Let My Patients Flow! Patient Flow Summit 2015
|
|
|
- Frederick Simpson
- 6 years ago
- Views:
Transcription

1 Let My Patients Flow! Patient Flow Summit
2 Agenda Background Approach Process Improvement Teams Simulation Model Results Q&A 2
3 Robert Wood Johnson University Hospital 965-bed Academic Medical Center located in New Brunswick, NJ Principal Teaching Hospital of Rutgers Robert Wood Johnson Medical School Flagship Hospital of multi-hospital system Centers of Excellence: Cardiovascular; Cancer; Women s & Neuroscience Center of Excellence; Level 1 Trauma Center Children s; Located mid-way between New York and Philadelphia, serving six county population of approximately 1.4 M Owner of Physician-Led Accountable Care Organization 3

4 4
5 Situation at RWJUH Anticipated a significant increase in patient volume for the OR suite. As a major source of revenue for the hospital, the leadership team needed to make sure the OR suite was as efficient as possible while also minimizing costs. Due to the highly variable nature of work flow in the OR and the expenses involved in managing the projected increase of volume, as well as the introduction of case carts into the OR system, leadership requested that an objective data driven analysis be conducted in order to assure optimal performance of the OR suite. 5
6 Problem Statement Key Considerations/Potential Pitfalls when writing the Problem Statement Is the problem based on observation (fact) or assumption (guess)? Does the problem statement prejudge a root cause? Can data be collected by the team to verify and analyze the problem? Is the problem statement too narrowly or broadly defined? Is a solution included in the statement? Would customers be happy if they knew we were working on this? 6
7 RWJUH Problem Environmental factors driving a significant volume increase Introducing case carts to improve material flow and control OR utilization not acceptable Significant OR churn resulting in staff and patient stress Significant OR hold time due to PACU utilization issues 7
8 Problem Statement A well formed problem statement should answer specific questions and include specific information: What is the problem? When or under what conditions does this problem occur? Where does this problem occur? What is the extent of the problem? What is the impact of the problem? 8
9 9 Simulation

10 Goal Statement Identify Your Business Goal From Your Project Sponsor Identify Which of Those Goals Your Project Supports 10
11 Problem vs. Goal Statement The Purpose of the Problem Statement Is to Describe What Is Wrong The Goal Statement Defines The Team s Improvement Objective 11
12 The Goal Statement Defines the improvement the team is seeking to accomplish Starts with a verb (e.g., reduce, eliminate, control, increase) Tends to start broadly eventually should include measurable target and completion date Must not assign blame, presume cause, or prescribe solution! Example: Reduce the number of ER turnaround times for level 2 type patients beyond 1.5 hours by 50% from 500 to 250 by January 1 Goal = Project Improvement Objective 12
13 RWJUH Problem / Goal Problem - Old system processes and infrastructure made efficiency a daily challenge with a growing perioperative service line. Competing stakeholders with competing cultures and goals. Highly variable work flow in the OR, high cost inefficient set-up with the introduction of new systems and targeted expansion putting pressure on phasing and new work flow processes. Goal Improve overall efficiency of the OR Suite for both adult and pediatric services while also minimizing costs. Leadership requested that lean teams were deployed to ensure maximum return on investment of our new COE dedicated to pediatric surgery, new dedicated robotic suites, expanded PACU capacity and a new highly functioning case cart system. 13
14 Stakeholder Analysis A Stakeholder is any person or group of people who are: Responsible for the final decision Likely to be affected, positively or negatively, by the outcomes you want In a position to assist or block achievement of the outcomes Experts or special resources that could substantially affect the quality of your end product/service Can have influence over other stakeholders Identify those individuals with an interest in the process and what their positions on a particular Six Sigma Change might be. 14
15 Stakeholder Analysis SA MA N MS SS Stakeholder A X Stakeholder B X Stakeholder C X X Stakeholder D X X Stakeholder E X X Stakeholder F X X Stakeholder G X Stakeholder H X Stakeholder I X Stakeholder J X Stakeholder K X X 15
16 Sources of Resistance Source of Resistance Definition/Causes of Resistance Some Strategies for Overcoming Resistance Technical Habit and inertia Difficulty in learning new skills Lack of skills Provide education and training Provide coaches, green belts, tools / job aids Get people involved Political Threat to status quo See Initiative as a loss Power and authority imbalance or selfpreservation Empathize with the loss and show WIIFM Do a political map to understand influence patterns Provide safe exits and/or alternate job designs New measures and rewards -- customer driven Clarify roles and responsibilities -- accountabilities Cultural Control Issues Locked into old "mindset Afraid of letting go Do a cultural audit: what beliefs drive us? Articulate desired mindset and gaps Give resistor control over the initiative Give the resistor credit for the change 16
17 Approach Form clinical based process improvement teams Teams define the processes Teams gather data on the processes Teams to recommend process changes Teams to guide change implementation Need arose to verify process changes prior to implementation and define which changes worked well together in combination 17
18 18 Charter Development
19 ANALYZE Define Measure Analyze Improve Who are the customers and what are their priorities? How is the process performing and how is it measured? What are the most important causes of the defects? How do we remove the causes of the defects? Control How can we maintain the improvements? 19
20 An approved charter establishes the purpose and plan for the project. The key elements of the charter are: Problem Statement Project Timeline Goal Project Scope Milestones Develop Team Charter - Objectives Team Members, Stakeholders and Roles A charter: Clarifies what is expected of the team Keeps the team focused Keeps the team aligned with organizational priorities Transfers the project from the Project Sponsor to the project team 20
21 Process Improvement Teams Formed steering team of clinical personnel who manage the work in the area affected Formed process oriented clinical teams for each major process Team supported by training and central quality improvement resources Started team and asked team if others were required to ensure all stakeholders involved Teams set goals for process improvement 21
22 Team Member Roles How do you want the Project Sponsor to work with the team? Is the team s role to implement or recommend? When must the team go to the Project Sponsor for approval? What authority does the team have to act independently? What and how do you want to inform the Project Sponsor about the team s progress? What is the role of the team leader (Black Belt) and the team coach (Master Black Belt)? Are the right members on the team? Functionally? Hierarchically? 22
23 Process Improvement Teams Teams created a flowchart of the process under study Teams measured current performance Teams brainstormed changes and selected those rated most effective in reaching the goal Team reported to central steering committee Team and steering committee agreed on implementation What How Time Frame 23
24 ROLE RESPONSIBILITIES BEHAVIORS Executive Sponsor Project Owner Team Leader Improvement Team (Typically 3-8 consistent members) Facilitator 24 Team Member Roles Strategic guidance Active participation (Regular mtgs, event kick offs & report outs) Eliminate barriers Communication to admin staff & organization Oversight & results of project Team selection Hold team accountable Communication: Report status (up and down) Monitor progress & attend regular progress mtgs Sustain improvements after project completion Recognize achievements Content expert & team member, Provide data as needed, coordinate observations Recommend team members Manage team focus / progress / follow-up, help lead meetings Communication (Work with facilitator & project owner) With project owner, own process & sustain changes Includes subject matter experts Participate in observations and data collection as appropriate Attend project meetings & improvement events (contribute ideas & execute action items) Communication with coworkers Guide the team (scope project, assist with team selection, provide structure for project) Lead pre-work w/ project owner / team leader incl. analysis Lead improvement events (e.g. Kaizen, Work-Out) Communication with entire project team Hand off of project including metrics to project owner Highlight achievements Committed to success of project Trusts process Fosters feeling of unity Respect for team Empowers team Mentors team members Inspires team members Utilizes listening skills Maintains team focus Positive (Trust) Motivated and motivates others (Commitment) Listens (Learning) Open to suggestions (Respect) Respectful of each other Holds self and others accountable Actively engaged Promotes positive environment Influential among coworkers Confident Committed to success of project Understanding of team s needs Inspires team Respect for team Supportive of improvement efforts throughout the project Objective
25 Approach Some processes were highly interdependent making process change effectiveness difficult to predict Some changes needed their effectiveness demonstrated to engage all stakeholders Needed to test alternatives quickly and quantify their relative effectiveness Collaborated with ProModel Corp. to construct a simulation model of the entire OR suite This model used to analyze and verify changes prior to implementation 25
26 Lean in the OR PI teams tasked with applying lean principles to the OR Eliminate waste! Excessive movement Excessive waiting Pull instead of push Paradigm shift for OR 26

27 Project Scope What process will the team focus on? What are the boundaries of the process we are to improve? Start point? Stop point? What resources are available to the team? What is out of bounds for the team? What constraints must the team work under? What is the time commitment expected of team members? What will happen to our regular jobs while we are doing the project? 27
28 Tools to Define Project Scope In/Out of the Frame Visual tool based on the analogy of a picture frame It challenges the team to identify those aspects of the project (the type and extent of end results or deliverables, the people impacted, timing, product lines impacted, sites involved, etc.) which are : in the frame (meaning clearly within the scope of work) out of the frame half-in-half-out (meaning this is either up for debate, or some aspects are in the scope of work but only in a partial way) 28
 Realistic (don t force yourselves into band-aid solution) Documented, shared with all project team members and Champion, and updated regularly")
29 Milestones A high-level project plan with dates Tied to phases of the project management process (define, measure, analyze, improve, and control/sustain) Aggressive (don t miss window of opportunity ) Realistic (don t force yourselves into band-aid solution) Documented, shared with all project team members and Champion, and updated regularly 29
30 Pediatric Suite Elevator Changes Scenario Patient Type Total Exits Average Total Cycle Time Differenc Class P Patients Above 120 Min Wait (/Year) Case Cart Utilization Time In Pre-Op As Is with Class P peds patient % Seventh Floor Peds Proposed Opening Day Configuration peds patient % % Seventh Floor Peds Proposed Opening Day Configuration With Elevator Policy peds patient % %


31 Histogram Represents data to evaluate: Central Tendency Spread Patterns in data ID sources of variation Summarizes large data sets into frequency intervals 31

32 Pediatric Room Use Effect Increased Time Spent in Pre-Op versus Current State Increase of 32 minutes 32

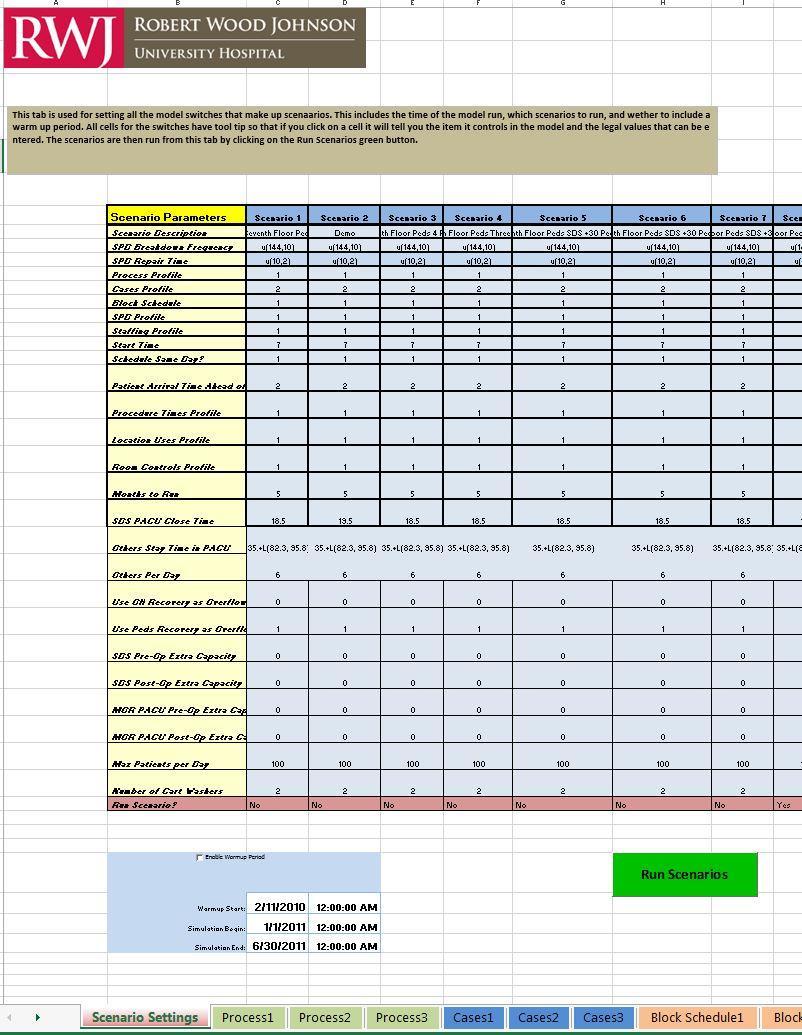
33 Cause and Effect Diagram Helps to ID possible causes related to a problem or a condition The team focuses on the content of the problem not the history Creates a snapshot of collective knowledge Builds support for resulting solutions 33
34 Fishbone Diagram Example * NOT RWJUH DATA 34

35 35 Nursing Staffing Requirements of Various Changes

36 Investigation into Three Possible Pediatric Configurations The majority of this extra time occurs due to patients spending extra time in pre-op and 1 st stage recovery due to contention for beds when these two stages are occurring in the same space. This is shown by the chart of patient time in stage shown below. 36
37 Run Charts * NOT RWJUH DATA Displays data in time order sequence 37
38 Throughput Affect of Various Changes As Is As Is with Class P Class P Bump Own Service Only Class P with Peds Recovery Total Exits Average Time In System (Min) Total Exits Average Time In System (Min) Total Exits Average Time In System (Min) Total Exits Average Time In System (Min) MOR patient peds patient SDS patient

39 Helps team focus on causes Based on the Pareto Principle 80/20 Rule Displays the relative importance of problems Shown by frequency or size in a descending bar graph Pareto Analysis 20% of the sources cause 80% of any problem 39
40 Need for Simulation Many processes interdependent Patient care processes too critical to experiment requiring proof of change effectiveness Case cart processes totally new to the OR suite All of these factors make it necessary to have a safe trial environment to test changes, investigate processes, and prove effectiveness BEFORE their introduction into the patient care process 40
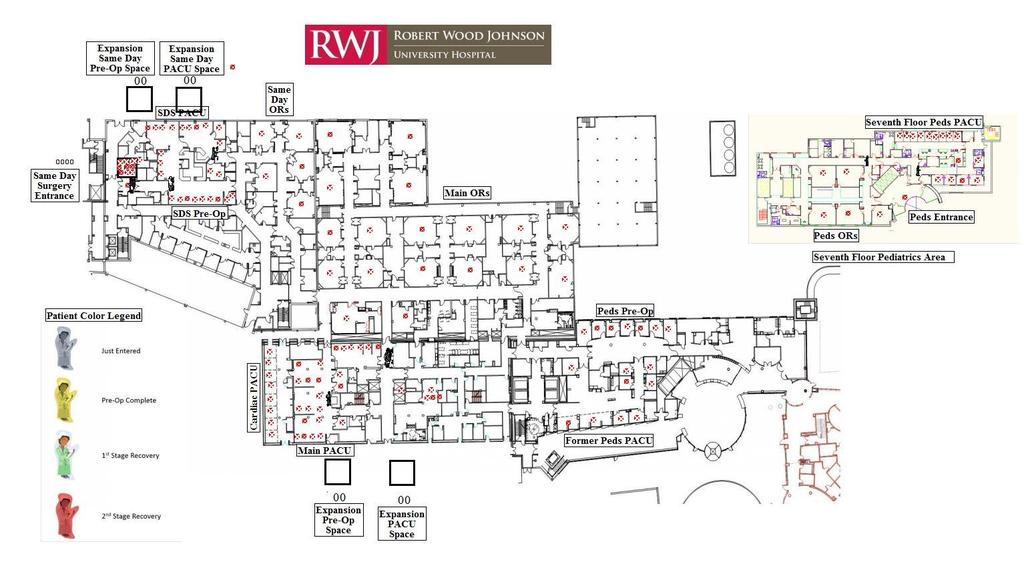
41 Simulation Collaborated with a trusted consultant Model constructed on floorplan (Autocad) of OR suite and scaled to drawing One year+ of data used to construct time and arrival distributions Model driven by Excel frontend for quick update and scenario creation Multiple scenarios created to test the introduction of case carts by itself and multiple process change combinations 41
42 42 Simulation
43 43
44 IMPROVE... determine and confirm the optimal solution... How can we fix the process? Generate alternatives Assess the risks Test the alternatives Select the best alternative Can we confirm the problem by turning it off and on? Process X s or Factors X 1 X 2 X 3 PROCESS Outputs Y 1 Y 2 X 4 Y 3 The after curve shows a more standardized practice with reduced variation a more predictable model Before Improvements After Improvements 44
45 Model Benefits Explain what the model provided Explain how it let us know the unknowable Explain how it let us experiment with the processes to define those changes that are effective 45



46 Hypothesis Testing Helps us determine whether observed differences are: statistically significant or due to chance (random variation) 46

47 Identify Improvement Strategy Utilize different methods to identify solutions: Brainstorming Creative Thinking Best Practice Should Be Process Map Run A Pilot Study Full Implementation Design of Experiments 47
48 IMPROVE Define Measure Analyze Improve Who are the customers and what are their priorities? How is the process performing and how is it measured? What are the most important causes of the defects? How do we remove the causes of the defects? Control How can we maintain the improvements? 48
49 Objective and Solution Objective To increase throughput while optimizing staff and plan for the necessary actions required to further accommodate a rise in patient volume. Solution The leadership team for the OR needed to understand; The overall constraints on throughput in the OR Suite The cycle time for patients flowing through the system Where patient flow problems existed, managers needed to determine if they were being caused by a lack of space or insufficient staff. The team was tasked with determining whether the OR suite could accommodate a 30% increase in patient volume without changing the OR s physical environment or adding additional space. Additionally, case carts were being introduced into the system and the team needed to make sure that the carts were properly resourced to keep up with patient flow through the OR. To deal with the effects of high variability in the OR it was decided that a simulation solution was the only way to reliably predict the impact of changes to the work and/or workflow. 49
50 Objective Objective and Solution To increase throughput while optimizing staff and plan for the necessary actions required to further accommodate a rise in patient volume. Solution Particular attention was paid to the two patient recovery (PACU) areas in the OR System, the Main PACU and Cardiac PACU. Expansion areas were also added to the model to help understand if they could potentially add capacity and improve patient flow through the OR, or if they were sources of further constraint to the system. The model was also designed to be fully costed, incorporating financial elements and reporting on how much profit is generated with each patient flow scenario. The output data of the model allowed the leadership team at RWJUH to design an optimal workflow process that consisted of adjusting their staffing levels to ensure maximum throughput with minimum patient delay and at minimum cost. 50
51 Objective Investigation into Three Possible Pediatric Configurations This study was to investigate the three different configurations under consideration for the Pediatrics department operating suite on the seventh floor of Robert Wood Johnson University Hospital. 51
52 Investigation into Three Possible Pediatric Configurations The analysis was performed using the RWJUH OR Suite flexible simulation model previously defined and validated. Data covering OR cases from November 1, 2012 to January 30, 2013 was used for all runs during this study. Any patient below eighteen years of age was considered pediatric for use in this study. This study also used the updated case cart washer configuration where the washer capacity is: Two large carts Four small carts One large and two small carts 52
 N/3 Voting (30 items/each person votes for 10 items) Must/Want Matrix (assign")
53 Prioritize Solutions Some solutions are easier to implement than others Some solutions are more expensive than others Some solutions have a bigger impact than others It is impossible to implement everything at once Tools: Pay-off Matrix (Benefit VS Effort) N/3 Voting (30 items/each person votes for 10 items) Must/Want Matrix (assign weights/quantify) 53
54 Prioritize Solutions A Pay-Off Matrix looks at the relationship of benefit and effort to reduce the number of solutions to address High Pursue Rescope / Reconsider Benefit Low Eliminate Eliminate Low High Effort 54
55 Pay-off Matrix Example Example: Improving Admission Cycle Time Redo admission into simpler form Develop new software system for registration/admission desk High Streamline packet completion step Benefit Low Call patients before completing admission Develop new training course for all employees Low Effort High 55

56 Pilot Pilots are important when: The scope of change is large Change could cause far-reaching unintended consequences Implementing the change will be a costly process Change would be difficult to reverse Test part or all of a proposed solution on a small scale It helps to better understand the effects of a change We learn how to make full scale implementation more effective 56
57 Investigation into Three Possible Pediatric Configurations Results - The key metrics of patient cycle time and PACU closing times are shown in the table below. Monthly Through put Patient Cycle Time Normal PACU Close Time Normal Late Close Time Scenario Name Current State MOR patient :30 PM Midnight Current State SDS patient :30 Current State peds patient :30 AM 1:00 PM All Recovery Seventh Floor MOR patient :30 PM 11:30 PM All Recovery Seventh Floor SDS patient :30 PM All Recovery Seventh Floor peds patient :00 PM 4:00 PM 1st Stage Recovery Seventh Floor MOR patient :45 PM 1:00 AM 1st Stage Recovery Seventh Floor SDS patient :30 PM 1st Stage Recovery Seventh Floor peds patient :30 PM 5:30 PM 1st Stage Recovery Seventh Floor With Revised Elevator Assignments MOR patient :30 PM 12:30 AM 1st Stage Recovery Seventh Floor With Revised Elevator Assignments SDS patient :30 PM 1st Stage Recovery Seventh Floor With Revised Elevator Assignments peds patient :45 PM 4:40 PM 57
58 Investigation into Three Possible Pediatric Configurations The most effective performing scenario is that with all Pediatric recovery occurring on the seventh floor. This scenario avoids contention for pediatric PACU beds between pre-operative and postoperative patients. Splitting the pediatric recovery between the first and seventh floor so that stage two occurs in the main OR floor increases the patient cycle time and the PACU closing times due to the transport for pediatric inpatients and the effect of reducing the ability to flex PACU to beds in this space. Reassigning the elevator transports to alleviate the elevator congestion reduces some amount of the impact but does not eliminate this reduction in efficiency versus having all pediatric recovery in one space. 58
59 Investigation into Three Possible Pediatric Configurations These configurations also affect the number and utilization of the case carts. This result is shown below. Scenario Large Carts Small Carts Cart Utilization Current State % All Recovery Seventh Floor % 1st Stage Recovery Seventh Floor % 1st Stage Recovery Seventh Floor With Revised Elevator Assignments % 59
60 Control / Impact Matrix High Medium Low Implementation of standardized order sets Turnaround time of echo Documentation of ACE/ARB In Control Selection of correct CareMap Consultations Initiation of D/C planning Documentation of echo Discharge disposition Out of Control Compliance of MD to utilize standardized order set Comorbidities Compliance of use of CareMap Necessity of needing echo during hospitalization Patient compliance to follow-up care Patient resistance to D/C Support system 60
61 Investigation into Three Possible Pediatric Configurations The split recovery configurations also take a higher level of labor due to the extra inefficiency of the transport. This is shown in the table below. Scenario Name Work Time (HR/Month) Difference (Hr/Month) Difference (%) All Recovery Seventh Floor ORRN All Recovery Seventh Floor PACURN All Recovery Seventh Floor PreOpHoldingRN All Recovery Seventh Floor Stage1RN All Recovery Seventh Floor Stage2RN All Recovery Seventh Floor PreOpRn All Recovery Seventh Floor pedsor rn All Recovery Seventh Floor pedspacu rn Total Direct Work Hours st Stage Recovery Seventh Floor ORRN % 1st Stage Recovery Seventh Floor PACURN % 1st Stage Recovery Seventh Floor PreOpHoldingRN % 1st Stage Recovery Seventh Floor Stage1RN % 1st Stage Recovery Seventh Floor Stage2RN % 1st Stage Recovery Seventh Floor PreOpRn % 1st Stage Recovery Seventh Floor pedsor rn % 1st Stage Recovery Seventh Floor pedspacu rn % Total Direct Work Hours % 1st Stage Recovery Seventh Floor With Revised Elevator Assignments ORRN % 1st Stage Recovery Seventh Floor With Revised 61 Elevator Assignments PACURN % 1st Stage Recovery Seventh Floor With
62 Investigation into Three Possible Pediatric Configurations Conclusions The configuration with pediatric pre-op in the main OR area and all pediatric recovery occurring on the seventh floor is the most efficient since it minimizes the elevator use and avoids contention for bed space in the seventh floor complex between incoming preoperative patients and outgoing post-operative patients. This option demonstrates superior metrics in the following areas versus the other two options: Lower overall patient cycle time for all patients including Pediatric patients Lower number of Class P patients that exceed the 120 minute threshold Lower patient hold times due to higher efficiency of Phase I and II recovery in the same physical space Lower number of case carts required to support the ORs in total The revision to the case cart process showed a marked decrease in the number of case carts required to support the ORs using the most recent volumes. This analysis shows that approximately 40 large carts and 26 small carts are required to ensure no delays due to unavailability of case carts. The case carts and case cart washer remain an area of concern. All possible measures need to be taken to ensure the reliability and uptime of the cart washer. 62
63 63 Simulation

64 64
65 Simulation Model found that the cart washer was an important point of failure Model found the best set of PACU changes to reduce OR hold time Model verified multiple staffing changes Model found the optimum set of changes to OR assignments Model verified smoothed OR schedule to improve patient flow through the OR suite and into inpatient units Model verified that current and next year projected volumes could be handled by the new configuration Model determined the volume increase that could be tolerated without further changes Model found the elevators to Seventh Floor to be problematic without usage policies in place 65
66 66 Simulation Inputs
67 Pediatric Suite OR Close Time Five Rooms Close at 1:30 PM Four Rooms Close at 3:00 PM Three Rooms Close at 5:00 PM 67
68 Investigation into Three Possible Pediatric Configurations 1. Pediatric patients would check into Pre-op on the first floor complex, then are transported Main OR area on the seventh floor using the back elevators, receive their procedure in seventh floor OR suite, recover in the seventh floor PACU for Phase I & Phase II and either depart home or move to an inpatient room from the seventh floor PACU. 2. Pediatric patients would check into the Pre-Op Area on the seventh floor complex using the back elevators, receive their procedure in seventh floor OR suite, then from the OR Suite patients will move to the Phase I PACU on the seventh floor, then be transported downstairs via the back elevators to Phase II recovery on the first floor. Finally, patients will either depart from Phase II PACU to inpatient unit or home. 3. Pediatric patients would check into the Pre-Op area on the seventh floor complex using the main elevators, receive their procedure in seventh floor OR suite, then from the OR Suite patients will move to the Phase I PACU on the seventh floor, then be transported downstairs via the back elevators to Phase II recovery on the first floor. Finally, patients will either depart from Phase II PACU to inpatient unit or home. 68
69 Results of project Learned which patient types and surgery types caused the most disruption in flow and the length of OR hold times by patient type. In particular, the model indicated that the PACU areas were the major limiting factor and constraint to OR flow. The OR suite simulation output significantly affected the decision making process and was used to determine which actions were needed to take regarding the PACU areas. 69
70 Investigation into Three Possible Pediatric Configurations Results The most effective performing scenario is that with all Pediatric recovery occurring on the seventh floor. This scenario avoids contention for pediatric PACU beds between pre-operative and postoperative patients. Splitting the pediatric recovery between the first and seventh floor so that stage two occurs in the main OR floor increases the patient cycle time and the PACU closing times due to the transport for pediatric inpatients and the effect of reducing the ability to flex PACU to beds in this space. Reassigning the elevator transports to alleviate the elevator congestion reduces some amount of the impact but does not eliminate this reduction in efficiency versus having all pediatric recovery in one space. 70
71 71 Appendix
72 Problem Statement Examples Poor Example: Under skilled staff takes too long to prepare and distribute Radiology reports. Updated training is needed. Improved Example: 60% of all Radiology reports over the past year have been delivered beyond 24 hours after exam at Speedy Medical Center. The result has been delayed diagnosis by our Radiologists and delayed treatment for our patients. Poor Example: ER is understaffed, causing patients to wait too long for treatment. This is making ER turnaround too long. Improved Example: ER patients are spending about 3 hours in ER before either being released or admitted. Time in ER is especially long during the hours between 10 AM and 1 PM. The long time issue is causing many patients & physicians to complain. 72
Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting
 Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting How many times have we heard that it s easy to apply Lean and Six Sigma techniques to hospital processes, and specifically
Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting How many times have we heard that it s easy to apply Lean and Six Sigma techniques to hospital processes, and specifically
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation
 Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Webinar: Practical Approaches to Improving Patient Pre-Op Preparation Your Presenters Michael Hicks, MD, MBA, FACHE Chief Executive Officer EmCare Anesthesia Services Lisa Kerich, PA-C Vice President Clinical
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Measure: Current State Spaghetti Diagram
 Visual representation of process Measure: Current State Spaghetti Diagram Registration Triage Nursing Station Walk In Patient Total Time - 4:52 Entry to Triage 45min Triage to Bed-1:30 Bed to Disposition-2:35
Visual representation of process Measure: Current State Spaghetti Diagram Registration Triage Nursing Station Walk In Patient Total Time - 4:52 Entry to Triage 45min Triage to Bed-1:30 Bed to Disposition-2:35
Michigan Medicine--Frankel Cardiovascular Center. Determining Direct Patient Utilization Costs in the Cardiovascular Clinic.
 Michigan Medicine--Frankel Cardiovascular Center Clinical Design and Innovation Determining Direct Patient Utilization Costs in the Cardiovascular Clinic Final Report Client: Mrs. Cathy Twu-Wong Project
Michigan Medicine--Frankel Cardiovascular Center Clinical Design and Innovation Determining Direct Patient Utilization Costs in the Cardiovascular Clinic Final Report Client: Mrs. Cathy Twu-Wong Project
Lean Six Sigma DMAIC Project (Example)
") Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Financial Disclosure. Learning Objectives. Reducing GI Surgery Re-Admissions, While Increasing Patient Satisfaction
 Reducing GI Surgery Re-Admissions, While Increasing Patient Satisfaction Michelle Guibault, BSN, BS, RN Co-Author: D. Leigh Webb, MPH, CTR WellStar Health System, Marietta, GA Nothing to disclose Financial
Reducing GI Surgery Re-Admissions, While Increasing Patient Satisfaction Michelle Guibault, BSN, BS, RN Co-Author: D. Leigh Webb, MPH, CTR WellStar Health System, Marietta, GA Nothing to disclose Financial
ATTACKING WASTE AND VARIATION HOSPITAL-WIDE: A COMPREHENSIVE LEAN SIGMA DEPLOYMENT
 ATTACKING WASTE AND VARIATION HOSPITAL-WIDE: A COMPREHENSIVE LEAN SIGMA DEPLOYMENT Charles Johnson, Ph.D., Richard H. Allen, Dr.P.H., Thomas A. Sonderman, M.D., and Ian D. Wedgwood, Ph.D. Abstract Columbus
ATTACKING WASTE AND VARIATION HOSPITAL-WIDE: A COMPREHENSIVE LEAN SIGMA DEPLOYMENT Charles Johnson, Ph.D., Richard H. Allen, Dr.P.H., Thomas A. Sonderman, M.D., and Ian D. Wedgwood, Ph.D. Abstract Columbus
Improving Mott Hospital Post-Operative Processes
 Improving Mott Hospital Post-Operative Processes Program and Operation Analysis Submitted To: Sheila Trouten, Client Nurse Manager, PACU, Mott OR Jesse Wilson, Coordinator Administrative Manager of Surgical
Improving Mott Hospital Post-Operative Processes Program and Operation Analysis Submitted To: Sheila Trouten, Client Nurse Manager, PACU, Mott OR Jesse Wilson, Coordinator Administrative Manager of Surgical
Inpatient Flow Real Time Demand Capacity: Building the System
 Inpatient Flow Real Time Demand Capacity: Building the System Roger Resar, MD, Kevin Nolan, and Deb Kaczynski We would like to acknowledge the conceptual contributions of Diane Jacobsen, Marilyn Rudolph,
Inpatient Flow Real Time Demand Capacity: Building the System Roger Resar, MD, Kevin Nolan, and Deb Kaczynski We would like to acknowledge the conceptual contributions of Diane Jacobsen, Marilyn Rudolph,
The Path to Sustainable Improvements
 What Do You Do When Your Improvement Project FAILS? The Path to Sustainable Improvements Thursday, March 3, 2016 10:00 AM Reza Ziaee, MA, MSE, MBB, PhD, FHIMSS - Antelope Valley Hospital James Bologna
What Do You Do When Your Improvement Project FAILS? The Path to Sustainable Improvements Thursday, March 3, 2016 10:00 AM Reza Ziaee, MA, MSE, MBB, PhD, FHIMSS - Antelope Valley Hospital James Bologna
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Healthcare Finance Management Association: Continuous Improvement Foundations
 Like us on Facebook and enjoy some helpful downloads and connections Continuous Improvement Solutions, LLC 8801 Bethnal Rd., Bella Vista, AR 72714 479.685.8380 cisolutionsllp@gmail.com Chad Smith: Trainer,
Like us on Facebook and enjoy some helpful downloads and connections Continuous Improvement Solutions, LLC 8801 Bethnal Rd., Bella Vista, AR 72714 479.685.8380 cisolutionsllp@gmail.com Chad Smith: Trainer,
Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA
 These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
Operational Excellence at Lifespan. Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence
 Operational Excellence at Lifespan Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence Objectives Discuss Lifespan s approach to establishing a system-based quality structure Describe the organization
Operational Excellence at Lifespan Sharon Tripp RN, MS, CPHQ Director of Clinical Excellence Objectives Discuss Lifespan s approach to establishing a system-based quality structure Describe the organization
Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience
 University of Michigan Health System Program and Operations Analysis Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience Final Report To: Stephen Napolitan, Assistant
University of Michigan Health System Program and Operations Analysis Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience Final Report To: Stephen Napolitan, Assistant
The Process Innovation Center at CHOP: An Inside View
 The Process Innovation Center at CHOP: An Inside View Harold Strawbridge HIMSS Management Engineering Performance Improvement Task Force, April, 2007 The Children s Hospital of Philadelphia Introductions
The Process Innovation Center at CHOP: An Inside View Harold Strawbridge HIMSS Management Engineering Performance Improvement Task Force, April, 2007 The Children s Hospital of Philadelphia Introductions
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
Tools & Resources for QI Success
 Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Enhancing Efficiency and Communication in Perioperative Services Through Technology
 Enhancing Efficiency and Communication in Perioperative Services Through Technology Linda Yoder, RN, BSN, MBA, Clinical Director, Perioperative Services, GI Lab, Cross Creek Ambulatory Center Every driver
Enhancing Efficiency and Communication in Perioperative Services Through Technology Linda Yoder, RN, BSN, MBA, Clinical Director, Perioperative Services, GI Lab, Cross Creek Ambulatory Center Every driver
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
THE USE OF SIMULATION TO DETERMINE MAXIMUM CAPACITY IN THE SURGICAL SUITE OPERATING ROOM. Sarah M. Ballard Michael E. Kuhl
 Proceedings of the 2006 Winter Simulation Conference L. F. Perrone, F. P. Wieland, J. Liu, B. G. Lawson, D. M. Nicol, and R. M. Fujimoto, eds. THE USE OF SIMULATION TO DETERMINE MAXIMUM CAPACITY IN THE
Proceedings of the 2006 Winter Simulation Conference L. F. Perrone, F. P. Wieland, J. Liu, B. G. Lawson, D. M. Nicol, and R. M. Fujimoto, eds. THE USE OF SIMULATION TO DETERMINE MAXIMUM CAPACITY IN THE
Improving operating room efficiency through the use of lean six sigma methodologies. Teodora O. Nicolescu
 Improving operating room efficiency through the use of lean six sigma methodologies Teodora O. Nicolescu Author detail: Teodora O. Nicolescu, MD Associate Professor Department of Anesthesiology The University
Improving operating room efficiency through the use of lean six sigma methodologies Teodora O. Nicolescu Author detail: Teodora O. Nicolescu, MD Associate Professor Department of Anesthesiology The University
Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty
 Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Examining a range of
Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Examining a range of
Creating a No Wait ED
 This presenter has nothing to disclose Creating a No Wait ED Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Process Improvement
This presenter has nothing to disclose Creating a No Wait ED Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Process Improvement
University of Michigan Health System. Inpatient Tracking Analysis and Process Standardization at. Mott Children s and Women s Hospital.
 University of Michigan Health System Program and Operations Analysis Inpatient Tracking Analysis and Process Standardization at Mott Children s and Women s Hospital Final Report Team 6 To: Perry Spencer,
University of Michigan Health System Program and Operations Analysis Inpatient Tracking Analysis and Process Standardization at Mott Children s and Women s Hospital Final Report Team 6 To: Perry Spencer,
Quality Management and Accreditation
 Quality Management and Accreditation Lina Mekawi, RPh, MS Epidemiology, CPHQ, Senior Quality Analyst, Quality, Accreditation and Risk Management Department, AUBMC November 2017 Disclosure Slide I, Lina
Quality Management and Accreditation Lina Mekawi, RPh, MS Epidemiology, CPHQ, Senior Quality Analyst, Quality, Accreditation and Risk Management Department, AUBMC November 2017 Disclosure Slide I, Lina
University of Michigan Health System. Program and Operations Analysis. CSR Staffing Process. Final Report
 University of Michigan Health System Program and Operations Analysis CSR Staffing Process Final Report To: Jean Shlafer, Director, Central Staffing Resources, Admissions Bed Coordination Center Amanda
University of Michigan Health System Program and Operations Analysis CSR Staffing Process Final Report To: Jean Shlafer, Director, Central Staffing Resources, Admissions Bed Coordination Center Amanda
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION
 UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION II UTILIZING LEAN MANAGEMENT PRINCIPLES DURING A MEDITECH 6.1 IMPLEMENTATION EXECUTIVE SUMMARY Healthcare may be the only industry
Quality Assurance and Performance Improvement (QAPI)
") Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
Quality Assurance and Performance Improvement () Carol Hill, MSN, RN, RAC-MT, DNS-CT, QCP-MT, CPC Objectives Identify the 5 key elements that form the framework of a program Recognize process tools that
Final Report. Karen Keast Director of Clinical Operations. Jacquelynn Lapinski Senior Management Engineer
 Assessment of Room Utilization of the Interventional Radiology Division at the University of Michigan Hospital Final Report University of Michigan Health Systems Karen Keast Director of Clinical Operations
Assessment of Room Utilization of the Interventional Radiology Division at the University of Michigan Hospital Final Report University of Michigan Health Systems Karen Keast Director of Clinical Operations
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
IS YOUR QAPI COP READY?
 IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care
 Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Part 4. Change Concepts for Improving Adult Cardiac Surgery. In this section, you will learn a group. of change concepts that can be applied in
 Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
University of Michigan Health System Program and Operations Analysis. Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients
 University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
Gantt Chart. Critical Path Method 9/23/2013. Some of the common tools that managers use to create operational plan
 Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Some of the common tools that managers use to create operational plan Gantt Chart The Gantt chart is useful for planning and scheduling projects. It allows the manager to assess how long a project should
Practical Applications on Efficiency
 Practical Applications on Efficiency Maryland MGMA September 19, 214 Owen J. Dahl, FACHE, LSSMBB Objectives To offer practical scenarios for the application of Lean Tools in YOUR practice To discuss and
Practical Applications on Efficiency Maryland MGMA September 19, 214 Owen J. Dahl, FACHE, LSSMBB Objectives To offer practical scenarios for the application of Lean Tools in YOUR practice To discuss and
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
uncovering key data points to improve OR profitability
 REPRINT March 2014 Robert A. Stiefel Howard Greenfield healthcare financial management association hfma.org uncovering key data points to improve OR profitability Hospital finance leaders can increase
REPRINT March 2014 Robert A. Stiefel Howard Greenfield healthcare financial management association hfma.org uncovering key data points to improve OR profitability Hospital finance leaders can increase
Directing and Controlling
 NUR 462 Principles of Nursing Administration Directing and Controlling (Leibler: Chapter 7) Dr. Ibtihal Almakhzoomy March 2007 Dr. Ibtihal Almakhzoomy Directing and Controlling Define the management function
NUR 462 Principles of Nursing Administration Directing and Controlling (Leibler: Chapter 7) Dr. Ibtihal Almakhzoomy March 2007 Dr. Ibtihal Almakhzoomy Directing and Controlling Define the management function
Decreasing Environmental Services Response Times
 Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
(Muda) Objectives. Determine what is Value added vs. Non-Value added. Identify the eight types of waste. Understand the Barriers to.
 Objectives. Determine what is Value added vs. Non-Value added. Identify the eight types of waste. Understand the Barriers to.") Identifying Waste (Muda) Erika Sundrud, MA AVP Quality, Safety & Performance Improvement 1 Objectives Determine what is Value added vs. Non-Value added Identify the eight types of waste Understand the
Identifying Waste (Muda) Erika Sundrud, MA AVP Quality, Safety & Performance Improvement 1 Objectives Determine what is Value added vs. Non-Value added Identify the eight types of waste Understand the
University of Michigan Comprehensive Stroke Center
 University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
Bringin it to the Bedside: Staff-Driven Savings
 Bringin it to the Bedside: Staff-Driven Savings Jackie Noll, MSN, RN, CEN, Senior Director of Nursing, The Children s Hospital of Philadelphia (CHOP) Amy Gallagher, MS, PharmD, Senior Director of Home
Bringin it to the Bedside: Staff-Driven Savings Jackie Noll, MSN, RN, CEN, Senior Director of Nursing, The Children s Hospital of Philadelphia (CHOP) Amy Gallagher, MS, PharmD, Senior Director of Home
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health
 REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
Operational Assessments: Utilizing Productivity Standards
 Operational Assessments: Utilizing Productivity Standards Mary Klimp CEO Queen of Peace Hospital 952.758.8101 mklimp@qofp.org Ross Manson Principal Eide Bailly 701.239.8634 rmanson@eidebailly.com Agenda
Operational Assessments: Utilizing Productivity Standards Mary Klimp CEO Queen of Peace Hospital 952.758.8101 mklimp@qofp.org Ross Manson Principal Eide Bailly 701.239.8634 rmanson@eidebailly.com Agenda
Partnerships- Cooperation with other care providers that is guided by open communication, trust, and shared decision-making.
 1 E P 7: Describe and demonstrate the structure(s) and process(es) used to engage internal experts and external consultants to improve care in the practice setting. When Riverside nurses from any level
1 E P 7: Describe and demonstrate the structure(s) and process(es) used to engage internal experts and external consultants to improve care in the practice setting. When Riverside nurses from any level
Take These Actions to Immediately Improve Patient Throughput
 Take These Actions to Immediately Improve Patient Throughput Webinar October 2, 2017 10:00 AM CST Results Delivered. Performance Improved. Presenters Bonnie Barndt-Maglio, RN, PhD Managing Director Prism
Take These Actions to Immediately Improve Patient Throughput Webinar October 2, 2017 10:00 AM CST Results Delivered. Performance Improved. Presenters Bonnie Barndt-Maglio, RN, PhD Managing Director Prism
Moving the Needle on Hospital Throughput: Breaking Through the Status Quo. Session ID: 325
 Moving the Needle on Hospital Throughput: Breaking Through the Status Quo Session ID: 325 Objectives Objective 1: Demonstrate how two common strategies can be deployed to maximum benefit to support improvements
Moving the Needle on Hospital Throughput: Breaking Through the Status Quo Session ID: 325 Objectives Objective 1: Demonstrate how two common strategies can be deployed to maximum benefit to support improvements
Matching Capacity and Demand:
 We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
Impact of Scribes on Performance Indicators in the Emergency Department
 CLINICAL PRACTICE Impact of Scribes on Performance Indicators in the Emergency Department Rajiv Arya, MD, Danielle M. Salovich, Pamela Ohman-Strickland, PhD, and Mark A. Merlin, DO Abstract Objectives:
CLINICAL PRACTICE Impact of Scribes on Performance Indicators in the Emergency Department Rajiv Arya, MD, Danielle M. Salovich, Pamela Ohman-Strickland, PhD, and Mark A. Merlin, DO Abstract Objectives:
A Publication for Hospital and Health System Professionals
 A Publication for Hospital and Health System Professionals S U M M E R 2 0 0 8 V O L U M E 6, I S S U E 2 Data for Healthcare Improvement Developing and Applying Avoidable Delay Tracking Working with Difficult
A Publication for Hospital and Health System Professionals S U M M E R 2 0 0 8 V O L U M E 6, I S S U E 2 Data for Healthcare Improvement Developing and Applying Avoidable Delay Tracking Working with Difficult
Optum Anesthesia. Completely integrated anesthesia information management system
 Optum Anesthesia Completely integrated anesthesia information management system 2 Completely integrated anesthesia information management system Optum Anesthesia Information Management System (AIMS) helps
Optum Anesthesia Completely integrated anesthesia information management system 2 Completely integrated anesthesia information management system Optum Anesthesia Information Management System (AIMS) helps
Driving Out Clinical Variation to Drive Up Your Bottom Line
 In Cooperation With: Executive White Paper Series, October 2017 Driving Out Clinical Variation to Drive Up Your Bottom Line Hospitals have always worked to be efficient. Now more than ever, it is increasingly
In Cooperation With: Executive White Paper Series, October 2017 Driving Out Clinical Variation to Drive Up Your Bottom Line Hospitals have always worked to be efficient. Now more than ever, it is increasingly
An Implementation Framework for Patient Safety in Ambulatory Care. To disseminate key findings from IHI s work on ambulatory safety
 An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
Analysis of Nursing Workload in Primary Care
 Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Fast Track Development at Aultman Hospital
 Fast Track Development at Aultman Hospital Academy for Excellence in Healthcare IAP C-12 Aultman Jan. 17, 2018 fisher.osu.edu 1 Fast Track Development Aultman Hospital improves ED turnaround times, patient
Fast Track Development at Aultman Hospital Academy for Excellence in Healthcare IAP C-12 Aultman Jan. 17, 2018 fisher.osu.edu 1 Fast Track Development Aultman Hospital improves ED turnaround times, patient
Introduction. Staffing to demand increases bottom line revenue for the facility through increased volume and throughput and elimination of waste.
 Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Critical Success Factors for Becoming a High Reliability Organization: Lean, Six Sigma, Change Leadership and Value-based Purchasing
 AHA Leadership Summit Critical Success Factors for Becoming a High Reliability Organization: Lean, Six Sigma, Change Leadership and Value-based Purchasing Presented by: Patty Toney, VP/Chief Nurse Executive,
AHA Leadership Summit Critical Success Factors for Becoming a High Reliability Organization: Lean, Six Sigma, Change Leadership and Value-based Purchasing Presented by: Patty Toney, VP/Chief Nurse Executive,
An Implementation Framework for Patient Safety in Ambulatory Care
 An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
4.09. Hospitals Management and Use of Surgical Facilities. Chapter 4 Section. Background. Follow-up on VFM Section 3.09, 2007 Annual Report
 Chapter 4 Section 4.09 Hospitals Management and Use of Surgical Facilities Follow-up on VFM Section 3.09, 2007 Annual Report Background Ontario s public hospitals are generally governed by a board of directors
Chapter 4 Section 4.09 Hospitals Management and Use of Surgical Facilities Follow-up on VFM Section 3.09, 2007 Annual Report Background Ontario s public hospitals are generally governed by a board of directors
Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic. Final Report
 Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic Final Report Prepared for: Kathy Lash, Director of Operations University of Michigan Health System Radiation Oncology
Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic Final Report Prepared for: Kathy Lash, Director of Operations University of Michigan Health System Radiation Oncology
A Comprehensive Framework for Patient Safety, Reliability and Clinical Excellence
 14 November 2016 Oslo, Norway A Comprehensive Framework for Patient, and Clinical Excellence Frank Federico A Framework 1. Link safety and reliability to organizational strategy and resources 2. Define
14 November 2016 Oslo, Norway A Comprehensive Framework for Patient, and Clinical Excellence Frank Federico A Framework 1. Link safety and reliability to organizational strategy and resources 2. Define
Getting the right case in the right room at the right time is the goal for every
 OR throughput Are your operating rooms efficient? Getting the right case in the right room at the right time is the goal for every OR director. Often, though, defining how well the OR suite runs depends
OR throughput Are your operating rooms efficient? Getting the right case in the right room at the right time is the goal for every OR director. Often, though, defining how well the OR suite runs depends
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process. Final Report
 University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process Final Report Submitted to: Ms. Angela Haley Ambulatory Care Manager, Department of Surgery 1540 E Medical
University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process Final Report Submitted to: Ms. Angela Haley Ambulatory Care Manager, Department of Surgery 1540 E Medical
How Allina Saved $13 Million By Optimizing Length of Stay
 Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE
 Publication Year: 2011 TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE Summary: The Team Assessment Pull Process (TAPP) is a technique to redesign emergency department patient
Publication Year: 2011 TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE Summary: The Team Assessment Pull Process (TAPP) is a technique to redesign emergency department patient
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
"Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital
 "Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital The University of Kansas Hospital Leading the Nation in Caring, Healing,
"Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital The University of Kansas Hospital Leading the Nation in Caring, Healing,
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
Using Lean Principles to Decrease Outpatient Registration Wait Times. It s a Journey not a Destination
 Using Lean Principles to Decrease Wait Times It s a Journey not a Destination 533 Bed Acute Care System 461 Beds at AnMed Health Medical Center 72 Beds at AnMed Health Women s and Children's Hospital 45
Using Lean Principles to Decrease Wait Times It s a Journey not a Destination 533 Bed Acute Care System 461 Beds at AnMed Health Medical Center 72 Beds at AnMed Health Women s and Children's Hospital 45
Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report
 Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
DELIVERING OUTSTANDING IMPROVEMENTS AT CANADA S WILLIAM OSLER HEALTHCARE SYSTEM
 DELIVERING OUTSTANDING IMPROVEMENTS AT CANADA S WILLIAM OSLER HEALTHCARE SYSTEM White Paper: William Osler Health System Diabetes Education Centre Brampton, Ontario Diabetes clinic pilot project expands
DELIVERING OUTSTANDING IMPROVEMENTS AT CANADA S WILLIAM OSLER HEALTHCARE SYSTEM White Paper: William Osler Health System Diabetes Education Centre Brampton, Ontario Diabetes clinic pilot project expands
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
World Health Organization Male Circumcision Quality Assurance Workshop 2010
 Male Circumcision Quality Assurance Workshop World Health Organization 1 DAY 3 2 Giving Feedback: The Debriefing Assessment team determines information to share Relate comments to the specific standard
Male Circumcision Quality Assurance Workshop World Health Organization 1 DAY 3 2 Giving Feedback: The Debriefing Assessment team determines information to share Relate comments to the specific standard
Clinical Operations in a Service Line Model
 Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
Clinical Operations in a Service Line Model John D Angelo, MD, FACEP Executive Director & Senior Vice President Sarah Healey Herod, MPH Director, Service Line Development Jill Castaneda Project Manager,
Major Areas of Focus for the Financial Risk of ICD-10 to Providers. From Imperative to Implementation: Collaboration in ICD-10 Planning & Adoption
 Major Areas of Focus for the Financial Risk of ICD-10 to Providers From Imperative to Implementation: Collaboration in ICD-10 Planning & Adoption Meeting with You Today Walter Houlihan Director of Health
Major Areas of Focus for the Financial Risk of ICD-10 to Providers From Imperative to Implementation: Collaboration in ICD-10 Planning & Adoption Meeting with You Today Walter Houlihan Director of Health
Demand and capacity models High complexity model user guidance
 Demand and capacity models High complexity model user guidance August 2018 Published by NHS Improvement and NHS England Contents 1. What is the demand and capacity high complexity model?... 2 2. Methodology...
Demand and capacity models High complexity model user guidance August 2018 Published by NHS Improvement and NHS England Contents 1. What is the demand and capacity high complexity model?... 2 2. Methodology...
Emergency Services. Time Study
 Prepared for: Peter Forster Management Systems University of Michigan Hospitals December 18,1991 by: Associate Hospital Administrator Emergency Services Ann Arbor, MI Don Suffivan Jeremy Roberts Lisa Clayton
Prepared for: Peter Forster Management Systems University of Michigan Hospitals December 18,1991 by: Associate Hospital Administrator Emergency Services Ann Arbor, MI Don Suffivan Jeremy Roberts Lisa Clayton
PERIOPERATIVE CONSULTING SERVICES
 SPT Sourcing PERIOPERATIVE CONSULTING SERVICES Improve efficiency and financial savings. Surgical Supply Management Solutions Keep everyone in-sync and in control with THE RIGHT SUPPLIES AT THE RIGHT TIME.
SPT Sourcing PERIOPERATIVE CONSULTING SERVICES Improve efficiency and financial savings. Surgical Supply Management Solutions Keep everyone in-sync and in control with THE RIGHT SUPPLIES AT THE RIGHT TIME.
Project Request and Approval Process
 The University of the District of Columbia Information Technology Project Request and Approval Process Kia Xiong Information Technology Projects Manager 13 June 2017 Table of Contents Project Management
The University of the District of Columbia Information Technology Project Request and Approval Process Kia Xiong Information Technology Projects Manager 13 June 2017 Table of Contents Project Management
Grand River Hospital and St Mary s General Hospital Increases Throughput, Cuts Costs using Lean
 LEAN CASE STUDY: Grand River Hospital and St Mary s General Hospital Increases Throughput, Cuts Costs using Lean In healthcare today, having to do more with less goes with the territory. Volumes are increasing
LEAN CASE STUDY: Grand River Hospital and St Mary s General Hospital Increases Throughput, Cuts Costs using Lean In healthcare today, having to do more with less goes with the territory. Volumes are increasing
University of Michigan Emergency Department
 University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
Hospital Patient Flow Capacity Planning Simulation Model at Vancouver Coastal Health
 Hospital Patient Flow Capacity Planning Simulation Model at Vancouver Coastal Health Amanda Yuen, Hongtu Ernest Wu Decision Support, Vancouver Coastal Health Vancouver, BC, Canada Abstract In order to
Hospital Patient Flow Capacity Planning Simulation Model at Vancouver Coastal Health Amanda Yuen, Hongtu Ernest Wu Decision Support, Vancouver Coastal Health Vancouver, BC, Canada Abstract In order to
University of Michigan Health System. Current State Analysis of the Main Adult Emergency Department
 University of Michigan Health System Program and Operations Analysis Current State Analysis of the Main Adult Emergency Department Final Report To: Jeff Desmond MD, Clinical Operations Manager Emergency
University of Michigan Health System Program and Operations Analysis Current State Analysis of the Main Adult Emergency Department Final Report To: Jeff Desmond MD, Clinical Operations Manager Emergency
Thinking of Going Lean? A 360-degree view of changing the culture of a healthcare system through a Lean Transformation
 Thinking of Going Lean? A 360-degree view of changing the culture of a healthcare system through a Lean Transformation AHA Leadership Summit Thursday, July 27, 2017 Please note that the views expressed
Thinking of Going Lean? A 360-degree view of changing the culture of a healthcare system through a Lean Transformation AHA Leadership Summit Thursday, July 27, 2017 Please note that the views expressed
ICD-10 Advantages to Providers Looking beyond the isolated patient provider encounter
 A Health Data Consulting White Paper 1056 6th Ave S Edmonds, WA 98020-4035 206-478-8227 www.healthdataconsulting.com ICD-10 Advantages to Providers Looking beyond the isolated patient provider encounter
A Health Data Consulting White Paper 1056 6th Ave S Edmonds, WA 98020-4035 206-478-8227 www.healthdataconsulting.com ICD-10 Advantages to Providers Looking beyond the isolated patient provider encounter
Basic Skills for CAH Quality Managers
 Basic Skills for CAH Quality Managers MARCH 20, 2014 THE BASICS OF DATA MANAGEMENT Data Management Systems COLLECTION AGGREGATION ASSESSMENT REPORTING 1 Some Data Management Terminology Objective data
Basic Skills for CAH Quality Managers MARCH 20, 2014 THE BASICS OF DATA MANAGEMENT Data Management Systems COLLECTION AGGREGATION ASSESSMENT REPORTING 1 Some Data Management Terminology Objective data