Redesign the System: Improving Med/Surg Efficiencies and Patient Flow
|
|
|
- Blaise Lucas Bradford
- 6 years ago
- Views:
Transcription
1 These presenters have nothing to disclose. Redesign the System: Improving Med/Surg Efficiencies and Patient Flow Amanda Stefancyk Oberlies, Pat Rutherford and Christine White Hospital Flow Professional Development Program November 2, 2016 Cambridge, MA
2 Challenges on Medical and Surgical Units Care teams in most medical and surgical units are facing increased demand due to shorter lengths-of-stay, aging of the population, increased complexity and acuity of patients, inefficient care processes and challenges in discharging patients with the appropriate care in a timely fashion. Delayed transfers of patients between nursing units and lack of available beds are significant problems that increase costs and decrease quality of care and satisfaction among patients and staff. The overwhelming majority of discharges occur on medical and surgical units, and discharge delays often create bottlenecks that negatively impact patient flow throughout the hospital.
3 Session Objectives Describe innovative models for multidisciplinary collaboration and rounding on medical and surgical units Identify approaches for creating clear, agreedupon care plans for each patient -- which are a result of active participation of patients and their family members, hospitalists, surgeons, nursing staff and other care team members.
4 Cultivating Great Teams: What Health Care Can Learn from Google Psychological safety: Can team members take risks by sharing ideas and suggestions without feeling insecure or embarrassed? Do team members feel supported, or do they feel as if other team members try to undermine them deliberately? Dependability: Can each team member count on the others to perform their job tasks effectively? When team members ask one another for something to be done, will it be? Can they depend on fellow teammates when they need help? Structure & clarity: Are roles, responsibilities, and individual accountability on the team clear? Meaning of work: Is the team working toward a goal that is personally important for each member? Does work give team members a sense of personal and professional fulfillment? Impact of work: Does the team fundamentally believe that the work they re doing matters? Do they feel their work matters for a higherorder goal? NEJM Blog Post October 19, 2016 by Jessica Wisdom & Henry Wei
5 Institute of Medicine report The current system shows too little cooperation and teamwork. Instead, each discipline and type of organization tends to defend its authority at the expense of the total system s function. (2003)

6
7 Findings Relationships shape the communication through which coordination occurs...
8 Nurses Case Managers Patient care: A coordination challenge Attending Physicians Nursing Assistants Patients Physical Therapists Social Workers Technicians Referring Physicians Administrators
9 For better... Shared goals Shared knowledge Mutual respect Frequent Timely Accurate Problem-solving communication
10 or worse Functional goals Specialized knowledge Lack of respect Infrequent Delayed Inaccurate Finger-pointing communication

11 This process is called Communicating and relating for the purpose of task integration
12 Efficiency & financial outcomes Reduced turnaround time Increased employee productivity Reduced length of hospital stay Reduced total cost of hospital care Reduced inpatient hospitalizations Reduced total costs of chronic care Increased profit growth Improved operational excellence
13 Relational mapping Identify a work process that needs better coordination maybe treating our patients Which workgroups are involved? Draw a circle for each workgroup and lines connecting between them WEAK RC = RED MODERATE RC = BLUE STRONG RC = GREEN Color of the circle says how we are doing within each workgroup, color of the line says how we are doing between the workgroups
14 Relational mapping of current state WEAK RC MODERATE RC STRONG RC Workgroup 1 Workgroup 5 Workgroup 2 Workgroup 4 Workgroup 3 RC = Shared Goals, Shared Knowledge, Mutual Respect, Supported by Frequent, Timely, Accurate, Problem-Solving Communication 14

15 Example
 2.62 2.40 4.02 2.29 2.29 3.50 2.40 Physicians 3.58 4.26 3.47 4.25 4.19 3.84 3.50 Physicians' Assistants and Nurse Practitioners (PAs & NPs) 3.75 4.29 3.39 4.30 4.")
16 RC matrix Ratings of Admin CC PCAs Phys PA&NP RNs ResTh R a t i n g s b y Administrative Support Care Coordination Personal Care Assistants (PCAs) Physicians Physicians' Assistants and Nurse Practitioners (PAs & NPs) Registered Nurses Respiratory Therapy Relational Coordination Analytics, Inc. All Rights Reserved
17 Assessing current state Where is relational coordination currently working well? Where does it work poorly? How does this impact performance? What are the underlying causes? Where are our biggest opportunities for change? 2015 Relational Coordination Analytics, Inc. All Rights Reserved
18 Assessing current state Reporting back Which of our current structures support relational coordination? Which do not? Where are our biggest opportunities for change? Consider structures that can be developed locally (huddles) Also consider structures that require top leadership support (shared accountability, shared rewards) 2015 Relational Coordination Analytics, Inc. All Rights Reserved
19 Three kinds of interventions Relational interventions to build the new relational dynamics Work process interventions to connect new relational dynamics to improvements in the work Structural interventions to support the new relational dynamics

20 Stanford University Press
21 Multidisciplinary Rounds at MGH Amanda Stefancyk Oberlies PhD, MBA, RN, CENP Chief Executive Officer Organization of Nurse Leaders MA, RI, NH, CT
22 Strategic Objectives at MGH To develop improvements and innovations on nursing care units that will: Improve the quality and safety of patient care Increase patient-centeredness Create more effective care teams Improve staff satisfaction and retention Improve efficiency Leadership development of frontline staff and manager Transformational leadership Nurse autonomy and ownership of practice Quality measures are tracked Health care reform


23 The TCAB Process Frontline teams generate new ideas: not the quality department, not administration Testing ideas and measuring outcomes: Rapid-cycle testing facilitates change: one nurse, one patient, one shift Implementing and spreading successful changes Staff generates idea Collaborative learning Small tests of change Spread 23
24 TCAB at MGH Why TCAB at MGH? Aligns with values and mission Aligns with focus on innovation Supports evidenced based practice Strategically positions MGH for the future 24
25 A New Role in Rounds Green books served as catalyst Restructured rounds in a way that created a more active role for the nurse; formalized a role for the nurse Changing the culture this was difficult One year later more positive feedback

26 A New Role in Rounds
27 Collaboration and Satisfaction About Care Decisions (CSACD) Q #1 Over the past month, nurses and physicians planned together to make decisions about care for patients. Q #2 Over the past month, open communication between physicians and nurses took place as the decisions about patients were made. Q #3 Over the past month, decision-making responsibilities for patient care were shared between nurses and physicians. Q #4 Over the past month, physicians and nurses cooperated in making decisions regarding patient care. Q #5 Over the past month, when making patient care decisions, both nursing and medical concerns about patients needs were considered. Q #6 Over the past month, decision-making for patients was coordinated between physicians and nurses. Q #7 How much collaboration between nurses and physicians occurred in making decisions for patients over the past month? Q #8 How satisfied were you overall with the decisions made for patients over the past month that is the decision-making process? C. J. Baggs 1988
28 Collaboration and Satisfaction About Care Decisions (CSACD) Pre and Post Collaboration Results Always Complete Collaboration Strongly Satisfied 6 5 Before After 4 3 Never No Collaboration Strongly Dissatisfied 2 1 Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Questions C. J. Baggs 1988

29 AJN TCAB Series (Sept Aug 2009)

30 This presenter has nothing to disclose Redesign the system: A Comprehensive Approach to Caring for Hospitalized Medically Complex Patients Christine White MD, MAT Associate Professor-Hospital Medicine Cincinnati Children s Hospital Cincinnati, Ohio November 2, 2016 James Anderson Center for Health Systems Excellence
31 Objectives Recognize the importance of inpatient care coordination for hospitalized children with medical complexity (CMC) Identify challenges and opportunities for the development and implementation of inpatient CMC services Identify strategies for achieving seamless coordination across the care continuum for CMC. Recognize the value of integrating bedside providers to improve the efficiency of inpatient rounds
32 Complex Care Patient 4 year old male with chromosomal disorder Severe neurologic impairment Hydrocephalus s/p Ventriculoperitoneal shunt Epilepsy (on multiple antiepileptic drugs) Gastrostomy tube dependent (s/p Nissen) Cleft lip and palate s/p repair with tracheostomy dependence Chronic respiratory failure (BiPAP dependent) Hypothyroidism Spasticity
33 Complex Care Patient Specialists Involved Complex Care Center Neurology GI ENT Pulmonary Physical Medicine & Rehab Plastic Surgery Endocrinology Utilization 7 medical admissions in last year 50 inpatient days 5 ICU bed days Average of 3 consults/admit Average of 25 discharge medications
34 Definition: Children with Complex Medical Needs Children with complex medical needs rapidly growing population Group includes children with: A clearly identified medical specialty home Neurologic impairment Technology dependence
 Tracheostomy tube Gastrostomy tube")
35 Definition: Children with Complex Medical Needs Neurologic impairment (ex: cerebral palsy, brain injury) Tracheostomy tube Gastrostomy tube
36 At Risk Population High utilization of hospital resources Increasing admissions At risk for medication errors Limited longitudinal handoff between inpatient and outpatient
37 Challenges and Opportunities
38 Our History/The Problem -Patients from CCC cohorted onto 1Hospital medicine (HM) team -Staffed by CCC attending (105 patients/year) -Other general HM patients also on team Complex patients distributed amongst all 5 HM teams Remainder of neurologically impaired and technology dependent patients distributed among other 4 HM teams -Staffed by HM attendings (350 pts/year) Creation of New Complex Care Team 38
39 Rationale for the Creation of an Inpatient Medical Home Improve care coordination Provide more family centered care Improve the safety for these at risk patients Develop a core group of HM attendings Cohort patients onto one unit (if medically safe)
40 Complex Care Team Created to provide specialized care to this unique patient population All patients who are neurologically impaired or technology dependent admitted onto 1 HM team, including: Complex Care Clinic patients Palliative Care patients Transition Adult Care Patients Maximum 10 Patients

41 Multidisciplinary Rounds
42 Team Members Hospital Medicine Attending/Fellows Pediatric residents Medical students Advanced Practice Registered Nurses (APRNs) Bedside Nurses Pharmacist Dietician Unit Care managers Social Worker Patient s Primary Physician/Consultant Chaplain resident
43 Care Coordination
44 Care Coordination Rounds A once/weekly meeting with unit care managers The team reviews each patient s discharge goals, outlining tasks to be completed prior to discharge Discharge goals are listed and updated in the electronic health record A needs assessment tool serves as the framework for the conversation
45 Needs Assessment Tool Equipment Home Health Care Needs Private Duty Nursing Transportation Medications Follow-up Appointments Social/Family Concerns Education Needs
46 Medication Reconciliation Rounds Medication reconciliation completed on admission, transfer, and discharge The team pharmacist reviews each patient s current medications with the team before rounds weekly Medication Pathway: As patients progress toward reaching discharge goals, the pharmacist proactively reviews medications and mitigates anticipated barriers: Prior authorizations Need for refills Secondary insurance

47 Multidisciplinary Handoff On Friday afternoons, the outgoing and oncoming attending physicians hand off patient care Team members from the outpatient complex care clinics attend facilitating planning for the hospital to home transition
48 Outcomes
49 Outcomes: Discharge Efficiency Prior Work Physicians define medical criteria in EHR on admission Patient meets medicallyready criteria Nurse places time stamp in EHR Goal to leave within 2 hours of meeting all criteria Patient-focused around disease process improvement Do not aim for an arbitrary time of day 49


50 Consult Timeliness Frontline Staff Engagement Pharmacy Process Change How will this process apply to complex patients with unique discharge needs? 50

51
52 SMART Aim Increase the percentage of medically complex pediatric patients discharged within 2 hours* of meeting medically ready criteria from 50% to 80% by September 1, 2014 *If criteria were met between 9:00pm 7:00am, patients were not expected to leave until 9am
53 Increase the percentage of medically complex Key pediatric Drivers patients discharged within 2 hours of meeting medically ready criteria from 50% to 80% by September 1, 2014 Optimization of Team Structure Discharge Goal Identification Anticipation of Discharge Care Needs Staff Engagement in Discharge Preparedness Care Coordination
54 Run Chart Cohort Patients on Complex Care Team 54
55 Run Chart Cohort Patients on Complex Care Team Creation of Complex Care Admission Order Set 55

56 Complex Care Order Set 2013 Epic Systems Corporation. Used with permission. 56


57 Needs Assessment Tool Group Patients on Complex Care Team Creation of Complex Care Admission Order Set Weekly Multidisciplinary Care Coordination Rounds Medication Pathway Role Assignments Bi-Weekly Start Dates (Number of Patients)
58 Secondary Outcomes Median LOS: 3.1 days to 2.2 days (p =.13) Readmission rates: 31% to 22% (p =.23)
59 Stakeholder Feedback P59
60 Family Feedback Very positive feedback from families: I feel like things get done faster now Yellow team has been the best thing that happened to my daughter since we have been here You guys said you talked to my pediatricians in complex care clinic and the rehabilitation physicians but I didn t believe it until I saw you in rounds together. This makes me feel great Is discharge always this easy?
61 Attending /APRN Feedback 61 In a focus group, attendings and APRNs felt: The dedicated team makes the care of complex patients easier and more rewarding Structured meetings simplified and addressed the complex needs of these high risk patients Communication and care coordination with the families, outpatient primary care providers, and subspecialists were strengths
62 Nurse Feedback 62 Item Strongly disagree % (n) Disagree % (n) Undecided % (n) Agree % (n) Strongly agree % (n) More resources than before complex care team More comfortable providing care than before complex care 0% (0) 0% (0) 43% (10) 48% (11) 9% (2) 0% (0) 9% (2) 39% (9) 52% (12) 0% (0) Complex care team members are approachable and work well with other disciplines Have the appropriate amount of staff/resources to care for complex care patients 0% (0) 0% (0) 23% (5) 59% (13) 18% (4) 9% (2) 17% (4) 35% (8) 39% (9) 0% (0)
63 Resident Feedback 63 Residents perceived the new team as an efficient way to provide care Working with the multidisciplinary team is the epitome of care coordination. Managing complex patients with many problems as well as thinking about all of the ancillary things they need going home is a good exercise in the management of the overall patient, whereas in other rotations, you are concentrated on one problem and once they are recovered from their short term insult, go home without another thought about their continued care after their hospital admission.
64 Rounds Integration of Bedside Providers: RN led Rounds
65 Overall Aim 65 Standardize chronic care processes and multidisciplinary collaboration and communication
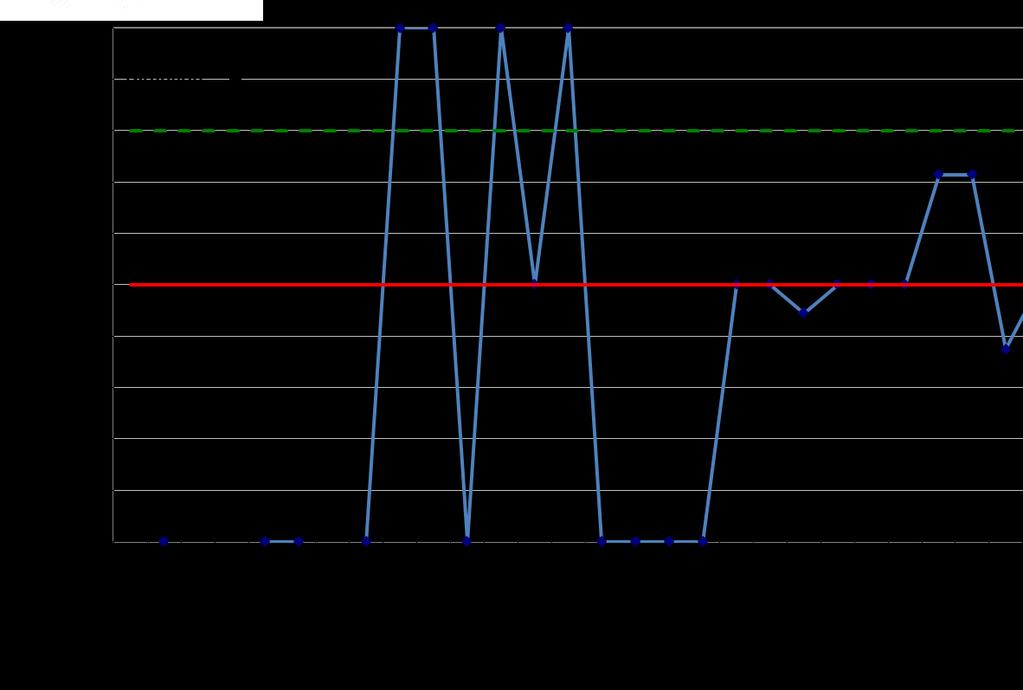
66 SMART Aim 66 Increase the weekly percentage of RNs presenting during daily pulmonary rounds in the tracheostomy unit from 73% to 95% by July 1st, 2017 Increase the weekly percentage of Respiratory therapists presenting during daily pulmonary rounds in the tracheostomy unit from 59% to 95% by July 1st, 2017
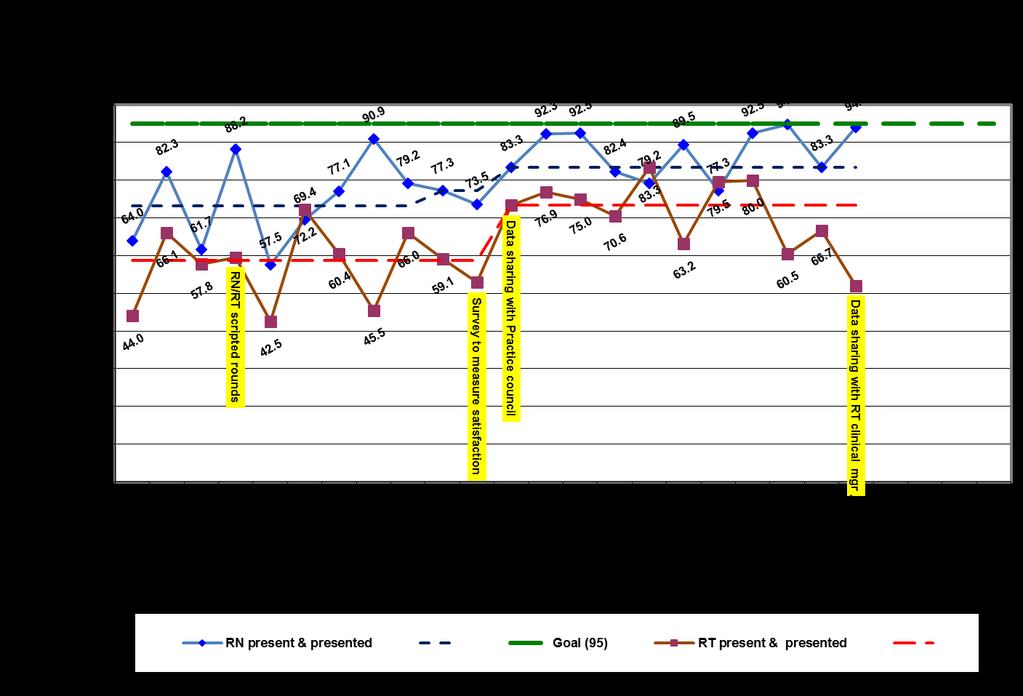

67 RN/Respiratory (RT) led rounds
68 RN Script 68 Pt Name: Tracheostomy Unit AM Rounding Sheet Nursing Date: Significant Overnight Events/Concerns: (Desaturations, PRN medications, vent changes, storming, seizures, abnormal labs, symptoms of respiratory illness). Please include nursing recommendations if applicable. Upcoming Tests/Procedures: Consent Transport needed NPO Status Trach change Labs sent Pre-op Meds Situational Awareness Specific to this Patient: Critical Airway Subglottic Stenosis Grade Malacia Breath holding Seizure Rescue Storming Plan Behavioral Plan Other Education Updates: Barriers to Prevention Standards: (CABSI, CAUTI, VARI, Pressure Ulcer, Safe Care Bundle) Medically Ready for Discharge: (Please circle one) Yes or No Needs to be completed: Barriers?:

69 Respiratory Therapy Script 69
70 Key Stakeholder Feedback P70

71 % of Staff Members who Completed the Survey
72 Summary of change
73 Resources 73 Cohen E, Kuo DZ, Agrawal R, et al. Children with medical complexity: an emerging population for clinical and research initiatives. Pediatrics. 2011;127(3): Statile AM, Schondelmeyer AC, Thomson JE, et al. Improving Discharge Efficiency in Medically Complex Pediatric Patients. Pediatrics. 2016;138(2):e
74 Thank You to Our Team! P74 Angela Statile MD, MEd Laura Brower MD Rebecca Brehob-Bucker, RD Suzan DeCicca LSW Stacey Litman-Padnos, LSW Julie Ostrye, PharmD Michelle Cobble, RN Abbie Ball, RN Rhonda Petsch, RN HM attendings/fellows HM APRNs Pediatric residents and chief residents Our outpatient partners Our unit nurses and RTs Dan Benscoter, MD Julie Clarke, RN Karen Tucker MSN, MBA, RN Julia Edmonson

75 Questions or Comments?
76 Comparison of Quality of Communication Before and Current
77 I Feel Involved Comparison
78 Patient Status and Plan of Care Comparison

79 Capacity 79
80 80 Total Census = 2544 Total days = 365 Yellow Days % Median Census 7.0 Days with census of % Days with census of % Days with census of 10 or more 39 11%

81 PDSA # 1
82 PDSA # 2
83 PDSA # 3
84 PDSA # 4
Using Quality Improvement to Optimize Pediatric Discharge Efficiency
 This presenter has nothing to disclose Using Quality Improvement to Optimize Pediatric Discharge Efficiency Christine White MD, MAT Associate Professor-Hospital Medicine Cincinnati Children s Hospital
This presenter has nothing to disclose Using Quality Improvement to Optimize Pediatric Discharge Efficiency Christine White MD, MAT Associate Professor-Hospital Medicine Cincinnati Children s Hospital
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
abstract QUALITY REPORT
 Improving Discharge Efficiency in Medically Complex Pediatric Patients Angela M. Statile, MD, MEd, a, b Amanda C. Schondelmeyer, MD, MSc, a, b, c Joanna E. Thomson, MD, MPH, a, b, c Laura H. Brower, MD,
Improving Discharge Efficiency in Medically Complex Pediatric Patients Angela M. Statile, MD, MEd, a, b Amanda C. Schondelmeyer, MD, MSc, a, b, c Joanna E. Thomson, MD, MPH, a, b, c Laura H. Brower, MD,
Improving Transition Home through a Standardized Discharge Process. Christopher D. Baker, MD Associate Professor of Pediatrics May 10, 2016
 Improving Transition Home through a Standardized Discharge Process Christopher D. Baker, MD Associate Professor of Pediatrics May 10, 2016 Objectives Identify components of the Children s Hospital Colorado
Improving Transition Home through a Standardized Discharge Process Christopher D. Baker, MD Associate Professor of Pediatrics May 10, 2016 Objectives Identify components of the Children s Hospital Colorado
INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program
 INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program INPATIENT PROGRAM ENVIRONMENT Upon admission, patients and families are oriented to the Rehabilitation Program, and are involved in an evaluation
INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program INPATIENT PROGRAM ENVIRONMENT Upon admission, patients and families are oriented to the Rehabilitation Program, and are involved in an evaluation
Hospital Flow Case Study: Cincinnati Children s Hospital
 Hospital Flow Case Study: Cincinnati Children s Hospital Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati,
Hospital Flow Case Study: Cincinnati Children s Hospital Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati,
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems NPSS Asheville, NC
 Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand
 This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov. 2016 Frederick C. Ryckman, MD Professor of Surgery / Transplantation
This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov. 2016 Frederick C. Ryckman, MD Professor of Surgery / Transplantation
Quality Improvement Project Control Report Out
 Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
The presentation will begin shortly.
 The presentation will begin shortly. The content provided herein is provided for informational purposes only. The views expressed by any individual presenter are solely their own, and not necessarily the
The presentation will begin shortly. The content provided herein is provided for informational purposes only. The views expressed by any individual presenter are solely their own, and not necessarily the
PEC GENERAL PEDIATRIC HOSPITALIST ELECTIVE
 PEC GENERAL PEDIATRIC HOSPITALIST ELECTIVE Rotation Director Jennifer Everhart, MD Introduction Welcome to the General Pediatric Hospitalist Elective at PEC! We are excited to have you join us! At the
PEC GENERAL PEDIATRIC HOSPITALIST ELECTIVE Rotation Director Jennifer Everhart, MD Introduction Welcome to the General Pediatric Hospitalist Elective at PEC! We are excited to have you join us! At the
Children with Medical Complexity: A Unique Population with Unique Needs
 Children with Medical Complexity: A Unique Population with Unique Needs Nancy Murphy MD, Professor and Chief, Division of Pediatric PM&R, University of Utah School of Medicine Rishi Agrawal MD, MPH, Lurie
Children with Medical Complexity: A Unique Population with Unique Needs Nancy Murphy MD, Professor and Chief, Division of Pediatric PM&R, University of Utah School of Medicine Rishi Agrawal MD, MPH, Lurie
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Select Medical TRANSITIONS OF CARE & CARE COORDINATION
 Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Initiating a Rapid Response Team
 Initiating a Rapid Response Team Trials and Tribulations! Washington County Hospital Facility Location Size Hagerstown, MD 320 bed Programs/Services History Emergency Services, Critical Care, Med/Surg,
Initiating a Rapid Response Team Trials and Tribulations! Washington County Hospital Facility Location Size Hagerstown, MD 320 bed Programs/Services History Emergency Services, Critical Care, Med/Surg,
OMC Strategic Plan Final Draft. Dear Community, Working together to provide excellence in health care.
 Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
8/31/2015. Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success. Vanderbilt University Medical Center
 Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
HIMSS 2011 Implementation of Standardized Terminologies Survey Results
 HIMSS 2011 Implementation of Standardized Terminologies Survey Results The current healthcare climate, with rising costs and decreased reimbursement, necessitates fiscal responsibility. Elements of the
HIMSS 2011 Implementation of Standardized Terminologies Survey Results The current healthcare climate, with rising costs and decreased reimbursement, necessitates fiscal responsibility. Elements of the
Leaning Care Management Documentation To Reflect The CMS Conditions Of Participation And Enhance Multidisciplinary Communication Of The Discharge Plan
 Leaning Care Management Documentation To Reflect The CMS Conditions Of Participation And Enhance Multidisciplinary Communication Of The Discharge Plan Stacey Willis Jr. MBA Emily Teesdale MSN RN 2 Spectrum
Leaning Care Management Documentation To Reflect The CMS Conditions Of Participation And Enhance Multidisciplinary Communication Of The Discharge Plan Stacey Willis Jr. MBA Emily Teesdale MSN RN 2 Spectrum
Bethesda Hospital PGY1 Residency Program Learning Experiences
 Bethesda Hospital PGY1 Residency Program Learning Experiences Required rotations Orientation This rotation will orient the resident to hospital pharmacy and the responsibilities of a staff pharmacist.
Bethesda Hospital PGY1 Residency Program Learning Experiences Required rotations Orientation This rotation will orient the resident to hospital pharmacy and the responsibilities of a staff pharmacist.
Quality Improvement in Neonatology. July 27, 2013
 Quality Improvement in Neonatology July 27, 2013 Disclosure Nothing to disclose Nothing off label No commercial products No financial affiliation Objectives Key components of Quality Improvement work Advances
Quality Improvement in Neonatology July 27, 2013 Disclosure Nothing to disclose Nothing off label No commercial products No financial affiliation Objectives Key components of Quality Improvement work Advances
at OU Medicine Leadership Development Institute August 6, 2010
 Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Decreasing Environmental Services Response Times
 Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Inpatient Rehabilitation. Scope of Services
 Inpatient Rehabilitation Scope of Services Inpatient Rehabilitation is a 12-bed inpatient unit located within Nationwide Children s Hospital. Nationwide Children s is a 451-bed, Level I Trauma Center.
Inpatient Rehabilitation Scope of Services Inpatient Rehabilitation is a 12-bed inpatient unit located within Nationwide Children s Hospital. Nationwide Children s is a 451-bed, Level I Trauma Center.
Enhancing Patient Care through Effective and Efficient Nursing Documentation
 Enhancing Patient Care through Effective and Efficient Nursing Documentation Session NI1, March 5, 2018 Jane Englebright, PhD, RN, CENP, FAAN HCA Senior Vice President & Chief Nurse Executive 1 Conflict
Enhancing Patient Care through Effective and Efficient Nursing Documentation Session NI1, March 5, 2018 Jane Englebright, PhD, RN, CENP, FAAN HCA Senior Vice President & Chief Nurse Executive 1 Conflict
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016
 Narrative for Health Care Organizations in Ontario 3/15/2016") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core
 Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
NURSING SPECIAL REPORT
 2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
Matching Capacity and Demand:
 We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Exploring the Care of Medically Complex Children
 Exploring the Care of Medically Complex Children Disclosure Wisdeen Wu, DO April 14, 2017 Wisdeen Wu, D.O. has no relationships with commercial companies to disclose. Learning Objectives At the end of
Exploring the Care of Medically Complex Children Disclosure Wisdeen Wu, DO April 14, 2017 Wisdeen Wu, D.O. has no relationships with commercial companies to disclose. Learning Objectives At the end of
Learning Experiences Descriptions
 Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Introduction to Value-Based Health Care Delivery
 Introduction to Value-Based Health Care Delivery Prof. Michael E. Porter Harvard Business School January 6, 2009 This presentation draws on Michael E. Porter and Elizabeth Olmsted Teisberg: Redefining
Introduction to Value-Based Health Care Delivery Prof. Michael E. Porter Harvard Business School January 6, 2009 This presentation draws on Michael E. Porter and Elizabeth Olmsted Teisberg: Redefining
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Care for Hospitalized Adults with Substance Use Disorder
 Improving Care for Hospitalized Adults with Substance Use Disorder Honora Englander, MD March 12, 2018 National Academies of Science, Engineering and Medicine I have no conflicts of interest to disclose.
Improving Care for Hospitalized Adults with Substance Use Disorder Honora Englander, MD March 12, 2018 National Academies of Science, Engineering and Medicine I have no conflicts of interest to disclose.
The Heart of Care Redesign; Care Protocols. Paul N. Casale, MD, FACC Chief, Division of Cardiology Lancaster General Health
 The Heart of Care Redesign; Care Protocols Paul N. Casale, MD, FACC Chief, Division of Cardiology Lancaster General Health Lancaster General Health By the Numbers (Fiscal Year 2012) Beds: 631 in service
The Heart of Care Redesign; Care Protocols Paul N. Casale, MD, FACC Chief, Division of Cardiology Lancaster General Health Lancaster General Health By the Numbers (Fiscal Year 2012) Beds: 631 in service
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
KEY QUESTIONS TO ASK when choosing an orthopaedic program
 7 KEY QUESTIONS TO ASK when choosing an orthopaedic program ASK THE RIGHT QUESTIONS so you can make the best choice The vast amount of information available to you makes choosing an orthopaedic surgery
7 KEY QUESTIONS TO ASK when choosing an orthopaedic program ASK THE RIGHT QUESTIONS so you can make the best choice The vast amount of information available to you makes choosing an orthopaedic surgery
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 2. Expedition Coordinator
 Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
1. PROMOTE PATIENT SAFETY.
 SAN FRANCISCO GENERAL HOSPITAL MEDICAL CENTER GOALS & ACCOMPLISHMENTS FISCAL YEAR 2006-2007 1. PROMOTE PATIENT SAFETY. Implemented medication reconciliation processes and procedures for admitted patients.
SAN FRANCISCO GENERAL HOSPITAL MEDICAL CENTER GOALS & ACCOMPLISHMENTS FISCAL YEAR 2006-2007 1. PROMOTE PATIENT SAFETY. Implemented medication reconciliation processes and procedures for admitted patients.
If you experience any problems, please call Marilyn Nichols at the MOCPS office at , ext 221 or The Basics of CUSP
 Welcome to The Basics of CUSPCoaching Call 6 The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842#. Participants received an email this morning
Welcome to The Basics of CUSPCoaching Call 6 The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842#. Participants received an email this morning
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Barriers to Early Rehabilitation in Critically Ill Patients. Shannon Goddard, MD Sunnybrook Health Sciences Centre
 Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
The curriculum is based on achievement of the clinical competencies outlined below:
 ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Project Title: Inter-professional Clinical Assessment Rounding & Evaluation (I-CARE) Rosiland Harris, DNP, RN, RNC, ACNS-BC, APRN
 Rosiland Harris, DNP, RN, RNC, ACNS-BC, APRN") Project Title: Inter-professional Clinical Assessment Rounding & Evaluation (I-CARE) Rosiland Harris, DNP, RN, RNC, ACNS-BC, APRN Grady Health System Level I Trauma Center Burn Center Comprehensive Stroke
Project Title: Inter-professional Clinical Assessment Rounding & Evaluation (I-CARE) Rosiland Harris, DNP, RN, RNC, ACNS-BC, APRN Grady Health System Level I Trauma Center Burn Center Comprehensive Stroke
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Conflict of Interest. Objectives. The Solution. The Need. Reaching for the Stars Advanced Roles for Pharmacy Technicians.
 8/14/2014 Reaching for the Stars Advanced Roles for Pharmacy Conflict of Interest No conflicts of interest to disclose Informatics Bryan Shaw, Pharm.D. PGY-1 Non-Traditional Resident Northwestern Memorial
8/14/2014 Reaching for the Stars Advanced Roles for Pharmacy Conflict of Interest No conflicts of interest to disclose Informatics Bryan Shaw, Pharm.D. PGY-1 Non-Traditional Resident Northwestern Memorial
Achieving the Triple Aim in Nursing: The Bellin Experience
 C23 This presenter has nothing to disclose Achieving the Triple Aim in Nursing: The Bellin Experience Laura Hieb, BSN, RN, MBA, NE-BC, Chief Nursing Officer, Bellin Health Lois Van Abel, BSN, RN, MBA,
C23 This presenter has nothing to disclose Achieving the Triple Aim in Nursing: The Bellin Experience Laura Hieb, BSN, RN, MBA, NE-BC, Chief Nursing Officer, Bellin Health Lois Van Abel, BSN, RN, MBA,
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation
 Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Project Title: Inter professional Clinical Assessment Rounding & Evaluation (I CARE)
") Project Title: Inter professional Clinical Assessment Rounding & Evaluation (I CARE) Rosiland Harris, DNP, RN, RNC, ACNS BC, APRN Project Director Pamela Gordon, DNP, RN Project Manager Grady Memorial
Project Title: Inter professional Clinical Assessment Rounding & Evaluation (I CARE) Rosiland Harris, DNP, RN, RNC, ACNS BC, APRN Project Director Pamela Gordon, DNP, RN Project Manager Grady Memorial
Supply and Demand of Health Care Workers in Minnesota. Speaker: Teri Fritsma Wednesday, March 8, :35 3:20 p.m.
 Supply and Demand of Health Care Workers in Minnesota Speaker: Teri Fritsma Wednesday, March 8, 2017 2:35 3:20 p.m. Teri Fritsma Teri Fritsma is a senior research analyst for the Minnesota Department of
Supply and Demand of Health Care Workers in Minnesota Speaker: Teri Fritsma Wednesday, March 8, 2017 2:35 3:20 p.m. Teri Fritsma Teri Fritsma is a senior research analyst for the Minnesota Department of
How can we provide the same world class care to patients with psychiatric disorders? 11/27/2016. Dec 2016 Orlando, FL
 The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
AAP SoOr Panel: Comanagement of the Pediatric Orthopedic Patient
 AAP SoOr Panel: Comanagement of the Pediatric Orthopedic Patient Joshua M. Abzug, MD, FAAP Becca Rosenberg, MD, MPH, FAAP David I. Rappaport, MD, FAAP Disclaimers We have no relevant conflicts of interests
AAP SoOr Panel: Comanagement of the Pediatric Orthopedic Patient Joshua M. Abzug, MD, FAAP Becca Rosenberg, MD, MPH, FAAP David I. Rappaport, MD, FAAP Disclaimers We have no relevant conflicts of interests
How to Initiate and Sustain Operational Excellence in Healthcare Delivery: Evidence from Multiple Field Experiments
 How to Initiate and Sustain Operational Excellence in Healthcare Delivery: Evidence from Multiple Field Experiments Aravind Chandrasekaran PhD Peter Ward PhD Fisher College of Business Ohio State University
How to Initiate and Sustain Operational Excellence in Healthcare Delivery: Evidence from Multiple Field Experiments Aravind Chandrasekaran PhD Peter Ward PhD Fisher College of Business Ohio State University
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Patient Encounters & Hospital Reach
 Patient Encounters & Hospital Reach Palliative Care Service Penetration Palliative care service penetration is the percentage of annual hospital admissions seen by the palliative care team. Penetration
Patient Encounters & Hospital Reach Palliative Care Service Penetration Palliative care service penetration is the percentage of annual hospital admissions seen by the palliative care team. Penetration
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
La Rabida Inpatient Rotation PL2 Residents
 PL2 Residents Residents rotate through the inpatient service at La Rabida Children s Hospital and Research Center over 1-2 months during the second year of residency. The inpatient service is separated
PL2 Residents Residents rotate through the inpatient service at La Rabida Children s Hospital and Research Center over 1-2 months during the second year of residency. The inpatient service is separated
TRANSLATING INSTITUTIONAL DATA INTO UNIT SPECIFIC OUTCOME METRICS USING CUSTOMIZED NURSING SCORECARDS
 TRANSLATING INSTITUTIONAL DATA INTO UNIT SPECIFIC OUTCOME METRICS USING CUSTOMIZED NURSING SCORECARDS Debra Campbell, BSN, RN, CPHQ Mary Stevie, MS, RN Cincinnati, Ohio Est. 1889 About TCHHN 621 Bed Tertiary
TRANSLATING INSTITUTIONAL DATA INTO UNIT SPECIFIC OUTCOME METRICS USING CUSTOMIZED NURSING SCORECARDS Debra Campbell, BSN, RN, CPHQ Mary Stevie, MS, RN Cincinnati, Ohio Est. 1889 About TCHHN 621 Bed Tertiary
Departments to Improve. February Chad Faiella RN, Terri Martin RN. 1 Process Excellence
 Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
The Effects of an Electronic Hourly Rounding Tool on Nurses Steps
 The Effects of an Electronic Hourly Rounding Tool on Nurses Steps Dr. Aimee Burch, DNP, APRN-CNS CHI Health St. Francis Katie Hottovy, Co-founder and Director of Client Services, Nobl Disclosures to Participants
The Effects of an Electronic Hourly Rounding Tool on Nurses Steps Dr. Aimee Burch, DNP, APRN-CNS CHI Health St. Francis Katie Hottovy, Co-founder and Director of Client Services, Nobl Disclosures to Participants
M7: Improving Transitions and Reducing Avoidable Rehospitalizations. St. Luke s Hospital Member, Iowa Health System
 M7: Improving Transitions and Reducing Avoidable Rehospitalizations Peg M. Bradke, RN, MA St. Luke s Hospital, Cedar Rapids, Iowa This presenter has nothing to disclose. St. Luke s Hospital Member, Iowa
M7: Improving Transitions and Reducing Avoidable Rehospitalizations Peg M. Bradke, RN, MA St. Luke s Hospital, Cedar Rapids, Iowa This presenter has nothing to disclose. St. Luke s Hospital Member, Iowa
Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management
 Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management Michelle Cline, RN, MSN, Care Model Redesign Manager Donna Litwinski, PT, Master Lean Fellow April 2018
Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management Michelle Cline, RN, MSN, Care Model Redesign Manager Donna Litwinski, PT, Master Lean Fellow April 2018
Introduction 4/7/2015
 The Perfect Storm: A Distinguished Post-Acute Rehabilitation Program (Session # W25) Wednesday April 29 th, 2:30-4:30 Presented by: Hilary Forman PT, RAC-CT Senior Vice President of Clinical Strategies
The Perfect Storm: A Distinguished Post-Acute Rehabilitation Program (Session # W25) Wednesday April 29 th, 2:30-4:30 Presented by: Hilary Forman PT, RAC-CT Senior Vice President of Clinical Strategies
Perfecting Emergency Department Operations
 These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
Neurocritical Care Fellowship Program Requirements
 Neurocritical Care Fellowship Program Requirements I. Introduction A. Definition The medical subspecialty of Neurocritical Care is devoted to the comprehensive, multisystem care of the critically-ill neurological
Neurocritical Care Fellowship Program Requirements I. Introduction A. Definition The medical subspecialty of Neurocritical Care is devoted to the comprehensive, multisystem care of the critically-ill neurological
Maroon Inpatient Rotation PL-1 Residents
 PL-1 Residents The Inpatient Maroon experience has been designed to develop the needed competencies for an intern to manage patients with a wide array of conditions requiring hospitalization, from the
PL-1 Residents The Inpatient Maroon experience has been designed to develop the needed competencies for an intern to manage patients with a wide array of conditions requiring hospitalization, from the
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
9/8/2014. I have no conflicts of interest to disclose. I have no conflicts of interest to disclose
 How to Start an APN Run Pain Service: From Conception to Continuation Mechele Fillman RN-BC, APRN, NP-C Acute Pain Service Nurse Practitioner Stanford Hospital and Clinics Carrie Brunson RN-BC, APRN, ANCS-BC
How to Start an APN Run Pain Service: From Conception to Continuation Mechele Fillman RN-BC, APRN, NP-C Acute Pain Service Nurse Practitioner Stanford Hospital and Clinics Carrie Brunson RN-BC, APRN, ANCS-BC
Running head: LEADERSHIP ANALYSIS: ROUNDING 1
 Running head: LEADERSHIP ANALYSIS: ROUNDING 1 Leadership Analysis: Rounding Jerrene Bramble, Tara Braun, Pamela Dusseau, Angelique Kinyon, William McKinley, Noranne Morin, Nicky Reed, and Ashleigh Wash
Running head: LEADERSHIP ANALYSIS: ROUNDING 1 Leadership Analysis: Rounding Jerrene Bramble, Tara Braun, Pamela Dusseau, Angelique Kinyon, William McKinley, Noranne Morin, Nicky Reed, and Ashleigh Wash
Please return your completed materials to: Duke University Medical Center Box 3417 Durham, NC 27710
 Thank you for your interest in the with the Child and Adolescent Life Program. Our internship program is offered two times a year: Fall (September-December) and Spring (January April) To be qualified for
Thank you for your interest in the with the Child and Adolescent Life Program. Our internship program is offered two times a year: Fall (September-December) and Spring (January April) To be qualified for
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
South Warwickshire s Whole System Approach Transforms Emergency Care. South Warwickshire NHS Foundation Trust
 South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Building Systems and Leadership for Transformation
 Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
Application of QSEN competencies in a practice setting: The case of Cincinnati Children s Hospital Medical Center
 Application of QSEN competencies in a practice setting: The case of Cincinnati Children s Hospital Medical Center Heather L. Tubbs Cooley, PhD, RN Assistant Professor & Nurse Scientist CCHMC Quality Scholar
Application of QSEN competencies in a practice setting: The case of Cincinnati Children s Hospital Medical Center Heather L. Tubbs Cooley, PhD, RN Assistant Professor & Nurse Scientist CCHMC Quality Scholar
THE SUPPORTING ROLE IT PLAYS FOR THE CHILD, PARENT AND CAREGIVER
 THE WOMEN S AND CHILDREN S HOSPITAL HOME ENTERAL NUTRITION SERVICE: THE SUPPORTING ROLE IT PLAYS FOR THE CHILD, PARENT AND CAREGIVER DANA WRIGHT RN, BNg, Grad. Cert. Health (CCAFHN) Clinical Nurse - Home
THE WOMEN S AND CHILDREN S HOSPITAL HOME ENTERAL NUTRITION SERVICE: THE SUPPORTING ROLE IT PLAYS FOR THE CHILD, PARENT AND CAREGIVER DANA WRIGHT RN, BNg, Grad. Cert. Health (CCAFHN) Clinical Nurse - Home
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
FY 13 Pillar Goal Update and FY 14 Pillar Goals
 FY 13 Pillar Goal Update and FY 14 Pillar Goals Summer Leadership Assembly C. Wright Pinson, MD, MBA Deputy Vice Chancellor, Health Affairs CEO, Vanderbilt Health System June 19, 2013 Staying Focused on
FY 13 Pillar Goal Update and FY 14 Pillar Goals Summer Leadership Assembly C. Wright Pinson, MD, MBA Deputy Vice Chancellor, Health Affairs CEO, Vanderbilt Health System June 19, 2013 Staying Focused on