University of Michigan Health System Program and Operations Analysis. Anesthesia Technical Support Work Distribution Analysis.
|
|
|
- Marilynn Reynolds
- 6 years ago
- Views:
Transcription
1 University of Michigan Health System Program and Operations Analysis Anesthesia Technical Support Work Distribution Analysis Final Report To: Paul Salow, Clinical Department Administrator, Anesthesiology Zach Shoup, Management Engineer Fellow Program and Operation Analysis Mary Duck, Senior Management Engineer, Program and Operation Analysis From: IOE 481 Project Team 12 Amgad El-Sisi Giorgio Mavroleon Nikita Patel Aditya Sthanunathan Date: December 10, 2008
2 !"#$%&'(&)'*+%*+,& Executive Summary...1 UH and CVC... 1 Mott... 2 Recommendations... 2 Introduction...3 Background... 3 Key Issues... 4 Goals and Objectives... 4 Project Scope... 4 Support Provided by Operating Entities... 5 Approach and Methodology...5 Literature Search... 5 Observations... 6 Interviews... 6 Work Sampling Study... 6 Pager Log Analysis... 7 Analysis and Results...8 UH and CVC Findings and Results... 8 Observations... 8 Work Sampling Study Pager Log Study Mott Findings and Results Observations Work Sampling Study Pager Log Analysis Conclusions...24 Decreased Hours of Anesthesia per Anesthesia Technician Hours Worked Breakdown of Anesthesia Technician Workload Distribution Recommendations...26 Process Improvements Increasing and Improving Communication Compare UH and Mott and Reducing Variability in Staffing Level and Training Expected Impact...27 APPENDIX A: UH Work Sampling Data Collection...28 APPENDIX B: Mott Work Sampling Data Collection Sheet...29 APPENDIX C: Questions for Anesthesia Technicians...30 APPENDIX D: Questions for Mott CRNA...31 APPENDIX E: Work Sampling Study List of Tasks...32 APPENDIX F: Descriptive Statistics of Pages per Day for UH...33 APPENDIX G: Descriptive Statistics of Pages per Day for Mott...34 APPENDIX H: Anesthesia Machine Shutdown Standard Procedure...35
3 List of Tables and Figures Table 1 Task Family Descriptions 7 Table 2 Technician Hours Worked and Anesthesia Hours 24 Figure 1 UH Anesthesia Technician Task Family 11 Figure 2 UH Anesthesia Technician Task Families from 6am to 10pm 11 Figure 3 UH Anesthesia Technician Assistance Tasks 12 Figure 4 UH Anesthesia Technician Standard Tasks 12 Figure 5 Top 4 UH Anesthesia Technician Tasks throughout Workday 13 Figure 6 Total Number of Pages Sent to UH ATs during Workday 14 Figure 7 Number of Pages Sent to UH ATs by OR during September Figure 8 Number of Pages Sent to CVC ATs by OR during September Figure 9 Types of Pages Sent to UH ATs during September Figure 10 Mott Anesthesia Technician Task Family 18 Figure 11 Mott Anesthesia Technician Task Families from 6am to 9pm 19 Figure 12 Mott Anesthesia Technician Standard Tasks 20 Figure 13 Mott Anesthesia Technician Assistance Tasks 20 Figure 14 Top 4 Mott Anesthesia Technician Tasks throughout Workday 21 Figure 15 Total Number of Pages Sent to Mott ATs during Workday 22 Figure 16 Percentage of Pages Sent to Mott ATs by Location during September Figure 17 Types of Pages Sent to Mott ATs during September ii
4 Executive Summary The Anesthesiology Department at the University of Michigan Health System has seen a sharp decline in the productivity of Anesthesia Technicians based on their existing metric (Hours of Anesthesia per Anesthesia Technician Hours Worked). Additionally, administrators have been unable to quantify the distribution of Anesthesia Technician (AT) efforts across all Anesthesia Technician activities. The Clinical Department Administrator for the Anesthesiology Department has requested that the team gather data pertaining to the processes and daily routines of Anesthesia Technicians. To determine why the Anesthesiology Department has seen a decline in productivity, the team observed processes, interviewed anesthesia providers, collected data on Anesthesia Technician activity, and determined day-to-day functions and routines of Anesthesia Technicians. Using this information, the team aims to provide Anesthesiology administrators with information regarding the Anesthesia Technicians workload distribution, identify areas and processes that need improvement, and establish groundwork for future projects. The team followed a two-tiered approach for collecting the data needed for analysis. Qualitative data was gathered through a literature search, observing the Anesthesia Technicians, and interviewing key stakeholders in the Anesthesia administration. Quantitative data was collected through a work sampling study and the Anesthesia Technicians pager logs for September This data allowed the team to quantify the distribution of Anesthesia Technician tasks and the distribution of demand for tasks. The activities of ATs in University Hospital/Cardiovascular Center and Mott Children s Hospital were analyzed separately. The information from the pager logs, the work sampling study, and onsite observations was used to develop conclusions to help the Clinical Department Administrator make recommendations and conduct future lean projects. UH and CVC The key findings from the UH and CVC analysis include the following: Work sampling and pager log results indicate that ATs perform mostly Assistance (52%) and Standard tasks (35%). Work sampling confirms that the frequency of Assistance tasks dominates the frequency of Standard tasks during surgery hours. During non-surgery hours, ATs perform more Standard tasks than Assistance tasks. The most common Assistance tasks performed by ATs in UH are Room Turnovers and Blood Gas Lab Testing and the most common Standard tasks performed are Cart Stocking and Room Setup/Shutdown. The pager log analysis indicates that ATs are demanded the most between the hours of 7:30am and 2pm, with the busiest hour being 11am-12pm. 1
5 Mott The key findings from the Mott analysis include the following: Work sampling and pager log results indicate that ATs perform mostly Standard (43%) and Assistance tasks (41%). Work sampling confirms that Assistance tasks dominate Standard tasks during surgery hours. During non-surgery hours, ATs perform more Standard tasks than Assistance tasks. The most common Assistance task performed by ATs in Mott is Room Turnovers while the most common Standard tasks performed are Cart Stocking, Room Setup/Shutdown, and Set-up IVs. The pager log analysis indicates that ATs are demanded mostly during peak Mott surgery hours, between 7:30am and 1pm. Recommendations Based on the team s observations and the results of the analyses, five recommendations for future projects have been developed. Increasing the Anesthesia Metric by Process Improvements o Future projects should conduct an in-depth study of Standard and Assistance tasks and explore options to perform them more efficiently while adhering to the work style of Anesthesia Technicians. o Reducing process times and non-value added activities will also lead to more efficient work processes. Comparing UH and Mott to Develop Best Practices o A comparison of the standard practices between Mott and UH revealed several differences in the scheduling and organizational structures of the two Anesthesia Departments. The team believes that examining the effect of these differences on overall productivity could lead to useful insights and best practices. Increasing Communication o Increasing the level of communication in the Anesthesia Department through feedback systems will help identify problematic areas quickly and facilitate the development of solutions. Reducing the Variability in Staffing Level and Training o Reducing the variability in AT staffing should increase the reliability of Anesthesia Technicians and their overall job satisfaction. Training will reduce errors and enforce standards of procedure. 2
6 Introduction Anesthesia Technicians in the University of Michigan Health System (UMHS) provide operating room support. Their activities include retrieving equipment, turning over operating rooms, stocking anesthesia carts, and transporting patients. The Anesthesiology Department at the University of Michigan Health System has seen a sharp decline in the productivity of Anesthesia Technicians based on the existing hospital metric. Additionally, administrators are unable to quantify the distribution of Anesthesia Technician (AT) effort across all Anesthesia Technician activity. Therefore, the Clinical Department Administrator for the Anesthesiology Department has requested that the team gather data pertaining to the processes and daily routines that Anesthesia Technicians use for their jobs as well as identify areas for improvement. This information will serve as a basis for future analysis and improvement. The team has utilized a variety of methodologies, such as historical pager log data, work sampling studies, and interviews with anesthesia providers, including Certified Registered Nurse Anesthetists (CRNA), to identify problematic areas in the various anesthesia processes and evaluate whether productivity has declined. The purpose of this report is to present the team s methods, findings and conclusions regarding the distribution and functionality of Anesthesia Technician activities. In addition, the team provides recommendations for topics for future projects. Background Anesthesiology administrators use one metric to examine the productivity of their department: Hours of Anesthesia per Anesthesia Technician Hours Worked. This metric is a ratio of the number of hours that patients require the constant care of an anesthetic provider to the number of hours of paid Technician work. Technician work consists of tasks such as searching for supplies, turning over rooms, stocking carts, transporting patients, and troubleshooting equipment. Anesthesia Technicians worked nearly 68,000 hours in the 2008 fiscal year. Since 2002, University Hospital has seen a decrease in overall Anesthesia Technician work productivity. Hours of Anesthesia per Anesthesia Technician Hours Worked has declined 24% for University Hospital and 43% for Mott Children s Hospital. Anesthesiology administrators have provided these figures. There has also been an observed increase in the number of offsite cases requiring Anesthesia Technician attention and assistance. An offsite case is an operation or procedure that takes place outside of the main operating rooms of the University Hospital (UH), Mott Children s Hospital (Mott) and the Cardiovascular Center (CVC). These offsite procedures increase the traveling time for the Anesthesia Technicians to and from the procedure room. This increase of anesthesia activity outside the operating room could potentially explain the drop in the productivity of the Anesthesia Technicians. The specific distribution of AT work is unknown to administrators because the Technicians work fairly independently and travel throughout the hospital as required or called. ATs use pagers to receive calls for service and to communicate with each other. Technicians at Mott receive group pages, while those at UH receive individual pages. 3
7 Additionally, the Anesthesia Technicians who work during the afternoon shift use phones to communicate with each other. This background information pertaining to technician tasks, offsite activities, pager protocol, and the decline in overall work productivity served as the basis for the key issues of this project. The team has observed and interviewed Anesthesia Technicians, analyzed pager log data, and conducted a work sampling study to determine the current Anesthesia Technician workload distribution and identify areas of improvement. Key Issues The following were identified as the key issues of the project: Decreased Hours of Anesthesia per Anesthesia Technician Hours Worked Increased anesthesia activity outside the operating rooms that potentially reduces the efficiency of the Anesthesia Technicians Lack of understanding of Anesthesia Technician workload distribution Absence of a highly-organized means for dispatching Anesthesia Technicians Goals and Objectives To determine why productivity in the Anesthesiology Department has declined, the team achieved the following tasks: Observed processes, interviewed anesthesia providers, and collected data regarding Anesthesia Technician activity Determined day-to-day functions and routines of Anesthesia Technicians With this information, the project aims to: Project Scope Provide Anesthesiology administrators with information about the current work distribution of the Anesthesia Technicians Identify areas and processes that need improvement Lay groundwork for future projects The project included examining the responsibilities and daily workflows of the Anesthesia Technicians both inside and outside the operating room at UH, Mott, and CVC. This also included their offsite activities. The project did not include the activities of physicians, nurses or anesthesiologists. The working cultural issues were not examined. The team will not change the work processes; the project scope is limited only to identifying areas in need of improvement and laying groundwork for future projects. 4
8 Support Provided by Operating Entities Paul Salow, the Anesthesiology Clinical Department Administrator, is the project client and provided the team with the ongoing details and logistical information to ensure effective communication regarding the scope and requirements of the project. Additionally, the client provided the team with past pager log data for analysis. Zach Shoup, a Management Engineer Fellow with Program and Operation Analysis (POA) is the project coordinator. He clarified details and provided the team with insight into the structure and frameworks currently in place. Also, the coordinator supplied the team with the tools necessary to collect data. Approach and Methodology The team followed a two-tiered approach for collecting the data needed for the analysis. Qualitative data was gathered through conducting a literature search, observing the Anesthesia Technicians, and interviewing key stakeholders in the Anesthesia administration. This data provided the team with a strong background on the Anesthesia Department as a whole and the role that Anesthesia Technicians play within the department. Quantitative data was collected through a work sampling study and the analysis of Anesthesia Technician s pager logs for September This data allowed the team to quantify the distribution of Anesthesia Technician tasks and the distribution of demand for tasks. Literature Search The team completed a literature search with the purpose of identifying standards of practice for Anesthesia Technicians and methodologies for collecting data. The team utilized Internet searches and also examined the IOE 481 project database to identify similar projects. The website of the American Society of Anesthesia Technologists and Technicians (ASATT) details the required competencies of Anesthesia Technicians. The team compared the standards from this organization to the daily practices and routines of technicians at UH and Mott and has concluded that their job routines meet the standard expectations of Anesthesia Technicians. For example, ATs at UH and Mott are very well versed in the structure, function and care of all components of anesthesia delivery systems. ( Standards of Practice. American Society of Anesthesia Technologists and Technicians. October < The IOE 481 database did not contain information regarding Anesthesia Technicians. However it did contain information about similar projects in other departments. This information guided the selection of appropriate data collection and analysis tools such as the work sampling study and the pager log analysis. 5
9 The team was not able to find any literature or data pertaining to how much time Technicians spend or should spend completing their required duties. This lack of information may be attributed to the fact that Technician work is unpredictable. Observations The team observed the Anesthesia Technicians at Mott and UH between October 14, 2008 and November 24, Anesthesia Technicians were observed during both the day and afternoon shifts to understand the differences in task distribution and demand between the shifts. The team used clipboards with clocks to time some of the common tasks that Anesthesia Technicians perform, such as room turnovers and blood gas lab tests. Members of the team talked to the Technicians while they were observing them and asked them questions regarding the nature of the processes that Anesthesia Technicians perform (Appendix C). Data regarding the historical changes in the Anesthesia Department was also collected through the conversations with the Anesthesia Technicians. The notes taken by team members during the observation phase helped gauge the key concerns of Technicians and their thoughts on the different tasks they perform. Interviews The team conducted one formal interview on October 24, 2008 with the lead Mott CRNA in order to determine the key issues and expectations from the administrative perspective. The team developed a standard question sheet (Appendix D) to guide the interview. The team gained insights on the critical requirements of the anesthesia administration, the organizational structure of the anesthesia department, and some of the major problems currently seen by the anesthesia administration. The details of the work scheduling process and the distribution of incoming work were also discussed. The information retrieved from the interview provided the team with an actionable base for areas on which to focus. Work Sampling Study The team implemented a work sampling study, also known as a random beeper study, between November 7, 2008 and November 30, The purpose of this study was to quantify the distribution of Anesthesia Technician tasks. The CRNAs in UH and Mott were given three beepers each and were asked to randomly assign the beepers to Technicians each day, for both the daytime and afternoon shifts. The team developed two data collection sheets for UH and Mott (Appendices A and B) that listed the different tasks Technicians perform, sorted into the following categories: Standard Tasks, Assistance Tasks, and Additional Tasks. These task families are explicitly defined in Table 1 and listed in Appendix E. 6
10 Table 1 Task Family Descriptions Task Family Standard Task Assistance Tasks Additional Tasks Task Family Definition Tasks that are part of ATs daily routines and are expected to be done without being prompted Tasks that ATs are asked to perform by Operating Room personnel Tasks that are not classified as Standard or Assistance but still take up AT work time (i.e.: meetings, lunch, etc.) A general term for Standard, Assistance, or Additional Tasks The team met with the Mott Technicians on November 6, 2008 and with the UH Technicians on November 7, During the meetings, the team explained how the data collection sheets should be filled out. The Anesthesia Technicians were also given the opportunity to ask questions and voice their concerns regarding the work sampling study and the team members addressed those questions and concerns. Each day three Technicians in Mott and UH were expected to receive a beeper and a data collection sheet. The Technicians were expected to place a check mark next to the task they were performing whenever the beeper sounded. The beepers were programmed to ring an average of four times per hour according to a uniform random distribution. The team expected to collect a total of 90 data sheets from Mott and UH over the course of two weeks, 30 from Mott and a total of 60 from both shifts at UH. The technicians at Mott cooperated fully with the work sampling study; 33 completed sheets were received from Mott. However, problems were encountered with the Technicians at UH. There was a lot of resistance from the Technicians in response to being asked to carry the random beeper for the day. Some of the data collection sheets were returned incomplete or blank. Additionally, one of the beepers provided to UH was lost halfway through the data collection process. Thus, a full 60 sheet sample from UH was not collected; instead, only 40 sheets were available for data analysis. The data from the work sampling study was compiled into a Microsoft Excel spreadsheet then analyzed using pivot tables. For the purpose of this study, the team considered the most popular tasks to be those that make up the top 50% of all tasks performed; this cutoff provides an adequate balance between ease of analysis and representative data. Using this breakdown, the most popular tasks were evaluated in depth. Pager Log Analysis The team compiled existing data from pager logs provided by the Anesthesiology Department administrators. This pager log data illustrates the variety and frequency of tasks that are routinely requested of Anesthesia Technicians by operating room personnel. The team received pager data for 29 Technicians for September Each page was categorized into one of three groups: equipment, supplies (pharmacy or medical/surgical), or assistance. To maintain consistency, the team members entered the pager log data into an Excel spreadsheet together. Each page constituted a row in the spreadsheet. 7
11 By analyzing this data, the team arrived at several aggregate numbers: Average number of calls per day Distribution of calls across the day Average number of calls by category Call backs to rooms for unanswered calls Analysis and Results This section details the analysis the team conducted on the pager log data and the work sampling data. The team aimed to use this information to develop conclusions to help the Clinical Department Administrator make recommendations and conduct any future lean studies. The team analyzed the activities of ATs in University Hospital and Mott Children s Hospital separately. Based on qualitative observations, the team determined that UH and Mott function as two separate entities. The analysis for each hospital will be divided into two segments: Task Distribution and Time Distribution. The former strives to answer the question What do Anesthesia Technicians do? while the latter answers, When are Anesthesia Technicians asked to work? The information from the pager logs, the work sampling study, and onsite observations has been analyzed to arrive at answers to the questions. UH and CVC Findings and Results For the purpose of this report, the main University Hospital (UH) and Cardiovascular Center (CVC) are considered as one entity. UH Technicians perform weeklong rotations at CVC covering all Anesthesia Technician roles. This section of the report presents observations, results from the work sampling study, and results from the pager log analysis. Observations UH has three operating cores consisting of a total of 27 rooms. Approximately 28 Anesthesia Technicians service UH and CVC; however this number includes Temporary Technicians who may only work one day per week. The regular Technicians rotate duties between UH and CVC, but only the more trained Technicians are assigned duties in CVC. Additionally, one Technician at UH is assigned offsite duties each day. The Anesthesia Technician Supervisor leads the Technicians. The Supervisor is in charge of determining the Anesthesia Technicians schedules for the week and handling last minute scheduling changes, including overtime, as well as performing the regular Anesthesia Technician duties. The major issues that affect UH and CVC are: variability in case load and Anesthesia Technician availability, lack of formal training for incoming Technicians, lack of 8
12 communication between Technicians in certain situations, and lack of standardization in the way tasks are implemented. Variability with Staffing Levels and Scheduling Anesthesia Technicians face variability in the complexity of cases, in changes in the total staffing level, and in staffing issues when scheduled Technicians are not available. Since cases vary in nature, some take longer than others and some end at or around the same time. When multiple rooms finish at once, technicians usually ask each other for assistance to avoid delays. The most complex operations, such as liver transplants, require a single Technician to be in the room for the entire procedure which generally lasts for the whole shift. When these complex surgeries take place, the staffing level of Technicians is reduced, leading to the redistribution of the Technician s rooms among the other Technicians. Sometimes multiple complex surgeries occur simultaneously, which leads to severe understaffing. The Supervisor often remedies this situation by calling Technicians who are off-duty and requesting that they work overtime, but often the available Technicians must carry the additional workload. The overall number of Anesthesia Technicians employed varies from time to time, which adds to the variability in Anesthesia Technician workload. Employee terminations and seasonal Technician staffing are the two main causes of the variation observed in the Full Time Equivalent (FTE) count. The latter does not have a large effect on workload because it is offset by the variation in seasonal case demand, but employee terminations lead to rescheduling and redistribution of the AT operating room assignments. The large number of temporary Technicians also adds to the level of variability in the department; most temporary Technicians have other commitments, such as classes, and tend to be less reliable than the full time Technicians. When temporary Technicians miss their shift, the Supervisor has to reassign their rooms or find another Technician to fill in. Since the number of Technicians on the afternoon shift (4) is much less than the day shift (8), if an afternoon Technician misses their shift, a day Technician is obligated to work overtime to fill that spot. Sick leave and vacation time also add to the variability in staffing levels. Vacation time has a smaller impact because it is anticipated, whereas sick and medical leaves cause greater scheduling problems. Staff Training Issues Technicians indicated that the type and amount of training they received before starting the job varied. Some Technicians had a single day of training, while others were trained for up to a week. The training that technicians receive is based on shadowing a full time Technician and observing how he or she completes different tasks. The Supervisor mentioned that in the past there was a Training Technician position that no longer exists. The Supervisor felt that having this position would improve the quality of incoming Technicians. In the past, new recruits would shadow only the Training Technician for six weeks; currently recruits shadow multiple Technicians depending on availability. Communication Issues between Technicians and between Shifts Anesthesia Technicians seek assistance from each other to balance their workload. This most frequently occurs when two of a Technician s operating rooms vacate at the same 9
13 time, or when a Technician is paged to do something while he is already busy. In these situations where the workload becomes too much for one person, other Technicians are called upon for help. For this reason, having an accessible and effective line of communication is critical. The current methods of communication are to use the paging computers in the operating rooms and to contact the nurse s desk. The afternoon Technicians use Nextel phones to directly contact other Technicians. The daytime Anesthesia Technicians told the team that they used phones in the past, and expressed the desire to have phones. Standardization Issues When observing the Anesthesia Technicians, the team noticed that while best practices exist, standardized operating procedures are not always followed. For example, the procedure for room shutdown is not always followed; this led the supervisor to post pictures of how rooms should look at the end of the day in the Anesthesia Workroom, see Appendix H. Another best practice is for the daytime Technicians, before leaving, to update the afternoon Technicians on anything they need to know regarding the rooms they will be taking over. These procedures are often dismissed which causes some Technicians to do excess work. When an operating room vacates, the nurse in the room is expected to notify the Technicians by calling out the room number using the OR intercom system. Anesthesia Technicians have complained that this standard procedure is not always followed, which often leads to physicians paging ATs to turnover a room. Because of this situation, some ATs have developed a best practice of periodically monitoring their rooms to ensure that the surgery has not finished. Having effective methods to communicate room vacancy will allow ATs to focus on their other tasks. Work Sampling Study The work sampling study identified the most frequent tasks performed by Anesthesia Technicians. Figure 1 breaks down the work ATs perform by task family. Refer to Table 1 for the task family descriptions and Appendix E for a complete list of tasks in each family. The chart indicates that ATs perform mostly Assistance and Standard Tasks. As per the Anesthesia Technician job description, ATs are expected to help Operating Room personnel and perform tasks as part of their daily routines. 10
14 )'#$!"#$!"#$"%&'(")*+),*&'-),'./.)'&)01)!'#$ ('#$ %'#$ "'#$ &'#$ %!#$ &%#$ '#$ *++,+-./01$ 2-./3.43$5.+6+$ *33,78/.9$ Figure 1 - UH Anesthesia Technician Task Family, n=752, Collected by UH ATs from Nov. 7 Nov. 30, 2008 Figure 2 displays how AT task families change throughout the workday.!"#$"%&'(")*+)23").4"%&)4"#)&'./))'&)01) &''#$ <'#$ ;'#$ :'#$ )'#$!'#$ ('#$ %'#$ "'#$ 2=4>14,1+$?1>,/$$.-$:@%'$.A$ 2-./3.43$5.+6+$ *++,+-./01$5.+6+$ &'#$ '#$ *33,-,8/.9$5.+6+$$ Figure 2 - UH Anesthesia Technician Task Families from 6am to 10pm, n=752, Collected by UH ATs from Nov. 7 Nov. 30, 2008 Figure 2 shows that as the day progresses, ATs perform more Assistance tasks and fewer Standard tasks. This pattern agrees with the observation that as the number of surgeries increase over the day, the ATs tend to be called on more to perform Assistance tasks. 11
15 Therefore, they have less time to perform Standard tasks. Furthermore, the increase in the number of Standard tasks from 6-10pm can be attributed to the decrease in surgeries, thereby giving the ATs more time to perform Standard tasks. Charts of Assistance and Standard Tasks (Figures 3 and 4 respectively) break down the tasks in these two categories.!"#$"%&'(")*+),*&'-),'./.)'&)01) &;#$ &)#$ &(#$ &"#$ &'#$ ;#$ )#$ (#$ "#$ '#$ &!#$ &&#$ <#$ )#$!#$ (#$ "#$ "#$ "#$ &#$ &#$ &#$ '#$ 5..6.&'%$"),'./.) Figure 3 UH Anesthesia Technician Assistance Tasks, n=752, Collected by UH ATs from Nov. 7 Nov. 30, 2008!"#$"%&'(")*+),*&'-),'./.)'&)01) &(#$ &"#$ &'#$ ;#$ )#$ (#$ "#$ '#$ &%#$ &"#$ )#$ (#$ %#$ "#$ &#$ 7&'%8'#8),'./.) Figure 4 - UH Anesthesia Technician Standard Tasks, n=752, Collected by UH ATs from Nov. 7 Nov. 30,
16 The above charts indicate that the most common Assistance tasks are Room Turnover and Blood Gas Lab Testing while the most common Standard tasks are Cart Stocking and Room Setup/Afternoon Shutdown. These results match the team s observations. Figure 5 plots the variations in the four most common UH tasks from 6am to 10pm. These four tasks comprise the top 50% of all tasks performed in UH.!"#$"%&'(")*+)23").4"%&)4"#)&'./))'&)01) <'#$ ;'#$ :'#$ )'#$!'#$ ('#$ %'#$ "'#$ &'#$ '#$ 2=4>14,1+$?1>,/$$.-$:@%'$.A$ B.4-$$ 2-806,/>$ C88A$21-=DE$ *F-14/88/$$ 2G=-38H/$ C88A$$ 5=4/8I14$ J9883$K.+$$ L.?$51+-,/>$ Figure 5 - Top 4 UH Anesthesia Technician Tasks throughout Workday, n=752, Collected by UH ATs from Nov. 7 Nov. 30, 2008 The peaks and troughs in Figure 5 are in accordance with the earlier statement that Assistance tasks are performed more often during surgery hours while Standard tasks are performed less. As the day progresses, Room Turnovers and Blood Gas Lab Testing increase while Cart Stocking and Room Setup fall sharply. Observations from UH maintained that the peak surgery hours are around 8am-1pm; the peaks in room turnovers and the increasing demands for blood gas labs match this statement. Lastly, Room Setup/Afternoon Shutdown peaks at 6am; on-site observations indicated that at this time, all ATs are preparing rooms for surgery. However, after surgeries begin at 7:30am, this value drops to nearly 0 until the end of peak surgery hours. Pager Log Study The pager log study for UH illustrates the times when anesthesia support is most demanded by operating room personnel. A categorical analysis of each entry also reveals the specific types of requests for which Technicians are most likely to be paged. Pagers are only one form of communication between hospital personnel and ATs; therefore, these results represent only a portion of requests made to the ATs. Using Microsoft Excel to compile all the relevant data, the team determined that ATs were sent an average of 167 pages per day during September
17 Figure 6 shows the distribution of pages sent to ATs in UH during the workday in September The values shown in the graph represent the total number of pages for all ATs from UH during each time period. 9:3;"#)*+)4'(".) "!'$ "''$ &!'$ &''$!'$ 2=4>14,1+$?1>,/$$.-$:@%'$.A$ '$ Figure 6 - Total Number of Pages Sent to UH Anesthesia Technicians during Workday in September 2008, n=2217, Compiled by IOE 481 F08 Team 12 Figure 6 shows that ATs receive a majority of their pages between 8am and 2pm, with the busiest hour being 11:00am to 12:00pm. These results are consistent with the team s observations that ATs receive most of their pages during peak surgery hours. The team also used the pager log data to determine which operating rooms most demand AT support. Figures 7 and 8 show the busiest UH and CVC operating rooms.!"#$"%&'(")*+)'--)01)<=)!'(".) &'M'#$ <M'#$ ;M'#$ :M'#$ )M'#$!M'#$ (M'#$ %M'#$ "M'#$ &M'#$ 'M'#$ ;$ )$ ($ ":$ :$!$ &'$ "$ %$ &($ &$ &)$&:$";$&%$&!$""$ <$ "<$"&$"($&&$"'$&<$&"$&;$"!$ Figure 7 - Number of Pages Sent to UH Anesthesia Technicians by OR during September 2008, n=1414, Compiled by IOE 481 F08 Team 12 14
18 !"#$"%&'(")*+)'--)>?>)<=)!'(".) "'M'#$ &;M'#$ &)M'#$ &(M'#$ &"M'#$ &'M'#$ ;M'#$ )M'#$ (M'#$ "M'#$ 'M'#$ &'$ ($ ;$ )$ %$ &$ "$!$ <$ :$ Figure 8 - Number of Pages Sent to CVC Anesthesia Technicians by OR during September 2008, n=169, Compiled by IOE 481 F08 Team 12 Figures 7 and 8 reveal uneven distributions of demand for Anesthesia Technicians in UH and CVC operating rooms. Management should use this information in the future to manage the AT room assignment process. The team determined the categorical distribution of tasks for which ATs in UH are paged (see Figure 9).!"#$"%&'(")*+)4'(".) %!#$ %'#$ "!#$ "'#$ &!#$ &'#$!#$ '#$ "<#$ ""#$ &:#$ &"#$ <#$ :#$ &#$ &#$ *++,+-./01$ *3A,/$ NO=,DA1/-$PG.4A.0Q$ R13E2=4>$ P14+8/.9$ B.99?.06$ R,+0$ Figure 9 - Type of Pages Sent to UH Anesthesia Technicians during September 2008, n=2217, Compiled by IOE 481 F08 Team 12 As noted in the observations, ATs in UH are paged most often for Assistance requests (blood gas labs, patient transfer, room turnover) and Administrative requirements (called to front desk, staff scheduling, etc.). It is important to note that only 1% of all pages are Callback requests corresponding to unperformed tasks. This low number indicates that ATs are performing almost all of their tasks successfully upon first request. 15
19 Mott Findings and Results This section of the report will be divided into observations, results from the work sampling study, and results from the pager log analysis. Observations Mott Technicians are responsible for nine onsite operating rooms, two treatment rooms, Obstetrics, MRI and all offsite locations handling pediatric cases. Shift Information Mott has twelve Anesthesia Technicians: eight work daily 6 am to 2:30 pm shifts, one works daily from 6:30 am to noon, one works daily from noon to 8:30 pm, and one works daily from 1:00 pm to 9:30 pm. Additionally, one Technician works from noon to midnight on Monday through Wednesday and Friday; on Thursday, two Technicians work this shift. Interview with Lead Mott CRNA Through the interview with the lead Mott CRNA, the key requirements of Anesthesia Technicians from an administrative standpoint were confirmed. The administration reported that the key Anesthesia Technician tasks include the following: Troubleshoot and set-up machines completely Know which equipment and supplies are needed for each type of case Monitor stock levels in anesthesia carts continuously Set-up IVs Keep a full oxygen tank in the operating room at all times The lead CRNA also named several factors that are critical to quality: timeliness and knowledge of case needs and machinery. Also, the key failure areas were introduced during the interview. The critical failure areas include supplies missing from the anesthesia cart, pages remaining unanswered, and improper setup of the operating rooms. All of these failure modes can lead to rework and delays. Additionally, the general organizational structure of Mott Anesthesia Technicians was conveyed to the team during the interview. Mott has three lead Technicians: the first monitors the equipment and is the expert on troubleshooting problems; the second allocates daily room assignments; and the third handles staff training, conducts the orientation of new Technicians, and ensures that each Technician maintains practical requirements. This system of three lead Technicians was implemented in July Prior to July 2008, the second lead Technician was in charge of all these duties and felt overwhelmed. Offsite and Communication Issues One of the Mott Technicians covers all of the offsite locations each day, and this role is rotated every week. The offsite locations include the Electrophysiology Lab, 16
20 Catheterization Lab, UH Burn Unit, Interventional Radiology, Radiation, etc. Technicians have expressed that two people (instead of just one) would much better manage the offsite role. The offsite cases are walking intensive. Technicians on occasion have worn pedometers and have discovered that on an exceptionally busy day, they can walk up to 11 miles while covering their offsite duties. This excess of walking is because offsite cases require multiple round trips throughout the hospital. At a minimum, an offsite procedure requires one trip for the anesthesia cart, one trip for the anesthesia machine, and if necessary, one more trip for a stretcher. This equipment ranges from approximately 200 lbs to 450 lbs, and only some of the Technicians are strong enough to transport multiple pieces of equipment at once. Moreover, if any requests are made for additional supplies, equipment, or assistance, extra trips are necessary. Communication between the offsite Technician and the rest of the Technicians is ineffective. Frequently, the offsite Technician will receive a page with a request for supplies, equipment, or assistance but will not be immediately available to respond. As a result, a page will be sent to all Technicians with the same request. By the time the offsite Technician is available, he or she will be unaware as to whether someone else has fulfilled the request. This lack of communication requires the offsite Technician to perform additional, non-value added work. Offsite equipment frequently becomes lost due to inadequate communication, especially between shift changes. At 2:30pm, most Technicians leave and only three are on staff for the afternoon. If the offsite Technician ends his or her workday at 2:30pm, one of the afternoon Technicians will need to locate and transport the offsite equipment. Sometimes, the offsite Technician does not effectively communicate the status of this equipment to the afternoon shift, which leads to very lengthy equipment searches. If multiple carts and machines need to be transported, two of the three afternoon Technicians will need to perform this task, leaving only one Technician to cover all requests from the operating rooms. On one observed occasion, two machines and two carts from Mott were at UH and needed to be returned. Two of the three afternoon Technicians spent a total of 38 minutes locating and transporting this equipment. One more source of excess effort comes from setting up anesthesia equipment that is ultimately not used. Frequently, Technicians are not informed of case cancellations; or children undergoing procedures at offsite locations will opt to forgo anesthesia. This ineffective communication leads to non-value added work. Space Inadequacies Space is valuable in the anesthesia workroom and other nearby locations. If an empty spot opens up, something promptly fills the void. The Technicians used to have a larger workroom, but it was turned into an operating room. The current room is much smaller. Also, there are no empty walls against which Technicians can place carts that are being stocked. Instead, the carts are situated against the supply shelves, effectively blocking access to that equipment. The carts must then be shuffled around the small space in order to reach equipment that needs to be stocked. Also, once the pharmacy closes at 3:00pm, 17
21 CRNA s must acquire narcotics from the dispenser and store them in the safe, both located in the anesthesia workroom. Technicians would prefer this equipment to be situated elsewhere because it takes up much of the limited space and leads to added clutter and commotion in the workroom during the afternoon shift. Source of Backups Technicians feel that there are many backups and delays and they must often work through their lunch break. Technicians ideally open their rooms by 7:00am, but they are required to wait for the nurses to start opening the sterile field. The nurses are frequently late to get started and the Technicians sometimes do not get a chance to begin until almost 7:30am, which is the scheduled start time for morning cases. Thus, the workload backs up and Technicians become pressed for time preparing for cases. Work Sampling Study The frequency of the different task categories performed by Anesthesia Technicians is shown in Figure 10.!"#$"%&'(")*+),*&'-),'./.)'&)@*A) (!#$ ('#$ %!#$ %'#$ "!#$ "'#$ &!#$ &'#$!#$ (%#$ (&#$ &)#$ '#$ 2-./3.43$5.+6+$ *++,+-./01$ *33,78/.9$ Figure 10 - Mott Anesthesia Technician Task Family, n=672, Collected by Mott ATs from Nov. 7 Nov. 30, 2008 The chart indicates that the ATs work distribution is approximately evenly divided between Standard Tasks (43%) and Assistance Tasks (41%), with Additional Tasks only taking up about 16% of the AT s time. Figure 11 expands the information from Figure 10 to provide insight into how the AT s work distribution changes over the course of the day. 18
22 &''#$ <'#$ ;'#$ :'#$ )'#$!'#$ ('#$ %'#$ "'#$ &'#$ '#$ *++,+-./01$5.+6+$ 2-./3.43$5.+6+$ *33,-,8/.9$5.+6+$$ Figure 11 - Mott Anesthesia Technician Task Families from 6am to 9 pm, n=672, Collected by Mott ATs from Nov. 7 Nov. 30, 2008 Surgeries begin at 7:30 am every day, except Thursday, which has a late start of 8:30 am. Figure 11 shows that between 7 am and 3pm, the peak surgery hours, ATs perform more Assistance tasks and fewer Standard Tasks. While surgeries are in progress, ATs are called upon to assist in the operating rooms. As long as they are primarily performing Assistance tasks, there is less time available for Standard tasks. Once the surgeries begin to drop off around 3pm, a sharp decrease in the number of Assistance tasks performed is observed, while the number of Standards tasks begins to increase. Figures 12 and 13 break down the most common tasks in the Standard and Assistance categories. 19
23 &)#$ &(#$ &"#$ &'#$ ;#$ )#$ (#$ "#$ &(#$ &%#$ &"#$ )#$ %#$ "#$ '#$ Figure 12 - Mott Anesthesia Technician Standard Tasks, n=672, Collected by Mott ATs from Nov. 7 Nov. 30, 2008!"#$"%&'(")*+),*&'-),'./.)'&)@*A) &"#$ &'#$ ;#$ )#$ (#$ "#$ &&#$ :#$!#$ (#$ (#$ %#$ %#$ "#$ "#$ "#$ "#$ &#$ &#$ &#$ '#$ Figure 13 - Mott Anesthesia Technician Assistance Tasks, n=672, Collected by Mott ATs from Nov. 7 Nov. 30,
24 Figure 11 indicates that the most common Standard Tasks are Cart Stocking, Room Setup/Afternoon Shutdown, and Setup IVs; these tasks make up 76% of ATs Standard Tasks. There is a wider range of Assistance tasks that ATs perform compared to Standard Tasks. Figure 13 indicates the most common Assistance Tasks are Room Turnover, OR Standby, and Bring Equipment; these tasks make up 47% of Assistance tasks. These results match the team s qualitative observations in Mott. Figure 14 plots the changes in the level of the four most common Mott tasks from 6am to 9pm. These four tasks comprise the top 50% of all tasks performed in Mott.!"#$"%&'(")*+)23").4"%&)4"#)&'./))'&)@*A) &"'#$ &''#$ ;'#$ )'#$ ('#$ "'#$ '#$ 2=4>14,1+$?1>,/$$.-$:@%'$.A$ $B.4-$2-806,/>$ $C88A$5=4/8I14$ $C88A$21-=DE*S14/88/$2G=-38H/$ 21-T=D$UV+$ Figure 14 - Top 4 Mott Anesthesia Technician Tasks throughout Workday, n=672, Collected by Mott ATs from Nov. 7 Nov. 30, 2008 Figure 14 illustrates that the demand for the Assistance task, Room Turnover, rises during surgery hours while the Standard tasks, Cart Stocking, Room Setup, and Set-up IVs, are performed less. As the day progresses and the number of surgeries rises, Room Turnover increases while Cart Stocking, Room Setup, and Set-up IVs fall sharply. Qualitative observations from Mott maintained that the peak surgery hours are around 8am-5pm; the peaks in room turnovers match this observation. ATs are frequently called in to perform Room Turnovers as surgeries begin and end. Lastly, Room Setup/Afternoon Shutdown peaks at the 6am timeslot; this is because at this time, all ATs are getting their respective rooms prepared for surgery. However, once surgeries begin, this value falls sharply until it is time to shut down the room later on in the afternoon or evening. 21
25 Pager Log Analysis The pager log studies at Mott gave the team great insight into when ATs are most demanded by hospital personnel. Further analysis also revealed the type of work ATs are most likely to be called in for. Since pagers are only one form of communication between hospital personnel and ATs, these results represent only a segment of what is truly requested of the ATs. Using Microsoft Excel to compile all of the relevant data, the team determined that ATs are sent an average of 97 pages per day over the month of September Figure 15 shows the distribution of pages sent to ATs in UH during the workday in September The values shown in the graph represent the total number of pages for all ATs from UH during each time period. B#"C:"%$D)*+),'./.) "!'$ "''$ &!'$ &''$!'$ 2=4>14,1+$?1>,/$$.-$:@%'$.A$ '$ Figure 15- Total Number of Pages Sent to Mott Anesthesia Technicians during Workday in September 2008 at Mott, n=1240, Compiled by IOE 481 F08 Team 12 Figure 16 (see next page) shows which locations most demand Mott AT support. 22
26 !"#$"%&'(")*+)'--)<=)!'(".) &)M'#$ &(M'#$ &"M'#$ &'M'#$ ;M'#$ )M'#$ (M'#$ "M'#$ 'M'#$ :$ ;$ <$ ($ %$ &$ RCU$!$ "$ B.-G$ )$ *PC$ 5W&$ X=0R13$ B5$ NP$ 5W"$ */>,8$ C.3$ J8/1$ 20./$ YJ$ RPZ$ UC$ P*BZ$ Figure 16 - Percentage of Pages sent to Mott Anesthesia Technicians by Location during September 2008, n=646, Compiled by IOE 481 F08 Team 12 Figure 16 reveals an uneven distribution of demand for Anesthesia Technicians in Mott anesthesia locations. Figure 17 shows the types of work for which Mott ATs were most requested as a percentage of work by category. %'#$ ";#$ "!#$ "'#$ ""#$ "'#$ &!#$ &(#$ &'#$ ;#$ :#$!#$ '#$ *++,+-./01$ *3A,/$ P14+8/.9$ NO=,DA1/-$ R13E2=4>$ PG.4A.0Q$ B.99?.06$ R,+0$ &#$ &#$ Figure 17 - Type of Pages Sent to Mott Anesthesia Technicians during September 2008, n=1240, Compiled by IOE 481 F08 Team 12 As noted in the observations, ATs in Mott are paged mostly for Assistance (blood gas labs, room turnover, patient transfers) and Administrative (call to front desk, staff scheduling, etc.) tasks. One anomaly is the large number of Personal pages sent to ATs in Mott; the graph shows that 20% of all pages sent were personal during September It is inconclusive whether this surge of personal pages hinders AT work efficiency; 23
27 however, it would be wise for management to gather further information with respect to the sources of these personal pages to ensure that AT work is not hindered. Conclusions This analysis has provided closure to many of the client s chief issues. The following section addresses two key issues: the decreasing anesthesia metric and the lack of understanding of Anesthesia Technician workload distribution. Decreased Hours of Anesthesia per Anesthesia Technician Hours Worked One of the main issues that prompted this investigation was the observed decline in Hours of Anesthesia per Anesthesia Technician Hours Worked. This study indicates that the decline of this ratio can be attributed to an increase in Technician Hours Worked. Unpredictable conditions such as employee termination, temporary Technician availability, sick leave, and vacation time have affected overall Technician staffing and are a large source of variability. Table 2 shows that from 2002 to 2008, Overtime hours (OT) are up 18.6% and Temporary hours (Temp/TOP) are up a staggering 332.7%. Based on observations and interviews, the team has concluded that staff shortages due to variability have required the department to authorize an excess of overtime and temporary hours, driving up Technician Hours Worked and thus decreasing the productivity metric. Table 2 Technician Hours Worked and Anesthesia Hours - Data provided by Anesthesia Department WORKED HOURS ANESTHESIA HOURS Fiscal Year Regular OT Temp/TOP Total OR Offsite Total ,906 3,507 1,986 37,399 77,986 5,971 83, ,684 2,938 3,154 40,776 81,496 6,689 88, ,524 3,608 2,466 41,598 87,818 6,857 94, ,613 4,067 2,578 47,258 93,335 8, , ,635 4,542 6,905 56,082 94,032 11, , ,820 4,708 10,067 61,595 90,991 12, , ,992 4,159 8,593 67,743 92,426 14, ,546 % Increase 72.40% 18.60% % 81.10% 18.50% % 26.90% However, the team has further concluded that a more significant reason for the decline in productivity stems from the 72.4% increase in Regular hours worked. Regular hours are a much larger fraction of Total hours worked in comparison to either Overtime or Temporary hours. The heavier weight of the 72.4% increase means that Regular hours contribute much more to the decline in the productivity metric. The required workload has increased as well, but not as much as Total Hours Worked. This indicates that more Regular hours are now needed to complete all duties during a given day, meaning that the Anesthesia Technician job over the last several years has 24
28 become less efficient. If Anesthesia Technician jobs were more efficient, fewer hours of work would be required on a given day, and the overall number of regular hours would go down, thus improving the anesthesia metric. Breakdown of Anesthesia Technician Workload Distribution The pattern of tasks performed over the workday and the distribution of the Anesthesia Technician workload varied considerably between UH and Mott. However, ATs at both locations received the majority of their pages during the same hours of the workday. University Hospital Work sampling studies show that ATs at UH perform mostly Assistance (52%) and Standard tasks (35%). Further stratification indicates that the most common Assistance tasks performed in UH are Room Turnovers and Blood Gas Lab Testing. The most common Standard tasks performed are Cart Stocking and Room Setup/Shutdown. Expanding this information over the span of a workday reveals that ATs perform most of their Standard tasks in the early morning hours. However, as surgeries begin, the number of Standard tasks performed drops by 66% (attributed to a sharp decline in Room Setup/Shutdown) while the number of Assistance tasks, namely Room Turnovers in the morning hours and Blood Gas Lab Testing in the afternoon hours, increase accordingly. This pattern is reversed again at approximately 5pm when the surgeries end. Thus, ATs have more time to perform Standard tasks and prepare for the next day. Demand analysis of ATs, quantified by pager log studies, indicated that 51% of all pages between the hours of 8am and 2pm were related to assistance and administrative tasks. These results correspond to the steep rise in Assistance tasks, as shown by the work sampling study over the same time frame. In conclusion, the distribution of AT tasks and demand of ATs are very closely related; as ATs are demanded more frequently during peak hours, Assistance tasks outnumber Standard tasks. In UH, the high variability of tasks for which ATs are demanded (as shown by pager log results) causes visible stress and fatigue. This is validated by the increase in Additional non-value added tasks at peak hours. Mott Children's Hospital Work-sampling results indicate that Mott ATs also perform mostly Standard and Assistance tasks; however the percentage breakdown is more even than that of UH: 43% and 41% for Standard and Assistance Tasks respectively. The most common Assistance task performed Room Turnover while the most common Standard tasks performed are Cart Stocking, Room Setup/Shutdown, and Set-up IVs. Together, these represent the four most common tasks performed in Mott over the time period that ATs were studied. When expanded over the span of a workday, the pattern is similar to that of UH; Standard tasks decrease while Assistance tasks (and Additional tasks) increase over the workday. In the early morning hours, Mott ATs perform Set-up IVs and Room Setups to prepare for surgeries. Work-sampling results show that after surgeries begin in Mott, ATs perform mostly Room Turnovers. As the peak hours end, Mott ATs perform Cart Stocking (a Standard task), to replenish stock and prepare for the upcoming day. 25
29 Demand analysis of ATs at Mott, quantified by pager log studies, indicated that 50% of all pages between the hours of 8am and 2pm are related to assistance and administrative tasks. These results correspond to the rise in Assistance tasks, as shown by the work sampling study, over the same time frame. Using qualitative observations, the team maintains that the organizational structure at Mott promotes active communication between ATs and managers. In conclusion, the distribution of AT tasks and demand of ATs are very closely related; as AT are demanded more frequently during peak hours, the number of Assistance tasks dominates the Standard tasks. Recommendations Based on the team s observations and the results of the analyses, four areas of focus have been identified as possible future projects. Process Improvements Due to the inefficiency indicated by the declining Hours of Anesthesia per Anesthesia Technician Hours Worked metric, future projects should look at the most common tasks of Anesthesia Technicians and improve those specific processes. Improvements in the most common processes (as quantified by the work sampling study) will lead to the greatest improvement in overall efficiency. Determining the effectiveness of each AT while they perform key tasks during peak hours and implementing standardized procedures will improve workload distribution. The team recommends that management take a closer look at the most frequently performed tasks, Standard and Assistance, to ensure that they are being performed at the right time and for the right amount of time to minimize AT stress at peak hours. Future projects should study these tasks and explore options to perform them more efficiently while adhering to the work style of Anesthesia Technicians. Increasing and Improving Communication The team recommends investigating different feedback methods that ATs can utilize to effectively communicate with each other regarding the status of complete and incomplete work. A lot of effort is wasted due to ineffective communication. Also, during the observations for this project, ATs had a lot of questions and comments pertaining to administrative procedures. Increasing communication between the various levels of the Anesthesia Department will help identify problematic areas quickly and facilitate the development of solutions. 26
30 Compare Practices Between UH and Mott A comparison of the standard practices between Mott and UH revealed several differences in the scheduling and organizational structures of the two Anesthesia Departments: the staggered AT shifts in Mott versus the two shift system in UH, and the three lead Technician organizational system in Mott versus the single Supervisor Technician system in UH. The team believes that examining these differences in greater detail could lead to useful insights and best practices which if implemented could greatly improve overall productivity Reducing Variability in Staffing Level and Training Another area of improvement is reducing the controllable variability in the Anesthesia Department. Although the caseload in both hospitals is not controllable, the level of staffing is. Reducing the variability in AT staffing should increase the reliability of Anesthesia Technicians and their overall job productivity. The level of AT training directly correlates to how effective and productive Technicians can be, so training procedures should be further examined in Mott and UH. Increasing the amount of formal training and standardizing procedures that ATs perform will reduce the amount of errors and wasted time. The Team believes that implementing these recommendations through lean projects will allow the anesthesia administration to increase the effectiveness and satisfaction of ATs without having to increase the number of AT hours, thus improving the productivity metric. Expected Impact This report provides for an increased awareness of Anesthesia Technician activities and quantifies the current state of AT workload distribution. Additionally, areas in need of improvement have been identified as a possible basis for future project consideration. 27

31 APPENDIX A: UH Work Sampling Data Collection 28

32 APPENDIX B: Mott Work Sampling Data Collection Sheet 29
33 APPENDIX C: Questions for Anesthesia Technicians 1. Can you list the different activities and tasks you perform? 2. Please rank them according to frequency. Please rank them according to the amount of time they take up. 3. Can you explain the key steps of the different procedures you perform? 4. Are there any issues that systemically lead to wasted time or effort? 5. Do you have any major frustrations and/or grievances about the way things are done? 6. How are offsite duties assigned? 7. What do you do to turnover a room? 8. How much overtime do you usually have? 9. What changes have occurred during your time? How have they affected your job? 30
34 APPENDIX D: Questions for Mott CRNA 1. What are the most important duties and roles that you need the techs to fulfill? Can you rank them by relative importance? 2. What are the key parameters that measure the quality of tech work? Are any of them currently being measured? 3. What are the biggest areas of failure/problems occurring right now? Are there any reoccurring or common causes for these failures/problems? 4. How is the anesthesia department organized? How is tech work delegated and managed? 5. Who is in charge of determining the tech schedules? Is there a specific scheduling process? How are call and week end hours assigned? 6. How is work delegated and divided? Are techs assigned to cores, work rooms, or charts? Do all of the techs perform the same set of tasks or is there any specialization? 7. What is the scheduling process for surgeries both onsite and offsite? 8. How can we get data on the historical schedules of surgeries and tech shifts? 9. Do you feel that there is a lot of variability in the quality of work between techs? If so, who are the best/worst performers? 10. What are the key cultural issues that we need to be aware about? How have they affected work in the past? 11. Any past successes/failures in the way the techs where administered that we can draw upon? 12. Any other objectives, issues, or information that you would like to bring up? 31
35 APPENDIX E: Work Sampling Study List of Tasks Standard Tasks Room Setup/Afternoon Shutdown Initial Machine Check Cart Stocking Set-up IVs Transfer Machine/Cart Search for Equipment Cleaning Scopes/TEs Assistance Room Turnover OR Assist (sterile tray, etc) Arterial Line Placement CVP Placement Difficult Airway Intubation OR Standby Troubleshoot Equipment Transfer Patients Blood Gas Lab Testing Cell Saver Pharmacy Work Stretchers Bring Supplies Bring Equipment Additional Meeting Break/Lunch Standby/Downtime Computer Use Office Work Schedule Other Tasks Helping Another Tech [Blank] 32
36 APPENDIX F: Descriptive Statistics of Pages per Day for UH Mean StdDev Median Min 1.00 Max Range Coef of Variation
37 APPENDIX G: Descriptive Statistics of Pages per Day for Mott Mean StdDev Median Min 1.00 Max Range Coef of Variation

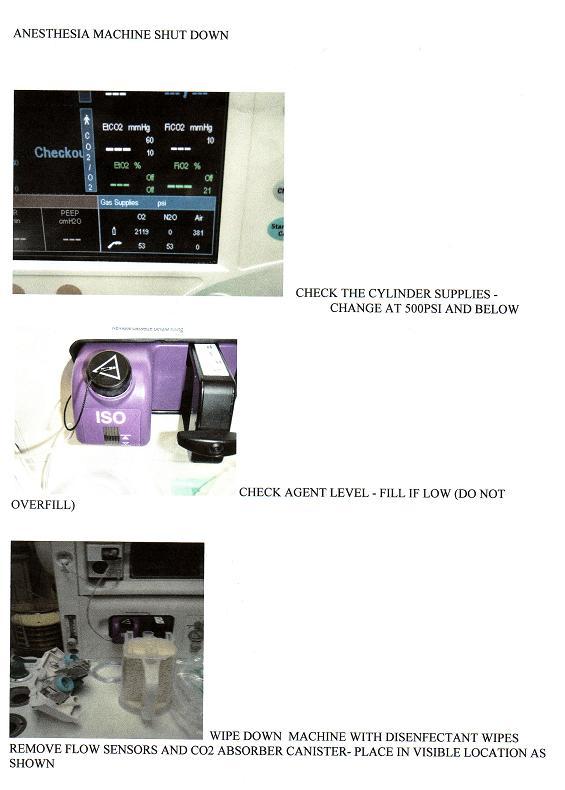
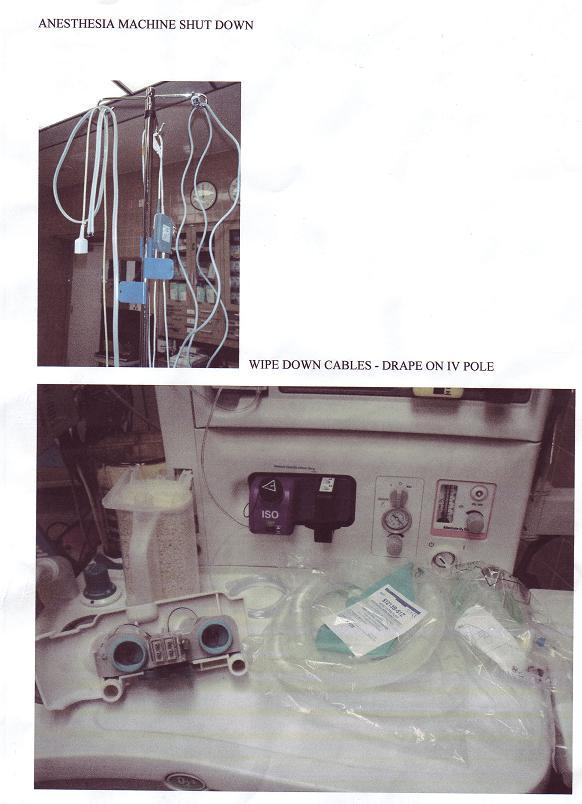
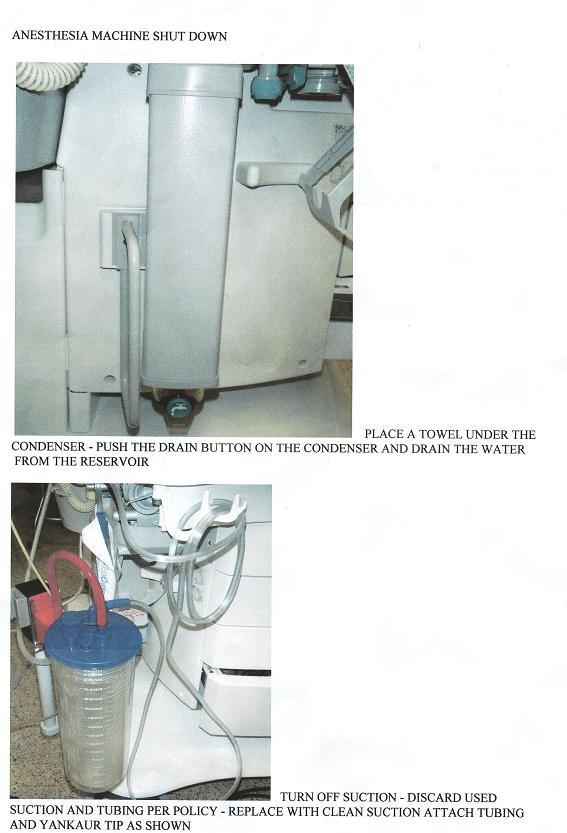
38 APPENDIX H: Anesthesia Machine Shutdown Standard Procedure 35
39 36
40 37
41 38
Analysis of Nursing Workload in Primary Care
 Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Final Report. Karen Keast Director of Clinical Operations. Jacquelynn Lapinski Senior Management Engineer
 Assessment of Room Utilization of the Interventional Radiology Division at the University of Michigan Hospital Final Report University of Michigan Health Systems Karen Keast Director of Clinical Operations
Assessment of Room Utilization of the Interventional Radiology Division at the University of Michigan Hospital Final Report University of Michigan Health Systems Karen Keast Director of Clinical Operations
Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience
 University of Michigan Health System Program and Operations Analysis Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience Final Report To: Stephen Napolitan, Assistant
University of Michigan Health System Program and Operations Analysis Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience Final Report To: Stephen Napolitan, Assistant
University of Michigan Health System. Program and Operations Analysis. CSR Staffing Process. Final Report
 University of Michigan Health System Program and Operations Analysis CSR Staffing Process Final Report To: Jean Shlafer, Director, Central Staffing Resources, Admissions Bed Coordination Center Amanda
University of Michigan Health System Program and Operations Analysis CSR Staffing Process Final Report To: Jean Shlafer, Director, Central Staffing Resources, Admissions Bed Coordination Center Amanda
The University of Michigan Health System. Geriatrics Clinic Flow Analysis Final Report
 The University of Michigan Health System Geriatrics Clinic Flow Analysis Final Report To: CC: Renea Price, Clinic Manager, East Ann Arbor Geriatrics Center Jocelyn Wiggins, MD, Medical Director, East Ann
The University of Michigan Health System Geriatrics Clinic Flow Analysis Final Report To: CC: Renea Price, Clinic Manager, East Ann Arbor Geriatrics Center Jocelyn Wiggins, MD, Medical Director, East Ann
University of Michigan Health System. Current State Analysis of the Main Adult Emergency Department
 University of Michigan Health System Program and Operations Analysis Current State Analysis of the Main Adult Emergency Department Final Report To: Jeff Desmond MD, Clinical Operations Manager Emergency
University of Michigan Health System Program and Operations Analysis Current State Analysis of the Main Adult Emergency Department Final Report To: Jeff Desmond MD, Clinical Operations Manager Emergency
Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report
 Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
University of Michigan Emergency Department
 University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Health System. Final Report
 University of Michigan Health System Program and Operations Analysis Analysis of Medication Turnaround in the 6 th Floor University Hospital Pharmacy Satellite Final Report To: Dr. Phil Brummond, Pharm.D,
University of Michigan Health System Program and Operations Analysis Analysis of Medication Turnaround in the 6 th Floor University Hospital Pharmacy Satellite Final Report To: Dr. Phil Brummond, Pharm.D,
Decreasing Environmental Services Response Times
 Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
University of Michigan Health System
 University of Michigan Health System Program and Operations Analysis Analysis of the Orthopedic Surgery Taubman Clinic Final Report To: Andrew Urquhart, MD: Orthopedic Surgeon Patrice Seymour, Administrative
University of Michigan Health System Program and Operations Analysis Analysis of the Orthopedic Surgery Taubman Clinic Final Report To: Andrew Urquhart, MD: Orthopedic Surgeon Patrice Seymour, Administrative
Michigan Medicine--Frankel Cardiovascular Center. Determining Direct Patient Utilization Costs in the Cardiovascular Clinic.
 Michigan Medicine--Frankel Cardiovascular Center Clinical Design and Innovation Determining Direct Patient Utilization Costs in the Cardiovascular Clinic Final Report Client: Mrs. Cathy Twu-Wong Project
Michigan Medicine--Frankel Cardiovascular Center Clinical Design and Innovation Determining Direct Patient Utilization Costs in the Cardiovascular Clinic Final Report Client: Mrs. Cathy Twu-Wong Project
University of Michigan Health System Programs and Operations Analysis. Order Entry Clerical Process Analysis Final Report
 University of Michigan Health System Programs and Operations Analysis Order Entry Clerical Process Analysis Final Report To: Richard J. Coffey: Director, Programs and Operations Analysis Bruce Chaffee:
University of Michigan Health System Programs and Operations Analysis Order Entry Clerical Process Analysis Final Report To: Richard J. Coffey: Director, Programs and Operations Analysis Bruce Chaffee:
Improving Patient Throughput in the Emergency Department
 University of Michigan Health System Program and Operations Analysis Improving Patient Throughput in the Emergency Department To: Jennifer Holmes, Director of Operations, Emergency Department Sam Clark,
University of Michigan Health System Program and Operations Analysis Improving Patient Throughput in the Emergency Department To: Jennifer Holmes, Director of Operations, Emergency Department Sam Clark,
EXECUTIVE SUMMARY. Introduction. Methods
 EXECUTIVE SUMMARY Introduction University of Michigan (UM) General Pediatrics offers health services to patients through nine outpatient clinics located throughout South Eastern Michigan. These clinics
EXECUTIVE SUMMARY Introduction University of Michigan (UM) General Pediatrics offers health services to patients through nine outpatient clinics located throughout South Eastern Michigan. These clinics
Analysis of Cardiovascular Patient Data during Preoperative, Operative, and Postoperative Phases
 University of Michigan College of Engineering Practicum in Hospital Systems Program and Operations Analysis Analysis of Cardiovascular Patient Data during Preoperative, Operative, and Postoperative Phases
University of Michigan College of Engineering Practicum in Hospital Systems Program and Operations Analysis Analysis of Cardiovascular Patient Data during Preoperative, Operative, and Postoperative Phases
University of Michigan Health System Program and Operations Analysis. Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients
 University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
University of Michigan Health System Program and Operations Analysis Analysis of Pre-Operation Process for UMHS Surgical Oncology Patients Final Report Draft To: Roxanne Cross, Nurse Practitioner, UMHS
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
Improving Mott Hospital Post-Operative Processes
 Improving Mott Hospital Post-Operative Processes Program and Operation Analysis Submitted To: Sheila Trouten, Client Nurse Manager, PACU, Mott OR Jesse Wilson, Coordinator Administrative Manager of Surgical
Improving Mott Hospital Post-Operative Processes Program and Operation Analysis Submitted To: Sheila Trouten, Client Nurse Manager, PACU, Mott OR Jesse Wilson, Coordinator Administrative Manager of Surgical
Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic. Final Report
 Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic Final Report Prepared for: Kathy Lash, Director of Operations University of Michigan Health System Radiation Oncology
Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic Final Report Prepared for: Kathy Lash, Director of Operations University of Michigan Health System Radiation Oncology
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Analysis of Room Allocation in the Taubman Center Clinic of Internal Medicine
 University of Michigan Health System Program and Operations Analysis Analysis of Room Allocation in the Taubman Center Clinic of Internal Medicine Final Report To: Cherie Freed, Administrative Associate
University of Michigan Health System Program and Operations Analysis Analysis of Room Allocation in the Taubman Center Clinic of Internal Medicine Final Report To: Cherie Freed, Administrative Associate
uncovering key data points to improve OR profitability
 REPRINT March 2014 Robert A. Stiefel Howard Greenfield healthcare financial management association hfma.org uncovering key data points to improve OR profitability Hospital finance leaders can increase
REPRINT March 2014 Robert A. Stiefel Howard Greenfield healthcare financial management association hfma.org uncovering key data points to improve OR profitability Hospital finance leaders can increase
University of Michigan Health System. Inpatient Tracking Analysis and Process Standardization at. Mott Children s and Women s Hospital.
 University of Michigan Health System Program and Operations Analysis Inpatient Tracking Analysis and Process Standardization at Mott Children s and Women s Hospital Final Report Team 6 To: Perry Spencer,
University of Michigan Health System Program and Operations Analysis Inpatient Tracking Analysis and Process Standardization at Mott Children s and Women s Hospital Final Report Team 6 To: Perry Spencer,
Department of Radiation Oncology
 Department of Radiation Oncology Final Report Department Analysis Management Systems Department Chad Cleveringa Chad Dejong Chris Gannon 19 April 1994 EXECUTIVE SUMMARY EXECUTIVE SUMMARY EXECUTIVE SUMMARY
Department of Radiation Oncology Final Report Department Analysis Management Systems Department Chad Cleveringa Chad Dejong Chris Gannon 19 April 1994 EXECUTIVE SUMMARY EXECUTIVE SUMMARY EXECUTIVE SUMMARY
University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process. Final Report
 University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process Final Report Submitted to: Ms. Angela Haley Ambulatory Care Manager, Department of Surgery 1540 E Medical
University of Michigan Health System Analysis of Wait Times Through the Patient Preoperative Process Final Report Submitted to: Ms. Angela Haley Ambulatory Care Manager, Department of Surgery 1540 E Medical
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Emergency Services. Time Study
 Prepared for: Peter Forster Management Systems University of Michigan Hospitals December 18,1991 by: Associate Hospital Administrator Emergency Services Ann Arbor, MI Don Suffivan Jeremy Roberts Lisa Clayton
Prepared for: Peter Forster Management Systems University of Michigan Hospitals December 18,1991 by: Associate Hospital Administrator Emergency Services Ann Arbor, MI Don Suffivan Jeremy Roberts Lisa Clayton
Click to edit Master subtitle style
 Operating Room Turnover Analysis and Improvement Click to edit Master title style Click to edit Master subtitle style Reza Maleki and Melissa Kram Department of Industrial and Manufacturing Engineering
Operating Room Turnover Analysis and Improvement Click to edit Master title style Click to edit Master subtitle style Reza Maleki and Melissa Kram Department of Industrial and Manufacturing Engineering
University of Michigan Health System
 University of Michigan Health System Programs and Operations Analysis Analysis of the Discharge Process at Internal Medicine Unit B Department of Internal Medicine Final Report To: Dr. Christopher Kim,
University of Michigan Health System Programs and Operations Analysis Analysis of the Discharge Process at Internal Medicine Unit B Department of Internal Medicine Final Report To: Dr. Christopher Kim,
Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital. Final Report. Submitted To:
 Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital Final Report Submitted To: Cathy Lewis, MSN, RN Clinical Nurse Specialist and Adjunct Clinical Instructor
Validating Pilot Program to Improve Discharge Medication in 12 West at C.S. Mott Children s Hospital Final Report Submitted To: Cathy Lewis, MSN, RN Clinical Nurse Specialist and Adjunct Clinical Instructor
University of Michigan Health System. Analysis of the Patient Admission Process in The University of Michigan Hospital Final Report
 University of Michigan Health System Analysis of the Patient Admission Process in The University of Michigan Hospital Final Report Submitted to: Lori Lathers Training Specialist Senior UMHS, Central Staffing
University of Michigan Health System Analysis of the Patient Admission Process in The University of Michigan Hospital Final Report Submitted to: Lori Lathers Training Specialist Senior UMHS, Central Staffing
Report on the Pilot Survey on Obtaining Occupational Exposure Data in Interventional Cardiology
 Report on the Pilot Survey on Obtaining Occupational Exposure Data in Interventional Cardiology Working Group on Interventional Cardiology (WGIC) Information System on Occupational Exposure in Medicine,
Report on the Pilot Survey on Obtaining Occupational Exposure Data in Interventional Cardiology Working Group on Interventional Cardiology (WGIC) Information System on Occupational Exposure in Medicine,
Establishing a Monitoring Process For Inpatient Room Cleaning at Discharge. Final Report
 Environmental Services and Infection Control & Epidemiology, University of Michigan Hospital Establishing a Monitoring Process For Inpatient Room Cleaning at Discharge Final Report December 13, 2010 To:
Environmental Services and Infection Control & Epidemiology, University of Michigan Hospital Establishing a Monitoring Process For Inpatient Room Cleaning at Discharge Final Report December 13, 2010 To:
University of Michigan Health System Program and Operations Analysis. Analysis of Problem Summary List and Medication Reconciliation Final Report
 University of Michigan Health System Program and Operations Analysis Analysis of Problem Summary List and Medication Reconciliation Final Report To: John Clark, PharmD, MS, University of Michigan Health
University of Michigan Health System Program and Operations Analysis Analysis of Problem Summary List and Medication Reconciliation Final Report To: John Clark, PharmD, MS, University of Michigan Health
INTRADEPARTMENTAL CORRESPONDENCE. June 7, 2016 BPC #
 INTRADEPARTMENTAL CORRESPONDENCE June 7, 2016 BPC #16-0173 1.0 TO: The Honorable Board of Police Commissioners FROM: Inspector General, Police Commission SUBJECT: OFFICE OF THE INSPECTOR GENERAL INVESTIGATION
INTRADEPARTMENTAL CORRESPONDENCE June 7, 2016 BPC #16-0173 1.0 TO: The Honorable Board of Police Commissioners FROM: Inspector General, Police Commission SUBJECT: OFFICE OF THE INSPECTOR GENERAL INVESTIGATION
Quality Management Building Blocks
 Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Contents. Page 1 of 42
 Contents Using PIMS to Provide Evidence of Compliance... 3 Tips for Monitoring PIMS Data Related to Standard... 3 Example 1 PIMS02: Total numbers of screens by referral source... 4 Example 2 Custom Report
Contents Using PIMS to Provide Evidence of Compliance... 3 Tips for Monitoring PIMS Data Related to Standard... 3 Example 1 PIMS02: Total numbers of screens by referral source... 4 Example 2 Custom Report
Full-time Equivalents and Financial Costs Associated with Absenteeism, Overtime, and Involuntary Part-time Employment in the Nursing Profession
 Full-time Equivalents and Financial Costs Associated with Absenteeism, Overtime, and Involuntary Part-time Employment in the Nursing Profession A Report prepared for the Canadian Nursing Advisory Committee
Full-time Equivalents and Financial Costs Associated with Absenteeism, Overtime, and Involuntary Part-time Employment in the Nursing Profession A Report prepared for the Canadian Nursing Advisory Committee
Demand and capacity models High complexity model user guidance
 Demand and capacity models High complexity model user guidance August 2018 Published by NHS Improvement and NHS England Contents 1. What is the demand and capacity high complexity model?... 2 2. Methodology...
Demand and capacity models High complexity model user guidance August 2018 Published by NHS Improvement and NHS England Contents 1. What is the demand and capacity high complexity model?... 2 2. Methodology...
A Comparison of Job Responsibility and Activities between Registered Dietitians with a Bachelor's Degree and Those with a Master's Degree
 Florida International University FIU Digital Commons FIU Electronic Theses and Dissertations University Graduate School 11-17-2010 A Comparison of Job Responsibility and Activities between Registered Dietitians
Florida International University FIU Digital Commons FIU Electronic Theses and Dissertations University Graduate School 11-17-2010 A Comparison of Job Responsibility and Activities between Registered Dietitians
An academic medical center is practicing wasteology to pare time, expense,
 Quality improvement Practicing wasteology in the OR An academic medical center is practicing wasteology to pare time, expense, and hassle from its OR processes. Using lean thinking, the center is streamlining
Quality improvement Practicing wasteology in the OR An academic medical center is practicing wasteology to pare time, expense, and hassle from its OR processes. Using lean thinking, the center is streamlining
From Big Data to Big Knowledge Optimizing Medication Management
 From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
UNIVERSITY OF CALIFORNIA, DAVIS AUDIT AND MANAGEMENT ADVISORY SERVICES. Counseling Services Audit & Management Advisory Services Project #17-67
 , DAVIS AUDIT AND MANAGEMENT ADVISORY SERVICES Counseling Services Audit & Management Advisory Services Project #17-67 December 2017 Fieldwork Performed by: Ryan Dickson, Senior Auditor Reviewed by: Tony
, DAVIS AUDIT AND MANAGEMENT ADVISORY SERVICES Counseling Services Audit & Management Advisory Services Project #17-67 December 2017 Fieldwork Performed by: Ryan Dickson, Senior Auditor Reviewed by: Tony
University of Michigan Health System MiChart Department Improving Operating Room Case Time Accuracy Final Report
 University of Michigan Health System MiChart Department Improving Operating Room Case Time Accuracy Final Report Submitted To: Clients Jeffrey Terrell, MD: Associate Chief Medical Information Officer Deborah
University of Michigan Health System MiChart Department Improving Operating Room Case Time Accuracy Final Report Submitted To: Clients Jeffrey Terrell, MD: Associate Chief Medical Information Officer Deborah
THE USE OF SIMULATION TO DETERMINE MAXIMUM CAPACITY IN THE SURGICAL SUITE OPERATING ROOM. Sarah M. Ballard Michael E. Kuhl
 Proceedings of the 2006 Winter Simulation Conference L. F. Perrone, F. P. Wieland, J. Liu, B. G. Lawson, D. M. Nicol, and R. M. Fujimoto, eds. THE USE OF SIMULATION TO DETERMINE MAXIMUM CAPACITY IN THE
Proceedings of the 2006 Winter Simulation Conference L. F. Perrone, F. P. Wieland, J. Liu, B. G. Lawson, D. M. Nicol, and R. M. Fujimoto, eds. THE USE OF SIMULATION TO DETERMINE MAXIMUM CAPACITY IN THE
University of Michigan Health System
 University of Michigan Health System Program and Operations Analysis Utilization Study of Linear Accelerators in the Radiation Oncology Department Project Report To: Kathy Lash: Director of Operations
University of Michigan Health System Program and Operations Analysis Utilization Study of Linear Accelerators in the Radiation Oncology Department Project Report To: Kathy Lash: Director of Operations
INPATIENT SURVEY PSYCHOMETRICS
 INPATIENT SURVEY PSYCHOMETRICS One of the hallmarks of Press Ganey s surveys is their scientific basis: our products incorporate the best characteristics of survey design. Our surveys are developed by
INPATIENT SURVEY PSYCHOMETRICS One of the hallmarks of Press Ganey s surveys is their scientific basis: our products incorporate the best characteristics of survey design. Our surveys are developed by
2013 Physician Inpatient/ Outpatient Revenue Survey
 Physician Inpatient/ Outpatient Revenue Survey A survey showing net annual inpatient and outpatient revenue generated by physicians in various specialties on behalf of their affiliated hospitals Merritt
Physician Inpatient/ Outpatient Revenue Survey A survey showing net annual inpatient and outpatient revenue generated by physicians in various specialties on behalf of their affiliated hospitals Merritt
Oklahoma Health Care Authority. ECHO Adult Behavioral Health Survey For SoonerCare Choice
 Oklahoma Health Care Authority ECHO Adult Behavioral Health Survey For SoonerCare Choice Executive Summary and Technical Specifications Report for Report Submitted June 2009 Submitted by: APS Healthcare
Oklahoma Health Care Authority ECHO Adult Behavioral Health Survey For SoonerCare Choice Executive Summary and Technical Specifications Report for Report Submitted June 2009 Submitted by: APS Healthcare
National Patient Experience Survey Mater Misericordiae University Hospital.
 National Patient Experience Survey 2017 Mater Misericordiae University Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017,
National Patient Experience Survey 2017 Mater Misericordiae University Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017,
Eugene Police Department
 Comprehensive Staffing Needs Projection Eugene Police Department Final Report Submitted by: Magellan Research Corporation April 2007 Table of Contents Introduction 1 Current Level of Police Service in
Comprehensive Staffing Needs Projection Eugene Police Department Final Report Submitted by: Magellan Research Corporation April 2007 Table of Contents Introduction 1 Current Level of Police Service in
Exemplary Professional Practice: Staffing Scheduling and Budgeting Processes
 Exemplary Professional Practice: Staffing Scheduling and geting Processes EP10 Nurses use trended data in the budgeting process, with clinical nurse input, to redistribute existing nursing resources or
Exemplary Professional Practice: Staffing Scheduling and geting Processes EP10 Nurses use trended data in the budgeting process, with clinical nurse input, to redistribute existing nursing resources or
CITY OF GRANTS PASS SURVEY
 CITY OF GRANTS PASS SURVEY by Stephen M. Johnson OCTOBER 1998 OREGON SURVEY RESEARCH LABORATORY UNIVERSITY OF OREGON EUGENE OR 97403-5245 541-346-0824 fax: 541-346-5026 Internet: OSRL@OREGON.UOREGON.EDU
CITY OF GRANTS PASS SURVEY by Stephen M. Johnson OCTOBER 1998 OREGON SURVEY RESEARCH LABORATORY UNIVERSITY OF OREGON EUGENE OR 97403-5245 541-346-0824 fax: 541-346-5026 Internet: OSRL@OREGON.UOREGON.EDU
7 NON-ELECTIVE SURGERY IN THE NHS
 Recommendations Debate whether, in the light of changes to the pattern of junior doctors working, non-essential surgery can take place during extended hours. 7 NON-ELECTIVE SURGERY IN THE NHS Ensure that
Recommendations Debate whether, in the light of changes to the pattern of junior doctors working, non-essential surgery can take place during extended hours. 7 NON-ELECTIVE SURGERY IN THE NHS Ensure that
ADMINISTRATIVE SUMMARY OF INVESTIGATION BY THE VA OFFICE OF INSPECTOR GENERAL IN RESPONSE TO ALLEGATIONS REGARDING PATIENT WAIT TIMES
 ADMINISTRATIVE SUMMARY OF INVESTIGATION BY THE VA OFFICE OF INSPECTOR GENERAL IN RESPONSE TO ALLEGATIONS REGARDING PATIENT WAIT TIMES VA Medical Center in Wilmington, Delaware March 1, 2016 1. Summary
ADMINISTRATIVE SUMMARY OF INVESTIGATION BY THE VA OFFICE OF INSPECTOR GENERAL IN RESPONSE TO ALLEGATIONS REGARDING PATIENT WAIT TIMES VA Medical Center in Wilmington, Delaware March 1, 2016 1. Summary
Getting the right case in the right room at the right time is the goal for every
 OR throughput Are your operating rooms efficient? Getting the right case in the right room at the right time is the goal for every OR director. Often, though, defining how well the OR suite runs depends
OR throughput Are your operating rooms efficient? Getting the right case in the right room at the right time is the goal for every OR director. Often, though, defining how well the OR suite runs depends
Employee Telecommuting Study
 Employee Telecommuting Study June Prepared For: Valley Metro Valley Metro Employee Telecommuting Study Page i Table of Contents Section: Page #: Executive Summary and Conclusions... iii I. Introduction...
Employee Telecommuting Study June Prepared For: Valley Metro Valley Metro Employee Telecommuting Study Page i Table of Contents Section: Page #: Executive Summary and Conclusions... iii I. Introduction...
Evaluation of NHS111 pilot sites. Second Interim Report
 Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
2016 REPORT Community Care for the Elderly (CCE) Client Satisfaction Survey
 Client Satisfaction Survey") 2016 REPORT Community Care for the Elderly (CCE) Client Satisfaction Survey Program Services, Direct Service Workers, and Impact of Program on Lives of Clients i Florida Department of Elder Affairs, 2016
2016 REPORT Community Care for the Elderly (CCE) Client Satisfaction Survey Program Services, Direct Service Workers, and Impact of Program on Lives of Clients i Florida Department of Elder Affairs, 2016
GAO. DEFENSE BUDGET Trends in Reserve Components Military Personnel Compensation Accounts for
 GAO United States General Accounting Office Report to the Chairman, Subcommittee on National Security, Committee on Appropriations, House of Representatives September 1996 DEFENSE BUDGET Trends in Reserve
GAO United States General Accounting Office Report to the Chairman, Subcommittee on National Security, Committee on Appropriations, House of Representatives September 1996 DEFENSE BUDGET Trends in Reserve
Disclosure. Do One More Case. Focusing on turnover time will improve OR throughput. Myths in Economics of Anesthesia Confirmed, Plausible, or Busted?
 Disclosure ECG Consultants Technical Advisor Focus on Staffing Models Amr Abouleish, MD, MBA Department of Anesthesiology The University of Texas Medical Branch Galveston, Texas aaboulei@utmb.edu throughput.
Disclosure ECG Consultants Technical Advisor Focus on Staffing Models Amr Abouleish, MD, MBA Department of Anesthesiology The University of Texas Medical Branch Galveston, Texas aaboulei@utmb.edu throughput.
ORGANIZATIONAL INFORMATION BRIEF SUMMARY OF THE PROBLEM
 F E L L O W P R O J E C T Implementation of a Contractual Relationship for Anesthesia Services in an Acute Care Facility Marcia Taylor, R.N., M.B.A., FACHE, director of surgical service, Rapid City Regional
F E L L O W P R O J E C T Implementation of a Contractual Relationship for Anesthesia Services in an Acute Care Facility Marcia Taylor, R.N., M.B.A., FACHE, director of surgical service, Rapid City Regional
A Qualitative Study of Master Patient Index (MPI) Record Challenges from Health Information Management Professionals Perspectives
 Record Challenges from Health Information Management Professionals Perspectives") A Qualitative Study of Master Patient Index (MPI) Record Challenges from Health Information Management Professionals Perspectives by Joe Lintz, MS, RHIA Abstract This study aimed gain a better understanding
A Qualitative Study of Master Patient Index (MPI) Record Challenges from Health Information Management Professionals Perspectives by Joe Lintz, MS, RHIA Abstract This study aimed gain a better understanding
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Nursing and Personal Care: Funding Increase Survey
 Nursing and Personal Care: Funding Increase Survey Prepared for: Ministry of Health and Long-Term Care Long Term Care Facilities Branch 5 th Floor, Hepburn Block 80 Grosvenor Street Toronto, Ontario Prepared
Nursing and Personal Care: Funding Increase Survey Prepared for: Ministry of Health and Long-Term Care Long Term Care Facilities Branch 5 th Floor, Hepburn Block 80 Grosvenor Street Toronto, Ontario Prepared
STATEMENT ON THE ANESTHESIA CARE TEAM
 Committee of Origin: Anesthesia Care Team (Approved by the ASA House of Delegates on October 18, 2006, and last amended on October 21, 2009) Anesthesiology is the practice of medicine including, but not
Committee of Origin: Anesthesia Care Team (Approved by the ASA House of Delegates on October 18, 2006, and last amended on October 21, 2009) Anesthesiology is the practice of medicine including, but not
DIRECT CARE STAFF ADJUSTMENT REPORT MEDICAID-PARTICIPATING NURSING HOMES
 DIRECT CARE STAFF ADJUSTMENT REPORT MEDICAID-PARTICIPATING NURSING HOMES Division of Medicaid Agency for Health Care Administration March 2001 TABLE OF CONTENTS Background... 1 Implementation... 1 Methodology...
DIRECT CARE STAFF ADJUSTMENT REPORT MEDICAID-PARTICIPATING NURSING HOMES Division of Medicaid Agency for Health Care Administration March 2001 TABLE OF CONTENTS Background... 1 Implementation... 1 Methodology...
University of Michigan Comprehensive Stroke Center
 University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
University of Michigan Comprehensive Stroke Center Improving the Discharge and Post-Discharge Process Flow Final Report Date: April 18, 2017 To: Jenevra Foley, Operating Director of Stroke Center, jenevra@med.umich.edu
UNC2 Practice Test. Select the correct response and jot down your rationale for choosing the answer.
 UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
Improving Access to Pediatric MR performed under General Anesthesia Benefits of a Rapid Improvement Event (RIE)
") /3/207 Improving Access to Pediatric MR performed under General Anesthesia Benefits of a Rapid Improvement Event (RIE) N I Sarwani, MD, FRCR, FSAR M A Bruno, MS, MD, FACR S Mrozowski, MHA, NRP, CPPS Corresponding
/3/207 Improving Access to Pediatric MR performed under General Anesthesia Benefits of a Rapid Improvement Event (RIE) N I Sarwani, MD, FRCR, FSAR M A Bruno, MS, MD, FACR S Mrozowski, MHA, NRP, CPPS Corresponding
Patient Blood Management Certification Program. Review Process Guide. For Organizations
 Patient Blood Management Certification Program Review Process Guide For Organizations 2018 What's New in 2018 Updates effective in 2018 are identified by underlined text in the activities noted below.
Patient Blood Management Certification Program Review Process Guide For Organizations 2018 What's New in 2018 Updates effective in 2018 are identified by underlined text in the activities noted below.
Society for Health Systems Conference February 20 21, 2004 A Methodology to Analyze Staffing and Utilization in the Operating Room
 Society for Health Systems Conference February 20 21, 2004 A Methodology to Analyze Staffing and Utilization in the Operating Room For questions about this report, please call Mary Coniglio, Director,
Society for Health Systems Conference February 20 21, 2004 A Methodology to Analyze Staffing and Utilization in the Operating Room For questions about this report, please call Mary Coniglio, Director,
Introduction. Staffing to demand increases bottom line revenue for the facility through increased volume and throughput and elimination of waste.
 Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
University of Michigan Health System. Analysis of the Central Intake Process at University of Michigan Home Care Services
 University of Michigan Health System Program and Operations Analysis Analysis of the Central Intake Process at University of Michigan Home Care Services Final Report To: Kenneth Bandy, Director, Home Care
University of Michigan Health System Program and Operations Analysis Analysis of the Central Intake Process at University of Michigan Home Care Services Final Report To: Kenneth Bandy, Director, Home Care
How to implement GP triage
 CHANGE PACKAGE How to implement GP triage What is GP triage? Receptionists receiving calls from patients asking for a same-day appointment offer the option of a doctor ringing them back. A GP then contacts
CHANGE PACKAGE How to implement GP triage What is GP triage? Receptionists receiving calls from patients asking for a same-day appointment offer the option of a doctor ringing them back. A GP then contacts
INCREASE ACCESS TO PRIMARY CARE SERVICES BY ALLOWING ADVANCED PRACTICE REGISTERED NURSES TO PRESCRIBE
 INCREASE ACCESS TO PRIMARY CARE SERVICES BY ALLOWING ADVANCED PRACTICE REGISTERED NURSES TO PRESCRIBE Both nationally and in Texas, advanced practice registered nurses have helped mitigate the effects
INCREASE ACCESS TO PRIMARY CARE SERVICES BY ALLOWING ADVANCED PRACTICE REGISTERED NURSES TO PRESCRIBE Both nationally and in Texas, advanced practice registered nurses have helped mitigate the effects
University of Michigan Health System. Inpatient Cardiology Unit Analysis: Collect, Categorize and Quantify Delays for Procedures Final Report
 Project University of Michigan Health System Program and Operations Analysis Inpatient Cardiology Unit Analysis: Collect, Categorize and Quantify Delays for Procedures Final Report To: Dr. Robert Cody,
Project University of Michigan Health System Program and Operations Analysis Inpatient Cardiology Unit Analysis: Collect, Categorize and Quantify Delays for Procedures Final Report To: Dr. Robert Cody,
LV Prasad Eye Institute Final Presentation
 LV Prasad Eye Institute Final Presentation Ali Kamil, Dmitriy Lyan, Nicole Yap, MIT Student MIT Sloan School of Management Global Health Lab May 8, 2013 1 Courtesy of Ali S. Kamil, Dmitriy E. Lyan, Nicole
LV Prasad Eye Institute Final Presentation Ali Kamil, Dmitriy Lyan, Nicole Yap, MIT Student MIT Sloan School of Management Global Health Lab May 8, 2013 1 Courtesy of Ali S. Kamil, Dmitriy E. Lyan, Nicole
A Study to Assess Patient Safety Culture amongst a Category of Hospital Staff of a Teaching Hospital
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 16-22 A Study to Assess Patient Safety Culture amongst a Category
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 16-22 A Study to Assess Patient Safety Culture amongst a Category
Patient Centric Model (PCM)
") Patient Centric Model (PCM) Operations Manual A product of your state pharmacy association For more information, contact: PCM Project Manager 804-285-4431 PCM@naspa.us Background The typical pharmacy model
Patient Centric Model (PCM) Operations Manual A product of your state pharmacy association For more information, contact: PCM Project Manager 804-285-4431 PCM@naspa.us Background The typical pharmacy model
North West Ambulance Service
 North West Ambulance Service Final Insight Summary Report July 2013 www.icegroupuk.com 1 ICE Creates and the North West Ambulance Service would like to thank the many people who have contributed to this
North West Ambulance Service Final Insight Summary Report July 2013 www.icegroupuk.com 1 ICE Creates and the North West Ambulance Service would like to thank the many people who have contributed to this
Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting
 Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting How many times have we heard that it s easy to apply Lean and Six Sigma techniques to hospital processes, and specifically
Using Lean, Six Sigma to Improve Surgical Services James Pearson J.O.P. Consulting How many times have we heard that it s easy to apply Lean and Six Sigma techniques to hospital processes, and specifically
Pediatric Hematology / Oncology Clinic
 Pediatric Hematology / Oncology Clinic Final Report for Analysis of Operations April 13, 1995 Program and Operations Analysis Project Team Cristina Bermudez Katherine Horvath Julie Pinsky Seth Roseman
Pediatric Hematology / Oncology Clinic Final Report for Analysis of Operations April 13, 1995 Program and Operations Analysis Project Team Cristina Bermudez Katherine Horvath Julie Pinsky Seth Roseman
Goals and Objectives University of Minnesota Department of Anesthesiology Senior Resident Supervising Rotation
 UM Anesthesiology Page 1 June, 2007 Introduction Goals and Objectives University of Minnesota Department of Anesthesiology Senior Resident Supervising Rotation The ABA defines the attributes of consultant
UM Anesthesiology Page 1 June, 2007 Introduction Goals and Objectives University of Minnesota Department of Anesthesiology Senior Resident Supervising Rotation The ABA defines the attributes of consultant
Negotiating a Hospital Anesthesia Financial Support Agreement
 Negotiating a Hospital Anesthesia Financial Support Agreement Negotiating a Hospital Anesthesia Financial Support Agreement 1 SUMMARY AT A GLANCE: Most anesthesia groups need to create or update agreements
Negotiating a Hospital Anesthesia Financial Support Agreement Negotiating a Hospital Anesthesia Financial Support Agreement 1 SUMMARY AT A GLANCE: Most anesthesia groups need to create or update agreements
The Benefits of Standardization: Anesthesia Cart Standardization in 62 Operating Rooms Over 5 Surgical Sites
 The Benefits of Standardization: Anesthesia Cart Standardization in 62 Operating Rooms Over 5 Surgical Sites By Abdul N. Mansour, MHA, DBA, Scottsdale Healthcare August 2011 One of Arizona s largest health
The Benefits of Standardization: Anesthesia Cart Standardization in 62 Operating Rooms Over 5 Surgical Sites By Abdul N. Mansour, MHA, DBA, Scottsdale Healthcare August 2011 One of Arizona s largest health
ResearcH JournaL 2012 / VOL
 ResearcH JournaL 2012 / VOL 04.02 www.perkinswill.com The Impact of an Operational Process on Space 05. THE IMPACT OF AN OPERATIONAL PROCESS ON SPACE: Improving the Efficiency of Patient Wait Times Amanda
ResearcH JournaL 2012 / VOL 04.02 www.perkinswill.com The Impact of an Operational Process on Space 05. THE IMPACT OF AN OPERATIONAL PROCESS ON SPACE: Improving the Efficiency of Patient Wait Times Amanda
Engaging Students Using Mastery Level Assignments Leads To Positive Student Outcomes
 Lippincott NCLEX-RN PassPoint NCLEX SUCCESS L I P P I N C O T T F O R L I F E Case Study Engaging Students Using Mastery Level Assignments Leads To Positive Student Outcomes Senior BSN Students PassPoint
Lippincott NCLEX-RN PassPoint NCLEX SUCCESS L I P P I N C O T T F O R L I F E Case Study Engaging Students Using Mastery Level Assignments Leads To Positive Student Outcomes Senior BSN Students PassPoint
Organization Review Process Guide Perinatal Care Certification
 Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
PEDIATRIC DENTIST. Dental Receptionist Manual
 PEDIATRIC DENTIST Dental Receptionist Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
PEDIATRIC DENTIST Dental Receptionist Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
Frequently Asked Questions: Anesthesiology Review Committee for Anesthesiology ACGME
 Frequently Asked Questions: Anesthesiology Review Committee for Anesthesiology ACGME Question Institutions What does the Review Committee mean that residents not should be required to rotate among multiple
Frequently Asked Questions: Anesthesiology Review Committee for Anesthesiology ACGME Question Institutions What does the Review Committee mean that residents not should be required to rotate among multiple
An Analysis of Waiting Time Reduction in a Private Hospital in the Middle East
 University of Tennessee Health Science Center UTHSC Digital Commons Applied Research Projects Department of Health Informatics and Information Management 2014 An Analysis of Waiting Time Reduction in a
University of Tennessee Health Science Center UTHSC Digital Commons Applied Research Projects Department of Health Informatics and Information Management 2014 An Analysis of Waiting Time Reduction in a
PANELS AND PANEL EQUITY
 PANELS AND PANEL EQUITY Our patients are very clear about what they want: the opportunity to choose a primary care provider access to that PCP when they choose a quality healthcare experience a good value
PANELS AND PANEL EQUITY Our patients are very clear about what they want: the opportunity to choose a primary care provider access to that PCP when they choose a quality healthcare experience a good value
The introduction of the first freestanding ambulatory
 Epidemiology of Ambulatory Anesthesia for Children in the United States: and 1996 Jennifer A. Rabbitts, MB, ChB,* Cornelius B. Groenewald, MB, ChB,* James P. Moriarty, MSc, and Randall Flick, MD, MPH*
Epidemiology of Ambulatory Anesthesia for Children in the United States: and 1996 Jennifer A. Rabbitts, MB, ChB,* Cornelius B. Groenewald, MB, ChB,* James P. Moriarty, MSc, and Randall Flick, MD, MPH*
Quick Guide to A3 Problem Solving
 Quick Guide to A3 Problem Solving What is it? Toyota Motor Corporation is famed for its ability to relentlessly improve operational performance. Central to this ability is the training of engineers, supervisors
Quick Guide to A3 Problem Solving What is it? Toyota Motor Corporation is famed for its ability to relentlessly improve operational performance. Central to this ability is the training of engineers, supervisors
Moving to 12-hour shift patterns:
 Moving to 12-hour shift patterns: to increase continuity and reduce costs Provided by: Basingstoke and North Hampshire NHS Foundation Trust Publication type: Quality and productivity example QIPP Evidence
Moving to 12-hour shift patterns: to increase continuity and reduce costs Provided by: Basingstoke and North Hampshire NHS Foundation Trust Publication type: Quality and productivity example QIPP Evidence
California Community Clinics
 California Community Clinics A Financial and Operational Profile, 2008 2011 Prepared by Sponsored by Blue Shield of California Foundation and The California HealthCare Foundation TABLE OF CONTENTS Introduction
California Community Clinics A Financial and Operational Profile, 2008 2011 Prepared by Sponsored by Blue Shield of California Foundation and The California HealthCare Foundation TABLE OF CONTENTS Introduction
PRE-SURVEY QUESTIONNAIRE AND SELF-ASSESSMENT CHECKLIST FOR ACCREDITATION OF: POSTGRADUATE YEAR ONE (PGY1) COMMUNITY PHARMACY RESIDENCY PROGRAMS
 COMMUNITY PHARMACY RESIDENCY PROGRAMS") PRE-SURVEY QUESTIONNAIRE AND SELF-ASSESSMENT CHECKLIST FOR ACCREDITATION OF: POSTGRADUATE YEAR ONE (PGY1) COMMUNITY PHARMACY RESIDENCY PROGRAMS PURPOSE The pre-survey questionnaire serves to maximize the
PRE-SURVEY QUESTIONNAIRE AND SELF-ASSESSMENT CHECKLIST FOR ACCREDITATION OF: POSTGRADUATE YEAR ONE (PGY1) COMMUNITY PHARMACY RESIDENCY PROGRAMS PURPOSE The pre-survey questionnaire serves to maximize the
MaRS 2017 Venture Client Annual Survey - Methodology
 MaRS 2017 Venture Client Annual Survey - Methodology JUNE 2018 TABLE OF CONTENTS Types of Data Collected... 2 Software and Logistics... 2 Extrapolation... 3 Response rates... 3 Item non-response... 4 Follow-up
MaRS 2017 Venture Client Annual Survey - Methodology JUNE 2018 TABLE OF CONTENTS Types of Data Collected... 2 Software and Logistics... 2 Extrapolation... 3 Response rates... 3 Item non-response... 4 Follow-up