University of Michigan Health System. Inpatient Tracking Analysis and Process Standardization at. Mott Children s and Women s Hospital.
|
|
|
- Rosalind Henry
- 6 years ago
- Views:
Transcription
1 University of Michigan Health System Program and Operations Analysis Inpatient Tracking Analysis and Process Standardization at Mott Children s and Women s Hospital Final Report Team 6 To: Perry Spencer, Manager of Security Operations Jackie Lapinski, Project Manager, Children s and Women s Project Mark Van Oyen, Professor, IOE 481 From: IOE 481 Student Project Team, Program and Operations Analysis Emily Andrews Emily Hammond Kyle Petersmark Date: December 1, 2009
2 Table of Contents Executive Summary 3 Introduction 5 Background and Current Situation 5 Approach and Methodology 7 Findings and Conclusions 9 Figure1: Hugs Alarms Locations 11 Figure 2: Causes of Hugs Alarms 12 Figure 3: Patient Transportation Destination Frequency 13 Figure 4: Parent Survey on Hugs Comprehensiveness 14 Figure 5: Parent Survey on Security Expectations 15 Figure 6: Parent Survey on Guidelines 16 Figure 7-13: Current State Maps 17 Figure 14: Five Why s Analysis 21 Figure 15: Impact vs. Effort 23 Recommendations and Implementation 23 Figure 16: Future State Map 24 Figure 17: Parent Information Card- Front Side 25 Figure 18: Standardized Transportation Form 26 Figure 19: Sample Sign-Out / Sign-In Log 26 Figure 20: Responsibility Matrix 27 Appendix A: Literature Search References 29 Appendix B: Patient Transportation Forms 30 Appendix C: Sample Interview Questions 40 Appendix D: Unit Sign-Out/ Sign-In Logs 41 Appendix E: Full Size Value Stream Maps 43 2
3 Executive Summary In a children s hospital, the security of patients is the responsibility of the hospital. Therefore, tracking the whereabouts of admitted patients is an important security function for a children s hospital. The inpatient tracking process at Mott Children s and Women s Hospital is not standard. When a patient needs to leave the floor, the process each unit uses to track the location of inpatients is subject to great variation. This variation and lack of standardization can lead to miscommunication and a decrease in overall patient safety. An IOE 481 team was asked to capture and analyze the current inpatient tracking process used at Mott Hospital, and to then develop recommendations to standardize and improve the transportation process. Mott Children s and Women s Hospital currently has 198 inpatient beds. Children under the age of two years old, along with patients labeled as high risk, are banded with a bracelet called a Hugs tag. This tag activates an alarm if the patient is taken off the floor. Patients who do not have a Hugs tag are not being tracked. The team looked at the inpatient tracking process for both Hugs tag patients as well as patients who did not have a Hugs tag. The project scope encompasses all units in Mott Hospital except for the Child Adolescent Psychiatric Hospital (CAPH) unit. The key issues driving this project were the high number of Hugs nuisance alarms (371 in the past 13 months), the seriousness of patient security in a children s hospital, and the free flow between inpatient floors that will be implemented in the new Mott Hospital, opening in The goals and objectives for the team included creating a snapshot of the current inpatient tracking process and developing a standardized inpatient tracking process. The team approached this project in four phases: Observations, interviews, and data collection Current state value stream mapping Root cause analysis Final recommendations The first phase involved collecting as much information about patient tracking as possible. The current state value stream mapping phase entailed analyzing the information collected from the first phase to develop a snapshot of the current process. The team then identified the areas of process deficiency in the root cause analysis phase. The final recommendations phase involved creating a future state value stream map and developing recommendations that could be implemented. From the observations, interviews, and data collection phase the team concluded: Eight different transportation forms are being used 3
4 Multiple tracking logs are being used to keep track of a patients location Patient transportation arrival time has great variation Family members set off the most Hugs nuisance alarms The current state map phase highlighted the great variation between different unit s tracking processes as the team developed six different current state value stream maps outlining these different hospital functions. These trips included patient transportation, operating room, MRI, SWAT, radiology, and parent trips. The root cause analysis phase used the lean Five Why s method to drill down causes of the variation. This involved asking why multiple times to find what truly caused a process deficiency. Based on this analysis, the team concluded that the unclear roles and responsibilities of the staff, the lack of parent training, the lack of communication between hospital personnel, the self concern of departments, the evolved transportation process, and the focus on the small picture seem to be the causes of the majority of the problems with the current tracking process. Based on these findings the team developed an Impact vs. Effort diagram to find the recommendations that would have the highest impact but require the least amount of effort. From this analysis the team looked to focus on standardizing clerk/nurse responsibilities, standardizing transportation forms, and developing family security training. A future state value stream map was developed to help with the recommendation, The team recommends to clearly define roles and responsibilities, develop a tracking sign out /in log for inpatient units, standardize a portion of the transportation forms, and create a parent Hugs information card. 4
5 Introduction Mott Children s and Women s Hospital is part of the University of Michigan Health System. With 198 beds, one of the biggest concerns of the hospital staff is knowing the location of each patient at all times. The current process of tracking inpatients in Mott Children s and Women s Hospital is not standardized, leading to decreased patient safety when the patients move from department to department. In addition, the Manager of Security Operations for the hospital has reported that the current tracking method results in too many false (or nuisance) alarms that alert hospital staff even though the locations of the patients are known. The Manager of Security Operations would like a uniform, efficient tracking process for all inpatient floors that increases the safety of the patients. The Manager asked an Industrial and Operations Engineering 481 team to create a current state value stream map of the tracking process and identify opportunities for improvement. This work has been completed. From the team s conclusions, a standard process for tracking inpatients being checked into and out of new departments at Mott Children s and Women s Hospital has been recommended. This report presents the team s analysis and recommendations of the inpatient tracking process at Mott Children s and Women s Hospital. Background and Current Situation When caring for children in a hospital, high security measures must be followed to create a safe environment for both patients and families. There have been many advances in hospital security systems recently, including the Hugs system that is currently in place at Mott Children s and Women s Hospital. With the Hugs program, children 24 months and younger wear a bracelet on either their ankle or their wrist. The bracelet activates an alarm if the patient is taken past a door sensor, if the patient is standing by an exit for more than 15 seconds, or if the bracelet is cut. However, Mott Children s and Women s hospital has experienced 371 false alarms in the past 13 months, decreasing the vigilance of the hospital staff and distracting visitors and patients. In addition, children over two years old do not have any form of tracking device unless they are labeled as high risk by the Child Protection Team or hospital staff. The Manager of Security Operations has indicated that there is room to improve the current tracking process by eliminating the inconsistencies. Most inconsistencies occur when patients are moved from one department to another and when family members take the patient off the floor for various reasons. This project created a standardized method for tracking all Mott Children s and Women s Hospital inpatients, making the tracking more efficient and increasing patient safety. The team found many variations and complexities in the patient tracking process. The amount of variation in the current system is a product of the different needs patients have, but it is also the product of an evolved system. Roles and responsibilities are not well defined, which was evident 5
6 from talking with staff members. After reporting the team s findings and conclusions the team will make recommendations to combat this variation and formalize the patient tracking process. Key Issues The following key issues compelled the need for this project. In the past 13 months, 371 infant security alarms have been set off at the Mott Children s and Women s Hospital. This data has been tracked by the Hugs security software, which records each alarm. The seriousness of child security and tracking within Mott has led to increased pressure on the hospital to ensure the safety of its patients. The free flow between floors allowed at the new Mott Children s and Women s Hospital exacerbates the patient tracking problem that the hospital is currently facing. Goals and Objectives The student team worked to achieve the following goal: Develop and recommend a standardized inpatient tracking process for all units in Mott Children s and Women s Hospital. This goal has led to the following objectives: Allow all staff and parents to know where patients are at all times Decrease risk of abduction Decrease nuisance alarms Project Scope This project included inpatient tracking in all units within Mott Children s and Women s Hospital except one. The proposed standardized process included an inpatient tracking process for all Mott inpatients. This planned process accounts for patients leaving the unit for tests, procedures, and family visits. The project does not include the Child Adolescent Psychiatric Hospital (CAPH) unit in Mott. The team did not study tasks or activities associated with units outside of Mott Children s and Women s Hospital, patients not admitted to Mott, and issues not dealing with patient security. Expected Impact The team performed and analyzed various studies of the current process. Upon completion, the team provided recommendations to standardize the current process. The recommendations will result in: Improved tracking process Increased patient safety Improved quality of patient care Decreased staff and patient complaints 6
7 Approach and Methodology With increasing patient security as the primary project goal, the team performed our analysis of the project in four phases: 1. Observations, interviews, and data collection 2. Current state value stream mapping 3. Root cause analysis 4. Final recommendations Phase One: Observations, Interviews, and Data Collection For the first phase of the project, the team collected observations, interviews and data from sources within Mott Hospital, other area hospitals, Mott parents, and other sources connected to patient security. Interviews The team interviewed over 20 nurses and unit clerks from all of the inpatient floors. The team also interviewed with patient transporters, and SWAT (nurses for high risk patients concerning patient transportation). The team interviewed transporters, nurses, and administration staff from these groups. Information was gathered on security perceptions, understanding of the current tracking processes, roles and responsibilities, and suggestions for streamlining inpatient tracking. Interviews were also conducted with possible destination sites of inpatients. A destination site is anywhere that a patient may be transferred to when they leave their unit floor. Examples of destination sites included Post Anesthesiology Care Unit (PACU), Radiology, Operating Room (OR), and Physical Therapy. Unit clerks, nurses, and administration staff were interviewed from these sites. Questions for destination sites consisted of their role in patient tracking, their current processes, and suggestions for the future. Observations For the observation portion of this phase, the team started by observing the interactions between staff on the inpatient floors. The team observed nurses and clerks on the 5 th and 6 th floors for a total of 20 hours. The team also shadowed pick-ups by patient transporters observing 10 pickups. The observations were used to validate the knowledge the team had learned from interviews, and to find discrepancies in perception about the process and what actually is done. Data Collection The team conducted a literature search to assist in gaining background knowledge of the problem. The team searched topics involving patient and hospital security, process standardization, and value stream mapping. The team compiled literature from books, online sources, and past IOE 481 final reports. A list of sources can be found in Appendix A. 7
8 Mott security staff provided the team with historical data of the Hugs security system. The data was compiled from June 2009 through September The team received data from patient transport which was summarized and collected from January 2009 to September The data contained information for average times of jobs and volume of jobs by location, and can be found in the Findings section of this report. The team also collated eight transporting and tracking forms used by different departments within the hospital; these forms are in Appendix B. Survey requests were sent to different audiences. One request was sent to other area children s and women s hospitals concerning security systems they have in place. The other request was a survey sent to inpatient families asking for information on hospital security training they received while at Mott. The team received three responses for the security systems survey, and 53 responses for the parent survey. The data compiled from the parent survey can be found in the Findings section of this report. Phase Two: Current State Value Stream Mapping After interviews and observations, the team analyzed the information and data collected to form a current process value stream map of the patient tracking process. The team completed a rough timeline of the process outlining the roles and responsibilities of key stakeholders to start the mapping of the current state. The team then constructed current state value stream maps of the inpatient tracking process within Mott Hospital. First time quality (FTQ) metrics were developed for key process steps. FTQ estimates how often a process step is done correctly the first time it is performed. Phase Three: Root Cause Analysis Once the team documented the current state through value stream mapping, root causes of the deficiencies in Mott s inpatient tracking process were identified. The team looked at the FTQ metrics as well as performed a Five why s analysis to determine root causes of the problem. The groups responsible for the most Hugs alarms were determined by looking at the Hugs data. Phase Four: Final Recommendations In the team s final recommendations, a future state value stream map was constructed to outline proposed changes, and provide a snapshot of the new standardized process. From this future state value stream map, the team developed final recommendations for Mott Children s and Women s Hospital inpatient tracking process. An Impact vs. Effort diagram was constructed to determine what proposed changes would have the greatest impact and require the least amount of effort to implement. The team s final recommendations were based off of a combination of improving the patient tracking process and implementing reasonable goals for Mott Children s and Women s Hospital. 8
9 Findings and Conclusions This section of the report contains the team s findings after completing interviews, observations and data collection at Mott Children s and Women s Hospital. The following were the most significant findings: Number of transportation forms being used is excessive Number of sign out/ in logs being used to keep track of patient s location is excessive Patients are experiencing long wait times at their destination because a transporter is not available Radiology Department has recently launched a new transportation program with their own personal transporter Alarms occur most often on the 6 th floor and are caused by parents and clerks Process for training parents in the Hugs system is unclear Seventy percent of parents with children not on the Hugs system received no training By analyzing these findings, the team completed a current state value stream map and root cause analysis of the current state. Through the use of these tools, the following conclusions were made: Current transportation process causes extra work and confusion for personnel Long wait time for transporters causes variability in the transportation of patients Variations in the training of parents are caused by different staff members presenting the information to parents Lack of standard training material for parents A more detailed description of the team s findings and conclusions follows, including the data that was collected, findings from interviews and observations, and results from surveys that were collected. Interviews and Observations The team interviewed nurses and clerks from all inpatient floors. In addition, the team interviewed patient transporters, SWAT, PACU, Radiology, OR, PT/OT, Echo, EKG, and MRI. Questions focused on the current inpatient transport process, roles and responsibilities of the personnel, and suggestions for improvements. A sample of the interview questions is included in Appendix C. In addition to these interviews, observations of the 5 th floor, 6 th floor, Radiology, MRI, Patient Transportation, and SWAT were conducted. The team observed patients leaving their unit for procedures in Radiology and MRI by shadowing patient transportation and SWAT for 20 hours. 9
10 From these interviews and observations, the team identified four key findings regarding the current inpatient tracking process in use at Mott. Number of transportation forms being used is excessive Number of sign out/ in logs being used to keep track of patient s location is excessive Patients are experiencing long wait times at their destination because a transporter is not available Radiology Department has recently launched a new transportation program with their own personal transporter Based on these findings, the team was able to make conclusions about the current process. Eight different transportation forms were collected and can be seen in Appendix B. When a patient is transported from the unit to a test or procedure, an inter-hospital transportation form is used. Although this form is the most common, the team found that the destination units frequently have their own transportation forms. This lack of consistency in forms was observed to cause extra work for the transporters, confusion among personnel, and complacency. Inpatient units in Mott currently use very different methods for tracking the location of their patients. Several units use forms to keep track of their patient s appointments for the day as can be seen in Appendix D; however, the units have no way of knowing the location of patients who have left the unit with a parent for a reason other than an appointment. This lack of standardization leads to confusion on the unit, especially with floating unit clerks. The transporters cover the entire University Hospital in addition to Mott. As a result, long travel times add up to ten minutes to the existing 30 minute wait time. Through root cause analysis, the team found that this long wait time was the leading cause of variation in patient transporter. When a patient waited for a significant amount of time, parents, nurses, clerks, and other personnel were more likely to transport the patient to their unit. As a result of the long wait times, the Radiology Supervisor for Mott Children s and Women s Hospital started a pilot program for her unit. Radiology has their own patient transporter used only to transport inpatients to and from their unit. Although the Radiology Supervisor did not have any data available at the time of the report, she did report significant decreases in wait time, increases in patient and family satisfaction, and decreases in transporter variability. Data Collection The team collected data from the Hugs security system, patient transportation, parent surveys, and area hospital surveys. This data was used to determine the quantity and causes of the Hugs alarms, gain parent feedback on the current inpatient tracking process, and make comparisons with other children s hospitals. 10
11 Hugs Security Data Mott Children s and Women s Hospital currently uses the Hugs system to tag children under two years of age. When a child with a Hugs tag is transported off the unit, the patient must be checked out of the Hugs system by the unit clerk. When the child is not properly checked out before leaving the floor, an alarm will sound. An alarm will also sound if a Hugs patient stands by a door or if a door is opened while the patient is within a certain distance of the door. The team used hospital data from Hugs alarms to draw several conclusions about the current process. The findings are following in Figures 1 and 2. Figure 1: Hugs Alarms Locations Hugs Data: Security Staff Hugs Data, sample= 371, collected from June 1, 2009 September 30, 2009 The team found that 44.2% of the Hugs alarms reported occurred on the 6 th floor. Stair 1on the 6 th caused 46.4% of the alarms on the 6 th floor. The team concluded that this occurs because the playroom on the floor is located next to stair 1 and the alarms are caused when a door is opened while a child is passing to enter the playroom. Through interviews and observations, it was determined that most of these alarms were accidental. 11
12 Figure 2: Causes of Hugs Alarms Hugs Data: Security Staff Hugs Data, sample= 371, collected from June 1, 2009 September 30, 2009 The highest contributing causes of the Hugs alarms are parents and clerks who cause a total of 60.2% of the Hugs alarms. Through interviews and observations of the units, the team concluded that parents cause Hugs alarms frequently because of the inconsistencies in the training material that is presented to them at the beginning of their child s stay. The responsibility of training parents falls on a combination of unit clerks, nurses, and volunteers. In addition, clerks are ultimately responsible for deactivating the Hugs tag when a patient is leaving the floor. The team found that lack of communication between the nurses, patient transporters, and unit clerks causes the clerk to not properly check out a Hugs patient who is leaving the floor. Patient Transportation Data For the majority of procedures, inpatients are taken to their appointments by patient transportation. Patient transportation is shared between University Hospital and Mott Children s and Women s Hospital, but is dispatched out of University Hospital. The transporters are required to call into a computer system when they are beginning and completing a job. The data that was collected can be found in Figure 3. The patient transport data was analyzed to develop the following conclusions about the patient transportation process. 12
13 Figure 3: Patient Transportation Destination Frequency Patient Transport Data: Transport Tracking, sample = 7,605, collected from January 1, 2009 October 20, 2009 The team concluded that before the Radiology pilot program was started, the majority of trips by patient transportation were to that destination. The destinations that frequently use patient transportation also experience more variability in who returns the patient to their unit. When a patient is forced to wait for a transporter, it was observed that a person from that destination was more likely to transport the patient. Parent Surveys The team administered internet surveys to a sample of Mott parents to obtain information on the training program they received when their child was admitted to an inpatient floor. Figures 4-6 represent the information that was collected 13
14 Figure 4: Parent Survey on Hugs Comprehensiveness Mott Parent Data: Parent Survey, sample= 53, collected from October 1, October 15, 2009 The survey indicates that 40% of the parents found that the Hugs training was not at all comprehensive. Based on this finding, the team concluded that the current program that is used to train parents on the rules of Hugs is not a sufficient amount of information. There is no standardized training material, which leads to the high number of Hugs alarms that are caused by parents or family members. 14
15 Figure 5: Parent Survey on Security Expectations Mott Parent Data: Parent Survey, sample= 53, collected from October 1, October 15, 2009 The survey results show that 75% of parents have very high expectations of their child s security while admitted in Mott Children s and Women s Hospital. While no issues have occurred under the current process to endanger a patient; inconsistencies and lack of standardization of the process have the potential to cause security breaches. Therefore, security should be a high priority for Mott. 15
16 Figure 6: Parent Survey on Guidelines Mott Parent Data: Parent Survey, sample= 53, collected from October 1, October 15, 2009 The parent survey indicates that 60% of parents received no information or guidelines for moving their child from the floor. Through interviews and observations, the team concluded that the lack of defined nurse and unit clerk roles and responsibilities for relaying this information leads to this problem. Area Hospital Surveys The team distributed surveys to area hospitals to gain insight into other inpatient tracking processes. The team inquired about a standardized process for tracking pediatric patients, a standardized process for tracking infants, the strengths and weaknesses of the system, and the age of their current processes. The team received responses for the survey from Beaumont Hospital in Royal Oak, MI; The University of Missouri Health Care; and The University of Iowa. All three hospitals currently use tags for infants in their hospitals; however, none have a standardized process for tracking patients who are not tagged. Current State Map The team created maps of the current state for patient tracking at Mott Children s and Women s Hospital. Based on these maps, the team found that there were significant differences in how the patient was transported based on the destination. The team found different processes for the 16
17 Operating Room, MRI, MRI with an anesthetized patient, Radiology, SWAT, procedures that use University Hospital Patient Transportation, and parent trips with patients. The current state value stream maps for these different processes are shown in Figures Full scale figures are shown in Appendix E. Figure 7: Current State Value Stream Map of Patient Transport Figure 8: Current State Value Stream Map of Radiology 17
18 Figure 9: Current State Value Stream Map of SWAT Figure 10: Current State Value Stream Map of Operating Room 18
19 Figure 11: Current State Value Stream Map of MRI (No Anesthesia) Figure 12: Current State Value Stream Map of MRI (Yes Anesthesia) 19
20 Figure 13: Current State Value Stream Map of a Parent Trip The team concluded that the variability in the transportation process is causing problems with the current tracking system. Nurses, unit clerks, transporters, and destination unit clerks do not have clearly defined roles and responsibilities in the tracking process. This lack of standardization causes confusion, longer wait times for transporters, and an increased safety risk for the patients. Root Cause Analysis Root cause analysis and the current state maps were used to analyze the current state. The team used the Five Why s method and an Impact vs. Effort Matrix to look into the root causes of the problems and to develop recommendations. Five Why s Method The team focused on the excessive number of Hugs alarms, the various transportation forms, and the lack of communication between the hospital personnel. A flowchart was used as a visual tool for the team to complete the Five Why s analysis. This involved asking why multiple times to find what truly caused a process deficiency. These flowcharts follow in Figure


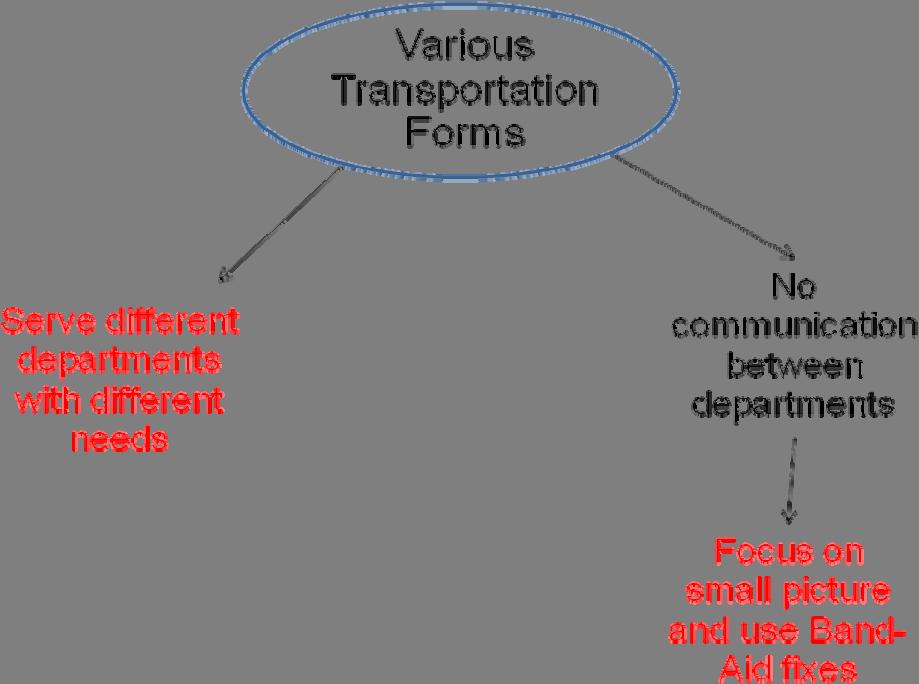
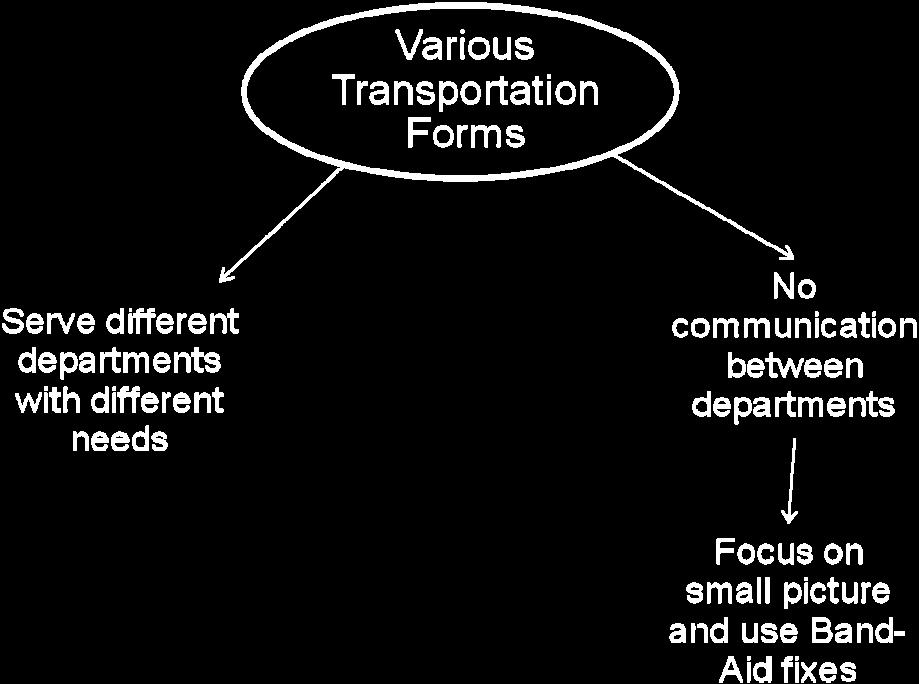
21 Figure 14: Five Why s Analysis Miscommunication Coincidence 21


22 Based on this analysis, the team concluded that the unclear roles and responsibilities of the staff, the lack of parent training, the lack of communication between hospital personnel, the self concern of departments, the evolved transportation process, and the focus on the small picture seem to be the causes of the majority of the problems with the current tracking process. These causes are highlighted in Figure 14. Impact vs. Effort To develop recommendations for Mott Children s and Woman s Hospital, the team used an Impact vs. Effort matrix to prioritize the possible fixes to the problems. This diagram compares the impact of a possible change to the effort that would be required to implement this change. The matrix follows in Figure


23 Figure 15: Impact vs. Effort The Impact vs. Effort matrix shows that the changes in the upper right quadrant will be the easiest to implement and will create the highest impact. Based on the comparison of impact and effort, the team determined to focus on standardized clerk and nurse responsibilities, standardized transportation forms, and patient family training. The following sections will focus on the team s recommendations and plan for implementation. Recommendations and Implementation The following represent recommendations for implementing the results reached during analysis of the Mott Children and Women s Hospital inpatient tracking system. Attempting to reduce the number of Hugs detector alarms while increasing patient safety and knowledge of patient location, the team created: An ideal process map for patient transportation A parent information card A standardized tracking form A new sign out/sign in log A matrix clarifying the roles and responsibilities of personnel involved in the transportation process 23
24 Future State Map To ensure that all patients in the hospital are being transported in a safe and secure way, the team created a future state map of an ideal inpatient transportation process. The sequence of events laid out on this map is the process that should be followed every time a patient needs to leave the floor. This future state map can be seen in Figure 16. A full size version of this map can be seen in Appendix E. Figure 16: Future State Map Transporter Unit Clerk Nurse Destination Patient Parent Information Card The team created a 3x5 index card highlighting all Hugs portal exciter alarm locations and key information about the Hugs alarm system and transporting the patient. The cards will be passed out to all parents who have a child staying in Mott. This index card will have a map of the child s floor on one side, and the key information about the alarm system and transportation process on the other side. The front side of the card can be seen in Figure

25 Figure 17: Parent Information Card-Front Side The back of the card will read: Alarms will sound if you take any Hugs patient near the areas highlighted on the flip side of this card. Please make sure to carefully note these locations and remain a good distance from all of these stairwells and elevators. Please do not disband, cut, or tamper with a Hugs band as this will set off the alarm. If you would like to remove your child from the floor, please speak with a unit clerk or nurse. Make sure to also sign your child out from the unit upon leaving. To implement the use of this card, cards will be given to the unit clerks of each floor. The unit clerks will then give a card to each family upon check in. The parents will be able to refer to this card through the entirety of their stay at the hospital. Standardized Portion of Patient Tracking Form Based on analysis of the various patient transportation forms, the team created a standardized portion of the form hoping to eliminate variability in transportation forms. The standardized portion can be seen in Figure
26 Figure 18: Standardized Transportation Form Check Patient ID Bracelet Patient Name: Registration #: Bed #: Patient Unit: Hugs Tag? Y / N Appointment Time: Actual Arrival Time: Actual Drop Off Time: Destination Unit: This portion was compiled based on analysis of each of the eight current transportation forms collected throughout Mott. Information common to each form was included in the standardized portion. Destination units and inpatient floors will add this standardized portion to their current form. The separate units and floors can then add any missing information that is necessary to their specific unit. The forms will be used in the same way that the current transportation forms are used. Patient Sign-Out/Sign-In Log The team also created a sign-out/sign-in log that should be used every time a patient leaves and returns to the floor. The destination units will also have a copy of this form. When a patient arrives and leaves the destination unit, this log should also be filled out. The log gives accountability to whoever is moving the patient at all times. The Sign-In/Sign-Out log that the team drafted can be seen in Figure 19. Figure 19: Sample Sign-Out/Sign-In Log Patient Name Unit Destination Time Out Transporter Time In Transporter Hugs (Y/N) This log will be implemented by placing a copy at the front of each unit clerk desk as well as at all destination unit desks. Unit clerks must ensure that every employee and parent does not remove a patient from the floor without completing the sign out log. Whenever a patient returns to the floor it the transporter must sign the patient back in immediately upon arrival. Clarification of Roles and Responsibilities Based on observations and interviews conducted throughout Mott, the team created a matrix clarifying the roles of the unit clerk, unit nurse, transporter, and destination site clerk throughout the transportation process. Assigning one person to the responsibility of the patient throughout each step ensures that the patient is never alone and is always safe. This matrix can be seen in Figure
27 Definition Figure 20: Responsibility Matrix Role Unit Clerk Unit Nurse Transporter Clerk that resides on patient's RN assigned to patient Person who travels with / unit transports the patient to and from the destination Before Trip Confirm appointment time Print transportation form Give completed transportation form and chart to transporter Track sign in / out log for unit Notify unit nurse of trip If Hugs tag: deactivate Prep patient for transportation before transporter arrives Fill out transport form Know patient destination and cause of trip Ultimately responsible for patient safety Notify unit nurse and clerk of arrival Arrive on time for appointment Receive patient chart and completed transport form Check for Hugs tag, if found ask unit clerk to deactivate Sign out patient from floor Destination Site Clerk Only used if patient is transported to another Hospital Unit Notify unit clerk and nurse of trip Enroute to destination At destination Enroute back to unit Back at unit Page unit nurse Handle patient chart Handle sign in / out log for floor Activate Hugs if necessary Ultimately responsible for patient safety If destination is a hospital Unit: Sign patient into destination on arrival Sign out patient from destination on departure Ultimately responsible for patient safety Check on patient Notify unit clerk of return Have exchange with Sign patient back in to unit transporter Hand chart back to Ultimately responsible transporter for patient safety Return patient to room Wait for nurse, to hand off patient Perform trip function Ultimately responsible for patient safety 27
28 This matrix should be distributed to all personnel employed in one of these four roles at Mott. The matrix will remind each employee of Mott s expectations and reinforce when each role is responsible for the patient. Out of Scope Recommendations Outside of the scope of this project, the team developed ideas to further improve patient security at Mott. Although the team did not finalize these recommendations, with more time and information the ideas could be pursued at a later date. These recommendations include: Assigning patient transporters to transport to and from a specific destination Incorporating travel time into the expected arrival time of the patient transporters to the patient floor The zoning of patient transporters would help keep the transporters on track throughout their daily schedule. The addition of travel time to the expected arrival time of the patient transporter would reduce the amount of time nurses waited for the transporters and reduce the amount of time transporters waited for the nurse to prepare the patient. 28
29 Appendix A: Literature Search References Lampland, Martha, and Susan Leigh Star, eds. Standards and Their Stories :How Quantifying, Classifying, and Formalizing Practices Shape Everyday Life. Cornell UP, Print. Latino, Robert. Root Cause Analysis. Hopewell, VI: Reliability Center, Inc., Print. Nash, Mark A., and Sheila R. Poling. Mapping the Total Value Stream :A Comprehensive Guide for Production and Transactional Processes. New York: Productivity, Print. Nicholas, John. The Portal to Lean Production. Boca Raton, FL: Auerback Publications, Print. Shingo, Shigeo. A Study of the Toyota Production System. Rev. ed. Cambridge, MA: Productivity Press, Print. Wilson, Paul F., Larry D. Dell, and Gaylord F. Anderson. Root Cause Analysis: A Tool for Total Quality Management. Asq, Print. Former IOE 481 Team Projects 1. University Hospital Operating Room Instrument Room Process Improvement 2. Assessing Nursing Time Spent Tracking Equipment University of Michigan Health System (UMHS) 3. Orders Management Project Post-CareLink Analysis of Clerical Workload 4. C.S. Mott Children s Hospital Operating Room Surgery Turnover Time Analysis Final Report 5. Nursing SWAT Patient Transport Analysis Regarding Workload and Tasks 6. Analysis of Patient Discharge Delay in Mott Children s Hospital 29

30 Appendix B: Patient Transportation Forms Inpatient Unit Patient Handoff Form 30
31 Appendix B: Patient Transportation Forms Radiology Inpatient Transportation Form 31
32 Appendix B: Patient Transportation Forms Operating Room Inpatient Transportation Form Appendix: Operating Room Transportation Log 32
33 Appendix B: Patient Transportation Forms Operation Room Transportation Log 33
")
34 Appendix B: Patient Transportation Forms SWAT Inpatient Transportation Form (Front) 34
")
35 Appendix B: Patient Transportation Forms SWAT Inpatient Transportation Form (Back) 35
36 Appendix B: Patient Transportation Forms SWAT Paramedic Transportation Log 36
 37")
37 Appendix B: Patient Transportation Forms SWAT Nurse Transportation Log (Front) 37

38 Appendix B: Patient Transportation Forms SWAT Nurse Transportation Log (Back) 38

39 Appendix B: Patient Transportation Forms PACU Inpatient Transportation Form Appendix B: Current State Map Timeline 39
40 Appendix C: Sample Interview Questions Mott Children s and Women s Hospital Clerk Interviews 1. What are the current tracking procedures for your unit? 2. What is your role in tracking patients? 3. What are some of the tools that you use to track patients? 4. What is the biggest issue or obstacle facing patient security and tracking from your perspective? 5. How comfortable are you with the Hugs system? What is your role in the Hugs system? 6. What ideas do you have for improving this process? Mott Children s and Women s Hospital Patient Transport Interviews 1. What is your role at Mott Children s and Women s Hospital? 2. How does this role correspond with the current process for tracking patients at Mott? 3. What are some of the tools you use to track patients? 4. What are some patient transportation methods? 5. Who are you in contact with during the patient transportation process? 6. What is the biggest issue or obstacle facing patient security and tracking from your perspective? 7. What ideas do you have for improving this process? Mott Children and Women s Hospital Nurse Interviews 1. What are your roles and responsibilities on this unit? 2. Specifically, what are your responsibilities regarding patient security? 3. What tools do you use to ensure patient safety? 4. Do you ever move a patient from his/her room to another unit in the hospital? If so, what process do you use to track the patient s location? 5. What is the biggest obstacle facing patient security and tracking from your perspective? 6. What ideas do you have for improving this process? 40
41 Appendix D: Unit Sign-Out / Sign-In Logs 7 Mott Patient Appointment Schedule 41
42 Appendix D: Unit Sign-in / Sign-out Logs 5 West Daily Referral Log 42
43 Appendix E: Full Size Value Stream Maps Current State - MRI (No Anesthetia) 43
44 Appendix E: Full Size Value Stream Maps Current State - MRI (No Anesthesia) 44
45 Appendix E: Full Size Value Stream Maps Current State - Operating Room 45
46 Appendix E: Full Size Value Stream Maps Current State - Parent Trip 46
47 Appendix E: Full Size Value Stream Maps Current State Patient Transportation 47
48 Appendix E: Full Size Value Stream Maps Current State Radiology 48
49 Appendix E: Full Size Value Stream Maps Current State SWAT 49
50 Appendix E: Full Size Value Stream Maps Future State Map 50
Michigan Medicine--Frankel Cardiovascular Center. Determining Direct Patient Utilization Costs in the Cardiovascular Clinic.
 Michigan Medicine--Frankel Cardiovascular Center Clinical Design and Innovation Determining Direct Patient Utilization Costs in the Cardiovascular Clinic Final Report Client: Mrs. Cathy Twu-Wong Project
Michigan Medicine--Frankel Cardiovascular Center Clinical Design and Innovation Determining Direct Patient Utilization Costs in the Cardiovascular Clinic Final Report Client: Mrs. Cathy Twu-Wong Project
Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience
 University of Michigan Health System Program and Operations Analysis Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience Final Report To: Stephen Napolitan, Assistant
University of Michigan Health System Program and Operations Analysis Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience Final Report To: Stephen Napolitan, Assistant
University of Michigan Health System Program and Operations Analysis. Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients
 University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
University of Michigan Emergency Department
 University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Health System
 University of Michigan Health System Program and Operations Analysis Analysis of the Orthopedic Surgery Taubman Clinic Final Report To: Andrew Urquhart, MD: Orthopedic Surgeon Patrice Seymour, Administrative
University of Michigan Health System Program and Operations Analysis Analysis of the Orthopedic Surgery Taubman Clinic Final Report To: Andrew Urquhart, MD: Orthopedic Surgeon Patrice Seymour, Administrative
University of Michigan Comprehensive Stroke Center
 University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
University of Michigan Health System. Current State Analysis of the Main Adult Emergency Department
 University of Michigan Health System Program and Operations Analysis Current State Analysis of the Main Adult Emergency Department Final Report To: Jeff Desmond MD, Clinical Operations Manager Emergency
University of Michigan Health System Program and Operations Analysis Current State Analysis of the Main Adult Emergency Department Final Report To: Jeff Desmond MD, Clinical Operations Manager Emergency
Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report
 Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
The University of Michigan Health System. Geriatrics Clinic Flow Analysis Final Report
 The University of Michigan Health System Geriatrics Clinic Flow Analysis Final Report To: CC: Renea Price, Clinic Manager, East Ann Arbor Geriatrics Center Jocelyn Wiggins, MD, Medical Director, East Ann
The University of Michigan Health System Geriatrics Clinic Flow Analysis Final Report To: CC: Renea Price, Clinic Manager, East Ann Arbor Geriatrics Center Jocelyn Wiggins, MD, Medical Director, East Ann
University of Michigan Health System. Analysis of the Patient Admission Process in The University of Michigan Hospital Final Report
 University of Michigan Health System Analysis of the Patient Admission Process in The University of Michigan Hospital Final Report Submitted to: Lori Lathers Training Specialist Senior UMHS, Central Staffing
University of Michigan Health System Analysis of the Patient Admission Process in The University of Michigan Hospital Final Report Submitted to: Lori Lathers Training Specialist Senior UMHS, Central Staffing
University of Michigan Health System. Program and Operations Analysis. CSR Staffing Process. Final Report
 University of Michigan Health System Program and Operations Analysis CSR Staffing Process Final Report To: Jean Shlafer, Director, Central Staffing Resources, Admissions Bed Coordination Center Amanda
University of Michigan Health System Program and Operations Analysis CSR Staffing Process Final Report To: Jean Shlafer, Director, Central Staffing Resources, Admissions Bed Coordination Center Amanda
University of Michigan Health System
 University of Michigan Health System Programs and Operations Analysis Analysis of the Discharge Process at Internal Medicine Unit B Department of Internal Medicine Final Report To: Dr. Christopher Kim,
University of Michigan Health System Programs and Operations Analysis Analysis of the Discharge Process at Internal Medicine Unit B Department of Internal Medicine Final Report To: Dr. Christopher Kim,
Improving Mott Hospital Post-Operative Processes
 Improving Mott Hospital Post-Operative Processes Program and Operation Analysis Submitted To: Sheila Trouten, Client Nurse Manager, PACU, Mott OR Jesse Wilson, Coordinator Administrative Manager of Surgical
Improving Mott Hospital Post-Operative Processes Program and Operation Analysis Submitted To: Sheila Trouten, Client Nurse Manager, PACU, Mott OR Jesse Wilson, Coordinator Administrative Manager of Surgical
University of Michigan Health System. Final Report
 University of Michigan Health System Program and Operations Analysis Analysis of Medication Turnaround in the 6 th Floor University Hospital Pharmacy Satellite Final Report To: Dr. Phil Brummond, Pharm.D,
University of Michigan Health System Program and Operations Analysis Analysis of Medication Turnaround in the 6 th Floor University Hospital Pharmacy Satellite Final Report To: Dr. Phil Brummond, Pharm.D,
Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital. Final Report. Submitted To:
 Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital Final Report Submitted To: Cathy Lewis, MSN, RN Clinical Nurse Specialist and Adjunct Clinical Instructor
Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital Final Report Submitted To: Cathy Lewis, MSN, RN Clinical Nurse Specialist and Adjunct Clinical Instructor
University of Michigan Health System Program and Operations Analysis. Analysis of Problem Summary List and Medication Reconciliation Final Report
 University of Michigan Health System Program and Operations Analysis Analysis of Problem Summary List and Medication Reconciliation Final Report To: John Clark, PharmD, MS, University of Michigan Health
University of Michigan Health System Program and Operations Analysis Analysis of Problem Summary List and Medication Reconciliation Final Report To: John Clark, PharmD, MS, University of Michigan Health
University of Michigan Health System Programs and Operations Analysis. Order Entry Clerical Process Analysis Final Report
 University of Michigan Health System Programs and Operations Analysis Order Entry Clerical Process Analysis Final Report To: Richard J. Coffey: Director, Programs and Operations Analysis Bruce Chaffee:
University of Michigan Health System Programs and Operations Analysis Order Entry Clerical Process Analysis Final Report To: Richard J. Coffey: Director, Programs and Operations Analysis Bruce Chaffee:
Analysis of Nursing Workload in Primary Care
 Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
She s one of a kind Give her the unique protection of the Hugs system. Reliable and secure infant protection
 She s one of a kind Give her the unique protection of the Hugs system Reliable and secure infant protection Protecting over 1 million babies every year The Hugs system delivers an unmatched level of security
She s one of a kind Give her the unique protection of the Hugs system Reliable and secure infant protection Protecting over 1 million babies every year The Hugs system delivers an unmatched level of security
Final Report. Karen Keast Director of Clinical Operations. Jacquelynn Lapinski Senior Management Engineer
 Assessment of Room Utilization of the Interventional Radiology Division at the University of Michigan Hospital Final Report University of Michigan Health Systems Karen Keast Director of Clinical Operations
Assessment of Room Utilization of the Interventional Radiology Division at the University of Michigan Hospital Final Report University of Michigan Health Systems Karen Keast Director of Clinical Operations
MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa
 MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa WOMEN S CARE CENTER POLICY & PROCEDURES Policy Number: L-27/14:12 Subject: Purpose: Policy: Security: Infant/Child To protect against infant/child
MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa WOMEN S CARE CENTER POLICY & PROCEDURES Policy Number: L-27/14:12 Subject: Purpose: Policy: Security: Infant/Child To protect against infant/child
Analysis of Cardiovascular Patient Data during Preoperative, Operative, and Postoperative Phases
 University of Michigan College of Engineering Practicum in Hospital Systems Program and Operations Analysis Analysis of Cardiovascular Patient Data during Preoperative, Operative, and Postoperative Phases
University of Michigan College of Engineering Practicum in Hospital Systems Program and Operations Analysis Analysis of Cardiovascular Patient Data during Preoperative, Operative, and Postoperative Phases
Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting
 Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting How many times have we heard that it s easy to apply Lean and Six Sigma techniques to hospital processes, and specifically
Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting How many times have we heard that it s easy to apply Lean and Six Sigma techniques to hospital processes, and specifically
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process. Final Report
 University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process Final Report Submitted to: Ms. Angela Haley Ambulatory Care Manager, Department of Surgery 1540 E Medical
University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process Final Report Submitted to: Ms. Angela Haley Ambulatory Care Manager, Department of Surgery 1540 E Medical
A Publication for Hospital and Health System Professionals
 A Publication for Hospital and Health System Professionals S U M M E R 2 0 0 8 V O L U M E 6, I S S U E 2 Data for Healthcare Improvement Developing and Applying Avoidable Delay Tracking Working with Difficult
A Publication for Hospital and Health System Professionals S U M M E R 2 0 0 8 V O L U M E 6, I S S U E 2 Data for Healthcare Improvement Developing and Applying Avoidable Delay Tracking Working with Difficult
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Let My Patients Flow! Patient Flow Summit 2015
 Let My Patients Flow! Patient Flow Summit 2015 1 Agenda Background Approach Process Improvement Teams Simulation Model Results Q&A 2 Robert Wood Johnson University Hospital 965-bed Academic Medical Center
Let My Patients Flow! Patient Flow Summit 2015 1 Agenda Background Approach Process Improvement Teams Simulation Model Results Q&A 2 Robert Wood Johnson University Hospital 965-bed Academic Medical Center
Patient Safety: Fall Prevention. Unlicensed Assistive Personnel
 Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
I. GENERAL INFORMATION
 I. GENERAL INFORMATION Our Mission Statement To provide quality healthcare and foster health and wellness. Our Vision Statement Vision Statement: Our Desired Future To be the preferred provider for high
I. GENERAL INFORMATION Our Mission Statement To provide quality healthcare and foster health and wellness. Our Vision Statement Vision Statement: Our Desired Future To be the preferred provider for high
Improving operating room efficiency through the use of lean six sigma methodologies. Teodora O. Nicolescu
 Improving operating room efficiency through the use of lean six sigma methodologies Teodora O. Nicolescu Author detail: Teodora O. Nicolescu, MD Associate Professor Department of Anesthesiology The University
Improving operating room efficiency through the use of lean six sigma methodologies Teodora O. Nicolescu Author detail: Teodora O. Nicolescu, MD Associate Professor Department of Anesthesiology The University
University of Michigan Health System. Inpatient Cardiology Unit Analysis: Collect, Categorize and Quantify Delays for Procedures Final Report
 Project University of Michigan Health System Program and Operations Analysis Inpatient Cardiology Unit Analysis: Collect, Categorize and Quantify Delays for Procedures Final Report To: Dr. Robert Cody,
Project University of Michigan Health System Program and Operations Analysis Inpatient Cardiology Unit Analysis: Collect, Categorize and Quantify Delays for Procedures Final Report To: Dr. Robert Cody,
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Outpatient Infusion Access Analysis
 Outpatient Infusion Access Analysis Evaluating the current processes for providing infusion services Final Report December 1, 2003 University of Michigan Health System Program and Operations Analysis Client:
Outpatient Infusion Access Analysis Evaluating the current processes for providing infusion services Final Report December 1, 2003 University of Michigan Health System Program and Operations Analysis Client:
QUESTIONS. Print Student s/faculty Name: Date of Test Completion: Site of Experience: School/University: Semester:
 2017 - QUESTIONS Print Student s/faculty Name: Date of Test Completion: Site of Experience: School/University: Semester: Instructions: Read each question, write an answer on space provided, and return
2017 - QUESTIONS Print Student s/faculty Name: Date of Test Completion: Site of Experience: School/University: Semester: Instructions: Read each question, write an answer on space provided, and return
Improving Pain Center Processes utilizing a Lean Team Approach
 Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Facilitating Change in the Patient Safety Culture of the Clinical Learning Environment
 Facilitating Change in the Patient Safety Culture of the Clinical Learning Environment Andrew R. Buchert, MD Dept. of Pediatrics Gregory M. Bump, MD Dept. of Medicine Associate Medical Directors for GME
Facilitating Change in the Patient Safety Culture of the Clinical Learning Environment Andrew R. Buchert, MD Dept. of Pediatrics Gregory M. Bump, MD Dept. of Medicine Associate Medical Directors for GME
University of Michigan Health System Program and Operations Analysis. Anesthesia Technical Support Work Distribution Analysis.
 University of Michigan Health System Program and Operations Analysis Anesthesia Technical Support Work Distribution Analysis Final Report To: Paul Salow, Clinical Department Administrator, Anesthesiology
University of Michigan Health System Program and Operations Analysis Anesthesia Technical Support Work Distribution Analysis Final Report To: Paul Salow, Clinical Department Administrator, Anesthesiology
Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic. Final Report
 Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic Final Report Prepared for: Kathy Lash, Director of Operations University of Michigan Health System Radiation Oncology
Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic Final Report Prepared for: Kathy Lash, Director of Operations University of Michigan Health System Radiation Oncology
Analysis and Optimization of Emergent & Urgent Response Nurses
 Analysis and Optimization of Emergent & Urgent Response Nurses Final Report The University of Michigan Health System The University Hospital, Nursing Department Submitted To: Kathleen Moore, Client Administrative
Analysis and Optimization of Emergent & Urgent Response Nurses Final Report The University of Michigan Health System The University Hospital, Nursing Department Submitted To: Kathleen Moore, Client Administrative
uncovering key data points to improve OR profitability
 REPRINT March 2014 Robert A. Stiefel Howard Greenfield healthcare financial management association hfma.org uncovering key data points to improve OR profitability Hospital finance leaders can increase
REPRINT March 2014 Robert A. Stiefel Howard Greenfield healthcare financial management association hfma.org uncovering key data points to improve OR profitability Hospital finance leaders can increase
Tufts Medical Center: Falls Prevention Education
 Tufts Medical Center: Falls Prevention Education Purpose of Tufts Medical Center s Fall Program Minimize the number of patient, visitor and employee falls Minimize injuries related to falls Promote an
Tufts Medical Center: Falls Prevention Education Purpose of Tufts Medical Center s Fall Program Minimize the number of patient, visitor and employee falls Minimize injuries related to falls Promote an
Improving Patient Throughput in the Emergency Department
 University of Michigan Health System Program and Operations Analysis Improving Patient Throughput in the Emergency Department To: Jennifer Holmes, Director of Operations, Emergency Department Sam Clark,
University of Michigan Health System Program and Operations Analysis Improving Patient Throughput in the Emergency Department To: Jennifer Holmes, Director of Operations, Emergency Department Sam Clark,
available at journal homepage:
 Australasian Emergency Nursing Journal (2009) 12, 16 20 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/aenj RESEARCH PAPER The SAPhTE Study: The comparison of the SAPhTE (Safe-T)
Australasian Emergency Nursing Journal (2009) 12, 16 20 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/aenj RESEARCH PAPER The SAPhTE Study: The comparison of the SAPhTE (Safe-T)
Decreasing Environmental Services Response Times
 Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
A Client Satisfaction Survey at a Large Rural Medical Facility
 A CLIENT SATISFACTION SURVEY AT A LARGE RURAL MEDICAL FACILITY 271 A Client Satisfaction Survey at a Large Rural Medical Facility Sarah Baier, Kim Mertes, and LuAnn Maternoski Faculty Sponsor: Sally Huffman,
A CLIENT SATISFACTION SURVEY AT A LARGE RURAL MEDICAL FACILITY 271 A Client Satisfaction Survey at a Large Rural Medical Facility Sarah Baier, Kim Mertes, and LuAnn Maternoski Faculty Sponsor: Sally Huffman,
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care
 The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care A Webinar Presentation for the AIA AAH 8 January 2013 1 Topic 1: Driving Safety through Good Design Presenter:
The Joint Commission and Facility Design: A Partnership for Patient Safety and Quality Care A Webinar Presentation for the AIA AAH 8 January 2013 1 Topic 1: Driving Safety through Good Design Presenter:
VIOLENCE PREVENTION IN THE HEALTHCARE SETTING
 VIOLENCE PREVENTION IN THE HEALTHCARE SETTING presented by Michael Mock, Security Manager Overview Completed first MHA GAP Analysis August 2014 Questions: What are we doing right currently? What improvements
VIOLENCE PREVENTION IN THE HEALTHCARE SETTING presented by Michael Mock, Security Manager Overview Completed first MHA GAP Analysis August 2014 Questions: What are we doing right currently? What improvements
University of Michigan Health System MiChart Department Improving Operating Room Case Time Accuracy Final Report
 University of Michigan Health System MiChart Department Improving Operating Room Case Time Accuracy Final Report Submitted To: Clients Jeffrey Terrell, MD: Associate Chief Medical Information Officer Deborah
University of Michigan Health System MiChart Department Improving Operating Room Case Time Accuracy Final Report Submitted To: Clients Jeffrey Terrell, MD: Associate Chief Medical Information Officer Deborah
American Medical Group Association Optimizing a Patient-Focused Approach to Primary Care
 American Medical Group Association Optimizing a Patient-Focused Approach to Primary Care May 6, 2015 Today s Speakers 1 Today s Speakers Cailin Purcell Senior Director Cailin Purcell is the Senior Director
American Medical Group Association Optimizing a Patient-Focused Approach to Primary Care May 6, 2015 Today s Speakers 1 Today s Speakers Cailin Purcell Senior Director Cailin Purcell is the Senior Director
Tools & Resources for QI Success
 Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
RTLS and the Built Environment by Nelson E. Lee 10 December 2010
 The purpose of this paper is to discuss the value and limitations of Real Time Locating Systems (RTLS) to understand the impact of the built environment on worker productivity. RTLS data can be used for
The purpose of this paper is to discuss the value and limitations of Real Time Locating Systems (RTLS) to understand the impact of the built environment on worker productivity. RTLS data can be used for
INCIDENT COMMAND SYSTEM MULTI-CASUALTY TREATMENT MANAGER I-MC-238. COURSE ADMINISTRATOR S GUIDE AND TRAINEE WORKBOOK Self-Paced Instruction
 INCIDENT COMMAND SYSTEM MULTI-CASUALTY TREATMENT MANAGER COURSE ADMINISTRATOR S GUIDE AND TRAINEE WORKBOOK Self-Paced Instruction NOVEMBER 1990 Revised March 1993 This document contains information relative
INCIDENT COMMAND SYSTEM MULTI-CASUALTY TREATMENT MANAGER COURSE ADMINISTRATOR S GUIDE AND TRAINEE WORKBOOK Self-Paced Instruction NOVEMBER 1990 Revised March 1993 This document contains information relative
UMHS Program and Operations Analysis Department. Orders Management Medication Project (OMP) Final Report. December 10, 2007.
 Final Report. December 10, 2007.") UMHS Program and Operations Analysis Department Orders Management Medication Project (OMP) Final Report December 10, 2007 Client: Bruce Chaffee, Medication Management Team Lead Coordinator: John Schumacher,
UMHS Program and Operations Analysis Department Orders Management Medication Project (OMP) Final Report December 10, 2007 Client: Bruce Chaffee, Medication Management Team Lead Coordinator: John Schumacher,
Using Lean Principles to Decrease Outpatient Registration Wait Times. It s a Journey not a Destination
 Using Lean Principles to Decrease Wait Times It s a Journey not a Destination 533 Bed Acute Care System 461 Beds at AnMed Health Medical Center 72 Beds at AnMed Health Women s and Children's Hospital 45
Using Lean Principles to Decrease Wait Times It s a Journey not a Destination 533 Bed Acute Care System 461 Beds at AnMed Health Medical Center 72 Beds at AnMed Health Women s and Children's Hospital 45
INFANT PROTECTION. Have you sealed off the perimeter of the hospital? Have you notified the police? Have you called a Code Pink?. and so on!
 INFANT PROTECTION It s every hospital Administrators worst nightmare. At 3:00 AM, the phone rings. A quick glance at caller ID shows a very familiar number. It s the security director. Numerous thoughts
INFANT PROTECTION It s every hospital Administrators worst nightmare. At 3:00 AM, the phone rings. A quick glance at caller ID shows a very familiar number. It s the security director. Numerous thoughts
2017 Annual Mandatory Education. Sarasota Memorial Health Care System
 2017 Annual Mandatory Education Sarasota Memorial Health Care System Self-Study Module Questionnaire The goals of Annual Mandatory Education are to provide employees with information pertinent to their
2017 Annual Mandatory Education Sarasota Memorial Health Care System Self-Study Module Questionnaire The goals of Annual Mandatory Education are to provide employees with information pertinent to their
Implementing Surgeon Use of a Patient Safety Checklist in Ophthalmic Surgery
 Report on a QI Project Eligible for Part IV MOC Implementing Surgeon Use of a Patient Safety Checklist in Ophthalmic Surgery Instructions Determine eligibility. Before starting to complete this report,
Report on a QI Project Eligible for Part IV MOC Implementing Surgeon Use of a Patient Safety Checklist in Ophthalmic Surgery Instructions Determine eligibility. Before starting to complete this report,
LEAN and Cardiology Nursing Management : Application of LEAN Principle in the Rectification of
 LEAN and Cardiology Nursing Management : Application of LEAN Principle in the Rectification of Flow Logistics in Patients Undergoing Coronary Angiograms in Queen Mary Hospital Wong M.S., Luk W.S., Chiang
LEAN and Cardiology Nursing Management : Application of LEAN Principle in the Rectification of Flow Logistics in Patients Undergoing Coronary Angiograms in Queen Mary Hospital Wong M.S., Luk W.S., Chiang
Study of current inpatient volume and quality metrics at the University of Michigan Health System: Final Report
 Study of current inpatient volume and quality metrics at the University of Michigan Health System: Final Report Client: Bruce Chaffee PhD Pharmacy Department University of Michigan Ann Arbor Coordinator:
Study of current inpatient volume and quality metrics at the University of Michigan Health System: Final Report Client: Bruce Chaffee PhD Pharmacy Department University of Michigan Ann Arbor Coordinator:
Quality Improvement Project Control Report Out
 Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
Quality Improvement Project Control Report Out Prince County Hospital Surgery Floor Lean Project July 10th, 2014 Define Health PEI s ELT ( Executive Leadership Team ) identified the service areas throughout
From Big Data to Big Knowledge Optimizing Medication Management
 From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
AT THE UNIVERSITY OF ILLINOIS HOSPITAL AND HEALTH SCIENCES SYSTEM
 PARENT HANDBOOK A PATIENT CENTERED ORGANIZATION The University of Illinois Hospital and Clinics is a patient centered organization. Providing safe, high-quality and cost-effective care for our patients
PARENT HANDBOOK A PATIENT CENTERED ORGANIZATION The University of Illinois Hospital and Clinics is a patient centered organization. Providing safe, high-quality and cost-effective care for our patients
A Sharper Phlebotomy Service
 A Sharper Phlebotomy Service Preparing for the future Submission for the 2014 Canterbury DHB Quality Improvement and Innovation Awards Megan Harris, Karen Heatley, Linda Boyce, Jaine Duncan Canterbury
A Sharper Phlebotomy Service Preparing for the future Submission for the 2014 Canterbury DHB Quality Improvement and Innovation Awards Megan Harris, Karen Heatley, Linda Boyce, Jaine Duncan Canterbury
Version 5010 Errata Provider Handout
 Version 5010 Errata Provider Handout 5010 Bringing Clarity & Consistency To Your Electronic Transactions Benefits Transactions Impacted Changes Impacting Providers While we have highlighted the HIPAA Version
Version 5010 Errata Provider Handout 5010 Bringing Clarity & Consistency To Your Electronic Transactions Benefits Transactions Impacted Changes Impacting Providers While we have highlighted the HIPAA Version
Northern Kentucky Independent District Health Department, KY. Accreditation Preparation and Quality Improvement Demonstration Sites Project
 Northern Kentucky Independent District Health Department, KY Accreditation Preparation and Quality Improvement Demonstration Sites Project Final Report May 30, 2008 Summary Northern Kentucky utilized an
Northern Kentucky Independent District Health Department, KY Accreditation Preparation and Quality Improvement Demonstration Sites Project Final Report May 30, 2008 Summary Northern Kentucky utilized an
SITE VISIT AGENDA Version
 Pre Site Visit -- Chart Review Preparation: 1. Contact your assigned Site Surveyor to discuss paper or electronic chart preferences for the chart review. 2. In addition to the charts requested below, please
Pre Site Visit -- Chart Review Preparation: 1. Contact your assigned Site Surveyor to discuss paper or electronic chart preferences for the chart review. 2. In addition to the charts requested below, please
Clerical Activities Study
 April, 1988 Chiistine J. Hanon Project Group: Carolyn M. Chang Evan L. Guttman Management Systems Department University of Michigan Hospitals Clerical Activities Study April, 1988 Project Group: Christine
April, 1988 Chiistine J. Hanon Project Group: Carolyn M. Chang Evan L. Guttman Management Systems Department University of Michigan Hospitals Clerical Activities Study April, 1988 Project Group: Christine
Operational Assessments: Utilizing Productivity Standards
 Operational Assessments: Utilizing Productivity Standards Mary Klimp CEO Queen of Peace Hospital 952.758.8101 mklimp@qofp.org Ross Manson Principal Eide Bailly 701.239.8634 rmanson@eidebailly.com Agenda
Operational Assessments: Utilizing Productivity Standards Mary Klimp CEO Queen of Peace Hospital 952.758.8101 mklimp@qofp.org Ross Manson Principal Eide Bailly 701.239.8634 rmanson@eidebailly.com Agenda
Root Cause Analysis (Part I) event/rca_assisttool.doc
 event/rca_assisttool.doc") (Part I) http://www.jcaho.org/accredited+organizations/sentinel+ event/rca_assisttool.doc Edited by Dr. E. Terry DIO Dr. S.K. Oliver OME Examines the reasons an error occurred Suggests changes to the system
(Part I) http://www.jcaho.org/accredited+organizations/sentinel+ event/rca_assisttool.doc Edited by Dr. E. Terry DIO Dr. S.K. Oliver OME Examines the reasons an error occurred Suggests changes to the system
Planning for Improved Access and Orientation Anjali Joseph Jain EDRA 35
 Hospital planning strategies for improving patient access and orientation within the hospital Anjali Joseph, College of Architecture, Georgia Institute of Technology Most hospitals have been designed through
Hospital planning strategies for improving patient access and orientation within the hospital Anjali Joseph, College of Architecture, Georgia Institute of Technology Most hospitals have been designed through
Title: VERIFICATION OF PROCEDURES TO BE PERFORMED
 Approved By: Garren Colvin, EVP/COO Responsible Parties: Alicia Humphrey, Director Outpatient Surgery Tracie Shelton, Director Patient Safety & Accreditation Policy No.: ACLIN-V-01 Originated: 01/01/11
Approved By: Garren Colvin, EVP/COO Responsible Parties: Alicia Humphrey, Director Outpatient Surgery Tracie Shelton, Director Patient Safety & Accreditation Policy No.: ACLIN-V-01 Originated: 01/01/11
Accreditation Beta Test Quality Improvement Project CENTRAL VALLEY HEALTH DISTRICT ENVIRONMENTAL HEALTH SERVICES IMPROVEMENT
 ENVIRONMENTAL HEALTH SERVICES IMPROVEMENT This report was completed by: Robin Iszler, Kali Lautt, Brenton Nesemeier EXECUTIVE SUMMARY Central Valley Health District (CVHD) is a two-county health department
ENVIRONMENTAL HEALTH SERVICES IMPROVEMENT This report was completed by: Robin Iszler, Kali Lautt, Brenton Nesemeier EXECUTIVE SUMMARY Central Valley Health District (CVHD) is a two-county health department
Caldwell Medical Center Departments
 Caldwell Medical Center Departments Surgery Medical / Surgery Same Day Surgery Lab Education Administration Special Care Unit Women s Center Admission Emergency Services Radiology Cardiac Rehab Admission
Caldwell Medical Center Departments Surgery Medical / Surgery Same Day Surgery Lab Education Administration Special Care Unit Women s Center Admission Emergency Services Radiology Cardiac Rehab Admission
PERIOPERATIVE CONSULTING SERVICES
 SPT Sourcing PERIOPERATIVE CONSULTING SERVICES Improve efficiency and financial savings. Surgical Supply Management Solutions Keep everyone in-sync and in control with THE RIGHT SUPPLIES AT THE RIGHT TIME.
SPT Sourcing PERIOPERATIVE CONSULTING SERVICES Improve efficiency and financial savings. Surgical Supply Management Solutions Keep everyone in-sync and in control with THE RIGHT SUPPLIES AT THE RIGHT TIME.
Decrease Doc-to-Decision Times for Major EMS Patients at Mount Carmel East
 Decrease Doc-to-Decision Times for Major EMS Patients at Mount Carmel East Academy for Excellence in Healthcare IAP C-08 MCE Sept. 14, 2016 fisher.osu.edu 1 Decrease Doc-to-Decision Times for Major EMS
Decrease Doc-to-Decision Times for Major EMS Patients at Mount Carmel East Academy for Excellence in Healthcare IAP C-08 MCE Sept. 14, 2016 fisher.osu.edu 1 Decrease Doc-to-Decision Times for Major EMS
Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home
 CANADIAN INCIDENT ANALYSIS FRAMEWORK Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home 2012 Canadian Patient Safety Institute All rights reserved. Permission is hereby granted to
CANADIAN INCIDENT ANALYSIS FRAMEWORK Case Study Comprehensive Analysis: Elopement from a Long- Term Care Home 2012 Canadian Patient Safety Institute All rights reserved. Permission is hereby granted to
AUDIT DEPARTMENT UNIVERSITY MEDICAL CENTER HIPAA COMPLIANCE. For the period October 2008 through May JEREMIAH P. CARROLL II, CPA Audit Director
 UNIVERSITY MEDICAL CENTER HIPAA COMPLIANCE For the period October 2008 through May 2009 JEREMIAH P. CARROLL II, CPA Audit Director Audit Department 500 S Grand Central Pkwy Ste 5006 PO Box 551120 Las Vegas
UNIVERSITY MEDICAL CENTER HIPAA COMPLIANCE For the period October 2008 through May 2009 JEREMIAH P. CARROLL II, CPA Audit Director Audit Department 500 S Grand Central Pkwy Ste 5006 PO Box 551120 Las Vegas
The Benefits of Standardization: Anesthesia Cart Standardization in 62 Operating Rooms Over 5 Surgical Sites
 The Benefits of Standardization: Anesthesia Cart Standardization in 62 Operating Rooms Over 5 Surgical Sites By Abdul N. Mansour, MHA, DBA, Scottsdale Healthcare August 2011 One of Arizona s largest health
The Benefits of Standardization: Anesthesia Cart Standardization in 62 Operating Rooms Over 5 Surgical Sites By Abdul N. Mansour, MHA, DBA, Scottsdale Healthcare August 2011 One of Arizona s largest health
Provider Service Expectations Transportation Services SPC 107 Provider Subcontract Agreement Appendix N
 Provider Service Expectations Transportation Services SPC 107 Provider Subcontract Agreement Appendix N Purpose: Defines requirements and expectations for the provision of subcontracted, authorized and
Provider Service Expectations Transportation Services SPC 107 Provider Subcontract Agreement Appendix N Purpose: Defines requirements and expectations for the provision of subcontracted, authorized and
A GUIDE TO Understanding & Sharing Your Survey Results. Organizational Development
 A GUIDE TO Understanding & Sharing Your Survey Results al Development Table of Contents The 2018 UVA Health System Survey provides insight and awareness gained through team member feedback, which is used
A GUIDE TO Understanding & Sharing Your Survey Results al Development Table of Contents The 2018 UVA Health System Survey provides insight and awareness gained through team member feedback, which is used
Security Management Plan
 Effective Date: 01/2017 1 of 10 I. Table of Contents: I Table of Contents II Authority III Purpose & Scope IV Policy Statement V The Joint Commission Standards VI Performance Standards VII DUPD Services
Effective Date: 01/2017 1 of 10 I. Table of Contents: I Table of Contents II Authority III Purpose & Scope IV Policy Statement V The Joint Commission Standards VI Performance Standards VII DUPD Services
A strategy for building a value-based care program
 3M Health Information Systems A strategy for building a value-based care program How data can help you shift to value from fee-for-service payment What is value-based care? Value-based care is any structure
3M Health Information Systems A strategy for building a value-based care program How data can help you shift to value from fee-for-service payment What is value-based care? Value-based care is any structure
Nurse to Nurse Handoff Report
 Patient Safety Exceeding Expectations Nurse to Nurse Handoff Report 6 Main Why are we here today? Patient Safety is at risk. 3 hour time gap of patients not being seen during report time. The most dangerous
Patient Safety Exceeding Expectations Nurse to Nurse Handoff Report 6 Main Why are we here today? Patient Safety is at risk. 3 hour time gap of patients not being seen during report time. The most dangerous
Enhancing Efficiency and Communication in Perioperative Services Through Technology
 Enhancing Efficiency and Communication in Perioperative Services Through Technology Linda Yoder, RN, BSN, MBA, Clinical Director, Perioperative Services, GI Lab, Cross Creek Ambulatory Center Every driver
Enhancing Efficiency and Communication in Perioperative Services Through Technology Linda Yoder, RN, BSN, MBA, Clinical Director, Perioperative Services, GI Lab, Cross Creek Ambulatory Center Every driver
The policy applies to all SHS employees involved in direct patient care and medical staff.
 Restraints Use of Violent - System Introduction Restraints, Use of Violent System Introduction SCOPE The policy applies to all SHS employees involved in direct patient care and medical staff. Implementation
Restraints Use of Violent - System Introduction Restraints, Use of Violent System Introduction SCOPE The policy applies to all SHS employees involved in direct patient care and medical staff. Implementation
University of Michigan Health System. Analysis of the Central Intake Process at University of Michigan Home Care Services
 University of Michigan Health System Program and Operations Analysis Analysis of the Central Intake Process at University of Michigan Home Care Services Final Report To: Kenneth Bandy, Director, Home Care
University of Michigan Health System Program and Operations Analysis Analysis of the Central Intake Process at University of Michigan Home Care Services Final Report To: Kenneth Bandy, Director, Home Care
Internship Program Information
 Internship Program Information Mission Statement: is dedicated to improving the health of the community through treatment, prevention, and enabling services Frances Nelson is a primary care medical and
Internship Program Information Mission Statement: is dedicated to improving the health of the community through treatment, prevention, and enabling services Frances Nelson is a primary care medical and
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NEWBORN INFANT/PEDIATRIC SECURITY POLICY #: EFFECTIVE DATE: REVISED DATE: (Neonatal) (Maternal) (Pediatric) (Security) 11/95 2/09, 11/09
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NEWBORN INFANT/PEDIATRIC SECURITY POLICY #: EFFECTIVE DATE: REVISED DATE: (Neonatal) (Maternal) (Pediatric) (Security) 11/95 2/09, 11/09
Organization Review Process Guide Perinatal Care Certification
 Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Workload Analysis of MVN Nurses Team 4 Final Report
 UNIVERSITY OF MICHIGAN Workload Analysis of MVN Nurses Team 4 Final Report Submitted to: Nancy Moran Rose, MPH, RN: Director of Home Care Nursing and MVN/MVC Operations Renee Curtis, RN: Vice-Chair UMPNC
UNIVERSITY OF MICHIGAN Workload Analysis of MVN Nurses Team 4 Final Report Submitted to: Nancy Moran Rose, MPH, RN: Director of Home Care Nursing and MVN/MVC Operations Renee Curtis, RN: Vice-Chair UMPNC