ACO) was established
Use Case Study: Remote Patient Monitoring for Chronic Disease Hackensack Alliance Accountable Care Organization New Jersey March 2014 The Hackensack Alliance Accountable Care Organization (ACO) was established
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Telehealth. January 7, 2016
 Telehealth January 7, 2016 Frances Gough, MD, Chief Medical Officer Molina Healthcare of Washington Co-Chair ATA Standard and Guidelines Committee for Primary and Urgent Care Telemedicine: The use of medical
Telehealth January 7, 2016 Frances Gough, MD, Chief Medical Officer Molina Healthcare of Washington Co-Chair ATA Standard and Guidelines Committee for Primary and Urgent Care Telemedicine: The use of medical
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Telehealthcare: Current Role and Future Challenges
 Telehealthcare: Current Role and Future Challenges Frances S Mair Professor of Primary Care Research Section of General Practice and Primary Care (Division of Community Based Sciences) University of Glasgow
Telehealthcare: Current Role and Future Challenges Frances S Mair Professor of Primary Care Research Section of General Practice and Primary Care (Division of Community Based Sciences) University of Glasgow
Drs Whittle, Scott, Bevz & Fairhead. Health & Social Care Act 2008
 Drs Whittle, Scott, Bevz & Fairhead Cleveleys Group Practice Health & Social Care Act 2008 Version 1 - August 2013 Version 2 - December 2015 Date of Next Review: December 2016 Service Provider Details
Drs Whittle, Scott, Bevz & Fairhead Cleveleys Group Practice Health & Social Care Act 2008 Version 1 - August 2013 Version 2 - December 2015 Date of Next Review: December 2016 Service Provider Details
Quality on the Frontlines: Coordinating Care Across Sectors and Achieving Better Outcomes
 Quality on the Frontlines: Coordinating Care Across Sectors and Achieving Better Outcomes Presenter Disclosures Moderator: Dr. Walter Wodchis Presenters: o Jocelyn Bennett o Mark Fam, Tory Merritt o Dr.
Quality on the Frontlines: Coordinating Care Across Sectors and Achieving Better Outcomes Presenter Disclosures Moderator: Dr. Walter Wodchis Presenters: o Jocelyn Bennett o Mark Fam, Tory Merritt o Dr.
4. If needed Add a home medication, right mouse click over a medication and Modify or Cancel/Dc medications that are inaccurate.
 How to Admit a Patient 1. Please communicate to the ER Unit Secretary to Move the patient in the Cerner system to the Overflow Location. A bed request order needs to be initiated by the ED doctor. 4. If
How to Admit a Patient 1. Please communicate to the ER Unit Secretary to Move the patient in the Cerner system to the Overflow Location. A bed request order needs to be initiated by the ED doctor. 4. If
THE CASE FOR CARE IN THE HOME: MAKING LIVES BETTER IN THE BEST, MOST AFFORDABLE WAY
 THE CASE FOR CARE IN THE HOME: MAKING LIVES BETTER IN THE BEST, MOST AFFORDABLE WAY Nine years of net rate cuts for home health has resulted in providers now receiving 86 cents on the dollar compared with
THE CASE FOR CARE IN THE HOME: MAKING LIVES BETTER IN THE BEST, MOST AFFORDABLE WAY Nine years of net rate cuts for home health has resulted in providers now receiving 86 cents on the dollar compared with
The MARYLAND HEALTH CARE COMMISSION
 The MARYLAND HEALTH CARE COMMISSION Our Role The MHCC is responsible to advance a strong, flexible health IT ecosystem that can appropriately support clinical decision-making, reduce redundancy, enable
The MARYLAND HEALTH CARE COMMISSION Our Role The MHCC is responsible to advance a strong, flexible health IT ecosystem that can appropriately support clinical decision-making, reduce redundancy, enable
Telehealth for Acute and Urgent Care
 Telehealth for Acute and Urgent Care the Andrew Waring, Consultant, Serengeti Projects Ltd Agenda Individual and workshop introductions and objectives Benefits Chronic Telehealth Benefits Acute and Urgent
Telehealth for Acute and Urgent Care the Andrew Waring, Consultant, Serengeti Projects Ltd Agenda Individual and workshop introductions and objectives Benefits Chronic Telehealth Benefits Acute and Urgent
Hot Spotter Report User Guide
 PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
CMS Mandated Training
 CMS Mandated Training Brand New Day Models of Care PRINT Your Name: SIGN Your Name: Print Today s Date: F:\QM\COMPLIANCE\COMPLIANCE TRAINING\MOC\BRAND NEW DAY MOC TRAINING.docx Brand New Day Medicare Mandated
CMS Mandated Training Brand New Day Models of Care PRINT Your Name: SIGN Your Name: Print Today s Date: F:\QM\COMPLIANCE\COMPLIANCE TRAINING\MOC\BRAND NEW DAY MOC TRAINING.docx Brand New Day Medicare Mandated
Community Data Update Knoxville Community Readmissions Coalition January 25 th, 2018
 Community Data Update Knoxville Community Readmissions Coalition January 25 th, 2018 Corley Roberts, MHA, CPHQ, ACSM EP-C, EIM Quality Improvement Advisor, Qsource/atom Alliance croberts@qsource.org Readmissions
Community Data Update Knoxville Community Readmissions Coalition January 25 th, 2018 Corley Roberts, MHA, CPHQ, ACSM EP-C, EIM Quality Improvement Advisor, Qsource/atom Alliance croberts@qsource.org Readmissions
Verdien av egengenerert helsedata. Oslo, Tor Jakob Ramsøy
 Verdien av egengenerert helsedata Oslo, 1.9.2015 Tor Jakob Ramsøy torjakob@arundo.com 0 Patient Generated Data is not new, but has taken on a much bigger role in this new era of data abundance and ubiquitous
Verdien av egengenerert helsedata Oslo, 1.9.2015 Tor Jakob Ramsøy torjakob@arundo.com 0 Patient Generated Data is not new, but has taken on a much bigger role in this new era of data abundance and ubiquitous
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Qualcomm Life, VRI and Tri-City Medical Center Collaborate to Reduce Hospital Readmissions
 For Immediate Release 12/04/2012 Tri-City Medical Center Contact: Tarcy Connors, Media Relations Director Phone: 1-760-940-5794 Email: ConnorsTR@TCMC.com Qualcomm Contacts: Emily Kilpatrick, Corporate
For Immediate Release 12/04/2012 Tri-City Medical Center Contact: Tarcy Connors, Media Relations Director Phone: 1-760-940-5794 Email: ConnorsTR@TCMC.com Qualcomm Contacts: Emily Kilpatrick, Corporate
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
CHF Education March Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN
 CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
PRIMARY PARTNERS, LLC. Our Journey with the State HIE
 PRIMARY PARTNERS, LLC Our Journey with the State HIE About Us As a 2012 starter, Primary Partners was one of the 1 st Medicare ACO s in the country Our 2 nd Medicare ACO was formed in 2013 In late 2014
PRIMARY PARTNERS, LLC Our Journey with the State HIE About Us As a 2012 starter, Primary Partners was one of the 1 st Medicare ACO s in the country Our 2 nd Medicare ACO was formed in 2013 In late 2014
Vision 2025: What Might Health Care Look Like a Decade from Now?
 Vision 2025: What Might Health Care Look Like a Decade from Now? Value-based care, coordinated care, information technology integration... healthcare is undergoing transformation. Sweeping changes are
Vision 2025: What Might Health Care Look Like a Decade from Now? Value-based care, coordinated care, information technology integration... healthcare is undergoing transformation. Sweeping changes are
4/8/2016. Remote Monitoring & Patient Coaching. Improving Outcomes and Reducing Costs. Objectives. What is RPM?
 Remote Monitoring & Patient Coaching Improving Outcomes and Reducing Costs Objectives Illustrate what Remote Patient Monitoring is. Highlight CBI s pioneering initiatives as it relates to RPM. Illustrate
Remote Monitoring & Patient Coaching Improving Outcomes and Reducing Costs Objectives Illustrate what Remote Patient Monitoring is. Highlight CBI s pioneering initiatives as it relates to RPM. Illustrate
Defying Distance: How Unified Communications Is Transforming Health Care
 Defying Distance: How Unified Communications Is Transforming Health Care The business of healthcare today is shifting away from the traditional fee- for- service model, towards a more holistic approach:
Defying Distance: How Unified Communications Is Transforming Health Care The business of healthcare today is shifting away from the traditional fee- for- service model, towards a more holistic approach:
Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1)
") Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1) Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Professor and Chair Titus Family Department of Clinical
Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1) Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Professor and Chair Titus Family Department of Clinical
THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON
 THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations
THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Boulder County Care Transitions Collaborative Age Well Conference
 Boulder County Care Transitions Collaborative 2016 Age Well Conference What is BCCTC Boulder County Care Transitions Collaborative started March 2012 CMS Grant Goal to reduce Readmission in Boulder County
Boulder County Care Transitions Collaborative 2016 Age Well Conference What is BCCTC Boulder County Care Transitions Collaborative started March 2012 CMS Grant Goal to reduce Readmission in Boulder County
Community Paramedicine: Lessons Learned from South Carolina
 Community Paramedicine: Lessons Learned from South Carolina Dr. Chris Oxendine, CP Medical Director Abbeville Area Medical Center Will Blackwell Abbeville County EMS Sarah M. Craig, MHA South Carolina
Community Paramedicine: Lessons Learned from South Carolina Dr. Chris Oxendine, CP Medical Director Abbeville Area Medical Center Will Blackwell Abbeville County EMS Sarah M. Craig, MHA South Carolina
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Looking Ahead: The Future of American Health Care. Ezekiel J. Emanuel, M.D., Ph.D.
 Looking Ahead: The Future of American Health Care Ezekiel J. Emanuel, M.D., Ph.D. US Health Care Spending (2016) $3.4 Trillion Rx for Cost Cutting GDP (nominal) in 2016 Rank USA $18.57 trillion #1 CHINA
Looking Ahead: The Future of American Health Care Ezekiel J. Emanuel, M.D., Ph.D. US Health Care Spending (2016) $3.4 Trillion Rx for Cost Cutting GDP (nominal) in 2016 Rank USA $18.57 trillion #1 CHINA
A Care Plan Guide. (Simple Steps To Caring For Your Loved Ones)
") A Care Plan Guide (Simple Steps To Caring For Your Loved Ones) The personal journey as a caretaker can be very rewarding yet overwhelming at times. When we are instantly put into a situation of caring
A Care Plan Guide (Simple Steps To Caring For Your Loved Ones) The personal journey as a caretaker can be very rewarding yet overwhelming at times. When we are instantly put into a situation of caring
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Pharmacist Led Transitions of Care in an Indigent Population JEANNA SEWELL, PHARMD, BCACP CLINICAL ASSISTANT PROFESSOR AUBURN UNIVERSITY HARRISON
 Pharmacist Led Transitions of Care in an Indigent Population JEANNA SEWELL, PHARMD, BCACP CLINICAL ASSISTANT PROFESSOR AUBURN UNIVERSITY HARRISON SCHOOL OF PHARMACY Conflicts of Interest I have no conflicts
Pharmacist Led Transitions of Care in an Indigent Population JEANNA SEWELL, PHARMD, BCACP CLINICAL ASSISTANT PROFESSOR AUBURN UNIVERSITY HARRISON SCHOOL OF PHARMACY Conflicts of Interest I have no conflicts
The Cleveland Super-Utilizer Project: Red Carpet Care
 The Cleveland Super-Utilizer Project: Red Carpet Care Alice Stollenwerk Petrulis, MD The MetroHealth System Cleveland, OH Bernadette Yohe, RN Buckeye Community Health Plan Picture of MH MetroHealth 750
The Cleveland Super-Utilizer Project: Red Carpet Care Alice Stollenwerk Petrulis, MD The MetroHealth System Cleveland, OH Bernadette Yohe, RN Buckeye Community Health Plan Picture of MH MetroHealth 750
Telehealth in Peritoneal Dialysis Patient Management
 Telehealth in Peritoneal Dialysis Patient Management Susie Lew, MD George Washington University March 3, 2018 Disclosures CareFirst Foundation: grant ACT/ The App Association: Steering committee member
Telehealth in Peritoneal Dialysis Patient Management Susie Lew, MD George Washington University March 3, 2018 Disclosures CareFirst Foundation: grant ACT/ The App Association: Steering committee member
AGENDA. QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, /21/2014
 QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, 2014 04 AGENDA Speaker Background Re Admissions Home Health Hospice Economic Incentivized Situations
QUANTIFYING THE THREATS & OPPORTUNITIES UNDER HEALTHCARE REFORM NAHC Annual Meeting Phoenix AZ October 21, 2014 04 AGENDA Speaker Background Re Admissions Home Health Hospice Economic Incentivized Situations
Building Wellness Communities for Chronic Diseases
 A Saviance Technologies Whitepaper Building Wellness Communities for Chronic Diseases The Growing Crisis of Chronic Diseases in the US In the US today, an estimated number of people who are suffering from
A Saviance Technologies Whitepaper Building Wellness Communities for Chronic Diseases The Growing Crisis of Chronic Diseases in the US In the US today, an estimated number of people who are suffering from
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
CONNECTED SM. Blue Care Connection SIMPLY AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT
 SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013
 NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013 1. WHAT EXACTLY IS MEDICATION ADHERENCE? Adhering to medication means taking the medication as directed by a health care professional-
NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013 1. WHAT EXACTLY IS MEDICATION ADHERENCE? Adhering to medication means taking the medication as directed by a health care professional-
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Medication Reconciliation
 Medication Reconciliation The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health Netsmart Technologies Today
Medication Reconciliation The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health Netsmart Technologies Today
VJ Periyakoil Productions presents
 VJ Periyakoil Productions presents Oscar thecare Cat: Advance Lessons Learned Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil,
VJ Periyakoil Productions presents Oscar thecare Cat: Advance Lessons Learned Planning Joan M. Teno, MD, MS Professor of Community Health Warrant Alpert School of Medicine at Brown University VJ Periyakoil,
California s Chronically Ill: Coping with Rising Health Care Costs
 California s Chronically Ill: 2005 Introduction As health plan coverage continues to move towards member cost sharing, particular concern has been raised about the impact of these changes on those with
California s Chronically Ill: 2005 Introduction As health plan coverage continues to move towards member cost sharing, particular concern has been raised about the impact of these changes on those with
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
The Future of Home Health is Here
 The Future of Home Health is Here How Home Health Agencies Can Bridge the Care Gap for ACOs and Hospital Networks The Future of Home Health is Here How Home Health Agencies Can Bridge the Care Gap for
The Future of Home Health is Here How Home Health Agencies Can Bridge the Care Gap for ACOs and Hospital Networks The Future of Home Health is Here How Home Health Agencies Can Bridge the Care Gap for
Smart Personal Health. the state of the art. Chris Johnson Berlin, September 2010
 1 Smart Personal Health Interoperability of personal health systems the state of the art Chris Johnson www.chrisjohnson.nl Berlin, September 2010 2 About your presenter Vice President Cypak since 2007:
1 Smart Personal Health Interoperability of personal health systems the state of the art Chris Johnson www.chrisjohnson.nl Berlin, September 2010 2 About your presenter Vice President Cypak since 2007:
Focus Group results RN Perspective
 Focus Group results RN Perspective Category Themes Communication Patient Condition Communicate Expectations and plan of care Early 1. Communicate to patient at beginning of shift and throughout shift (pain
Focus Group results RN Perspective Category Themes Communication Patient Condition Communicate Expectations and plan of care Early 1. Communicate to patient at beginning of shift and throughout shift (pain
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Instructions and Background on Using the Telehealth ROI Estimator
 Instructions and Background on Using the Telehealth ROI Estimator Introduction: Costs and Benefits How do investments in remote patient monitoring (RPM) devices affect the bottom line? The telehealth ROI
Instructions and Background on Using the Telehealth ROI Estimator Introduction: Costs and Benefits How do investments in remote patient monitoring (RPM) devices affect the bottom line? The telehealth ROI
AARP Foundation Isolation Impact Area. Grant Opportunity. Identifying Outcome/Evidence-Based Isolation Interventions. Request for Proposals
 AARP Foundation Isolation Impact Area Grant Opportunity Identifying Outcome/Evidence-Based Isolation Interventions Request for Proposals Letter of Inquiry Deadline: October 26, 2015 I. AARP Foundation
AARP Foundation Isolation Impact Area Grant Opportunity Identifying Outcome/Evidence-Based Isolation Interventions Request for Proposals Letter of Inquiry Deadline: October 26, 2015 I. AARP Foundation
Bahrain Botswana Egypt Ghana India Jordan Kuwait Mauritius Nigeria Qatar Saudi Arabia Thailand UAE
 TELEHEALTH Prestige Blue Chip,# 9, 4th Floor, 3rd Block, Hosur Road, Near Dairy Circle, Bangalore - 560029 GYS Universal Plot No. - A 3,4,5, Sec. 125 Noida, UP - 201301 P O Box 73030, ED 22, Building 16,
TELEHEALTH Prestige Blue Chip,# 9, 4th Floor, 3rd Block, Hosur Road, Near Dairy Circle, Bangalore - 560029 GYS Universal Plot No. - A 3,4,5, Sec. 125 Noida, UP - 201301 P O Box 73030, ED 22, Building 16,
Naples Internal Medicine Associates
 CASE STUDY Implementing Chronic Care Management to Improve Patient Outcomes The Challenge How to effectively implement a Medicare rule that pays medical providers up to $42 per patient, per month, for
CASE STUDY Implementing Chronic Care Management to Improve Patient Outcomes The Challenge How to effectively implement a Medicare rule that pays medical providers up to $42 per patient, per month, for
The Green House. Project: An Innovative Non-Institutional Rehab Program. Real Home - PHYSICAL ENVIRONMENT. Meaningful Life - PHILOSOPHY OF CARE
 Slide 1 The Woodlands of John Knox Village Kandice Robinson krobinson@jkvfl.com The Green House Project The Green House Project: An Innovative Non-Institutional Rehab Program Slide 2 The Green House Model
Slide 1 The Woodlands of John Knox Village Kandice Robinson krobinson@jkvfl.com The Green House Project The Green House Project: An Innovative Non-Institutional Rehab Program Slide 2 The Green House Model
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
The TeleHealth Model THE TELEHEALTH SOLUTION
 The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
ICRC Extended Study Hall Call Series: An Update on Using Medicare Data to Integrate Care for Medicare-Medicaid Enrollees
 ICRC Extended Study Hall Call Series: An Update on Using Medicare Data to Integrate Care for Medicare-Medicaid Enrollees December 3, 2012 For audio, dial: 1-800-273-7043; Passcode 596413 The Integrated
ICRC Extended Study Hall Call Series: An Update on Using Medicare Data to Integrate Care for Medicare-Medicaid Enrollees December 3, 2012 For audio, dial: 1-800-273-7043; Passcode 596413 The Integrated
Telehealth in Kent: what s behind its success?
 Telehealth in Kent: what s behind its success? 1 What kit did Kent use? The governing factor for KCC when choosing their telehealth kit was simplicity for the user. Typically, each telehealth patient has:
Telehealth in Kent: what s behind its success? 1 What kit did Kent use? The governing factor for KCC when choosing their telehealth kit was simplicity for the user. Typically, each telehealth patient has:
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT
 Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Using telehealth to monitor patients remotely:
 ehealth and nursing practice Using telehealth to monitor patients remotely: an RCN guide on using technology to complement nursing practice RCN Legal Disclaimer This publication contains information, advice
ehealth and nursing practice Using telehealth to monitor patients remotely: an RCN guide on using technology to complement nursing practice RCN Legal Disclaimer This publication contains information, advice
Caregiver Stress. F r e q u e n t l y A s k e d Q u e s t i o n s. Q: Who are our nation's caregivers?
 Caregiver Stress Q: What is a caregiver? A: A caregiver is anyone who provides help to another person in need. Usually, the person receiving care has a condition such as dementia, cancer, or brain injury
Caregiver Stress Q: What is a caregiver? A: A caregiver is anyone who provides help to another person in need. Usually, the person receiving care has a condition such as dementia, cancer, or brain injury
Collaborative Care- Bridging the Gap in Healthcare
 Collaborative Care- Bridging the Gap in Healthcare Ron Emerson RN BSN, Global Director of Healthcare Polycom, Inc. All rights reserved. Unnecessary Hospital Readmissions The Accountable Care Act mandated
Collaborative Care- Bridging the Gap in Healthcare Ron Emerson RN BSN, Global Director of Healthcare Polycom, Inc. All rights reserved. Unnecessary Hospital Readmissions The Accountable Care Act mandated
User Guide for Patients
 User Guide for Patients December 2016 Contents Health365 Overview... 3 What can I do with Health365?... 3 How to get started... 4 Sign In... 4 Home Page - Patient options... 6 Appointments... 7 To make
User Guide for Patients December 2016 Contents Health365 Overview... 3 What can I do with Health365?... 3 How to get started... 4 Sign In... 4 Home Page - Patient options... 6 Appointments... 7 To make
ADMITTING A PATIENT & DISCHARGE FROM HOSPITAL. Joe Camilleri
 ADMITTING A PATIENT & DISCHARGE FROM HOSPITAL Joe Camilleri S.Luke s Hospital Approximately Total Number of Admissions: 84,000 70% ward in-patients admissions 30% Day Cases 39% A&E, Out-Patients 48% Males/
ADMITTING A PATIENT & DISCHARGE FROM HOSPITAL Joe Camilleri S.Luke s Hospital Approximately Total Number of Admissions: 84,000 70% ward in-patients admissions 30% Day Cases 39% A&E, Out-Patients 48% Males/
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
Using information and technology to transform health and care
 Using information and technology to transform health and care Welcome to NHS Digital We are the national information and technology partner to the health and social care system. We re at the forefront
Using information and technology to transform health and care Welcome to NHS Digital We are the national information and technology partner to the health and social care system. We re at the forefront
TELEMEDICINE PORTAL West Walnut Hill Lane Suite 240 Irving, TX Phone: Fax:
 TELEMEDICINE PORTAL 1304 West Walnut Hill Lane Suite 240 Irving, TX 75038 Phone: 469.586.3317 Fax: 214.292.8841 www.shamsgroup.com 03/25/2016 V1.0 About The Shams Group The Shams Group Philosophy Telemedicine
TELEMEDICINE PORTAL 1304 West Walnut Hill Lane Suite 240 Irving, TX 75038 Phone: 469.586.3317 Fax: 214.292.8841 www.shamsgroup.com 03/25/2016 V1.0 About The Shams Group The Shams Group Philosophy Telemedicine
Health Plan Tools Telemedicine, Expert Second Opinion, Urgent Care & Wellness Centers
 Health Plan Tools Telemedicine, Expert Second Opinion, Urgent Care & Wellness Centers Compiled August 2014 Prepared by Aon Hewitt February 16, 2016 Health & Benefits Prepared by Aon Hewitt Health & Benefits
Health Plan Tools Telemedicine, Expert Second Opinion, Urgent Care & Wellness Centers Compiled August 2014 Prepared by Aon Hewitt February 16, 2016 Health & Benefits Prepared by Aon Hewitt Health & Benefits
Welcome to BCHC Your Medical Home
 START HERE 1 Welcome to BCHC Your Medical Home Thank you for choosing Berks Community Health Center (BCHC) as your medical home. This booklet gives you information about being a patient at BCHC and what
START HERE 1 Welcome to BCHC Your Medical Home Thank you for choosing Berks Community Health Center (BCHC) as your medical home. This booklet gives you information about being a patient at BCHC and what
REDUCING READMISSIONS FOR SNF PATIENTS
 REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Using Patient and Family Centered Care Fundamentals in Establishing an Office of Patient Experience
 Using Patient and Family Centered Care Fundamentals in Establishing an Office of Patient Experience Presenters: Keith Gran, CPA, MBA, Chief Patient Experience Officer Molly Dwyer-White, MPH, Administrative
Using Patient and Family Centered Care Fundamentals in Establishing an Office of Patient Experience Presenters: Keith Gran, CPA, MBA, Chief Patient Experience Officer Molly Dwyer-White, MPH, Administrative
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Post-Acute Care COMM UN I CATING T HE VA LU E L ES L IE MA RSH, CEO, L E X INGTON R EG I ONAL HEA LT H CE N T ER L E X I NGTON, N E BR ASKA
 Post-Acute Care COMMUNICATING THE VALUE LESLIE MARSH, CEO, LEXINGTON REGIONAL HEALTH CENTER LEXINGTON, NEBRASKA Swingbed CMS Definition Initially communicated to patients as a way to avoid a premature
Post-Acute Care COMMUNICATING THE VALUE LESLIE MARSH, CEO, LEXINGTON REGIONAL HEALTH CENTER LEXINGTON, NEBRASKA Swingbed CMS Definition Initially communicated to patients as a way to avoid a premature
CGS Administrators, LLC Clinical Hospice Documentation from CGS Missouri Hospice & Palliative Care Assoc. October 3, 2016
 Missouri Hospice & Palliative Care Conference Reviewer s decision is reliant upon documentation Results in a full denial for the submission Documentation must be legible Medical necessity is always based
Missouri Hospice & Palliative Care Conference Reviewer s decision is reliant upon documentation Results in a full denial for the submission Documentation must be legible Medical necessity is always based